Hyponatremia is One of the Most Common Electrolyte Disturbances Encountered in Clinical Practice (Am J Med, 2006) [MEDLINE]
Inpatient
Study of Incidence of Hyponatremia (Clin Chim Acta, 2003) [MEDLINE]: n >300,000 sodium samples measured in >120,000 patients (from acute care hospital, ambulatory hospital, and community-based clinics in Singapore)
Incidence of Hyponatremia (Serum Sodium <136 mEq/L) in Acute Care Hospital Setting: 42.6%
Incidence of Hyponatremia (Serum Sodium <126 mEq/L) in Acute Care Hospital Setting: 6.2%
Incidence of Hyponatremia (Serum Sodium <116 mEq/L) in Acute Care Hospital Setting: 1.2%
Outpatient
Study of Incidence of Hyponatremia (Clin Chim Acta, 2003) [MEDLINE]: n >300,000 sodium samples measured in >120,000 patients (from acute care hospital, ambulatory hospital, and community-based clinics in Singapore)
Incidence of Hyponatremia (Serum Sodium <136 mEq/L) in Ambulatory Hospital Care Setting: 21%
Incidence of Hyponatremia (Serum Sodium <136 mEq/L) in Community Care Ambulatory Setting: 7.2%
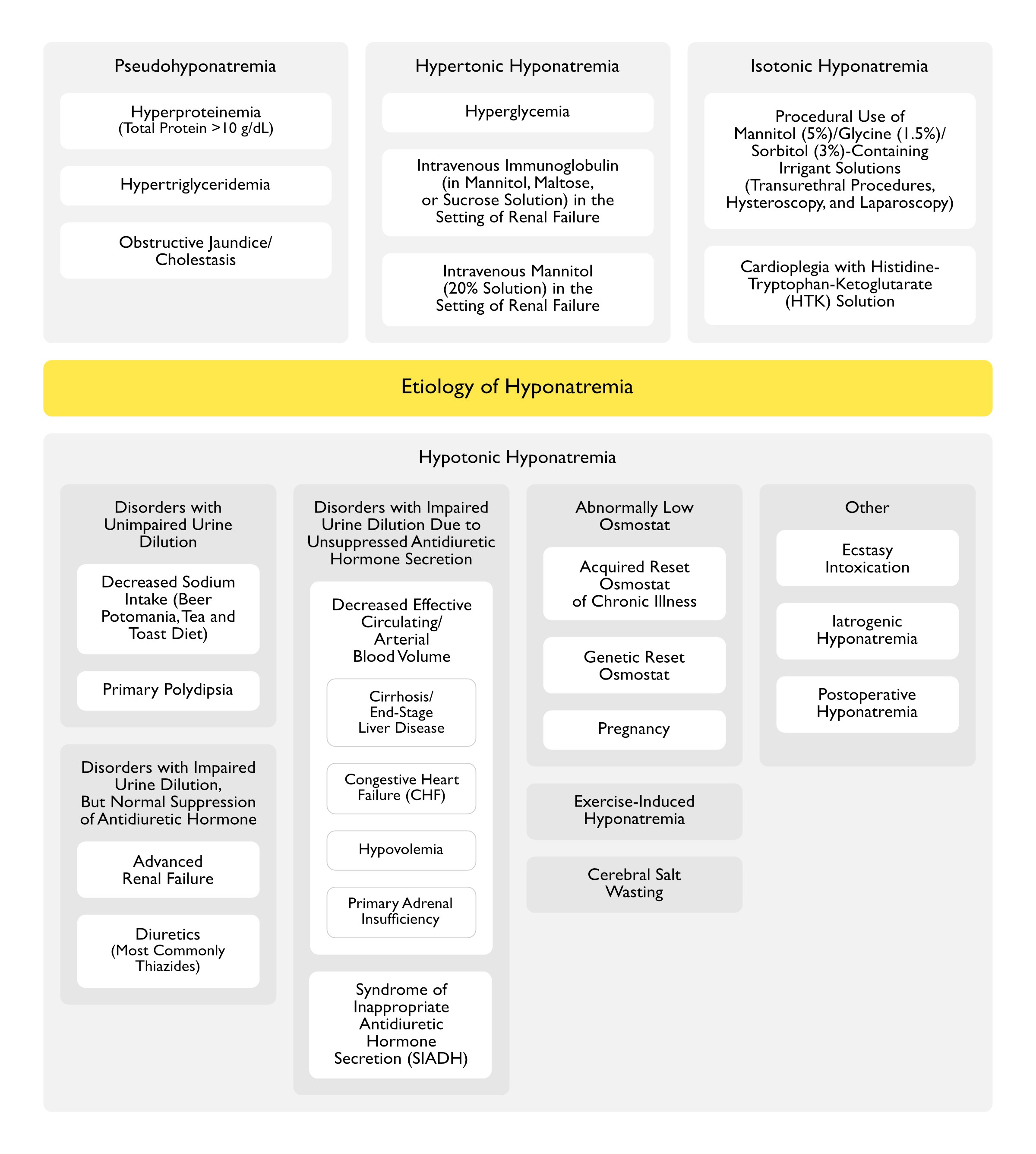
Etiology
Pseudohyponatremia
General Comments
Pseudohyponatremia Due to Either Hyperproteinemia or Hypertriglyceridemia are Considered Isotonic Hyponatremia (Since the Sodium Concentration in Plasma Water and Interstitial Fluid are Normal)
Patients with Pseudohyponatremia are Asymptomatic
Hyperproteinemia (Severe, Total Protein Usually >10 g/dL) (see Hyperproteinemia)
Epidemiology
Severe Hyperproteinemia May Occur in Multiple Myeloma (see Multiple Myeloma)
Mechanism
Pseudohyponatremia Occurs Due to a Laboratory Artifact When Using Flame Photometry or Indirect Potentiometry (Which Measure Sodium Concentration Per Volume of Plasma)
Note that the Laboratory Artifact Does Not Occur When Using Direct Potentiometry (Which Directly Measure the Sodium Concentration in the Water Phase of Plasma)
Note that the Sodium Concentration Will Be Assayed as Normal by Direct Sodium-Selective Electrodes Used by Blood Gas Analyzers and Some Point-of-Care Devices
Hyperproteinemia Increases the Mass of the Nonaqueous Protein Component of Serum and a Concomitant Decrease in the Proportion of the Water Component
Sodium Concentration is Usually Reported by the Laboratory as mEq/L of Plasma or Serum
Normal Plasma or Serum is 93% Water and 7% Fats/Proteins
However, in the Setting of Significant Hypertriglyceridemia/Hyperproteinemia, the Plasma or Serum Water Fraction May Fall to <80%
Sodium is Restricted to the Serum Water Component (Although the Sodium Concentration in the Water Phase is Not Affected, the Sodium Concentration Per Unit of Plasma is Decreased)
The Sodium Concentration in Plasma Water is What is Physiologically Important
Numerical Impact of Hyperproteinemia on the Serum Sodium Concentration
A 1 g/dL Increase in Plasma Protein Will Decrease the Serum Sodium by Approximately 0.7 mEq/L (Nephrol Dial Transplant, 2015) [MEDLINE]
Diagnosis
Hyponatremia (When Assessed by Autoanalyzer Which Uses Flame Photometry or Indirect Potentiometry)
Normonatremia (When Assessed by Sodium-Selective Electrode)
Severe Hypertriglyceridemia May Occur in Uncontrolled Diabetes Mellitus (see Diabetes Mellitus)
Severe Hypertriglyceridemia May Occur Due to Other Etiologies
In Patients with Acute Pancreatitis, the Presence of Pseudohyponatremia at Presentation Increases the Probability that the Pancreatitis is Due to the Hypertriglyceridemia (Pancreas, 2019) [MEDLINE]
Mechanism
Pseudohyponatremia Occurs Due to a Laboratory Artifact When Using Flame Photometry or Indirect Potentiometry (Which Measure Sodium Concentration Per Volume of Plasma)
Note that the Laboratory Artifact Does Not Occur When Using Direct Potentiometry (Which Directly Measure the Sodium Concentration in the Water Phase of Plasma)
Note that the Sodium Concentration Will Be Assayed as Normal by Direct Sodium-Selective Electrodes Used by Blood Gas Analyzers and Some Point-of-Care Devices
Hypertriglyceridemia Increases the Mass of the Nonaqueous Lipid Component of Serum and a Concomitant Decrease in the Proportion of the Water Component
Sodium Concentration is Usually Reported by the Laboratory as mEq/L of Plasma or Serum
Normal Plasma or Serum is 93% Water and 7% Fats/Proteins
However, in the Setting of Significant Hypertriglyceridemia/Hyperproteinemia, the Plasma or Serum Water Fraction May Fall to <80%
Sodium is Restricted to the Serum Water Component (Although the Sodium Concentration in the Water Phase is Not Affected, the Sodium Concentration Per Unit of Plasma is Decreased)
The Sodium Concentration in Plasma Water is What is Physiologically Important
Numerical Impact of Hypertriglyceridemia on the Serum Sodium Concentration
A 886 mg/dL (10 mmol/L) Increase in Plasma Triglycerides Will Decrease the Serum Sodium Concentration by Approximately 1 mEq/L (Clin Chem, 2006) [MEDLINE]
Diagnosis
Hyponatremia (as Assessed by Autoanalyzer Which Uses Flame Photometry or Indirect Potentiometry)
Normonatremia (as Assessed by Sodium-Selective Electrode)
Severe Elevation of Total Serum Cholesterol and Elevated Lipoprotein X
The Lowest Reported Total Serum Cholesterol Resulting in Pseudohyponatremia was 977 mg/dL (with Corresponding Serum Sodium of 129 mmol/L) (J Clin Lipidol, 2015) [MEDLINE]
The Highest Reported Total Serum Cholesterol was 4091 mg/dL (with Corresponding Serum Sodium of 101 mmol/L) (J Clin Lipidol, 2015) [MEDLINE]
Lipoprotein X is an Insoluble Compound Which Forms When There is a Reflux of Unesterified Cholesterol and Phospholipids into the Circulation
Lipoprotein X Does Not Accumulate in Other Hyperlipidemic States with Severely Elevated Total Serum Cholesterol (Such as Homozygous Familial Hypercholesterolemia)
In Contrast to Hypertriglyceridemia, Elevated Lipoprotein X Does Not Cause the Serum to Appear Lipemic
