

Etiology

Hereditary Syndrome of Inappropriate Antidiuretic Hormone Secretion (SIADH)
- Mechanism
- Mutation in the Gene for the Renal V2 Receptor (“Nephrogenic Syndrome of Inappropriate Antidiuresis”)
- Most Patients Have a Mutation Which Locks the V2 Receptor in the Open Position, Making it Unresponsive to Vasopressin Antagonists (Clin Endocrinol-Oxf, 2016) [MEDLINE]
- Clinical
- May Be Diagnosed in Adult Males/Females
Endocrine Disease
- Hypothyroidism (see Hypothyroidism)
- Epidemiology
- Hyponatremia May Occur with Moderate-Severe Hypothyroidism (Especially with Primary Hypothyroidism and Myxedema)
- Mechanism
- Decreased Ability to Excrete Free Water: patients fail to maximally dilute urine after a water load
- Increased Serum Vasopressin: has been observed in some, but not all, studies (possibly related to decreased cardiac output)
- Decreased Glomerular Filtration Rate: decreases water delivery to diluting segments of the renal tubules
- Epidemiology
- Hypopituitarism with Secondary Adrenal Insufficiency (see Adrenal Insufficiency)
- Clinical
- In Contrast, Primary Adrenal Insufficiency is Associated with Hypovolemic Hyponatremia
- Clinical
Gastrointestinal Disease
- Acute Intermittent Porphyria (see Acute Intermittent Porphyria)
- Nausea (see Nausea and Vomiting)
- Physiology
- Stimulation of Vasopressin Secretion
- Physiology
Neoplastic Disease
- Adrenocortical Carcinoma
- Brain Tumor
- Carcinoid Tumor
- Bronchial Carcinoid (see Bronchial Carcinoid)
- Cervical Cancer (see Cervical Cancer)
- Colorectal Cancer (see Colorectal Cancer)
- Duodenal Carcinoma
- Ewing Sarcoma (see Ewing Sarcoma)
- Extrapulmonary Small Cell Cancer
- Head and Neck Cancer (see Head and Neck Cancer) (Laryngoscope, 1996) [MEDLINE] (Ann Otol Rhinol Laryngol, 1997) [MEDLINE]
- Leukemia
- Lung Cancer (see Lung Cancer)
- Small Cell Lung Cancer (see Lung Cancer)
- Epidemiology
- SIADH is Associated Predominantly with Small Cell Histology
- Approximately 10% of Small Cell Lung Cancer Cases Manifest SIADH
- Small Cell Lung Cancer Accounts for Approximately 75% of All Malignancy-Associated SIADH Cases (Am J Respir Crit Care Med, 1997) [MEDLINE]
- Mechanism Involving SIADH
- SIADH is Associated Predominantly with Small Cell Histology
- Approximately 10% of Small Cell Lung Cancer Cases Manifest SIADH
- Small Cell Lung Cancer Accounts for Approximately 75% of All Malignancy-Associated SIADH Cases
- Mechanism Involving Ectopic Atrial Natriuretic Peptide (ANP) Secretion, Resulting in Secondary Arginine Vasopressin Secretion
- SIADH Occurs More Commonly in Small Cell Lung Cancer than Ectopic Atrial Natriuretic Peptide (ANP) Secretion
- Ectopic Atrial Natriuretic Peptide (ANP) Secretion May Also Exacerbate SIADH-Related Hyponatremia by Inducing Sodium Excretion into a Concentrated Urine without Extracellular Volume Expansion
- Clinically Present with Hypovolemia
- Small Cell Lung Cancer (see Lung Cancer)
- Lymphoma (see Lymphoma)
- Mesothelioma (see Pleural Mesothelioma)
- Nasopharyngeal Carcinoma (see Nasopharyngeal Carcinoma)
- Olfactory Neuroblastoma (Esthesioneuroblastoma) (see Neuroblastoma)
- Ovarian Cancer (see Ovarian Cancer)
- Pancreatic Cancer (see Pancreatic Cancer)
- Prostate Cancer (see Prostate Cancer)
- Thymoma (see Thymoma)
- Urothelial Cell Carcinoma (see Urothelial Cell Carcinoma)
- Bladder Cancer (see Bladder Cancer)
- Ureteral Cancer (see Ureteral Cancer)
Neuropsychiatric Disease
- General Comments
- Similar to Other Etiologies of Syndrome of Inappropriate Antidiuretic Hormone Secretion (SIADH), Hyponatremia in These Conditions is Due to Antidiuretic Hormone-Induced Water Retention and Urinary Sodium Loss
- However, it is Not Certain if the Sodium Losses are Due to an Antidiuretic Hormone-Induced Expansion in the Extracellular Volume or Whether They are Due to Cerebral Salt-Wasting with a Secondary Release of Antidiuretic Hormone in Response to Decreased Extracellular Volume
- Due to This Uncertainty, Therapy of This Group of Etiologies Typically Involves the Use of Hypertonic (3%) Saline, Rather than Fluid Restriction or Isotonic Saline
- Similar to Other Etiologies of Syndrome of Inappropriate Antidiuretic Hormone Secretion (SIADH), Hyponatremia in These Conditions is Due to Antidiuretic Hormone-Induced Water Retention and Urinary Sodium Loss
- Acute Intermittent Porphyria (see Acute Intermittent Porphyria)
- Acute Psychosis (see Psychosis)
- Brain Abscess (see Brain Abscess)
- Cavernous Sinus Thrombosis (see Cerebral Venous Thrombosis)
- Cerebellar/Cerebral Atrophy
- Delirium Tremens/Ethanol Withdrawal (see Ethanol)
- Epilepsy (see Seizures)
- Guillain-Barre Syndrome (GBS) (see Guillain-Barre Syndrome)
- Epidemiology
- Hyponatremia is a Predictor of Poor Outcome in Guillain-Barre Syndrome (Neurol Res, 2015) [MEDLINE]
- Epidemiology
- Human Immunodeficiency Virus (HIV)/Acquired Immune Deficiency Syndrome (AIDS) (see Human Immunodeficiency Virus)
- Epidemiology
- Hyponatremia Has Been Reported in as Many as 40% of Adult Patients with HIV Infection (JAMA, 1990) [MEDLINE]
- Mechanisms of Hyponatremia
- Due to Volume Depletion
- Although 33% of Hyponatremic Patients with AIDS are Clinically Hypovolemic, the Remaining Hyponatremic Patients Fulfill Most of the Criteria for SIADH
- Due to Infection of the Lungs and the Central Nervous System with SIADH-Associated Mechanism
- Due to Volume Depletion
- Epidemiology
- Hydrocephalus (see Hydrocephalus)
- Hypoxic-Ischemic Brain Injury (see Hypoxic-Ischemic Brain Injury)
- Intracerebral Hemorrhage (ICH) (see Intracerebral Hemorrhage)
- Ischemic Cerebrovascular Accident (CVA) (see Ischemic Cerebrovascular Accident)
- Lupus Cerebritis (see Systemic Lupus Erythematosus)
- Meningitis/Encephalitis (see Meningitis and Encephalitis)
- Midfacial Hypoplasia
- Multiple Sclerosis (see Multiple Sclerosis)
- Perinatal Hypoxia
- Rocky Mountain Spotted Fever (see Rocky Mountain Spotted Fever)
- Schizophrenia (see Schizophrenia)
- Shy-Drager Syndrome (see Shy-Drager Syndrome)
