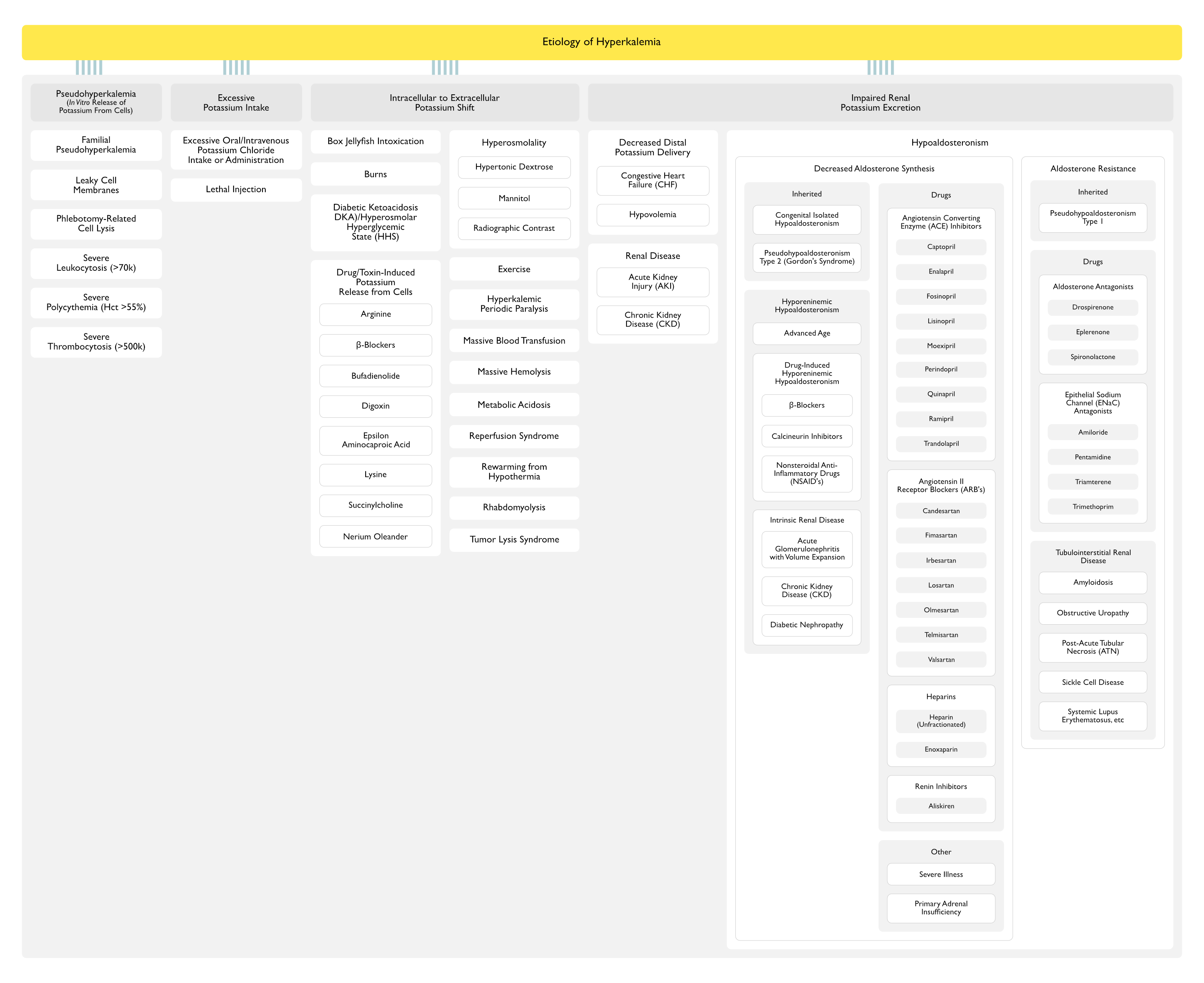
Pseudohyperkalemia (In Vitro Release of Potassium From Cells) (Am J Kidney Dis, 2000) [MEDLINE] (BMJ, 2007) [MEDLINE]
Familial Pseudohyperkalemia
Genetics
Autosomal Dominant Inheritance (Maps to the 16q23–ter Locus)
Mechanism
Abnormally Increased Potassium Permeability of the Red Blood Cell Membrane, Resulting in a Temperature-Dependent Loss of Potassium from Red Blood Cells When Stored at Room Temperature
Clinical
Characterized by Hyperkalemia in Whole Blood Stored at or Below Room Temperature, without Additional Hematologic Abnormalities
Pseudohyperkalemia May Be the Only Clinical Manifestation of the Disorder, or it May Be Accompanied by Abnormal Red Blood Cell Morphology (Stomatocytosis, etc), Varying Degrees of Hemolysis, and/or Perinatal Edema in Specific Kindreds
“Leaky” Cell Membranes
Mechanism
These Patients Appear to Be Prone to Hemolysis During Phlebotomy
Phlebotomy-Related Cell Lysis
Mechanisms
Delay in Processing of Blood Sample (Ann Clin Biochem, 2008) [MEDLINE]
May Result in Red Blood Cell Lysis
Excessive Vacuum with a Very Small Gauge Needle During Phlebotomy
May Result in Red Blood Cell Lysis
Mechanical Trauma During Venipuncture Can Result in the Release of Potassium from Red Blood Cells and a Characteristic Reddish Tint of the Serum (Due to the Concomitant Release of Hemoglobin)
Note that Red-Tinted Serum Can Also Be Seen in the Setting of Severe Intravascular Hemolysis (Rather than Due to a Hemolyzed Specimen), in Which Case the Measured Serum Potassium is Actually the True Circulating Potassium Value (BMJ, 2005) [MEDLINE]
Prolonged Tourniquet Time or Fist-Clenching During Phlebotomy (NEJM, 1990) [MEDLINE]
Exercise Causes Potassium to Move Out of Myocytes (Fist-Clenching During Phlebotomy May Increase Potassium by as Much as 1–2 mmol/L)
If a Tourniquet is Required During Phlebotomy, Tourniquet Should Be Released After the Needle Has Entered the Vein, Followed by Waiting for 1-2 min Before Drawing the Blood Sample
Transportation of Blood Samples in Pneumatic Tube System
Due to Potassium Release from White Blood Cells in Sample
In the Setting of Acute Myeloid Leukemia (AML) (JAMA, 1970) [MEDLINE]
However, Hypokalemia is More Commonly Observed in the Setting of Acute Myeloid Leukemia (AML), Due to the Movement of Potassium into Rapidly Proliferating Cells After the Blood Has Been Drawn (Pseudohypokalemia) or to Renal Potassium Wasting (True Hypokalemia)
In the Setting of Chronic Lymphocytic Leukemia (CLL) with White Blood Cell Count >120,000/μL), Cell Fragility Can Result in Falsely Elevated Potassium Concentrations
Unlike Thrombocytosis, This Type of Pseudohyperkalemia Occurs in Both Serum and Plasma Samples and May Be More Prominent When Blood is Sampled in Heparinized Tubes (Clin Chim Acta, 2008) [MEDLINE]
