Systolic Blood Pressure (SBP): first Korotkoff sound
Diastolic Blood Pressure (DBP): second Korotkoff sound
Pulse Pressure: SBP – DBP
Mean Arterial Pressure (MAP): DBP + 1/3 (pulse pressure)
Assumes a Normal Heart Rate
Mid-Blood Pressure: (SBP + DBP)/2
Clinical Efficacy
Systematic Review and Network Meta-Analysis Studying Agreement Between Different Types of Blood Pressure Measurements (Ann Intern Med, 2025) [MEDLINE]: n = 40,022 (from 65 studies)
Compared with Research Office Systolic Blood Pressure Measurement, the Pooled Mean Differences from Corresponding Systolic Blood Pressures were 2.69 mm Hg (95% CI: -0.13 to 5.51 mm Hg) Higher for Convenient Office Blood Pressure Measurement (OBPM), 4.57 mm Hg (95% CI: 2.54 to 6.60 mm Hg) Lower for Automated Office Blood Pressure Measurement (OBPM), 4.59 mm Hg (95% CI: 2.83 to 6.34 mm Hg) Lower for Home Blood Pressure Measurement, 4.22 mm Hg (95% CI: 2.62 to 5.82 mm Hg) Lower for Daytime Ambulatory Blood Pressure Measurement (ABPM), 18.14 mm Hg (95% CI: 16.21 to 20.06 mm Hg) Lower for Nighttime Ambulatory Blood Pressure Measurement (ABPM), and 8.63 mm Hg (95% CI: 6.97 to 10.28 mm Hg) Lower for 24 Hour Ambulatory Blood Pressure Measurement (ABPM)
Differences Varied by Reference Research Office Blood Pressure Measurement (OBPM) Levels
Higher Reference Blood Pressure Levels are Associated with Larger Differences Between Research Office and Other Blood Pressure Measurement Methods
Study of the Effect of Systolic Blood Pressure Measurement Error on the Cost-Effectiveness of Intensive Blood Pressure Targets (Ann Intern Med, 2025) MEDLINE]For Systolic Blood Pressure Intervention Trial (SPRINT)-Eligible Patients at High Cardiovascular Risk (But without Diabetes or Prior Stroke) a Systolic Blood Pressure (SBP) Target <120 mm Hg Seems Cost-Effective Across Most Settings with Systolic Blood Pressure (SBP) Measurement ErrorLimitation There is Uncertainty in the Relationship Between Low Treated Systolic Blood Pressure (SBP) (For Example: <115 mm Hg) and Cardiovascular Risk
Recommendations-2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults (Circulation, 2018) [MEDLINE]
For Diagnosis and Management of Hypertension, Proper Methods are Recommended for Accurate Measurement and Documentation of Blood Pressure (Class of Recommendation: I, Level of Evidence: C-EO)
Step 1: Properly Prepare the Patient
Have the Patient Relax, Sitting in a Chair (Feet on Floor, Back Supported) for >5 min
Patient Should Avoid Caffeine, Exercise, and Smoking for ≥30 min Before Blood Pressure Measurement
Ensure patient has emptied his/her bladder
Neither the Patient Nor the Observer Should Talk During the Rest Period or During Blood Pressure Measurement
Remove All Clothing Covering the Location of Cuff Placement
Measurements Made While the Patient is Sitting or Lying on an Examining Table Do Not Fulfill These Criteria
Step 2: Use Proper Technique for Blood Pressure Measurements
Use a Blood Pressure Measurement Device Which Has Been Validated, and Ensure that the Device is Calibrated Periodically
Support the Patient’s Arm (Resting on a Desk)
Position the Middle of the Cuff on the Patient’s Upper Arm at the Level of the Right Atrium (the Midpoint of the Sternum)
Use the Correct Cuff Size, Such that the Bladder Encircles 80% of the Arm, and Note if a Larger or Smaller-than-Normal Cuff Size is Used
Arm Circumference 22–26 cm: small adult cuff
Arm Circumference 27-34 cm: adult cuff
Arm Circumference 35-44 cm: large adult cuff
Arm Circumference 45-52 cm: adult thigh cuff
Either the Stethoscope Diaphragm or Bell May Be Used for Auscultatory Readings
Step 3: Take the Proper Measurements Needed for Diagnosis and Treatment of Hypertension
At the First Visit, Record Blood Pressure in Both Arms
Use the Arm Which Gives the Higher Reading for Subsequent Readings
