

History
- Historical Recognition: first recognized in 1950
- Hyponatremia is Common in the Setting of Central Nervous System Disease (Ann Neurol, 1990) [MEDLINE]
- Hyponatremia is Most Commonly Attributed to the Syndrome of Inappropriate Secretion of Antidiuretic Hormone (SIADH) (see Syndrome of Inappropriate Secretion of Antidiuretic Hormone)
- However, Cerebral Salt Wasting is an Additional (Although Less Common) Etiology of Hyponatremia in Patients with Central Nervous System Disease (Especially in Patients with Subarachnoid Hemorrhage)

Etiology
Neurologic Disease
- Brain Tumor
- Carcinomatous Meningitis
- Epidemiology
- Case Reports (Arch Intern Med, 1983) [MEDLINE]
- Epidemiology
- Central Nervous System Surgery
- Epidemiology
- Case Reports (J Endocrinol Invest, 2002) [MEDLINE]
- Epidemiology
- Central Nervous System Tumor
- Epidemiology
- Case Reports
- Epidemiology
- Craniosynostosis Repair
- Drugs
- Trastuzumab (see Trastuzumab)
- Epidemiology
- Case Reports in the Presence of Brain Metastases
- Epidemiology
- Ado-Trastuzumab Emtansine (Kadcyla) (see Ado-Trastuzumab Emtansine)
- Epidemiology
- Case Reports in the Presence of Brain Metastases
- Epidemiology
- Trastuzumab (see Trastuzumab)
- Encephalitis (see Encephalitis)
- Epidemiology
- Case Reports
- Epidemiology
- Intracerebral Hemorrhage (Hemorrhagic Cerebrovascular Accident) (see Intracerebral Hemorrhage)
- Intracranial Surgery
- Ischemic Cerebrovascular Accident (CVA) (see Ischemic Cerebrovascular Accident)
- Poliomyelitis (see Poliomyelitis)
- Epidemiology
- Case Reports
- Epidemiology
- Subarachnoid Hemorrhage (SAH) (see Subarachnoid Hemorrhage)
- Epidemiology
- Common Neurologic Etiology of Cerebral Salt Wasting
- In Patients with Subarachnoid Hemorrhage-Associated Hyponatremia, SIADH Accounts for Approximately 69% of Cases of Hyponatremia, as Compared to Cerebral Salt Wasting Which Accounts for Only 7% of Cases of Hyponatremia (Clin Endocrinol-Oxf, 2006) [MEDLINE]
- In Patients with Subarachnoid Hemorrhage, Hyponatremia Occurs in 49% of Cases (J Clin Endocrinol Metab, 2014) [MEDLINE]
- In This Study, Hyponatremia was Attributable to SIADH in 71% of Cases, to Glucocorticoid Deficiency in 8% of Cases, and to Cerebral Salt Wasting in None of the Cases
- All Patients in the Study were Serially Evaluated for Volume Status, Plasma Cortisol, Arginine Vasopressin, and Brain Natriuretic Peptide
- Epidemiology
- Traumatic Brain Injury (TBI) (see Traumatic Brain Injury)
- Infectious Meningitis
- Bacterial Meningitis (see Meningitis)
- Epidemiology
- Case Reports (Acta Paediatr, 1997) [MEDLINE]
- Epidemiology
- Tuberculous Meningitis (see Tuberculosis)
- Epidemiology