Centrifugation of a Heparinized Tube Causes In Vitro Cell Destruction and the Release of Potassium as These Cells are Freely Suspended in Plasma
Accurate Assessment of the Potassium Concentration in This Setting Requires Allowing Clotting to Separate Serum (Plasma without the Clotting Factors) from the Cells Before Centrifugation (the Fibrin Clot Entraps and Protects Fragile Leukemic Cells, Minimizing Cell Lysis)
Pseudohyperkalemia in the Setting of Very High White Blood Cell Counts (Due to Leukemia or Lymphoma) Has Also Been Reported After Mechanical Disruption of White Blood Cells During Transport of a Blood Sample Via a Pneumatic Tube System (Am J Kidney Dis, 2005) [MEDLINE] (Am J Hematol, 2009) [MEDLINE]
Due to Potassium Release from Platelets in the Blood Sample
Normally, Potassium Moves Out of Platelets After Blood Clotting Has Occurred (Therefore, the Serum Potassium Value Which is Measured by the Laboratory Normally Exceeds the True Plasma Potassium Value 0.1-0.5 mEq/L) (Am J Kidney Dis, 1988) [MEDLINE]
For Every 100 x 10(9)/L of Platelets, Potassium Increases Approximately 0.07 to 0.15 mmol/L (Am J Kidney Dis, 1988) [MEDLINE]
In One Study, Hyperkalemia in a Serum Sample Occurred in 34% of Patients with a Platelet Count >500,000/μL, as Compared to 9% of Patients with a Platelet Count <250,000/μL (Am J Kidney Dis, 1988) [MEDLINE]
The Plasma Potassium Concentration (Assessed by Centrifugation of Heparinized, Unclotted Blood) was Normal
Clinical
Plasma, Rather than Serum, Potassium Should Be Measured (Plasma Potassium Will Be Normal in These Cases)
Excessive Potassium Intake
Excessive Oral/Intravenous Potassium Chloride Intake or Administration
Epidemiology
Associated with Oral/Intravenous Potassium Chloride Administration (see Potassium Chloride)
Associated with Excessive Oral Salt Substitute Intake
Usually Causes Hyperkalemia Only in the Setting of Impaired Renal Function
Associated with Intravenous Total Parenteral Nutriton (TPN) Administration (see Total Parenteral Nutriton)
Mechanism
Excessive Potassium Content (Relative to the Patient’s Renal Function)
May Be Patient-Related (in the Outpatient Setting) or Iatrogenic (in the Inpatient Setting)
Lethal Injection
Mechanism
Capital Punishment Technique Uses Lethal Injection of Potassium Chloride
A nomogram to identify hyperkalemia risk in patients with advanced chronic kidney disease. Kidney360 September 2022. doi:10.34067/KID.0004752022 [MEDLINE]
Low or Low-Normal Plasma Renin Activity and Aldosterone Level
Metabolic Acidosis
Normal Renal Function
Hyporeninemic Hypoaldosteronism
General Comments
