

Clinical-Sepsis Scoring
Systemic Inflammatory Response Syndrome (SIRS) Score
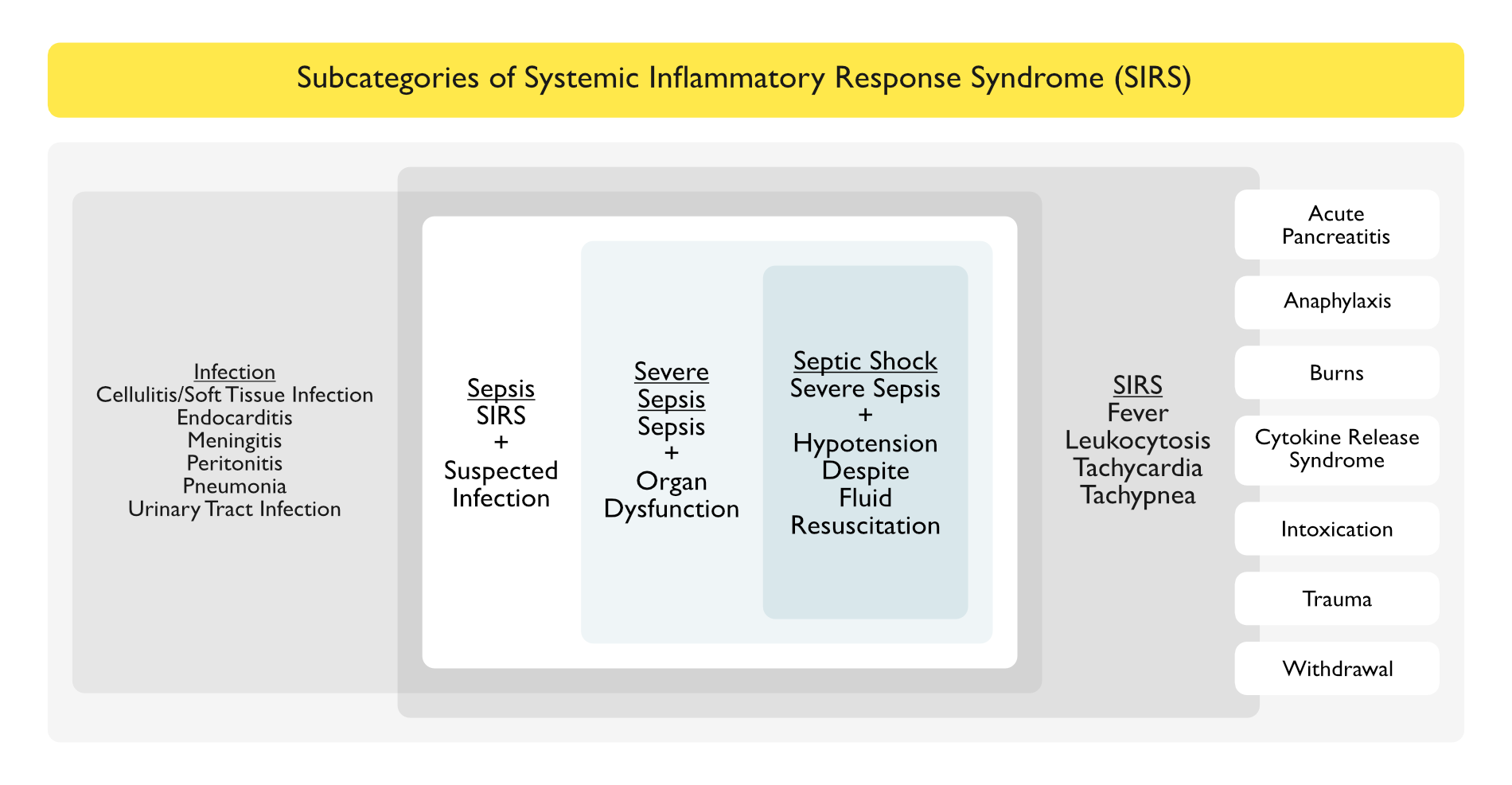
- SIRS Criteria were Originally Developed in 1991 (Chest, 1992) [MEDLINE]
- Severe Sepsis: sepsis complicated by organ dysfunction
- Septic Shock: sepsis-induced hypotension persisting despite adequate fluid resuscitation
- Systemic Inflammatory Response Syndrome (SIRS) Criteria
- Fever (Temperature >100.9° F) or Hypothermia (Temperature <96.8° F)
- Leukocytosis (White Blood Cell >12k) or Leukopenia (WBC <4k) or Bandemia (Bands >10%)
- Tachycardia (Heart Rate >90 bpm)
- Tachypnea (Respiratory Rate >20 breaths/min)
- Sepsis Criteria: including both of the following
- Suspected or Possible Source of Infection
- ≥2 Systemic Inflammatory Response Syndrome (SIRS) Criteria
- Severe Sepsis Criteria: including both of the following
- Sepsis
- Organ Dysfunction as Evidenced by Any of the Following Criteria
- Systolic Blood Pressure <90 or Mean Arterial Pressure <65 or a Systolic Blood Pressure Decrease of >40 mm Hg
- Acute Respiratory Failure as Evidenced by a New Need for Invasive or Noninvasive Mechanical Ventilation
- Serum Creatinine >2.0 or Urine Output <0.5 mL/kg/hr for 2 hrs
- Serum Bilirubin >2 mg/dL
- Platelet Count <100k
- International Normalized Ratio >1.5 or Activated Partial Thromboplastin Time >60 sec (in a Non-Anticoagulated Patient)
- Serum Lactate >2 mmol/L
- Septic Shock Criteria: including both of the following
- Severe Sepsis
- Hypotension Persisting in the Hour After the Intravenous Fluid Bolus as Evidenced By Either
- Systolic Blood Pressure <90 or Mean Arterial Pressure <65 or a Systolic Blood Pressure Decrease of >40 mm Hg
- Tissue Hypoperfusion Present with Initial Serum Lactate Level ≥4 mmol/L
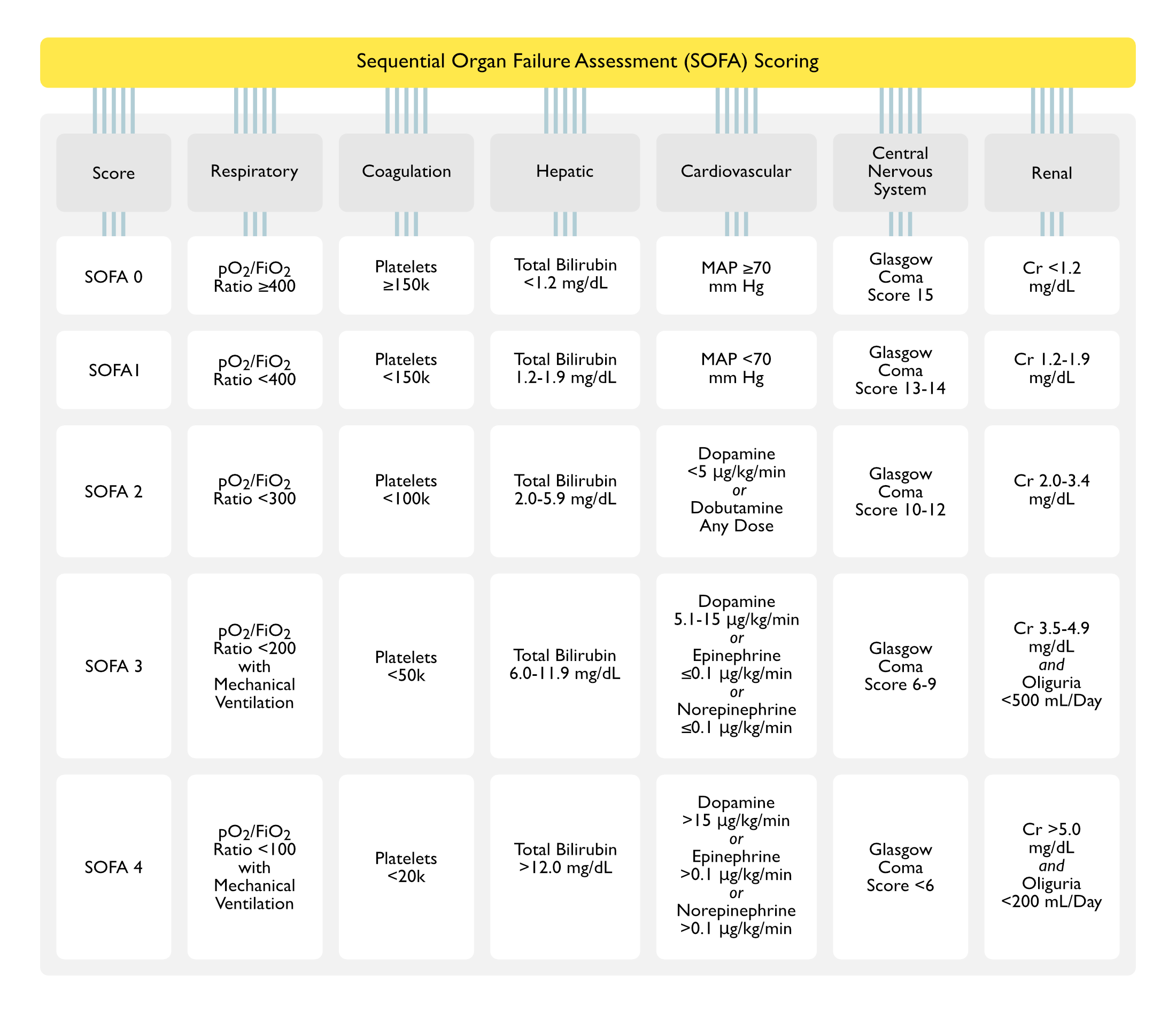
Sequential Organ Failure Assessment (SOFA) Score (Third International Consensus Definitions for Sepsis and Septic Shock, Sepsis-3: Society of Critical Care Medicine and European Society of Intensive Care Medicine; JAMA, 2016) [MEDLINE]
- Background
- The Sequential Organ Failure Assessment (SOFA) Score was Originally Developed (as the “Sepsis-Related Organ Failure Assessment”) in 1994 to Provide a Scoring System for Sepsis Severity (Intensive Care Med, 1996) [MEDLINE] (Crit Care Med. 1998) [MEDLINE]
- SOFA was Developed Using Data from 1,449 Patients in 40 ICU’s in 16 Countries
- SOFA Has Been Used to Predict Mortality from Multiple Organ Failure in a Number of Disorders, Including Sepsis, Acute Liver Failure Associated with Acetaminophen Intoxication, Chronic Liver Failure (CLIF-SOFA), Cancer, Post-Cardiac Surgery, and Post-Hematopoietic Stem Cell Transplant
- In Sepsis, the SOFA Score is Used to Predict Mortality and Should Not Be Used to Diagnose Sepsis
- The Sequential Organ Failure Assessment (SOFA) Score was Originally Developed (as the “Sepsis-Related Organ Failure Assessment”) in 1994 to Provide a Scoring System for Sepsis Severity (Intensive Care Med, 1996) [MEDLINE] (Crit Care Med. 1998) [MEDLINE]
- Calculation
- SOFA Score is Initially Calculated 24 hrs After ICU Admission, then q48hrs Thereafter (Characterizing it as a “Sequential” Score)
- In Sepsis, Baseline SOFA Score Can Be Assumed to Be Zero in Patients Not Known to Have Preexisting Organ Dysfunction
Quick Sequential Organ Failure Assessment (qSOFA) Score
- General Comments
- The qSOFA was Originally Designed and Validated in 2016 as a Tool to Predict Sepsis Mortality Outside of the Intensive Care Unit (JAMA, 2016) [MEDLINE]
- Similar to SOFA, the qSOFA was Not Designed as a Tool to Diagnose Sepsis
- In Patients Outside of the ICU, Any 2 of 3 Clinical qSOFA Variables Offered Predictive Validity (Area Under ROC = 0.81; 95% CI, 0.80-0.82), Similar to that of the Full SOFA Score (JAMA, 2016) [MEDLINE]
- The qSOFA was Originally Designed and Validated in 2016 as a Tool to Predict Sepsis Mortality Outside of the Intensive Care Unit (JAMA, 2016) [MEDLINE]
- Poor Outcome is Associated with at Least Two of the Following Clinical Criteria
- Altered Mental Status (see Altered Mental Status)
- Hypotension (SBP ≤100 mm Hg) (see Hypotension)
- Tachypnea (RR ≥22/min) (see Tachypnea)
National Early Warning Score (NEWS)
Scoring Criteria (Infect Drug Resist, 2020) [MEDLINE]
- Respiratory Rate (Breaths/min)
- ≤8 Breaths/min = 3 pts
- 9-11 Breaths/min = 1 pts
- 12-20 Breaths/min = 0 pt
- 21-24 Breaths/min = 2 pts
- ≥25 Breaths/min = 3 pts
- Oxygen Saturation
- ≤91% = 3 pts
- 92-93% = 2 pts
- 94-95% = 1 pt
- ≥96% = 0 pts
- Any Supplemental Oxygen
- Yes = 2 pts
- No = 0 pts
- Temperature
- ≤35°C = 3 pts
- 35.1-36.0°C = 1 pts
- 36.1-38°C = 0 pts
- 38.1-39.0°C = 1 pts
- ≤39.1°C = 2 pts
- Systolic Blood Pressure (SBP)
- ≤90 mm Hg = 3 pts
- 91-100 mm Hg = 2 pts
- 101-110 = 1 pts
- 111-219 mm Hg = 0 pts
- ≥220 mm Hg = 3 pts
- Heart Rate (Beats/min)
- ≤40 Beats/min = 3 pts
- 41-50 Beats/min = 1 pts
- 51-90 Beats/min = 0 pts
- 91-110 Beats/min = 1 pt
- 111-130 Beats/min = 2 pts
- ≥131 Beats/min = 3 pts
- Level of Consciousness
- Alert = 0 pts
- Unresponsive/React to Pain or Loud Voice = 3 pts
Scoring
- Score Range: 0-20
- Low Score = NEWS 1–4
- Medium Score = NEWS 5–6
- High Score = NEWS ≥7
Modified Early Warning Score (MEWS)
Scoring Criteria (Am J Respir Crit Care Med, 2017) [MEDLINE]
- Respiratory Rate (Breaths/min)
- <8 Breaths/min = 2 pts
- 9-14 Breaths/min = 0 pts
- 15-20 Breaths/min = 1 pts
- 21-29 Breaths/min = 2 pts
- ≥29 Breaths/min = 3 pts
- Temperature
- <35°C = 2 pts
- 35.1–36.0°C = 1 pts
- 36.1–38.0°C (95–101.1°F) = 0 pts
- 38.1-38.5°C = 1 pts
- ≥38.6°C = 2 pts
- Systolic Blood Pressure (SBP)
- ≤70 mm Hg = 3 pts
- 71-80 mm Hg = 2 pts
- 81-100 mm Hg = 1 pts
- 101-199 mm Hg = 0
- ≥200 mm Hg = 2 pts
- Heart Rate (Beats/min)
- <40 Beats/min = 2 pts
- 41-50 Beats/min = 1 pts
- 51-100 Beats/min = 0 pts
- 101-110 Beats/min = 1 pts
- 111-129 Beats/min = 2 pts
- >129 Beats/min = 3 pts
- Alert/Voice/Pain/Unresponsive (AVPU) Score
- Alert = 0 pts
- Reacts to Voice = 1 pts
- Reacts to Pain = 2 pts
- Unresponsive = 3 pts
- Urine Output (ml/kg/hr)
- <0.5 ml/kg/hr= 2 pts
- 0 ml/kg/hr = 3 pts
Clinical Efficacy-Sepsis Scoring
General
- Australian/New Zealand Study of SIRS Criteria for Sepsis (N Engl J Med, 2015) [MEDLINE]
- Of 1,171,797 Patients, a Total of 109,663 Had Infection and Organ Failure
- Approximately 87.9% of Patients Had SIRS-Positive Severe Sepsis
- Approximately 12.1% of Patients Had SIRS-Negative Severe Sepsis
- Over the 14 Years of the Study, These Groups Had Similar Characteristics and Changes in Mortality (SIRS-Positive Group: from 36.1% to 18.3%, P<0.001; SIRS-Negative Group: from 27.7% to 9.3%, P<0.001)
- This Pattern Remained Similar After Adjustment for Baseline Characteristics (Odds Ratio in the SIRS-Positive Group, 0.96; 95% confidence interval [CI], 0.96 to 0.97; Odds Ratio in the SIRS-Negative Group, 0.96; 95% CI, 0.94 to 0.98; P=0.12 for Between-Group Difference)
- In the Adjusted Analysis, Mortality Rate Increased Linearly with Each Additional SIRS Criterion (Odds Ratio for Each Additional Criterion, 1.13; 95% CI, 1.11 to 1.15; P<0.001) without Any Transitional Increase in Risk at a Threshold of Two SIRS Criteria: the need for two or more SIRS criteria to define severe sepsis excluded one in eight otherwise similar patients with infection, organ failure, and substantial mortality and failed to define a transition point in the risk of death
- Of 1,171,797 Patients, a Total of 109,663 Had Infection and Organ Failure
- Study of SIRS Criteria in Hospital Ward Patients (Am J Respir Crit Care Med, 2015) [MEDLINE]
