Patients with Stage 2 Hypertension (with Both Office Systolic Blood Pressure/SBP ≥140 mm Hg and Office Diastolic Blood Pressure/DBP ≥90 mm Hg) in Whom Blood Pressure is Not at Goal Despite Taking ≥4 Antihypertensive Medications at Optimal Dosages (Angiotensin Converting Enzyme Inhibitor/ACE-I/Angiotensin II Receptor Blocker/ARB + Calcium Channel Blocker + Thiazide-Type Diuretics + Mineralocorticoid Receptor Antagonist)
Patients with Stage 2 Hypertension (with Both Office Systolic Blood Pressure/SBP ≥140 mm Hg and Office Diastolic Blood Pressure/DBP ≥90 mm Hg) Who are Unable to Take Antihypertensive Medications at the Optimal Dosages or Additional Medications
Recommendations-2025 AHA/ACC/AANP/AAPA/ABC/ACCP/ACPM/AGS/AMA/ASPC/NMA/PCNA/SGIM Guideline for the Prevention, Detection, Evaluation and Management of High Blood Pressure in Adults (Circulation, 2025) MEDLINE]
In Adults with Resistant Hypertension, a More Detailed Evaluation for Secondary Causes (Including Careful Review of All Medications and Removal of Those with Interfering Effects on Blood Pressure) is Beneficial for Lowering Blood Pressure and Simplifying Treatment (Class of Recommendation: 1; Level of Evidence: B-NR)
In Adults with Uncontrolled Resistant Hypertension Despite Optimal Treatment with First-Line Antihypertensives (i.e. a Combination of Angiotensin Converting Enzyme (ACE) Inhibitor or Angiotensin II Receptor Blocker (ARB) Plus Calcium Channel Blocker and Thiazide-Type Diuretic (Chlorthalidone, Indapamide) and with an eGFR of ≥45 mL/min/1.73 m2), Addition of a Mineralocorticoid Receptor Antagonist is Recommended to Control Blood Pressure (Class of Recommendation: 1; Level of Evidence: B-R)
In Adults with Uncontrolled Resistant Hypertension Who Cannot Tolerate or Have Contraindications to Mineralocorticoid Receptor Antagonists, the Addition of One of the Following Agents or Classes (Amiloride, β-Blockers, α-Blockers, Central Sympatholytic Medications, Dual Endothelin Receptor Antagonists, or Direct Vasodilators) is Reasonable to Control Blood Pressure (Class of Recommendation: 2a; Level of Evidence: B-NR)
In Carefully Selected Patients with Systolic and Diastolic Hypertension (Office Systolic Blood Pressure/SBP 140-180 mm Hg and Diastolic Blood Pressure/DBP ≥90 mm Hg) and eGFR ≥40 mL/min/1.73 m2 Who Have Resistant Hypertension Despite Optimal Treatment, or Intolerable Side Effects to Additional Antihypertensives, Renal Denervation May Be Reasonable as an Adjunct Treatment toAntihypertensives and Lifestyle Modification to Decrease Blood Pressure (Class of Recommendation: 2b; Level of Evidence: B-R)
All Patients with Hypertension Who are Being Considered for Renal Denervation Should Be Evaluated by a Multidisciplinary Team with Expertise in Resistant Hypertension and Renal Denervation (Class of Recommendation: 1; Level of Evidence: B-NR)
For Patients with Hypertension for Whom Renal Denervation is Contemplated, the Benefits of Lowering Blood Pressure and Potential Procedural Risks Compared with Continuing Medical Therapy Should Be Discussed as Part of a Shared Decision-Making Process to Ensure Patients Choose the Therapy Which Meets Their Preference (Class of Recommendation: 1; Level of Evidence: C-EO)
Management of Hypertension in the Setting of Heart Disease
Recommendations-2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults (Circulation, 2018) [MEDLINE]
Treatment of Hypertension in the Setting of Stable Ischemic Heart Disease (see Coronary Artery Disease)
In Adults with Stable Ischemic Heart Disease and Hypertension, a Blood Pressure Target of <130/80 mm Hg is Recommended (Class of Recommendation: I; Level of Evidence: SBP: B-R, DBP: C-EO)
Adults with Stable Ischemic Heart Disease and hypertension (BP ≥130/80 mm Hg) Should Be Treated with Medications (i.e. Goal-Directed Medical Therapy β-Blockers, ACE Inhibitors, or ARB’s) for Compelling indications (eg, previous MI, Stable Angina) as First-Line Therapy, with the Addition of Other Medications (i.e. Dihydropyridine Calcium Channel Blockers, Thiazide Diuretics, and/or Mineralocorticoid Receptor Antagonists) as Required to Further Control Hypertension (Class of Recommendation: I; Level of Evidence: SBP: B-R, DBP: C-EO)
In Adults with Stable Ischemic Heart Disease with Angina and Persistent Uncontrolled Hypertension, the Addition of Dihydropyridine Calcium Channel Blockers to Goal-Directed Medical Therapy β-Blockers is Recommended (Class of Recommendation: I; Level of Evidence: B-NR)
In Adults Who Have Had an Myocardial Infarction/Acute Coronary Syndrome, it is Reasonable to Continue Goal-Directed Medical Therapy β-Blockers Beyond 3 yrs as Long-Term Therapy for Hypertension (Class of Recommendation: IIa; Level of Evidence: B-NR)
β-Blockers and/or Calcium Channel Blockers Might Be Considered to Control Hypertension in Patients with Coronary Artery Disease (without HFrEF) Who Had an Myocardial Infarction >3 yrs Ago and Have Angina (Class of Recommendation: IIb; Level of Evidence: C-EO)
Treatment of Hypertension in Patients at Risk for Developing Congestive Heart Failure (CHF)
In Adults with Hypertension, Adjusting Systolic Blood Pressure (SBP) to <130 mm Hg is Recommended to Decrease the Risk of Developing Heart Failure (Class of Recommendation: I; Level of Evidence: B-R)
In Adults with Hypertension, Adjusting Diastolic Heart Failure (DBP) to <80 mm Hg is Recommended to Decrease the Risk of Developing Heart Failure (Class of Recommendation: I; Level of Evidence: C-EO)
Treatment of Hypertension in the Setting of Heart Failure with Reduced Ejection Fraction (HFrEF)
Adults with Heart Failure with Reduced Ejection Fraction (HFrEF) and Hypertension Should Be Prescribed Guideline-Directed Medical Therapy (GDMT) Titrated to Attain a Blood Pressure <130/80 mm Hg (Class of Recommendation: I; Level of Evidence: C-EO)
In Patients with Heart Failure with Reduced Ejection Fraction (HFrEF) (Even if Asymptomatic) Use One of the Three β-Blockers Proven to Reduce Mortality and Hospitalizations
In Patients with Symptomatic Heart Failure with Reduced Ejection Fraction (HFrEF) and eGFR is >30 mL/min/1.73 m2 with Potassium is <5.0 mEq/L, Spironolactone or Eplerenone is Recommended to Reduce Morbidity and Mortality (see Spironolactone and Eplerenone)
In Patients with Heart Failure with Reduced Ejection Fraction (HFrEF) and NYHA Functional Class II-III Symptoms, An Angiotensin Receptor-Neprilysin Inhibitor is Recommended to Decrease Morbidity and Mortality (see Sacubitril/Valsartan)
When the Use of an Angiotensin Receptor-Neprilysin Inhibitor is Not Feasible, an Angiotensin Converting Enzyme (ACE) Inhibitor or an Angiotensin II Receptor Blocker (ARB) is Recommended to Decrease Morbidity and Mortality (see Angiotensin Converting Enzyme Inhibitors and Angiotensin II Receptor Blockers)
In Patients with Symptomatic Heart Failure with Reduced Ejection Fraction (HFrEF) (Irrespective of the Presence of Type 2 Diabetes Mellitus), Sodium-Glucose Cotransporter-2 (SGLT2) Inhibitors are Recommended to Decrease Hospitalization and Cardiovascular Mortality (see Sodium-Glucose Cotransporter-2 Inhibitors)
In Patients Self-Identified as Black with NYHA Functional Class III-IV Heart Failure with Reduced Ejection Fraction (HFrEF) Who are Receiving Optimal Guideline-Directed Medical Therapy (GDMT), the Combination of Hydralazine and Isosorbide Dinitrate is Recommended to Improve Symptoms and Decrease Morbidity and Mortality (see Hydralazine and Isosorbide)
In Patients with Current or Previous Symptomatic Heart Failure with Reduced Ejection Fraction (HFrEF) Who Cannot Be Given First-Line Agents (Such as Angiotensin Receptor-Neprilysin Inhibitors, Angiotensin Converting Enzyme/ACE Inhibitors or an Angiotensin II Receptor Blockers/ARB) Because of Drug Intolerance or Renal Insufficiency, a Combination of Hydralazine and Isosorbide Dinitrate Might Be Considered to Decrease Morbidity and Mortality