Hyporeninemic Hypoaldosteronism is Characterized by a Combination of Decreased Renin Release and an Intra-Adrenal Defect, Resulting in Decreased Systemic and Intra-Adrenal Angiotensin II Synthesis, Culminating in Decreased Aldosterone Secretion
The Intra-Adrenal Defect May Be Related to the Local Renin-Angiotensin System (This is Supported by the Fact that Angiotensin II Produced Locally Within the Adrenal Gland May Stimulate the Release of Aldosterone)
Many of These Patients May Also Have Decreased Aldosterone Responsiveness, Since They Require a Higher Mineralocorticoid Dose for Physiologic Replacement
Dose-Dependent COX-Inhibition, Resulting in Decreased Renal Prostaglandin Synthesis (Since PGI2 Stimulates the Juxtaglomerular Cells in the Kidney to Release Renin, This Results in Decreased Renal Renin Secretion)
Additionally, Impaired Angiotensin II-Induced Release of Aldosterone May Occur
NSAID-Induced Decrease in Glomerular Filtration Rate May Also Contribute to the Development of Hyperkalemia
Angiotensin Converting Enzyme Inhibitors Decrease the Conversion of Angiotensin I to Angiotensin II Systemically (and Possibly Within the Adrenal Zona Glomerulosa)
Since the Normal Stimulatory Effect of Hyperkalemia on Aldosterone Release May Be Mediated in Part by the Adrenal Generation of Angiotensin II, ACE Inhibitors Can Decrease Both Angiotensin II-Mediated and Potassium-Mediated Aldosterone Release
In Contrast to ARB’s and Renin Inhibitors, ACE Inhibitors Increase Renin Levels
Heparins Have a Direct Toxic Effect on the Adrenal Zona Glomerulosa Cells (This May Be Mediated by a Decrease in the Number and Affinity of Adrenal Angiotensin II Receptors)
May Occur Even with the Low Doses of Heparin Used for Deep Venous Thrombosis Prophylaxis
In Contrast, Pituitary Disease Does Not Result in Hypoaldosteronism, Since Corticotropin (ACTH) Does Not Play a Major Role in the Regulation of Aldosterone Release
Aldosterone Resistance
Inherited Disorders
Pseudohypoaldosteronism Type 1
Subtypes
Autosomal Recessive Pseudohypoaldosteronism Type 1
Autosomal Dominant/Sporadic Pseudohypoaldosteronism Type 1
Epithelial Sodium Channel (ENaC) Antagonists Act to Close Sodium Channels on the Luminal Membrane of Collecting Tubule Cells (Collecting Tubule is the Site of Action of Aldosterone)
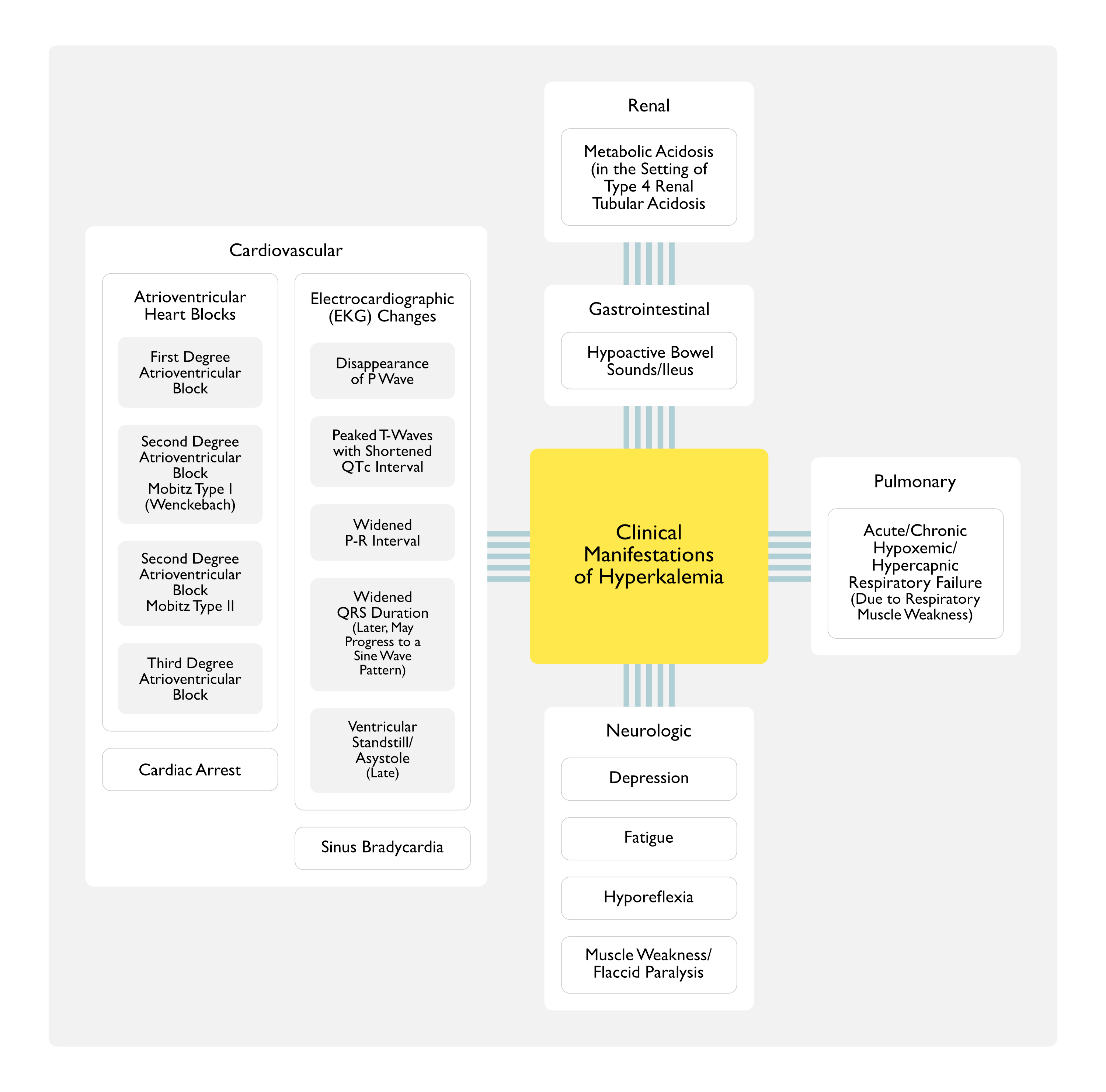
In Type 4 Renal Tubular Acidosis in Animal Models, Hyperkalemia Decreases Proximal Tubule Ammonia Generation and Collecting Duct Ammonia Transport, Leading to Impaired Ammonia Excretion Which Causes Metabolic Acidosis (J Am Soc Nephrol, 2018) [MEDLINE]
Weight-Based Intravenous Insulin Dosing (0.1 U/kg up to maximum of 10 U) for Hyperkalemia Decreases the Risk of Hypoglycemia (J Hosp Med, 2016) [MEDLINE]