- Almost Half of Patients Hospitalized on the Wards Developed SIRS at Least Once During Their Ward Stay
- Study Findings Suggest that Screening Ward Patients Using SIRS Criteria for Identifying Those with Sepsis is Impractical
- Study of Quick Sepsis-Related Organ Failure Assessment, Systemic Inflammatory Response Syndrome, and Early Warning Scores for Detecting Clinical Deterioration in Infected Patients Outside of the Intensive Care Unit (in Emergency Department or Hospital Wards) (Am J Respir Crit Care Med, 2017) [MEDLINE]: n = 30,677
- NEWS/MEWS were More Accurate than qSOFA for for Predicting Death and Intensive Care Unit Transfer in Non-Intensive Care Unit Patients
- Discrimination for In-Hospital Mortality was Highest for NEWS (Area Under the Curve 0.77; 95% CI: 0.76–0.79), followed by MEWS (Area Under the Curve 0.73; 95% CI: 0.71–0.74), qSOFA (Area Under the Curve 0.69; 95% CI: 0.67–0.70), and SIRS (Area Under the Curve 0.65; 95% CI: 0.63–0.66) (P , 0.01 for All Pairwise Comparisons)
- Using the Highest Non-ICU Score of Patients, >2 SIRS had a Sensitivity of 91% and Specificity of 13% for the Composite Outcome Compared with 54% and 67% for qSOFA >2, 59% and 70% for MEWS >5, and 67% and 66% for NEWS >8, Respectively
- Most Patients Met >2 SIRS Criteria 17 hrs Before the Combined Outcome Compared with 5 hrs for >2 and 17 hrs for >1 qSOFA Criteria
- NEWS/MEWS were More Accurate than qSOFA for for Predicting Death and Intensive Care Unit Transfer in Non-Intensive Care Unit Patients
- Australian/New Zealand Retrospective Cohort Analysis Examining the Accuracy of Sepsis Scoring Criteria in Predicting In-Hospital Mortality of Patients with Suspected Infection Admitted to the Intensive Care Unit (JAMA, 2017) [MEDLINE]: n = 184,875
- Most Common Diagnosis was Bacterial Pneumonia (Accounted for 17.7% of Cases)
- Overall, 18.7% of Patients Died in the Hospital
- Increase in SOFA Score of ≥2 Had Greater Prognostic Accuracy for In-Hospital Mortality than SIRS Criteria or qSOFA Score
- Study of Value of qSOFA in the Emergency Department (JAMA, 2017) [MEDLINE]
- In Patients Presenting to the Emergency Department with Suspected Infection, the Use of qSOFA Resulted in Greater Prognostic Accuracy for In-Hospital Mortality Than Did Either SIRS or Severe Sepsis Criteria
- Post Hoc Subgroup Analysis of qSOFA in Patients with Sepsis Outside of the Intensive Care Unit (J Infect Chemother, 2017) [MEDLINE]: n = 387
- Area Under the ROC Curve for the qSOFA Score was 0.615, Which was Superior to SIRS Score (0.531, P = 0.019), But Inferior to the SOFA Score (0.702, P = 0.005)
- Multivariate Logistic Regression Analysis Demonstrated that Hypothermia Might Be Associated with Poor Outcome Independently of qSOFA Criteria
- Findings Suggested that qSOFA had a Suboptimal Level of Predictive Value Outside of the ICU and Could Not Identify 16.3% of Patients Who were Once Actually Diagnosed with Sepsis
- Hypothermia Might Be Associated with an Increased Risk of death that Cannot Be Identified by qSOFA
- Retrospective Study of qSOFA and SIRS Criteria in the Emergency Department (Am J Emerg Med, 2017)
- Although qSOFA May Be Valuable in Predicting Sepsis-Related Mortality, it Performed Poorly as a Screening Tool for Identifying Sepsis in the Emergency Department
- As the Time to Meet qSOFA Criteria was Significantly Longer than for SIRS, Relying on qSOFA Alone May Delay Initiation of Evidence-Based Interventions Known to Improve Sepsis-Related Outcomes
- Retrospective, Single-Center Study of Value of qSOFA in the Emergency Department (Ann Emerg Med, 2018) [MEDLINE]
- The Diagnostic Performance of Positive qSOFA Score for Predicting 28-Day Mortality was Low in Critically Ill Septic Patients, Particularly dDuring the Early Period After ED Presentation
- Systematic Review and Meta-Analysis of Sepsis Scoring with Quick-SOFA and Systemic Inflammatory Response Syndrome Criteria for the Diagnosis of Sepsis and Prediction of Mortality (Chest, 2018) [MEDLINE]: n = 229,480 patients (from 10 studies)
- SIRS Criteria were Significantly Superior to the qSOFA for the Diagnosis of Sepsis
- Meta-Analysis of Sensitivity for the Diagnosis of Sepsis Comparing the qSOFA Criteria and SIRS Criteria was in Favor of SIRS Criteria (risk ratio [RR], 1.32; 95% CI, 0.40-2.24; P < .0001; I2 = 100%)
- qSOFA Criteria were Slightly Better than the SIRS Criteria in Predicting Hospital Mortality
- Meta-Analysis of the Area Under the Receiver Operating Characteristic Curve of 6 Studies Comparing the qSOFA Criteria and SIRS Criteria Favored the qSOFA Criteria (RR, 0.03; 95% CI, 0.01-0.05; P = .002; I2 = 48%) as a Predictor of In-Hospital Mortality
- SIRS Criteria were Significantly Superior to the qSOFA for the Diagnosis of Sepsis
- Systematic Review/Meta-Analysis of the Prognostic Accuracy of qSOFA Scoring in Predicting Sepsis Mortality (Ann Intern Med, 2018) [MEDLINE]: n = 385, 333 (from 38 studies)
- Overall, qSOFA Score Had 60.8% Sensitivity and 72% Specificity for Predicting Short-Term (28-Day or 30-Day) Sepsis Mortality
- Sensitivity of qSOFA in Predicting Sepsis Mortality was Higher in the ICU Population (87.2% [CI, 75.8%-93.7%]) than the non-ICU Population (51.2% [CI, 43.6%-58.7%])
- Specificity of qSOFA in Predicting Sepsis Mortality was Higher in the Non-ICU Population (79.6% [CI, 73.3%-84.7%]) than the ICU Population (33.3% [CI, 23.8%-44.4%]
- SIRS Criteria Had High Sensitivity (88.1%) and Low Specificity (25.8%) for Predicting Short-Term (28-Day or 30-Day) Sepsis Mortality
- Overall, qSOFA Score Had 60.8% Sensitivity and 72% Specificity for Predicting Short-Term (28-Day or 30-Day) Sepsis Mortality
- Meta-Analysis of Machine Learning for Detection of Sepsis in Hospitalized Patients (Comput Methods Programs Biomed. 2019 Mar;170:1-9. doi: 10.1016/j.cmpb.2018.12.027 [MEDLINE]: = n = 42,623 (7 studies)
- For Machine Learning, the Pooled Area Under the Receiving Operating Curve (SAUROC) was 0.89 (95% CI, 0.86−0.92), the Sensitivity was 81% (95% CI, 80−81), and the Specificity was 72% (95% CI, 72−72)
- These were All Higher for Machine Learning than the SAUROC for Traditional Screening Tools (SIRS 0.70, MEWS 0.50, and SOFA 0.78)*
- For Machine Learning, the Pooled Area Under the Receiving Operating Curve (SAUROC) was 0.89 (95% CI, 0.86−0.92), the Sensitivity was 81% (95% CI, 80−81), and the Specificity was 72% (95% CI, 72−72)
- Study of Oxygen Saturation (SpO2) in SOFA Sepsis Scoring (Crit Care Med, 2021) [MEDLINE]: n = 19,396 sepsis episodes (main cohort) and n = 10,586 episodes (validation cohort)
- Oxygen Saturations 96-95% Were Not Significantly Associated with Increased Mortality Rate in the Main or Validation Cohorts
- Oxygen Saturation 94%, the Adjusted Odds Ratio of Death was 1.56 (95% CI: 1.10-2.23) in the Main Cohort and 1.36 (95% CI: 1.00-1.85) in the Validation Cohorts and Increased Gradually Below This Level
- Oxygen Saturation/FIO2 Ratio Had Slightly Better Predictive Performance, as Compared with Oxygen Saturation Alone
- These Findings Provide Evidence for Assessing Respiratory Function with Oxygen Saturation in the Sequential Organ Failure Assessment (SOFA) Score and the Sepsis-3 Criteria
Hospitalized Patients in Low/Middle-Income Countries
- Sepsis Assessment and Identification in Low Resource Settings (SAILORS) Study of qSOFA Score in Hospitalized Adults With Suspected Infection in Low/Middle-Income Countries (JAMA, 2018) [MEDLINE]
- In Hospitalized Adults With Suspected Infection in Low/Middle-Income Countries, the qSOFA Score Identified Infected Patients at Risk of Death Beyond that Explained by Baseline Factors
