While Skin/Mucosal Breaches May Increase the Absorption of Anesthetic Agents, MethemoglobinemiaMay Occur Due to Either a Previously-Undiagnosed Methemoglobin Reductase Enzyme Deficiency or Idiosyncratic Toxicity
Dapsone is a Well-Documented Etiology of Methemoglobinemia (Liver Transpl Surg, 1997) [MEDLINE] (Pharmacother, 1998) [MEDLINE] (Pharmacother, 2011) [MEDLINE] (Intern Med, 2015) [MEDLINE] (Cureus, 2021) [MEDLINE]
Methemoglobinemia is Known to Occur More Frequently with Dapsone Doses >200 mg/day (and Dapsone-Induced Development of Methemoglobinemia is Dose-Dependent)
Induction of Dapsone Tolerance
Cimetidine May Be Used to Chronically Enhance Dapsone Tolerance, as it is a Selective Inhibitor of N-Hydroxylation and Chronically Lowers Methemoglobin Levels by >25% (see Cimetidine)
Ingestion of Fava Beans in a Patient with G6PD Deficiency (see Favism)
At High Doses, Methylene Blue Functions as an Oxidant: it can cause acute hemolysis in patients with G6PD deficiency -> further decreasing oxygen delivery
At High Doses, Methylene Blue Can also Paradoxically Cause Methemoglobinemia
Cases of Combined Oxidative Hemolysis and Methemoglobinemia Have Been Reported with the Use of Rasburicase in the Setting of G6PD Deficiency (Acta Haematol, 2013) [MEDLINE] (see Glucose-6-Phosphate Dehydrogenase Deficiency)
Patients with Low Inherited or Acquired Catalase Activity May Be at Risk for Methemoglobinemia After Rasburicase Administration (Due to the Formation of Hydrogen Peroxide)
Some Experts Recommend the Measurement of Catalase Activity Before Administering Rasburicase
Red Blood Cells in Cirrhotic Patients Undergo Severe Oxidative Stress, Especially in the Setting of Bleeding Complications
Levels of Methemoglobin are Significantly Higher in the Red Blood Cells of Bleeding Cirrhotics than in Non-Bleeding Cirrhotics (Indian J Med Res, 2007) [MEDLINE]
Methemoglobin Levels May Increase in Sepsis (Acta Anaesthesiol Scand, 1998) [MEDLINE]
Physiology
May Be Related to the Synthesis of Nitric Oxide Which Occurs in Sepsis: nitric oxide is converted to methemoglobin and nitrate
Physiology
Normal Physiologic Conversion of Hemoglobin to Methemoglobin
As Part of Normal Physiology, Iron within Hemoglobin is Normally Auto-Oxidized at a Low Rate of 0.5-3.0% Per Day from its Ferrous (Fe2+) State (i.e. within Hemoglobin) to a Ferric (Fe3+) State (i.e. within Methemoglobin)