Glucose is an Osmotically Active Solute (and an “Effective Osmole”), Which Increases Serum Tonicity and Causes Water to Be Pulled Out of Cells, Expanding the Extracellular Water Space and Resulting in Dilution of the Serum Sodium and Hypertonic Hyponatremia
The Development of Hyponatremia is at Least Partially Countered by Free Water Loss Resulting from the Associated Glycosuria-Induced Osmotic Diuresis
Hypertonic Hyponatremia Due to Hyperglycemia Does Not Increase the Risk of Cerebral Edema, Because Water Moves Out of Cells
However, the Rapid Correction of Hyperglycemia without a Commensurate Increase in Serum Sodium May Result in a Precipitous Decrease in Effective Osmolality and Cause Cerebral Edema (Particularly in Children and Young Adults with Diabetic Ketoacidosis) (J Pediatr, 2007) [MEDLINE]
Therefore, One Should Monitor Effective Serum Osmolality During the Treatment of Severe Hyperglycemia/Diabetic Ketoacidosis, Targeting a Gradual Decrease in Effective Serum Osmolality
Correction of Serum Sodium Concentration for Hyperglycemia
Correct the Serum Sodium Concentration Upward by Approximately 2 mEq/L for Each 100 mg/dL (5.5 mmol/L) Increase in the Serum Glucose
Studies of Experimentally-Induced Hyperglycemia Suggest that the Previously Utilized 1.6/100 Ratio Applies Only When the Serum Glucose is <400 mg/dL (with Serum Glucose >400 mg/dL, a 4/100 Ratio was Instead Observed) (Am J Med, 1999) [MEDLINE]
Intravenous Immunoglobulin Parenteral Solutions are Suspended in Hypertonic Mannitol, Maltose, or Sucrose
Mannitol/Maltose/Sucrose are “Effective Osmoles” (Solutes Which Do Not Move Freely Across Cell Membranes and Obligate Water to Move with Them)
Mannitol/Maltose/Sucrose are Osmotically-Active Solutes, Which Cause Water to Be Pulled Out of Cells, Resulting in Dilution of the Serum Sodium (and Hypertonic Hyponatremia) (Ann Intern Med, 1993) [MEDLINE] (South Med J, 2000) [MEDLINE] (Nephron Clin Pract, 2007) [MEDLINE]
Use of Intravenous Immunoglobulin in the Presence of Renal Failure
If Renal Failure is Present (Preventing Renal Excretion of These Substances), Mannitol/Maltose/Sucrose are Undesirably Retained in the Blood, Increasing Serum Tonicity and Resulting in Water Movement Out of Cells into the Serum (Resulting in Hyponatremia)
Hyponatremia May Be Severe and Prolonged (Especially in Cases with Concomitant Intravenous Immunoglobulin-Associated Renal Failure, Which Impairs Water Excretion)
Some Investigators Have Suggested that the Intravenous Immunoglobulin-Associated Decrease in Serum Sodium is Actually Pseudohyponatremia Caused by Hyperproteinemia and Hyperviscosity (Am J Hematol, 2003) [MEDLINE]
However, Pseudohyponatremia Has Not Been Supported by Studies Measuring the Serum Sodium Using a Sodium-Selective Electrode (Ann Intern Med, 1993) [MEDLINE] (South Med J, 2000) [MEDLINE] (Nephron Clin Pract, 2007) [MEDLINE]
Additionally, the Observed Increase in Serum Protein After Intravenous Immunoglobulin is Insufficient to Result in a Significant Decrease in the Serum Sodium
Diagnosis
Elevated Serum Osmolal Gap >10 mOsmol/kg Indicates that the Mannitol/Maltose/Sucrose Has Been Retained (see Elevated Serum Osmolal Gap)
Intravenous Mannitol Use in the Setting of Renal Failure (see Mannitol)
Clinical Uses of Intravenous Mannitol
Intravenous Mannitol Used to Treat Increased Intracranial Pressure
Administration
20% Mannitol Solution (20 g Mannitol/100 mL) is Hyperosmotic (with 1098 mOsmol/L
Typical Intravenous Dose: 50 g (of 20% solution) infused over 30-60 min
Mechanism
Mannitol is an Osmotically-Active Solute (it is an “Effective Osmole”, Similar to Hyperglycemia), Which Causes Water to Be Pulled Out of Cells, Resulting in Dilution of the Serum Sodium (and Hypertonic Hyponatremia)
As Mannitol is Subsequently Excreted in the Urine (Similar to Hyperglycemia), it Acts as an Osmotic Diuretic Promoting Urinary Water Loss and Consequently Increases the Serum Sodium
Use of Mannitol in the Presence of Renal Failure
If Renal Failure is Present, Mannitol Can Be Undesirably Retained in the Extracellular Space, Causing Hypertonicity, Which Pulls Water Out of Cells, Resulting in Hyponatremia
Therefore, If Hyponatremia Occurs After Mannitol Treatment, Serum Osmolality Should Be Monitored
Diagnosis
Elevated Serum Osmolal Gap >10 mOsmol/kg Indicates that the Mannitol Has Been Retained (see Elevated Serum Osmolal Gap) (Crit Care Med, 2004) [MEDLINE]
Isotonic Hyponatremia
Procedural Use of Glycine/Sorbitol/Mannitol-Containing Irrigation Solutions (see Glycine and Sorbitol, and Mannitol)
Etiology
Intravesical Glycine/Sorbitol/Mannitol Irrigant Used During Transurethral Resection of the Prostate (TURP) or Transurethral Resection of the Bladder Tumors (“Transurethral Resection Syndrome”) (see Transurethral Resection of the Prostate)
Transurethral Resection Syndrome Occurs in 2% of TURP Cases (J Urol, 2002) [MEDLINE] (J Endourol, 2008) [MEDLINE]
Glycine/Sorbitol/Mannitol Irrigation During Hysteroscopy (for Submucosal Leiomyoma Resection, etc) (see Hysteroscopy)
Glycine/Sorbitol/Mannitol Irrigation During Percutaneous Nephrolithotomy (Removal of Kidney Stones)
Glycine/Sorbitol/Mannitol Irrigation During Laparoscopy (see Laparoscopy)
Mechanism
Previously Used Electrosurgery Devices were Monopolar and Could Not Be Used with Conductive (Electrolyte-Containing) Irrigation Solutions
Bipolar Devices are Now More Commonly Used (These are Compatible with Conductive (Electrolyte-Containing) Irrigation Solutions Such as Normal Saline, Lactated Ringers)
However, with These Newer-Generation Devices, the Large Volumes of Saline Irrigant Used May Exhibit Other Adverse Effects (Expansion of the Extracellular Fluid Volume with Fluid Overload/Pulmonary Edema, Hyperchloremia, etc) (Acta Anaesthesiol Scand, 2017) [MEDLINE]
The Following are the Most Commonly Used Non-Conductive (Non-Electrolyte) Solutions Used During These Procedures
1.5% Glycine (see Glycine): hypoosmotic (200 mOsmol/kg)