- However, the Predictive Validity Varied Among Cohorts and Settings, and Further Research is Required to Better Understand Potential Generalizability
Sepsis Scoring in Pregnant Patients (see Pregnancy
Obstetrically-Modified SOFA (omSOFA) Score (Aust N Z J Obstet Gynaecol, 2017) [MEDLINE]
- Respiration
- pO2/FIO2 Ratio ≥400: 0 points
- pO2/FIO2 Ratio 300-399: 1 point
- pO2/FIO2 Ratio ≤299: 2 points
- Coagulation
- Platelets ≥150k: 0 points
- Platelets 100-149k: 1 point
- Platelets ≥99k: 2 points
- Liver
- Total Bilirubin ≤20 μmol/L: 0 points
- Total Bilirubin 21-32 μmol/L: 1 point
- Total Bilirubin >32 μmol/L: 2 points
- Cardiovascular
- MAP ≥70 mm Hg: 0 points
- MAP <70 mm Hg: 1 point
- Vasopressors Required: 2 points
- Central Nervous System
- Alert: 0 points
- Arousable by Voice: 1 point
- Arousable by Pain: 2 points
- Renal
- Serum Cr ≤90 μmol/L: 0 points
- Serum Cr 90-120 μmol/L: 1 point
- Serum Cr >120 μmol/L: 2 points
Obstetrically-Modified qSOFA (omqSOFA) Score (Aust N Z J Obstet Gynaecol, 2017) [MEDLINE]
- Respiration
- RR <25/min: 0 points
- RR ≥25/min: 1 point
- Cardiovascular
- SBP ≥90 mm Hg: 0 points
- SBP <90 mm Hg: 1 point
- Central Nervous System
- Alert: 0 points
- Not Alert: 1 point
Clinical Efficacy
- Conventional Sepsis Scoring Systems (Both SIRS and SOFA) Have Excluded Pregnant Patients, Since the Physiology of Pregnancy is Unique with Normal Physiologic Parameters in Pregnancy Overlap with the Clinical Criteria for Sepsis (Obstet Gynecol, 2014) [MEDLINE]
- Sepsis in Obstetrics Score Has Been Alternatively Proposed and Validated to Identify Pregnant Patients with Sepsis (Obstet Gynecol, 2017) [MEDLINE]
- Society of Obstetric Medicine Australia and New Zealand (SOMANZ) Sepsis Guidelines in Pregnant Patients (Aust N Z J Obstet Gynaecol, 2017) [MEDLINE]
- Alternative Guidelines Proposed (But Not Validated) to Diagnose and Manage Sepsis in Pregnant Patients
Recommendations (Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock 2021) (Crit Care Med, 2021) [MEDLINE]
- Systemic Inflammatory Response Syndrome (SIRS), National Early Warning Score (NEWS), or Modified Early Warning System (MEWS) Should Be Used Instead of qSOFA as a Single-Screening Tool for Sepsis/Septic Shock (Strong Recommendation, Moderate Quality of Evidence

Clinical Manifestations
General Comments
- Up to 40% of Patients Admitted to the ICU with Suspected Sepsis Do Not Actually Have Sepsis (Crit Care, 2015) [MEDLINE]
- Since the Benefit of Treating The Patients Who Do Not Have Sepsis with the Recommended Sepsis Resuscitation Procedures and Antibiotics is Unclear (and May Be Harmful), the Infectious Diseases Society of America (IDSA) Did Not Endorse the 2016 Surviving Sepsis Guidelines (Clin Infect Dis, 2018) [MEDLINE]
- The Surviving Sepsis Campaign Guidelines Also Do Not Differentiate Between Patients with Suspected Sepsis and Suspected Septic Shock (Clin Infect Dis, 2018) [MEDLINE]
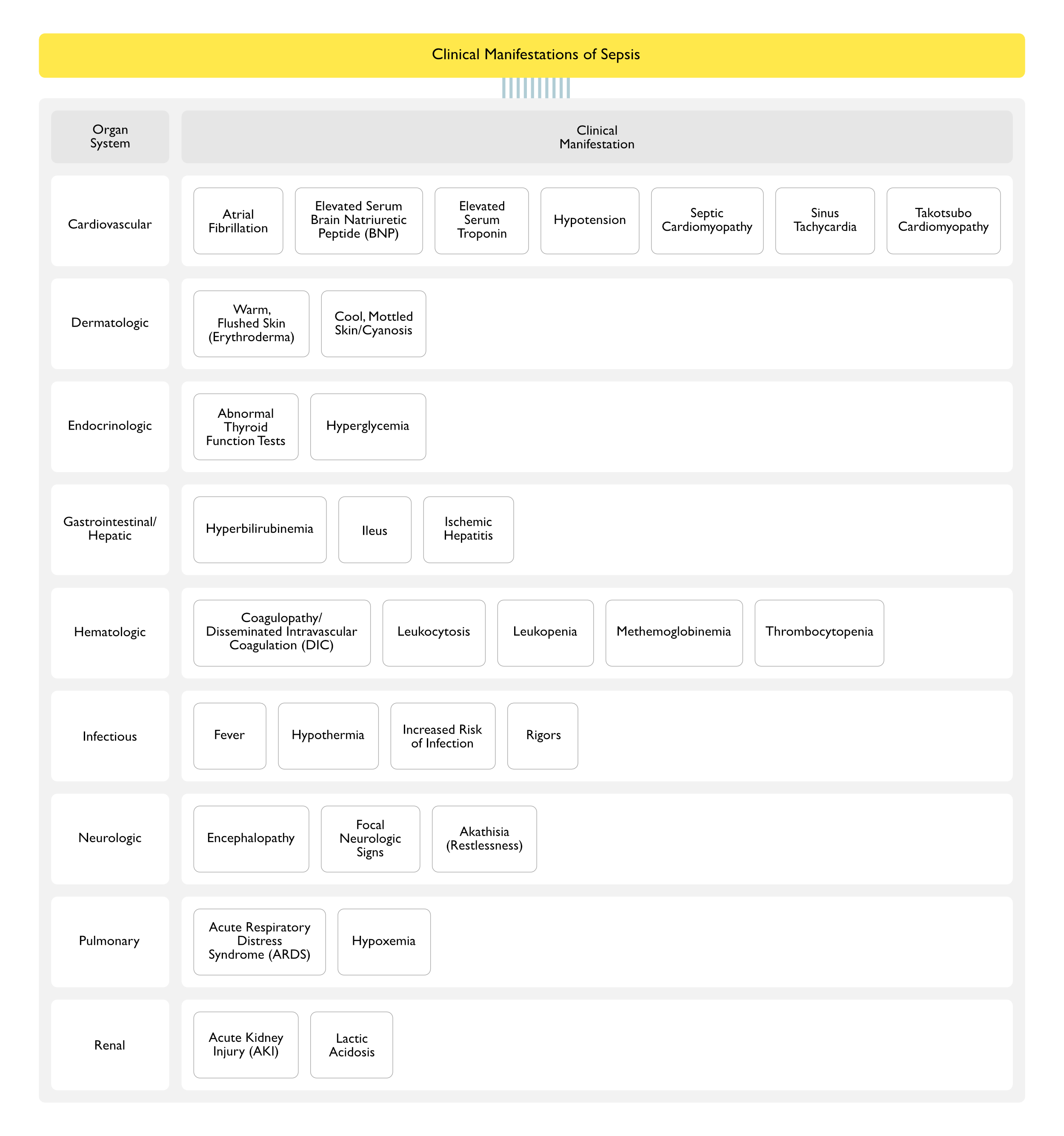
Cardiovascular Manifestations
Atrial Fibrillation (AF) (see Atrial Fibrillation)
- Epidemiology
- Approximately 6-20% of Patients with Severe Sepsis Develop New-Onset Atrial Fibrillation
- Exacerbation of Pre-Existing Atrial Fibrillation or the Occurrence of New-Onset Atrial Fibrillation May Occur Due to Sepsis Itself or May Be Due to Catecholamine Vasopressors Used in the Treatment of Septic Shock
- The Addition of Vasopressin to Catecholamine Vasopressors (as Compared with Catecholamines Alone) was Associated with a Lower Risk of Atrial Fibrillation ( JAMA, 2018) [MEDLINE]
- Exacerbation of Pre-Existing Atrial Fibrillation or the Occurrence of New-Onset Atrial Fibrillation May Occur Due to Sepsis Itself or May Be Due to Catecholamine Vasopressors Used in the Treatment of Septic Shock
- Approximately 6-20% of Patients with Severe Sepsis Develop New-Onset Atrial Fibrillation
- Clinical Data
- Study of New-Onset Atrial Fibrillation in Severe Sepsis (JAMA, 2011) [MEDLINE]
- Patients with New-Onset AF and Severe Sepsis are at 4x Increased Risk of In-Hospital CVA and a 7% Increased Risk of Death, as Compared with Patients with No AF and Patients with Preexisting AF
- Possible Mechanisms for Increased Risk of CVA in New-Onset AF in Severe Sepsis: new-onset AF might just be a marker for the sickest patients with greatest inherent CVA risk, sepsis itself might result in an increased risk for CVA (by hemodynamic collapse, coagulopathy, or systemic inflammation), or new-onset AF might be a source of cardioembolic CVA
- Patients with Severe Sepsis Had a 6x Increased Risk of In-Hospital CVA, as Compared with Hospitalized Patients without Severe Sepsis
- Patients with Severe Sepsis and Preexisting AF Did Not Have an Increased Risk of CVA, as Compared with Patients without AF
- Prospective Observational Study of Atrial Fibrillation as a Predictor of Mortality in Critically Ill Patients (Crit Care Med, 2016) [MEDLINE]
- AF in Critical Illness (Whether New-Onset or Recurrent) is Independently Associated with Increased Hospital Mortality (31% vs 17%), Especially in Patients without Sepsis
- New-Onset AF (But Not Recurrent AF) was Associated with Increased Diastolic Dysfunction and Vasopressor Use and a Greater Cumulative Positive Fluid Balance
- Dutch Cohort Study of the Incidence, Predictors, and Outcomes of New-Onset Atrial Fibrillation in Critically Ill Patients with Sepsis (Am J Respir Crit Care Med, 2017) [MEDLINE]
- Atrial Fibrillation is a Common Complication of Sepsis and is Independently Associated with Excess Mortality
- Systematic Review and Meta-Analysis of Efficacy of Vasopressin with Catecholamines vs Catecholamines Alone in Septic Shock (JAMA, 2018) [MEDLINE]
- The Addition of Vasopressin to Catecholamine Vasopressors (as Compared with Catecholamines Alone) was Associated with a Lower Risk of Atrial Fibrillation
- Study of New-Onset Atrial Fibrillation in Severe Sepsis (JAMA, 2011) [MEDLINE]
Elevation of Serum Brain Natriuretic Peptide (BNP) (see Serum Brain Natriuretic Peptide)
- Physiology
- Elevation of Serum Brain Natriuretic Peptide is Likely Due to Sepsis-Related Inflammatory Myocardial Dysfunction (Crit Care Med, 2004) [MEDLINE]
- Clinical Data
Elevation of Serum Troponin (see Serum Troponin)
- Epidemiology
- Troponin Elevation is Common in Adult Patients with Septic Shock (Crit Care, 2013) [MEDLINE]
- Physiology
- Mechanisms of Troponin Elevation in Sepsis (J Intensive Care Soc, 2015) [MEDLINE]
- Demand-Supply Mismatch
- Due to Tachycardia, Hypoxemia, Hypotension, Decreased Oxygen Delivery, and Decreased Coronary Perfusion Pressure
- Direct Myocarditis
- Due to Bacteraemia, Resulting in Cytokine/Endotoxin Release (and Microvascular Dysfunction), Bacterial Myocarditis, Myocardial Depression, and Increased Myocardial Cell Membrane Permeability
- Free Radicals/Superoxide Radicals
- Due to Sepsis-Associated Activation of NADPH Oxidases Complexes, Resulting in the Formation of Free Radicals (Which Cause Myocardial Cell Damage and Apoptosis)
- Elevated Filling Pressures and Ventricular Wall Stress
- Resulting in Activation of Intracellular Signalling Cascade, Resulting in Cardiac Myocyte Apoptosis, Myocytes Damage and Micronecrosis, and Decreased Coronary Perfusion Pressure
- Left Ventricular Diastolic and Right Ventricular Systolic Dysfunction
- Demand-Supply Mismatch
- Mechanisms of Troponin Elevation in Sepsis (J Intensive Care Soc, 2015) [MEDLINE]
- Clinical Data
- Study of Troponin in Critically Ill ICU Patients (Arch Intern Med, 2006) [MEDLINE]: n = 23 studies
- Elevated Troponin was Associated with Increased ICU Mortality Rate and Length of Stay