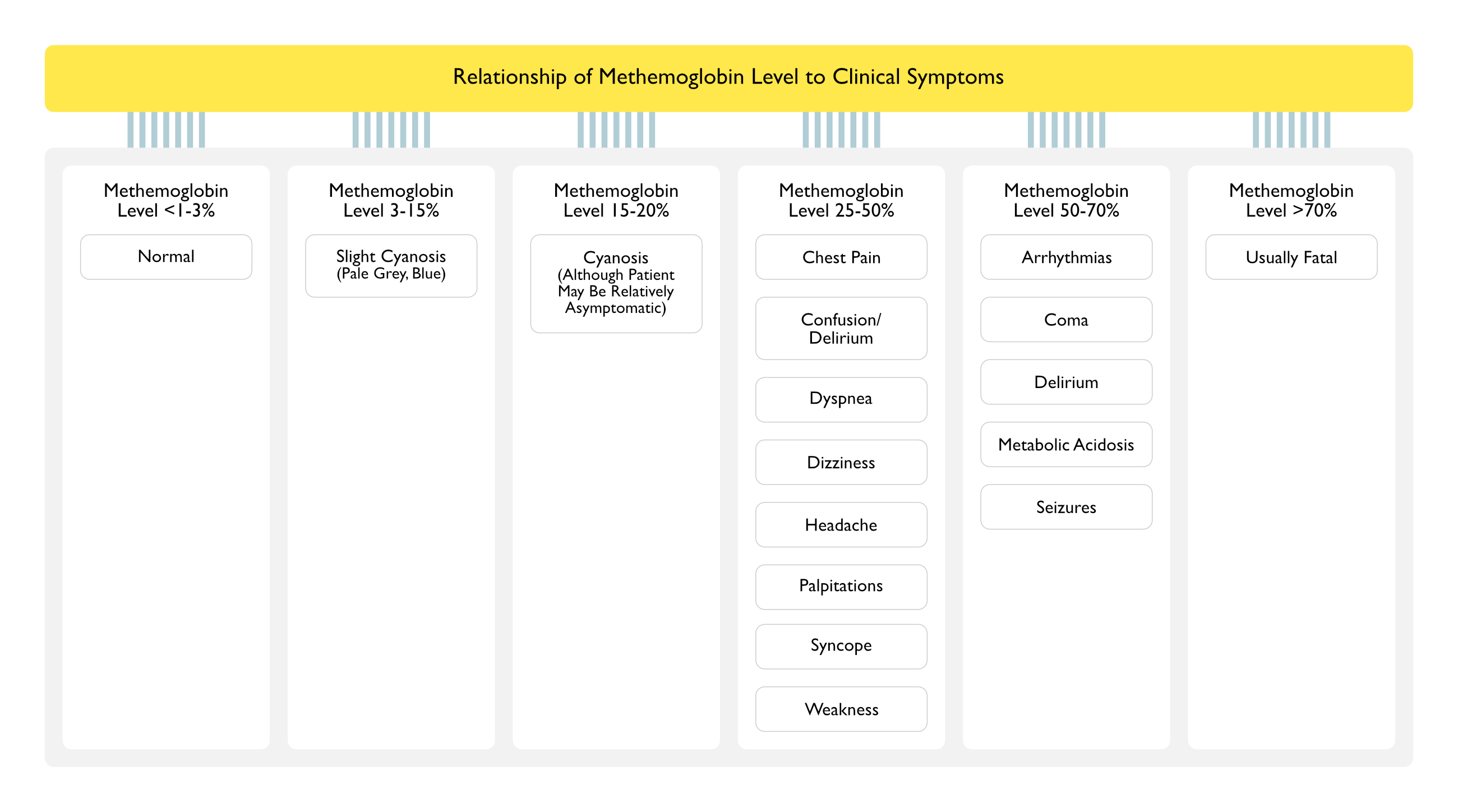
Consequently, Methemoglobin Levels of <1-3% are Considered Normal
Two Potential Chemical Mechanisms Exist to Reduce Methemoglobin Back to Hemoglobin
NADH-Dependent Reaction Catalyzed by Cytochrome b5 Reductase (b5R)
This is the Only Physiologically Important Mechanism Under Normal Conditions (Accounting for Clearance of 95-99% of the Methemoglobin That is Produced Under Normal Circumstances)
Generation of NADPH by Glucose-6-Phosphate Dehydrogenase (G6PD) in the Hexose Monophosphate Shunt within the Red Blood Cell
This Mechanism is Not Natively Physiologically Active, as it Requires an Extrinsically-Administered Electron Acceptor (Such as Methylene Blue and Riboflavin)
This Mechanism Becomes Important in the Treatment of Methemoglobinemia as Methylene Blue Accelerates the NADPH-Dependent Methemoglobin Reduction Pathway
Note: G6PD Deficiency is a Risk Factor for Acquired Methemoglobinemia
Pathophysiology in the Setting of Methemoglobinemia
Oxidation of Iron in Hemoglobin from the Ferrous (Fe2+) to the Ferric (Fe3+) State
Ferric Hemes of Methemoglobin are Unable to Bind Oxygen and Therefore, Result in a “Functional Anemia” with Decreased Oxygen Delivery to Tissues
Left-Shifting of the Hemoglobin Dissociation Curve (see Hypoxemia)
While the Ferric Heme is Unable to Bind Oxygen, the Remaining Three Ferrous Hemes in the Hemoglobin Tetramer Have Increased Avidity for Oxygen, Resulting in Impaired Oxygen Unloading at the Tissues (Exacerbating Tissue Hypoxia)
Predisposition of Premature Neonates and Infants to Methemoglobinemia
Factors Increasing the Risk of Methemoglobinemia in Premature Neonates/Infants <4 mo of Age
Propensity of Fetal Hemoglobin to More Easily Oxidize than Adult Hemoglobin
Low Levels of NADH Reductase at Birth
NADH Reducase Levels Increase to Adult Levels by 4 mo of Age
Higher Gastric pH with Increased Bacterial Conversion of Dietary Nitrates to Nitrites
Association of Methemoglobinemia with Gastroenteritis Illnesses in Ifants
This May Be Related to Increased Stool Loss of Bicarbonate
Pulse Oximeter Only Measures the Relative Absorbance of 2 Light Wavelengths (660 nm and 940 nm) to Differentiate Oxyhemoglobin from Deoxyhemoglobin
Methemoglobin Increases the Absorption of Both Light Wavelengths (Although More So at 940 nm), Optically Interfering with the Pulse Oximetry Measurement