Separate Repeated Measurements by 1–2 min
For Auscultatory Determinations, Use a Palpated Estimate of Radial Pulse Obliteration Pressure to Estimate Systolic Blood Pressure (SBP)
Inflate the cuff 20–30 mm Hg above this level for an auscultatory Determination of the Blood Pressure Level
For Auscultatory Readings, Deflate the Cuff Pressure 2 mm Hg Per Second, and Listen for Korotkoff Sounds
Step 4: Properly Document Accurate Blood Pressure Readings
Record Systolic Blood Pressure (SBP) and Diastolic Blood Pressure (DBP)
If Using the Auscultatory Technique, Record Systolic Blood Pressure (SBP) and Diastolic Blood Pressure (DBP) as Onset of the First Korotkoff Sound and Disappearance of All Korotkoff Sounds, Respectively, Using the Narest Even Number
Note the Time of Most Recent Blood Pressure Medication Taken Before Blood Pressure Measurement
Step 5: Average the Blood Pressure Readings
Use an Average of ≥2 Readings Obtained on ≥2 Occasions to Estimate the Blood Pressure
Step 6: Provide Blood Pressure Readings to the Patient
Provide Patient the Systolic Blood Pressure (SBP)/Diastolic Blood Pressure (DBP) Readings Both Verbally and in Writing
Recommendations-2025 AHA/ACC/AANP/AAPA/ABC/ACCP/ACPM/AGS/AMA/ASPC/NMA/PCNA/SGIM Guideline for the Prevention, Detection, Evaluation and Management of High Blood Pressure in Adults (Circulation, 2025) MEDLINE]
Accurate Measurement of In-Office Blood Pressure
When Diagnosing and Managing High Blood Pressure in Adults, Standardized Methods are Recommended for the Accurate Measurement and Documentation of In-Office Blood Pressure (Class of Recommendation: 1; Level of Evidence: C-LD)
When Measuring In-Office Blood Pressure in Adults, it is Reasonable to Use the Oscillometric Method with an Automated Device Over the Auscultatory Method (Class of Recommendation: 2a; Level of Evidence: C-EO)
Ambulatory Blood Pressure Monitoring (ABPM) and Home Blood Pressure Monitoring (HBPM)
In Adults with Suspected hypertension, Out-of-Office Blood Pressure Measurements by Either Ambulatory Blood Pressure Monitoring (ABPM) or Home Blood Pressure Monitoring (HBPM) are Recommended to Confirm the Diagnosis of Hypertension (Class of Recommendation: 1; Level of Evidence: A)
In Adults Who are Taking Antihypertensives, Home Blood Pressure Monitoring (HBPM) is Recommended for Monitoring the Titration of Blood Pressure-Lowering Medication, Along with Cointerventions (Such as Patient Education, Telehealth Counseling, and Clinical Interventions) (Class of Recommendation: 1; Level of Evidence: A)
Cuffless Blood Pressure Devices
In Adults, the Use of Cuffless Blood Pressure Devices is Not Recommended for the Diagnosis or Management of High Blood Pressure (Class of Recommendation: 3 = No Benefit; Level of Evidence: C-LD)
White-Coat Hypertension and Masked Hypertension, White-Coat Effect and Masked Uncontrolled Hypertension
In Adults with Untreated Office Systolic Blood Pressure (SBP) ≥130 mm Hg or Diastolic Blood Pressure (DBP) ≥80 mm Hg, and without Office Systolic Blood (SBP) ≥160 mm Hg or Diastolic Blood Pressure (DBP) ≥100 mm Hg, it is Reasonable to Exclude White-Coat Hypertension Using Out-of-Office Blood Pressure Monitoring Before a Diagnosis of Hypertension is Made (Class of Recommendation: 2a; Level of Evidence: B-NR)
In Adults with White-Coat Hypertension or Masked Hypertension, Out-of-Office Blood Pressure Monitoring is Reasonable to Exclude Transition to a Diagnosis of Sustained Hypertension (Class of Recommendation: 2a; Level of Evidence: B-NR)
In Adults with Apparent Treatment-Resistant Hypertension on Office Blood Pressure, it is Reasonable to Exclude White-Coat Effect, a Form of Pseudoresistance, Using Out-of-Office Blood Pressure Monitoring (Class of Recommendation: 2a; Level of Evidence: C-LD)