- Retrospective Study of the Value of Troponin-I in Predicting Sepsis Mortality Rate (Using Data from the Prowess Trial) (J Crit Care, 2010) [MEDLINE]: n = 598
- Positive Troponin-I was Associated with Increased Age (61 y/o), as Compared to Negative Troponin-I (56 y/o)
- Positive Troponin-I was Associated with Higher APACHE II Score (26.1), as Compared to Negative Troponin-I (22.3)
- Troponin-I Elevation was Associated with an Increased 28-Day Sepsis Mortality Rate
- After Adjusting for Other Variables, Elevated Troponin-I Had Odds Ratio of 2.020 for Mortality (95% CI: 1.153-3.541)
- Study of Troponin-T in Sepsis (Am J Med, 2013) [MEDLINE]: n = 645
- Troponin-T Elevation was Associated with In-Hospital Mortality Rate 30-Day Mortality Rate (But Not Long-Term 1/2/3-Year Mortality Rates) in Sepsis Patients Admitted to the Intensive Care Unit
- Prospective Substudy of a Randomized Trial in Septic Shock (Crit Care, 2013) [MEDLINE]: n = 121 patients
- Troponin Elevation was Commonly Observed in Adult Patients with Septic Shock
- No Differences were Observed in Troponin Elevation, CK Elevation, or EKG Changes in Patients Treated with Vasopressin vs Epinephrine
- Systematic Review of Troponin Elevation in Sepsis in the Absence of Angiographically Documented Coronary Artery Disease (J Intensive Care Soc, 2015) [MEDLINE]
- In Multivariate Analyses, Elevated Troponin was Not Found to Be an Independent Predictor of Mortality After Adjusting for Other Variables
- Study of Troponin in Critically Ill ICU Patients (Arch Intern Med, 2006) [MEDLINE]: n = 23 studies
Hypotension (see Hypotension)
- Epidemiology
- Hypotension is a Common Manifestation of Sepsis
- Physiology
- Due to Endothelial Cell Release of Prostacyclin and Nitric Oxide-Induced Vasodilation
- Due to Increased Endothelial Permeability and Decreased Arterial Vascular Tone with to Increased Capillary Pressure, Resulting in Redistribution of Intravascular Fluid
- Due to Impaired Compensatory Secretion of the Antidiuretic Hormone, Vasopressin
- Due to Myocardial Depression (Decreased Systolic and Diastolic Function)
- Due to Regional Microvascular Dysfunction Resulting in Impaired Redistribution of Blood Flow from the Splanchnic Organs to the Core Organs (Brain, Heart)
- Clinical
- Note that Patients with Chronic Hypertension May Develop Critical End-Organ Hypoperfusion at Higher Blood Pressures than Healthy Patients (i.e. Relative Hypotension)
Prolonged QT Interval (see Torsade)
- Epidemiology
- Multicenter Retrospective Study of QT Prolongation in the Setting of Sepsis (Crit Care, 2024) [MEDLINE]
- New-Onset QT Prolongation Occurred in 22.9% of Patients
- The Majority Demonstrated a Similar Pattern as Type 1 Long QT Syndrome
- Patients with QT Prolongation Had a Higher 30-Day In-Hospital Mortality Rate (P < 0.001)
- Patients with QT Prolongation Had a Higher Risk of Tachyarrhythmias (Including Paroxysmal Atrial Fibrillation or Tachycardia [P < 0.001] and Ventricular Arrhythmias [P < 0.001]) During Hospitalization
- QT Prolongation Independently Predicted 30-Day Mortality (P = 0.044) After Multivariate Analysis
- Independent Predictors of QT Prolongation in Sepsis
- Acute Cardiac Dysfunction (P = 0.021)
- Acute Renal Dysfunction (P = 0.013)
- Acute Respiratory Dysfunction (P < 0.001)
- History of Coronary Artery Disease (P = 0.001)
- Septic Shock (P = 0.008)
- New-Onset QT Prolongation Occurred in 22.9% of Patients
- Multicenter Retrospective Study of QT Prolongation in the Setting of Sepsis (Crit Care, 2024) [MEDLINE]
Septic Cardiomyopathy/Congestive Heart Failure-Systolic/Cardiogenic Shock (see Congestive Heart Failure and Cardiogenic Shock)
- Physiology
- Septic Cardiomyopathy is Due to Sepsis-Related Myocardial Depression
- Evidence Suggests that Circulating Histones May Be Implicated in the Pathogenesis of Septic Cardiomyopathy (Crit Care Med, 2015) [MEDLINE]
- Septic Cardiomyopathy is Due to Sepsis-Related Myocardial Depression
Sinus Tachycardia (see Sinus Tachycardia)
- Epidemiology
- Tachycardia is Common in Sepsis
- However, it May Be Absent in Older Patients, in Diabetics, and in Patients Who Have Been Taking β-Blockers
- Tachycardia May Be Pronounced and Prolonged (Prior to the Development of Hypotension) in Younger Patients
- Tachycardia is Common in Sepsis
- Physiology
- Tachycardia is Due to Vasodilation-Induced Increased in Heart Rate
Takotsubo Cardiomyopathy (Stress-Induced Cardiomyopathy) (see Takotsubo Cardiomyopathy)
- Epidemiology
- Systematic Review of 26 Case Reports of Sepsis-Associated Takotsubo Cardiomyopathy (Angiology, 2017) [MEDLINE]
- Mean Age of 62.8 y/o (SD 14 yrs)
- Female Predominance (16/26 Cases)
- Favorable Outcome in 92.3% of Cases Once the Sepsis was Treated
- Systematic Review of 26 Case Reports of Sepsis-Associated Takotsubo Cardiomyopathy (Angiology, 2017) [MEDLINE]
Dermatologic Manifestations
Clinical Changes Due to Alteration in Skin Perfusion
- Warm, Flushed Skin (Erythroderma) (see Erythroderma)
- Epidemiology: may be observed early in the course
- Physiology: peripheral vasodilation
- Cool Skin/Mottling/Cyanosis (see Cyanosis)
- Epidemiology: observed as shock develops
- Physiology: peripheral vasoconstriction
Endocrinologic Manifestations
Abnormal Thyroid Function Tests (see Abnormal Thyroid Function Tests in Non-Thyroidal Illness)
- Epidemiology
- May Occur in Some Cases
Hyperglycemia (see Hyperglycemia)
- Epidemiology
- Hyperglycemia (“Stress Hyperglycemia”) is Common During Critical Illness
- Mechanisms of Hyperglycemia
- Catecholamine Secretion
- Cortisol Secretion
- Glucagon Secretion
- Growth Hormone Secretion
- Gluconeogenesis
- Glycogenolysis
- Insulin Resistance: overt insulin resistance was noted on admission in 67% of critically ill patients, with the percentage of patients having insulin resistance increasing to 70% when assessed later in the course (J Parenter Enteral Nutr, 2008) [MEDLINE]
- Prognosis
- Retrospective Study of Hyperglycemia in Critically Ill (Medical and Surgical) Patients (Mayo Clin Proc, 2003) [MEDLINE]
- Hyperglycemia (as Assessed by Admission, Mean, and Maximal Blood Glucose Levels) was Associated with Increased Mortality Rate: there was a dose-response effect
- Study of Admission Hyperglycemia in Critically Ill Sepsis Patients (Crit Care Med, 2016) [MEDLINE]
- Admission Hyperglycemia was Associated with Adverse Sepsis Outcome of Irrespective of the Presence or Absence of Preexisting Diabetes Mellitus
- Mechanism Appears to Be Unrelated to Exaggerated Inflammation or Coagulation
- Admission Hyperglycemia was Associated with Adverse Sepsis Outcome of Irrespective of the Presence or Absence of Preexisting Diabetes Mellitus
- Retrospective Study of Hyperglycemia in Critically Ill (Medical and Surgical) Patients (Mayo Clin Proc, 2003) [MEDLINE]
Gastrointestinal Manifestations
Hyperbilirubinemia (see Hyperbilirubinemia)
- Epidemiology
- May Occur in Some Cases
- Prognosis
- Early Hepatic Dysfunction (Hyperbilirubinemia >2 mg/dL within 48 hrs of Admission) Occurred in 11% of Patients and was Associated with an Increased Mortality Rate (30.4% vs. 16.4%; p < 0.001) (Crit Care Med, 2007) [MEDLINE]
Ileus (see Ileus)
- Physiology
- Due to Bowel Hypoperfusion
- Clinical
- Decreased Bowel Sounds
Ischemic Hepatitis (see Ischemic Hepatitis)
- Epidemiology
- May Occur in Septic Shock (or Any Other Type of Shock)
Hematologic Manifestations
Sepsis-Induced Coagulopathy (SIC)/Disseminated Intravascular Coagulation (DIC) (see Coagulopathy and Disseminated Intravascular Coagulation)
- Epidemiology