Newer Generation Multi-Wavelength Pulse Oximeters are in Development
Methemoglobinemia Results in Interference with the Pulse Oximetry Measurement, Causing Inaccurate Readings
Decreased SpO2 on the Pulse Oximeter
When Methemoglobin is <30%
Pulse Oximetry Will Overestimate the Percentage of Oxyhemoglobin in Presence of Methemoglobin by an Amount Roughly Equal to 50% of the Amount of Methemoglobin Present
In the Presence of 20% Methemoglobin and a SpO2 90%, Percentage of Oxyhemoglobin Will Be About 80%
When Methemoglobin is >30%
Pulse Oximetry Will Plateau at About 85%
Note that Severity of the Cyanosis Does Not Correspond to the Pulse Oximetry Reading
Note that the Arterial pO2 Reflects the Plasma Oxygen Content and Does Not Reflect the Oxygen-Carrying Capacity of Hemoglobin
Methods to Determine the SaO2 from an Arterial Blood Gas Sample
General Comments
It is Critical to Know Which Device is Being Used by Your Specific Laboratory to Report the SaO2, Since the Presence of Dyshemoglobinemias Can Lead to Misinterpretation of the Data
Blood Gas Analyzer without Co-Oximetry
Principle: pO2 is measured by the analyzer and the SaO2 is calculated using a standard equation
Technical Issues
Blood Gas Analyzer Uses a Calculated or Default Hemoglobin Value
Blood Gas Analyzer Assumes a Normal Hemoglobin Value and the Absence of Dyshemoglobinemias (Such as Methemoglobin, Carboxyhemoglobin, Sulfhemoglobin)
Clinical Scenarios
Methemoglobinemia (see Methemoglobinemia): pO2 and (calculated) SaO2 will both be reported as normal
Functional Hemoglobin Saturation from Simple Co-Oximetry
Principle: determination of SaO2 utilizing measurement of oxyhemoglobin (O2Hb) and deoxyHb (DeO2Hb) only
Methemoglobinemia (see Methemoglobinemia): the reported FO2Hb will be considerably lower than the SaO2 reported by the blood gas analyzer
Co-Oximetry on Arterial Blood Gas (ABG) Sample
Principle
Co-Oximeter is a Simplified Spectrophotometer Which Measures Light Absorbance at Various Different Wavelengths of Light
Early Co-Oximeters Were Capable of Measuring Light Absorbance at Four Wavelengths of Light
Modern Co-Oximeters (Continuous Wave Spectrophotometers) are Capable of Measuring Absorbance at >100 Different Wavelengths of Light
Additional Wavelengths Improve Accuracy, Minimize Artifacts from Interfering Substances, and Enable Reporting of Additional Components