- Subarachnoid Hemorrhage (SAH) (see Subarachnoid Hemorrhage)
- Physiology
- Hyponatremia in SAH is Usually Due to SIADH, But Cerebral Salt Wasting May Instead Be Etiologic (J Am Soc Nephrol, 2008) [MEDLINE] (see Cerebral Salt Wasting)
- Since SIADH and Cerebral Salt Wasting are Similar, the Main Differentiating Feature is Clinical Hypovolemia Despite a Urine Sodium Which is Not Low, Which Supports the Diagnosis of Cerebral Salt Wasting Instead
- Physiology
- Subdural Hematoma (see Subdural Hematoma)
- Traumatic Brain Injury (TBI) (see Traumatic Brain Injury)
- Varicella-Zoster Virus (VZV) Infection of Chest Wall (see Varicella-Zoster Virus)
- Ventriculoatrial Shunt Obstruction
- Wernicke Encephalopathy (see Thiamine)
Pulmonary Disease
- Acute Bronchitis (see Acute Bronchitis)
- Acute Respiratory Failure/Mechanical Ventilation (see Respiratory Failure) (Kidney Int, 1986) [MEDLINE]
- Asthma (see Asthma) (Kidney Int, 1986) [MEDLINE]
- Atelectasis (see Atelectasis) (Kidney Int, 1986) [MEDLINE]
- Bronchiolitis (see Bronchiolitis)
- Carcinoid Tumor
- Bronchial Carcinoid (see Bronchial Carcinoid)
- Chronic Obstructive Pulmonary Disease (COPD) (see Chronic Obstructive Pulmonary Disease)
- Cystic Fibrosis (CF) (see Cystic Fibrosis)
- Empyema (see Pleural Effusion-Parapneumonic)
- Human Immunodeficiency Virus (HIV)/Acquired Immune Deficiency Syndrome (AIDS) (see Human Immunodeficiency Virus)
- Epidemiology
- Hyponatremia Has Been Reported in as Many as 40% of Adult Patients with HIV Infection (JAMA, 1990) [MEDLINE]
- Mechanisms of Hyponatremia
- Due to Volume Depletion
- Although 33% of Hyponatremic Patients with AIDS are Clinically Hypovolemic, the Remaining Hyponatremic Patients Fulfill Most of the Criteria for SIADH
- Due to Infection of the Lungs and the Central Nervous System with SIADH-Associated Mechanism
- Due to Volume Depletion
- Epidemiology
- Lung Abscess (see Lung Abscess)
- Lung Cancer (see Lung Cancer)
- Small Cell Lung Cancer (see Lung Cancer): see above
- Pneumonia
- Community-Acquired Pneumonia (CAP) (see Community-Acquired Pneumonia)
- Pneumonia (Especially Viral, Bacterial, Tuberculous) is the Most Common Pulmonary Etiology of Hyponatremia
- Mechanism is Unclear (Kidney Int, 1986) [MEDLINE]
- Pneumonia (Especially Viral, Bacterial, Tuberculous) is the Most Common Pulmonary Etiology of Hyponatremia
- Hospital-Acquired Pneumonia/Ventilator-Associated Pneumonia (VAP) (see Hospital-Acquired Pneumonia and Ventilator-Associated Pneumonia)
- Pneumonia (Especially Viral, Bacterial, Tuberculous) is the Most Common Pulmonary Etiology of Hyponatremia
- Mechanism is Unclear (Kidney Int, 1986) [MEDLINE]
- Pneumonia (Especially Viral, Bacterial, Tuberculous) is the Most Common Pulmonary Etiology of Hyponatremia
- Cavitary Aspergillosis Has Also Been Reported to Be Etiologic (see Aspergillus)
- Community-Acquired Pneumonia (CAP) (see Community-Acquired Pneumonia)
- Pneumothorax (see Pneumothorax) (Kidney Int, 1986) [MEDLINE]
- Pulmonary Fibrosis
- Idiopathic Pulmonary Fibrosis (IPF) (see Idiopathic Pulmonary Fibrosis)
- Sarcoidosis (see Sarcoidosis)
Surgery
- Epidemiology
- Associated with Surgical Procedures (Including Ones as Noninvasive as Cardiac Catheterization, etc) (Am J Kidney Dis, 2002) [MEDLINE]
- May Occur as a Late Complication of Transsphenoidal Pituitary Surgery (Occurs in 21-35% of Cases (J Clin Endocrinol Metab, 1994) [MEDLINE] (J Clin Endocrinol Metab, 1995) [MEDLINE]
- Mechanism Likely Involves Predominantly SIADH (Due to Antidiuretic Hormone Release from the injured Posterior Pituitary Gland), Although Relative Cortisol Deficiency May Contribute to a Lesser Extent
- Hyponatremia is the Most Severe ob the 6th-7th Postoperative Day
- The Occurrence of Delayed Hyponatremia is Likely a Subset of the Classic Triphasic Cycle (Initial Polyuria, Followed by Transient SIADH, and Then, Either Recovery or a Third Phase of Permanent Central Diabetes Insipidus)
- Physiology
Drugs/Toxins
- Acetylcholine
- Pharmacology
- Stimulation of Vasopressin Release
- Pharmacology
- Amiodarone (Cordarone) (see Amiodarone)
- Barbiturates (see Barbiturates)
- Agents
- Thiopental (see Thiopental)
- Pharmacology
- Stimulation of Vasopressin Release
- Agents
- Bromocriptine (Parlodel, Cycloset, Brotin) (see Bromocriptine)
- Pharmacology
- Stimulation of Vasopressin Release
- Pharmacology
- Butyrophenones (see Butyrophenones)
- Agents
- Haloperidol (Haldol) (see Haloperidol)
- Pharmacology
- Stimulation of Vasopressin Release
- Agents
- Carbachol (Miostat) (see Carbachol)
- Pharmacology
- Stimulation of Vasopressin Release
- Pharmacology
- Carbamazepine (Tegretol) (see Carbamazepine)
- Epidemiology
- Known Drug-Associated Etiology (Expert Opin Drug Saf, 2017) [MEDLINE]
- Pharmacology
- Stimulation of Vasopressin Release
- At Least in Part, Increases Sensitivity to Antidiuretic Hormone
- Epidemiology
- Ciprofloxacin (Cipro) (see Ciprofloxacin)
- Cisplatin (Platinol) (see Cisplatin)
- Epidemiology
- Known Association Between Platinum Use and SIADH (Eur Endocrinol, 2020) [MEDLINE]
- Pharmacology
- Platinum Compounds Can Cause Hyponatremia by Multiple Mechanisms
- Overzealous Administration of Large Volume of Hypotonic Intravenous Fluid
- Renal Tubular Necrosis Resulting in Renal Salt-Wasting
- SIADH (Via Unclear Mechanism)
- Nausea-Associated Stimulation of Antidiuretic Hormone Release
- Platinum Compounds Can Cause Hyponatremia by Multiple Mechanisms
- Epidemiology
- Clofibrate (Atromid-S) (see Clofibrate)
- Pharmacology
- Stimulation of Vasopressin Release
- Potentiation of Peripheral Activity of Vasopressin
- Pharmacology
- Cyclophosphamide (Cytoxan) (see Cyclophosphamide)
- Epidemiology
- Most Associated with High-Dose Intravenous Use (30-50 mg/kg used to treat malignancy or 6 g/m2 as given in the STAMP protocol in preparation for bone marrow rescue)
- Although less common, hyponatremia can also occur with the lower doses (10-15 mg/kg) that are given as pulse therapy in autoimmune diseases such as lupus nephritis