- Case Reports (Anaesth Intensive Care, 1998) [MEDLINE]
- Epidemiology
- Bacterial Meningitis (see Meningitis)
- Other Neurologic Disorders
Non-Neurologic Disease
- Femoral Fracture (Kidney Int, 2007) [MEDLINE]
- Epidemiology
- Case Report
- Epidemiology
Physiology
Potential Mechanisms
- General Comments
- Cerebral Salt Wasting May Be a Protective Mechanism, Since Salt Wasting a Hypovolemia May Limit Rises in Intracranial Pressure
- Renal Salt Wasting Results in Hypovolemia, Which Induces a Baroreceptor-Mediated Stimulus for Antidiuretic Hormone Secretion
- ADH Release Then Impairs Renal Ability to Create a Dilute Urine, Resulting in Hyponatremia
- Secretion of Brain Natriuretic Peptide (BNP) (or Possibly a Ouabain-Like Peptide) by Hormone-Producing Neurons in the Brain: most likely mechanism
- Brain Natriuretic Peptide Decreases Renal Tubular Sodium Reabsorption (Lancet, 1997) [MEDLINE] (Crit Care Med, 2002) [MEDLINE] (NEJM, 1998) [MEDLINE]
- Brain Natriuretic Peptide Inhibits Renin Release (Lancet, 1997) [MEDLINE] (NEJM, 1998) [MEDLINE]
- Brain Natriuretic Peptide Decreases Autonomic Outflow Via Effects on the Brainstem (Am J Physiol, 1991) [MEDLINE] (NEJM, 1998) [MEDLINE]
- Disruption of Neural Input to the Kidney
- Sympathetic Nervous System Enhances Proximal Tubular Sodium, Water, and Uric Acid Reabsorption
- Sympathetic Nervous System Enhances Renin Release
- Consequently, Impaired Sympathetic Neural Output Results in Increased Sodum/Water/Uric Acid Loss in the Urine, as Well as Impaired Renin-Aldosterone Release
- The Failure of Aldosterone to Increase in Response to Hypovolemia Explains the Absence of Potassium Wasting (Despite an Increase in Distal Sodium Delivery)
Diagnosis
Urine Sodium (see Urine Sodium)
- Urine Sodium: increased (usually >40 mEq/L)
Serum Osmolality (see Serum Osmolality)
- Decreased
Urine Osmolality (see Urine Osmolality)
- Urine Osmolality: high (>100 mOsm/kg and usually >300 mOsm/kg)
Serum Uric Acid (see Serum Uric Acid)
- Decreased: due to urate wasting in the urine
Diagnostic Strategies to Differentiate Cerebral Salt Wasting from Syndrome of Inappropriate Antidiuretic Hormone Secretion (see Syndrome of Inappropriate Antidiuretic Hormone Secretion)
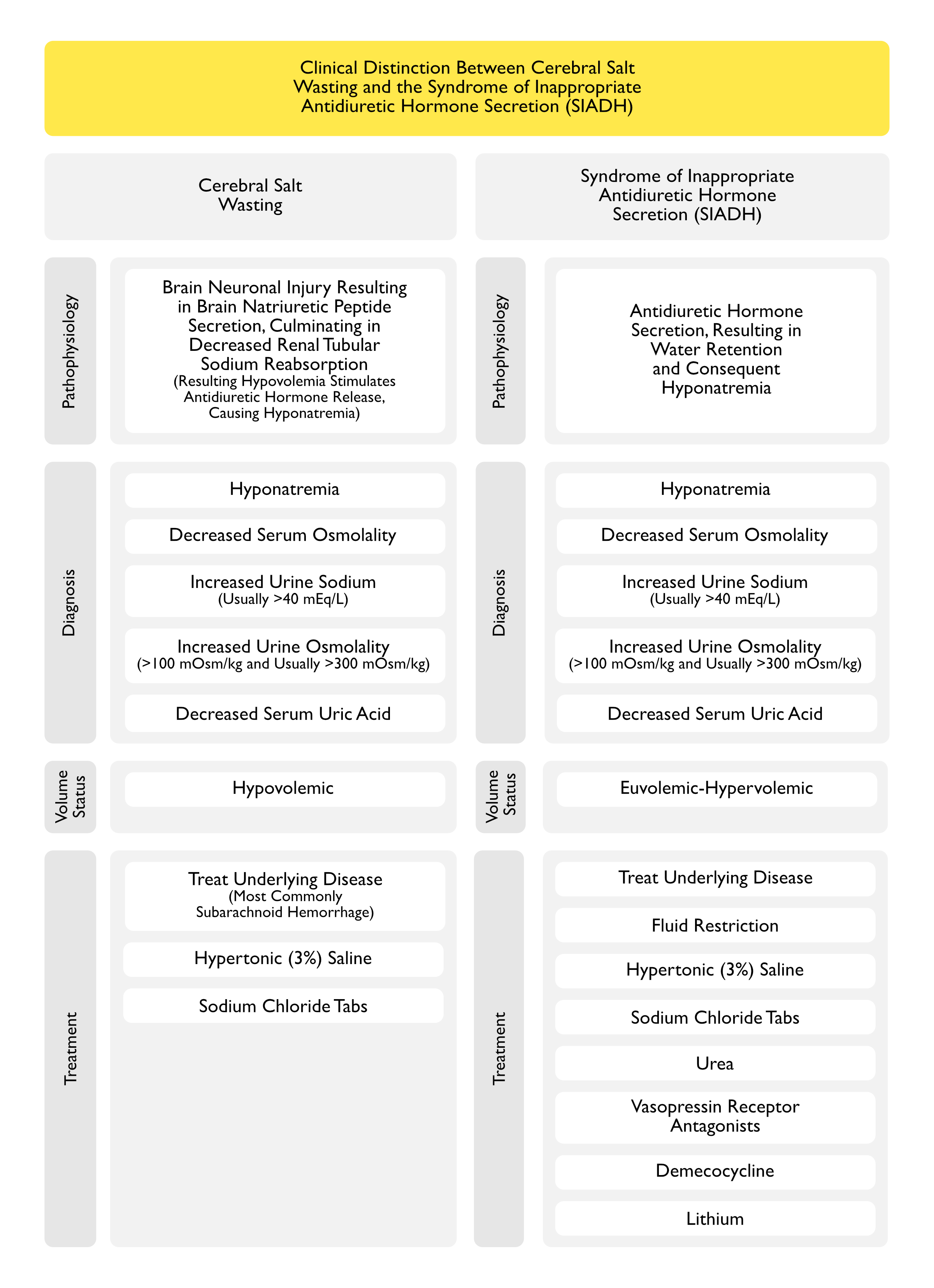
Cerebral Salt Wasting and the Syndrome of Inappropriate Antidiuretic Hormone Secretion Share the Following Clinical Features (see Syndrome of Inappropriate Antidiuretic Hormone Secretion)
- Hyponatremia with Increased ADH Release and Inappropriately Increased Urine Osmolality
- Hyponatremia Would Normally Inhibit ADH Release
- The Increased ADH Release is an Appropriate Response in Cerebral Salt Wasting, But is an Inappropriate Response in SIADH