- Either Sepsis-Induced Coagulopathy (SIC)/Disseminated Intravascular Coagulation (DIC) May Occur
- Cohort Study of Coagulation in Severe Sepsis (Intensive Care Med, 2015) [MEDLINE]
- Progressive Coagulopathy (as Defined by Thromboelastography Variables) was Associated with an Increased Risk of Death and Increased Risk of Hemorrhage
- Physiology (J Thromb Haemost, 2019) [MEDLINE]
- Sepsis‐Associated Disseminated Intravascular Coagulation (DIC) is Characterized by Overproduction of Plasminogen Activator Inhibitor‐1 with Excessive Suppression of Fibrinolysis, Resulting in Prothrombotic Effects
- In Contrast, This Suppression of Plasminogen Activator Inhibitor‐1 is Rarely Observed in Malignancy‐Associated Disseminated Intravascular Coagulation (DIC)
- Consequently, Organ Dysfunction Frequently Develops in Sepsis‐Associated Disseminated Intravascular Coagulation (DIC) Due to Decreased Tissue Perfusion
- In Contrast, Systemic Bleeding is a More Common Feature in (Non-Sepsis) Fibrinolytic Phenotype Disseminated Intravascular Coagulation (DIC)
- Consequently, Hypofibrinogenemia is Not Common in Sepsis‐Associated Disseminated Intravascular Coagulation (DIC) and Elevation in Fibrin‐Related Markers is Not Associated with Sepsis Severity
- In Contrast, Thrombocytopenia and Prolongation of the INR are Correlated with an Increase in the Sepsis Mortality Rate
- Sepsis‐Associated Disseminated Intravascular Coagulation (DIC) is Characterized by Overproduction of Plasminogen Activator Inhibitor‐1 with Excessive Suppression of Fibrinolysis, Resulting in Prothrombotic Effects
- Clinical Scoring (International Society on Thrombosis and Haemostasis) (Thromb Haemost, 2001) [MEDLINE] (J Thromb Haemost, 2019) [MEDLINE]
- Sepsis-Induced Coagulopathy (SIC)
- Platelet Count (see Complete Blood Count)
- 100-149k -> 1 pt
- <100k -> 2 pts
- International Normalized Ratio (INR) (see Prothrombin Time)
- 1.3-1.4 -> 1 pt
- >1.4 -> 2 pts
- SOFA Score
- 1 -> 1 pt
- ≥2 -> 2 pts
- Total ≥4 Indicates Sepsis-Induced Coagulopathy
- Platelet Count (see Complete Blood Count)
- Overt Disseminated Intravascular Coagulation (DIC)
- Platelet Count (see Complete Blood Count)
- 50-99k -> 1 pt
- <50k -> 2 pts
- Fibrinogen (see Serum Fibrinogen)
- ≥100 g/mL -> 0 pts
- <100 g/mL -> 1 pt
- Fibrin Split Product/D-Dimer (see Serum Fibrin Degradation Products and Plasma D-Dimer)
- Absent -> 0 pts
- Moderate Increase -> 2 pts
- Strong Increase -> 3 pts
- International Normalized Ratio (INR) (see Prothrombin Time)
- 3-5.9 -> 1 pt
- ≥6 -> 2 pts
- Total ≥5 Indicates Overt Disseminated Intravascular Coagulation (DIC)
- If Negative, Repeat in 1-2 Days
- Platelet Count (see Complete Blood Count)
- Sepsis-Induced Coagulopathy (SIC)
Leukocytosis (see Leukocytosis)
- Epidemiology
- Leukocytosis is Common
- Clinical
- White Blood Cell (WBC) Count >12k
Leukopenia (see Leukopenia)
- Epidemiology
- May Occur in Some Cases
- Clinical
- White Blood Cell (WBC) Count <4k
- Clinical Data
- Study of Gram-Negative Bacteremia (Am J Med, 1980) [MEDLINE]
- Leukopenia <4k was More Common in Non-Survivors (15%) than Non-Survivors (7%) in Gram-Negative Sepsis
- Study of Gram-Negative Bacteremia (Am J Med, 1980) [MEDLINE]
Methemoglobinemia (see Methemoglobinemia)
- Epidemiology
- Methemoglobin Levels May Increase in Sepsis (Acta Anaesthesiol Scand, 1998) [MEDLINE]
- Physiology
- Nitric Oxide is Synthesized in Sepsis and is Converted to Methemoglobin and Nitrate
Thrombocytopenia (see Thrombocytopenia)
- Epidemiology
- Thrombocytopenia Has Been Reported in 14.5% of Severe Sepsis Patients in the ICU and is Associated with Worse Outcome (9.9% in Survivors, 22.5% in Non-Survivors) (Crit Care Med, 2009) [MEDLINE]
- Mechanisms of Thrombocytopenia
- Consumptive Coagulopathy: related to sepsis-induced platelet activation with/without frank disseminated intravascular coagulation (DIC)
- Hemodilution: associated with intravenous fluid resuscitation
- Increased Circulating Histones (JAMA, 2016) [MEDLINE]
- Platelet Sequestration
- Prognosis
- Thrombocytopenia is Associated with Worse Outcome in Severe Sepsis (9.9% in Survivors, 22.5% in Non-Survivors) (Crit Care Med, 2009) [MEDLINE]
- Thrombocytopenia During the First 24 hrs is Associated with Worse 28-Day Mortality Rate in Septic Shock (Crit Care Med, 2016) [MEDLINE]
- Thrombocytopenia Severity was Associated with Increased 28-Day Mortality Rate (by Kaplan-Meier Method)
- Thrombocytopenia Severity was Associated with Increased 28-Day Mortality Rate (Hazard Ratio, 1.65; 95% CI, 1.31-2.08 for Platelet Count <50k vs>150k; p<0.0001)
- Thrombocytopenia <100k was Associated with Increased 28-Day Mortality (by Multivariate Cox Regression)
Infectious Manifestations
Fever (see Fever)
- Clinical
- Temperature >38.5°C
- Study of Sepsis Definitions (Chest, 1992) [MEDLINE]
- Failure to Develop a Fever (Defined as a Temperature <35.5ºC) was More Frequent in Sepsis Non-Survivors (17%) than Sepsis Survivors (5%)
Hypothermia (see Hypothermia)
- Clinical
- Temperature <36°C
- Clinical Data
- Study of Sepsis Definitions (Chest, 1992) [MEDLINE]
- Failure to Develop a Fever (Defined as a Temperature <35.5ºC) was More Frequent in Sepsis Non-Survivors (17%) than Sepsis Survivors (5%)
- Study of Sepsis Definitions (Chest, 1992) [MEDLINE]
Increased Risk of Acquiring Other Infections
- Clinical Data
- Study of Acquisition of Secondary Infections After Intensive Care Unit Admission for Sepsis (JAMA, 2016) [MEDLINE]
- Intensive Care Unit-Acquired Infections Occurred More Commonly in Patients with Sepsis with Higher Disease Severity, But Such Infections Contributed Only Modestly to Overall Mortality
- The Genomic Response of Patients with Sepsis was Consistent with Immune Suppression (Decreased Expression of Genes Involved in Gluconeogenesis and Glycolysis) at the Onset of Secondary Infection
- Study of Acquisition of Secondary Infections After Intensive Care Unit Admission for Sepsis (JAMA, 2016) [MEDLINE]
Rigors (see Rigors)
- Epidemiology
- Common
Neurologic Manifestations
Altered Mental Status/Encephalopathy (see Altered Mental Status)
- Epidemiology
- Encephalopathy is Common in Sepsis
- Clinical
- Delirium (see Delirium)
- BRAIN-ICU Study of Patients with Respiratory Failure or Shock in the Medical or Surgical Intensive Care Unit (NEJM, 2013) [MEDLINE]: 74% of patients had delirium
- Obtundation/Coma (see Obtundation/Coma)
- Delirium (see Delirium)
Focal Neurologic Signs
- Epidemiology
- May Be Seen in Some Cases
- Physiology
- Due to Cerebral Hypoperfusion
Akathisia/Restlessness (see Akathisia)
- Epidemiology
- May Be Seen in Some Cases
- Physiology
- Due to Cerebral Hypoperfusion
Pulmonary Manifestations
Acute Respiratory Distress Syndrome (ARDS) (see Acute Respiratory Distress Syndrome)
- Epidemiology
- Sepsis is the Most Common Etiology of ARDS
- Risk Factors for the Development of Sepsis-Associated ARDS
- Acute Abdomen (Ann Intensive Care, 2017) [MEDLINE]
- Acute Pancreatitis (Ann Intensive Care, 2017) [MEDLINE]
- Alcohol Abuse (Crit Care Med, 2003) [MEDLINE] and (Crit Care Med, 2008) [MEDLINE]: ethanol may decrease glutathione concentrations in the epithelial lining fluid, increasing the risk of oxidative injury to the lung
- Delayed Antibiotics (Crit Care Med, 2008) [MEDLINE]
- Delayed Goal-Directed Resuscitation (Crit Care Med, 2008) [MEDLINE]
- Diabetes Mellitus (Crit Care Med, 2008) [MEDLINE]
- Higher APACHE II Score (Ann Intensive Care, 2017) [MEDLINE]
- Higher Intravenous Fluid Resuscitation within the First 6 hrs (Ann Intensive Care, 2017) [MEDLINE]: in stratified analysis, the total fluid infused within the first 6 hrs was a risk factor in the non-shock group, but not in the shock group