- Exacerbated by the Fact that These Patients Also Receive Intravenous Fluid Loading to Prevent the Complication of Hemorrhagic Cystitis
- Pharmacology
- Stimulation of Vasopressin Release
- Chemotherapy-Induced Nausea May Contribute Since Nausea is a Potent Stimulus to Antidiuretic Hormone Release
- Management
- The fall in the plasma sodium concentration in this setting can be minimized by using isotonic saline rather than free water to maintain a high urine output
- Epidemiology
- Cyclopropane
- Pharmacology
- Stimulation of Vasopressin Release
- Pharmacology
- Ecstasy Intoxication (see Ecstasy)
- Mechanisms of Hyponatremia
- Increased Water Intake
- SIADH, Resulting in Impairment of Water Excretion
- Mechanisms of Hyponatremia
- Eslicarbazepine (Aptiom, Zebinix) (see Eslicarbazepine)
- Epidemiology
- Case Reports (Expert Opin Drug Saf, 2017) [MEDLINE]
- Epidemiology
- Gabapentin (Neurontin) (see Gabapentin)
- Epidemiology
- Case Reports (Expert Opin Drug Saf, 2017) [MEDLINE]
- Epidemiology
- Gonadotropin-Releasing Hormone Agonists
- Agents
- Goserelin
- Leuprolide (see Leuprolide)
- Leuprorelin
- Triptorelin
- Pharmacology
- Multiple Mechanisms of Hyponatremia
- Hypothyroidism (see Hypothyroidism)
- Pituitary Apoplexy (Associated with Undiagnosed Pituitary Macroadenoma), Resulting in Secondary Adrenal Insufficiency (see Adrenal Insufficiency)
- SIADH
- Multiple Mechanisms of Hyponatremia
- Agents
- Griseofulvin (Gris-peg, Grifulvin V) (see Griseofulvin)
- Pharmacology
- Potentiation of Peripheral Activity of Vasopressin
- Pharmacology
- Halothane (see Halothane)
- Pharmacology
- Stimulation of Vasopressin Release
- Pharmacology
- Histamine
- Pharmacology
- Stimulation of Vasopressin Release
- Pharmacology
- Hypoglycemic Agents
- Agents
- Chlorpropamide (Diabinese) (see Chlorpropamide): commonly-associated etiology
- Metformin (Glucophage) (see Metformin)
- Phenformin (see Phenformin)
- Tolbutamide (Orinase) (see Tolbutamide)
- Pharmacology
- Potentiation of Peripheral Activity of Vasopressin
- Chlorpropamide Stimulates Vasopressin Release and Increases Concentrating Ability Both by Increasing Sodium Chloride Reabsorption in the Loop of Henle (Enhancing the Efficiency of Countercurrent Exchange) and by Augmenting Collecting Tubule Water Permeability (the Latter Effect Mediated by an Increased Number of Antidiuretic Hormone Receptors in the Collecting Tubule Cells)
- Agents
- Ifosfamide (see Ifosfamide)
- Pharmacology
- Stimulation of Vasopressin Release
- Pharmacology
- Interferon-α (see Interferon-α)
- Interferon-γ (see Interferon-γ)
- Interleukin-2 (IL-2) (see Interleukin-2)
- Isoproterenol (Isuprel) (see Isoproterenol)
- Pharmacology
- Stimulation of Vasopressin Release
- Pharmacology
- Lamotrigine (Lamictal) (see Lamotrigine)
- Epidemiology
- Case Reports (Expert Opin Drug Saf, 2017) [MEDLINE]
- Epidemiology
- Levamisole (Ergamisol) (see Levamisole)
- Levatiracetam (Keppra) (see Levatiracetam)
- Epidemiology
- Case Reports (Expert Opin Drug Saf, 2017) [MEDLINE]
- Epidemiology
- Lorcainide
- Pharmacology
- Stimulation of Vasopressin Release
- Pharmacology
- Melphalan (Alkeran, Evomela, Phelinun) (see Melphalan)
- Epidemiology
- Known Association Between Alkylating Agent Use and SIADH (Eur Endocrinol, 2020) [MEDLINE]
- Epidemiology
- Methotrexate (see Methotrexate)
- Monoamine Oxidase (MAO) Inhibitors (see Monoamine Oxidase Inhibitors)
- Agents
- Clorgyline
- Furazolidone
- Isoniazid (INH) (see Isoniazid)
- Iproniazid
- Isocarboxazide
- Linezolid (Zyvox, Zyvoxid) (see Linezolid)
- Methylene Blue (see Methylene Blue)
- Moclobemide
- Nialamid(e)
- Pargyline
- Phenelzine (Nardil) (see Phenelzine)
- Procarbazine (Matulane, Natulan, Indicarb) (see Procarbazine)
- Selegiline (Anipryl, L-Deprenyl, Eldepryl, Emsam, Zelapar) (see Selegiline)
- Toloxatone
- Tranylcypromine (Parnate) (see Tranylcypromine)
- Pharmacology
- Stimulation of Vasopressin Release
- Agents
- Monoclonal Antibodies
- Epidemiology
- Case Reports with Alemtuzumab (Campath, Mabcampath, Lemtrada) (see Alemtuzumab) (Eur Endocrinol, 2020) [MEDLINE]
- Case Reports with Proteasome Inhibitors (Eur Endocrinol, 2020) [MEDLINE]
- Bortezomib (Velcade, Chemobort, Bortecad) (see Bortezomib): hyponatremia may be severe
- Case Reports with Multiple Tyrosine Kinase Inhibitors (Eur Endocrinol, 2020) [MEDLINE]
- Afatinib (Gilotrif, Giotrif, Afanix) (see Afatinib)
- Axitinib (Inlyta, Axinix) (see Axitinib)
- Bosutinib (Bosulif) (see Bosutinib)
- Brivanib (see Brivanib)
- Dasatinib (Sprycel, Dasanix) (see Dasatinib)
- Erlotinib (Tarceva) (see Erlotinib)
- Gefitinib (Iressa) (see Gefitinib)
- Imatinib (Gleevec) (see Imatinib)
- Nilotinib (Tasigna) (see Nilotinib)
- Sorafenib (Nexavar) (see Sorafenib)
- Epidemiology
- Nicotine (see Nicotine)
- Pharmacology
- Stimulation of Vasopressin Release
- Pharmacology
- Nitrous Oxide (see Nitrous Oxide)
- Pharmacology
- Stimulation of Vasopressin Release
- Pharmacology
- Nonsteroidal Anti-Inflammatory Drugs (NSAID’s) (see Nonsteroidal Anti-Inflammatory Drug)
- Pharmacology
- Inhibition of Renal PGE2 Synthesis
- Pharmacology
- Opiates (see Opiates)
- Agents
- Morphine (see Morphine)
- Pharmacology
- Stimulation of Vasopressin Release
- Agents
- Oxcarbazepine (Trileptal) (see Oxcarbazepine)
- Epidemiology
- Known Drug-Associated Etiology (Expert Opin Drug Saf, 2017) [MEDLINE]
- Pharmacology
- Stimulation of Vasopressin Release
- At Least in Part, Increases Sensitivity to Antidiuretic Hormone
- Epidemiology
- Oxytocin (see Oxytocin)
- Pentostatin (see Pentostatin)
- Phenothiazines (see Phenothiazines)
- Agents
- Aliphatic Compounds
- Chlorpromazine (Thorazine, Largactil, Megaphen) (see Chlorpromazine)
- Levomepromazine
- Methotrimeprazine (Nozinan, Levoprome)
- Promazine (Sparine)
- Triflupromazine
- Piperidines
- Mesoridazine (Serentil) (see Mesoridazine)
- Thioridazine (Mellaril, Novoridazine, Thioril) (see Thioridazine)
- Piperazines
- Fluphenazine (Prolixin) (see Fluphenazine)
- Perphenazine (Trilafon) (see Perphenazine)
- Prochloperazine (Compazine) (see Prochlorperazine)