More Complex Modern Co-Oximetry Devices Can Measure Absorbance at 128 Wavelengths, Allowing Determination of Total Hemoglobin Concentration, SaO2, Fractional Oxyhemoglobin, and Fractional Carboxyhemoglobin, Fractional Methemoglobin, and Fractional Sulfhemoglobin
Hemoglobin Species Detected by Co-Oximetry Devices
Oxyhemoglobin
Deoxyhemoglobin
Carboxyhemoglobin
Methemoglobin: peak absorbance at 630 nm
Sulfhemoglobin: peak absorbance at 614 nm (overlaps to 630 nm and may be reported as methemoglobin on older machines)
Normal Range of Methemoglobin: <1-3%
Clinical Symptoms are Correlated with the Percentage of Methemoglobin Present (See Below)
Addition of Cyanide, Which Binds to Positively Charged Methemoglobin: eliminates the peak at 630-635 nm
Subsequent Addition of Ferricyanide: converts entire specimen to cyanomethemoglobin, which then allows measurement of total hemoglobin concentration
Specificity: Evelyn-Malloy assay is more specific than co-oximetry for detection of methemoglobin
Clinical Utility: Evelyn-Malloy assay is a good confirmatory test and is especially useful after methylene blue administration
Potassium Cyanide Test
Distinguishes Between Methemoglobin and Sulfhemoglobin
Methemoglobin reacts with cyanide to form cyanomethemoglobin: bright red color change
Sulfhemoglobin does not react with cyanide: lack of bright red color change
Drop Test
Technique: place 1-2 drops of blood onto white filter paper -> in the presence of significant methemoglobinemia, blood will remain dark (ie: will not oxygenate as normal blood would)
May accelerate process by gently blowing 100% onto the blood drop on the filter paper
Aeration of Tube of Blood with 100% Oxygen
Technique: bubble 100% oxygen through blood -> in the presence of significant methemoglobinemia, blood will remain dark (ie: will not oxygenate as normal blood would)
Influence of Heterozygous State for Cytochrome b5R Deficiency
Although Patients Heterozygous for Cytochrome b5R Deficiency May Develop Methemoglobinemia More Readily than Normals, Most Acquired Methemoglobinemia Cases Occur in Patients Who are Not Heterozygous for Cytochrome b5R Deficiency
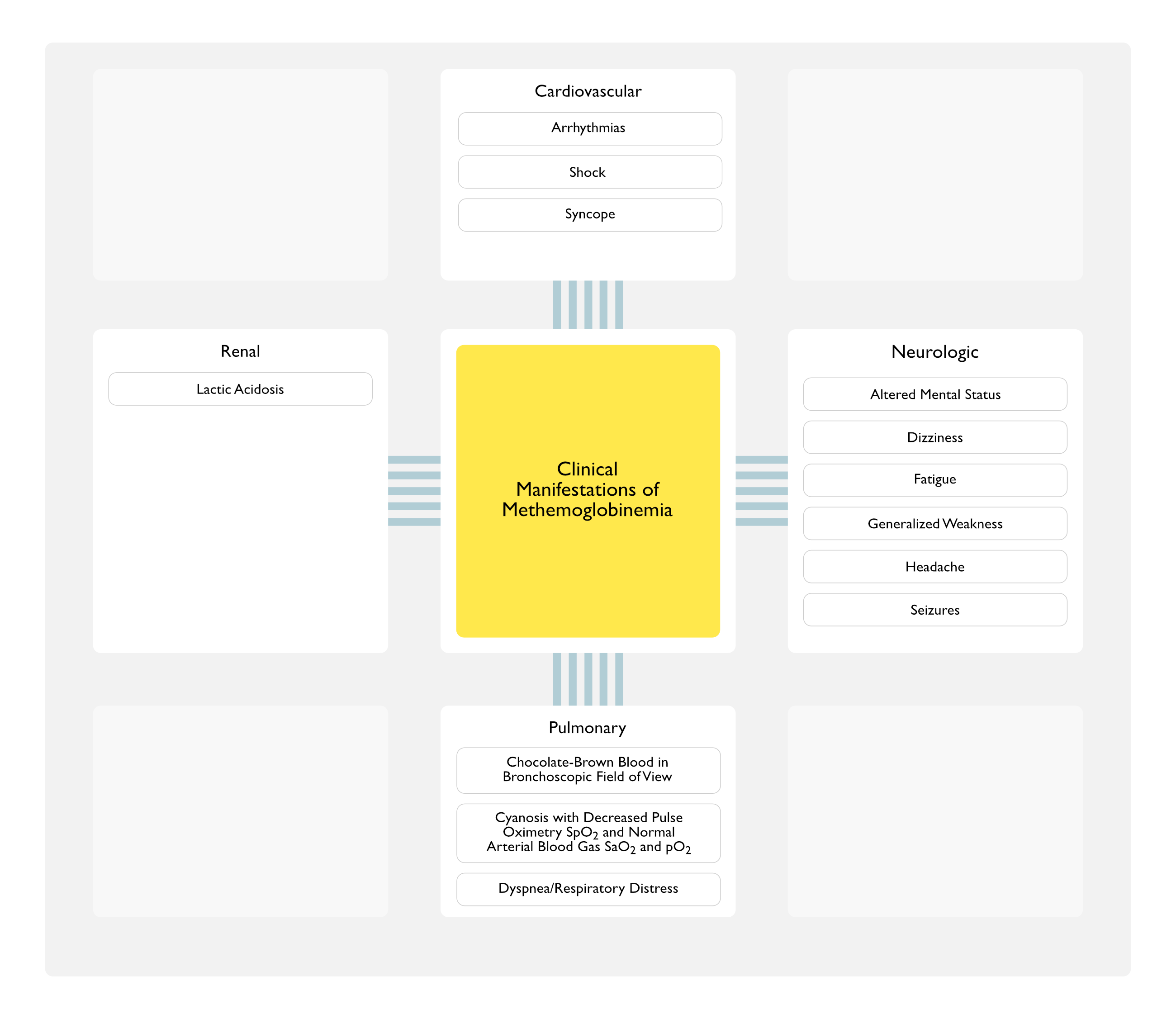
Appearance of Chocolate-Brown Blood in the Bronchoscopic Field of View (see Bronchoscopy)
Epidemiology
May Be Observed in Cases that Occur During Bronchoscopy (or During Other Videoscopic Procedures)
