Treatment of Hypertensive Emergency in the Setting of Congestive Heart Failure (CHF) (see Congestive Heart Failure)
Recommendations-2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults (Circulation, 2018) [MEDLINE]
Treatment of Hypertension in Patients at Risk for Developing Congestive Heart Failure (CHF)
In Adults with Hypertension, Adjusting Systolic Blood Pressure (SBP) to <130 mm Hg is Recommended to Decrease the Risk of Developing Heart Failure (Class of Recommendation: I; Level of Evidence: B-R)
In Adults with Hypertension, Adjusting Diastolic Heart Failure (DBP) to <80 mm Hg is Recommended to Decrease the Risk of Developing Heart Failure (Class of Recommendation: I; Level of Evidence: C-EO)
Treatment of Hypertension in the Setting of Heart Failure with Reduced Ejection Fraction (HFrEF)
Adults with Heart Failure with Reduced Ejection Fraction (HFrEF) and Hypertension Should Be Prescribed Guideline-Directed Medical Therapy (GDMT) Titrated to Attain a Blood Pressure <130/80 mm Hg (Class of Recommendation: I; Level of Evidence: C-EO)
In Patients with Heart Failure with Reduced Ejection Fraction (HFrEF) (Even if Asymptomatic) Use One of the Three β-Blockers Proven to Reduce Mortality and Hospitalizations
In Patients with Symptomatic Heart Failure with Reduced Ejection Fraction (HFrEF) and eGFR is >30 mL/min/1.73 m2 with Potassium is <5.0 mEq/L, Spironolactone or Eplerenone is Recommended to Reduce Morbidity and Mortality (see Spironolactone and Eplerenone)
In Patients with Heart Failure with Reduced Ejection Fraction (HFrEF) and NYHA Functional Class II-III Symptoms, An Angiotensin Receptor-Neprilysin Inhibitor is Recommended to Decrease Morbidity and Mortality (see Sacubitril/Valsartan)
When the Use of an Angiotensin Receptor-Neprilysin Inhibitor is Not Feasible, an Angiotensin Converting Enzyme (ACE) Inhibitor or an Angiotensin II Receptor Blocker (ARB) is Recommended to Decrease Morbidity and Mortality (see Angiotensin Converting Enzyme Inhibitors and Angiotensin II Receptor Blockers)
In Patients with Symptomatic Heart Failure with Reduced Ejection Fraction (HFrEF) (Irrespective of the Presence of Type 2 Diabetes Mellitus), Sodium-Glucose Cotransporter-2 (SGLT2) Inhibitors are Recommended to Decrease Hospitalization and Cardiovascular Mortality (see Sodium-Glucose Cotransporter-2 Inhibitors)
In Patients Self-Identified as Black with NYHA Functional Class III-IV Heart Failure with Reduced Ejection Fraction (HFrEF) Who are Receiving Optimal Guideline-Directed Medical Therapy (GDMT), the Combination of Hydralazine and Isosorbide Dinitrate is Recommended to Improve Symptoms and Decrease Morbidity and Mortality (see Hydralazine and Isosorbide)
In Patients with Current or Previous Symptomatic Heart Failure with Reduced Ejection Fraction (HFrEF) Who Cannot Be Given First-Line Agents (Such as Angiotensin Receptor-Neprilysin Inhibitors, Angiotensin Converting Enzyme/ACE Inhibitors or an Angiotensin II Receptor Blockers/ARB) Because of Drug Intolerance or Renal Insufficiency, a Combination of Hydralazine and Isosorbide Dinitrate Might Be Considered to Decrease Morbidity and Mortality