- Trifluoperazine (Stelazine) (see Trifluoperazine)
- Aliphatic Compounds
- Pharmacology
- Stimulation of Vasopressin Release
- Agents
- Phenoxybenzamine (Dibenzyline) (see Phenoxybenzamine)
- Proton Pump Inhibitors (PPI’s) (see Proton Pump Inhibitors)
- Agents
- Esomeprazole (Nexium) (see Esomeprazole)
- Lansoprazole (Prevacid) (see Lansoprazole)
- Omeprazole (Losec, Prilosec, Zegerid) (see Omeprazole)
- Pantoprazole (Protonix) (see Pantoprazole)
- Epidemiology
- Agents
- Selective Serotonin Reuptake Inhibitors (SSRI’s) (see Selective Serotonin Reuptake Inhibitors)
- Epidemiology
- Agents
- Citalopram (Celexa) (see Citalopram)
- Escitalopram (Lexapro) (see Escitalopram)
- Fluoxetine (Prozac) (see Fluoxetine)
- Fluvoxamine (Luvox) (see Fluvoxamine)
- Paroxetine (Paxil) (see Paroxetine)
- Sertraline (Zoloft) (see Sertraline)
- Vortioxetine (Brintellix) (see Vortioxetine)
- Thalidomide Analogues
- Agents
- Lenalidomide (Revlimid, Linamide) (see Lenalidomide)
- Thalidomide (Contergan, Thalomid, Talidex) (see Thalidomide)
- Epidemiology
- SIADH Associated with Thalidomide Analogue Use is Very Rare
- Agents
- Theophylline (Theolair, Slo-Bid) (see Theophylline)
- Pharmacology
- Potentiation of Peripheral Activity of Vasopressin
- Pharmacology
- Thiothixene (Navane) (see Thiothixene)
- Tricyclic Antidepressants (TCA’s) (see Tricyclic Antidepressants)
- Agents
- Amitriptyline (Tryptomer, Elavil) (see Amitriptyline)
- Clomipramine (Anafranil) (see Clomipramine)
- Desipramine (Norpramin, Pertofrane) (see Desipramine)
- Doxepin (Adapin, Sinequan) (see Doxepin)
- Imipramine (Tofranil, Janimine, Praminil) (see Imipramine)
- Nortriptyline (Pamelor, Aventyl, Norpress) (see Nortriptyline)
- Protriptyline (Vivactil) (see Protriptyline)
- Trimipramine (Surmontil) (see Trimipramine)
- Pharmacology
- Stimulation of Vasopressin Release
- Agents
- Triiodothyronine
- Pharmacology
- Potentiation of Peripheral Activity of Vasopressin
- Pharmacology
- Valproic Acid (Depakene, Valproate Sodium, Depacon, Stavzor) (see Valproic Acid)
- Epidemiology
- Case Reports (Expert Opin Drug Saf, 2017) [MEDLINE]
- Epidemiology
- Vasopressin Analogs
- Pharmacology
- Potentiation of Peripheral Activity of Vasopressin
- Agents
- Desmopressin (DDAVP) (see Desmopressin) (J Pediatr, 1989) [MEDLINE] (Am J Hematol, 1993) [MEDLINE] (Haemophilia, 2000) [MEDLINE]
- Terlipressin (Teripress, Glypressin) (see Terlipressin)
- Vasopressin (see Vasopressin)
- Low Serum Osmolality was Present in the Described Cases (with Vasopressin Use in the Treatment of Septic Shock), Suggesting Either Hypovolemia or an SIADH-Type Mechanism (J Intensive Care Med, 2015) [MEDLINE]
- Pharmacology
- Venlafaxine (Effexor) (see Venlafaxine)
- Epidemiology
- Pharmacology
- Serotonin-Norepinephrine Reuptake Inhibitor (see Serotonin-Norepinephrine Reuptake Inhibitors)
- Vidarabine (Vira-A) (see Vidarabine)
- Pharmacology
- Stimulation of Vasopressin Release
- Pharmacology
- Vinca Alkaloids
- Agents
- Vinblastine (Velban) (see Vinblastine)
- Vincristine (Oncovin, Vincasar, Marqibo) (see Vincristine)
- Epidemiology
- Known Association Between Vinca Alkaloid Use and SIADH (Eur Endocrinol, 2020) [MEDLINE]
- Pharmacology
- Stimulation of Vasopressin Release
- Agents
Other
- Exercise-Induced Hyponatremia
- Associated Groups
- Desert Hikers
- Football Players
- Marathon/Ultramarathon Runners
- Military
- Mechanism
- Excessive Water Intake
- Sodium Loss
- Persistent Antidiuretic Hormone Secretion with Impaired Water Excretion
- Associated Groups
- Giant Cell Arteritis (Temporal Arteritis, Horton Disease, Cranial Arteritis) (see Giant Cell Arteritis)
- Epidemiology
- Case Reports (Am J Med, 1988) [MEDLINE]
- Epidemiology
Idiopathic Syndrome of Inappropriate Antidiuretic Hormone Secretion (SIADH)

Physiology
Background
- Antidiuretic Hormone (ADH, Also Known as Arginine Vasopressin) Secretion Results in a Concentrated Urine and, Consequently, a Decreased Urine Volume
- The Higher the Plasma ADH, the More Concentrated the Urine
Syndrome of Inappropriate Secretion of Antidiuretic Hormone Secretion (SIADH) is a Disorder Characterized by Impaired Water Excretion Due to an Inability to Suppress the Secretion of Antidiuretic Hormone (ADH)

If Water Intake Exceeds the Decreased Urine Output, Water Retention Will Result in the Development of Hyponatremia
- In Most Patients with SIADH, the Ingestion of Water Does Not Adequately Suppress Antidiuretic Hormone Secretion
- Consequently, the Urine is Concentrated with Associated Water Retention
- Water Retention Increases Total Body Water, Which Results in a Dilutional Decrease in the Plasma Sodium Concentration
- The Increase in Total Body Water Transiently Expands the Extracellular Fluid Volume, Triggering Increased Urinary Sodium Excretion
- This Returns the Extracellular Fluid Volume Back Toward Normal and Further Decreases the Plasma Sodium Concentration, Exacerbating the Hyponatremia
Clinical Features of Syndrome of Inappropriate Secretion of Antidiuretic Hormone Secretion (SIADH)
- Hyponatremia
- Hypoosmolality
- Increased Urine Sodium (>20 mEq/L and Usually >40 mEq/L)
- High Urine Osmolality (>100 mosmol/kg)
- Other Features
- Normal Serum Potassium Concentration
- Absence of Acid-Base Disturbance
- Low Serum Uric Acid Concentration (Frequently)
Due to the Phenomenon of “Desalination”, Syndrome of Inappropriate Antidiuretic Hormone Secretion (SIADH) Can Occur Even if the Only Fluid Given is Isotonic/Normal Saline
- In Patients with Postoperative Hyponatremia Due to Surgery-Associated Syndrome of Inappropriate Antidiuretic Hormone Secretion (SIADH), Isotonic Intravenous Fluid Administration Results in Volume Expansion, Resulting in Increased Urinary Sodium Excretion
- With High Antidiuretic Hormone Levels, Sodium Excretion in a Concentrated Urine Results in a Further Decrease in the Serum Sodium (“Desalination”) (Ann Intern Med, 1997) [MEDLINE]
Patterns of Antidiuretic Hormone Secretion
General Comments