In Adults Who are Taking Antihypertensives and Have Elevated Office Blood Pressure (Office Systolic Blood Pressure/SBP ≥130 mm Hg or Diastolic Blood Pressure/DBP ≥80 mm Hg) But Do Not Have Resistant Hypertension or Office Systolic Blood Pressure (SBP) ≥160 mm Hg or Diastolic Blood Pressure ≥100 mm Hg, it is Reasonable to Exclude White-Coat Effect Using Out-of-Office Blood Pressure Monitoring (Class of Recommendation: 2a; Level of Evidence: B-NR)
In Adults with Untreated Office Systolic Blood Pressure (SBP) <130 mm Hg and Diastolic Blood Pressure (DBP) <80 mm Hg, it May Be Reasonable to Exclude Masked Hypertension Using Out-of-Office Blood Pressure Monitoring (Class of Recommendation: 2b; Level of Evidence: B-NR)
In Adults Who are Taking Antihypertensives and Have Office Systolic Blood Pressure (SBP) <130 mm Hg and Diastolic Blood Pressure (DBP) <80 mm Hg, it May Be Reasonable to Exclude Masked Uncontrolled Hypertension Using Out-of-Office Blood Pressure Monitoring (Class of Recommendation: 2a; Level of Evidence: B-NR)
Classification of High Blood Pressure
Recommendations-2025 AHA/ACC/AANP/AAPA/ABC/ACCP/ACPM/AGS/AMA/ASPC/NMA/PCNA/SGIM Guideline for the Prevention, Detection, Evaluation and Management of High Blood Pressure in Adults (Circulation, 2025) MEDLINE]
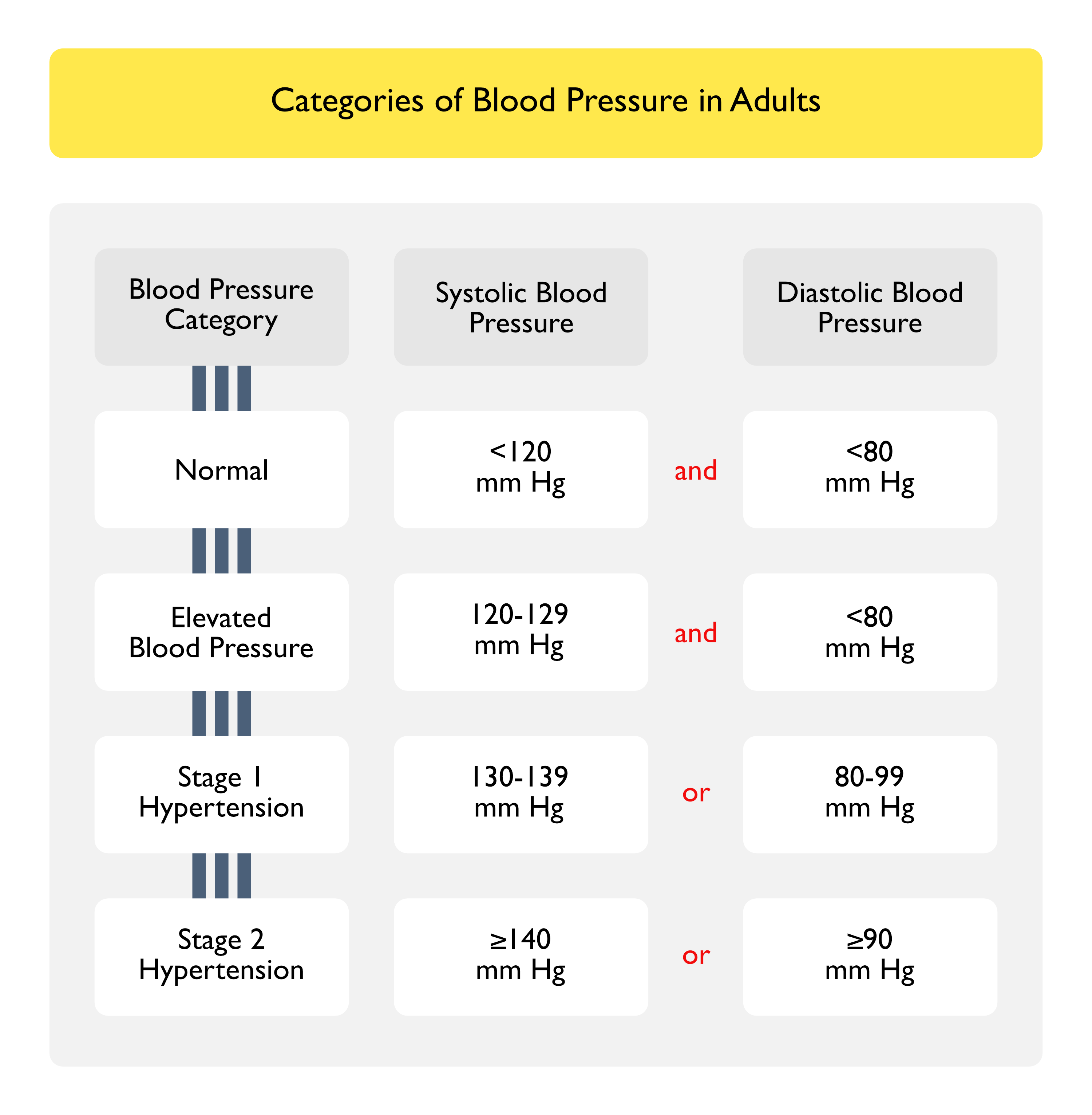
Classification of High Blood Pressure
In Adults, Blood Pressure Should Be Categorized as Normal, Elevated, Stage 1, Stage 2 Hypertension to Prevent and Treat High Blood Pressure (Class of Recommendation: 1; Level of Evidence: B-NR)
Normal
Systolic Blood Pressure (SBP) <120 mm Hg and Diastolic Blood Pressure (DBP) <80 mm Hg
Elevated Blood Pressure
Systolic Blood Pressure (SBP) 120-129 mm Hg and Diastolic Blood Pressure (DBP) <80 mm Hg
Stage 1 Hypertension
Systolic Blood Pressure (SBP) 130-139 mm Hg or Diastolic Blood Pressure (DBP) 80-89 mm Hg
Stage 2 Hypertension
Systolic Blood Pressure (SBP) ≥140 mm Hg or Diastolic Blood Pressure (DBP) ≥90 mm Hg
Diagnostic Testing
Recommendations-2025 AHA/ACC/AANP/AAPA/ABC/ACCP/ACPM/AGS/AMA/ASPC/NMA/PCNA/SGIM Guideline for the Prevention, Detection, Evaluation and Management of High Blood Pressure in Adults (Circulation, 2025) MEDLINE]
Patient Evaluation (Including Laboratory Tests and Other Diagnostic Procedures)
For Adults Who are Diagnosed with Hypertension, the Following Diagnostic Testing Should Be Performed to Optimize Management (Class of Recommendation: 1; Level of Evidence: C-EO)
Arterial Line (see Arterial Line) Arterial Lines are Preferred for Monitoring the Rate of Blood Pressure Decline and the Use of Intravenous Antihypertensive Medications in the Setting of Hypertensive Emergency Studies Have Found that When Blood Pressures are >180/100 mm Hg in Critical Care or Surgical Inpatient Populations, Oscillometric Devices May Underestimate Blood Pressure by as Much as 50/30 mm Hg, as Compared with Blood Pressure Measured by an Arterial Line (Anesthesiology, 2011) [MEDLINE] (Sci World J, 2014) [MEDLINE] Even Research-Quality Manual Auscultatory Methods with Aneroid or Mercury Devices Exhibit Notable Discrepancies, as Compared to Arterial Line Readings (Crit Care Med, 2013 [MEDLINE] (J Hypertens, 2017) [MEDLINE]
Unprovoked/Excessive Hypokalemia (see Hypokalemia)
Cardiovascular Manifestations
General Comments
Relationship Between Hypertension and Fatal/NonFatal Cardiovascular Disease Events
Blood Pressure is Associated with Fatal/NonFatal Cardiovascular Disease Events in a Graded, Log-Linear Fashion, with an Approximate Doubling of Risk for Each 20 mm Hg Higher in the Systolic Blood Pressure and 10 mm Hg Higher Diastolic Blood Pressure (Hypertension, 2018) [MEDLINE] (Circulation, 2025) MEDLINE]
In Patients without Major Risk Factors, Relative Cardiovascular Disease Event Rates Increase, Starting at Systolic Blood Pressure Levels as Low as 90 mm Hg