In Adults with Heart Failure with Reduced Ejection Fraction (HFrEF), Non-Dihydropyridine Calcium Channel Blockers (Diltiazem, Verapamil) are Not Recommended in the Treatment of Hypertension (Class of Recommendation: III-No Benefit; Level of Evidence: B-R)
Treatment of Hypertension in the Setting of Heart Failure with Preserved Ejection Fraction (HFpEF)
In Adults with Heart Failure with Preserved Ejection Fraction (HFpEF) Who Present with Symptoms of Volume Overload, Diuretics Should Be Prescribed to Control Hypertension (Class of Recommendation: I; Level of Evidence: C-EO)
In Adults with Heart Failure with Preserved Ejection Fraction (HFpEF) Who and Persistent Hypertension After Management of Volume Overload, Angiotensin Converting (ACE) Inhibitors or Angiotensin II Receptor Blockers (ARB’s) and β-Blockers Titrated to Attain Systolic Blood Pressure of <130 mm Hg Should Be Prescribed (Class of Recommendation: I; Level of Evidence: C-LD)
Treatment of Hypertension in the Setting of Atrial Fibrillation (see Atrial Fibrillation)
Treatment of Hypertension with an Angiotensin II Receptor Blocker (ARB) Can Be Useful for the Prevention of Recurrence of Atrial Fibrillation (Class of Recommendation: IIa; Level of Evidence: B-R)
Treatment of Hypertension in the Setting of Valvular Heart Disease
In Adults with Asymptomatic Aortic Stenosis, Hypertension Should Be Treated with Antihypertensives, Starting at a Low Dose and Gradually Titrating Upward (as Required) (Class of Recommendation: I; Level of Evidence: B-NR)
In Patients with Chronic Aortic Insufficiency, Treatment of Systolic Hypertension with Antihypertensives Which Do Not Slow the Heart Rate (i.e. Avoid β-Blockers) is Reasonable (Class of Recommendation: IIa; Level of Evidence: C-LD)
Recommendations-2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure (Circulation, 2022) [MEDLINE]
Assessment of Patients Hospitalized With Decompensated Heart Failure
In Patient Hospitalized with Heart Failure, Severity of Congestion and Adequacy of Perfusion Should Be Assessed to Guide Triage and Initial Therapy (Class of Recommendation: 1; Level of Evidence: C-LD)
In Patient Hospitalized with Heart Failure, the Common Precipitating Factors and the Overall Patient Trajectory Should Be Assessed to Guide Appropriate Therapy (Class of Recommendation: 1; Level of Evidence: C-LD)
For Patient Admitted with Heart Failure, Treatment Should Address Reversible Factors, Establish Optimal Volume Status, and Advance Guideline-Directed Medical Therapy (GDMT) Toward Targets for Outpatient Therapy (Class of Recommendation: 1; Level of Evidence: C-LD)
Maintenance or Optimization of Guideline-Directed Medical Therapy (GDMT) During Hospitalization
In Patients with HFrEF Requiring Hospitalization, Preexisting Guideline-Directed Medical Therapy (GDMT) Should Be Continued and Optimized to Improve Outcome, Unless Contraindicated (Class of Recommendation: 1; Level of Evidence: B-NR)
In Patients Experiencing a Mild Decrease in Renal Function or Asymptomatic Reduction of Blood Pressure During Heart Failure Hospitalization, Diuresis and Other Guideline-Directed Medical Therapy (GDMT) Should Not Routinely Be Discontinued (Class of Recommendation: 1; Level of Evidence: B-NR)
In Patients with HFrEF, Goal-Directed Medical Therapy (GDMT) Should Be Initiated During Hospitalization After Clinical Stability is Achieved (Class of Recommendation: 1; Level of Evidence: B-NR)
In Patients with HFrEF, if Discontinuation of Guideline-Directed Medical Therapy (GDMT) is Necessary During Hospitalization, it Should Be Reinitiated and Further Optimized as Soon as Possible (Class of Recommendation: 1; Level of Evidence: B-NR)
Use of Diuretics
Patients with Heart Failure Admitted with Significant Fluid Overload Should Be Treated with Intravenous Loop Diuretics to Improve Symptoms and Decrease Morbidity (Class of Recommendation: 1, Level of Evidence: B-NR)
For Patients Hospitalized with Heart Failure, Therapy with Diuretics and Other Guideline-Directed Medications Should Be Titrated with a Goal to Resolve Clinical Evidence of Congestion to Decrease Symptoms and Rehospitalizations (Class of Recommendation: 1; Level of Evidence: B-NR)
For Patients Requiring Diuretic Treatment During Hospitalization for Heart Failure, the Discharge Regimen Should Include a Plan for Adjustment of Diuretics to Decrease Rehospitalizations (Class of Recommendation: 1; Level of Evidence: B-NR)
In Patient Hospitalized with Heart Failure When Diuresis is Inadequate to Relieve Symptoms/Signs of Congestion, Intensify the Diuretic Regimen Using Either Higher Doses of Intravenous Loop Diuretics or Addition of a Second Diuretic (Class of Recommendation: 2a; Level of Evidence: B-NR)
Use of Vasodilators
In Patient Admitted with Decompensated Heart Failure, in the Absence of Systemic Hypotension, Intravenous Nitroglycerin or Nitroprusside May be Considered as an Adjuvant to Diuretic Therapy for Relief of Dyspnea (Class of Recommendation: 2b; Level of Evidence: B-NR)
Recommendations-2025 AHA/ACC/AANP/AAPA/ABC/ACCP/ACPM/AGS/AMA/ASPC/NMA/PCNA/SGIM Guideline for the Prevention, Detection, Evaluation and Management of High Blood Pressure in Adults (Circulation, 2025) [MEDLINE]
Treatment of Hypertension in Patients at Risk for Developing Congestive Heart Failure (CHF)
In Adults with Hypertension, Adjusting Systolic Blood Pressure (SBP) to <130 mm Hg is Recommended to Decrease the Risk of Developing Heart Failure (Class of Recommendation: 1; Level of Evidence: B-R)
In Adults with Hypertension, Adjusting Diastolic Heart Failure (DBP) to <80 mm Hg is Recommended to Decrease the Risk of Developing Heart Failure (Class of Recommendation: 1; Level of Evidence: B-NR)
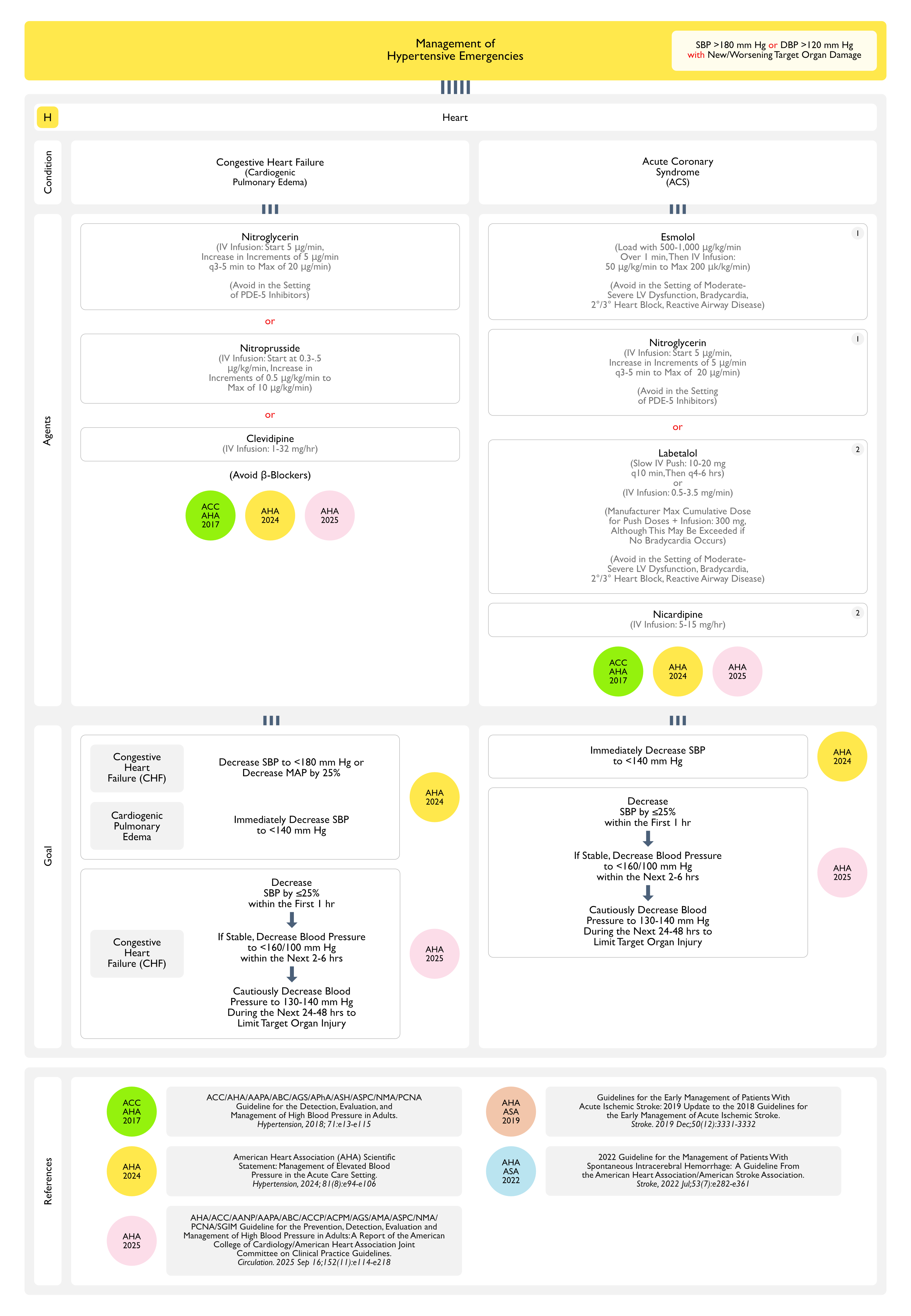
Hypertensive Emergency in the Setting of Congestive Heart Failure (CHF)
For Adults with a Hypertensive Emergency But without a Compelling Condition (Such as an Acute Aortic Syndrome), Systolic Blood Pressure (SBP) Should Be Decreased with Oral/Parenteral Therapy by ≤25% within the First Hour (Class of Recommendation: 1; Level of Evidence: C-LD)
Then, if Stable, Decreased to Systolic Blood Pressure (SBP <160/100 mm Hg within the Next 2-6 hrs (Class of Recommendation: 1; Level of Evidence: C-LD)
Then Cautiously Decrease to Systolic Blood Pressure (SBP 130-140 mm Hg During the Next 24-48 hrs to Limit Target Organ Injury (Class of Recommendation: 1; Level of Evidence: C-LD)
Management of Hypertension in the Setting of Obesity/Metabolic Syndrome (see Obesity)
Recommendations-2025 AHA/ACC/AANP/AAPA/ABC/ACCP/ACPM/AGS/AMA/ASPC/NMA/PCNA/SGIM Guideline for the Prevention, Detection, Evaluation and Management of High Blood Pressure in Adults (Circulation, 2025) MEDLINE]
In Adults with Hypertension Who are Overweight/Obese (with a BMI ≥27 kg/m2), Incretin Mimetics (eg, GLP-1 Receptor Agonists) When Used for Weight Management May Be Effective as an Adjunct to Lower Blood Pressure (Class of Recommendation: 2b; Level of Evidence: B-R)
In Adults with Hypertension Who are Obese (with a BMI ≥35.0 kg/m2), Bariatric Surgery (When Considered for Weight Loss) in Combination with Behavioral Interventions and Antihypertensives May Be Effective at Lowering Blood Pressure (Class of Recommendation: 2b; Level of Evidence: B-R)
Management of Hypertension in the Setting of Obstructive Sleep Apnea (OSA) (see Obstructive Sleep Apnea)
Recommendations-2025 AHA/ACC/AANP/AAPA/ABC/ACCP/ACPM/AGS/AMA/ASPC/NMA/PCNA/SGIM Guideline for the Prevention, Detection, Evaluation and Management of High Blood Pressure in Adults (Circulation, 2025) MEDLINE]