In Adults with Heart Failure with Reduced Ejection Fraction (HFrEF), Non-Dihydropyridine Calcium Channel Blockers (Diltiazem, Verapamil) are Not Recommended in the Treatment of Hypertension (Class of Recommendation: III-No Benefit; Level of Evidence: B-R)
Treatment of Hypertension in the Setting of Heart Failure with Preserved Ejection Fraction (HFpEF)
In Adults with Heart Failure with Preserved Ejection Fraction (HFpEF) Who Present with Symptoms of Volume Overload, Diuretics Should Be Prescribed to Control Hypertension (Class of Recommendation: I; Level of Evidence: C-EO)
In Adults with Heart Failure with Preserved Ejection Fraction (HFpEF) Who and Persistent Hypertension After Management of Volume Overload, Angiotensin Converting (ACE) Inhibitors or Angiotensin II Receptor Blockers (ARB’s) and β-Blockers Titrated to Attain Systolic Blood Pressure of <130 mm Hg Should Be Prescribed (Class of Recommendation: I; Level of Evidence: C-LD)
Treatment of Hypertension in the Setting of Atrial Fibrillation (see Atrial Fibrillation)
Treatment of Hypertension with an Angiotensin II Receptor Blocker (ARB) Can Be Useful for the Prevention of Recurrence of Atrial Fibrillation (Class of Recommendation: IIa; Level of Evidence: B-R)
Treatment of Hypertension in the Setting of Valvular Heart Disease
In Adults with Asymptomatic Aortic Stenosis, Hypertension Should Be Treated with Antihypertensives, Starting at a Low Dose and Gradually Titrating Upward (as Required) (Class of Recommendation: I; Level of Evidence: B-NR)
In Patients with Chronic Aortic Insufficiency, Treatment of Systolic Hypertension with Antihypertensives Which Do Not Slow the Heart Rate (i.e. Avoid β-Blockers) is Reasonable (Class of Recommendation: IIa; Level of Evidence: C-LD)
Recommendations-2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure (Circulation, 2022) [MEDLINE]
Assessment of Patients Hospitalized With Decompensated Heart Failure
In Patient Hospitalized with Heart Failure, Severity of Congestion and Adequacy of Perfusion Should Be Assessed to Guide Triage and Initial Therapy (Class of Recommendation: 1; Level of Evidence: C-LD)
In Patient Hospitalized with Heart Failure, the Common Precipitating Factors and the Overall Patient Trajectory Should Be Assessed to Guide Appropriate Therapy (Class of Recommendation: 1; Level of Evidence: C-LD)
For Patient Admitted with Heart Failure, Treatment Should Address Reversible Factors, Establish Optimal Volume Status, and Advance Guideline-Directed Medical Therapy (GDMT) Toward Targets for Outpatient Therapy (Class of Recommendation: 1; Level of Evidence: C-LD)
Maintenance or Optimization of Guideline-Directed Medical Therapy (GDMT) During Hospitalization
In Patients with HFrEF Requiring Hospitalization, Preexisting Guideline-Directed Medical Therapy (GDMT) Should Be Continued and Optimized to Improve Outcome, Unless Contraindicated (Class of Recommendation: 1; Level of Evidence: B-NR)