Cyanosis Accompanied by Decreased Pulse Oximetry SpO2 and a Normal Arterial Blood Gas SaO2 and pO2 (see Cyanosis)
Physiology
This Constellation of Findings Reflects the Dysfunction of the Pulse Oximeter Caused the Presence of the Methemoglobin
XXXXXX
Clinical
Bluish-Brown Coloration of Skin and Mucous Membranes
Cyanosis is Clinically Apparent at Methemoglobin Level >8-12% (at a Normal Hemoglobin Concentration): equivalent to >1.5 g/dL
Note: in Contrast, a Deoxyhemoglobin Level of 5 g/dL is Required to Produce Clinical Cyanosis
In Patients with Severe Anemia, a Higher Percentage of Methemoglobin is Required for Cyanosis to Be Clinically Apparent
These Patients are More Likely to Exhibit Signs of Hypoxemia and Have Lesser Degrees of Cyanosis, as Compared to Non-Anemic Patients
The Clinical Symptoms of Methemoglobinemia are Exacerbated in the Presence of Anemia
Management
Lack of Response of Cyanosis to Supplemental Oxygen (in the Absence of Cardiopulmonary Disease) is a Hallmark of Methemoglobinemia
While Cyanosis in Most Pulmonary Diseases Will Respond to Supplemental Oxygen, Cyanosis in Cardiac Disease with a Right-to-Left Intracardiac Shunt Usually Does Not Respond to Supplemental Oxygen Administration
Methylene Blue Functions as a Reversible Monoamine Oxidase (MAO) Inhibitor (see Monoamine Oxidase Inhibitors): in the setting of other serotonergic agents, methylene blue may preceipitate the serotonin syndrome
FDA Alert (7/26/11): avoid use of methylene blue in conjunction with selective serotonin reuptake inhibitors (SSRI’s) (see Selective Serotonin Reuptake Inhibitors)
Resolution Typically Occurs within 1 hr (Often within 20 min)
Re-Treatment
Treatment Can Be Repeated in 1 hr if the Methemoglobin Level Remains Elevated
Serial Monitoring of Methemoglobin Level (by Evans-Malloy Method) is Recommended Due to Prolonged Absorption of the Offending Drug from Topical Sites/Gastrointestinal Tract
Co-Oximetry Cannot Be Used to Follow Serial Methemoglobin Levels After Methylene Blue Dosing Since Methylene Blue is Erroneously “Read” as Methemoglobin
Some Cases May Manifest Significant Rebound Methemoglobinemia Up to 18 hrs Later
Dapsone Undergoes Enterohepatic Recirculation (see Dapsone): re-treatment may be necessary in some cases
Adverse Effects/Cautions
Blue Discoloration of Skin After Administration (see Cyanosis)