- Increased Urine Sodium (Usually >40 mEq/L)
- In Cerebral Salt Wasting, This is Due to Renal Salt Wasting
- In SIADH, This is Due to Volume Expansion
- Decreased Serum Uric Acid Due to Decreased Urinary Uric Acid Excretion
- In Cerebral Salt Wasting, This is Likely Due to BNP
- In SIADH, This is Likely Due to Volume Expansion and a Direct Effect of ADH on the V1 Receptor (Am J Kidney Dis, 1992) [MEDLINE]
Cerebral Salt Wasting from Syndrome of Inappropriate Antidiuretic Hormone Secretion (SIADH) are Distinguished by the Following Clinical Features (see Syndrome of Inappropriate Antidiuretic Hormone Secretion)
- In Cerebral Salt Wasting, Clinical Hypovolemia is Present
- In SIADH, Extracellular Fluid Volume is Normal-Slightly Increased
Trial of Isotonic Normal Saline
- In Theory, a Trial of Isotonic/Normal Saline Might Help Differentiate Cerebral Salt Wasting from Syndrome of Inappropriate Antidiuretic Hormone Secretion (SIADH) for the Following Reasons
- Restoration of Euvolemia in Cerebral Salt Wasting Should Remove the Stimulus for Antidiuretic Hormone Release, Resulting in a Dilute Urine and Correction of the Hyponatremia (Curr Opin Nephrol Hypertens, 2020) [MEDLINE]
- However, This Has Not Been Documented to Occur in Cerebral Salt Wasting
- Also, a Lack of Urinary Dilution Does Not Necessarily Preclude the Diagnosis of Cerebral Salt Wasting, Since Patients with Subarachnoid Hemorrhage May Also Have SIADH
- In Contrast, Isotonic/Normal Saline Often Worsens the Hyponatremia in SIADH, as the Salt is Excreted and Some of the Water is Retained
- For This Reason, a Trial of Isotonic/Normal Saline is Discouraged as a Means to Differentiate These Clinical Syndromes
- Restoration of Euvolemia in Cerebral Salt Wasting Should Remove the Stimulus for Antidiuretic Hormone Release, Resulting in a Dilute Urine and Correction of the Hyponatremia (Curr Opin Nephrol Hypertens, 2020) [MEDLINE]
Other Diagnostic Strategies
- While Difficult to Perform, Evidence of Net Negative Sodium Balance Prior to Therapy is Also Consistent with the Diagnosis of Cerebral Salt Wasting
- Calculation of the Sodium Intake Includes that Obtained by Both Oral/Intravenous Routes (Including Sodium supplements, Food, etc), While Sodium Excretion Involves Frequent Measurement of Urine Sodium Concentrations and Measurement of Urine Volume
Clinical Manifestations
Summary of Clinical Features
- Clinical Hypovolemia: this aspect distinguishes cerebral salt wasting from SIADH (see Syndrome of Inappropriate Secretion of Antidiuretic Hormone)
- High Urine Osmolality
- Increased Urine Sodium (Natriuresis)
- Urine Na is Usually >25 mmol/L