Higher Blood Pressure is Associated with an Increased Risk for Total Cardiovascular Disease, Coronary Artery Disease (CAD), Congestive Heart Failure (CHF), Aortic and Peripheral Artery Disease (PAD), Chronic Kidney Disease (CKD), Ischemic and Hemorrhagic Stroke, Dementia, and Cognitive Impairment
Among Middle-Aged and Older Adults, the Prevalence and Risks Associated with Higher Systolic Blood Pressure are Greater than the Prevalence and Risks Associated with Higher Diastolic Blood Pressure
Once Blood Pressure is Above Normal (Systolic Blood Presssure ≥120 mm Hg or Diastolic Blood Pressure ≥80 mm Hg), There May Be Irreversible Vascular Damage and Residual Risk, Even if Antihypertensive Treatment is Initiated
Patients with a Diagnosis of Hypertension Who Have Treated Systolic Blood Pressure/Diastolic Blood Pressure Levels <120/80 mm Hg Have 2x the Risk for Cardiovascular Disease Events of Adults without Hypertension Who Have Untreated Systolic Blood Pressure/Diastolic Blood Pressure Levels <120/80 mm Hg,, Highlighting the Importance of Primary Hypertension Prevention
Left Ventricular Hypertrophy is Associated with Body Size (Particularly Lean Body Mass), Tobacco Use, Heart Rate (Inverse Relationship), and Longstanding Diabetes Mellitus
Electrocardiographic Criteria for Left Ventricular Hypertrophy Correlate Weakly with Echocardiographic and Cardiac MRI Definitions of Left Ventricular Hypertrophy and are Less Strongly Associated with Adverse Cardiovascular Disease Outcomes
Clinical
Left Ventricular Hypertrophy (LVH) is a Secondary Manifestation of Hypertension and is an Independent Predictor of Cardiovascular Events
Blood Pressure Reduction Results in a Decrease in Left Ventricular Mass (Which Decreases the Risk of Cardiovascular Disease, Even in the Absence of Decrease in Blood Pressure)
Angiotensin Converting Enzyme Inhibitors (ACE-I), Angiotensin Receptor Blockers (ARB’s), and Calcium Channel Blockers are Superior to β-Blockers in Terms of Effectiveness in Decreasing Left Ventricular Hypertrophy (Hypertension, 2018) [MEDLINE]
Meta-Analysis of Alzheimer and Non-Alzheimer Dementia Risk in Patients with Hypertension (Neurology, 2024) [MEDLINE]: n = 31,250 (from 14 countries)
Participants with Untreated Hypertension had a 36% (Hazard Ratio 1.36; 95% CI: 1.01-1.83, p = 0.0406) and 42% (Hazard Ratio 1.42; 95% CI: 1.08-1.87, p = 0.0135) Increased Risk of Alzheimer Dementia, as Compared with Healthy Controls and Those with Treated Hypertension, Respectively
Compared with Healthy Controls, Both Those with Treated Hypertension (Hazard Ratio 1.29; 95% CI: 1.03-1.60, p = 0.0267) and Untreated Hypertension (Hazard Ratio 1.69: 95% CI: 1.19-2.40, p = 0.0032) Had Greater Non-Alzheimer Dementia Risk, But There was No Difference Between the Treated and Untreated Groups
Baseline Diastolic Blood Pressure Had a Significant U-Shaped Relationship (p = 0.0227) with Non-Alzheimer Dementia Risk in an Analysis Restricted to Those with 5 yr Follow-Up, But Otherwise There was No Significant Relationship Between Baseline Blood Pressure and Either Alzheimer or Non-Alzheimer Dementia Risk
Antihypertensive Use was Associated with Decreased Alzheimer Dementia Risk (But Not Non-Alzheimer Dementia Risk) Throughout Late Life
Treating Hypertension Throughout Late Life Continues to Be Crucial in Alzheimer Dementia Risk Mitigation
Obstructive Sleep Apnea (OSA) is Independently Associated with an Increased Risk of Chronic Kidney Disease in Hypertension (Sleep Med, 2023) [MEDLINE]
Clinical
XXXXXXX
Other Manifestations
XXXXX
xxx
Clinical Manifestations of Hypertension in Pregnancy (see Pregnancy)
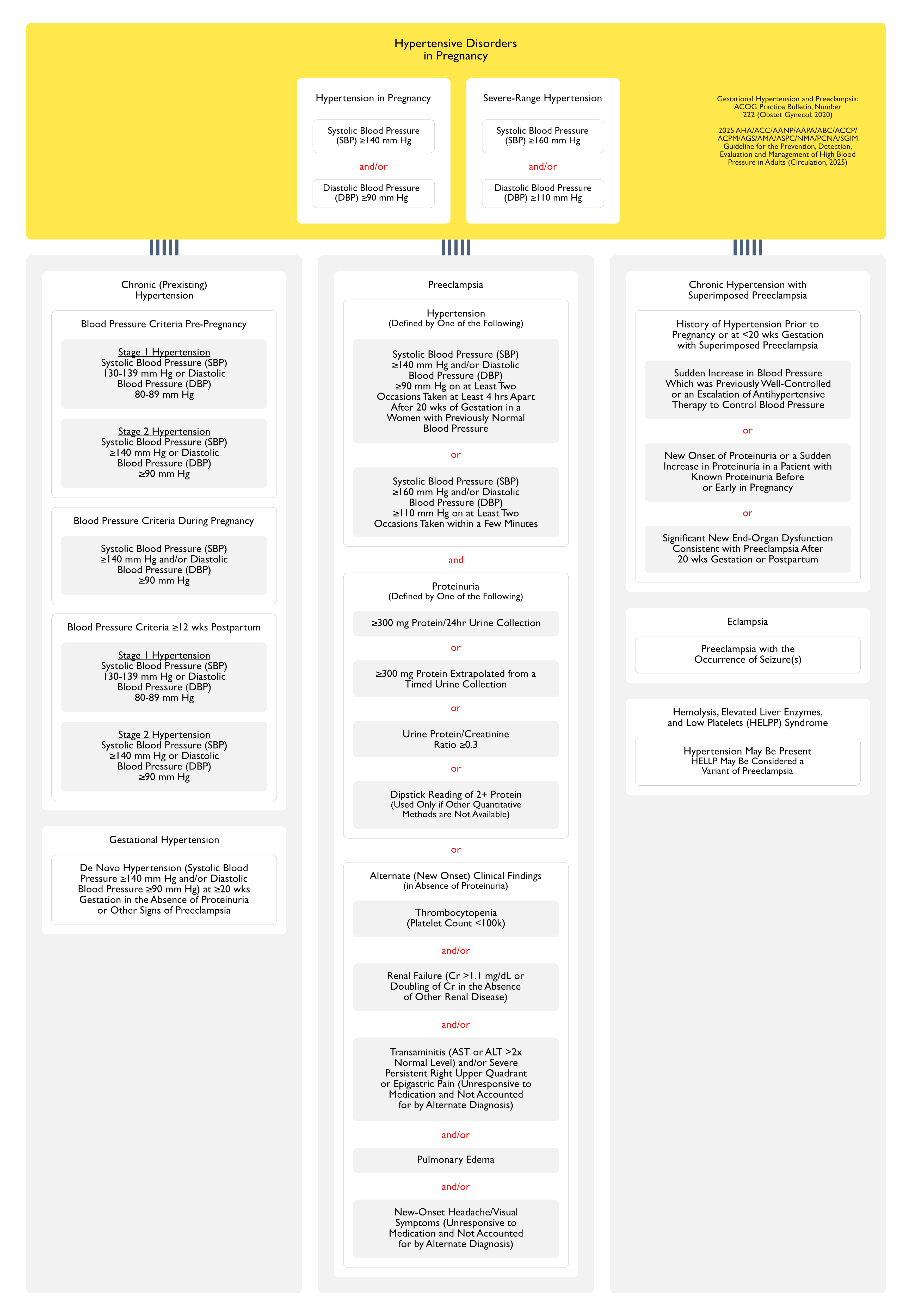
American College of Gynecology Diagnostic Criteria for Hypertension in Pregnancy (Circulation, 2025) MEDLINE]