In Patients Experiencing a Mild Decrease in Renal Function or Asymptomatic Reduction of Blood Pressure During Heart Failure Hospitalization, Diuresis and Other Guideline-Directed Medical Therapy (GDMT) Should Not Routinely Be Discontinued (Class of Recommendation: 1; Level of Evidence: B-NR)
In Patients with HFrEF, Goal-Directed Medical Therapy (GDMT) Should Be Initiated During Hospitalization After Clinical Stability is Achieved (Class of Recommendation: 1; Level of Evidence: B-NR)
In Patients with HFrEF, if Discontinuation of Guideline-Directed Medical Therapy (GDMT) is Necessary During Hospitalization, it Should Be Reinitiated and Further Optimized as Soon as Possible (Class of Recommendation: 1; Level of Evidence: B-NR)
Use of Diuretics
Patients with Heart Failure Admitted with Significant Fluid Overload Should Be Treated with Intravenous Loop Diuretics to Improve Symptoms and Decrease Morbidity (Class of Recommendation: 1, Level of Evidence: B-NR)
For Patients Hospitalized with Heart Failure, Therapy with Diuretics and Other Guideline-Directed Medications Should Be Titrated with a Goal to Resolve Clinical Evidence of Congestion to Decrease Symptoms and Rehospitalizations (Class of Recommendation: 1; Level of Evidence: B-NR)
For Patients Requiring Diuretic Treatment During Hospitalization for Heart Failure, the Discharge Regimen Should Include a Plan for Adjustment of Diuretics to Decrease Rehospitalizations (Class of Recommendation: 1; Level of Evidence: B-NR)
In Patient Hospitalized with Heart Failure When Diuresis is Inadequate to Relieve Symptoms/Signs of Congestion, Intensify the Diuretic Regimen Using Either Higher Doses of Intravenous Loop Diuretics or Addition of a Second Diuretic (Class of Recommendation: 2a; Level of Evidence: B-NR)
Use of Vasodilators
In Patient Admitted with Decompensated Heart Failure, in the Absence of Systemic Hypotension, Intravenous Nitroglycerin or Nitroprusside May be Considered as an Adjuvant to Diuretic Therapy for Relief of Dyspnea (Class of Recommendation: 2b; Level of Evidence: B-NR)
Recommendations-2025 AHA/ACC/AANP/AAPA/ABC/ACCP/ACPM/AGS/AMA/ASPC/NMA/PCNA/SGIM Guideline for the Prevention, Detection, Evaluation and Management of High Blood Pressure in Adults (Circulation, 2025) [MEDLINE]
Treatment of Hypertension in Patients at Risk for Developing Congestive Heart Failure (CHF)
In Adults with Hypertension, Adjusting Systolic Blood Pressure (SBP) to <130 mm Hg is Recommended to Decrease the Risk of Developing Heart Failure (Class of Recommendation: 1; Level of Evidence: B-R)
In Adults with Hypertension, Adjusting Diastolic Heart Failure (DBP) to <80 mm Hg is Recommended to Decrease the Risk of Developing Heart Failure (Class of Recommendation: 1; Level of Evidence: B-NR)
Hypertensive Emergency in the Setting of Congestive Heart Failure (CHF)
For Adults with a Hypertensive Emergency But without a Compelling Condition (Such as an Acute Aortic Syndrome), Systolic Blood Pressure (SBP) Should Be Decreased with Oral/Parenteral Therapy by ≤25% within the First Hour (Class of Recommendation: 1; Level of Evidence: C-LD)