- In Normal Patients, Plasma Antidiuretic Hormone Levels are Very Low when the Plasma Osmolality is <280 mOsmol/kg, Permitting the Excretion of Ingested Water
- As the Plasma Osmolality Increases Above 280 mOsmol/kg, Antidiuretic Hormone Levels Increase Progressively
Various Patterns of Antidiuretic Hormone Secretion in Patient Populations with the Syndrome of Inappropriate Antidiuretic Hormone Secretion (SIADH)
- Type A: elevated antidiuretic hormone unresponsive to osmotic deviations
- Antidiuretic Hormone are Typically Above Levels Required for Maximum Antidiuresis
- Antidiuretic Hormone Levels Above the Physiologic Range Suggest Ectopic Antidiuretic Hormone Production (Due to Lung Cancer, etc)
- Urine Osmolality is Typically Very High
- Antidiuretic Hormone are Typically Above Levels Required for Maximum Antidiuresis
- Type B: abnormally low threshold for antidiuretic hormone release (threshold below the level of plasma osmolality at which plasma antidiuretic hormone becomes detectable in normal patients) and a linear increase in plasma antidiuretic hormone in response to a increasing plasma osmolality
- Typically, These Patients are Defined as Having a “Reset Osmostat
- In These Patients, the Plasma Sodium Will Not Continue to Decrease without Therapy, Since Antidiuretic Hormone Will Be Suppressed When the Plasma Osmolality Decrease Below the Reset Osmolality Threshold
- Type C: antidiuretic hormone levels within the physiologic range and neither suppressed by decreased plasma osmolality nor stimulated by increasing plasma osmolality
- This Pattern May Occur in Patients with Ectopic Antidiuretic Hormone Production
- Type D: antidiuretic hormone levels vary appropriately with the plasma osmolality, but the urine remains concentrated even if antidiuretic hormone release is suppressed
- May Occur Due to Germ Cell Mutation in Which the Vasopressin V2 Receptor is Constitutively Activated
- May Occur Due to Production of an Antidiuretic Substance Other than Immunoreactive Arginine Vasopressin and a Postreceptor Defect in Trafficking of Aquaporin-2 Water Channels (Which Mediate Antidiuretic Hormone-Induced Antidiuresis)
- Type E: decrease in plasma antidiuretic hormone as the serum sodium concentration increase during the infusion of hypertonic saline
- Due to Altered Baroreceptor Signaling Despite Normovolemia, Such that a Minor Decrease in Blood Pressure or Blood Volume Results in a Large Increase in Antidiuretic Hormone Secretion
- Similarly, a Minor Increase in Blood Pressure or Blood Volume During Saline Infusion Results in a Large Decrease in Antidiuretic Hormone Secretion
Determinants of Urine Output
In Addition to the Effect of Antidiuretic Hormone, Two Other Determinants of Urine Output Occur in Patients with Patients with the Syndrome of Inappropriate Antidiuretic Hormone Secretion (SIADH)
- Rate of Solute Excretion
- In Normal Patients, the Urine Output is Primarily Determined by Water Intake
- Increased Water Intake Results in a Decrease in Plasma Osmolality, Sensed by Hypothalamic Osmoreceptors (Which Regulate Both Antidiuretic Hormone Release and Thirst)
- Antidiuretic Hormone Secretion is Then Decreased, Resulting in Decreased Collecting Tubule Permeability to Water
- Net Effect is the Rapid Excretion of Excess Water in Dilute Urine
- In SIADH, an Increase in Water Intake Does Not Produce an Increase in Water Excretion Because Antidiuretic Hormone Secretion is Relatively Fixed
- Because the Urine Osmolality Cannot Be Reduced, the Urien Output Will Be Determined by the Rate of excretion of Solutes (Sodium Salts, Potassium Salts, and Urea)
- This Strategy to Use Ingested Solutes (Such as Oral Urea) with a High Salt/High Protein Diet Will Increase Water Excretion, Raising the Serum Sodium Toward Toward Normal
- In Normal Patients, the Urine Output is Primarily Determined by Water Intake
- Partial Escape from the Effect of Antidiuretic Hormone
- Animal Studies Using the Administration of Both Antidiuretic Hormone and Water Suggest that There is an Initial Phase of Water Retention and Hyponatremia, Followed by Partial Escape from the Antidiuresis
- Due to This Escape, Despite High Antidiuretic Hormone Levels, Urine Osmolality May Decrease, Resulting in Increased Water Excretion (Matching Water Intake) and the Plasma Sodium Tends to Stabilize
- The Escape is Likely Mediated by Decreased Aquaporin-2 Expression (the Antidiuretic Hormone-Sensitive Water Channel in the Renal Collecting Tubule)
- Due to This Escape, Despite High Antidiuretic Hormone Levels, Urine Osmolality May Decrease, Resulting in Increased Water Excretion (Matching Water Intake) and the Plasma Sodium Tends to Stabilize
- Animal Studies Using the Administration of Both Antidiuretic Hormone and Water Suggest that There is an Initial Phase of Water Retention and Hyponatremia, Followed by Partial Escape from the Antidiuresis
Diagnosis
Chest X-Ray (CXR) (see Chest X-Ray)
- Useful to Rule Out Pulmonary Disease
Head Computed Tomography (CT) (see Head Computed Tomography)
- Useful to Rule Out Central Nervous System Pathology
Brain Magnetic Resonance Imaging (MRI) (see Brain Magnetic Resonance Imaging)
- Useful to Rule Out Central Nervous System Pathology
Suggested Laboratory Evaluation of Hyponatremia
Serum Studies
- Serum Sodium (see Serum Sodium)
- Laboratory Serum Sodium Measurement Technology
- Flame Photometry Assay of Serum Sodium
- Measures Sodium Concentration in Whole Plasma
- In the Presence of Hyperproteinemia/Hypertriglyceridemia (with Expansion of Nonaqueous Component of the Serum), Pseudohyponatremia May Be Seen with This Assay Method
- Sodium-Selective Electrode Assay of Sodium
- Measures Sodium Activity in Serum Water: this assay gives the true, physiologically relevant sodium concentration as it measures sodium activity in serum water alone
- Indirect Potentiometry: current assay used in many hospital laboratories
- Direct Potentiometry
- Flame Photometry Assay of Serum Sodium
- Laboratory Serum Sodium Measurement Technology
- Serum Chloride (see Serum Chloride)