Metabolic Alkalosis (see Metabolic Alkalosis): reported when kayexelate has been given in combination with non-absorbable cation-donating antacids and laxatives (such as magnesium hydroxide and aluminum carbonate)
Management of Hyperkalemia in Cardiorenal Patients on Renin–Angiotensin–Aldosterone System Inhibitors
Recommendations of International Delphi Consensus for Management of Hyperkalemia in Patients with Cardiorenal Syndrome (Eur J Heart Fail, 2022) [MEDLINE]
Risk Factors and Risk Stratification for Managing Hyperkalemia in the Setting of Cardiorenal Syndrome
Optimizing Renin–Angiotensin–Aldosterone System Inhibitor Therapy Provides Better Patient Outcome
Patients with Chronic Kidney Disease, Heart Failure, or Diabetes Mellitus are at Increased Risk of Hyperkalemia
Renin–Angiotensin–Aldosterone System Inhibitor Use is a Risk Factor for Hyperkalemia
Hyperkalemia Can Be Effectively Managed to Optimize Disease-Modifying Therapies, Which Improve Morbidity, Mortality, and Outcomes
New Risk Prediction Tools are Required if Clinicians are to Fully Individualize Risk Assessment for Patients with Cardiorenal Syndrome
Managing the Risk of Hyperkalemia Should Be Part of the Individualized Care Plan Already in Place or Planned
There is a Need for Consistent Thresholds for Defining and Treating Hyperkalemia Among Sub-Specialties
Hyperkalemia is Associated with Down-Titration or Discontinuation of Renin–Angiotensin–Aldosterone System Inhibitor Therapy
When Managing mild-to-moderate Hyperkalemia in Cardiorenal Patients, Renin–Angiotensin–Aldosterone System Inhibitors Should Be Maintained Due to the Inherent Benefit in This Patient Population
Mild-Moderate Hyperkalemia Should Be Managed without De-Escalating or Discontinuing Renin–Angiotensin–Aldosterone System Inhibitors
Hyperkalemia is a Known and Manageable Side Effect of Renin–Angiotensin–Aldosterone System Inhibitor Treatment
Hyperkalemia Should Be Recognized as a Predictable, Treatable, and Manageable Side Effect of Optimal Heart Failure/Chronic Kidney Disease Therapy
Prevention of Hyperkalemia for At-Risk Cardiorenal Patients
For High-Risk Patients Who are Not Currently Hyperkalemic, Preventative Measures Should Be Considered (Removal of Salt Substitutes from the Diet, Considering Diuretics for Patients with Hypertension or Volume Expansion)
For Those Patients Who have a Known History of Hyperkalemia Preventing Optimization of Renin–Angiotensin–Aldosterone System Inhibitor Therapy, a Novel Potassium Binder Can Be Used to Enable a Trial of Renin–Angiotensin–Aldosterone System Inhibitor Optimization
For High-risk Patients Who are Not Currently Hyperkalemic, the Use of a Novel Potassium Binder Can Be Considered When Starting or Up-Titrating a Renin–Angiotensin–Aldosterone System Inhibitor