Then, if Stable, Decreased to Systolic Blood Pressure (SBP <160/100 mm Hg within the Next 2-6 hrs (Class of Recommendation: 1; Level of Evidence: C-LD)
Then Cautiously Decrease to Systolic Blood Pressure (SBP 130-140 mm Hg During the Next 24-48 hrs to Limit Target Organ Injury (Class of Recommendation: 1; Level of Evidence: C-LD)
Treatment of Hypertensive Emergency in the Setting of Acute Coronary Syndrome (ACS) (see Coronary Artery Disease)
Recommendations-2015 American Heart Association (AHA)/American College of Cardiology (ACC)/American Society of Hypertension (ASH) Guideline on Treatment of Hypertension in Those with Coronary Artery Disease (Heart Lung Circ, 2015) [MEDLINE]
Recommended Blood Pressure Target is 140/90
Blood Pressure <130/80 is Recommended at Time of Hospital Discharge
Recommendations-2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults (Circulation, 2018) [MEDLINE]
Treatment of Hypertension in the Setting of Stable Ischemic Heart Disease (see Coronary Artery Disease)
In Adults with Stable Ischemic Heart Disease and Hypertension, a Blood Pressure Target of <130/80 mm Hg is Recommended (Class of Recommendation: I; Level of Evidence: SBP: B-R, DBP: C-EO)
Adults with Stable Ischemic Heart Disease and hypertension (BP ≥130/80 mm Hg) Should Be Treated with Medications (i.e. Goal-Directed Medical Therapy β-Blockers, ACE Inhibitors, or ARB’s) for Compelling indications (eg, previous MI, Stable Angina) as First-Line Therapy, with the Addition of Other Medications (i.e. Dihydropyridine Calcium Channel Blockers, Thiazide Diuretics, and/or Mineralocorticoid Receptor Antagonists) as Required to Further Control Hypertension (Class of Recommendation: I; Level of Evidence: SBP: B-R, DBP: C-EO)
In Adults with Stable Ischemic Heart Disease with Angina and Persistent Uncontrolled Hypertension, the Addition of Dihydropyridine Calcium Channel Blockers to Goal-Directed Medical Therapy β-Blockers is Recommended (Class of Recommendation: I; Level of Evidence: B-NR)
In Adults Who Have Had an Myocardial Infarction/Acute Coronary Syndrome, it is Reasonable to Continue Goal-Directed Medical Therapy β-Blockers Beyond 3 yrs as Long-Term Therapy for Hypertension (Class of Recommendation: IIa; Level of Evidence: B-NR)
β-Blockers and/or Calcium Channel Blockers Might Be Considered to Control Hypertension in Patients with Coronary Artery Disease (without HFrEF) Who Had an Myocardial Infarction >3 yrs Ago and Have Angina (Class of Recommendation: IIb; Level of Evidence: C-EO)
Recommendations-2025 AHA/ACC/AANP/AAPA/ABC/ACCP/ACPM/AGS/AMA/ASPC/NMA/PCNA/SGIM Guideline for the Prevention, Detection, Evaluation and Management of High Blood Pressure in Adults (Circulation, 2025) [MEDLINE]
Hypertensive Emergency in the Setting of Acute Coronary Syndrome (ACS)
For Adults with a Hypertensive Emergency But without a Compelling Condition (Such as an Acute Aortic Syndrome), Systolic Blood Pressure (SBP) Should Be Decreased with Oral/Parenteral Therapy by ≤25% within the First Hour (Class of Recommendation: 1; Level of Evidence: C-LD)
