Acute Hyponatremia is More Likely to Produce Clinical Symptoms than Chronic Hyponatremia
Risk of Complications (of Hyponatremia Itself and/or as a Result of Treatment of Hyponatremia)
The More Acute that the Hyponatremia is, the Higher the Risk of Clinical Complications (and the Greater the Need for Aggressive Therapy)
Chronic Hyponatremia
Defintion: hyponatremia of ≥48 hrs in duration or of unclear duration (if the patient develops hyponatremia in the outpatient setting)
Probability of Clinical Symptoms
Chronic Hyponatremia is Less Likely to Produce Clinical Symptoms than Acute Hyponatremia
Risk of Complications (of Hyponatremia Itself and/or as a Result of Treatment of Hyponatremia)
The More Chronic that the Hyponatremia is, the Lower the Risk of Clinical Complications (and the Greater the Risk for Complications from Corrective Therapy Itself)
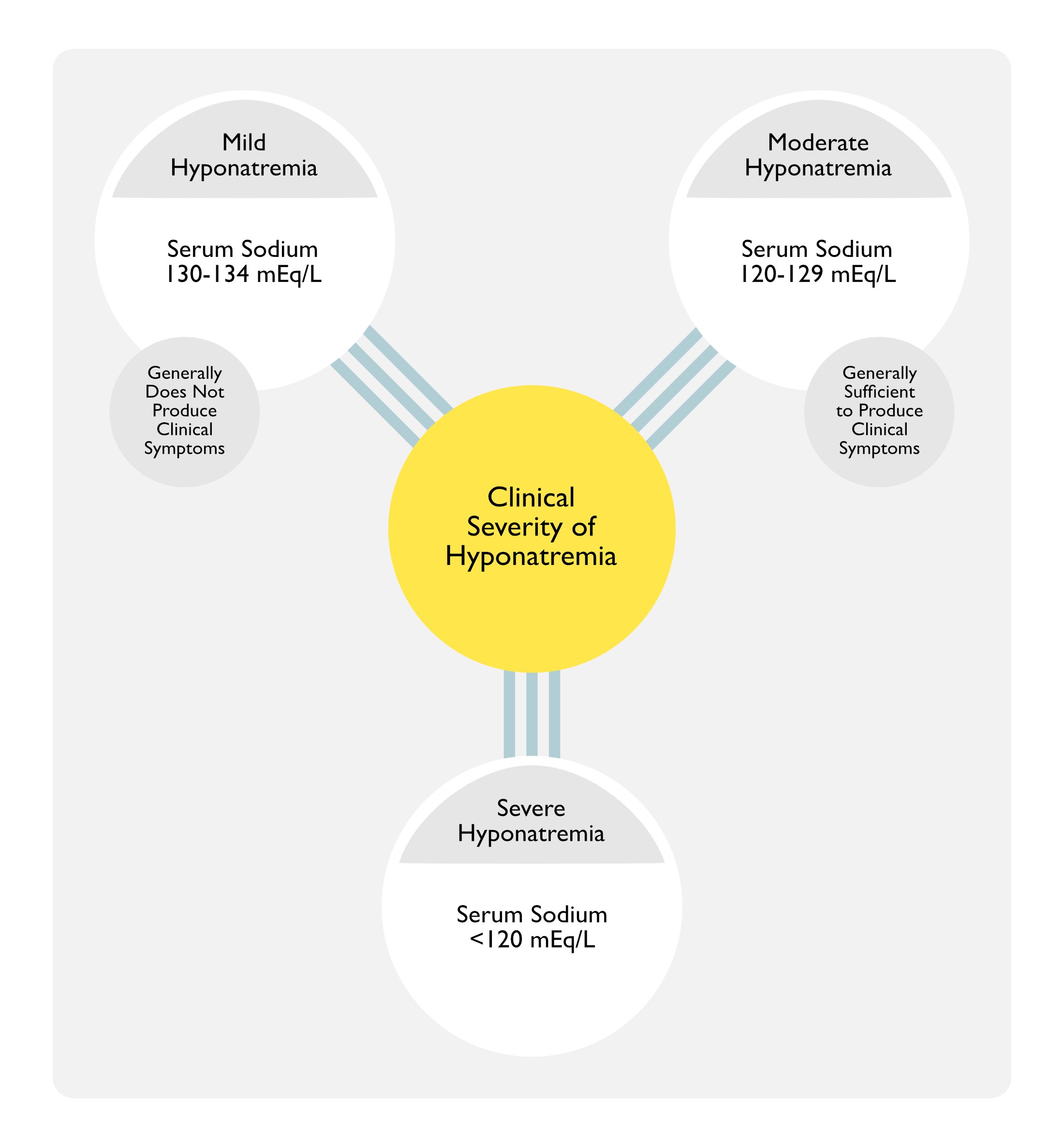
Severity of Hyponatremia
Mild Hyponatremia: serum sodium 130-134 mEq/L
Serum Na 130-134 mEq/L Generally Does Not Produce Clinical Symptoms
Moderate Hyponatremia: serum sodium 120-129 mEq/L
Serum Na <130 mEq/L is Generally Sufficient to Produce Clinical Symptoms
Severe Hyponatremia: serum sodium <120 mEq/L
Severity of Clinical Symptoms
Asymptomatic
Many Apparently “Asymptomatic” Patients with Chronic Hyponatremia (Especially with Moderate Hyponatremia of 120-129 mEq/L) May Have Subtle Neurologic Impairments (Abnormal Mentation, Gait Impairment with Increased Risk of Falls) (Am J Med, 2006) [MEDLINE] (QJM, 2008) [MEDLINE]
Mild-Moderate Clinical Symptoms
General Comments
Mild-Moderate Clinical Symptoms are Most Commonly Encountered in Patients with Chronic, Severe (Na <120 mEq/L) Hyponatremia
Mild-Moderate Clinical Symptoms Result from Brain Adaptations Which Minimize the Development of Cerebral Edema, But Modify the Composition of Brain Cells
Mild-Moderate Clinical Symptoms are Not Typically Associated with a Increased Risk of Impending Brain Herniation
However, in Patients with Very Severe Hyponatremia (Na <110 mEq/L), Mild-Moderate Clinical Symptoms May Precede the Development of Seizures
Additionally, the Presence of Mild-Moderate Clinical Symptoms in a Patient with Acute Hyponatremia (Even with Na >120 mEq/L) Should Be Considered as an Ominous Precursor of Seizures/Respiratory Arrest/Cerebral Edema with Brain Herniation (Ann Intern Med, 2000) [MEDLINE]
Nausea is an Early Finding and Occurs When the Serum Sodium Falls Below 125-130 mEq/L
Nausea/Vomiting Occur in Approximately 30% of Patients with Serum Sodum <120 mEq/L (J Natl Med Assoc, 2004) [MEDLINE] (Am J Med, 2012) [MEDLINE] (J Am Geriatr Soc, 2015) [MEDLINE]
Clinical
In Acute Hyponatremia, Nausea/Vomiting Can Be a Harbinger of Life-Threatening Cerebral Edema
In Chronic Hyponatremia, Nausea/Vomiting is Not Typically Associated with Adverse Outcomes
Neurologic Manifestations
Ataxia/Gait Disturbance (with Increased Risk of Falls) (see Ataxia)
Epidemiology
Mild-Moderate Hyponatremia (Na 120-130 mEq/L) is Associated with an Increased Risk of Falls in Elderly Patients (Mean Age 72 y/o), Possibly Due to Marked Gait and Attention Impairment (Am J Med, 2006) [MEDLINE]
Correction of Hyponatremia (Usually with Urea) Improved Reaction Time and Gait Performance (Eur J Intern Med, 2017) [MEDLINE]
The Effect was Significant Among Patients >65 y/o, But Not in Younger Patients
Cerebral Edema with Brain Herniation Occurs Almost Exclusively in the Following Hyponatremic Patient Subsets
Patients with Hyponatremia Associated with Self-Induced Water Intoxication (Runners, Psychotic Patients with Severe Polydipsia, Ecstasy Users, etc
Children/Females with Acute Postoperative Hyponatremia (NEJM, 1986) [MEDLINE] (BMJ, 1992) [MEDLINE] (Ann Intern Med, 1992) [MEDLINE]: this may be due to a hormonally-mediated decrease in the degree of osmotic adaptation, brain size relative to the cranial vault size, or smaller body size with less muscle mass to absorb the excess water (Am J Physiol, 1989) [MEDLINE]
Patients with with Hyponatremia Associated with Intracranial Pathology (Traumatic Brain Injury, Intracranial Hemorrhage, Intracranial Surgery, Intracranial Mass, etc)
In Other Patient Subsets, Hyponatremia-Induced Cerebral Edema is Rare
In One Study of 664 Patients with Hyponatremia <120 mEq/L, Only 1 Patient Died from Cerebral Edema and the Patient Had Concomitant Intracranial Pathology (Clin J Am Soc Nephrol, 2011) [MEDLINE]
Concomitant Hypoxemia (of Any Etiology) Increases the Risk of Hyponatremia-Induced Cerebral Edema (Ann Intern Med, 2000) [MEDLINE]
Lethargy/Obtundation/Coma Occurs when the Serum Sodium Falls to <115-120 mEq/L
Lethargy/Obtundation/Coma May Occur in Acute Hyponatremia Due to a Rapid Decline in the Serum Sodium (Not Allowing the Brain Adequate Time for Adaptation)
Prognosis
Acute Hyponatremic Encephalopathy is Generally Reversible
However, Permanent Neurologic Damage May Occur, Particularly in Premenopausal Females (Ann Intern Med, 1992) [MEDLINE] (Nephrol Dial Transplant, 2003) [MEDLINE]
Risk of Seizures is Related to the Chronicity of Hyponatremia
Seizures are Common in Acute Hyponatremia Due to a Rapid Decline in the Serum Sodium (Not Allowing the Brain Adequate Time for Adaptation)
In Acute Hyponatremia with Serum Sodium <110 mEq/L, Seizures Occurred in 30% of Cases (Ann Intern Med, 1987) [MEDLINE]
Seizures are Less Common in Chronic Hyponatremia (Even Severe Chronic Hyponatremia)
In Chronic Hyponatremia with Serum Sodium <110 mEq/L, Seizures Occurred in Only 7% of Cases (Ann Intern Med, 1987) [MEDLINE]
In a Study of 223 Hospitalized Patients with Symptomatic Chronic Thiazide-Induced Hyponatremia, Seizure Incidence was Only 1% (and There were No Cases of Herniation) (J Natl Med Assoc, 2004) [MEDLINE]
In Chronic Hyponatremia, the Risk of Seizures May Be Increased in Patients with an Underlying Seizure Disorder or Alcohol Withdrawal
Risk of Seizures is Related to the Severity of Hyponatremia (Epilepsia, 2011) [MEDLINE]
Serum Sodium 115-119 mEq/L: Seizures Occurred in 2.5% of Cases
Serum Sodium 110-114 mEq/L: Seizures Occurred in 5.4% of Cases
Serum Sodium <110 mEq/L: Seizures Occurred in 10% of Cases
May Occur in Some Cases When the Serum Sodium Falls <115-120 mEq/L (Ann Intern Med, 2000) [MEDLINE]
Rheumatologic Manifestations
Increased Risk of Osteoporosis (with Increased Risk of Fractures) (see Osteoporosis)
Epidemiology
May Be Seen in Chronic Hyponatremia (Due to Loss of Bone Sodium) (QJM, 2008) [MEDLINE] (J Bone Miner Res, 2010) [MEDLINE]
Treatment
General Comments
General Indications for Hospitalization in the Setting of Hyponatremia
Acute Hyponatremia
Severe Hyponatremia (Na <120 mEq/L)
Symptomatic Hyponatremia
Need for Correction of Hyponatremia
Correction of Hyponatremia is Associated with a Decreased Mortality Rate (PLoS, 2015) [MEDLINE]
Association was Even Stronger When Only Studies with Serum Sodium Threshold of >130 mEq/L were Considered