- Serum Osmolality (see Serum Osmolality)
- Normal Serum Osmolality: 275-290 mosmol/kg
- Indications for Measurement of Serum Osmolality in the Evaluation of Hyponatremia (i.e. When Either Isotonic or Hypertonic Hyponatremia are Suspected)
- Recent Transurethral Surgery/Hysteroscopy/Laparoscopy (Due to Use of Glycine/Sorbitol/Mannitol Irrigant)
- Recent Use of Mannitol (see Mannitol)
- Recent Use of Glycerol (see Glycerol)
- Recent Use Intravenous Immunoglobulin (IVIG) (see Intravenous Immunoglobulin)
- Presence of Lipemic (Hypertriglyceridemic) Serum
- Presence of Obstructive Jaundice
- Suspected Plasma Cell Dyscrasia (with Hyperproteinemia)
- Serum Cortisol (or Cosyntropin Stimulation Test) (see Serum Cortisol)
- Serum Thyroid Stimulating Hormone (TSH) (see Thyroid Stimulating Hormone)
Urine Studies
- Urine Sodium (see Urine Sodium)
- Urine Chloride (see Urine Chloride)
- Urine Osmolality (see Urine Osmolality)
- Normal Minimum Urine Osmolality is 40-100 mOsmol/kg
Diagnostic Strategies to Differentiate Cerebral Salt Wasting from Syndrome of Inappropriate Antidiuretic Hormone Secretion (see Cerebral Salt Wasting)
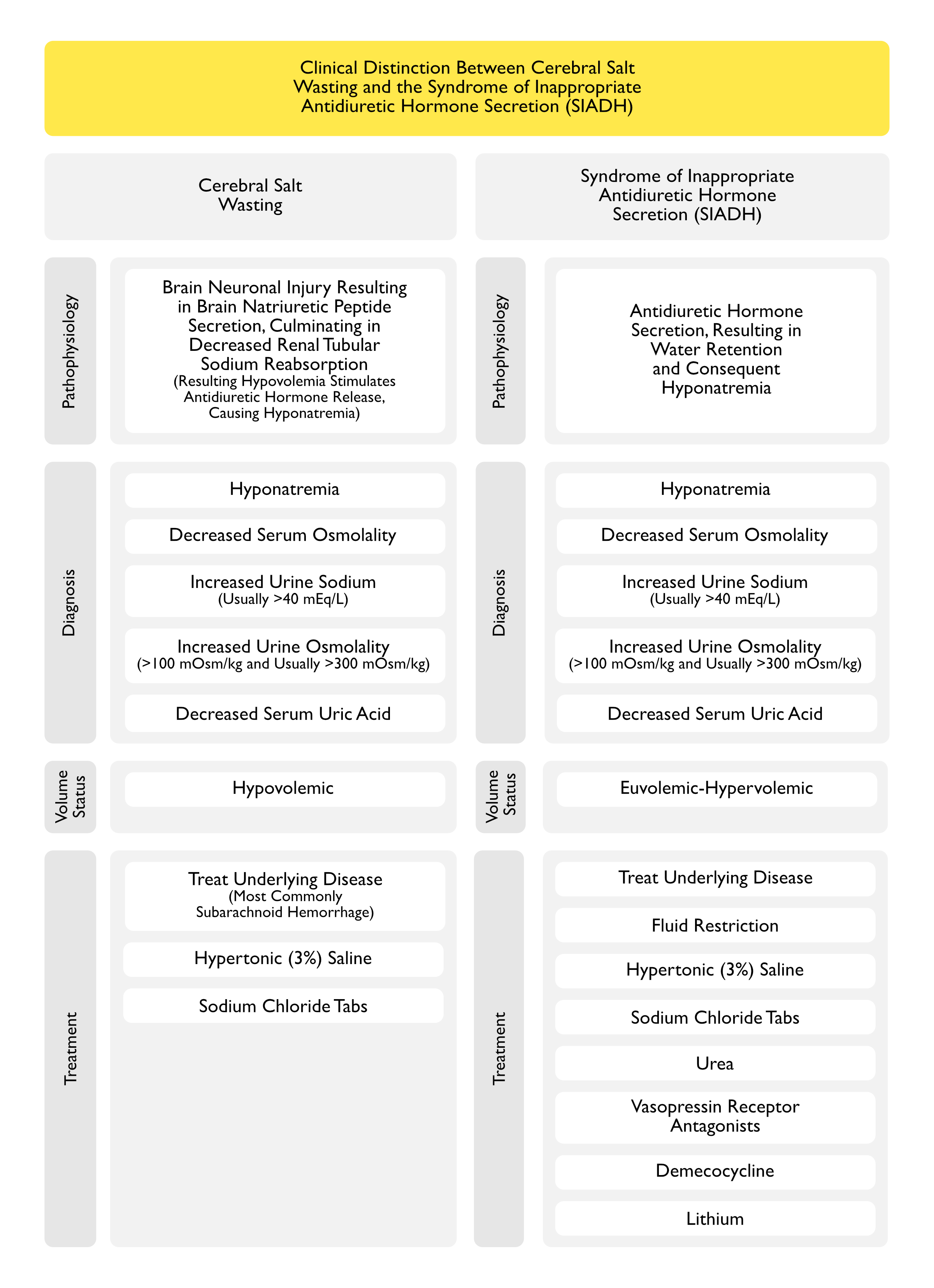
Cerebral Salt Wasting and Syndrome of Inappropriate Antidiuretic Hormone Secretion Share the Following Clinical Features (see Cerebral Salt Wasting)
- Hyponatremia with Increased Antidiuretic Hormone Release and Inappropriately Increased Urine Osmolality
- Hyponatremia Would Normally Inhibit Antidiuretic Hormone Release
- The Increased ADH Release is an Appropriate Response in Cerebral Salt Wasting, But is an Inappropriate Response in SIADH
- Increased Urine Sodium (Usually >40 mEq/L)
- In Cerebral Salt Wasting, This is Due to Renal Salt Wasting
- In SIADH, This is Due to Volume Expansion
- Decreased Serum Uric Acid Due to Decreased Urinary Uric Acid Excretion
- In Cerebral Salt Wasting, This is Likely Due to Brain Natriuretic Peptide (BNP)
- In SIADH, This is Likely Due to Volume Expansion and a Direct Effect of Antidiuretic Hormone on the V1 Receptor (Am J Kidney Dis, 1992) [MEDLINE]
Cerebral Salt Wasting from Syndrome of Inappropriate Antidiuretic Hormone Secretion (SIADH) are Distinguished by the Following Clinical Features (see Cerebral Salt Wasting)
- In Cerebral Salt Wasting, Clinical Hypovolemia is Present
- In SIADH, Extracellular Fluid Volume is Normal-Slightly Increased
Clinical Manifestations
General Comments
Schwartz and Bartter Criteria for the Diagnosis of the Syndrome of Inappropriate Antidiuretic Hormone Secretion (SIADH) (Am J Med, 1957) [MEDLINE] (Am J Med, 1967) [MEDLINE]
- Criteria were Developed in 1967
- Criteria
- Hyponatremia with Corresponding Hypo-Osmolality of Plasma and Extracellular fluid
- Continued Renal Excretion of Sodium
- Urine Less than Maximally Dilute
- Urinary Osmolality Greater than Appropriate Considering the Plasma Osmolality
- Absence of Clinical Volume Depletion
- Absence of Other Causes of Hyponatremia
- Normal Renal and Adrenal Function
- Correction of Hyponatremia by Fluid Restriction
Cardiovascular Manifestations
- Euvolemia/Modest Hypervolemia
- This Distinguishes SIADH from Cerebral Salt Wasting, Where the Patient is Typically Hypovolemic (see Cerebral Salt Wasting)
Renal Manifestations
- Hyponatremia (see Hyponatremia)
Treatment
Treat the Underlying Etiology of the Syndrome of Inappropriate Antidiuretic Hormone Secretion (SIADH)
- Critical Aspect of Management
Demeclocycline (see Demeclocycline)
- Pharmacology
- Demeclocycline Inhibits the Renal Action of Antidiuretic Hormone
- Demeclocycline Interferes with Intracellular Adenylyl Cyclase Activation After Antidiuretic Hormone Binds to Renal Vasopressin V2 Receptors
- Demeclocycline Inhibits the Renal Action of Antidiuretic Hormone
- Administration
- Oral Dose: 300 mg PO BID
Fluid Restriction
Clinical Use
- Fluid Restriction is the Most Commonly Used First-Line Therapy for Syndrome of Inappropriate Antidiuretic Hormone Secretion (SIADH)
- Fluid Restriction is the Most Commonly Used Treatment for SIADH (Used in 48% of Cases) (Am J Med, 2016) [MEDLINE]
Clinical Efficacy
- Fluid Restriction to 50-60% of the Daily Requirement (Approximately <800 mL/Day) May be Required to Achieve Negative Water Balance (NEJM, 2000) [MEDLINE]
- However, This Level of Fluid Restriction is Difficult for Most Patients to Maintain
- Practically, Most Patients are Able to Tolerate a Fluid Restriction Between 1000-1200 mL/Day
- Effectiveness of Fluid Restriction is Predicted by Urine/Plasma Electrolyte Ratio (Urine Na + Urine K/ Serum Na) <0.5 (Am J Med Sci, 2000) [MEDLINE]
- Urine/Plasma Electrolyte Ratio >1.0 Suggests that Fluid Restriction Will Not Be Effective
- Fluid Restriction Typically Results in a Median Increase in the Serum Sodium of Approximately 2 mEq/L in the First 24 hrs of Therapy (Am J Med, 2016) [MEDLINE]
- In a Small Trial (n = 46) in Patients with Chronic Asymptomatic SIADH, Fluid Restriction of <1L/day Resulted in an Increase in Serum Sodium by 3 mEq/L at 3 Days with Minimal Subsequent Additional Improvement (J Clin Endocrinol Metab, 2020) [MEDLINE]
Contraindications
- Syndrome of Inappropriate Antidiuretic Hormone Secretion (SIADH) in the Setting of Subarachnoid Hemorrhage (SAH) (see Subarachnoid Hemorrhage)
- In This Clinical Setting, Fluid Restriction May Cause Undesirable Hypovolemia and Hypotension, Which May Impair Cerebral Perfusion and Exacerbate Cerebral Vasospasm (and Worsen Cerebral Infarction) (Clin Neurol Neurosurg, 1990) [MEDLINE]
Hypertonic (3%) Saline (see Hypertonic Saline)
Pharmacology
- Hypertonic Saline Contains 512 mEq Na/L
- Approximate Hypertonic Saline Infusion Rate = Desired Rate of Correction Per Hour (ex: 1 mEq/L/hr) x Lean Body Weight (in kg)
Rationale
- If the Serum Sodium Concentration is to Be Increased, the Sodium Concentration of the Fluid Administered Must Exceed the Sodium Concentration of the Urine, Not Simply the Sodium Concentration of the Plasma (Am J Med, 1986) [MEDLINE]
- Sodium and Water Excretion in the Urine are Regulated Independently