Hypertension in Pregnancy
Systolic Blood Pressure (SBP) ≥140 mm Hg and/or Diastolic Blood Pressure (DBP) ≥90 mm Hg
Severe-Range Hypertension
Systolic Blood Pressure (SBP) ≥160 mm Hg and/or Diastolic Blood Pressure (DBP) ≥110 mm Hg
Classification of Hypertensive Disorders in Pregnancy (Obstet Gynecol, 2020) [MEDLINE] (Circulation, 2025) [MEDLINE]
Chronic (Preexisting) Hypertension
Diagnosis of Hypertension Prior to Pregnancy or at <20 wks Gestation
Blood Pressure Criteria Pre-Pregnancy
Stage 1 Hypertension
Systolic Blood Pressure (SBP) 130-139 mm Hg or Diastolic Blood Pressure (DBP) 80-89 mm Hg
Stage 2 Hypertension
Systolic Blood Pressure (SBP) ≥140 mm Hg or Diastolic Blood Pressure (DBP) ≥90 mm Hg
Blood Pressure Criteria During Pregnancy
Systolic Blood Pressure (SBP) ≥140 mm Hg and/or Diastolic Blood Pressure (DBP) ≥90 mm Hg
Blood Pressure Criteria ≥12 wks Postpartum
Stage 1 Hypertension
Systolic Blood Pressure (SBP) 130-139 mm Hg or Diastolic Blood Pressure (DBP) 80-89 mm Hg
Stage 2 Hypertension
Systolic Blood Pressure (SBP) ≥140 mm Hg or Diastolic Blood Pressure (DBP) ≥90 mm Hg
Gestational Hypertension
De Novo Hypertension (Systolic Blood Pressure ≥140 mm Hg and/or Diastolic Blood Pressure ≥90 mm Hg) at ≥20 wks Gestation in the Absence of Proteinuria or Other Signs of Preeclampsia
Systolic Blood Pressure (SBP) ≥140 mm Hg and/or Diastolic Blood Pressure (DBP) ≥90 mm Hg on at Least Two Occasions Taken at Least 4 hrs Apart After 20 wks of Gestation in a Women with Previously Normal Blood Pressure
Systolic Blood Pressure (SBP) ≥160 mm Hg and/or Diastolic Blood Pressure (DBP) ≥110 mm Hg on at Least Two Occasions Taken within a Few Minutes
Proteinuria (Defined by One of the Following (see Proteinuria)
≥300 mg Protein/24hr Urine Collection
≥300 mg Protein Extrapolated from a Timed Urine Collection)
Urine Protein/Creatinine Ratio ≥0.3
Dipstick Reading of 2+ Protein (Used Only if Other Quantitative Methods are Not Available)
Alternate (New Onset) Clinical Findings in the Absence of Proteinuria (These are Considered Severe Features of Preeclampsia)
Transaminitis (AST or ALT >2x Normal Level) and/or Severe Persistent Right Upper Quadrant or Epigastric Pain (Unresponsive to Medication and Not Accounted for by Alternate Diagnosis) (see Increased Liver Function Tests)
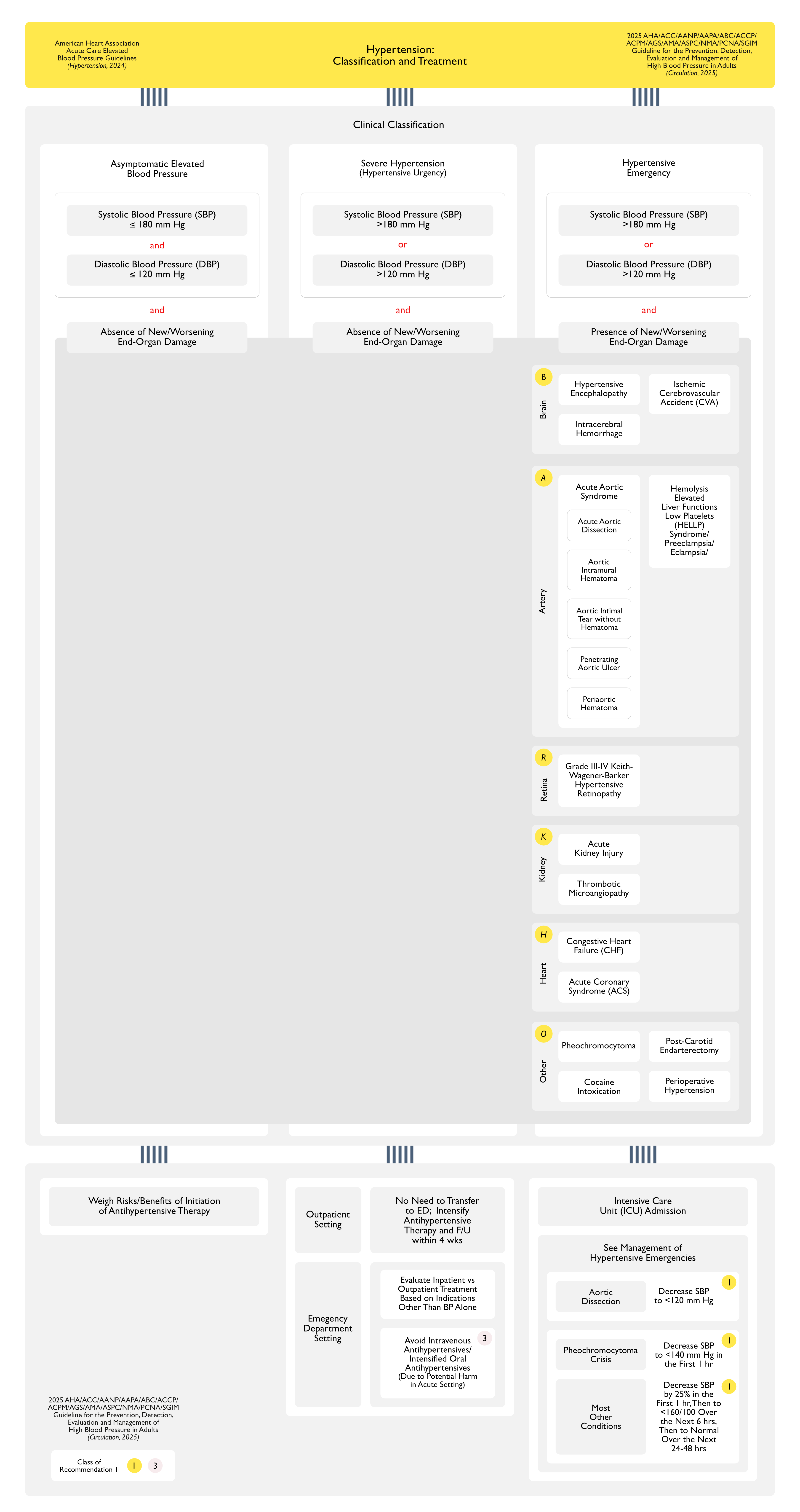
Systolic Blood Pressure (SBP) >180 mm Hg or Diastolic Blood Pressure (DBP) >120 mm Hg without Evidence of New/Worsening Target-Organ Damage
Asymptomatic Elevated Inpatient Blood Pressure
Systolic Blood Pressure (SBP) ≥130 mm Hg or Diastolic Blood Pressure (DBP) ≥80 mm Hg without Evidence of New/Worsening Target-Organ Damage
Assessment for Target-Organ Damage
BARKHO Acronym
Brain
Arteries
Retina
Kidney
Heart
Other
Relationship of Clinical Symptoms to Blood Pressure
Blood Pressure-Related Target-Organ Damage May be Present Even with Systolic Blood Pressure (SBP) ≤180 mm Hg and Diastolic Blood Pressure (DBP) ≤110 mm Hg
Specific Clinical Symptoms (Chest Pain, Dyspnea, Focal Neurological Symptoms, and/or Headache) were More Common in Patients with Hypertensive Emergency, as Compared to Hypertensive Urgency (J Hypertens, 2020) [MEDLINE]
Brain Manifestations
Hypertensive Encephalopathy
Epidemiology
Systematic Review and Meta-Analysis (8 Studies) of Hypertensive Urgency/Emergency Patients Presenting to the Emergency Department (J Hypertens, 2020) [MEDLINE]
Acute Heart Failure/Cardiogenic Pulmonary Edema: accounted for 32% of hypertensive emergency presentations
Ischemic Cerebrovascular Accident: accounted for 29% of hypertensive emergency presentations
Acute Coronary Syndrome: accounted for 18% of hypertensive emergency presentations
Hemorrhagic Stroke: accounted for 11% of hypertensive emergency presentations