Impact on Mortality is Even Greater in Older Patients and in Those with Lower Serum Sodium on Enrollment
General Goals of Hyponatremia Therapy
Prevent a Further Decline in the Serum Sodium (This Goal is Particularly Applicable in Specific Hyponatremia Patient Groups)
Patients with Hyponatremia Associated with Self-Induced Water Intoxication (Runners, Psychotic Patients with Severe Polydipsia, Ecstasy Users, etc)
Continuing Absorption of Ingested Water from the Gastrointestinal Tract May Result in a Further Decrease in the Serum Sodium
Patients with Hyponatremia Associated with Intravenous Fluid Administration (Postoperative Hyponatremia Associated with Surgery-Associated SIADH, etc)
Isotonic Intravenous Fluid Administration Results in Volume Expansion, Resulting in Increased Urinary Sodium Excretion
With High Antidiuretic Hormone Levels, Sodium Excretion in a Concentrated Urine Results in a Further Decrease in the Serum Sodium (“Desalination”) (Ann Intern Med, 1997) [MEDLINE]
Therefore, Isotonic Saline Administration Should Be Avoided in this Setting (i.e in the Setting of SIADH)
Specific Hyponatremia Patient Groups with High-Risk of Herniation
Acute Hyponatremia Associated with Massive Water Ingestion (Due to Psychosis, Extreme Exercise, Ecstasy Intoxication)
Children/Women with Acute Postoperative Hyponatremia
Hyponatremia Associated with Intracranial Pathology (Traumatic Brain Injury, Recent Intracranial Surgery, Intracranial Hemorrhage, Intracranial Neoplasm or Space-Occupying Lesion)
Outside of These Patients Group, the Development of Brain Herniation is Rare
In a Series of Patients with Hyponatremia, Only 1 Out of 664 Patients with a Na <120 mEq/L Admitted to a Community Hospital Died from Cerebral Edema (and the Patient Had Coexistent Intracranial Pathology) (Clin J Am Soc Nephrol, 2011) [MEDLINE]
General Comments
In the Above High-Risk Patients, Rapid Progression of Hyponatremia to Na <130 mEq/L, Even with Mild-Moderate Clinical Symptoms, Can Rapidly Progress to Seizures, Respiratory Arrest, and Brain Herniation
If Noncardiogenic Pulmonary Edema Occurs, Hypoxemia May Further Exacerbate the Development of Cerebral Edema (Ann Intern Med, 2000) [MEDLINE]
Impending Brain Herniation Can Be Effectively Reversed with a Relatively Modest 4-6 mEq/L Increase in the Serum Sodium (Semin Nephrol, 2009) [MEDLINE]
Relieve the Symptoms of Hyponatremia
The Urgency to Correct Hyponatremia Varies Depending on the Chronicity of the Hyponatremia, the Serum Sodium Concentration, and the Severity of the Clinical Symptoms
Importantly, Even the Most Severe Clinical Symptoms Can Be Effectively Reversed with a Relatively Modest 4-6 mEq/L Increase in the Serum Sodium (Semin Nephrol, 2009) [MEDLINE]
This Fact Accentuates the Caution that There is Potential Harm with Correcting Hyponatremia at Faster Rate
Target an Appropriate Rate of Hyponatremia Correction
Rationale
During the Correction of Hyponatremia, the Reuptake of Solutes by Brain Cells Occurs More Slowly than the Loss of Brain Solutes During the Onset of Hyponatremia
For This Reason (and Out of Concern for the Potential Development of Osmotic Demyelination Syndrome), the Rate of Correction of Hyponatremia is Critical
Overly Rapid Correction of the Sodium Concentration Can Occur Following Almost All of the Usual Hyponatremia Therapies
Elimination of the Underlying Etiology of Hyponatremia
Glucocorticoid Therapy in the Setting of Adrenal Insufficiency (see Corticosteroids)
Case Series Examining the Use of 3% Saline to Treat Hyponatremic Encephalopathy in the ED Setting (Am J Kidney Dis, 2015) [MEDLINE]: n = 64 (71 instances of hyponatremia)
Baseline Mean Serum Sodium was 114.1 ± 0.8 (SEM) mEq/L
Mean 3 hr Serum Sodium Correction to 117.9 ± 1.3
Mean 12 hr Serum Sodium Correction to 121.2 ± 1.2
Mean 24 hr Serum Sodium Correction to 123.9 ± 1.0 (Delta of Approximately 10 mEq/L in the First 24 hrs)
Mean 48 hr Serum Sodium Correction to 128.3 ± 0.8 mEq/L
No Cases of Osmotic Demyelination were Observed
Retrospective Cohort Study of Risk Factors for Rapid Correction of Hyponatremia (Clin J Am Soc Nephrol, 2018) [MEDLINE]: n = 1,490 patients admitted with serum sodium <120 mEq/L
Median Change in Serum Sodium at 24 hrs was 6.8 mEq/L (Interquartile Range, 3.4-10.2)
Rapid Correction of Hyponatremia Occurred in 41% of Patients
Risk Factors Associated with Rapid Correction
Younger Age
Female Sex
Schizophrenia
Lower Charlson Comorbidity Index
Lower Presentation Serum Sodium
Urine Sodium <30 mEq/L
Risk Factors Associated with Lower Risk of Rapid Correction
Prior Hyponatremia
Outpatient Aldosterone Antagonist Use
Treatment at an Academic Center
Approximately 88% of Patients with Incident Osmotic Demyelination Had a Documented Episode of Rapid Correction of Hyponatremia (with Serum Sodium Increase >8 mEq/L Over 24 hrs)
Retrospective Cohort Multicenter Study of the Rate of Hyponatremia Correction in Critical Care Patients with Serum Sodum <120 mEq/L (J Crit Care, 2023) [MEDLINE]: n = 1,024
Rapid Correction (>8 mEq/L Per Day) was Associated with Lower In-Hospital Mortality (Absolute Difference: -4.37%; 95% CI: -8.47 to -0.26%), Higher Number of Hospital-Free Days (1.80 Days; 95% CI: 0.82-2.79 Days), and Higher Number of Intensive Care Unit-Free Days (1.16 Days; 95% CI: 0.15-2.17 days)
There was No Significant Difference in Neurological Complications (2.31%; 95% CI: -0.77 to 5.40%)
Multicenter Observational Study of the Rate of Hyponatremia Correction in Patients with Serum Sodium <120 mEq/L (NEJM Evid, 2023) [MEDLINE]: n = 3,274
Correction Rate of <6 mEq/L Per 24 hrs was Observed in 38% of Cases, 6-10 mEq/L Per 24 hrs in 29% of Cases, and >10 mEq/L Per 24 hrs in 33% of Cases
As Compared to the 6-10 mEq/L Per 24 hrs Group, the <6 mEq/L Per 24 hrs Group was Associated with Higher In-Hospital Mortality Rate in Multivariable-Adjusted and Propensity Score-Weighted Analyses
As Compared to 6-10 mEq/L Per 24 hrs Group, the >10 mEq/L Per 24 hrs was Associated with Lower In-Hospital Mortality Rate and Shorter Length of Stay in Multivariable Analyses
Only 7 Patients Developed Osmotic Demyelination Syndrome (ODS)
5/7 Patients Developing ODS Despite a Correction Rate ≤8 mEq/L Per 24 hrs
6/7 Patients Had Alcohol Use Disorder, Malnutrition, Hypokalemia, or Hypophosphatemia
Canadian Multicenter Cohort Study of Rate of Hyponatremia Correction in Adult Patients (NEJM Evid, 2023) [MEDLINE]: n = 22,858 (from 5 academic hospitals between 2010-2020)
Mean Initial Serum Sodium was 125 mEq/L (SD: 4.6)
Serum Sodium 110-119 mmol/L: 11.9% of patients
Serum Sodium <110 mmol/L: 1.2% of patients
Overall, Rapid Correction of Serum Sodium Occurred in 17.7% of Patients
Only 12 Patients (0.05%) Developed Osmotic Demyelination Syndrome (ODS)
58% of Patients Who Developed ODS Did Not Have Rapid Correction of Sodium