- Sodium Excretion in the Urine is Regulated by Aldosterone and Atrial Natriuretic Peptide
- Water Excretion in the Urine is Regulated by Antidiuretic Hormone (Arginine Vasopressin)
- Urine Volume is Normally Regulated by Antidiuretic Hormone (Arginine Vasopressin) in Response to Changes in Water Intake
- When Antidiuretic Hormone Does Not Respond to Changes in Water Intake, as Occurs in Syndrome of Inappropriate Antidiuretic Hormone Secretion (SIADH), the Urine Osmolality is Relatively Fixed and the Urine Volume Varies with Changes in Solute Excretion
- Increasing Urine Solute Excretion by Giving Salt or Urea Will Increase the Urine Volume and Raise the Serum Sodium
Indications
- Life-Threatening Hyponatremia
Loop Diuretics
- Clinical Effectiveness
- In Addition to Other Measures, Loop Diuretics May Be Effective in the Syndrome of Inappropriate Antidiuretic Hormone Secretion (SIADH) if the Urine/Serum Cation Ratio is >1.0
- Loop Diuretics
- Furosemide (Lasix) (see Furosemide)
- Furosemide Inhibits Sodium chloride Reabsorption in the Thick Ascending Limb of the Loop of Henle, Resulting in Interference with the Countercurrent Mechanism and Inducing Renal Antidiuretic Hormone Resistance and Excretion of Water
- Furosemide (Lasix) (see Furosemide)
Oral Urea (see Urea)
Potassium Replacement (When Required for Hypokalemia) (see Potassium Chloride)
- Pharmacology
- Potassium is as Osmotically Active as Potassium and Replacing Potassium in the Setting of Hypokalemia Will Increase Serum Osmolality (Am J Kidney Dis, 2010) [MEDLINE]
- Potassium Movement Intracellularly Increases the Serum Sodium by the Following Mechanisms
- Intracellular Movement of Potassium Will Result in an Exchange of Sodium into the Extracellular Fluid (to Maintain Intracellular Electroneutrality)
- Intracellular Movement of Potassium Will Result in an Exchange of Hydrogen Ions into the Extracellular Fluid
- Hydrogen Ions are Buffered by Extracellular Bicarbonate (and Plasma Proteins), Creating Carbon Dioxide and Water (Bicarbonate is Replaced by Chloride Which was Administered with the Potassium)
- Intracellular Movement of Potassium Drags Drags Chloride into the Cells, Increasing the Intracellular Osmolality, Which Results in Free Water Movement into Cells
- Intracellular Movement of Potassium Increases the Intracellular Osmolality, Which Results in Free Water Movement into Cells
Sodium Chloride Tablets (see Sodium Chloride)
Clinical Utility
- Sodium Chloride Tablets are Commonly Utilized (in Conjunction with Fluid Restriction) in Patients with Na >120 mE/L
- Hourly Sodium Chloride Tablets Can Even Be Used Instead of Hypertonic (3%) Saline) in Non-Urgent Situations (Clin Nephrol, 2014) [MEDLINE]
Pharmacology
- A Quantity of 9 g of Oral Sodium Chloride Provides a Similar Quantity of Sodium as 1 L of Normal Saline (154 mEq), But without Any Water
- A Quantity of 1 g of Oral Sodium Chloride is Equivalent to 35 mL of 3% Saline
Administration
- Dose1-3g PO BID-q4hrs
Adverse Effects
- Nausea (see Nausea and Vomiting)
Vasopressin Receptor Antagonists (see Vasopressin Receptor Antagonists)
Agents
- Conivaptan (Vaprisol) (see Conivaptan)
- Pharmacology
- 1a/V2 Vasopressin Receptor Antagonist: causes aquaresis (water loss)
- Pharmacology
- Tolvaptan (Samsca) (see Tolvaptan)
- Pharmacology
- V2 Vasopressin Receptor Antagonist: causes aquaresis (water loss)
- Clinical Efficacy
- The SALT-1 Trial/SALT-2 Trials Comparing Tolvaptan to Placebo in Patients with Chronic Hyponatremia (None with Clinically Apparent Neurologic Symptoms at Baseline; Almost All Patients Had Na ≥120 mEq/L) Demonstrated a Benefit in Mental Status in Patients with Na 120-129 mEq/L, But Not in Patients with Na 130-134 mEq/L (NEJM, 2006) [MEDLINE]
- Pharmacology
Avoid Use of the Following
- Normal Saline (see Normal Saline): sodium will generally worsen the hyponatremia in Syndrome of Inappropriate Antidiuretic Hormone Secretion (SIADH)
- In Patients with Postoperative Hyponatremia Due to Surgery-Associated Syndrome of Inappropriate Antidiuretic Hormone Secretion (SIADH), Isotonic Intravenous Fluid Administration Results in Volume Expansion, Resulting in Increased Urinary Sodium Excretion
- With High Antidiuretic Hormone Levels, Sodium Excretion in a Concentrated Urine Results in a Further Decrease in the Serum Sodium (“Desalination”) (Ann Intern Med, 1997) [MEDLINE]
- In Patients with Postoperative Hyponatremia Due to Surgery-Associated Syndrome of Inappropriate Antidiuretic Hormone Secretion (SIADH), Isotonic Intravenous Fluid Administration Results in Volume Expansion, Resulting in Increased Urinary Sodium Excretion
Therapy of Syndrome of Inappropriate Antidiuretic Hormone Secretion in the Setting Subarachnoid Hemorrhage (SAH) (see Subarachnoid Hemorrhage)
- Avoid Fluid Restriction
- Since Patients with Subarachnoid Hemorrhage are Susceptible to Cerebral Vasospasm and Infarction, Fluid Restriction is Contraindicated, as it May Cause Hypotension and Exacerbate the Prior Complications (Clin Neurol Neurosurg, 1990) [MEDLINE]
- Hypertonic (3%) Saline (see Hypertonic Saline)
- Recommended Regimen is to Start at 20 mL/hr with Serial Sodium Measurement q4-6hrs (Neurocrit Care, 2009) [MEDLINE]
- Sodium Chloride Tablets (see Sodium Chloride)
References
Etiology
- Water intoxication and oxytocin. Br Med J (Clin Res Ed). 1982;285(6337):243 [MEDLINE]
- Idiopathic syndrome of inappropriate antidiuretic hormone secretion possibly related to advanced age. Ann Intern Med. 1983 Aug;99(2):185-8 [MEDLINE]
- The effect of vasopressin on solute and water excretion during and after surgical operations. Ann Surg. 1985;201(3):383 [MEDLINE]
- Hospital-associated hyponatremia. Kidney Int. 1986;29(6):1237 [MEDLINE]
- Temporal arteritis revealed by a syndrome of inappropriate secretion of antidiuretic hormone. Am J Med. 1988;85(4):559 [MEDLINE]
- Hyponatremia and seizures after intravenous administration of desmopressin acetate for surgical hemostasis. J Pediatr. 1989;114(3):470 [MEDLINE]