Acute Aortic Syndrome: accounted for 2% of hypertensive emergency presentations
Hypertensive Encephalopathy: accounted for 2% of hypertensive emergency presentations
Physiology
In the Setting of Severe Hypertension, Cerebral Autoregulation Cannot Prevent an Increase in Intracranial Pressure (ICP), Resulting in Cerebral Edema
Especially in the Posterior Brain Regions, Where Sympathetic Innervation is Less Pronounced Leading to Less Effective Damping of Blood Pressure Oscillations (Brain Res, 1976) [MEDLINE]
Histopathological Changes in Hypertensive Encephalopathy
Hypertensive Encephalopathy is an Etiology of Posterior Reversible Encephalopathy Syndrome (PRES)
Posterior Reversible Encephalopathy Syndrome (PRES is Also Observed in other Disorders Characterized by Acute Microcirculatory Damage (Such as Antiphospholipid Antibody Syndrome, Thrombotic Thrombocytopenic Purpura, Hemolytic Uremic Syndrome, Use of Cytotoxic Drugs, Use of Anti-Angiogenic Drugs, etc)
Systematic Review and Meta-Analysis (8 Studies) of Hypertensive Urgency/Emergency Patients Presenting to the Emergency Department (J Hypertens, 2020) [MEDLINE]
Acute Heart Failure/Cardiogenic Pulmonary Edema: accounted for 32% of hypertensive emergency presentations
Ischemic Cerebrovascular Accident: accounted for 29% of hypertensive emergency presentations
Acute Coronary Syndrome: accounted for 18% of hypertensive emergency presentations
Hemorrhagic Stroke: accounted for 11% of hypertensive emergency presentations
Acute Aortic Syndrome: accounted for 2% of hypertensive emergency presentations
Hypertensive Encephalopathy: accounted for 2% of hypertensive emergency presentations
Epidemiology-Hypertension as a Risk Factor for Ischemic Cerebrovascular Accident (CVA)
Hypertension is a Well-Established Risk Factor for Ischemic Cerebrovascular Accident (CVA)
Systematic Review and Meta-Analysis (8 Studies) of Hypertensive Urgency/Emergency Patients Presenting to the Emergency Department (J Hypertens, 2020) [MEDLINE]
Acute Heart Failure/Cardiogenic Pulmonary Edema: accounted for 32% of hypertensive emergency presentations
Ischemic Cerebrovascular Accident: accounted for 29% of hypertensive emergency presentations
Acute Coronary Syndrome: accounted for 18% of hypertensive emergency presentations
Hemorrhagic Stroke: accounted for 11% of hypertensive emergency presentations
Acute Aortic Syndrome: accounted for 2% of hypertensive emergency presentations
Hypertensive Encephalopathy: accounted for 2% of hypertensive emergency presentations
Epidemiology-Hypertension During the Course of Ischemic Cerebrovascular Accident (CVA)
Hypertension is Common During Ischemic Cerebrovascular Accident (CVA) (Stroke, 2013) [MEDLINE]
In an Observational Study, Systolic Blood Pressure was >139 mm Hg in 77% of Cases and >184 mm HG in 15 of Cases of Ischemic Cerebrovascular Accident (CVA) on Emergency Department Arrival (Am J Emerg Med, 2007) [MEDLINE]
Physiology
Theoretically, Moderate Hypertension During Acute Ischemic Cerebrovascular Accident (CVA) Might Be Advantageous by Improving Cerebral Perfusion of the Ischemic Tissue
However, Hypertension Might Be Detrimental by Exacerbating Cerebral Edema and Hemorrhagic Transformation of the Ischemic Tissue
Extreme Hypertension is Clearly Detrimental, as it Decreases Perfusion of the Ischemic Brain (and Other Organs), Exacerbating the Ischemic Brain Injury
Based on the Above Observations and Studies, the Optimal Blood Pressure Range in the Setting of Acute Ischemic Cerebrovascular Accident (CVA) Consists of Systolic Blood Pressure Ranging from 121-200 mm Hg and Diastolic Blood Pressure Ranging from 81-110 mm Hg (Stroke, 2013) [MEDLINE]
However, Elevated In-Hospital Blood Pressure During Acute Ischemic Cerebrovascular Accident (CVA) Has Been Associated with Worse Clinical Outcomes with a More Linear Relationship