Recommended Maximum Rate of Correction is ≤8 mEq/L in the First 24 hrs (Am J Med, 2007) [MEDLINE] (Semin Nephrol, 2009) [MEDLINE] (Curr Opin Nephrol Hypertens, 2010) [MEDLINE] (J Am Soc Nephrol, 2012) [MEDLINE]
Since the Actual Rate of Correction Often Exceeds the Goal Rate of Correction, this Recommendation May Help to Keep the Actual Rate of Correction Below the Maximal Rate of Correction of ≤8 mEq/L in the First 24 hrs
Specific Therapies for Selected Etiologies of Hyponatremia
Hypovolemic Hyponatremia
Crystalloid Intravenous Fluids
Normal Saline (NS) (see Normal Saline): contains 154 mEq Na/L
Normal Saline Would Be Expected to Increase Serum Sodium 1 mEq/L for Every Liter of Saline Infused, Since the Normal Saline Has Higher Sodium Concentration than the Hyponatremic Plasma
Normal Saline Correction of Hypovolemia Will Remove the Stimulus for Antidiuretic Hormone Secretion, Resulting in a Water Diuresis (Typically Evidence by an Increase in Urine Output)
Hypertonic Saline (3%) (see Hypertonic Saline): contains 512 mEq Na/L
In Patients with Symptomatic or Severe Hyponatremia (Na <120 mEq/L), Hypertonic Saline is Preferred Over Normal Saline, Since it More Reliably Increases the Serum Sodium (Especially if There is an Element of Coexistent SIADH)
In This Setting, Hypertonic Saline Combined with Desmopressin is Likely the Most Effective and Predictable Strategy
Approximate Hypertonic (3%) Saline Infusion Rate
Desired Rate of Correction Per Hour (ex: 1 mEq/L/hr) x Lean Body Weight (in kg)
One Should Avoid Using Lactated Ringers (LR) in a Hyponatremic Patient, Since it is Hypotonic (Contains 130 mEq Na/L) (see Lactated Ringers)
Potassium Replacement (When Required for Hypokalemia) (see Potassium Chloride)
Potassium is as Osmotically Active as Potassium and Replacing Potassium in the Setting of Hypokalemia Will Increase Serum Osmolality (Am J Kidney Dis, 2010) [MEDLINE]
Potassium Movement Intracellularly Increases the Serum Sodium by the Following Mechanisms
Intracellular Movement of Potassium Will Result in an Exchange of Sodium into the Extracellular Fluid (to Maintain Intracellular Electroneutrality)
Intracellular Movement of Potassium Will Result in an Exchange of Hydrogen Ions into the Extracellular Fluid
Hydrogen Ions are Buffered by Extracellular Bicarbonate (and Plasma Proteins), Creating Carbon Dioxide and Water (Bicarbonate is Replaced by Chloride Which was Administered with the Potassium)
Intracellular Movement of Potassium Drags Drags Chloride into the Cells, Increasing the Intracellular Osmolality, Which Results in Free Water Movement into Cells
Intracellular Movement of Potassium Increases the Intracellular Osmolality, Which Results in Free Water Movement into Cells
Primary Polydipsia
Fluid Restriction
Obviously, Fluid Restriction is a Key Component in This Subset of Hyponatremic Patients in Which Oral Fluid Intake is the Primary Etiology
Effectiveness of Fluid Restriction is Predicted by Urine/Plasma Electrolyte Ratio (Urine Na + Urine K/ Serum Na) <0.5 (Am J Med Sci, 2000) [MEDLINE]
Urine/Plasma Electrolyte Ratio >1.0 Suggests that Fluid Restriction Will Not Be Effective
Demeclocycline Inhibits the Renal Action of Antidiuretic Hormone
Demeclocycline Interferes with Intracellular Adenylyl Cyclase Activation After Antidiuretic Hormone Binds to Renal Vasopressin V2 Receptors
Dose: 300 mg PO BID
Fluid Restriction
Fluid Restriction to 50-60% of the Daily Requirement (Approximately <800 mL/Day) May be Required to Achieve Negative Water Balance (NEJM, 2000) [MEDLINE]
Effectiveness of Fluid Restriction is Predicted by Urine/Plasma Electrolyte Ratio (Urine Na + Urine K/ Serum Na) <0.5 (Am J Med Sci, 2000) [MEDLINE]
Urine/Plasma Electrolyte Ratio >1.0 Suggests that Fluid Restriction Will Not Be Effective
Furosemide Inhibits Sodium chloride Reabsorption in the Thick Ascending Limb of the Loop of Henle, Resulting in Interference with the Countercurrent Mechanism and Inducing Renal Antidiuretic Hormone Resistance and Excretion of Water
Potassium Replacement (When Required for Hypokalemia) (see Potassium Chloride)
Potassium is as Osmotically Active as Potassium and Replacing Potassium in the Setting of Hypokalemia Will Increase Serum Osmolality (Am J Kidney Dis, 2010) [MEDLINE]
Potassium Movement Intracellularly Increases the Serum Sodium by the Following Mechanisms
Intracellular Movement of Potassium Will Result in an Exchange of Sodium into the Extracellular Fluid (to Maintain Intracellular Electroneutrality)
Intracellular Movement of Potassium Will Result in an Exchange of Hydrogen Ions into the Extracellular Fluid
Hydrogen Ions are Buffered by Extracellular Bicarbonate (and Plasma Proteins), Creating Carbon Dioxide and Water (Bicarbonate is Replaced by Chloride Which was Administered with the Potassium)
Intracellular Movement of Potassium Drags Drags Chloride into the Cells, Increasing the Intracellular Osmolality, Which Results in Free Water Movement into Cells
Intracellular Movement of Potassium Increases the Intracellular Osmolality, Which Results in Free Water Movement into Cells
The SALT-1 Trial/SALT-2 Trials Comparing Tolvaptan to Placebo in Patients with Chronic Hyponatremia (None with Clinically Apparent Neurologic Symptoms at Baseline; Almost All Patients Had Na ≥120 mEq/L) Demonstrated a Benefit in Mental Status in Patients with Na 120-129 mEq/L, But Not in Patients with Na 130-134 mEq/L (NEJM, 2006) [MEDLINE]
Avoid Use of the Following
Normal Saline (see Normal Saline): sodium will generally worsen the hyponatremia in SIADH
In Patients with Postoperative Hyponatremia Due to Surgery-Associated SIADH, etc), Isotonic Intravenous Fluid Administration Results in Volume Expansion, Resulting in Increased Urinary Sodium Excretion
With High Antidiuretic Hormone Levels, Sodium Excretion in a Concentrated Urine Results in a Further Decrease in the Serum Sodium (“Desalination”) (Ann Intern Med, 1997) [MEDLINE]
Syndrome of Inappropriate Antidiuretic Hormone Secretion in the Setting Subarachnoid Hemorrhage (SAH) (see Subarachnoid Hemorrhage)
Avoid Fluid Restriction
Since Patients with Subarachnoid Hemorrhage are Susceptible to Cerebral Vasospasm and Infarction, Fluid Restriction is Contraindicated, as it May Cause Hypotension and Exacerbate the Prior Complications (Clin Neurol Neurosurg, 1990) [MEDLINE]
Hypervolemic Hyponatremia (Associated with Advanced Renal Failure)
Fluid and Sodium Restriction
Fluid Restriction to 50-60% of the Daily Requirement (Approximately <800 mL/Day) May be Required to Achieve Negative Water Balance (NEJM, 2000) [MEDLINE]
Effectiveness of Fluid Restriction is Predicted by Urine/Plasma Electrolyte Ratio (Urine Na + Urine K/ Serum Na) <0.5 (Am J Med Sci, 2000) [MEDLINE]
Urine/Plasma Electrolyte Ratio >1.0 Suggests that Fluid Restriction Will Not Be Effective
Fluid Restriction to 50-60% of the Daily Requirement (Approximately <800 mL/Day) May be Required to Achieve Negative Water Balance (NEJM, 2000) [MEDLINE]