3% Sorbitol (see Sorbitol): hypoosmotic (165 mOsmol/kg
5% Mannitol (see Mannitol): isoosmotic (275 mOsmol/kg)
Inadvertent Systemic Absorption of Sodium-Free Glycine/Sorbitol/Mannitol-Containing Solution from the Urinary Bladder/Uterus/Peritoneal Space During the Procedure with Distribution to the Extracellular Space
Fluid Absorption into the Vascular Space (Intravasation, Presumably Through Opened Vessels) Occurs When the Fluid Pressure Exceeds the Venous Pressure (at Approximately 10 mm Hg) (Br J Anaesth, 2006) [MEDLINE]
Fluid Can Also Be Absorbed Via Inadvertent Surgical Perforation of a Viscus (in Which Case the Serum Sodium May Instead Nadir 1-2 hrs Postoperatively and the Degree of Decrease in the Serum Sodium is Generally Less than that Observed with Intravasation) (Scand J Urol Nephrol, 1993) [MEDLINE]
Mannitol/Glycine/Sorbitol are “Effective Osmoles” (Solutes Which Do Not Move Freely Across Cell Membranes and Obligate Water to Move with Them)
If a Large Volume of Glycine Solution is Absorbed, the Serum Osmolality will Decrease Slightly, But the Serum Sodium Will Decrease Significantly
Glycine Enters Cells Over Several Hours (Pulling Water into the Cells with it) and, by 4 hrs Later, Glycine is Almost Equally Distributed Between the Intracellular and Extracellular Compartments (with a Gradual Increase in the Serum Sodium Back Toward Baseline)
Glycine is Also Metabolized into Ammonia, Serine, and/or Glyoxylate with the Development of Neurologic Symptoms
Sorbitol Solutions Which are Not Renally Excreted Will Be Slowly Hepatically Metabolized to Glucose and Fructose, Then to Carbon Dioxide and Water (with Only 5-10% Being Excreted Unchanged in the Urine), Resulting in a Delayed Onset of Hyponatremia
Since Glycine and Sorbitol Solutions are Hypoosmotic, the Initial Serum Osmolality Will Be Decreased
However, Since Mannitol 5% Solution is Isoosmotic, the Initial Serum Osmolality Will Be Relatively Unchanged
Elevated Serum Osmolal Gap >10 mOsmol/kg (Indicating that the Glycine/Sorbitol/Mannitol Has Been Retained) (see Elevated Serum Osmolal Gap)
The Osmolal Gap Can Exceed 30-60 mOsmol/kg Immediately Postoperatively
The Serum Osmolal Gap Will Gradually Disappear Over Time (Due to Glycine Entering Cells, the Metabolism of Glycine/Sorbitol, and the Urinary Excretion of Glycine/Sorbitol/Mannitol)
While One Might Expect the Urine Osmolality to Be Maximally Dilute (<100 mOsmol/kg) to Facilitate Water Excretion in this Clinical Scenario, Factors Such as Postoperative Stress-Related Antidiuretic Hormone Release Can Counter This (by Impairing Water Excretion and Slowing the Correction of the Hyponatremia), Mannitol Causes an Osmotic Diuresis, and Glycine Can Directly Stimulate Antidiuretic Hormone Release (Am J Kidney Dis, 1997) [MEDLINE]
Clinical
In the Case of Glycine Use, Neurologic Symptoms (Due to Hyponatremia, Glycine Toxicity, and Accumulation of Ammonia/Serine/Glyoxylate, Which are Glycine Metabolites) May Occur (see Glycine)
Cardioplegia with Histidine-Tryptophan-Ketoglutarate (HTK) Solution
Etiology
Histidine-Tryptophan-Ketoglutarate (HTK) Solution is Widely Used to Induce Electromechanical Cardiac Arrest During Cardiac Surgery
Mechanism
Histidine-Tryptophan-Ketoglutarate (HTK) Solution is Slightly Hypertonic (with 310 mOsmol/L) and a Low Sodium
In One Study, HTK (Median Amount of 2L), Resulted in a Decreased Serum Sodium of 15 mmol/L within 30-60 min (with the Hyponatremia Resolving Spontaneously by the End of Surgery) (J Cardiothorac Surg, 2012) [MEDLINE]
Malnourished Patient with Ingestion of Large Quantities of Beer (Lancet, 1975) [MEDLINE] (Am J Kidney Dis, 1998) [MEDLINE] (Lancet, 2002) [MEDLINE]
Mechanism
Beer Contains Little or No Sodium/Potassium/Protein to Generate Solutes for Excretion
In Addition, the Alcohol and Carbohydrates in Beer Suppresses Endogenous Protein Degradation and Consequent Urea Excretion
In a Normal Patient (on Normal Diet), There is Generation and Excretion of 600-900 mOsmol of Solute Per Day (Composed Predominantly of Sodium Salts, Potassium Salts, and Urea)
If the Minimum Urine Osmolality is Around 60 mOsmol/kg, the Maximum Urine Output Would Be Around 10-15L Per Day (900 mOsmol Per Day ÷ 60 mOsmol Per kg = 15 L)
However, in a Patient with Beer Potomania, the Daily Solute Excretion May Decrease to <250 mOsmol of Solute Per Day and Even with Maximal Urine Dilution, Daily Free Water Excretion Would Decrease to <4 L/Day (240 mOsmol Per Day ÷ 60 mOsmol Per kg = 4 L)
Therefore, Hyponatremia Can Occur if >4L of Water is Ingested Per Day (This Equates to Approximately 12 Cans of Beer Per Day)
If a Patient Develops Any Superimposed Nausea or Hypovolemia (Both of Which Stimulate Antidiuretic Hormone Secretion). Impairment of Urine Dilution Occurs, Worsening the Hyponatremia
Tea and Toast Diet with Decreased Dietary Sodium (Solute) Intake
Epidemiology
Ingestion of Low Protein/High Water Diet (Lancet, 1975) [MEDLINE] (Am J Kidney Dis, 1998) [MEDLINE] (Lancet, 2002) [MEDLINE]
Mechanism
Low Protein Diet Results in Suppression of Endogenous Protein Degradation and Decreased Urea Excretion, Decreasing the Water Excretory Capacity
If a Patient Develops Any Superimposed Nausea or Hypovolemia (Both of Which Stimulate Antidiuretic Hormone Secretion). Impairment of Urine Dilution Occurs, Worsening the Hyponatremia
Psychiatric Patients with Polydipsia and Hyponatremia Have Unexplained Defects in Urinary Dilution, Osmoregulation of Water Intake, and the Secretion of Vasopressin (NEJM, 1988) [MEDLINE]
In Some Patients, the Osmotic Threshold for Thirst is Decreased Below the Threshold for the Release of Antidiuretic Hormone (Clin Endocrinol-Oxf, 1991) [MEDLINE]: this is in contrast to normal patients, in whom the thirst threshold is roughly equal to or a few mosmol/kg higher than the threshold for antidiuretic hormone release