- Increased Baseline Respiratory Rate (Crit Care Med, 2008) [MEDLINE]
- Older Age (Ann Intensive Care, 2017) [MEDLINE]
- Pneumonia as the Site of Infection (Ann Intensive Care, 2017) [MEDLINE]
- Recent Chemotherapy (Crit Care Med, 2008) [MEDLINE]
- Shock (Ann Intensive Care, 2017) [MEDLINE]
- Transfusion (Crit Care Med, 2008) [MEDLINE]
- Clinical
Hypoxemia (see Hypoxemia)
- Epidemiology
- Hypoxemia is Common in Sepsis
- Physiology
- Pulmonary Vascular Endothelial Injury with Impairment of Capillary Blood Flow and Increased Microvascular Permeability (with Development of Interstitial and Alveolar Edema)
Renal Manifestations
Acute Kidney Injury (AKI) (see Acute Kidney Injury)
- Epidemiology
- Retrospective Cohort Study of Acute Kidney Injury Requiring Dialysis in Severe Sepsis (from 2000-2009) (Am J Respir Crit Care Med, 2015) [MEDLINE]
- Approximately 6.1% of Patients with Severe Sepsis Develop AKI Requiring Dialysis: the odds of requiring dialysis increased by 14% from 2000-2009 (while the odds of mortality decreased by 61% from 2000-2009)
- Mortality Rate was Higher in Patients Requiring Dialysis (43.6% vs. 24.9%)
- Retrospective Cohort Study of Acute Kidney Injury Requiring Dialysis in Severe Sepsis (from 2000-2009) (Am J Respir Crit Care Med, 2015) [MEDLINE]
- Mechanisms
- Acute Tubular Necrosis (ATN): due to renal hypoperfusion, hypoxemia, etc
- Hypotension with Renal Hypoperfusion
- Neutrophil Activation by Endotoxin and the Chemotactic Peptide, fMet-Leu-Phe (FMLP) Released from Bacterial Cell Walls
- Renal Vasoconstriction
- Tumor Necrosis Factor-α (TNFα)
- Clinical
- Oliguria/Anuria
- Prevention of Acute Kidney Injury
- Measures to Prevent Acute Kidney Injury in the Intensive Care Unit (ATS/ERS/ESICM/SCCM/SRLF Statement-Prevention and Management of Acute Renal Failure in the ICU Patient; Am J Resp Crit Care Med, 2010) [MEDLINE]
- Avoid Nephrotoxic Exposure (NSAID’s, Aminoglycosides, etc)
- Avoid Radiographic Contrast Exposure (see Radiographic Contrast)
- Avoid Hyper-Oncotic Resuscitation Fluids (Hydroxyethyl Starch, Dextrans, 20-25% Albumin), Due to Their Risk of Renal Dysfunction
- Maintain MAP >65 mm Hg with Intravenous Fluids/Vasopressors
- Higher MAP May Be Required in Patients with Long-Standing Hypertension (Where Autoregulation of Renal Blood Flow Might Be Impaired)
- Vasopressors are Recommended in Patients with Hypotension (MAP <65) Despite Intravenous Fluid Resuscitation: there is no data to support the use of any specific vasopressor over another
- Use of Inotropic Agents to Increase Cardiac Output to Supraphysiologic Levels to Improve Renal Function is Not Recommended
- Low-Dose Dopamine (Intended to Improve Renal Function) is Not Recommended
- Measures to Prevent Acute Kidney Injury in the Intensive Care Unit (ATS/ERS/ESICM/SCCM/SRLF Statement-Prevention and Management of Acute Renal Failure in the ICU Patient; Am J Resp Crit Care Med, 2010) [MEDLINE]
- Complications and Prognosis
- Prospective Observational Study of Septic Acute Kidney Injury (J Intensive Care Med, 2018) [MEDLINE]
- Patients with Septic AKI Had a 40% 1-Year Mortality
- Factors Associated with Increased 1-Year Mortality
- Older Age
- Ischemic Heart Disease
- Higher Simplified Acute Physiology Score II
- Central Nervous System or Musculoskeletal Primary Infections
- Higher Daily Fluid Balance
- Furosemide Administration During ICU Stay
- Risk of Progression to Chronic Kidney Disease is High
- Initial AKI Reversal: 21% progressed to CKD
- Initial AKI Recovery: 30% progressed to CKD
- Initial AKI Non-Recovery: 79% progressed to CKD
- Prospective Observational Study of Septic Acute Kidney Injury (J Intensive Care Med, 2018) [MEDLINE]
Hypocalcemia (see Hypocalcemia)
- Mechanisms
- Severe Acute Illness and/or Sepsis Cause Loss of Calcium from Circulation Due to the Following
- Decreased Calcitriol Production
- Decreased Parathyroid Hormone (PTH) Secretion
- End-Organ Parathyroid Hormone (PTH) Resistance
- Severe Acute Illness and/or Sepsis Cause Loss of Calcium from Circulation Due to the Following
Lactic Acidosis (see Lactic Acidosis)
- Physiology
- Decreased Lactate Clearance, Likely Due to Inhibition of Pyruvate Dehydrogenase
- Epinephrine-Induced β2-Adrenergic Receptor Stimulation with/without Decreased Oxygen Delivery to Tissues
Vascular Manifestations
Symmetrical Peripheral Gangrene (SPG)
- Physiology
- Disturbed Procoagulant-Anticoagulant Balance in Susceptible Tissue Beds Secondary to Shock (Cardiogenic, Septic)
- A Causal Role of Vasopressor Therapy in Symmetrical Peripheral Gangrene is Unproven and is Unlikely
- Since Critically Ill Patients Who Develop Symmetrical Peripheral Gangrene Do So Usually After >36–48 hrs of Vasopressor Therapy, Implicating Some Type of Time-Dependent Pathophysiological Mechanism (Transfus Apher Sci, 2021) [MEDLINE]
- Clinical
- Tissue Necrosis of Acral (Distal) Extremities
- Characteristic Triad
- Shock
- Hypotension (see Hypotension)
- Lactic Acidosis (see Lactic Acidosis)
- Multiple Organ Dysfunction
- Normoblastemia
- Disseminated Intravascular Coagulation (DIC) (see Disseminated Intravascular Coagulation)
- Natural Anticoagulant (Protein C, Antithrombin) Depletion
- Acute Ischemic Hepatitis (“Shock Liver”) is Observed in >90% of Patients Who Develop Symmetrical Peripheral Gangrene and Likely Plays a Role in Natural Anticoagulant Depletion (see Ischemic Hepatitis)
- Characteristic Time Interval of 2–5 Days (Median: 3 Days) Between the Onset of Shock/Shock Liver and the Beginning of Ischemic Injury Secondary to Peripheral Microthrombosis (“Limb Ischemia with Pulses”), Consistent with the Time Required to Develop Depletion in Hepatically-Synthesized Natural Anticoagulants
- Other Risk Factors for Natural Anticoagulant Depletion Include Chronic Liver Disease (i.e Cirrhosis) and, Possibly Colloid (Albumin, High-Dose Immunoglobulin) Transfusion (Which Cause Hemodilution, Since They Lack Lack Coagulation Factors)
- Shock
Special Clinical Situation-Sepsis in Pregnancy
Non-Infectious Conditions Which Can Mimic Sepsis in Pregnancy (Aust N Z J Obstet Gynaecol, 2017) [MEDLINE]
- Acute Pulmonary Embolism (PE) (see Acute Pulmonary Embolism)
- Clinical
- Hypotension (see Hypotension)
- Low-Grade Fever (see Fever)
- Tachycardia (see Sinus Tachycardia)
- Tachypnea (see Tachypnea)
- Clinical
- Amniotic Fluid Embolism (see Amniotic Fluid Embolism)
- Clinical
- Hemorrhage
- Hypotension (see Hypotension)
- Tachycardia (see Sinus Tachycardia)
- Clinical
- Acute Pancreatitis (see Acute Pancreatitis)
- Clinical
- Abdominal Pain (see Abdominal Pain)
- Fever (see Fever)
- Nausea/Vomiting (see Nausea and Vomiting)
- Clinical
- Acute Fatty Liver of Pregnancy (see Acute Fatty Liver of Pregnancy)
- Clinical
- Abdominal Pain (see Abdominal Pain)
- Altered Mental Status (see Altered Mental Status)
- Fatigue (see Fatigue)
- Jaundice (see Jaundice)
- Nausea/Vomiting (see Nausea and Vomiting)
- Clinical
- Adverse Drug Reaction/Drug Fever
- Clinical
- Angioedema (see Angioedema)
- Fever (see Fever)
- Hypotension (see Hypotension)
- Rash
- Relative Bradycardia (see Sinus Bradycardia)
- Clinical
- Acute Liver Failure (Drug-Associated/Viral)
- Clinical
- Abdominal Pain (see Abdominal Pain)
- Altered Mental Status (see Altered Mental Status)
- Jaundice (see Jaundice)
- Nausea/Vomiting (see Nausea and Vomiting)
- Clinical
- Acute Adrenal Insufficiency (see Acute Adrenal Insufficiency)
- Clinical
- Anorexia (see Anorexia)
- Fatigue (see Fatigue)
- Fever (see Fever)
- Hypotension (see Hypotension)
- Nausea (see Nausea and Vomiting)