Then, if Stable, Decreased to Systolic Blood Pressure (SBP <160/100 mm Hg within the Next 2-6 hrs (Class of Recommendation: 1; Level of Evidence: C-LD)
Then Cautiously Decrease to Systolic Blood Pressure (SBP 130-140 mm Hg During the Next 24-48 hrs to Limit Target Organ Injury (Class of Recommendation: 1; Level of Evidence: C-LD)
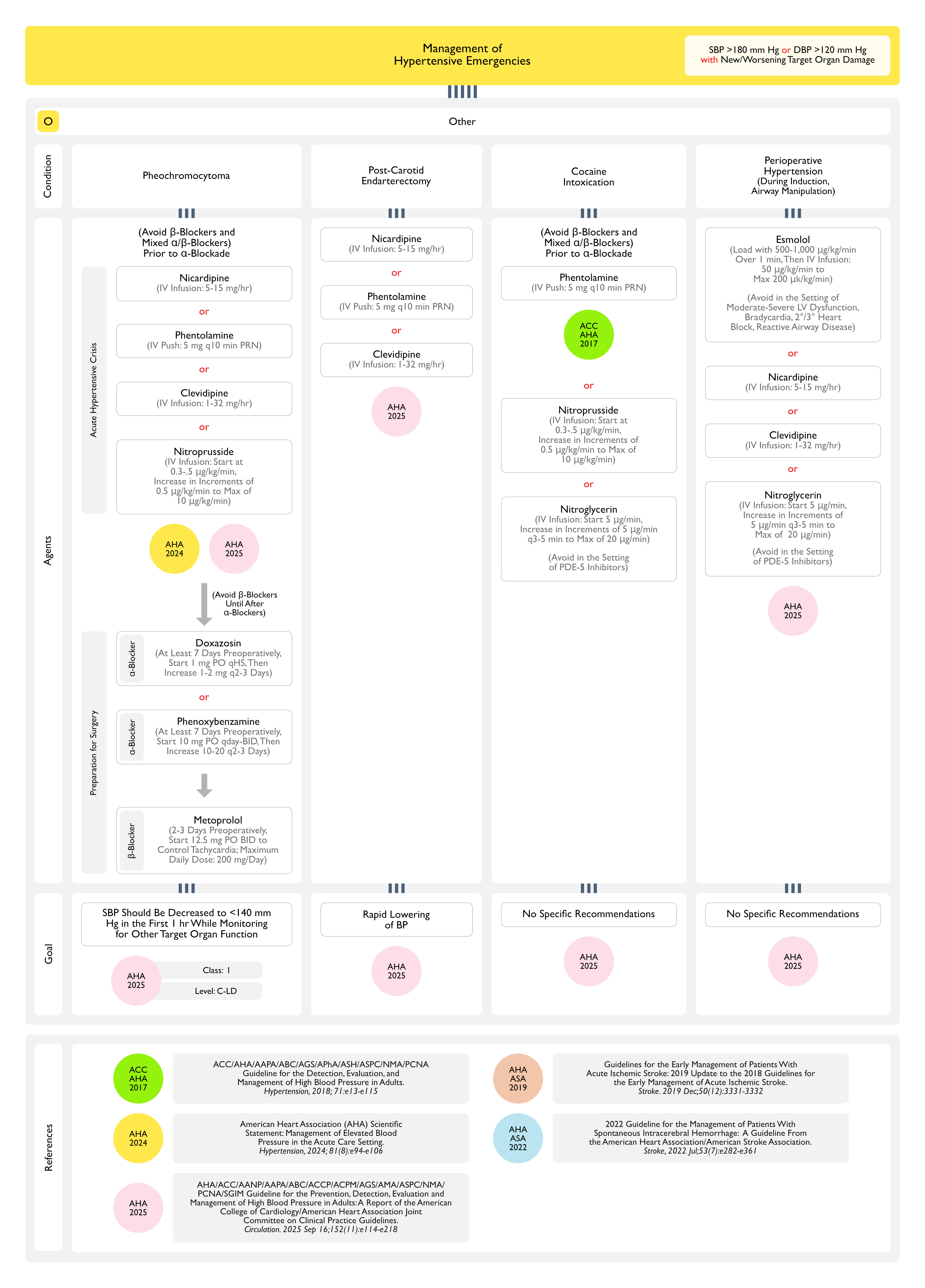
Treatment of Hypertensive Emergency in the Setting of Pheochromocytoma (see Pheochromocytoma)
Recommendations-2025 AHA/ACC/AANP/AAPA/ABC/ACCP/ACPM/AGS/AMA/ASPC/NMA/PCNA/SGIM Guideline for the Prevention, Detection, Evaluation and Management of High Blood Pressure in Adults (Circulation, 2025) [MEDLINE]
Decrease Systolic Blood Pressure to <140 mm Hg in the First 1 hr (Class of Recommendation: 1; Level of Evidence: C-LD)
Despite Potential Cardiovascular Complications of Pheochromocytoma Crisis (Including a Takotsubo-Like Cardiomyopathy), Pheochromocytoma Should Not Be Considered a Compelling Indication to Decrease Systolic Blood Pressure (SBP) Immediately to <120 mm Hg in the First Hour
Clinical Trials in Patients without Aortic Dissection or Pheochromocytoma Demonstrated Increased Risk of Adverse Renal Events Associated with Early Intensive Lowering of Systolic Blood Pressure (SBP) to 110-139 mm Hg, Particularly Among Patients with Extremely High Initial Systolic Blood Pressure (SBP) of >220 mm Hg
Treatment of Hypertensive Emergency in the Setting of Carotid Endarterectomy (CEA) (see Carotid Endarterectomy)
Recommendations-2025 AHA/ACC/AANP/AAPA/ABC/ACCP/ACPM/AGS/AMA/ASPC/NMA/PCNA/SGIM Guideline for the Prevention, Detection, Evaluation and Management of High Blood Pressure in Adults (Circulation, 2025) MEDLINE]
Requires Rapid Decrease in Blood Pressure
Treatment of Hypertensive Emergency in the Setting of Cocaine Intoxication (see Cocaine)
Recommendations-2025 AHA/ACC/AANP/AAPA/ABC/ACCP/ACPM/AGS/AMA/ASPC/NMA/PCNA/SGIM Guideline for the Prevention, Detection, Evaluation and Management of High Blood Pressure in Adults (Circulation, 2025) [MEDLINE]
No Specific Recommendation
Treatment of Hypertensive Emergency in the Setting of Perioperative Hypertension
Definition
Blood Pressure ≥160/90 mm Hg or Systolic Blood Pressure (SBP) Increase ≥20% of the Preoperative Value Which Persists for >15 min
Intraoperative Hypertension is Most Frequently Observed During Anesthesia Induction and Airway Manipulation
Recommendations-2025 AHA/ACC/AANP/AAPA/ABC/ACCP/ACPM/AGS/AMA/ASPC/NMA/PCNA/SGIM Guideline for the Prevention, Detection, Evaluation and Management of High Blood Pressure in Adults (Circulation, 2025) [MEDLINE]
No Specific Recommendation
Antihypertensive Agents for Hypertensive Emergencies (Hypertension, 2018) [MEDLINE]
Particularly Useful for Hypertensive Emergencies Induced by Excess Catecholamine (Pheochromocytoma, Interactions Between Monamine Oxidase Inhibitors and Other Drugs or Food, Cocaine Intoxication, Amphetamine Intoxication, or Clonidine Withdrawal