Some Polydipsia Patients with Hyponatremia Have a Higher Urine Osmolality than is Expected, Suggesting a Concurrent Increase in Antidiuretic Hormone Release and/or Response (Due to Various Mechanisms)
Since Normal Patients Can Excrete >400-600 mL of Urine Per Hour (Mediated by Suppression of Antidiuretic Hormone Secretion and the Subsequent Formation of a Dilute Urine with a Minimum Urine Osmolality of 40-100 mosmol/kg), Assuming Normal Renal Function and Intact Antidiuretic Hormone Regulation, Primary Polydipsia Should Not Result in Clinically Significant Hyponatremia Unless There is a Massive Increase in Water Intake (Q J Med, 1959) [MEDLINE]
In Some Institutionalized Patients with Severe Psychosis, Water Intake May Exceed 400-600 mL Per Hour, Overtasking the Renal Water Excretion Mechanism
Acute Water Loading of 3-4L (Prior to a Radiologic Exam or in an Attempt to Avoid a Positive Urine Drug Test) May Result in Hyponatremia (JAMA, 1991) [MEDLINE]
Primary Polydipsia Can Also Occur with Hypothalamic Thirst Center Lesions (Sarcoidosis, etc)
Disorders with Impaired Urine Dilution, But Normal Suppression of Antidiuretic Hormone (ADH)
Moderate-Severe Renal Failure May Have a Serum Osmolality Which is Higher Than Predicted by Their Serum Sodium Concentration, Due to the Presence of Urea in Extracellular Fluid
However, Since Urea is an “Ineffective Osmole” (It Can Freely Cross Cell Membranes and Does Not Obligate Water Movement Out of Cells), the Effective Serum Osmolality (Measured Osmolality Minus the Contribution of Urea) is Low
Mechanism
Ability of the Kidney to Excrete Free Water (Free Water Excretion/GFR) is Generally Preserved in Mild-Moderate Renal Failure
Therefore, Normonatremia is Usually Present
However, in Advanced Renal Failure (GFR <15 mL/min), the Minimum Urine Osmolality Can Increase to as High as 200-250 mOsm/kg, Despite Appropriate Suppression of Antidiuretic Hormone Secretion
This Results in an Impaired Ability to Excrete Free Water
Study of Sodium Alterations in the EPHESUS Trial of Myocardial Infarction with Left Ventricular Systolic Dysfunction (Clin Res Cardiol, 2022) [MEDLINE]: n = 6,221
Eplerenone Group Had a Lower Mean Serum Sodium During the Follow-Up Period (140 vs 141 mmol/L; p < 0.0001)
Eplerenone Group More Frequently Developed Hyponatremia (15 vs 11% p = 0.0001) and Less Frequently, Hypernatremia (22 vs 26% p = 0.0003)
FE Uric Acid >12% Has Been Reported in a Small Study to Diagnose SIADH (Over Thiazide-Associated Hyponatremia) with a 100% Positive Predictive Value, While an FE Uric Acid <8% Excluded SIADH with a 100% Negative Predictive Value (J Clin Endocrinol Metab, 2008) [MEDLINE]
However, Other Larger Studies Have Not Supported These Findings (Cureus, 2020) [MEDLINE]
Clinical
Euvolemia: common
Treatment
Trial of Discontinuation of Thiazide: hyponatremia should improve (but some patients may remain mildly hyponatremic for a week or more after discontinuation of the thiazide)
Cirrhosis/End-Stage Liver Disease (ESLD) (see Cirrhosis)
Mechanisms
Arterial Vasodilation, Resulting in Decreased Effective Arterial Blood Volume and Consequently, Decreased Blood Pressure Sensed at the Carotid Sinus Baroreceptors
Decreased Tissue Perfusion
Increased Plasma and Extracellular Fluid Volumes
Increased Antidiuretic Hormone Secretion
Diagnosis
Serum Antidiuretic Hormone Level Correlates with the Severity of the Underlying Cirrhosis
Dermal Fluid/Sodium Loss (Due to Burns, Heat Stroke, Prolonged Environmental Exposure, etc)
Gastrointestinal Fluid/Sodium Loss (Due to Diarrhea, Vomiting, Sodium Picosulfate Solutions for Bowel Preparation, etc)
Renal Fluid/Sodium Loss (Excessive Diuresis, Pheochromocytoma, Salt-Wasting Nephropathy, Severe Hyperglycemia, etc)
Third-Space Fluid/Sodium Loss (Due to Acute Pancreatitis, Ascites, Bowel Obstruction, Burns, Muscle Trauma, Peritonitis, Large-Volume Paracentesis, etc)
Mechanism
Increased Antidiuretic Hormone Secretion
Diagnosis
With Clinical Evidence of Hypovolemia, Low Urine Sodium (<25 mEq/L) Indicates a Diagnosis Such as Gastrointestinal Fluid Loss, Third-Space Fluid Loss, or Prior Diuresis (After the Effect of the Diuretic Has Diminished)
With Clinical Evidence of Hypovolemia, High Urine Sodium (>40 mEq/L) with Low Urine Chloride (<25 mEq/L) Indicates a Diagnosis Such as Metabolic Alkalosis Due to Vomiting
With Clinical Evidence of Hypovolemia, High Urine Sodium (>40 mEq/L) with High Urine Chloride (>40 mEq/L) Indicates a Diagnosis Such as Renal Salt Loss (Such as During Active Diuretic Therapy, Primary Adrenal Insufficiency with Deficiency of Cortisol and Aldosterone, Cerebral Salt Wasting, etc)
Hypotension and Decreased Cardiac Output, Resulting in Decreased Effective Arterial Blood Volume
Lack of Cortisol (Which Would Normally Function to Suppress Antidiuretic Hormone Release)
Diagnosis
While May Be Associated with Hyperkalemia, it is Important to Note that Hyperkalemia is Absent in 33% of Patients with Adrenal Insufficiency
Clinical
Note that Primary Adrenal Insufficiency is Associated with Hypovolemic Hyponatremia, While Secondary Adrenal Insufficiency (Below, Under SIADH) is Associated with Euvolemic Hyponatremia
Secondary Adrenal Insufficiency (Hypopituitarism) (see Adrenal Insufficiency): note that primary adrenal insufficiency (above) is associated with hypovolemic hyponatremia, while secondary adrenal insufficiency is associated with euvolemic hyponatremia
Gastrointestinal Disease
Neoplastic Disease
Neuropsychiatric Disease
Pulmonary Disease
Drugs/Toxins
Hereditary (Nephrogenic SIADH Due to Abnormal Vasopressin V2 Receptor)
Other
Idiopathic
Mechanism
Excessive Antidiuretic Hormone (ADH) Release Causing Renal Water Reabsorption (and Expansion of the Body’s Intracellular and Extracellular Fluid Compartments), Resulting in Hyponatramia
Diagnosis
Euvolemia
Hypoosmolality
Increased Urine Sodium (>20 mEq/L and Usually >40 mEq/L)