Clinical
Blood Pressure is Frequently Higher in Acute Ischemic Cerebrovascular Accident (CVA) Patients with a History of Hypertension than in Patients without Premorbid Hypertension
Blood Pressure Typically Decreases Spontaneously During the Acute Phase of Ischemic Cerebrovascular Accident (CVA), Starting within 90 min After the Onset of Stroke Symptoms
Optimal Blood Pressure Range May Be Dependent on Stroke Subtype and/or Patient-Specific Comorbidities
Systematic Review and Meta-Analysis (8 Studies) of Hypertensive Urgency/Emergency Patients Presenting to the Emergency Department (J Hypertens, 2020) [MEDLINE]
Acute Heart Failure/Cardiogenic Pulmonary Edema: accounted for 32% of hypertensive emergency presentations
Ischemic Cerebrovascular Accident: accounted for 29% of hypertensive emergency presentations
Acute Coronary Syndrome: accounted for 18% of hypertensive emergency presentations
Hemorrhagic Stroke: accounted for 11% of hypertensive emergency presentations
Acute Aortic Syndrome: accounted for 2% of hypertensive emergency presentations
Hypertensive Encephalopathy: accounted for 2% of hypertensive emergency presentations
Microangiopathic Hemolytic Anemia (MAHA) (“Malignant Hypertension”) (see Hemolytic Anemia)
Epidemiology
Microangiopathic Hemolytic Anemia (MAHA) Can Occur with Severe Hypertension (Systolic Blood Pressure >220 mm Hg/Diastolic Blood Pressure >100 mm Hg)
Clarification of the Temporal Relationship Between Hematologic Abnormalities and the Hypertension
Thrombotic Microangiopathy-Associated Acute Kidney Injury (AKI) May Be the Etiology of the Hypertension
However, New/Worsening Hypertension is Also Common in Complement-Mediated Thrombotic Microangiopathy (Occurring in 8-54% of Cases) (see xxxx)
This is Especially True if the Patient is Younger, Has a Poor Response to Antihypertensive Therapy, or if the Thrombotic Microangiopathy Does Not Improve with Antihypertensive Therapy Alone (Clin J Am Soc Nephrol, 2010) [MEDLINE] (Haematologica, 2019) [MEDLINE] (Hypertension, 2020) [MEDLINE]
Physiology
Activation of Pro-Inflammatory and Pro-Coagulant Pathways
Endothelial Detachment is a Pathological Hallmarks of Hypertensive Microangiopathy and is Believed to Result from High Shear Forces
Exposure of Blood to the Subendothelium Results in Coagulation Activation, Platelet Activation, and the Formation of a Fibrin Network
Formation of Platelet-Rich Thrombi with Obliteration of the Microcirculation
Platelet Consumption and Intravascular Hemolysis (Due to Trapping and Destruction of Red Blood Cells within the Fibrin Network)
Diagnosis
Discrimination of Malignant Hypertension from Other Etiologies of Thrombotic Microangiopathy (Such as Thrombotic Thrombocytopenic Purpura and Hemolytic Uremic Syndrome (HUS) May be Difficult
Malignant Hypertension-Associated Thrombotic Microangiopathy is Usually Less Severe, as Compared to Patients with Thrombotic Thrombocytopenic Purpura (TTP) and Hemolytic Uremic Syndrome (HUS)
Malignant Hypertension-Associated Thrombotic Microangiopathy Typically Has Only Moderate Thrombocytopenia and Few Schistocytes on the Peripheral Smear
Additionally, the Coexistence of a Severe Hypertension with Advanced Retinopathy is Usually Sufficient to Discriminate Hypertension-Associated Thrombotic Microangiopathy from Other Etiologies of Thrombotic Microangiopathy
A Disintegrin And Metalloprotease with a Thrombospondin Type 1 Motif, Member 13 (ADAMTS13) Activity (see ADAMTS13 Activity)
Blood Pressure Control Alone Will Usually Result in Clinical Improvement in Malignant Hypertension-Associated Thrombotic Microangiopathy within 24-48 hrs (Whereas, Thrombotic Thrombocytopenic Purpura and Hemolytic Uremic Syndrome Will Require Other Therapies)