- Polyuria (see Polyuria)
Cardiovascular Manifestations
- Hypovolemia (see Hypovolemic Shock)
- Diagnosis
- Presence of Hypovolemia Distinguishes Cerebral Salt Wasting from Syndrome of inappropriate Antidiuretic Hormone Secretion (SIADH), Where the Patient is Typically Euvolemic or Modestly Hypervolemic (see Syndrome of Inappropriate Antidiuretic Hormone Secretion)
- Clinical
- Extracellular Fluid Depletion with Hypotension, Decreased Skin Turgor, and/or Polycythemia
- In the Setting of Subarachnoid Hemorrhage
- Hypovolemia May Worsen Cerebral Perfusion
- Hypotension May Precipitate Vasospasm
- Hyponatremia May Worsen Cerebral Edema
- Diagnosis
Renal Manifestations
- Hyponatremia (see Hyponatremia)
- Epidemiology
- Typical Onset is Within the First 10 Days After a Neurosurgical Procedure or Event
- However, Cases Have Been Reported with an Onset One Month Later
- Clinical
- Hyponatremia May Be Moderate-Severe
- Epidemiology
- Polyuria (see Polyuria)
Treatment
Fluid Restriction is Contraindicated (Especially in the Setting of Subarachnoid Hemorrhage (SAH)
- While Fluid Restriction is the Usual First-Line Therapy in the Treatment of SIADH, it is Contraindicated in the Treatment of Cerebral Salt Wasting in Association with Subarachnoid Hemorrhage
- Fluid Restriction May Worsen the Hypovolemia, Cause Hypotension, and Increase the Risk of Cerebral Infarction
Hypertonic (3%) Saline (see Hypertonic Saline)
General Comments
- Some Experts Suggest that the Distinction Between Cerebral Salt Wasting and SIADH in Patients with an Active Intracranial Disease Process is Not Necessary, Since the Patient Will Be Treated with Hypertonic (3%) Saline in Both Cases to Increase the Serum Sodium and Avoid a Decrease in Extracellular Fluid Volume (J Am Soc Nephrol, 2008) [MEDLINE]
- Hypertonic Saline Will Increase the Serum Sodium Concentration in Patients with Either Cerebral Salt Wasting or the Syndrome of Inappropriate Antidiuretic Hormone Secretion (SIADH) (see Syndrome of Inappropriate Antidiuretic Hormone Secretion)
Sodium Chloride Tablets (see Sodium Chloride)
- Salt Tablets Can Be Administered Once the Patient is Able to Take Oral Medications
Fludrocortisone (Florinef) (see Fludrocortisone)
Prognosis
- Resolution Usually Occurs within 3-4 wks (Nephrol Dial Transplant, 2000) [MEDLINE]
References
- A salt-wasting syndrome associated with cerebral disease. Trans Assoc Am Physicians. 1950;63:57-64 [MEDLINE]
- Hyponatremia in intracranial disease: perhaps not the syndrome of inappropriate secretion of antidiuretic hormone (SIADH). J Neurosurg. 1981;55(6):938 [MEDLINE]
- Cerebral salt wasting in a man with carcinomatous meningitis. Arch Intern Med. 1983;143(11):2187 [MEDLINE]