Effectiveness of Fluid Restriction is Predicted by Urine/Plasma Electrolyte Ratio (Urine Na + Urine K/ Serum Na) <0.5 (Am J Med Sci, 2000) [MEDLINE]
Urine/Plasma Electrolyte Ratio >1.0 Suggests that Fluid Restriction Will Not Be Effective
Although Fluid Restriction is Commonly Used in Cirrhotic Patients with Ascites, it is Frequently Difficult to Achieve a Fluid Restriction <1-1.5L/Day (Gastroenterology, 2003) [MEDLINE]
Potassium Replacement (When Required for Hypokalemia) (see Potassium Chloride)
Potassium is as Osmotically Active as Potassium and Replacing Potassium in the Setting of Hypokalemia Will Increase Serum Osmolality (Am J Kidney Dis, 2010) [MEDLINE]
Potassium Movement Intracellularly Increases the Serum Sodium by the Following Mechanisms
Intracellular Movement of Potassium Will Result in an Exchange of Sodium into the Extracellular Fluid (to Maintain Intracellular Electroneutrality)
Intracellular Movement of Potassium Will Result in an Exchange of Hydrogen Ions into the Extracellular Fluid
Hydrogen Ions are Buffered by Extracellular Bicarbonate (and Plasma Proteins), Creating Carbon Dioxide and Water (Bicarbonate is Replaced by Chloride Which was Administered with the Potassium)
Intracellular Movement of Potassium Drags Drags Chloride into the Cells, Increasing the Intracellular Osmolality, Which Results in Free Water Movement into Cells
Intracellular Movement of Potassium Increases the Intracellular Osmolality, Which Results in Free Water Movement into Cells
The SALT-1 Trial/SALT-2 Trials Comparing Tolvaptan to Placebo in Patients with Chronic Hyponatremia Due to SIADH, Congestive Heart Failure, or Cirrhosis (None with Clinically Apparent Neurologic Symptoms at Baseline; Almost All Patients Had Na ≥120 mEq/L) Demonstrated a Benefit in Mental Status in Patients with Na 120-129 mEq/L, But Not in Patients with Na 130-134 mEq/L (NEJM, 2006) [MEDLINE]
While the FDA Recommends Against Using Tolvaptan in the Setting of Liver Disease/Cirrhosis (Due to Worsening of Liver Function), it Might Be Considered in a Patient with End-Stage Liver Disease Awaiting Liver Transplant (J Hepatol, 2012) [MEDLINE]
Conivaptan (Vaprisol) is Generally Avoided in Cirrhosis, Due to the Adverse Effects of Hypotension and Esophageal Variceal Hemorrhage (see Conivaptan)
Treat Hypotension
Discontinue β-Blockers and Other Antihypertensives (When MAP is <82 mm Hg)
MAP <82 mm Hg are Associated with Hyponatremia and Increased Mortality Rate in Cirrhotic Patients with Ascites (Gastroenterology, 1988) [MEDLINE] (J Hepatol, 2014) [MEDLINE]
Intravenous Albumin Infusion (Approximately 50-100 g Per Day) May Be Useful to Increase the Serum Sodium While Other Therapies are Initiated (Gut, 1990) [MEDLINE] (Am J Gastroenterol, 2018) [MEDLINE]
ACE-I’s/ARB’s Improve Cardiac Function, Decreasing the Release of Antidiuretic Hormone and Norepinephrine (Ann Intern Med, 1984) [MEDLINE]
Via the Local Generation of Prostaglandins, ACE-I’s Antagonize the Effect of Antidiuretic Hormone on the Collecting Tubules, Decreasing Collecting Tubular Water Reabsorption (Am J Cardiol, 1986) [MEDLINE]
Fluid and Sodium Restriction
Fluid Restriction is Commonly Used in the Hospital Setting to Manage Hyponatremia in the Setting of Congestive Heart Failure (Am Heart J, 1994) [MEDLINE]
Fluid Restriction is Generally Less Effective in the Outpatient Setting (Due to Thirst, etc)
Fluid Restriction to 50-60% of the Daily Requirement (Approximately <800 mL/Day) May be Required to Achieve Negative Water Balance (NEJM, 2000) [MEDLINE]
Effectiveness of Fluid Restriction is Predicted by Urine/Plasma Electrolyte Ratio (Urine Na + Urine K/ Serum Na) <0.5 (Am J Med Sci, 2000) [MEDLINE]
Urine/Plasma Electrolyte Ratio >1.0 Suggests that Fluid Restriction Will Not Be Effective
Loop Diuretics Decrease the Concentration Gradient in the Renal Medulla, Decreasing Water Reabsorption in the Collecting Duct (J Am Coll Cardiol, 2015) [MEDLINE]
Potassium Replacement (When Required for Hypokalemia) (see Potassium Chloride)
Potassium is as Osmotically Active as Potassium and Replacing Potassium in the Setting of Hypokalemia Will Increase Serum Osmolality (Am J Kidney Dis, 2010) [MEDLINE]
Potassium Movement Intracellularly Increases the Serum Sodium by the Following Mechanisms
Intracellular Movement of Potassium Will Result in an Exchange of Sodium into the Extracellular Fluid (to Maintain Intracellular Electroneutrality)
Intracellular Movement of Potassium Will Result in an Exchange of Hydrogen Ions into the Extracellular Fluid
Hydrogen Ions are Buffered by Extracellular Bicarbonate (and Plasma Proteins), Creating Carbon Dioxide and Water (Bicarbonate is Replaced by Chloride Which was Administered with the Potassium)
Intracellular Movement of Potassium Drags Drags Chloride into the Cells, Increasing the Intracellular Osmolality, Which Results in Free Water Movement into Cells
Intracellular Movement of Potassium Increases the Intracellular Osmolality, Which Results in Free Water Movement into Cells
The SALT-1 Trial/SALT-2 Trials Comparing Tolvaptan to Placebo in Patients with Chronic Hyponatremia Due to SIADH, Congestive Heart Failure, or Cirrhosis (None with Clinically Apparent Neurologic Symptoms at Baseline; Almost All Patients Had Na ≥120 mEq/L) Demonstrated a Benefit in Mental Status in Patients with Na 120-129 mEq/L, But Not in Patients with Na 130-134 mEq/L (NEJM, 2006) [MEDLINE]
Avoid Perioperative Hypotonic Intravenous Fluids and Excessive Intravenous Fluid Administration
Treat Pain
Potassium Replacement (When Required for Hypokalemia) (see Potassium Chloride)
Potassium is as Osmotically Active as Potassium and Replacing Potassium in the Setting of Hypokalemia Will Increase Serum Osmolality (Am J Kidney Dis, 2010) [MEDLINE]
Potassium Movement Intracellularly Increases the Serum Sodium by the Following Mechanisms
Intracellular Movement of Potassium Will Result in an Exchange of Sodium into the Extracellular Fluid (to Maintain Intracellular Electroneutrality)
Intracellular Movement of Potassium Will Result in an Exchange of Hydrogen Ions into the Extracellular Fluid
Hydrogen Ions are Buffered by Extracellular Bicarbonate (and Plasma Proteins), Creating Carbon Dioxide and Water (Bicarbonate is Replaced by Chloride Which was Administered with the Potassium)
Intracellular Movement of Potassium Drags Drags Chloride into the Cells, Increasing the Intracellular Osmolality, Which Results in Free Water Movement into Cells
Intracellular Movement of Potassium Increases the Intracellular Osmolality, Which Results in Free Water Movement into Cells
Hypertonic Saline Will Also Replace the Fluid Losses Resulting from Osmotic Diuresis by These Agents
Dose
Bolus 100 mL of 3% Saline (Provides 51 mEq of Sodium) at 10 min Intervals (as Required)
Each Bolus Should Increase the Serum Sodium 2-3 mEq/L.