- Weakness (see Weakness)
- Weight Loss (see Weight Loss,)
- Clinical
- Acute Pituitary Insufficiency (see Acute Pituitary Insufficiency)
- Clinical
- Failure to Lactate
- Hypotension (see Hypotension)
- Polydipsia (see Polydipsia)
- Polyuria (see Polyuria)
- Relative Bradycardia (see Sinus Bradycardia)
- Clinical
- Autoimmune Disease
- Clinical
- Arthritis (see Arthritis)
- Diagnostic Serology
- Dry Eyes (see Dry Eyes)
- Dry Mouth (Xerostomia) (see Xerostomia)
- Low-Grade Fever (see Fever)
- Malar Rash (see Malar Rash)
- Oral Ulcers (see Mucocutaneous Ulcers)
- Clinical
- Concealed Hemorrhage including Ectopic Pregnancy
- Clinical
- Hypotension (see Hypotension)
- Low-Grade Fever (see Fever)
- Tachycardia (see Tachycardia)
- Clinical
- Disseminated Malignancy
- Clinical
- Low-Grade Fever (see Fever)
- Weight Loss (see Weight Loss)
- Clinical
- Pelvic Thrombosis
- Clinical
- Fever (see Fever)
- Pelvic Pain (see Abdominal Pain)
- Clinical
- Transfusion Reactions
- Clinical
- Arrhythmia
- Hematuria (see Hematuria)
- Hemorrhage
- High Fever (see Fever)
- Hypotension (see Hypotension)
- Rash
- Rigors (see Rigors)
- Tachypnea (see Tachypnea)
- Clinical
Prevention
Clinical Data
Decontamination Strategies
- Randomized Trial of Decontamination in the Prevention of ICU-Acquired Bloodstream Infection in Mechanically-Ventilated Intensive Care Unit Patients (with Moderate-High Antibiotic Resistance Prevalence) (JAMA, 2018) [MEDLINE]
- Chlorhexidine Gluconate 2% Mouthwash, Selective Oropharyngeal Decontamination (Mouth Paste with Colistin, Tobramycin, and Nystatin), and Selective Digestive Tract Decontamination (Same Mouth Paste and Gastrointestinal Suspension with the Same Antibiotics) Were Not Associated with a Decrease in ICU-Acquired Bloodstream Infections Caused by Multidrug-Resistant Gram-Negative Bacteria, as Compared to Standard Care
References
General
- Cardiovascular management of septic shock. Crit Care Med 2003; 31:946-955
- Management of sepsis. N Engl J Med. 2006;355:1699-1713
- Sepsis-associated encephalopathy and its differential diagnosis. Crit Care Med. 2009 Oct;37(10 Suppl):S331-6. doi: 10.1097/CCM.0b013e3181b6ed58 [MEDLINE]
- Bundled care for septic shock: an analysis of clinical trials. Crit Care Med. 2010;38(2):668–78 [MEDLINE]
- The Surviving Sepsis Campaign: results of an international guideline-based performance improvement program targeting severe sepsis. Crit Care Med. 2010;38(2):367–74 [MEDLINE]
- Surviving sepsis campaign: international guidelines for management of severe sepsis and septic shock: 2012. Crit Care Med. 2013 Feb;41(2):580-637. doi: 10.1097/CCM.0b013e31827e83af [MEDLINE]
- Novel therapies for septic shock over the past 4 decades. JAMA. 2011 Jul 13;306(2):194-9 [MEDLINE]
- Outcomes of the Surviving Sepsis Campaign in intensive care units in the USA and Europe: a prospective cohort study. Lancet Infect Dis. 2012;12(12):919–24 [MEDLINE]
- The Surviving Sepsis Campaign’s Revised Sepsis Bundles. Curr Infect Dis Rep. 2013 Oct;15(5):385-93 [MEDLINE]
- Severe sepsis and septic shock. N Engl J Med. 2013 Aug 29;369(9):840-51. doi: 10.1056/NEJMra1208623 [MEDLINE]
- Current controversies in the support of sepsis. Curr Opin Crit Care. 2014 Dec;20(6):681-4. doi: 10.1097/MCC.0000000000000154 [MEDLINE]
- Severe sepsis during pregnancy. Clin Obstet Gynecol. 2014 Dec;57(4):827-34. doi: 10.1097/GRF.0000000000000066 [MEDLINE]
- Sepsis: a roadmap for future research. Lancet Infect Dis. 2015 May;15(5):581-614 [MEDLINE]
- Assessment of Clinical Criteria for Sepsis For the Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA. 2016 Feb 23;315(8):762-74. doi: 10.1001/jama.2016.0288 [MEDLINE]
- Developing a New Definition and Assessing New Clinical Criteria for Septic Shock: For the Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA. 2016 Feb 23;315(8):775-87. doi: 10.1001/jama.2016.0289 [MEDLINE]
- The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA. 2016 Feb 23;315(8):801-10. doi: 10.1001/jama.2016.0287 [MEDLINE]
- Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016. Intensive Care Med. 2017 Jan 18. doi: 10.1007/s00134-017-4683-6 [MEDLINE]
- Infectious Diseases Society of America (IDSA) POSITION STATEMENT: Why IDSA Did Not Endorse the Surviving Sepsis Campaign Guidelines. Clin Infect Dis. 2018;66(10):1631 [MEDLINE]
Clinical Sepsis Scoring
- Definitions for sepsis and organ failure and guidelines for the use of innovative therapies in sepsis. The ACCP/SCCM Consensus Conference Committee. American College of Chest Physicians/Society of Critical Care Medicine. Chest. 1992 Jun;101(6):1644-55 [MEDLINE]
- 2001 SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference. Intensive Care Med. 2003 Apr;29(4):530-8 [MEDLINE]
- The SOFA (Sepsis-related Organ Failure Assessment) score to describe organ dysfunction/failure. On behalf of the Working Group on Sepsis-Related Problems of the European Society of Intensive Care Medicine. Intensive Care Med. 1996 Jul;22(7):707-10 [MEDLINE]
- Use of the SOFA score to assess the incidence of organ dysfunction/failure in intensive care units: results of a multicenter, prospective study. Working group on “sepsis-related problems” of the European Society of Intensive Care Medicine. Crit Care Med. 1998;26(11):1793 [MEDLINE]
- Application of the Sequential Organ Failure Assessment (SOFA) score to patients with cancer admitted to the intensive care unit. Am J Hosp Palliat Care. 2009 Oct-Nov;26(5):341-6 [MEDLINE]
- Sequential Organ Failure Assessment predicts the outcome of SCT recipients admitted to intensive care unit. Bone Marrow Transplant. 2010 Apr;45(4):682-8 [MEDLINE]
- The sequential organ failure assessment (SOFA) score is prognostically superior to the model for end-stage liver disease (MELD) and MELD variants following paracetamol (acetaminophen) overdose. Aliment Pharmacol Ther. 2012 Mar;35(6):705-13 [MEDLINE]
- Comparison between Sequential Organ Failure Assessment score (SOFA) and Cardiac Surgery Score (CASUS) for mortality prediction after cardiac surgery. Thorac Cardiovasc Surg. 2012 Feb;60(1):35-42 [MEDLINE]
- Maternal physiologic parameters in relationship to systemic inflammatory response syndrome criteria: a systematic review and meta-analysis. Obstet Gynecol. 2014;124(3):535 [MEDLINE]
- Scoring systems for 6-month mortality in critically ill cirrhotic patients: a prospective analysis of chronic liver failure – sequential organ failure assessment score (CLIF-SOFA). Aliment Pharmacol Ther. 2014 Nov;40(9):1056-65 [MEDLINE]
- Systemic inflammatory response syndrome criteria in defining severe sepsis. N Engl J Med. 2015 Apr;372(17):1629-38 [MEDLINE]
- Incidence and Prognostic Value of the Systemic Inflammatory Response Syndrome and Organ Dysfunctions in Ward Patients. Am J Respir Crit Care Med. 2015 Oct;192(8):958-64 [MEDLINE]
- Predictors of outcome in decompensated liver disease: validation of the SOFA-L score. Ir Med J. 2015 Apr;108(4):114-6 [MEDLINE]
- Assessment of Clinical Criteria for Sepsis: For the Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA. 2016 Feb 23;315(8):762-74. doi: 10.1001/jama.2016.0288 [MEDLINE]
- Developing a New Definition and Assessing New Clinical Criteria for Septic Shock: For the Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA. 2016 Feb 23;315(8):775-87. doi: 10.1001/jama.2016.0289 [MEDLINE]
- Prognostic Accuracy of the SOFA Score, SIRS Criteria, and qSOFA Score for In-Hospital Mortality Among Adults With Suspected Infection Admitted to the Intensive Care Unit. JAMA. 2017 Jan 17;317(3):290-300. doi: 10.1001/jama.2016.20328 [MEDLINE]