In Adults with Hypertension and Obstructive Sleep Apnea (OSA) Who are Overweight/Obese, Weight Loss Interventions When Combined with Continuous Positive Airway Pressure (CPAP) Treatment Can Be Effective in Reducing Systolic Blood Pressure (Class of Recommendation: 2a, Level of Evidence: B-R)
In Adults with Resistant Hypertension and Moderate-to-Severe Obstructive Sleep Apnea (OSA), Continued Positive Airway Pressure (CPAP) Treatment Can Be Useful in Reducing Blood Pressure (Class of Recommendation: 2a, Level of Evidence: B-R)
Management of Hypertension in the Setting of Diabetes Mellitus (DM) (see Diabetes Mellitus)
Recommendations-2025 AHA/ACC/AANP/AAPA/ABC/ACCP/ACPM/AGS/AMA/ASPC/NMA/PCNA/SGIM Guideline for the Prevention, Detection, Evaluation and Management of High Blood Pressure in Adults (Circulation, 2025) MEDLINE]
In adults with Type 2 Diabetes Mellitus and Hypertension, Antihypertensive Treatment Should Be Initiated at a Systolic Blood Pressure (SBP) of ≥130 mm Hg with a Treatment Goal of <130 mm Hg, with Encouragement to Achieve an Systolic Blood Pressure (SBP) <120 mm Hg to Reduce Cardiovascular Disease Morbidity and Mortality (Class of Recommendation: I; Level of Evidence: A)
In Adults with Type 2 Diabetes Mellitus and Hypertension, Antihypertensive Treatment Should Be Initiated at a Diastolic Blood Pressure (DBP) of ≥80 mm Hg with a Treatment Goal of <80 mm Hg to Reduce Cardiovascular Disease Morbidity and Mortality (Class of Recommendation: I; Level of Evidence: C-LD)
In Adults with Type 2 Diabetes Mellitus and Hypertension, All First-Line Classes of Antihypertensives (i.e. Thiazide-Type Diuretics, Long-Acting Calcium Channel Blockers, Angiotensin Converting Enzyme Inhibitors, and Angiotensin II Receptor Blockers/ARB’s) are Useful and Effective for Blood Pressure Lowering (Class of Recommendation: I; Level of Evidence: A)
In Adults with Diabetes and Hypertension, Angiotensin Converting Enzyme (ACE) Inhibitors or Angiotensin II Receptor Blockers (ARB’s) are Recommended in the Presence of Chronic Kidney Disease (CKD) as Identified by eGFR <60 mL/min/1.73 m2 or Albuminuria ≥30 mg/g and Should Be Considered When Mild Albuminuria (<30 mg/g) is Present to Delay Progression of Diabetes-Related Kidney Disease (Class of Recommendation: I; Level of Evidence: A)
Management of Hypertension in the Setting of Pregnancy (see Pregnancy)
Antihypertensives in Pregnancy
Recommendations-2025 AHA/ACC/AANP/AAPA/ABC/ACCP/ACPM/AGS/AMA/ASPC/NMA/PCNA/SGIM Guideline for the Prevention, Detection, Evaluation and Management of High Blood Pressure in Adults (Circulation, 2025) MEDLINE]
For Females with Hypertension Who are Planning a Pregnancy or Who Become Pregnant, Labetalol and Extended-Release Nifedipine are Preferred Agents to Treat Hypertension and Minimize Fetal Risk (Class of Recommendation: I; Level of Evidence: A)
Females with Hypertension Who are Planning a Pregnancy or Who Become Pregnant Should Be Counseled About the Benefits of Low-Dose Aspirin (81 mg/day) to Reduce the Risk of Preeclampsia and its Sequelae (Class of Recommendation: I; Level of Evidence: B-R)
Pregnant Females with Systolic Blood Pressure (SBP) ≥160 mm Hg or Diastolic Blood Pressure (DBP) ≥110 mm Hg Confirmed on Repeat Measurement within 15 min Should Receive Antihypertensives to Lower Blood Pressure to <160/<110 mm Hg within 30-60 min to Prevent Adverse Events (Class of Recommendation: I; Level of Evidence: B-R)
Pregnant Females with Chronic Hypertension (Defined as Pre-Pregnancy Hypertension or Systolic Blood Pressure (SBP) 140-159 mm Hg and/or Diastolic Blood Pressure (DBP) 90-109 mm Hg Prior to 20 wks Gestation) Should Receive Antihypertensive Therapy to Achieve Blood Pressure <140/90 mm Hg to Prevent Maternal and Perinatal Morbidity and Mortality (Class of Recommendation: I; Level of Evidence: B-R)
Females with Hypertension Who are Planning a Pregnancy or Who Become Pregnant Should Not Be Treated with Atenolol, Angiotensin Converting Enzyme (ACE) Inhibitors, Angiotensin II Receptor Blockers (ARB’s), Direct Renin Inhibitors, Nitroprusside, or Mineralocorticoid Receptor Antagonists to Avoid Fetal Harm (Class of Recommendation: 3 = Harm; Level of Evidence: C-LD)
Management of Hypertension with Respect to Racial/Ethnic and Age-Related Differences
Recommendations-2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults (Circulation, 2018) [MEDLINE]
Racial/Ethnic Differences in Hypertension Treatment
In Black Adults with Hypertension But without Congestive Heart Failure or Chronic Kidney Disease, Including those with Diabetes Mellitus, Initial Antihypertensives Should Include a Thiazide-Type Diuretic or Calcium Channel Blocker (Class of Recommendation: I; Level of Evidence: B-R)
Two or More Antihypertensives are Recommended to Achieve a Blood Pressure Target of <130/80 mm Hg in Most Adults with Hypertension, Especially in Black Adults with Hypertension (Class of Recommendation: I; Level of Evidence: C-LD)
Age-Related Issues in Hypertension Treatment
Treatment of Hypertension with a Systolic Blood Pressure Treatment Goal of <130 mm Hg is Recommended for Noninstitutionalized Ambulatory Community-Dwelling Adults (≥65 y/o) with an Average Systolic Blood Pressure of ≥130 mm Hg (Class of Recommendation: I; Level of Evidence: A)
For Older Adults (≥65 y/o) with Hypertension and a High Burden of Comorbidity and Limited Life Expectancy, Clinical judgment, patient preference, and a team-based approach to assess Risk/Benefit is Reasonable for Decisions Regarding Intensity of Blood Pressure Lowering and Choice of Antihypertensives (Class of Recommendation: IIa; Level of Evidence: C-EO)
Management of Hypertension in the Setting of a Patient Undergoing a Surgical Procedure
Recommendations-2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults (Circulation, 2018) [MEDLINE]
Intraoperative
Patients with intraoperative Hypertension Should Be Managed with Intravenous medications (Table 19) Until Such Time as Oral Medications Can Be Resumed (Class of Recommendation: I; Level of Evidence: C-EO)
Recommendations-2025 AHA/ACC/AANP/AAPA/ABC/ACCP/ACPM/AGS/AMA/ASPC/NMA/PCNA/SGIM Guideline for the Prevention, Detection, Evaluation and Management of High Blood Pressure in Adults (Circulation, 2025) MEDLINE]
Preoperative
In Patients with Hypertension Scheduled for Major Surgery Who Have Been on Chronic β-Blockers, β-Blockers Should Be Continued Throughout the Perioperative Period to Assist with Blood Pressure Control (Class of Recommendation: 1; Level of Evidence: B-NR)
In Patients with Hypertension Scheduled for Elective Major Surgery, it is Reasonable to Continue Most Medications for Hypertension Throughout the Perioperative Period (Class of Recommendation: 2a; Level of Evidence: C-EO)
In Patients with Hypertension Scheduled for Major Surgery, Discontinuation of Angiotensin Converting Enzyme (ACE) Inhibitors or Angiotensin II Receptor Blockers (ARB’s) Preoperatively May Be Considered to Prevent Hypotension During Surgery (Class of Recommendation: 2b; Level of Evidence: B-NR)
In Patients with Hypertension Scheduled for Elective Major Surgery with Systolic Blood Pressure (SBP) ≥180 mm Hg or Diastolic Blood Pressure (DBP) ≥110 mm Hg, Deferring Surgery May Be Considered (Especially in High-Risk Patients) Minimize Perioperative Complications (Class of Recommendation: 2b; Level of Evidence: C-LD)
In Patients with Hypertension Scheduled for Surgery, Abrupt Preoperative Discontinuation of β-Blockers or Clonidine May Result in Rebound Hypertension and is Potentially Harmful (Class of Recommendation: 3-Harm; Level of Evidence: B-NR)
For Patients with Hypertension Scheduled for Surgery, β-Blockers Should Not Be Started on the Day of Surgery in β-Blocker-Naïve Patients Because of Increased Risk of Postoperative Mrtality (Class of Recommendation: 3-Harm; Level of Evidence: B-R)
Management of Orthostatic Hypotension