Severe Hyponatremia with Near Normal/Normal Serum Osmolality (>270 mOsmol/kg)
Hemodialysis (see Hemodialysis): likely the safest treatment (Am J Kidney Dis, 1994) [MEDLINE]
Hemodialysis Corrects the Hyponatremia, Corrects the Osmotic Derangement, Normalizes Volume Status, and Removes the Glycine/Sorbitol/Mannitol Solution (and Their Metabolites)
If the Serum Sodium is Autocorrecting Due to a Water Diuresis, Monitor the Serum Sodium Until it Has Increased by 4-6 mEq/L from the Level at Presentation
Obviously, Autocorrection Can Be Detected by Remeasuring the Serum Sodium
Serum Sodium Should Be Monitored q1-2 hrs (a Point-of-Care Analyzer May Be Useful in This Situation)
Autocorrection Can Also Be Evidenced by the Following
Etiology of the Hyponatremia Has Been Reversed (Such as in Hypovolemia)
Urine Output Has Increased
Urine is Dilute (Specific Gravity <1.005, Urine Osmolality <200 mOsmol/kg, and the Sum of the Urine Sodium + Potassium Concentrations is <50% of the Serum Sodium
If the Serum Sodium is Not Autocorrecting, Administer 50 mL bolus of 3% Saline to Prevent a Further Decrease in the Serum Sodium
A Further Decline in the Serum Sodium Indicates a Lack of Autocorrection or Delayed Absorption of Ingested Water
3% Saline Can Be Safely Administered Via a Peripheral Intravenous Line and Does Not Require a Central Venous Catheter (Am J Crit Care, 2016) [MEDLINE] J Intensive Care Med, 2018) [MEDLINE]
Administer 100 mL bolus of 3% Saline Over 10 min with Two Additional Boluses (as Required by Symptoms to a Max of 300 mL) to a Goal Correction of 4-6 mEq/L Over the First Few Hours (and Goal Correction of <8 mEq/L in the First 24 hrs)
The Goal Rate of Correction Balances the Risk of Cerebral Edema Due to Acute Hyponatremia with the Risk of Osmotic Demyelination Syndrome Due to Overly Rapid Correction of Hyponatremia (see Osmotic Demyelination Syndrome)
Correction of Hyponatremia by 4-6 mEq/L within 6 hrs (Using Bolus Infusions of 3% Saline, as Required) is Sufficient to Manage the Most Severe Clinical Manifestations of Hyponatremia (Including Cerebral Edema with Potential Brain Herniation) (Semin Nephrol, 2009) [MEDLINE] (Curr Opin Nephrol Hypertens, 2010) [MEDLINE] (Am J Kidney Dis, 2015) [MEDLINE]
3% Saline is the Most Effective Means of Increasing the Serum Sodium and Improve Neurologic Outcomes in Severe, Symptomatic Hyponatremia (Am J Med, 2007) [MEDLINE]
Avoid Mannitol/Vasopressin Antagonists (Either Instead of or in Addition to 3% Saline) in the Treatment of Acute Hyponatremia
Mannitol is Potentially Nephrotoxic and Can Decrease the Serum Sodium
Vasopressin Antagonists Have Variable Efficacy and Their Onset of Action is Too Slow to be Used in the Treatment Acute Hyponatremia
Treatment of Chronic Hyponatremia within the First 6 hrs
Treatment of Chronic Hyponatremia with Serum Sodium 130-134 mEq/L
Employ General Measures (Above) Only
Treatment of Chronic Hyponatremia with Serum Sodium 120-129 mEq/L in Asymptomatic/Mild-Moderately Symptomatic Patient (Fatigue, Headache, Nausea/Vomiting, Gait Disturbance, Confusion) with No Known Intracranial Pathology
Employ General Measures Only
Treatment of Chronic Hyponatremia with Serum Sodium <120 mEq/L in Asymptomatic/Mild-Moderately Symptomatic Patient (Fatigue, Headache, Nausea/Vomiting, Gait Disturbance, Confusion) with No Known Intracranial Pathology
Administer Intravenous 3% Saline at 15-30 mL/hr with Goal Correction of <8 mEq/L in the First 24 hrs
The Following Subsets of Patients Have a Rapidly Reversible Etiology of Hyponatremia and May Develop a Water Diuresis During the Course of Therapy
Correction of Hypovolemia Inhibits Antidiuretic Hormone Secretion (Note that Antidiuretic Hormone has a Half-Life of Only 15-20 min), Resulting in a Water Diuresis
Administration of Glucocorticoid Steroids Directly Inhibits Antidiuretic Hormone Secretion (Note that Antidiuretic Hormone has a Half-Life of Only 15-20 min), Resulting in a Water Diuresis
Since Inappropriate Antidiuretic Hormone Secretion is Present, Removal of the Stimulus for its Secretion (Discontinuation of the Drug, Treatment of Pain, etc) May Rapidly Decrease Antidiuretic Hormone Secretion (Note that Antidiuretic Hormone has a Half-Life of Only 15-20 min), Resulting in a Water Diuresis
Desmopressin is Recommended (to Prevent Overly Rapid Sodium Correction) in Patients with Rapidly Reversible Etiology of Hyponatremia Who are Likely to Develop a Water Diuresis During the Course of Therapy and in Patients with High Risk for ODS (Alcohol Abuse Burns, Hypokalemia, Liver Disease, Malnutrition, Severe Hyponatremia with Serum Sodium ≤105 mEq/L)
Desmopressin is Administered at the Beginning of 3% Saline Infusion (or, if Isotonic Saline was Used, After the Serum Sodium Has Been Corrected by 4-6 mEq/L): 1-2 μg IV/SQ q6-8 hrs x 24-48 hrs (or until the serum sodium has been increased to at least 125 mEq/L) with restricted free water intake
During 3% Saline, Desmopressin Makes the Rate of Correction More Predictable Because it Prevents the Unexpected Water Diuresis During the Course of Therapy, Effectively Decreasing the Risk of ODS (Am J Kidney Dis, 2013) [MEDLINE] (Clin J Am Soc Nephrol, 2014) [MEDLINE]
While Administration of D5W Can Be Attempted (to Correct Free Water Losses During the Water Diuresis) Instead of Desmopressin, it is Typically Less Effective and More Difficult to Manage
Desmopressin in Not Indicated in Patients Who are Unlikely to Develop a Water Diuresis During the Course of Therapy (Edematous Patients with Congestive Heart Failure/Cirrhosis, Recurrent Hyponatremia Due to Chronic SIADH, etc)
Treatment of Chronic Hyponatremia with Serum Sodium <130 mEq/L in Severely Symptomatic Patient (Obtundation/Coma, Seizures, Respiratory Arrest) or Patient with Known Intracranial Pathology (Traumatic Brain Injury, Intracranial Hemorrhage, Intracranial Surgery, Intracranial Mass, etc)
Administer 100 mL Bolus of 3% Saline Over 10 min with Two Additional Boluses (as Required by Symptoms to a Max of 300 mL) to a Goal Correction of 4-6 mEq/L Over the First Few Hours (and Goal Correction of <8 mEq/L in the First 24 hrs)
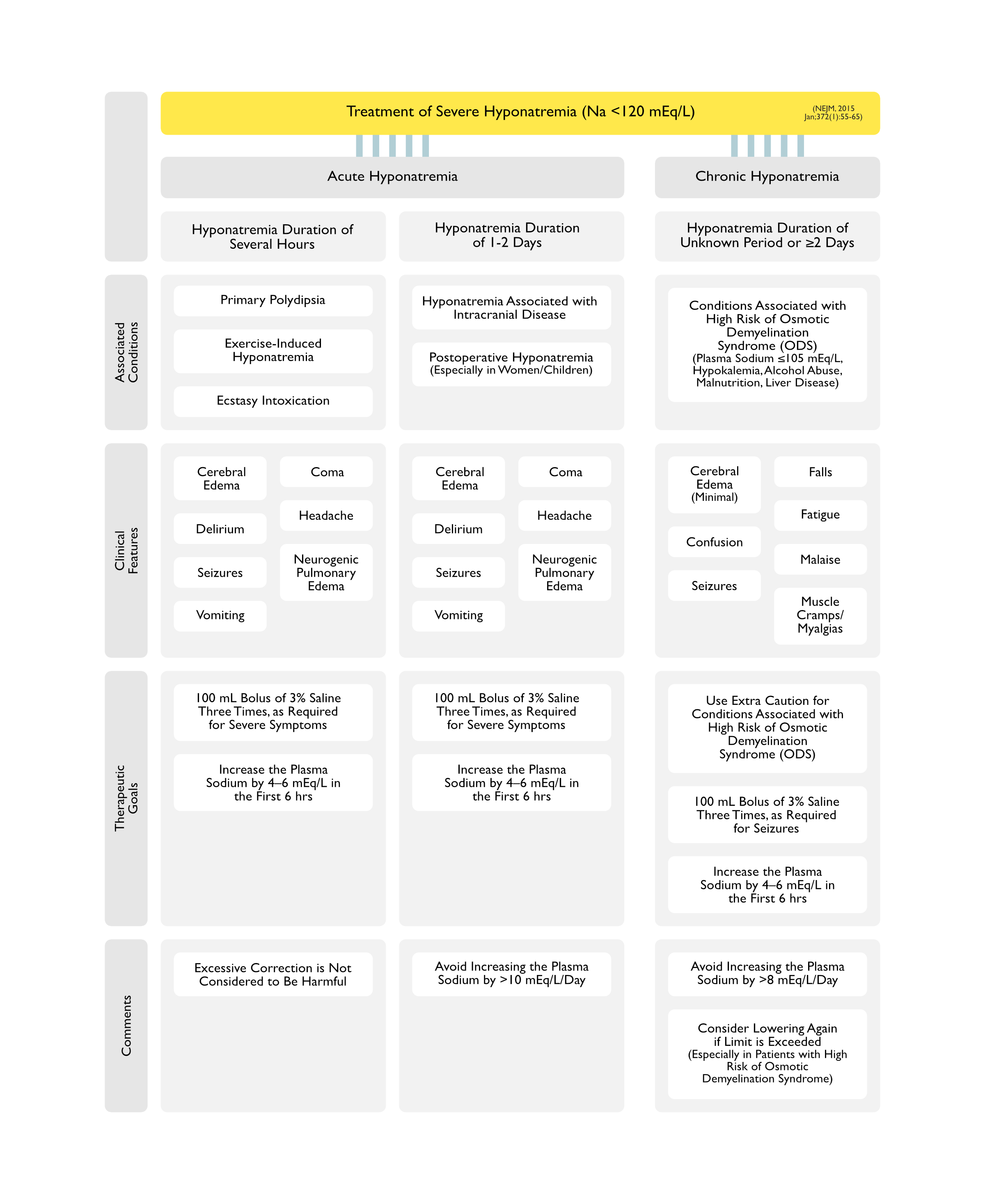
Overview of Treatment of Severe Hyponatremia (Na <120 mEq/L) (NEJM, 2015) [MEDLINE]
Seizures (see Seizures): 10% incidence with with plasma sodium <110 mEq/L)
Therapeutic Goal
Use Extra Caution for Conditions Associated with High Risk of Osmotic Demyelination Syndrome (ODS)
100 mL Bolus of 3% Saline Three Times, as Required for Seizures
Increase Plasma Sodium by 4–6 mEq/L in the First 24 hrs
Comments
Avoid Increasing Plasma Sodium by >8 mEq/L/Day