Methylene Blue Can Impart a Blue Discoloration to the Skin After Administration, This Does Not Imply Treatment Failure
Excessive Dosing
Cumulative Methylene Blue Doses >7 mg/kg Can Result in Hemolysis, Dyspnea, and Chest Pain
Since Methylene Blue Interferes with Subsequent Pulse Oximetry, Must Not Rely on an Improving SpO2 (by Pulse Oximetry) as a Marker for Successful Treatment
Failure of methylene blue treatment in toxic methemoglobinemia. Association with glucose-6-phosphate dehydrogenase deficiency. Ann Intern Med 1971;75:83-6
Toxic methemoglobinemia after topical anesthesia for transesophageal echocardiography. J Am Soc Echocardiogr. Nov-Dec 1996;9(6):874-6
Acute effects of inhaled nitric oxide in adult respiratory distress syndrome. Eur Respir J 1998; 12:1164-1171
Effects of inhaled nitric oxide in patients with acute respiratory distress syndrome: results of a randomized phase II trial. Crit Care Med 1998; 26:15-23
Elevated methemoglobin in patients with sepsis. Acta Anaesthesiol Scand. Jul 1998;42(6):713-6 [MEDLINE]
Innovations in mechanical ventilation. Current Opin Crit Care 1999; 5:43-51
Inhalation of nitric oxide in acute lung injury: results of a European multicentre study. Intensive Care Med 1999; 25:911-919
Inhaled nitric oxide in ARDS: modulator of lung injury? Intensive Care Med 1999; 25:1024-1026
Metoclopramide-induced methemoglobinemia in a patient with co-existing deficiency of glucose-6-phosphate dehydrogenase and NADH-cytochrome b5 reductase: failure of methylene blue treatment Haematologica 2001;86:659
Toxicol Review 2003: 22: 13-27
J Am Soc Echocardiograpy 2003: 16: 170-175
Recognition and management of methemoglobinemia and hemolysis in a G6PD-deficient patient on experimental anticancer drug Triapine. Am J Hematol 2006;81:210-1 [MEDLINE]
Methemoglobinemia and transesophageal echo. Proc West Pharmacol Soc. 2007;50:134-5
Level of oxidative stress in the red blood cells of patients with liver cirrhosis. Indian J Med Res. Sep 2007;126(3):204-10 [MEDLINE]
Infection and the Risk of Topical Anesthetic Induced Clinically Significant Methemoglobinemia after Transesophageal Echocardiography. Echocardiography. Aug 31 2009
Coma, metabolic acidosis, and methemoglobinemia in a patient with acetaminophen toxicity. J Popul Ther Clin Pharmacol. 2013;20(3):e207-11. Epub 2013 Sep 6 [MEDLINE]