Non-Disease-Modifying Therapies Which Cause Hyperkalemia (NSAIDs, Amiloride, and Herbal Supplements) Should Be Avoided in Patients at High-Risk of Hyperkalemia
Low Potassium Diet is Often Advised to Help Manage Potassium Levels, with No or Little Evidence to Support, and is Counter to a Healthy Diet Which is Beneficial to Cardiorenal Patients
In Patients for Whom Dietary Restrictions May Not Be Appropriate or Desirable, the Use of Novel Potassium Binders May Enable a Balanced Diet
Patients at Risk for Hyperkalemia Should Be Monitored Closely with a Strategy in Place to Manage Potassium Levels Effectively
Correction of Hyperkalemia for At-Risk Cardiorenal Patients with Potassium Lowering Therapy
A Reduction in Emergency Department Visits and Unplanned Hospitalizations Due to Complications Associated with Hyperkalemia Should Be a Goal of Good Management
A Goal for the Management of High-Risk Cardiorenal Patients Should Be to Utilize the Maximum Recommended Dose of Renin–Angiotensin–Aldosterone System Inhibitor Therapy
Renin–Angiotensin–Aldosterone System Inhibitor-Induced Hyperkalemia Should Not Be Considered Intolerance Until Other Strategies to Decrease Potassium Have Been Exhausted
De-Escalation or Discontinuation of Renin–Angiotensin–Aldosterone System Inhibitor Therapy is Associated with Worse Cardiovascular and Renal Outcomes in Cardiorenal Patients
Permanent Discontinuation of Renin–Angiotensin–Aldosterone System Inhibitor Therapy Should Only Be Considered as a Last Resort Strategy for Chronic Hyperkalemia
Hyperkalemia Should No Longer Be Seen as a Barrier to Optimization of Guideline-Directed Therapy
Novel Potassium Binders Enable Guideline-Recommended Renin–Angiotensin–Aldosterone System Inhibitor Dosing and the Proven Clinical Benefits
Use of Novel Potassium Binders in Patients with Mild Hyperkalemia Can Enable Guideline-Recommended Doses of Renin–Angiotensin–Aldosterone System Inhibitor Therapy
Renin–Angiotensin–Aldosterone System Inhibitor Use Should Not Be De-Escalated or Discontinued Due to Hyperkalemia Unless Alternative Measures of Hyperkalemia Management Have Been Optimized (Including the Initiation of POtassium Binder Therapy)
Novel Potassium Binders can enable optimization of Renin–Angiotensin–Aldosterone System Inhibitor therapy in a similar way that antiemetics can enable optimization of chemotherapy
Novel Potassium Binders Should Not Need to Demonstrate a Mortality Benefit
They Enable Renin–Angiotensin–Aldosterone System Inhibitor Therapy, Which Have an Already Proven Mortality Benefit
The Use of Sodium Polystyrene Sulfonate Should Be Avoided Due to Concerns with Gastrointestinal Toxicity, Low Compliance Due to Poor Palatability, and is Only Indicated in Severely Oliguric or Anuric Patients