High Urine Osmolality (>100 mosmol/kg)
Other Features
Normal Serum Potassium Concentration
Absence of Acid-Base Disturbance
Low Serum Uric Acid Concentration (Frequently)
Clinical
Euvolemic Hyponatremia
Abnormally Low Osmostat
General Comments
In These Patients, a Water Load Will Appropriately Suppresses Antidiuretic Hormone Release, But at a Lower Serum Osmolality than in Normal Patients
These Patients Typically Present with a Moderate Hyponatremia (Usually 125-135 mEq/L) Which Remains Stable on Multiple Measurements
Hyponatremia is a Major Cause of Mortality Related to Ecstasy Intoxication
Females are More Likely to Develop Ecstasy-Induced Hyponatremia and are More Likely to Develop Severe Neurologic Complications (Coma, Death)
Mechanisms
Increased Water Intake
SIADH, Resulting in Impairment of Water Excretion
Iatrogenic Hyponatremia
Mechanism
Hypotonic Intravenous Fluid Administration
Epidemiology
Particularly Occurs with D5W Infusion
Postoperative Hyponatremia
Mechanisms
Administration of Hypotonic Intravenous Fluid During Surgery
Increased Secretion of Antidiuretic Hormone (Due to Pain/Drugs/Nausea/Stress/Low Circulating Blood Volume), Resulting in Water Retention
Excessive Intravenous Fluid Administration, Resulting in Increased Circulating Blood Volume and Overexpansion of Extracellular Fluid Volume, Culminating in Increased Volume of Hypertonic Urine (Sodium Loss)
Physiology
Definition of Hyponatremia
Hyponatremia is Defined as Serum Sodium <135 mEq/L
Definitions of Serum Tonicity and Osmolality
Serum Tonicity Reflects the Concentrations of “Effective Osmoles” (Solutes Which Do Not Move Freely Across Cell Membranes and Obligate Water to Move with Them)
Serum Tonicity is the Property Which is Detected by Osmoreceptors
Serum Tonicity Also Modulates the Movement of Water Between Cells and Extracellular Fluid (i.e. the Transcellular Distribution of Water)
Water Freely Crosses All Cell Membranes, Moving from an Area of Lower Tonicity (Higher Water Content) to an Area of Higher Tonicity (Lower Water Content)
Plasma Hypotonicity Makes Cells Swell, While Plasma Hypertonicity Makes Cells Shrink
Hypernatremia Always Indicates Hypertonicity
Hyponatremia May Be Hypotonic (in Most Cases), Isotonic, or Hypertonic
Serum Osmolality Reflects the Concentrations of Both “Effective Osmoles” (Solutes Which Do Not Move Freely Across Cell Membranes and Obligate Water to Move with Them) and “Ineffective Osmoles” (Solutes Which Equilibrate Across Cell Membranes and Do Not Obligate Water to Move with Them) (see Serum Osmolality)
Serum Sodium is Restricted to the Serum Water Fraction
Nonaqueous Components (Mostly Lipids and Proteins) Account for 7% of the Serum Volume
Normal Sodium Movement Across Capillary Membranes (NEJM, 2015) [MEDLINE]
Under Normal Conditions, Sodium Readily Crosses Systemic Capillary Membranes Via Clefts Between the Endothelial Cells
As a Result, Plasma Sodium Concentration and Systemic Interstitial Fluid Sodium Concentration are Nearly Identical (with Only a Small Difference Created by the Presence of Intravascular Albumin)
In Contrast, Under Normal Conditions, the Brain Capillaries Have Tight Endothelial Junctions and are Lined by Astrocytic Foot Processes
Astrocytes Possess Aquaporin-4 Channels Which Allow Water to Cross, But Not Sodium, Creating a Blood-Brain Barrier Which is Impermeable to Sodium
Animal Studies Indicate that Aquaporin-4 Mediates a Significant Portion of Osmotic Water Transport into the Brain (Nat Med, 2000) [MEDLINE]
Consequently, an Abnormal Plasma Sodium Concentration Results in Water Entering or Leaving the Brain
Due to the Confined Space of the Skull Compartment, Only a Small Degree of Brain Swelling or Shrinkage Can Be Tolerated without Brain Compromise
Plasma Sodium, Therefore, Affects Brain Volume
For This Reason, Cell Volume Receptors Which Modulate Thirst and Vasopressin Secretion are Located in the Brain
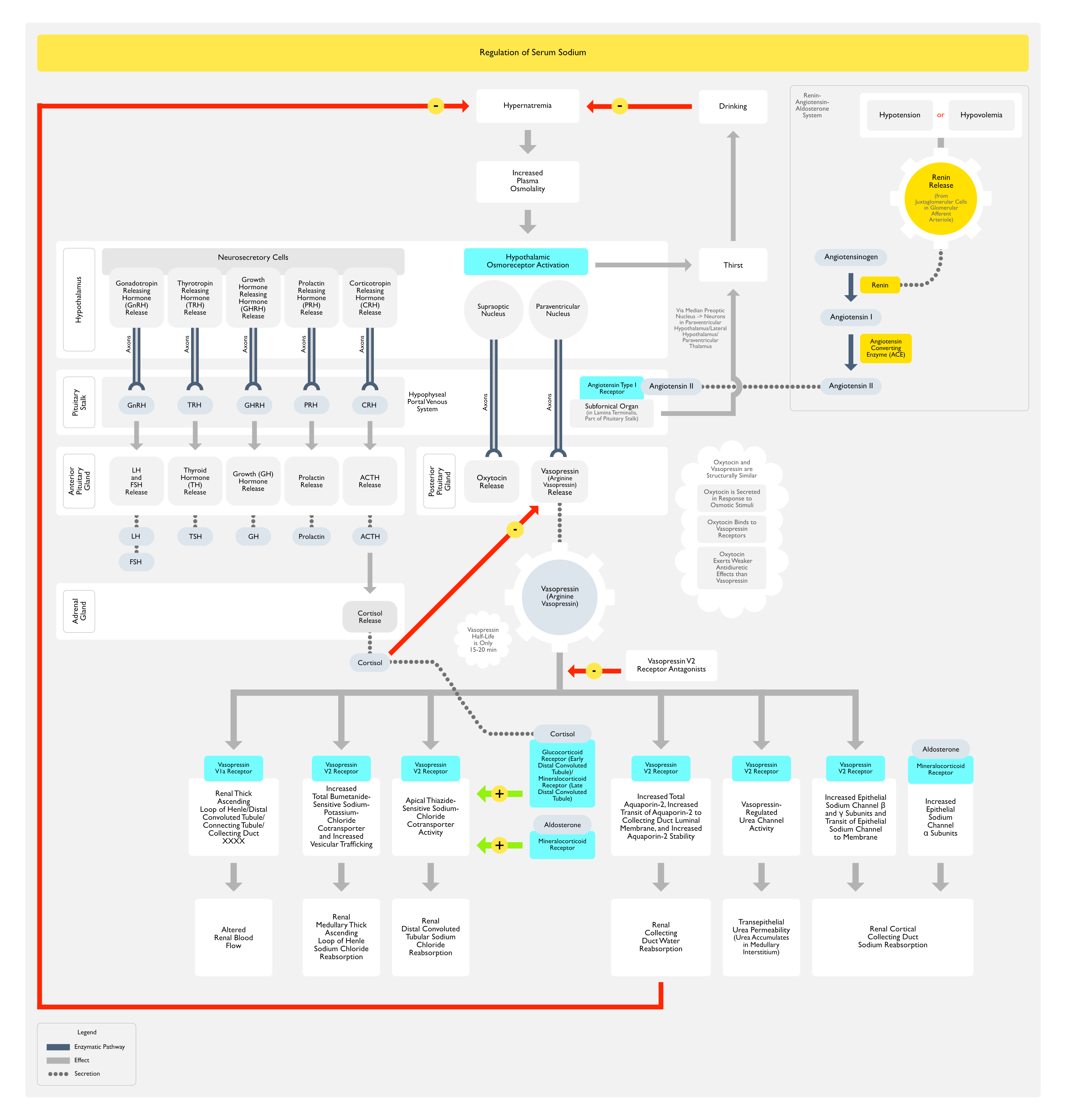
Osmoreceptors (Most Accurately Called “Tonicity Receptors”) are Hypothalamic Neurons Which Express Transient Receptor Potential Cation Channel Subfamily Vanilloid Member 1 (TRPV1) and Member 4 (TRPV4) Channels on Their Cell Membranes
Regulation of Plasma Sodium Concentration (NEJM, 2015) [MEDLINE]
During Normal Physiologic Osmoregulation, When the Plasm Sodium Concentration is Decreased to <135 mEq/L (<135 mmmol/L), Serum Hypotonicity Results in the Swelling of Osmoreceptor Cells, Causing the Inhibition of Thirst and Inhibition of Posterior Pituitary Vasopressin Antidiuretic Hormone Secretion (the Latter of Which Results in Aquaresis) (Clin J Am Soc Nephrol, 2015) [MEDLINE]
In the Absence of Vasopressin, Urine Osmolality Can Decrease to as Low as 50 mOsm/kg
At a Plasma Sodium Concentration >135 mEq/L, Vasopressin Levels are Usually Detectable and They Increase Linearly with an Increase in Plasma Sodium Concentration
Vasopressin May Also Be Secreted in Response to Hypovolemia
Vasopressin Binds to V2 Receptors on the Basolateral Membranes of the Principal Cells Lining the Renal Collecting Ducts
In the Presence of Vasopressin, Aquaporins are Inserted into the Luminal Membranes, Allowing Water to Flow Out, Attracted by the High Solute Concentration of the Surrounding Medullary Interstitium
When the Plasma Sodium Concentration Increases to Approximately 145 mEq/L, Vasopressin Levels are Normally Elevated Enough to Result in Maximally Concentrated Urine (About 1200 mOsm/kg)
Development of Hypernatremia
The Presence of a Dilute Urine When the Plasma Sodium Concentration is >145 mEq/L Indicates Either Deficient Vasopressin Secretion (as Occurs in Neurogenic Diabetes Insipidus) or a Failure of the Kidneys to Respond to Vasopressin (as Occurs in Nephrogenic Diabetes Insipidus) (see Diabetes Insipidus)