Recommendations-2025 AHA/ACC/AANP/AAPA/ABC/ACCP/ACPM/AGS/AMA/ASPC/NMA/PCNA/SGIM Guideline for the Prevention, Detection, Evaluation and Management of High Blood Pressure in Adults (Circulation, 2025) MEDLINE]
In Adults with Hypertension, Improved Blood Pressure Control is Recommended to Decrease the Risk for Orthostatic Hypotension (Class of Recommendation: I, Level of Evidence: A)
In Adults Receiving Intensive Blood Pressure-Lowering Therapy with Asymptomatic Orthostatic Hypotension, Treatment with a Goal of Systolic Blood Pressure <130 mm Hg is Reasonable Due to Increased Cardiovascular Disease and Mortality Benefit (Class of Recommendation: 2a, Level of Evidence: A)
In Adults with Hypertension Initiating Treatment or Adding Medication with a Goal of SBP <130 mm Hg, Assessment for Symptomatic Orthostatic Hypotension is Reasonable to Detect Other Chronic Conditions (Class of Recommendation: 2a, Level of Evidence: B-R)
Treatment of Asymptomatic Elevated Inpatient Blood Pressure
Rationale
Blood Pressure May Take Several Days-Weeks to Adjust to an Antihypertensive Medication Change
Therefore, a Typical Inpatient Stay is Unlikely to Be Sufficient to Fully Assess the Effect of a Single Antihypertensive Medication Change,
Close Outpatient Follow-Up is Required
Clinical Efficacy
Although There are No Randomized Trials Studying the Treatment of Asymptomatic Elevated Inpatient Blood Pressure, Observational Studies Suggest that Pharmacologic Blood Pressure Treatment May Carry Risks in This Setting
Study of Treatment of Inpatient Hypertension in Adults Hospitalized for Non-Cardiac Diagnoses (JAMA Intern Med, 2021) [MEDLINE]: n = 22, 834
In a Propensity-Matched Sample Controlling for Patient and Blood Pressure Characteristics, Treated Patients Had Higher Rates of Subsequent Acute Kidney Injury (10.3% vs 7.9%; P < 0.001) and Myocardial Injury (1.2% vs 0.6%; P = 0.003)
Retrospective Cohort Study of Use of PRN Intravenous Antihypertensives in Severe Inpatient Hypertension (J Clin Hypertens-Greenwich, 2022) [MEDLINE]: n = 22,000
Patients Treated with Intravenous Antihypertensives were 40% More Likely to Have a ≥30% Reduction in Mean Arterial Pressure
Intravenous Antihypertensive Treatment was Associated with a 60% Greater Risk of Myocardial Injury
VA Retrospective Cohort Study of Inpatient Blood Pressure Management in Patients >65 y/o Hospitalized for Non-Cardiac Diagnoses (JAMA Intern Med, 2023) [MEDLINE]: n = 66,140
Primary Outcome was a Composite of Inpatient Mortality, Intensive Care Unit Transfer, Stroke, Acute Kidney Injury, B-Natriuretic Peptide Elevation, and Troponin Elevation
Intensive Blood Pressure Treatment was Associated with an Increased Risk of the Primary Composite Outcome (8.7% vs 6.9%); Weighted Odds Ratio 1.28; 95% CI: 1.18-1.39)
Highest Risk was in Patients Who Received Intravenous Antihypertensives (Weighted Odds Ratio 1.90; 95% CI: 1.65-2.19)
Intensively-Treated Patients were More Likely to Experience Each Component of the Composite Outcome Except for Stroke and Mortality
Findings were Consistent Across Subgroups Stratified by Age, Frailty, Preadmission Blood Pressure, Early Hospitalization Blood Pressure, and History of Cardiovascular Disease
Recommendations
Recommendations-2025 AHA/ACC/AANP/AAPA/ABC/ACCP/ACPM/AGS/AMA/ASPC/NMA/PCNA/SGIM Guideline for the Prevention, Detection, Evaluation and Management of High Blood Pressure in Adults (Circulation, 2025) MEDLINE]
Inpatients with Severe Hypertension
For Adults with Severe Hypertension (Blood Pressure >180/120 mm Hg) Who are Hospitalized for Non-Cardiac Conditions without Evidence of Acute Target Organ Damage, Intermittent Use of Additional Oral/Intravenous Antihypertensive Medications is Not Recommended to Acutely Decrease Blood Pressure (Class of Recommendation: 3 = Harm; Level of Evidence: B-NR)
Treatment of Hypertensive Emergency
General Comments
Intensive Care Unit (ICU) Admission for for Hypertensive Urgency/Emergency
Recommendations-2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults (Hypertension, 2018) [MEDLINE]
In Adults with Hypertensive Emergency, Intensive Care Unit (ICU) Admission is Recommended for Continuous Blood Pressure Monitoring, Monitoring for Target Organ Damage, and Intravenous Antihypertensive Administration (Class of Recommendation: 1; Level of Evidence: B-NR)
Recommendations-2025 AHA/ACC/AANP/AAPA/ABC/ACCP/ACPM/AGS/AMA/ASPC/NMA/PCNA/SGIM Guideline for the Prevention, Detection, Evaluation and Management of High Blood Pressure in Adults (Circulation, 2025) MEDLINE]
In Adults with Hypertensive Emergency (Systolic Blood Pressure >180 and/or Diastolic Blood Pressure >120 mm Hg and Evidence of Acute Target Organ Damage), Admission to an Intensive Care Unit is Recommended for Continuous Monitoring of Blood Pressure and Target Organ Damage and for Consideration of Parenteral Administration of Appropriate Therapy (Class of Recommendation: 1; Level of Evidence: B-NR)
Treatment of Hypertensive Emergency in the Setting of Hypertensive Encephalopathy (see Hypertensive Encephalopathy) (Hypertension, 2024) [MEDLINE]
Recommendations-2025 AHA/ACC/AANP/AAPA/ABC/ACCP/ACPM/AGS/AMA/ASPC/NMA/PCNA/SGIM Guideline for the Prevention, Detection, Evaluation and Management of High Blood Pressure in Adults (Circulation, 2025) [MEDLINE]
For Adults with a Hypertensive Emergency But without a Compelling Condition (Such as an Acute Aortic Syndrome), Systolic Blood Pressure (SBP) Should Be Decreased with Oral/Parenteral Therapy by ≤25% within the First Hour (Class of Recommendation: 1; Level of Evidence: C-LD)
Then, if Stable, Decrease Blood Pressure to <160/100 mm Hg within the Next 2-6 hrs (Class of Recommendation: 1; Level of Evidence: C-LD)
Then Cautiously Decrease Blood Pressure to 130-140 mm Hg During the Next 24-48 hrs to Limit Target Organ Injury (Class of Recommendation: 1; Level of Evidence: C-LD)
Treatment of Hypertensive Emergency in the Setting of Ischemic Cerebrovascular Accident (CVA) (see Ischemic Cerebrovascular Accident)
Recommendations-American Heart Association (AHA)/American Stroke Association (ASA) Guidelines for the Early Management of Patients with Acute Ischemic Stroke (Stroke, 2013) [MEDLINE]
Blood Pressure Management in the Setting of Thrombolytic Therapy
Antihypertensive Options in a Patient Otherwise Eligible for Acute Reperfusion Therapy, Except that Blood Pressure is >185/110 mm Hg
Labetalol 10–20 mg IV Over 1–2 min (May Repeat x 1) (see Labetalol)
Nicardipine 5 mg/h IV Infusion, Titrate Up by 2.5 mg/hr q5–15 min (Maximum: 15 mg/hr) (see Nicardipine)
When Desired Blood Pressure is Reached, Adjust to Maintain Proper Blood Pressure Limits
If Blood Pressure is Not Maintained at ≤185/110 mm Hg, Do Not Administer Thrombolytic Therapy
Management of Blood Pressure During and After Thrombolytic Therapy or Other Acute Reperfusion Therapy to Maintain Blood Pressure ≤180/105 mm Hg
Monitor Blood Pressure q15 min x 2 hrs from the Start of Thrombolytic Therapy, then q30 min x 6 hrs, and then q1hr x 16 hrs
Antihypertensive Options if Systolic Blood Pressure >180–230 mm Hg or Diastolic Blood Pressure >105–120 mm Hg
Labetalol 10 mg IV, Followed by Continuous IV Infusion 2–8 mg/min (see Labetalol)
Nicardipine 5 mg/h IV Infusion, Titrate Up to Desired Effect by 2.5 mg/hr q5–15 min (Maximum: 15 mg/hr) (see Nicardipine)
If Blood Pressure is Not Controlled or Diastolic Blood Pressure is >140 mm Hg, Consider Nitroprusside IV Infusion (see Nitroprusside)
Recommendations-2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults (Circulation, 2018) [MEDLINE]
During the Acute Management of Ischemic Stroke
Starting or Restarting Antihypertensive Therapy During Hospitalization in Patients with Blood Pressure >140/90 mm Hg Who are Neurologically Stable is Safe and Reasonable to Improve Long-Term Blood Pressure Control, Unless Contraindicated (Class of Recommendation: IIa; Level of Evidence: B-NR)