Consider Lowering Again if Limit is Exceeded (Especially in Patients with High Risk of Osmotic Demyelination Syndrome)
Etiology of “Autocorrection” of Hyponatremia During Therapy
General Comments
“Autocorrection” is Defined as a Rapid Water Diuresis Occurring During the Course of Hyponatremia Therapy (Generally Manifested by Urine Osmolality <100 mOsmol/kg)
If Autocorrection is Unrecognized, Rapid Correction of Hyponatremia May Occur, Exceeding the Recommended Limit of 8 mEq/L Per Day
Treatment of Hypovolemic Hyponatremia (with Fluid Resuscitation) (see Hypovolemic Shock) (Clin J Am Soc Nephrol, 2018) [MEDLINE]
Correction of the Hypovolemia Inhibits Antidiuretic Hormone Secretion (Note that Antidiuretic Hormone has a Half-Life of Only 15-20 min), Resulting in a Water Diuresis
Treatment of Adrenal Insufficiency with Glucocorticoid Steroid Replacement (see Adrenal Insufficiency) (J Clin Invest, 1967) [MEDLINE]
Administration of Glucocorticoid Steroids Directly Inhibits Antidiuretic Hormone Secretion, Resulting in a Water Diuresis
Note: Antidiuretic Hormone has a Half-Life of Only 15-20 min
Since Inappropriate Antidiuretic Hormone Secretion is Present, Removal of the Stimulus for its Secretion (Discontinuation of the Drug, Treatment of Pain, etc) May Rapidly Decrease Antidiuretic Hormone Secretion, Resulting in a Water Diuresis
Note: Antidiuretic Hormone has a Half-Life of Only 15-20 min
Discontinuation of Thiazide Diuretic (see Thiazides)
However, Osmotic Demyelination Syndrome is Uncommon in This Setting, Since the Increase in Serum Osmolality Associated with the Increase in Serum Sodium During Hemodialysis is Counterbalanced by a Decrease in Serum Osmolality Associated with the Removal of Urea
Strategies During the Treatment of Hyponatremia (J Med, 2015) [MEDLINE]
Proactive (Preventative) Strategy
Proactive (Preventative) Strategy May Be Useful in Patients Who are Likely to Develop Rapid Correction of Their Hyponatremia (i.e. Hypovolemic Patient Who Will Likely Develop a Water Diuresis During the Course of Treatment, etc)
Administer Desmopressin at the Beginning of Hyponatremia Treatment and at Regular Intervals (to Induce a State of Iatrogenic SIADH, Preventing Urinary Water Losses), Followed Then by the Use of Hypertonic (3%) Saline (Usually 15-30 mL/hr) to Slowly Increase the Serum Sodium in a Controlled Manner (see Desmopressin)
Typical Desmopressin Dosing: 1-2 μg IV q6-8hrs x 24-48 hrs (see Desmopressin)
Clinical Efficacy
In a Large Study (n = 254 Hyponatremic Patients Treated with Desmopressin), the Proactive Strategy (Although without Hypertonic Saline Use) was More Effective in Achieving Correction at <8 mEq/L (79% vs 30% in the Reactive Strategy Group), But was Less Used than the Reactive Strategy (Am J Med, 2018) [MEDLINE]
Reactive Strategy
Reactive Strategy May Be Useful in Patients with Concerning Trajectory with a Rapidly Increasing Serum Sodium
If Water Diuresis Occurs During Treatment or if the Trajectory is Predicted to Exceed Goal of 8 mEq/L Per Day, Replace Urinary Water Losses with D5W Infusion (Usually Less Effective) or Stop Urinary Water Losses with Desmopressin (Usually More Effective) (see Desmopressin)
Typical Desmopressin Dosing: 1-2 μg IV q6-8hrs x 24-48 hrs (see Desmopressin)
Rescue Strategy
Rescue Strategy May Be Used in Patients Who Have Already Exceeded the Sodium Correction Limit
Administer Desmopressin (2 μg q6 hrs IV) to Re-Lower the Serum Sodium (at Approximately 1 mEq/L Per Hour) (see Desmopressin)
Note that the Efficacy of Desmopressin to Inhibit the Water Diuresis (and Re-Lower the Serum Sodium) is Reduced in Hyponatremic Patients Who Have Been Treated with Vasopressin Receptor Antagonists (Tolvaptan, etc)
Although Human Data is Limited, Re-Lowering the Serum Sodium with D5W or Desmopressin May Abort the Development of Osmotic Demyelination Syndrome Following Inadvertent Rapid Correction of Hyponatremia
Complications of Overly Rapid Correction of Hyponatremia
Osmotic Demyelination Syndrome (ODS) is a Frequently Irreversible Neurologic Disorder Which Predominantly Occurs in Patients with Severe Hyponatremia (Na ≤120 mE/L) Which Has Been Present for >2-3 Days and in Whom the Serum Sodium Has Been Rapidly Corrected (Ann Intern Med, 1987) [MEDLINE] (J Am Soc Nephrol, 1994) [MEDLINE] (J Med, 2013) [MEDLINE] (Acta Neurol Scand, 2019) [MEDLINE]
Osmotic Demyelination Syndrome was Previously Called Central Pontine Myelinolysis
However, the Name was Subsequently Changed Since the Demyelination is More Diffuse and Does Not Necessarily Involve the Pons, Not All Patients Have Identifiable Anatomic Lesions, and Not All Patients Have Experienced a Preceding Rapid Correction of the Serum Sodium (Ann Intern Med, 1992) [MEDLINE]
Epidemiology
Low-Risk Groups for Osmotic Demyelination Syndrome (ODS)
Hyponatremic Patients with Self-Induced Water Intoxication (Runners, Psychotic Patients with Severe Polydipsia, Ecstasy Users, etc)
These Patients Have Not Had Adequate Time for Brain Cells to Expel Osmotic Substances
Patients with Mild-Moderate Hyponatremia (Serum Sodium >120 mEq/L)
Since Almost All Patients Who Develop Osmotic Demyelination Syndrome Initially Presented with a Serum Sodium ≤120 mEq/L
Risk Factors Which Increase the Risk of Osmotic Demyelination Syndrome (Clin J Am Soc Nephrol, 2018) [MEDLINE] (Acta Neurol Scand, 2019) [MEDLINE]
Protective Factors Which Decrease the Risk of Osmotic Demyelination Syndrome (ODS)
Elevated Blood Urea Nitrogen (BUN) in the Setting of Renal Failure
Relationship of Rate of Correction to the Risk of Osmotic Demyelination Syndrome (ODS)
Case Series Examining the Use of 3% Saline to Treat Hyponatremic Encephalopathy in the ED Setting (Am J Kidney Dis, 2015) [MEDLINE]: n = 64 (71 instances of hyponatremia)
Baseline Mean Serum Sodium was 114.1 ± 0.8 (SEM) mEq/L
Mean 3 hr Serum Sodium Correction to 117.9 ± 1.3
Mean 12 hr Serum Sodium Correction to 121.2 ± 1.2
Mean 24 hr Serum Sodium Correction to 123.9 ± 1.0 (Delta of Approximately 10 mEq/L in the First 24 hrs)
Mean 48 hr Serum Sodium Correction to 128.3 ± 0.8 mEq/L
No Cases of Osmotic Demyelination were Observed
Retrospective Cohort Study of Risk Factors for Rapid Correction of Hyponatremia (Clin J Am Soc Nephrol, 2018) [MEDLINE]: n = 1,490 patients admitted with serum sodium <120 mEq/L
Median Change in Serum Sodium at 24 hrs was 6.8 mEq/L (Interquartile Range, 3.4-10.2)
Rapid Correction of Hyponatremia Occurred in 41% of Patients
Risk Factors Associated with Rapid Correction
Younger Age
Female Sex
Schizophrenia
Lower Charlson Comorbidity Index
Lower Presentation Serum Sodium
Urine Sodium <30 mEq/L
Risk Factors Associated with Lower Risk of Rapid Correction