Intermittent Intravenous Administration
Initial 5 mg Intravenous Push
Repeat 5 mg Doses q10 min (as Required)
Prognosis
XXXXXXXXX
One Year Mortality Rate XXXX
References
Treatment
Pharmacological basis for antihypertensive effects of intravenous labetalol. Br Heart J. 1977;39(1):99 [MEDLINE]
Hypertensive crises: challenges and management. Chest. 2007;131(6);1949-1962. doi: 10.1378/chest.06-2490 [MEDLINE]
Pharmacological management of hypertensive emergencies and urgencies: focus on newer agents. Expert Opin Investig Drugs. 2012;21(8):1089-1106. doi: 10.1517/13543784.2012.693477 [MEDLINE]
Diagnostic and therapeutic approach to the hypertensive crisis. Med Clin (Barc). 2018 Apr 23;150(8):317-322. doi: 10.1016/j.medcli.2017.09.027 [MEDLINE]
Initial Treatment of Hypertension. N Engl J Med. 2018 Feb 15;378(7):636-644. doi: 10.1056/NEJMcp1613481 [MEDLINE]
2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Hypertension. 2018 Jun;71(6):e13-e115. doi: 10.1161/HYP.0000000000000065 [MEDLINE]
ESC Council on hypertension position document on the management of hypertensive emergencies. European Heart Journal – Cardiovascular Pharmacotherapy (2019) 5, 37–46 doi:10.1093/ehjcvp/pvy032 [MEDLINE]
Hypertensive Emergencies: A Review of Common Presentations and Treatment Options. Cardiol Clin. 2019 Aug;37(3):275-286. doi: 10.1016/j.ccl.2019.04.003 [MEDLINE]
Acute severe hypertension. N Engl J Med. 2019;381(19):1843-1852. doi: 10.1056/NEJMcp1901117 [MEDLINE]
Management of hypertensive emergencies: a practical approach. Blood Press. 2021 Aug;30(4):208-219. doi: 10.1080/08037051.2021.1917983 [MEDLINE]
Treatment and outcomes of inpatient hypertension among adults with noncardiac admissions. JAMA Intern Med. 2021;181:345–352. doi: 10.1001/jamainternmed.2020.7501 [MEDLINE]
Omega-3 polyunsaturated fatty acids intake and blood pressure: A dose-response meta-analysis of randomized controlled trials. J Am Heart Assoc. 2022 Jun 7;11(11):e025071. doi: 10.1161/JAHA.121.025071 [MEDLINE]
Feasibility and short-term effects of a multi-component emergency department blood pressure intervention: a pilot randomized trial. J Am Heart Assoc. 2022 Mar;11(5):e024339. doi: 10.1161/JAHA.121.024339 [MEDLINE]
Clinical outcomes of intensive inpatient blood pressure management in hospitalized older adults. JAMA Intern Med. 2023;183:715–723. doi: 10.1001/jamainternmed.2023.1667 [MEDLINE]
Mortality and Morbidity Among Individuals With Hypertension Receiving a Diuretic, ACE Inhibitor, or Calcium Channel Blocker: A Secondary Analysis of a Randomized Clinical Trial. JAMA Netw Open. 2023 Dec 1;6(12):e2344998. doi: 10.1001/jamanetworkopen.2023.44998 [MEDLINE]
The Management of Elevated Blood Pressure in the Acute Care Setting: A Scientific Statement From the American Heart Association. Hypertension. 2024 May 28. doi: 10.1161/HYP.0000000000000238 [MEDLINE]
Impact of hypertension duration on the cardiovascular benefit of intensive blood pressure control. Hypertension. 2024 Sep;81(9):1945-1955. doi: 10.1161/HYPERTENSIONAHA.124.23439 [MEDLINE]