- Internal Validation of the Sepsis in Obstetrics Score to Identify Risk of Morbidity From Sepsis in Pregnancy. Obstet Gynecol. 2017;130(4):747 [MEDLINE]
- Assessment of mortality by qSOFA in patients with sepsis outside ICU: A post hoc subgroup analysis by the Japanese Association for Acute Medicine Sepsis Registry Study Group. J Infect Chemother. 2017 Nov;23(11):757-762. doi: 10.1016/j.jiac.2017.07.005 [MEDLINE]
- SOMANZ guidelines for the investigation and management sepsis in pregnancy. Aust N Z J Obstet Gynaecol. 2017;57(5):540 [MEDLINE]
- Prognostic Accuracy of Sepsis-3 Criteria for In-Hospital Mortality Among Patients With Suspected Infection Presenting to the Emergency Department. JAMA. 2017;317(3):301 [MEDLINE]
- Comparison of QSOFA score and SIRS criteria as screening mechanisms for emergency department sepsis. Am J Emerg Med. 2017;35(11):1730 [MEDLINE]
- Accuracy of Positive qSOFA Criteria for Predicting 28-Day Mortality in Critically Ill Septic Patients During the Early Period After Emergency Department Presentation. Ann Emerg Med. 2018;71(1):1 [MEDLINE]
- A Comparison of the Quick-SOFA and Systemic Inflammatory Response Syndrome Criteria for the Diagnosis of Sepsis and Prediction of Mortality: A Systematic Review and Meta-Analysis. Chest. 2018;153(3):646 [MEDLINE]
- SAILORS Study. Association of the Quick Sequential (Sepsis-Related) Organ Failure Assessment (qSOFA) Score With Excess Hospital Mortality in Adults With Suspected Infection in Low- and Middle-Income Countries. JAMA. 2018;319(21):2202 [MEDLINE]
- Peripheral Oxygen Saturation Facilitates Assessment of Respiratory Dysfunction in the Sequential Organ Failure Assessment Score With Implications for the Sepsis-3 Criteria. Crit Care Med. 2021 Aug 18. doi: 10.1097/CCM.0000000000005318 [MEDLINE]
Clinical Manifestations
General
- A prospective, observational registry of patients with severe sepsis: the Canadian Sepsis Treatment and Response Registry. Crit Care Med. 2009 Jan;37(1):81-8. doi: 10.1097/CCM.0b013e31819285f0 [MEDLINE]
- Likelihood of infection in patients with presumed sepsis at the time of intensive care unit admission: a cohort study. Crit Care. 2015 Sep 7;19:319. doi: 10.1186/s13054-015-1035-1 [MEDLINE]
Cardiovascular Manifestations
- Brain natriuretic peptide: a marker of myocardial dysfunction and prognosis during severe sepsis. Crit Care Med 2004;32:660–5 [MEDLINE]
- Utility of B-type natriuretic peptide for the evaluation of intensive care unit shock. Crit Care Med 2004;32:1643–7 [MEDLINE]
- Relationship between B-type natriuretic peptides and pulmonary capillary wedge pressure in the intensive care unit. J Am Coll Cardiol 2005;45:1667–71 [MEDLINE]
- Elevated cardiac troponin measurements in critically ill patients. Arch Intern Med. 2006 Dec 11-25;166(22):2446-54 [MEDLINE]
- Troponin-I as a prognosticator of mortality in severe sepsis patients. J Crit Care. 2010 Jun;25(2):270-5. doi: 10.1016/j.jcrc.2009.12.001. Epub 2010 Feb 10 [MEDLINE]
- Incident stroke and mortality associated with new-onset atrial fibrillation in patients hospitalized with severe sepsis. JAMA. 2011 Nov;306(20):2248-54 [MEDLINE]
- Elevated cardiac troponin T levels in critically ill patients with sepsis. Am J Med. 2013 Dec;126(12):1114-21. doi: 10.1016/j.amjmed.2013.06.029. Epub 2013 Sep 28 [MEDLINE]
- Cardiac ischemia in patients with septic shock randomized to vasopressin or norepinephrine. Crit Care. 2013 Jun 20;17(3):R117. doi: 10.1186/cc12789 [MEDLINE]
- Atrial Fibrillation Is an Independent Predictor of Mortality in Critically Ill Patients. Crit Care Med. 2015 Oct;43(10):2104-11. doi: 10.1097/CCM.0000000000001166 [MEDLINE]
- Raised cardiac troponin in intensive care patients with sepsis, in the absence of angiographically documented coronary artery disease: A systematic review. J Intensive Care Soc. 2015 Feb;16(1):52-57. doi: 10.1177/1751143714555303 [MEDLINE]
- Practice Patterns and Outcomes of Treatments for Atrial Fibrillation During Sepsis: A Propensity-Matched Cohort Study. Chest. 2016 Jan;149(1):74-83. doi: 10.1378/chest.15-0959. Epub 2016 Jan 6 [MEDLINE]
- Incidence, Predictors, and Outcomes of New-Onset Atrial Fibrillation in Critically Ill Patients with Sepsis. A Cohort Study. Am J Respir Crit Care Med. 2017 Jan;195(2):205-211 [MEDLINE]
- Takotsubo Cardiomyopathy and Sepsis. Angiology. 2017 Apr;68(4):288-303. doi: 10.1177/0003319716653886 [MEDLINE]
- Characteristics, predictors and outcomes of new-onset QT prolongation in sepsis: a multicenter retrospective study. Crit Care. 2024 Apr 9;28(1):115. doi: 10.1186/s13054-024-04879-2 [MEDLINE]
Endocrinologic Manifestations
- Association between hyperglycemia and increased hospital mortality in a heterogeneous population of critically ill patients. Mayo Clin Proc. 2003;78(12):1471 [MEDLINE]
- Prevalence, incidence, and clinical resolution of insulin resistance in critically ill patients: an observational study. JPEN J Parenter Enteral Nutr. 2008;32(3):227 [MEDLINE]
Gastrointestinal Manifestations
- Incidence and prognosis of early hepatic dysfunction in critically ill patients–a prospective multicenter study. Crit Care Med. 2007 Apr;35(4):1099-104 [MEDLINE]
Hematologic Manifestations
- Towards definition, clinical and laboratory criteria, and a scoring system for disseminated intravascular coagulation. Thromb Haemost. 2001;86:1327–30 [MEDLINE]
- Circulating Histones Are Major Mediators of Cardiac Injury in Patients With Sepsis. Crit Care Med. 2015 Oct;43(10):2094-103. doi: 10.1097/CCM.0000000000001162 [MEDLINE]
- Sepsis-associated thrombocytopenia. Thromb Res. 2016 May;141:11-6. doi: 10.1016/j.thromres.2016.02.022. Epub 2016 Mar 2 [MEDLINE]
- Histone-Associated Thrombocytopenia in Patients Who Are Critically Ill. JAMA. 2016;315(8):817-819. doi:10.1001/jama.2016.0136 [MEDLINE]
- Diagnosis and management of sepsis-induced coagulopathy and disseminated intravascular coagulation. J Thromb Haemost. 2019 Nov;17(11):1989-1994. doi: 10.1111/jth.14578 [MEDLINE]
Infectious Manifestations
- Incidence, Risk Factors, and Attributable Mortality of Secondary Infections in the Intensive Care Unit After Admission for Sepsis. JAMA. 2016;315(14):1469 [MEDLINE]
Pulmonary Manifestations
- Chronic alcohol abuse is associated with an increased incidence of acute respiratory distress syndrome and severity of multiple organ dysfunction in patients with septic shock. Crit Care Med. 2003;31(3):869 [MEDLINE]
- Risk factors for the development of acute lung injury in patients with septic shock: an observational cohort study. Crit Care Med. 2008;36(5):1518 [MEDLINE]
- Early risk factors and the role of fluid administration in developing acute respiratory distress syndrome in septic patients. Ann Intensive Care. 2017;7(1):11. Epub 2017 Jan 23 [MEDLINE]
Renal Manifestations
- Acute Kidney Injury Requiring Dialysis in Severe Sepsis. Am J Respir Crit Care Med. 2015 Oct 15;192(8):951-7. doi: 10.1164/rccm.201502-0329OC [MEDLINE] -Extended Mortality and Chronic Kidney Disease After Septic Acute Kidney Injury. J Intensive Care Med. 2018 Jan 1:885066618764617. doi: 10.1177/0885066618764617 [MEDLINE]
Toxicologic Manifestations
- Elevated methemoglobin in patients with sepsis. Acta Anaesthesiol Scand. 1998 Jul;42(6):713-6 [MEDLINE]
Vascular Manifestations
- Symmetrical peripheral gangrene in critical illness. Transfus Apher Sci. 2021 Apr;60(2):103094. doi: 10.1016/j.transci.2021.103094 [MEDLINE]
Prevention
- Decontamination Strategies and Bloodstream Infections With Antibiotic-Resistant Microorganisms in Ventilated Patients: A Randomized Clinical Trial. JAMA. 2018;320(20):208 [MEDLINE]