- Frequency of hyponatremia and nonosmolar vasopressin release in the acquired immunodeficiency syndrome. JAMA. 1990;263(7):973 [MEDLINE]
- Significant hyponatremia following DDAVP administration in a healthy adult. Am J Hematol. 1993;44(1):12 [MEDLINE]
- Hyponatremia after transsphenoidal surgery for pituitary tumors. J Clin Endocrinol Metab. 1994;79(5):1395 [MEDLINE]
- Isolated hyponatremia after transsphenoidal pituitary surgery. J Clin Endocrinol Metab. 1995;80(1):85 [MEDLINE]
- Syndrome of inappropriate secretion of antidiuretic hormone (SIADH) in malignant disease. J Intern Med. 1995;238(2):97 [MEDLINE]
- Elevated arginine vasopressin levels in squamous cell cancer of the head and neck. Laryngoscope. 1996;106(3 Pt 1):317 [MEDLINE]
- Syndrome of inappropriate antidiuretic hormone secretion associated with head neck cancers: review of the literature. Ann Otol Rhinol Laryngol. 1997;106(10 Pt 1):878 [MEDLINE]
- A prospective study of patients with lung cancer and hyponatremia of malignancy. Am J Respir Crit Care Med. 1997;156(5):1669 [MEDLINE]
- Acute hyponatremia in the perioperative period: insights into its pathophysiology and recommendations for management. Clin Nephrol. 1998;50(6):352 [MEDLINE]
- Hyponatremia with venlafaxine. Ann Pharmacother. 1998 Jan;32(1):49-51. doi: 10.1345/aph.17117 [MEDLINE]
- The syndrome of inappropriate antidiuretic hormone secretion of unknown origin. Am J Kidney Dis. 1999;33(1):161 [MEDLINE]
- Hyponatremia. N Engl J Med. 2000;342(21):1581 [MEDLINE]
- Adverse events during use of intranasal desmopressin acetate for haemophilia A and von Willebrand disease: a case report and review of 40 patients. Haemophilia. 2000;6(1):11 [MEDLINE]
- Chronic idiopathic hyponatremia in older people due to syndrome of inappropriate antidiuretic hormone secretion (SIADH) possibly related to aging. J Am Geriatr Soc. 2001 Jun;49(6):788-92 [MEDLINE]
- Hyponatremia as a complication of cardiac catheterization: a prospective study. Am J Kidney Dis. 2002;40(5):940 [MEDLINE]
- A review of drug-induced hyponatremia. Am J Kidney Dis. 2008 Jul;52(1):144-53. doi: 10.1053/j.ajkd.2008.03.004 [MEDLINE]
- Molecular mechanisms of antidiuretic effect of oxytocin. J Am Soc Nephrol. 2008;19(2):225 [MEDLINE]
- Clinical practice guideline on diagnosis and treatment of hyponatraemia. Neprhol Dial Transplant 2014; 29 Suppl 2:i1 [MEDLINE]
- Severe hyponatremia in older patients at admission in an internal medicine department. Arch Gerontol Geriatr. Nov-Dec 2014;59(3):642-7. doi: 10.1016/j.archger.2014.08.002 [MEDLINE]
- Antidepressants and the risk of hyponatremia: a class-by-class review of literature. Psychosomatics. Nov-Dec 2014;55(6):536-47. doi: 10.1016/j.psym.2014.01.010 [MEDLINE]
- Hyponatremia is a predictor for poor outcome in Guillain-Barré syndrome. Neurol Res. 2015 Apr;37(4):347-51. doi: 10.1179/1743132814Y.0000000455 [MEDLINE]
- Nephrogenic syndrome of inappropriate antidiuresis secondary to an activating mutation in the arginine vasopressin receptor AVPR2. Clin Endocrinol (Oxf). 2016;85(2):306 [MEDLINE]
- J Syndrome of Inappropriate Secretion of Antidiuretic Hormone Preceding Guillain-Barré Syndrome. Clin Diagn Res. 2017 Sep;11(9):OD16-OD17. doi: 10.7860/JCDR/2017/30445.10662 [MEDLINE]
- Medication-induced SIADH: distribution and characterization according to medication class. Br J Clin Pharmacol. 2017 Aug;83(8):1801-1807. doi: 10.1111/bcp.13256 [MEDLINE]
- Hyponatremia induced by antiepileptic drugs in patients with epilepsy. Expert Opin Drug Saf. 2017 Jan;16(1):77-87. doi: 10.1080/14740338.2017.1248399 [MEDLINE]
- Associations of proton pump inhibitors and hospitalization due to hyponatremia: A population-based case-control study. Eur J Intern Med. 2019 Jan;59:65-69. doi: 10.1016/j.ejim.2018.08.012 [MEDLINE]
- Anticancer Medications and Sodium Dysmetabolism. Eur Endocrinol. 2020 Oct;16(2):122-130. doi: 10.17925/EE.2020.16.2.122 [MEDLINE]
- Syndrome of Inappropriate Secretion of Antidiuretic Hormone Caused by Very Short-term Use of Proton Pump Inhibitor. Keio J Med. 2021 Mar 25;70(1):19-23. doi: 10.2302/kjm.2020-0008-CR [MEDLINE]
- Unusual Neurological Manifestation of Proton Pump Inhibitor: A Case Report of Acute Disseminated Encephalomyelitis and Severe Hyponatremia After Brief Use of Proton Pump Inhibitor. Cureus. 2021 Jun; 13(6): e15571 [MEDLINE]
Diagnosis
- Diagnosing and Treating the Syndrome of Inappropriate Antidiuretic Hormone Secretion. Am J Med. 2016;129(5):537.e9 [MEDLINE]
Clinical
- A syndrome of renal sodium loss and hyponatremia probably resulting from inappropriate secretion of antidiuretic hormone. Am J Med. 1957 Oct;23(4):529-42. doi: 10.1016/0002-9343(57)90224-3 [MEDLINE]
- The syndrome of inappropriate secretion of antidiuretic hormone. Am J Med 1967; 42: 790-806 [MEDLINE]
- Cerebral salt wasting versus SIADH: what difference? J Am Soc Nephrol. 2008;19(2):194 [MEDLINE]
Treatment
- New approach to disturbances in the plasma sodium concentration. Am J Med. 1986;81(6):1033 [MEDLINE]
- Hyponatremia responsive to fludrocortisone acetate in elderly patients after head injury. Ann Intern Med. 1987;106(2):187 [MEDLINE]
- Effect of fludrocortisone acetate in patients with subarachnoid hemorrhage. Stroke. 1989;20(9):1156 [MEDLINE]
- The effects of treating hypertension following aneurysmal subarachnoid hemorrhage. Clin Neurol Neurosurg. 1990;92(2):111 [MEDLINE]
- Fludrocortisone therapy in cerebral salt wasting. Pediatrics. 2006;118(6):e1904 [MEDLINE]
- Performance characteristics of a sliding-scale hypertonic saline infusion protocol for the treatment of acute neurologic hyponatremia. Neurocrit Care. 2009;11(2):228 [MEDLINE]
- Clinical practice guideline on diagnosis and treatment of hyponatraemia. Neprhol Dial Transplant 2014; 29 Suppl 2:i1 [MEDLINE]
- Diagnosing and Treating the Syndrome of Inappropriate Antidiuretic Hormone Secretion. Am J Med. 2016;129(5):537.e9 [MEDLINE]
- Fluid Restriction Therapy for Chronic SIAD; Results of a Prospective Randomized Controlled Trial. J Clin Endocrinol Metab. 2020;105(12) [MEDLINE]