However, Even Complete Diabetes Insipidus (with Total Absence of Vasopressin or an Absence of Tubular Response to Vasopressin) Typically Does Not Cause Hypernatremia, Because Thirst Results in the Voluntary Replacement of Urinary Water Losses
Hypernatremia Can Then Develop if Oral Water Intake Does Not Occur (Due to Inadeqaute Access to Water, Illness/Extremes of Age Preventing Oral Water Intake, Hypodipsia, etc)
Development of Hyponatremia
The Normal Physiologic Ability to Maximally Dilute the Urine Prevents the Development of Hyponatremia Unless Oral Water Intake Exceeds 1L/hr (as in Schizophrenia with High Water Intake, etc) or in Patients with Low Urinary Solute Excretion (as in Beer Potomania, Where Oral Food Intake is Very Low)
Except for These Two Scenarios, Hypotonic Hyponatremia is Associated with Impaired Generation of a Dilute Urine Due to Decreased Sodium Transport in Renal Tubular Diluting Sites (Due Most Commonly to Diuretics, But Also to Presence of Vasopressin, or Rarely, an Inherited Activating Mutation of the Vasopressor Receptor)
Because Vasopressin (with Renin/Angiotension/Aldosterone and the Sympathetic Nervous System) Participates in the Neurohumoral Response to Hypovolemia, Vasopressin-Induced Hyponatremia May Complicate Hypovolemia or Edema States (Congestive Heart Failurem, Cirrhosis, etc)
Physiologic Changes Associated with Hyponatremia
General Comments
Since Intracellular and Extracellular Osmolality Must Remain Equal, Hyponatremia Causes Cells to Either Swell with Water or Expel Solutes (to Counter the Swelling)
Decreased Serum Osmolality Results in an Osmolal Gradient Which Favors the Movement of Water into Brain Cells
Within the Confined Space of the Brain, Any Cellular Swelling Can Result in Cerebral Edema (J Am Soc Nephrol, 1992) [MEDLINE] (NEJM, 1995) [MEDLINE] (NEJM, 2015) [MEDLINE]
Over Time, Brain Cells Expel Organic Solutes from their Cytoplasm, Allowing the Intracellular Osmolality to Equal Plasma Osmolality Without a Large Increase in Cellular Water
Acute vs Chronic Hyponatremia
In Acute Hyponatremia (<48 hrs)
Movement of Water into Brain Cells (Cellular Swelling) Occurs Over a Few Hours and Outpaces the Brain’s Ability to Expel Solutes, Resulting in Cerebral Edema (and Potentially Herniation)
In Chronic Hyponatremia (≥48 hrs)
While There is Propensity of Water to Move into Brain Cells (Causing Cellular Swelling) Over a Period of Days, the Brain is Able to Expel Osmotic Solutes/Organic Osmolytes (Mostly, Choline and Myoinositol, with Glutamine and Glutamate to a Lesser Extent) Via Swelling-Activated Membrane Channels (Which Also Transport Chloride and Other Anions) and Minimize the Development of Cerebral Edema (J Clin Invest, 1995) [MEDLINE]
Significant Depletion of Brain Organic Osmolytes Occurs Within 24 hrs (and Additional Losses Occur Over 2-3 Days, Due to Downregulation of the Synthesis and Uptake of These Organic Osmolytes) (J Am Soc Nephrol, 1992) [MEDLINE] (NEJM, 1995( [MEDLINE]
As a Result, Patients with Chronic Hyponatremia Have More Modest Clinical Symptoms and Almost Never Die of Cerebral Edema with Brain Herniation
During the Correction of Chronic Hyponatremia, the Reuptake of Brain Organic Osmolytes Occurs More Slowly than the Loss of the Organic Osmolytes During the Onset of Hyponatremia: this observation is the basis for corretcing chronic chronic hyponatremia more slowly
Hyponatremia in the Setting of Advanced Renal Failure or Ethanol Intoxication
In These Two Clinical Situations, if Hyponatremia is Present, These Patients May Have a Higher Serum Osmolality than that Predicted by their Sodium Concentration Due to the Contribution of Urea or Ethanol in the Extracellular Fluid
However, Since Both Urea and Ethanol are “Ineffective Osmoles” (They Can Freely Cross Cell Membranes and Do Not Obligate Water Movement Out of Cells), the Effective Serum Osmolality (Measured Osmolality Minus the Contribution of Urea) is Low
For This Reason, Hyponatremic Patients with Advanced Renal Failure or Ethanol Intoxication are as Likely to Develop Clinical Symptoms at a Given Serum Sodium Concentration as Patients without These Conditions
In the Presence of Hyperproteinemia/Hypertriglyceridemia (with Expansion of Nonaqueous Component of the Serum), Pseudohyponatremia May Be Seen with This Assay Method
Sodium-Selective Electrode Assay of Sodium
Measures Sodium Activity in Serum Water: this assay gives the true, physiologically relevant sodium concentration as it measures sodium activity in serum water alone
Indirect Potentiometry: current assay used in many hospital laboratories
Normal Patients Can Excrete >400-600 mL of Urine Per Hour (Mediated by Suppression of Antidiuretic Hormone Secretion and the Subsequent Formation of a Dilute Urine with a Minimum Urine Osmolality of 40-100 mosmol/kg)
Urine Osmolality Ranges from Approximately 50-1,200 mOsm/kg (BMJ, 2011) [MEDLINE]
Urine Osmolality >100 mOsm/kg Implies ADH-Mediated Free Water Reabsorption and Would Be Considered Abnormally Concentrated Urine in a Hyponatremic State
Urine Osmolality <100 mOsm/kg Denotes a Dilute Urine and Implies the Absence of ADH (or Lack of Response to ADH)
Laboratory Patterns
Clinically Hypovolemic Patient
Dermal Fluid Loss/Gastrointestinal Fluid Loss/Third-Space Fluid Loss/Prior Diuresis (After the Effect of the Diuretic Has Diminished) (see Hypovolemic Shock)
Low Urine Sodium (<25 mEq/L): due to hypovolemia-induced renal sodium retention
In a Study of Hyponatremic Patients without Edema (n = 58), the Mean Urine Sodium was 18 mEq/L in Patients Who Were Assessed to Hypovolemic (Determined by a Significant Increase in Serum Sodium Following Isotonic Saline Challenge), as Compared to 72 mEq/L in Patients with SIADH (Determined by No Increase in Serum Sodium Following Isotonic Saline Challenge) (Am J Med, 1987) [MEDLINE]
Clinical Assessment of Volume Status Correctly Identified Only 48% of the Patients in This Study
High Urine Sodium (>40 mEq/L): since diuretics are natriuretics