Prior Hyponatremia
Outpatient Aldosterone Antagonist Use
Treatment at an Academic Center
Approximately 88% of Patients with Incident Osmotic Demyelination Had a Documented Episode of Rapid Correction of Hyponatremia (with Serum Sodium Increase >8 mEq/L Over 24 hrs)
Retrospective Cohort Multicenter Study of the Rate of Hyponatremia Correction in Critical Care Patients with Serum Sodum <120 mEq/L (J Crit Care, 2023) [MEDLINE]: n = 1,024
Rapid Correction (>8 mEq/L Per Day) was Associated with Lower In-Hospital Mortality (Absolute Difference: -4.37%; 95% CI: -8.47 to -0.26%), Higher Number of Hospital-Free Days (1.80 Days; 95% CI: 0.82-2.79 Days), and Higher Number of Intensive Care Unit-Free Days (1.16 Days; 95% CI: 0.15-2.17 days)
There was No Significant Difference in Neurological Complications (2.31%; 95% CI: -0.77 to 5.40%)
Multicenter Observational Study of the Rate of Hyponatremia Correction in Patients with Serum Sodium <120 mEq/L (NEJM Evid, 2023) [MEDLINE]: n = 3,274
Correction Rate of <6 mEq/L Per 24 hrs was Observed in 38% of Cases, 6-10 mEq/L Per 24 hrs in 29% of Cases, and >10 mEq/L Per 24 hrs in 33% of Cases
As Compared to the 6-10 mEq/L Per 24 hrs Group, the <6 mEq/L Per 24 hrs Group was Associated with Higher In-Hospital Mortality Rate in Multivariable-Adjusted and Propensity Score-Weighted Analyses
As Compared to 6-10 mEq/L Per 24 hrs Group, the >10 mEq/L Per 24 hrs was Associated with Lower In-Hospital Mortality Rate and Shorter Length of Stay in Multivariable Analyses
Only 7 Patients Developed Osmotic Demyelination Syndrome (ODS)
5/7 Patients Developing ODS Despite a Correction Rate ≤8 mEq/L Per 24 hrs
6/7 Patients Had Alcohol Use Disorder, Malnutrition, Hypokalemia, or Hypophosphatemia
Canadian Multicenter Cohort Study of Rate of Hyponatremia Correction in Adult Patients (NEJM Evid, 2023) [MEDLINE]: n = 22,858 (from 5 academic hospitals between 2010-2020)
Mean Initial Serum Sodium was 125 mEq/L (SD: 4.6)
Serum Sodium 110-119 mmol/L: 11.9% of patients
Serum Sodium <110 mmol/L: 1.2% of patients
Overall, Rapid Correction of Serum Sodium Occurred in 17.7% of Patients
Only 12 Patients (0.05%) Developed Osmotic Demyelination Syndrome (ODS)
58% of Patients Who Developed ODS Did Not Have Rapid Correction of Sodium
In a Study of Osmotic Demyelination Syndrome, 51% of Patients Had Central Pontine Demyelination Only, 45% of Patients Had Both Central Pontine Demyelination and Extrapontine Demyelination, and 4% of Patients Had Extrapontine Demyelination Only (Acta Neurol Scand, 2019) [MEDLINE]
Clinical
Delayed Onset of Symptoms Occurs Approximately 2-6 Days After the Rapid Sodium Correction Event
Treatment
Supportive Care
Respiratory Support (Endotracheal Intubation with Invasive Mechanical Ventilation (If Required)
Recommended that the Serum Sodium Be Lowered to a Level Just Below the Initial 48 hr Serum Sodium Target (i.e. to <16 mEq/L Above the Initial Target Serum Sodium)
The 48 hr Target is the Most Practical to Implement Since Osmotic Demyelination Syndrome General Presents 2-6 Days After the Rapid Sodium Correction Event
Procedure
Start Either Hypotonic Intravenous Fluids (D5W, etc) or Desmopressin within Hours of the Onset of Neurologic Symptoms
While the Optimal Timing of Re-Lowering is Unclear, it is Recommended to Start Re-Lowering as Soon as Possible
Prognosis
Hyponatremia (Even if Mild) Increases the Mortality Rate in Both Ambulatory and Hospitalized Patients (Am J Med, 2009) [MEDLINE] (Arch Intern Med, 2010) [MEDLINE] (Am J Kidney Dis, 2012) [MEDLINE] (Kidney Int, 2013) [MEDLINE] (Eur J Endocrinol, 2015) [MEDLINE]
This May Be Due to Adaptations to Hyponatremia Which Allow the Organs to Function at Decreased Serum Concentrations (Am J Kidney Dis, 2019) [MEDLINE]
Interestingly, the Relationship Between Serum Sodium Level and Mortality Rate is Not Linear (with Higher Mortality Rates at Serum Sodium Levels Down to 125 mEq/L and Lower Mortality Rates at Serum Sodium Levels <120 mEq/L) (Clin J Am Soc Nephrol, 2011) [MEDLINE] (Eur J Endocrinol, 2016) [MEDLINE] (BMC Nephrol, 2016) [MEDLINE]
This May Be Due to the Fact that Mild-Moderate Hyponatremia is More Likely to Be Associated with a Significant Underlying Disease (Malignancy, Renal Failure, Congestive Heart Failure, Cirrhosis), While Severe Hyponatremia is Most Commonly Drug-Induced
Drug-Induced Hyponatremia is More Likely to Resolve After Discontinuation of the Drug (While Disease-Associated Hyponatremia is More Likely to Be Persistent/Chronic)
Data from Meta-Analyses (15 Studies, Including 13,816 Hyponatremic Patients) Indicate that Improvement in the Serum Sodium Concentration Results in Decreased Overall Mortality Rate (PLoS One, 2015) [MEDLINE]
Across All 15 Studies, Any Improvement of Hyponatremia was Associated with a Decreased Risk of Overall Mortality (Odds Ratio: 0.57; 0.40-0.81)
Association was Even Stronger When Only Those 8 Studies Reporting a Threshold for Serum Sodium Improvement to >130 mmol/L were Considered (Odds Ratio: 0.51; 0.31-0.86)
The Decreased Mortality Rate Persisted at Follow-Up at 12 Months (Odds Ratio: 0.55; 0.36-0.84)
Meta-Regression Analyses Demonstrated that the Decreased Mortality Rate Associated with Hyponatremia Improvement was More Evident in Older Subjects and in Those with Lower Sodium at Enrollment
Hyponatremia Increases Postoperative 30-Day Mortality Rate (5.2% vs 1.3%)
Especially in Patients Undergoing Non-Emergency Surgery with ASA Class 1-2
Hyponatremia Increases Rate of Perioperative Coronary Events
Hyponatremia Increases Wound Infection Rates
Hyponatremia Increases Pneumonia RatesHyponatremia Prolongs the Median Length of Stay (by Approximately 1 Day)
References
General
Common fluid-electrolyte and acid-base problems in the intensive care unit: selected issues. Semin Nephrol 1994; 14:8-22 [MEDLINE]
Hyponatremia. N Engl J Med. 2000 May 25;342(21):1581-9 [MEDLINE]
Hyponatraemia in clinical practice. Postgrad Med J. Jun 2007; 83(980): 373–378. doi: 10.1136/pgmj.2006.056515 [MEDLINE]
Clinical
Hyponatremia, convulsions, respiratory arrest, and permanent brain damage after elective surgery in healthy women. N Engl J Med. 1986;314(24):1529 [MEDLINE]
Severe symptomatic hyponatremia: treatment and outcome. A study of 64 cases. Ann Intern Med. 1987;107(5):656 [MEDLINE]
Sex differences result in increased morbidity from hyponatremia in female rats. Am J Physiol. 1989;256(4 Pt 2):R880 [MEDLINE]
Hyponatremia and death or permanent brain damage in healthy children. BMJ. 1992;304(6836):1218 [MEDLINE]
Postoperative hyponatremic encephalopathy in menstruant women. Ann Intern Med. 1992;117(11):891 [MEDLINE]