Intravenous Thrombolytic Treatment
Adults with Acute Ischemic Stroke and Elevated Blood Pressure Who are Eligible for Treatment with Intravenous Thrombolytic Should Have Their Blood Pressure Slowly Decreased to <185/110 mm Hg Before Thrombolytic Therapy is Initiated (Class of Recommendation: I; Level of Evidence: B-NR)
In Adults with an Acute Ischemic Stroke, Blood Pressure Should Be <185/110 mm Hg Before Administration of Intravenous Thrombolytic and Should Be Maintained <180/105 mm Hg for at Least the First 24 hrs After Initiating Thrombolytic Drug Therapy (Class of Recommendation: I; Level of Evidence: B-NR)
No Intravenous Thrombolytic or Endovascular Treatment
In Patients with Blood Pressure ≥220/120 mm Hg Who Did Not Receive Intravenous Thrombolytic or Endovascular Treatment and Have No Comorbid Conditions Requiring Acute Antihypertensive Treatment, the Benefit of Initiating or Reinitiating Treatment of Hypertension within the First 48-72 hrs is Uncertain (Class of Recommendation: IIb; Level of Evidence: C-EO)
It Might Reasonable to Decrease Blood Pressure Blood Pressure by 15% During the First 24 hrs After Onset of Stroke
In Patients with Blood Pressure <220/120 mm Hg Who Did Not Receive Intravenous Thrombolytic or Endovascular Treatment and Do Not Have a Comorbid Condition Requiring Acute Antihypertensive Treatment, Initiating or Reinitiating Treatment of Hypertension within the first 48-72 hrs After an Acute Ischemic Stroke is Not Effective (Class of Recommendation: III = No Benefit; Level of Evidence: A)
Secondary Stroke Prevention
General
For Adults Who Experience a Acute Ischemic Stroke or Transient Ischemic Attack (TIA), Treatment with a Thiazide-Type Diuretic, Angiotensin Converting Enzyme (ACE) Inhibitor, or Angiotensin II Receptor Blocker (ARB), or Combination Treatment Consisting of a Thiazide-Type Diuretic Plus Angiotensin Converting Enzyme (ACE) Inhibitor, is Useful (Class of Recommendation: I: No Benefit; Level of Evidence: A)
For Adults Who Experience a Acute Ischemic Stroke or Transient Ischemic Attack (TIA), Selection of Specific Drugs Should Be Individualized on the Basis of Patient Comorbidities and Agent Pharmacological Class (Class of Recommendation: I: No Benefit; Level of Evidence: B-NR)
For Adults Who Experience a Acute Ischemic Stroke or Transient Ischemic Attack (TIA), a Blood Pressure Goal of <130/80 mm Hg May Be Reasonable (Class of Recommendation: IIb: No Benefit; Level of Evidence: B-R)
For Adults with a Lacunar Stroke, a Target Systolic Blood Pressure (SBP) Goal of <130 mm Hg May Be Reasonable (Class of Recommendation: IIb: No Benefit; Level of Evidence: B-R)
No Prior History of Hypertension
Adults Previously Untreated for Hypertension Who Experience a Stroke or Transient Ischemic Attack (TIA) and Have an Established Blood Pressure of ≥140/90 mm Hg Should Be Prescribed Antihypertensive Treatment a Few Days After the Index Event to Decrease the Risk of Recurrent Stroke and Other Vascular Events (Class of Recommendation: I; Level of Evidence: B-NR)
In Adults Previously Untreated for Hypertension Who Experience a Stroke or Transient Ischemic Attack (TIA) and Have a Systolic Blood Pressure (SBP) <140 mm Hg and a Diastolic Blood Pressure (DBP) <90 mm Hg, the Usefulness of Initiating Antihypertensive Treatment is Not Well Established (Class of Recommendation: IIb; Level of Evidence: C-LD)
Prior History of Hypertension
Adults with Previously Treated Hypertension and the Occurrence of Acute Ischemic Stroke or Transient Ischemic Attack (TIA) Should Be Restarted on Antihypertensive Treatment After the First Few Days of the Index Event to Decrease the Risk of Recurrent Stroke and Other Vascular Events (Class of Recommendation: I; Level of Evidence: A)
Recommendations-American Heart Association (AHA)/American Stroke Association (ASA) 2018 Guidelines for the Early Management of Patients With Acute Ischemic Stroke (Stroke, 2018) [MEDLINE]
Hypotension/Hypovolemia Should Be Corrected to Maintain Systemic Perfusion (Class of Recommendation: I; Level of Evidence: C-EO)
The Blood Pressure Level Which Should Be Maintained in Patients with Acute Ischemic Stroke to Ensure the Best Outcome is Unknown
Some Observational Studies Demonstrate an Association Between Worse Outcome and Lower Blood Pressure, Whereas Other Studies Have Not
No Studies Have Addressed the Treatment of Low Blood Pressure in Patients with Acute Ischemic Stroke
Type of Intravenous Fluid
In a Systematic Analysis of 12 Studies Comparing Colloids with Crystalloids, the Odds of Death/Dependency were Similar (Clinically Important Benefirs/Harms Could Not Be Excluded)
No Studies Have Compared Different Isotonic Intravenous Fluids
Volume/Duration of Intravenous Fluid
No Data to Guide Volume/Duration of Intravenous Fluid Delivery
Patients Who Have Elevated Blood Pressure and are Otherwise Eligible for Treatment with Thrombolytic Therapy Should Have Their Blood Carefully Lowered to <185/110 mm Hg Before Thrombolytic Therapy is Initiated (Class of Recommendation: I, Level of Evidence: B-NR)
The Randomized Controlled Trials of Intravenous Alteplase Required the Systolic Blood Pressure to Be <185 mm Hg and Diastolic Blood Pressure to Be <110 mm Hg Before Treatment and <180/105 mm Hg for the First 24 hrs After Treatment
Some Observational Studies Suggest that the Risk of Hemorrhage After Administration of Thrombolytics is Greater in Patients with Higher Blood Pressure and in Patients with More Blood Pressure Variability
The Exact Blood Pressure at which the Risk of Hemorrhage After Thrombolysis Increases is Unknown
Therefore, it is Reasonable to Target the Blood Pressures Used in the Randomized Controlled Trials of Intravenous Thrombolytics
The Usefulness of Drug-Induced Hypertension in the Setting of Acute Ischemic Stroke is Not Well Established (Class of Recommendation: IIb; Level of Evidence: C-LD)
Recommendations-American Heart Association (AHA)/American Stroke Association (ASA) 2019 Guidelines for the Early Management of Patients With Acute Ischemic Stroke (Stroke, 2019) [MEDLINE]
Hypotension/Hypovolemia Should Be Corrected to Maintain Systemic Perfusion Levels Necessary to Support Organ Function (Class of Recommendation: I; Level of Evidence: C-EO)
The Optimal Blood Pressure Level Which Should Be Maintained in Patients with Acute Ischemic Stroke is Unknown
Some Observational Studies Demonstrate an Association Between Worse Outcomes and Lower Blood Pressures, Whereas Other Studies Do Not
No Studies Address the Treatment of Hypotension in Patients with Stroke
Type of Intravenous Fluid
In a Systematic Analysis of 12 Studies Comparing Colloids with Crystalloids, the Odds of Death or Dependence were Similar (and Clinically Important Benefits or Harms Could Not Be Excluded)
No Studies Have Compared Different Isotonic Intravenous Fluids
Volume/Duration of Intravenous Fluid
No Data to Guide Volume/Duration of Intravenous Fluid Delivery
General Blood Pressure Management
In Patients with Acute Ischemic Stroke, Early Antihypertensive Treatment is Indicated When Required by the Presence of Comorbid Conditions (Such as Concomitant Acute Coronary Syndrome, Acute Congestive Heart Failure, Aortic Dissection, Hypertensive Encephalopathy, Post-Fibrinolysis Intracerebral Hemorrhage, Preeclampsia/Eclampsia) (Class of Recommendation: I; Level of Evidence: C-EO)
Patients with Acute Ischemic Stroke Can Present with Severe Acute Comorbidities Which Demand Emergency Blood Pressure Reduction to Prevent Serious Complications
However, Since Excessive Blood Pressure Reduction Can Exacerbate Cerebral Ischemia, Management Should Be Individualized
Initial Blood Pressure Reduction by 15% is a Reasonable Goal
There is No Data to Demonstrate Efficacy of One Blood Pressure Control Strategy Over Another After Acute Ischemic Stroke