High Urine Chloride (>40 mEq/L)
Primary Adrenal Insufficiency (i.e. Deficiency of Cortisol and Aldosterone) (see Adrenal Insufficiency)
High Urine Sodium (>40 mEq/L)
High Urine Chloride (>40 mEq/L)
Cerebral Salt Wasting: laboratory parameters resemble that of SIADH, except that the patient has clinical hypovolemia
High Urine Sodium (>40 mEq/L)
High Urine Chloride (>40 mEq/L)
Clinically Euvolemic Patient
Pseudohyponatremia
Normal Serum Sodium
Normal Serum Osmolality: since osmometers measure the activity of solutes in plasma water
Decreased Sodium Intake (Beer Potomania, Tea and Toast Diet)
Low Urine Sodium (<25 mEq/L)
Low Urine Osmolality (<100 mosmol/kg)
In a Study Examining the Additional Utility of Urine Osmolality and Urine Urea and Creatinine Concentrations in Patients Who were Suspected of Having Primary Polydipsia vs Malnutrition as the Etiology of Their Hyponatremia (J Clin Med, 2019) [MEDLINE]
Authors Suggested that Patients with Low Solute Intake (FE.Osm<1.4%) and Low Diuresis (V/eCcr<0.8%) Should Increase Their Intake by Taking Oral Urea
Authors Suggested that Patients with High Solute Intake (FE.Osm>2.5%) and High Diuresis (V/eCcr>1.5%) Should Be Treated with Mild Water Restriction (<1.5-2L/day)
Primary Polydipsia
Low Urine Sodium (<25 mEq/L)
Low Urine Osmolality (<100 mosmol/kg)
In a Study Examining the Additional Utility of Urine Osmolality and Urine Urea and Creatinine Concentrations in Patients Who were Suspected of Having Primary Polydipsia vs Malnutrition as the Etiology of Their Hyponatremia (J Clin Med, 2019) [MEDLINE]
Authors Suggested that Patients with Low Solute Intake (FE.Osm<1.4%) and Low Diuresis (V/eCcr<0.8%) Should Increase Their Intake by Taking Oral Urea
Authors Suggested that Patients with High Solute Intake (FE.Osm>2.5%) and High Diuresis (V/eCcr>1.5%) Should Be Treated with Mild Water Restriction (<1.5-2L/day)
Euvolemic Patient in Whom Hypopituitarism, Hypoadrenalism, Hypothyroidism, Renal Insufficiency, and Diuretic Use Have Been Excluded
Normal Serum Potassium and Bicarbonate (Typically) (Am J Kidney Dis, 1991) [MEDLINE]
While Water Retention May Decrease the Serum Potassium by Dilution, Cells Release Potassium in an Attempt to Minimize Hypoosmolality-Induced Cell Swelling, Raising the Serum Potassium Back Toward Normal
While Water Retention May Decrease the Plasma Bicarbonate by Dilution, Increased Acid Excretion Due to Mild Hyperaldosteronism Induced by Hyponatremia Will Raise the Plasma Bicarbonate Back Toward Normal ( J Clin Endocrinol Metab, 2003) [MEDLINE]
In a Study of Hyponatremia Patients without Edema (n = 58), the Mean Urine Sodium was 18 mEq/L in Patients Who Were Assessed to Hypovolemic (Determined by a Significant Increase in Serum Sodium Following Isotonic Saline Challenge), as Compared to 72 mEq/L in Patients with SIADH (Determined by No Increase in Serum Sodium Following Isotonic Saline Challenge) (Am J Med, 1987)* [MEDLINE]
Clinical Assessment of Volume Status Correctly Identified Only 48% of the Patients in This Study
Low Blood Urea Nitrogen (BUN) (<5 mg/dL): due to increased urea clearance
However, This Finding is Variable (and its Absence Does Not Exclude the Presence of SIADH)
Low Serum Osmolality (<270 mOsm/L)
Hypouricemia (<4 mg/dL): due to increased urinary uric acid clearance
However, This Finding is Variable (and its Absence Does Not Exclude the Presence of SIADH)
High Urine Osmolality (Usually >300 mOsm/L)
High Fractional Excretion of Uric Acid (FE Uric Acid >10-12%)
FE Uric Acid >12% Has Been Reported in a Small Study to Diagnose SIADH (Over Thiazide-Associated Hyponatremia) with a 100% Positive Predictive Value, While an FE Uric Acid <8% Excluded SIADH with a 100% Negative Predictive Value (J Clin Endocrinol Metab, 2008) [MEDLINE]
However, Other Larger Studies Have Not Supported These Findings (Cureus, 2020) [MEDLINE]
FENa is Not Recommended to Evaluate Patients with Hyponatremia
In Patients with Oliguric Acute Kidney Injury (AKI) Where FENa is Typically Employed in the Evaluation of These Patients, FENa Provides a More Accurate Assessment of Volume Status than the Urine Sodium Because it Corrects for the Effect that Variations in Urine Volume Have on the Urine Sodium
However, FENa is Far Less Useful in Patients without Oliguria
A FENa <1% is Not an Indicator of Effective Hypovolemia in Patients with Normal or Mild-Moderate Renal Dysfunction Who Have a Much Higher Glomerular Filtration Rate and a Much Greater Filtered Sodium Load
References
General
Common fluid-electrolyte and acid-base problems in the intensive care unit: selected issues. Semin Nephrol 1994; 14:8-22 [MEDLINE]
Hyponatremia. N Engl J Med. 2000 May 25;342(21):1581-9 [MEDLINE]
Hyponatraemia in clinical practice. Postgrad Med J. Jun 2007; 83(980): 373–378. doi: 10.1136/pgmj.2006.056515 [MEDLINE]
Epidemiology
Hyponatremia: a prospective analysis of its epidemiology and the pathogenetic role of vasopressin. Ann Intern Med. 1985;102:164–168 [MEDLINE]
Age and gender as risk factors for hyponatremia and hypernatremia. Clin Chim Acta. 2003;337:169–172 [MEDLINE]
Incidence and prevalence of hyponatremia. Am J Med. 2006;119(suppl 1):S30–S35 [MEDLINE]
Etiology
Prognostic importance of serum sodium concentration and its modification by converting-enzyme inhibition in patients with severe chronic heart failure. Circulation. 1986 Feb;73(2):257-67 [MEDLINE]
Clinical assessment of extracellular fluid volume in hyponatremia. Am J Med. 1987;83(5):905 [MEDLINE]
Pseudohyponatremia: a reappraisal. Am J Med. 1989;86(3):315 [MEDLINE]
The electrolytes in hyponatremia. Am J Kidney Dis. 1991;18(5):527 [MEDLINE]
Postoperative hyponatremic encephalopathy in menstruant women. Ann Intern Med. 1992;117(11):891 [MEDLINE]
Maltose-induced hyponatremia. Ann Intern Med. 1993;118(7):526 [MEDLINE]
Transurethral resection syndrome from extravascular absorption of irrigating fluid. Scand J Urol Nephrol. 1993;27(3):387 [MEDLINE]