Hyponatremia, cerebral edema, and noncardiogenic pulmonary edema in marathon runners. Ann Intern Med. 2000;132(9):711 [MEDLINE]
Clinical studies of thiazide-induced hyponatremia. J Natl Med Assoc. 2004;96(10):1305 [MEDLINE]
Mild chronic hyponatremia is associated with falls, unsteadiness, and attention deficits. Am J Med. 2006;119(1):71.e1 [MEDLINE]
Mild hyponatremia and risk of fracture in the ambulatory elderly. QJM. 2008;101(7):583 [MEDLINE]
Hyponatremia-induced osteoporosis. J Bone Miner Res. 2010;25(3):554 [MEDLINE]
Hyponatremia and risk of seizures: a retrospective cross-sectional study. Epilepsia. 2011 Feb;52(2):410-3 [MEDLINE]
Mortality and serum sodium: do patients die from or with hyponatremia? Clin J Am Soc Nephrol. 2011 May;6(5):960-5 [MEDLINE]
Characteristics, symptoms, and outcome of severe dysnatremias present on hospital admission. Am J Med. 2012;125(11):1125.e1 [MEDLINE]
Symptoms and characteristics of individuals with profound hyponatremia: a prospective multicenter observational study. J Am Geriatr Soc. 2015;63(3):470 [MEDLINE]
Attention and postural balance are much more affected in older than in younger adults with mild or moderate chronic hyponatremia. Eur J Intern Med. 2017;41:e25 [MEDLINE]
Allostasis and the Clinical Manifestations of Mild to Moderate Chronic Hyponatremia: No Good Adaptation Goes Unpunished. Am J Kidney Dis. 2019;73(3):391 [MEDLINE]
Treatment
Changing concepts in treatment of severe symptomatic hyponatremia. Rapid correction and possible relation to central pontine myelinolysis. Am J Med. 1985;78(6 Pt 1):897 [MEDLINE]
New approach to disturbances in the plasma sodium concentration. Am J Med 1986; 81:1033 [MEDLINE]
Severe symptomatic hyponatremia: treatment and outcome. A study of 64 cases. Ann Intern Med. 1987;107(5):656 [MEDLINE]
The management of hyponatremic emergencies. Crit Care Clin 1991; 7:127-42 [MEDLINE]
Endometrial ablation complicated by fatal hyponatremic encephalopathy. JAMA. 1993;270(10):1230 [MEDLINE]
Pontine and extrapontine myelinolysis: a neurologic disorder following rapid correction of hyponatremia. Medicine (Baltimore). 1993;72(6):359 [MEDLINE]
The post-transurethral resection of prostate syndrome: therapeutic proposals. Am J Kidney Dis. 1994;24(1):108 [MEDLINE]
Therapeutic recommendations for management of severe hyponatremia: current concepts on pathogenesis and prevention of neurologic complications. Clin Nephrol. 1996 Sep;46(3):149-69 [MEDLINE]
The treatment of severe hyponatremia. Kidney Int Suppl. 1998;64:S6 [MEDLINE]
The pathophysiology and treatment of hyponatraemic encephalopathy: an update. Nephrol Dial Transplant. 2003;18(12):2486 [MEDLINE]
Tolvaptan, a selective vasopressin V2-receptor antagonist, for hyponatremia. N Engl J Med 2006;355:2099-2112 [MEDLINE]
Assessment of the efficacy and safety of intravenous conivaptan in euvolemic and hypervolemic hyponatremia. Am J Nephrol 2007;27:447-457 [MEDLINE]
Effects of oral tolvaptan in patients hospitalized for worsening heart failure: The EVEREST Outcome Trial. JAMA 2007;297:1319-1331 [MEDLINE]
The treatment of hyponatremia. Semin Nephrol. 2009;29(3):282 [MEDLINE]
Treatment of hyponatremia. Curr Opin Nephrol Hypertens. 2010;19(5):493 [MEDLINE]
Central pontine and extrapontine myelinolysis: from epileptic and other manifestations to cognitive prognosis. J Neurol. 2010 Jul;257(7):1176-80 [MEDLINE]
The challenge of hyponatremia. J Am Soc Nephrol. 2012;23(7):1140 [MEDLINE]
Osmotic demyelination syndrome associated with hypophosphataemia: 2 cases and a review of literature. Acta Paediatr. 2013 Apr;102(4):e164-8. Epub 2013 Jan 21 [MEDLINE]
Hypertonic saline and desmopressin: a simple strategy for safe correction of severe hyponatremia. Am J Kidney Dis. 2013 Apr;61(4):571-8 [MEDLINE]
Use of desmopressin acetate in severe hyponatremia in the intensive care unit. Clin J Am Soc Nephrol. 2014 Feb;9(2):229-37 [MEDLINE]
Hyponatremia improvement is associated with a reduced risk of mortality: evidence from a meta-analysis. PLoS One. 2015;10(4):e0124105. Epub 2015 [MEDLINE]
Diagnosis and management of sodium disorders: hyponatremia and hypernatremia. Am Fam Physician . 2015 Mar 1;91(5):299-307 [MEDLINE]
Treatment of hyponatremic encephalopathy with a 3% sodium chloride protocol: a case series. Am J Kidney Dis. 2015 Mar;65(3):435-42 [MEDLINE]
Disorders of plasma sodium–causes, consequences, and correction. N Engl J Med. 2015 Jan;372(1):55-65 [MEDLINE]
Safety of Continuous Peripheral Infusion of 3% Sodium Chloride Solution in Neurocritical Care Patients. Am J Crit Care. 2016;26(1):37 [MEDLINE]
Treatment of Severe Hyponatremia. Clin J Am Soc Nephrol. 2018;13(4):641 [MEDLINE]
Risk Factors and Outcomes of Rapid Correction of Severe Hyponatremia. Clin J Am Soc Nephrol. 2018 Jul 6;13(7):984-992. doi: 10.2215/CJN.13061117 [MEDLINE]
Incidence of Adverse Events During Peripheral Administration of Sodium Chloride 3. J Intensive Care Med. 2018;33(1):48 [MEDLINE]
Effects of correction rate for severe hyponatremia in the intensive care unit on patient outcomes. J Crit Care. 2023 Oct:77:154325. doi: 10.1016/j.jcrc.2023.154325 [MEDLINE]
Severe Hyponatremia Correction, Mortality, and Central Pontine Myelinolysis. NEJM Evid. 2023 Oct;2(10):EVIDoa2300107. doi: 10.1056/EVIDoa2300107 [MEDLINE]
Osmotic demyelination syndrome in patients hospitalized with hyponatremia. NEJM Evid 2023; 2(4):EVIDoa2200215. doi:10.1056/Evidoa2200215 [MEDLINE]
Prognosis
Mortality after hospitalization with mild, moderate, and severe hyponatremia. Am J Med. 2009;122(9):857 [MEDLINE]
Impact of hospital-associated hyponatremia on selected outcomes. Arch Intern Med. 2010;170(3):294 [MEDLINE]
Mortality and serum sodium: do patients die from or with hyponatremia? Clin J Am Soc Nephrol. 2011 May;6(5):960-5 [MEDLINE]
Hyponatremia in hospitalized cancer patients and its impact on clinical outcomes. Am J Kidney Dis. 2012;59(2):222 [MEDLINE]
Mild hyponatremia is associated with an increased risk of death in an ambulatory setting. Kidney Int. 2013 Apr;83(4):700-6 [MEDLINE]
Hyponatremia improvement is associated with a reduced risk of mortality: evidence from a meta-analysis. PLoS One. 2015;10(4):e0124105. Epub 2015 [MEDLINE]
Hyponatremia and mortality risk: a Danish cohort study of 279 ,508 acutely hospitalized patients. Eur J Endocrinol. 2015 Jul;173(1):71-81 [MEDLINE]
Long-term outcome of profound hyponatremia: a prospective 12 months follow-up study. Eur J Endocrinol. 2016;175(6):499 [MEDLINE]
Prognosis of patients with severe hyponatraemia is related not only to hyponatraemia but also to comorbidities and to medical management: results of an observational retrospective study. BMC Nephrol. 2016;17(1):159 [MEDLINE]