The Usefulness of Drug-Induced Hypertension in the Setting of Acute Ischemic Stroke is Not Well Established (Class of Recommendation: IIb, Level of Evidence: B-NR)
Blood Pressure Management in the Setting of Thrombolytic Therapy
Patients Who Have Elevated Blood Pressure and are Otherwise Eligible for Treatment with Thrombolytic Therapy Should Have Their Blood Pressure Carefully Decreased so that Their Systolic Blood Pressure is <185 mm Hg and Their Diastolic Blood Pressure is <110 mm Hg Before Thrombolytic Therapy is Initiated (Class of Recommendation: I; Level of Evidence: B-NR)
The Randomized Controlled Trials of Intravenous Alteplase Required Systolic <185 mm Hg and Diastolic Blood Pressure <110 mm Hg Before Thrombolytic Therapy and <180/105 mm Hg for the First 24 hrs After Thrombolytic Therapy
Some Observational Studies Suggest that the Risk of Hemorrhage After Administration of Alteplase is Greater in Patients with Higher Blood Pressures and in Patients with More Blood Pressure Variability
The Exact Blood Pressure at Which the Risk of Hemorrhage After Thrombolytics Increases is Unknown
Therefore, it is Reasonable to Target the Blood Pressures Used in the Randomized Controlled Trials of Intravenous Alteplase
Blood Pressure Management in the Setting of Mechanical Thrombectomy
In Patients for Whom Mechanical Thrombectomy is Planned and Who Have Not Received Thrombolytic Therapy, it is Reasonable to Maintain Blood Pressure ≤185/110 mm Hg Before the Procedure (Class of Recommendation: IIa, Level of Evidence: B-NR)
Of the 6 Randomized Controlled trials Which Each Independently Demonstrated Clinical Benefit of Mechanical Thrombectomy with Stent Retrievers when Performed <6 hrs from Stroke Onset, the REVASCAT/SWIFT PRIME/EXTEND-IA/THRACE/MR CLEAN Trials Had Eligibility Exclusions for Blood Pressure >185/110 mm Hg, While the ESCAPE Trial Had No Blood Pressure Eligibility Exclusions
The DAWN Trial Also Used an Exclusion for Blood Pressure >185/110 mm Hg
Randomized Controlled trial Data for Optimal Blood Pressure Management Approaches in this Setting are Not Available
Because the Vast Majority of Patients Enrolled in these Randomized Controlled Trials Had Preprocedural Blood Pressure Managed <185/110 mm Hg, it is Reasonable to Use This Level as a Guideline Until Additional Data Become Available
In Patients Who Undergo Mechanical Thrombectomy with Successful Reperfusion, it is Reasonable to Maintain Blood Pressure at <180/105 mm Hg (Class of Recommendation: IIb; Level of Evidence: B-NR)
In Patients Who Undergo Mechanical Thrombectomy, it is Reasonable to Maintain the Blood Pressure at ≤180/105 mm Hg During and for 24 hrs After the Procedure (Class of Recommendation: IIa; Level of Evidence: B-NR)
Blood Pressure Management in the Absence of Thrombolytic Therapy
In Patients with BP ≥220/120 mm Hg Who Did Not Receive Reperfusion Therapy (Thrombolytic Therapy, Mechanical Thrombectomy) and Have No Comorbid Conditions Requiring Urgent Antihypertensive Treatment, the Benefit of Initiating/Reinitiating Antihypertensive Treatment within the First 48-72 hrs is Uncertain (Class of Recommendation: IIb; Level of Evidence: C-EO)
It is Reasonable to Lower Blood Pressure by 15% During the First 24 hrs After Onset of Acute Ischemic Stroke
Patients with Severe Hypertension (Most Commonly >220/120 mm Hg) were Excluded from Clinical Trials Evaluating Blood Pressure Reduction After Acute Ischemic Stroke
Rapid Blood Pressure Reduction Has Traditionally Been Advised for These Cases, But the Benefit of Such Treatment in the Absence of Comorbid Conditions Which May Be Acutely Exacerbated by Severe Hypertension Has Not Been Formally Studied
Ideal Management in These Situations Should Be Individualized, But an Initial Blood Pressure Reduction by 15% is a Reasonable Goal
Excessive Decrease in Blood Pressure Could Result in Complications, Such as Stroke Progression (by Compromising Cerebral Perfusion in Penumbral Tissue) and Acute Kidney Injury (from Renal Hypoperfusion)
There is No Data to Demonstrate Efficacy of One Blood Pressure Control Strategy Over Another After Acute Ischemic Stroke
In Patients with Blood Pressure <220/120 mm Hg Who Did Not Receive Reperfusion Therapy (Thrombolytic Therapy, Mechanical Thrombectomy) and Do Not Have a Comorbid Condition Requiring Urgent Antihypertensive Therapy (Aortic Dissection, Severe HELLP Syndrome/Preeclampsia/Eclampsia, Pheochromocytoma, etc), Initiating/Reinitiating Antihypertensive Treatment within the First 48-72 hrs After an Acute Ischemic Stroke is Not Effective to Prevent Death or Dependency (Class of Recommendation: III-No Benefit; Level of Evidence: A)
Multiple Randomized Controlled Trials and Meta-Analyses of These Trials Have Consistently Demonstrated that Initiating/Reinitiating Antihypertensive Treatment within the first 48-72 hrs After an Acute Ischemic Stroke is Safe, But This Strategy is Not Associated with Improved Mortality or Functional Outcomes
However, None of These Trials were Designed to Study Blood Pressure Reduction within the First 6 hrs After Stroke, and All Excluded Patients with Extreme Hypertension or Coexistent Indications for Rapid Blood Pressure Reduction
Recommendations-2025 AHA/ACC/AANP/AAPA/ABC/ACCP/ACPM/AGS/AMA/ASPC/NMA/PCNA/SGIM Guideline for the Prevention, Detection, Evaluation and Management of High Blood Pressure in Adults (Circulation, 2025) MEDLINE]
General
In Acute Ischemic Stroke, Hypotension/Hypovolemia Should Be Corrected to Maintain Systemic Perfusion Levels Necessary to Support Organ Function (Class of Recommendation: 1; Level of Evidence: C-LD)
Intravenous Thrombolytic Treatment
In Acute Ischemic Stroke with Elevated Blood Pressure and Eligibility for Intravenous Thrombolytic Treatment, Blood Pressure Should Be Decreased to Systolic Blood Pressure (SBP) <185 mm Hg and Diastolic Blood Pressure (DBP) <110 mm Hg Before Intravenous Thrombolytic Therapy is Initiated and Should Be Maintained <180/105 mm Hg for at Least the First 24 hrs After Initiating Thrombolytic Therapy to Avoid Complications (Class of Recommendation: 1; Level of Evidence: B-NR)
Endovascular Treatment
In Acute Ischemic Stroke with Endovascular Treatment, it is Reasonable to Maintain the Blood Pressure at ≤180/105 mm Hg During and for 24 hrs After Endovascular Treatment to Improve Long-Term Functional Outcomes and Prevent Death (Class of Recommendation: 2a; Level of Evidence: B-NR)
In Acute Ischemic Stroke with Successful Brain Reperfusion with Endovascular Treatment for a Large Vessel Occlusion, Lowering the Systolic Blood Pressure (SBP) to <140 mm Hg within the First 24-72 hrs After Reperfusion Can Worsen Long-Term Functional Outcome (Class of Recommendation: 3 = Harm; Level of Evidence: A)
No Intravenous Thrombolytic or Endovascular Treatment
In Acute Ischemic Stroke with Blood Pressure of ≥220/120 mm Hg and No Intravenous Thrombolytic or Endovascular Treatment and No Comorbid Conditions Requiring Acute Antihypertensive Treatment, it Might Be Reasonable to Lower Blood Pressure by 15% During the First 24 hrs After the Onset of Stroke to Improve Outcomes (Class of Recommendation: 2b; Level of Evidence: C-LD)
In Acute Ischemic Stroke with Blood Pressure <220/120 mm Hg and No Intravenous Thrombolytic or Endovascular Treatment and No Comorbid Condition Requiring Urgent Antihypertensive Treatment, Initiating or Reinitiating Treatment of Hypertension within the First 48-72 hrs After an Acute Ischemic Stroke is Not Effective to Prevent Death or Disability (Class of Recommendation: 3 = No Benefit; Level of Evidence: A)
Secondary Stroke Prevention
No Prior History of Hypertension