Postoperative hyponatremia despite near-isotonic saline infusion: a phenomenon of desalination. Ann Intern Med. 1997;126(1):20 [MEDLINE]
Posthysteroscopic hyponatremia: evidence for a multifactorial cause. Am J Kidney Dis. 1997;30(5):717 [MEDLINE]
Hyponatremia: evaluating the correction factor for hyperglycemia. Am J Med. 1999;106(4):399 [MEDLINE]
Reemergence of sucrose nephropathy: acute renal failure caused by high-dose intravenous immune globulin therapy. South Med J. 2000;93(9):901 [MEDLINE]
Hyponatremia, cerebral edema, and noncardiogenic pulmonary edema in marathon runners. Ann Intern Med. 2000;132(9):711 [MEDLINE]
Mechanisms of hyponatraemia in alcohol patients. Alcohol Alcohol. 2000;35(6):612 [MEDLINE]
Derivation and validation of a formula to calculate the contribution of ethanol to the osmolal gap. Ann Emerg Med. 2001;38(6):653 [MEDLINE]
Transurethral prostatectomy: immediate and postoperative complications. Cooperative study of 13 participating institutions evaluating 3,885 patients. J Urol, 141: 243-247, 1989. J Urol. 2002;167(1):5 [MEDLINE]
Intravenous immunoglobulin therapy results in post-infusional hyperproteinemia, increased serum viscosity, and pseudohyponatremia. Am J Hematol. 2003;73(2):97 [MEDLINE]
Low plasma bicarbonate level in hyponatremia related to adrenocorticotropin deficiency. J Clin Endocrinol Metab. 2003;88(11):5255 [MEDLINE]
Clinical problem-solving. Mind the gap. N Engl J Med. 2003;349(15):1465 [MEDLINE]
Osmole gap in neurologic-neurosurgical intensive care unit: Its normal value, calculation, and relationship with mannitol serum concentrations. Crit Care Med. 2004;32(4):986 [MEDLINE]
Clinical studies of thiazide-induced hyponatremia. J Natl Med Assoc. 2004;96(10):1305 [MEDLINE]
Effects of hyperlipidemia on plasma sodium, potassium, and chloride measurements by an indirect ion-selective electrode measuring system. Clin Chem. 2006 Jan;52(1):155-6 [MEDLINE]
Fluid absorption in endoscopic surgery. Br J Anaesth. 2006;96(1):8 [MEDLINE]
Pseudohyponatremia: does it matter in current clinical practice? Electrolyte Blood Press. 2006 Nov;4(2):77-82. doi: 10.5049/EBP.2006.4.2.77 [MEDLINE]
Preventing a drop in effective plasma osmolality to minimize the likelihood of cerebral edema during treatment of children with diabetic ketoacidosis. J Pediatr. 2007;150(5):467 [MEDLINE]
Beer potomania: an unusual cause of hyponatremia at high risk of complications from rapid correction. Am J Kidney Dis. 2007 Oct;50(4):673-80 [MEDLINE]
Acute renal failure, translocational hyponatremia and hyperkalemia following intravenous immunoglobulin therapy. Nephron Clin Pract. 2007;106(4):c143 [MEDLINE]
Technological advances in transurethral resection of the prostate: bipolar versus monopolar TURP. J Endourol. 2008;22(8):1587 [MEDLINE]
Value of fractional uric acid excretion in differential diagnosis of hyponatremic patients on diuretics. J Clin Endocrinol Metab. 2008;93(8):2991 [MEDLINE]
The harmful health effects of recreational ecstasy: a systematic review of observational evidence. Health Technol Assess. 2009;13(6):iii [MEDLINE]
Acute hyponatremia after cardioplegia by histidine-tryptophane-ketoglutarate–a retrospective study. J Cardiothorac Surg. 2012;7:52 [MEDLINE]
Preoperative hyponatremia and perioperative complications. Arch Intern Med. 2012 Oct 22;172(19):1474-81. doi: 10.1001/archinternmed.2012.3992 [MEDLINE]
Fluid, electrolyte, and acid-base disturbances. Case 6: Diabetes and acidosis. Nephrol Self Assess Program. 2013;12:193
Desmopressin to Prevent Rapid Sodium Correction in Severe Hyponatremia: A Systematic Review. Am J Med. 2015 Dec;128(12):1362.e15-24 [MEDLINE]
Pseudohypernatremia and pseudohyponatremia: a linear correction. Nephrol Dial Transplant. 2015 Feb;30(2):252-7 [MEDLINE]
Extreme hypercholesterolemia presenting with pseudohyponatremia – a case report and review of the literature. J Clin Lipidol. 2015 Mar-Apr;9(2):260-4 [MEDLINE]
Exogenous Vasopressin-Induced Hyponatremia in Patients With Vasodilatory Shock: Two Case Reports and Literature Review. J Intensive Care Med. 2015 Jul;30(5):253-8. doi: 10.1177/0885066613507410 [MEDLINE]
Disorders of plasma sodium–causes, consequences, and correction. N Engl J Med. 2015 Jan;372(1):55-65 [MEDLINE]
Symptomatic absorption of isotonic saline during transcervical endometrial resection. Acta Anaesthesiol Scand. 2017;61(1):121 [MEDLINE]
Pseudohyponatremia in Hypertriglyceridemia-Induced Acute Pancreatitis: A Tool for Diagnosis Rather Than Merely a Laboratory Error? Pancreas. 2019;48(1):126 [MEDLINE]
Estimated Daily Urine Volume and Solute Excretion from Spot Urine Samples to Guide the Therapy of Hyponatremia in SIADH. J Clin Med. 2019;8(10) [MEDLINE]
The Role of Fractional Excretion of Uric Acid in the Differential Diagnosis of Hypotonic Hyponatraemia in Patients with Diuretic Therapy. Cureus. 2020;12(4):e7762 [MEDLINE]
Serum sodium and eplerenone use in patients with a myocardial infarction and left ventricular dysfunction or heart failure: insights from the EPHESUS trial. Clin Res Cardiol. 2022 Apr;111(4):380-392. doi: 10.1007/s00392-021-01853-8 [MEDLINE]
Physiology
Regulation of solute and water balance and cell volume in the central nervous system. J Am Soc Nephrol. 1992;3(1):12 [MEDLINE]
Regulation of cell volume in health and disease. N Engl J Med. 1995;333(19):1260 [MEDLINE]
Human cerebral osmolytes during chronic hyponatremia. A proton magnetic resonance spectroscopy study. J Clin Invest. 1995;95(2):788 [MEDLINE]
Aquaporin-4 deletion in mice reduces brain edema after acute water intoxication and ischemic stroke. Nat Med. 2000;6(2):159 [MEDLINE]
The pathophysiology and treatment of hyponatraemic encephalopathy: an update. Nephrol Dial Transplant. 2003;18(12):2486 [MEDLINE]
Osmotic homeostasis. Clin J Am Soc Nephrol. 2015 May;10(5):852-62 [MEDLINE]