- Volume depletion and natriuresis in patients with a ruptured intracranial aneurysm. Ann Neurol. 1985;18(2):211 [MEDLINE]
- Hyponatremia is associated with cerebral ischemia in patients with aneurysmal subarachnoid hemorrhage. Ann Neurol. 1990;27(1):106 [MEDLINE]
- The effects of treating hypertension following aneurysmal subarachnoid hemorrhage. Clin Neurol Neurosurg. 1990;92(2):111 [MEDLINE]
- Interactions between ANP and ANG II in regulating blood pressure and sympathetic outflow. Am J Physiol. 1991;260(6 Pt 2):R1145 [MEDLINE]
- Abnormal urate transport in patients with intracranial disease. Am J Kidney Dis. 1992;19(1):10 [MEDLINE]
- Management of neurosurgical patients with hyponatremia and natriuresis. Neurosurgery. 1994;34(2):269 [MEDLINE]
- Cerebral salt wasting syndrome: a review. Neurosurgery. 1996 Jan;38(1):152-60 [MEDLINE]
- Another cause of hyponatraemia in patients with bacterial meningitis: cerebral salt wasting. Acta Paediatr. 1997;86(10):1150 [MEDLINE]
- Secretion of brain natriuretic peptide in patients with aneurysmal subarachnoid haemorrhage. Lancet. 1997;349(9047):245 [MEDLINE]
- Acute hyponatraemia secondary to cerebral salt wasting syndrome in a patient with tuberculous meningitis. Anaesth Intensive Care. 1998;26(4):420 [MEDLINE]
- Natriuretic peptides. N Engl J Med. 1998;339(5):321 [MEDLINE]
- Hyponatraemia in a neurosurgical patient: syndrome of inappropriate antidiuretic hormone secretion versus cerebral salt wasting. Nephrol Dial Transplant. 2000;15(2):262 [MEDLINE]
- Fludrocortisone treatment in a child with severe cerebral salt wasting. Pediatr Neurosurg. 2001;35(4):216 [MEDLINE]
- Hyponatremia in the postoperative craniofacial pediatric patient population: a connection to cerebral salt wasting syndrome and management of the disorder. Plast Reconstr Surg. 2001;108(6):1501 [MEDLINE]
- A method to estimate urinary electrolyte excretion in patients at risk for developing cerebral salt wasting. J Neurosurg. 2001;95(3):42 [MEDLINE]
- Management of hyponatraemia in patients with acute cerebral insults. Arch Dis Child. 2001;85(3):246 [MEDLINE]
- Cerebral salt wasting. Indian Pediatr. 2002;39(5):488 [MEDLINE]
- Very delayed hyponatremia after surgery and radiotherapy for a pituitary macroadenoma. J Endocrinol Invest. 2002;25(2):163[MEDLINE]
- Hyponatremia in a pediatric stroke patient: syndrome of inappropriate antidiuretic hormone secretion or cerebral salt wasting? Crit Care Med. 2002;30(4):792 [MEDLINE]
- Hyponatremia in acute brain disease: the cerebral salt wasting syndrome. Eur J Intern Med. 2002 Feb;13(1):9-14 [MEDLINE]