With No Prior History of Hypertension and with an Acute Ischemic Stroke, Transient Ischemic Attack (TIA), or Intracerebral Hemorrhage and Average Office Systolic Blood Pressure (SBP)/Diastolic Blood Pressure (DBP) of ≥130/80 mm Hg, Antihypertensive Treatment Can Be Beneficial to Decrease the Risk of Recurrent Stroke, Intracerebral Hemorrhage, and Other Vascular Events (Class of Recommendation: 2; Level of Evidence: B-R)
Prior History of Hypertension
With Prior History of Hypertension and Occurence of Acute Ischemic Stroke, Transient Ischemic Attack (TIA), or Intracerebral Hemorrhage, Treatment with a Thiazide-Type Diuretic, Angiotensin Converting Enzyme (ACE) Inhibitor, or Angiotensin II Receptor Blocker (ARB) is Recommended for Lowering Blood Pressure and Reducing Recurrent Stroke and Intracerebral Hemorrhage Risk (Class of Recommendation: 1; Level of Evidence: A)
With Prior History of Hypertension and Occurence of Acute Ischemic Stroke, Transient Ischemic Attack (TIA), or Intracerebral Hemorrhage, an Office Systolic Blood Pressure (SBP)/Diastolic Blood Pressure (DBP) Goal of <130/80 mm Hg is Recommended to Decrease the Risk of Recurrent Stroke, Intracerebral Hemorrhage, and Other Vascular Events (Class of Recommendation: 1; Level of Evidence: B-R)
Treatment of Hypertensive Emergency in the Setting of Intracerebral Hemorrhage (ICH) (see Intracerebral Hemorrhage)
Recommendations-2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults (Circulation, 2018) [MEDLINE]
In Adults with Intracerebral Hemorrhage Who Present with Systolic Blood Pressure (SBP) >220 mm Hg, Use Continuous Intravenous Antihypertensives (with Close Blood Pressure Monitoring to Decrease the Systolic Blood Pressure (SBP) (Class of Recommendation: IIa; Level of Evidence: C-EO)
In Adults with Spontaneous Intracerebral Hemorrhage Who Present within 6 hrs of the Acute Event and Have an Systolic Blood Pressure (SBP) Between 150-220 mm Hg, Immediately Decreasing the Systolic Blood Pressure (SBP) to <140 mm Hg Does Not Decrease the Mortality Rate/Risk of Severe Disability and Can Be Potentially Harmful (Class of Recommendation: III: Harm; Level of Evidence: A)
Recommendations-American Heart Association (AHA)/American Stroke Association (ASA) 2022 Guideline for the Management of Patients With Spontaneous Intracerebral Hemorrhage (Stroke, 2022) [MEDLINE]
In Patients with Spontaneous Intracerebral Hemorrhage Requiring Acute Antihypertensive Therapy, Careful Titration to Ensure Continuous Smooth and Sustained Blood Pressure Control (Avoiding Peaks and Large Variability in Systolic Blood Pressure), Can Improve Functional Outcome (Class of Recommendation: 2a, Level of Evidence: B-NR)
In Patients with Spontaneous Intracerebral Hemorrhage in Whom Acute Blood Pressure Lowering is Considered, Initiating Treatment within 2 hrs of Intracerebral Hemorrhage Onset and Reaching the Blood Pressure Target within 1 hrs Can Decrease the Risk of Hematoma Expansion and Improve Functional Outcome (Class of Recommendation: 2a, Level of Evidence: C-LD)
In Patients with Spontaneous Mild-Moderate Intracerebral Hemorrhage Presenting with Systolic Blood Pressure between 150-220 mm Hg, Acute Decrease in the Systolic Blood Pressure to a Target of 140 mm Hg with the Goal of Maintaining Systolic Blood Pressure in the Range of 130-150 mm Hg is Safe and May Be Reasonable for Improving Functional Outcomes (Class of Recommendation: 2b, Level of Evidence: B-R)
In Patients with Spontaneous Large-Severe Intracerebral Hemorrhage or Those Requiring Surgical Decompression, the Safety and Efficacy of Intensive Blood Pressure Decrease are Not Well Established (Class of Recommendation: 2b, Level of Evidence: C-LD)
In Patients with Spontaneous Mild-Moderate Intracerebral Hemorrhage Presenting with SBP >150 mm Hg, Acute Decrease in Systolic Blood Pressure to <130 mm Hg is Potentially Harmful (Class of Recommendation: 3-Harm, Level of Evidence: B-R)
Recommendations-2025 AHA/ACC/AANP/AAPA/ABC/ACCP/ACPM/AGS/AMA/ASPC/NMA/PCNA/SGIM Guideline for the Prevention, Detection, Evaluation and Management of High Blood Pressure in Adults (Circulation, 2025) MEDLINE]
During Acute Management of Intracerebral Hemorrhage
For Adult Patients with Acute Spontaneous Intracerebral Hemorrhage Who Present with Systolic Blood Pressure (SBP) Between 150-220 mm Hg, it Can Be Beneficial to Immediately Lower Systolic Blood Pressure (SBP) to 130-140 mm Hg for at Least 7 Days After Intracerebral Hemorrhage to Improve Functional Outcomes, But Stop Antihypertensives if Systolic Blood Pressure (SBP) is <130 mm Hg (Class of Recommendation: 2; Level of Evidence: A)
In Adults with Acute Spontaneous Intracerebral Hemorrhage Requiring Acute Blood Pressure Lowering, Careful Titration to Ensure Smooth, Non-Labile, and Sustained Control of Blood Pressure, Avoiding Peaks and Large Variability in Systolic Blood Pressure (SBP), Can Be Beneficial for Improving Functional Outcomes (Class of Recommendation: 2a; Level of Evidence: B-NR)
For Adult Patients with Acute Spontaneous Intracerebral Hemorrhage Who Present with Systolic Blood Pressure (SBP) >220 mm Hg, Systolic Blood Pressure (SBP) Should Not Be Lowered <130 mm Hg to Reduce Adverse Events (Class of Recommendation: 3 = Harm; Level of Evidence: B-NR)
Secondary Stroke Prevention
Prior History of Hypertension
With Prior History of Hypertension and Occurence of Acute Ischemic Stroke, Transient Ischemic Attack (TIA), or Intracerebral Hemorrhage, Treatment with a Thiazide-Type Diuretic, Angiotensin Converting Enzyme (ACE) Inhibitor, or Angiotensin II Receptor Blocker (ARB) is Recommended for Lowering Blood Pressure and Decreasing Recurrent Stroke and Intracerebral Hemorrhage Risk (Class of Recommendation: 1; Level of Evidence: A)
With Prior History of Hypertension and Occurence of Acute Ischemic Stroke, Transient Ischemic Attack (TIA), or Intracerebral Hemorrhage, an Office Systolic Blood Pressure (SBP)/Diastolic Blood Pressure (DBP) Goal of <130/80 mm Hg is Recommended to Decrease the Risk of Recurrent Stroke, Intracerebral Hemorrhage, and Other Vascular Events (Class of Recommendation: 1; Level of Evidence: B-R)
No Prior History of Hypertension
With No Prior History of Hypertension and with an Acute Ischemic Stroke, Transient Ischemic Attack (TIA), or Intracerebral Hemorrhage and Average Office Systolic Blood Pressure (SBP)/Diastolic Blood Pressure (DBP) of ≥130/80 mm Hg, Antihypertensive Treatment Can Be Beneficial to Decrease the Risk of Recurrent Stroke, Intracerebral Hemorrhage, and Other Vascular Events (Class of Recommendation: 2; Level of Evidence: B-R)
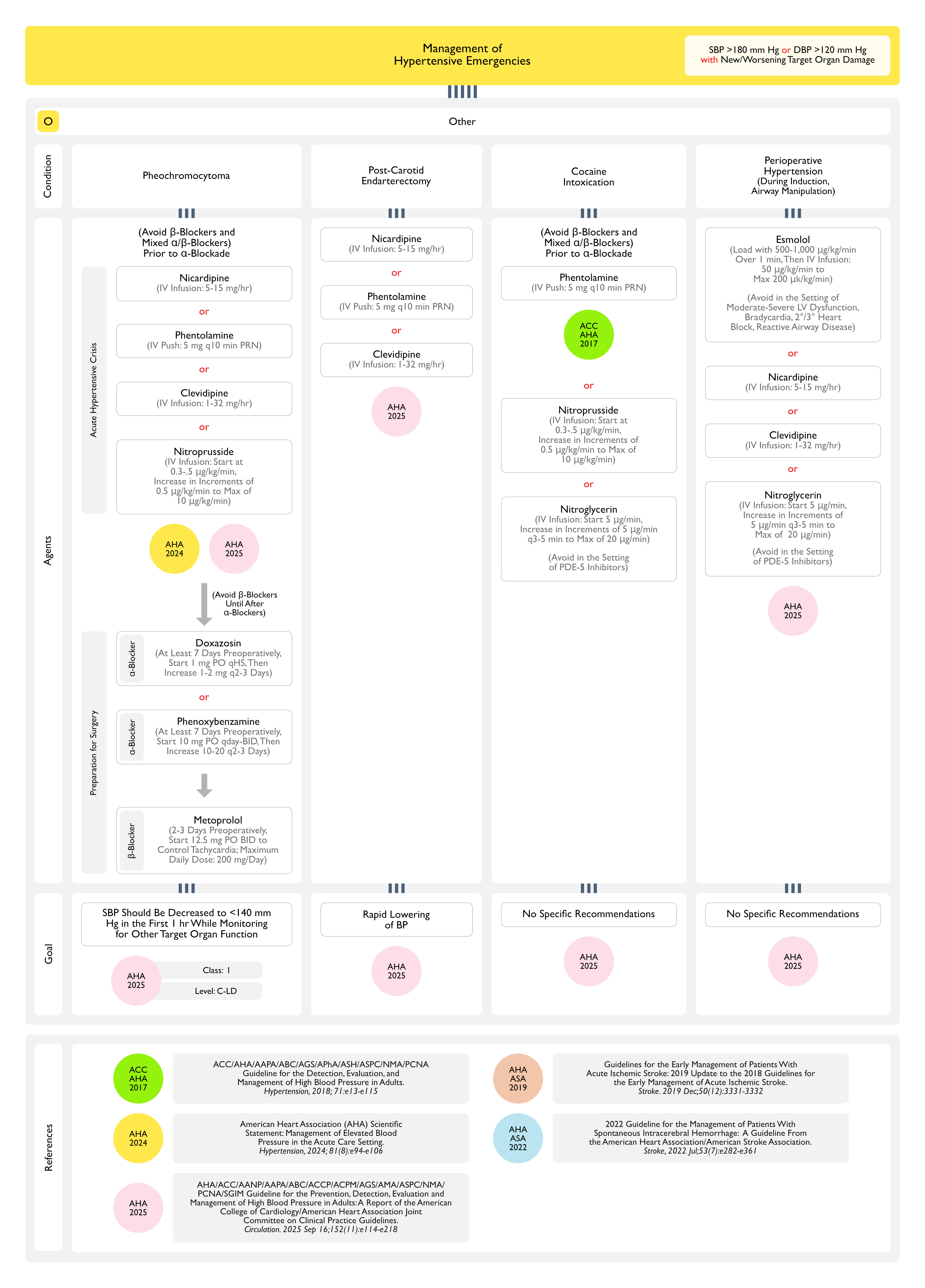
Treatment of Hypertensive Emergency in the Setting of Acute Aortic Syndrome (Aortic Intramural Hematoma, Aortic Intimal Tear without Hematoma, Penetrating Aortic Ulcer, Periaortic Hematoma, or Aortic Dissection) (see Aortic Dissection)
Recommendations-2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults (Circulation, 2018) [MEDLINE]
For Adults with a Compelling Condition (Aortic Dissection, Severe Preeclampsia/Eclampsia, Pheochromocytoma), Systolic Blood Pressure Should Be Decreased to <140 mm Hg During the First 1 hr and to <120 mm Hg in Aortic Dissection (Class of Recommendation: I; Level of Evidence: C-EO)
Aortic Dissection Requires Rapid Lowering of Systolic Blood Pressure to <120 mm Hg (within Approximately 20 min)
β-Blockade Should Precede any Required Vasodilator (Nicardipine, Nitroprusside) Administration to Prevent Reflex Tachycardia or Increased Inotropy
Recommendations-2025 AHA/ACC/AANP/AAPA/ABC/ACCP/ACPM/AGS/AMA/ASPC/NMA/PCNA/SGIM Guideline for the Prevention, Detection, Evaluation and Management of High Blood Pressure in Adults (Circulation, 2025) MEDLINE]
For Adults with a Hypertensive Emergency Related to an Acute Aortic Syndrome (Aortic Intramural Hematoma, Aortic Intimal Tear without Hematoma, Penetrating Aortic Ulcer, Periaortic Hematoma, Acute Aortic Dissection), Systolic Blood Pressure (SBP) Should Be Decreased as Follows While Monitoring for Other Target Organ Dysfunction (Class of Recommendation: 1; Level of Evidence: C-LD)