Sodium Polystyrene Sulfonate Should Not Be Used in the Medium or Long-Term as it May Cause Severe Gastrointestinal Side Effects (Including Bowel Necrosis)
Cross-Specialty Alignment of Cardiology and Nephrology
Patients with Cardiorenal Comorbidities Should Be Managed by a Multidisciplinary Team with an Shared Management Plan
Cross-Specialty Alignment Can Enable Optimal Doses of Renin–Angiotensin–Aldosterone System Inhibitors to Be Maintained
Cross-Specialty Management Improves Patient Satisfaction, Patient Outcomes, and Quality of Life
Cross-Specialty Management is a Good Use of Resources and Should Improve Patient Outcomes
Enhanced Communication Between Interdisciplinary Teams Could Improve Patient Outcomes
Cardiology and Nephrology Guidelines Should Contain Consistent Recommendations for the Management of Hyperkalemia
Collaborative Care and Evidence-Based Decision Making (Based on Guidelines and Expert Consensus) is an Example of Best Practice and Patient-Centered Care
Hyperkalemia Should Be Recognized as a Predictable, Treatable, and Manageable Side Effect of Optimal Heart Failure/Chronic Kidney Disease Therapy in People with a History or at High-Risk of Hyperkalemia
Renin–Angiotensin–Aldosterone System Inhibitors Use Should Not Be De-Escalated or Discontinued Due to Hyperkalemia Unless Alternative Measures of Hyperkalemia Management Have Been Optimized
Novel Potassium Binders Should Be the Preferred Agent to Manage Hyperkalemia, and Should Be Used to Enable and Maintain Optimized Renin–Angiotensin–Aldosterone System Inhibitors Therapy
For High-Risk Individuals Who are Currently Not Hyperkalemic, a Thorough History is Critical to Inform Preventative Measures
Closer Cross-Specialty Collaboration Would Help Optimize Outcomes for Individuals with Cardiorenal Disease
Clinical Teams Should Be Encouraged and Supported to Identify Suitable Methods to Achieve This within Their Care Setting
Consistent Treatment Approach Should Be the Goal of New and Updated Guidelines Which Support People with Cardiorenal Disease, and Cross-Specialty Support Should Be Sought for These to Ensure Aligned Clinical Practice
Methods to Manage Hyperkalemia
Loop and Thiazide Diuretics Can Be Used to Increase Potassium Excretion by Increasing the Delivery of Sodium to the Collecting Ducts
Diuretics are Recommended for Use in Treating Mild-Moderate Hyperkalemia in Individuals with Adequate Renal Function
Diuretics Also Have Utility in Those with Hyperkalemia and Concomitant Volume Overload or Hypertension
Oral Sodium Bicarbonate May Be Considered in Patients with Hyperkalemia and Metabolic Acidosis, Particularly in Those with a Serum Bicarbonate Level of <22 mmol/L, But it is Important to Consider Sodium Load, Particularly in Those at Risk of Fluid Overload