Systematic Review and Meta-Analysis (8 Studies) of Hypertensive Urgency/Emergency Patients Presenting to the Emergency Department (J Hypertens, 2020) [MEDLINE]
Acute Heart Failure/Cardiogenic Pulmonary Edema: accounted for 32% of hypertensive emergency presentations
Ischemic Cerebrovascular Accident: accounted for 29% of hypertensive emergency presentations
Acute Coronary Syndrome: accounted for 18% of hypertensive emergency presentations
Hemorrhagic Stroke: accounted for 11% of hypertensive emergency presentations
Acute Aortic Syndrome: accounted for 2% of hypertensive emergency presentations
Hypertensive Encephalopathy: accounted for 2% of hypertensive emergency presentations
Systematic Review and Meta-Analysis (8 Studies) of Hypertensive Urgency/Emergency Patients Presenting to the Emergency Department (J Hypertens, 2020) [MEDLINE]
Acute Heart Failure/Cardiogenic Pulmonary Edema: accounted for 32% of hypertensive emergency presentations
Ischemic Cerebrovascular Accident: accounted for 29% of hypertensive emergency presentations
Acute Coronary Syndrome: accounted for 18% of hypertensive emergency presentations
Hemorrhagic Stroke: accounted for 11% of hypertensive emergency presentations
Acute Aortic Syndrome: accounted for 2% of hypertensive emergency presentations
Hypertensive Encephalopathy: accounted for 2% of hypertensive emergency presentations
Autonomic nerves, mast cells, and amine receptors in human brain vessels. A histochemical and pharmacological study. Brain Res 1976;115:377–393 [MEDLINE]
Prevalence of elevated blood pressure in 563,704 adult patients with stroke presenting to the ED in the United States. Am J Emerg Med. 2007;25:32-38 [MEDLINE]
Antiproteinuric response to dual blockade of the renin-angiotensin system in primary glomerulonephritis: meta-analysis and metaregression. Am J Kidney Dis. 2008;52(3):475 [MEDLINE]
Relative role of genetic complement abnormalities in sporadic and familial aHUS and their impact on clinical phenotype. Clin J Am Soc Nephrol. 2010 Oct;5(10):1844-59 [MEDLINE]
Hypertensive Emergencies in the Emergency Department. Emerg Med Clin North Am. 2015 Aug;33(3):539-51. doi: 10.1016/j.emc.2015.04.005 [MEDLINE]
Guidelines for the Management of Spontaneous Intracerebral Hemorrhage. A Guideline for Healthcare Professionals From the American Heart Association/American Stroke Association. Stroke. 2015;46:2032-2060. DOI: 10.1161/STR.0000000000000069 [MEDLINE]
Diagnostic and therapeutic approach to the hypertensive crisis. Med Clin (Barc). 2018 Apr 23;150(8):317-322. doi: 10.1016/j.medcli.2017.09.027 [MEDLINE]
New Developments in Hypertensive Encephalopathy. Curr Hypertens Rep. 2018 Feb 26;20(2):13. doi: 10.1007/s11906-018-0813-y [MEDLINE]
Hypertensive Emergencies: A Review of Common Presentations and Treatment Options. Cardiol Clin. 2019 Aug;37(3):275-286. doi: 10.1016/j.ccl.2019.04.003 [MEDLINE]
Impact of hypertensive emergency and rare complement variants on the presentation and outcome of atypical hemolytic uremic syndrome. Haematologica. 2019;104(12):2501 [MEDLINE]
Diagnostic and Risk Factors for Complement Defects in Hypertensive Emergency and Thrombotic Microangiopathy. Hypertension. 2020;75(2):422 [MEDLINE]
2022 Guideline for the Management of Patients With Spontaneous Intracerebral Hemorrhage: A Guideline From the American Heart Association/American Stroke Association. Stroke. 2022 Jul;53(7):e282-e361. doi: 10.1161/STR.0000000000000407 [MEDLINE]
The relationship between obstructive sleep apnea and risk of renal impairment in patients with hypertension, a longitudinal study. Sleep Med. 2023 Jun 20;109:18-24. doi: 10.1016/j.sleep.2023.05.020 [MEDLINE]
Blood Pressure, Antihypertensive Use, and Late-Life Alzheimer and Non-Alzheimer Dementia Risk: An Individual Participant Data Meta-Analysis. Neurology. 2024 Sep 10;103(5):e209715. doi: 10.1212/WNL.0000000000209715 [MEDLINE]