Aortic Dissection: Decrease Blood Pressure to <120 mm Hg During the First 1 hr
Other Acute Aortic Syndrome (Aortic Intramural Hematoma, Aortic Intimal Tear without Hematoma, Penetrating Aortic Ulcer, Periaortic Hematoma): Decrease Blood Pressure to <140 mm Hg During the First 1 hr
Treatment of Hypertensive Emergency in the Setting of Hemolysis Elevated Liver Functions Low Platelets (HELLP) Syndrome/Preeclampsia/Eclampsia (see HELLP Syndrome) and Preeclampsia/Eclampsia)
Recommendations-2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults (Circulation, 2018) [MEDLINE]
For Adults with a Compelling Condition (Aortic Dissection, Severe Preeclampsia/Eclampsia, Pheochromocytoma), Systolic Blood Pressure Should Be Decreased to <140 mm Hg During the First 1 hr and to <120 mm Hg in Aortic Dissection (Class of Recommendation: I; Level of Evidence: C-EO)
Recommendations-2025 AHA/ACC/AANP/AAPA/ABC/ACCP/ACPM/AGS/AMA/ASPC/NMA/PCNA/SGIM Guideline for the Prevention, Detection, Evaluation and Management of High Blood Pressure in Adults (Circulation, 2025) [MEDLINE]
For Females with Hypertension Who are Planning a Pregnancy or Who Become Pregnant, Labetalol and Extended-Release Nifedipine are Preferred Agents to Treat Hypertension and Minimize Fetal Risk (Class of Recommendation: I; Level of Evidence: A)
Females with Hypertension Who are Planning a Pregnancy or Who Become Pregnant Should Be Counseled About the Benefits of Low-Dose Aspirin (81 mg/day) to Reduce the Risk of Preeclampsia and its Sequelae (Class of Recommendation: I; Level of Evidence: B-R)
Pregnant Females with Systolic Blood Pressure (SBP) ≥160 mm Hg or Diastolic Blood Pressure (DBP) ≥110 mm Hg Confirmed on Repeat Measurement within 15 min Should Receive Antihypertensives to Lower Blood Pressure to <160/<110 mm Hg within 30-60 min to Prevent Adverse Events (Class of Recommendation: I; Level of Evidence: B-R)
Pregnant Females with Chronic Hypertension (Defined as Pre-Pregnancy Hypertension or Systolic Blood Pressure (SBP) 140-159 mm Hg and/or Diastolic Blood Pressure (DBP) 90-109 mm Hg Prior to 20 wks Gestation) Should Receive Antihypertensive Therapy to Achieve Blood Pressure <140/90 mm Hg to Prevent Maternal and Perinatal Morbidity and Mortality (Class of Recommendation: I; Level of Evidence: B-R)
Females with Hypertension Who are Planning a Pregnancy or Who Become Pregnant Should Not Be Treated with Atenolol, Angiotensin Converting Enzyme (ACE) Inhibitors, Angiotensin II Receptor Blockers (ARB’s), Direct Renin Inhibitors, Nitroprusside, or Mineralocorticoid Receptor Antagonists to Avoid Fetal Harm (Class of Recommendation: 3 = Harm; Level of Evidence: C-LD)
Recommendations-2025 AHA/ACC/AANP/AAPA/ABC/ACCP/ACPM/AGS/AMA/ASPC/NMA/PCNA/SGIM Guideline for the Prevention, Detection, Evaluation and Management of High Blood Pressure in Adults (Circulation, 2025) MEDLINE]
Preeclampsia/Eclampsia Require Rapid Decrease in Blood Pressure
Treatment of Hypertensive Emergency in the Setting of Grade III-IV Keith-Wagener-Barker Hypertensive Retinopathy
Recommendations-2025 AHA/ACC/AANP/AAPA/ABC/ACCP/ACPM/AGS/AMA/ASPC/NMA/PCNA/SGIM Guideline for the Prevention, Detection, Evaluation and Management of High Blood Pressure in Adults (Circulation, 2025) [MEDLINE]
For Adults with a Hypertensive Emergency But without a Compelling Condition (Such as an Acute Aortic Syndrome), Systolic Blood Pressure (SBP) Should Be Decreased with Oral/Parenteral Therapy by ≤25% within the First Hour (Class of Recommendation: 1; Level of Evidence: C-LD)
Then, if Stable, Decreased to Systolic Blood Pressure (SBP <160/100 mm Hg within the Next 2-6 hrs (Class of Recommendation: 1; Level of Evidence: C-LD)
Then Cautiously Decrease to Systolic Blood Pressure (SBP 130-140 mm Hg During the Next 24-48 hrs to Limit Target Organ Injury (Class of Recommendation: 1; Level of Evidence: C-LD)
Treatment of Hypertensive Emergency in the Setting of Acute Kidney Injury or Thrombotic Microangiopathy
Recommendations-2025 AHA/ACC/AANP/AAPA/ABC/ACCP/ACPM/AGS/AMA/ASPC/NMA/PCNA/SGIM Guideline for the Prevention, Detection, Evaluation and Management of High Blood Pressure in Adults (Circulation, 2025) [MEDLINE]
For Adults with a Hypertensive Emergency But without a Compelling Condition (Such as an Acute Aortic Syndrome), Systolic Blood Pressure (SBP) Should Be Decreased with Oral/Parenteral Therapy by ≤25% within the First Hour (Class of Recommendation: 1; Level of Evidence: C-LD)
Then, if Stable, Decreased to Systolic Blood Pressure (SBP <160/100 mm Hg within the Next 2-6 hrs (Class of Recommendation: 1; Level of Evidence: C-LD)
Then Cautiously Decrease to Systolic Blood Pressure (SBP 130-140 mm Hg During the Next 24-48 hrs to Limit Target Organ Injury (Class of Recommendation: 1; Level of Evidence: C-LD)
References
Treatment
Pharmacological basis for antihypertensive effects of intravenous labetalol. Br Heart J. 1977;39(1):99 [MEDLINE]
Hypertensive crises: challenges and management. Chest. 2007;131(6);1949-1962. doi: 10.1378/chest.06-2490 [MEDLINE]
Pharmacological management of hypertensive emergencies and urgencies: focus on newer agents. Expert Opin Investig Drugs. 2012;21(8):1089-1106. doi: 10.1517/13543784.2012.693477 [MEDLINE]
Diagnostic and therapeutic approach to the hypertensive crisis. Med Clin (Barc). 2018 Apr 23;150(8):317-322. doi: 10.1016/j.medcli.2017.09.027 [MEDLINE]
Initial Treatment of Hypertension. N Engl J Med. 2018 Feb 15;378(7):636-644. doi: 10.1056/NEJMcp1613481 [MEDLINE]
2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Hypertension. 2018 Jun;71(6):e13-e115. doi: 10.1161/HYP.0000000000000065 [MEDLINE]
ESC Council on hypertension position document on the management of hypertensive emergencies. European Heart Journal – Cardiovascular Pharmacotherapy (2019) 5, 37–46 doi:10.1093/ehjcvp/pvy032 [MEDLINE]
Hypertensive Emergencies: A Review of Common Presentations and Treatment Options. Cardiol Clin. 2019 Aug;37(3):275-286. doi: 10.1016/j.ccl.2019.04.003 [MEDLINE]
Acute severe hypertension. N Engl J Med. 2019;381(19):1843-1852. doi: 10.1056/NEJMcp1901117 [MEDLINE]
Management of hypertensive emergencies: a practical approach. Blood Press. 2021 Aug;30(4):208-219. doi: 10.1080/08037051.2021.1917983 [MEDLINE]
Treatment and outcomes of inpatient hypertension among adults with noncardiac admissions. JAMA Intern Med. 2021;181:345–352. doi: 10.1001/jamainternmed.2020.7501 [MEDLINE]
Omega-3 polyunsaturated fatty acids intake and blood pressure: A dose-response meta-analysis of randomized controlled trials. J Am Heart Assoc. 2022 Jun 7;11(11):e025071. doi: 10.1161/JAHA.121.025071 [MEDLINE]
Feasibility and short-term effects of a multi-component emergency department blood pressure intervention: a pilot randomized trial. J Am Heart Assoc. 2022 Mar;11(5):e024339. doi: 10.1161/JAHA.121.024339 [MEDLINE]
Clinical outcomes of intensive inpatient blood pressure management in hospitalized older adults. JAMA Intern Med. 2023;183:715–723. doi: 10.1001/jamainternmed.2023.1667 [MEDLINE]
Mortality and Morbidity Among Individuals With Hypertension Receiving a Diuretic, ACE Inhibitor, or Calcium Channel Blocker: A Secondary Analysis of a Randomized Clinical Trial. JAMA Netw Open. 2023 Dec 1;6(12):e2344998. doi: 10.1001/jamanetworkopen.2023.44998 [MEDLINE]
The Management of Elevated Blood Pressure in the Acute Care Setting: A Scientific Statement From the American Heart Association. Hypertension. 2024 May 28. doi: 10.1161/HYP.0000000000000238 [MEDLINE]
Impact of hypertension duration on the cardiovascular benefit of intensive blood pressure control. Hypertension. 2024 Sep;81(9):1945-1955. doi: 10.1161/HYPERTENSIONAHA.124.23439 [MEDLINE]