- Prognostic significance of hypernatremia and hyponatremia among patients with aneurysmal subarachnoid hemorrhage. Neurosurgery. 2002;50(4):749 [MEDLINE]
- Cerebral salt wasting: truths, fallacies, theories, and challenges. Crit Care Med. 2002;30(11):2575 [MEDLINE]
- Hyponatremia in patients with central nervous system disease: SIADH versus CSW. Trends Endocrinol Metab. 2003;14(4):182 [MEDLINE]
- The incidence and pathophysiology of hyponatraemia after subarachnoid haemorrhage. Clin Endocrinol (Oxf). 2006;64(3):250 [MEDLINE]
- Controversies in the management of aneurysmal subarachnoid hemorrhage. Crit Care Med. 2006;34(2):511 [MEDLINE]
- Fludrocortisone therapy in cerebral salt wasting. Pediatrics. 2006;118(6):e1904 [MEDLINE]
- The incidence and pathophysiology of hyponatraemia after subarachnoid haemorrhage. Clin Endocrinol (Oxf). 2006;64(3):250 [MEDLINE]
- Impact of medical complications on outcome after subarachnoid hemorrhage. Crit Care Med. 2006;34(3):617 [MEDLINE]
- Cerebral salt-wasting syndrome in a patient with neuroleptic malignant syndrome. Arch Neurol. 2007;64(1):122 [MEDLINE]
- Renal salt wasting without cerebral disease: diagnostic value of urate determinations in hyponatremia. Kidney Int. 2007; 71(8):822-6 [MEDLINE]
- Refractory hyponatremia. Kidney Int. 2007;71(1):79 [MEDLINE]
- Cerebral salt wasting versus SIADH: what difference? J Am Soc Nephrol. 2008;19(2):194 [MEDLINE]
- Cerebral salt wasting syndrome: review. Eur J Intern Med. 2008 Jun;19(4):249-54. doi: 10.1016/j.ejim.2007.06.019 [MEDLINE]
- Is it cerebral or renal salt wasting? Kidney Int. 2009 Nov;76(9):934-8. doi: 10.1038/ki.2009.263. Epub 2009 Jul 29 [MEDLINE]
- Cerebral salt wasting: pathophysiology, diagnosis, and treatment. Neurosurg Clin N Am. 2010 Apr;21(2):339-52. doi: 10.1016/j.nec.2009.10.011 [MEDLINE]
- Hyponatremia following mild/moderate subarachnoid hemorrhage is due to SIAD and glucocorticoid deficiency and not cerebral salt wasting. J Clin Endocrinol Metab. 2014 Jan;99(1):291-8 [MEDLINE]
- Cerebral salt wasting after traumatic brain injury: a review of the literature. Scand J Trauma Resusc Emerg Med. 2015 Nov 11;23:98 [MEDLINE]
- Safety and Efficacy of Fludrocortisone in the Treatment of Cerebral Salt Wasting in Patients With Tuberculous Meningitis: A Randomized Clinical Trial. JAMA Neurol. 2018;75(11):1383 [MEDLINE]
- Inappropriate Antidiuretic Hormone Secretion and Cerebral Salt-Wasting Syndromes in Neurological Patients. Front Neurosci. 2019 Nov 8;13:1170. doi: 10.3389/fnins.2019.01170. eCollection 2019 [MEDLINE]
- Evolution and evolving resolution of controversy over existence and prevalence of cerebral/renal salt wasting. Curr Opin Nephrol Hypertens. 2020;29(2):213 [MEDLINE]