In Those at Risk of Fluid Overload, Concurrent Diuretic Use Should Be Considered
Two Novel Potassium Binders Have Recently Been Developed, Patiromer (Veltassa) and Sodium Zirconium Cyclosilicate (Lokelma)
Both Have Demonstrated Efficacy, and the European Society of Cardiology Heart Failure guidelines (2021) and the Kidney Disease: Improving Global Outcomes (KDIGO) Guidelines for Managing Diabetes in Chronic Kidney Disease (2020) and for Managing Blood Pressure in Chronic Kidney Disease (2021) Recommend Their Use for the Treatment of Renin–Angiotensin–Aldosterone System Inhibitor-Associated Hyperkalemia
Sodium Polystyrene Sulfonate Has Traditionally Been Used to Treat Hyperkalemia, But There are Questions Regarding the Safety and Efficacy of This Agent
References
General
A case of pseudohyperkalaemia and thrombocytosis. Ann Acad Med Singapore. 1998 May;27(3):442-3 [MEDLINE]
Acute hyperkalemia associated with intravenous epsilon-aminocaproic acid therapy. Am J Kidney Dis. 1999 Apr;33(4):782-5 [MEDLINE]
An unusual case of pseudohyperkalaemia. Nephrol. Dial. Transplant. (2003) 18 (8): 1657-1659 [MEDLINE]
Etiology
Studies in disorders of muscle. VII. Clinical manifestations and inheritance of a type of periodic paralysis without hypopotassemia. J Clin Invest. 1951;30(5):492 [MEDLINE]
Periodic paralysis and voltage-gated ion channels. Kidney Int. 1996;49(1):9 [MEDLINE]
Correlating phenotype and genotype in the periodic paralyses. Neurology. 2004;63(9):1647 [MEDLINE]
Review of the Diagnosis and Treatment of Periodic Paralysis. Muscle Nerve. 2018;57(4):522 [MEDLINE]
Clinical
Clinical syndrome of potassium intoxication. Am J Med. 1946;1:337 [MEDLINE]
Hyperkalemia Paralysis Due to Adrenal Insufficiency. Arch Intern Med. 1965;115:418 [MEDLINE]
Muscular paralysis and ventilatory failure caused by hyperkalaemia. Br J Anaesth. 1993;70(2):226[MEDLINE]
How Dangerous Is Hyperkalemia? J Am Soc Nephrol. 2017;28(11):3155 [MEDLINE]
Treatment
Effect of bicarbonate administration on plasma potassium in dialysis patients: interactions with insulin and albuterol. Am J Kidney Dis. 1996 Oct;28(4):508-14 [MEDLINE]
Fludrocortisone for the treatment of heparin-induced hyperkalemia. Ann Pharmacother. 2000 May;34(5):606-10 [MEDLINE]
Patiromer in Patients with Kidney Disease and Hyperkalemia Receiving RAAS Inhibitors. N Engl J Med. 2015 Jan 15;372(3):211-21. doi: 10.1056/NEJMoa1410853. Epub 2014 Nov 21. [MEDLINE]
Weight-based insulin dosing for acute hyperkalemia results in less hypoglycemia. J Hosp Med. 2016 May;11(5):355-7. doi: 10.1002/jhm.2545. Epub 2016 Jan 13 [MEDLINE]
An international Delphi consensus regarding best practice recommendations for hyperkalaemia across the cardiorenal spectrum. Eur J Heart Fail. Published online July 5, 2022. doi:10.1002/ejhf.2612 [MEDLINE]