Acute Ventilatory Failure Exists when pCO2 Increases Enough Above the Patient’s Baseline pCO2 to Produce a Clinically Significant Decrease in pH (i.e. Acidemia)
Note that the Absolute pCO2 Value Alone Does Not Necessarily Indicate the Presence of Acute Ventilatory Failure (as Increased pCO2 Values Can Also Be Observed as Part of Physiologic Respiratory Compensation in Metabolic Alkalosis and in Chronic Hypoventilation)
The Normal Physiologic Response to Hypercapnia is Renal Reabsorption of Bicarbonate (a Process Which Usually Takes a Period of Days)
Pre-Existing Chronic Hypoventilation
In the Special Clinical Context of a Patient with Pre-Existing Chronic Hypercapnia (Chronic Hypoventilation), the Rise in pCO2 Above the Patient’s Baseline Must Be Large Enough to Produce a Clinically Significant Decrease in pH to Be Considered Concomitant Acute Ventilatory Failure
In Some Patients with Pre-Existing Chronic Hypoventilation (with Chronically Elevated Serum Bicarbonate), an Acute Decrease in the Serum Bicarbonate (Due to an Unrelated Metabolic Acidosis) May Be Sufficient to Produce Acidemia without Technically Being Due to Concomitant Acute Ventilatory Failure
In Such Cases, the Clinical Context of the Combined Acid-Base Disturbance is Crucial to Correctly Interpret the Respiratory Component
Example: 50 y/o Morbidly Obese Male with Prior History of Obstructive Sleep Apnea (OSA) and Associated Chronic Hypoventilation (Baseline ABG: ph 7.40, pCO2 60 and Serum Bicarbonate: 36), Now Presents with Superimposed Diabetic Ketoacidosis (Current ABG: pH 7.22, pCO2 60, Serum Bicarbonate: 24)
In This Example, without a Prior ABG (Indicating the Presence of Chronic Hypoventilation), the Patient Might Be Mistakenly Interpreted to Have Acute Ventilatory Failure
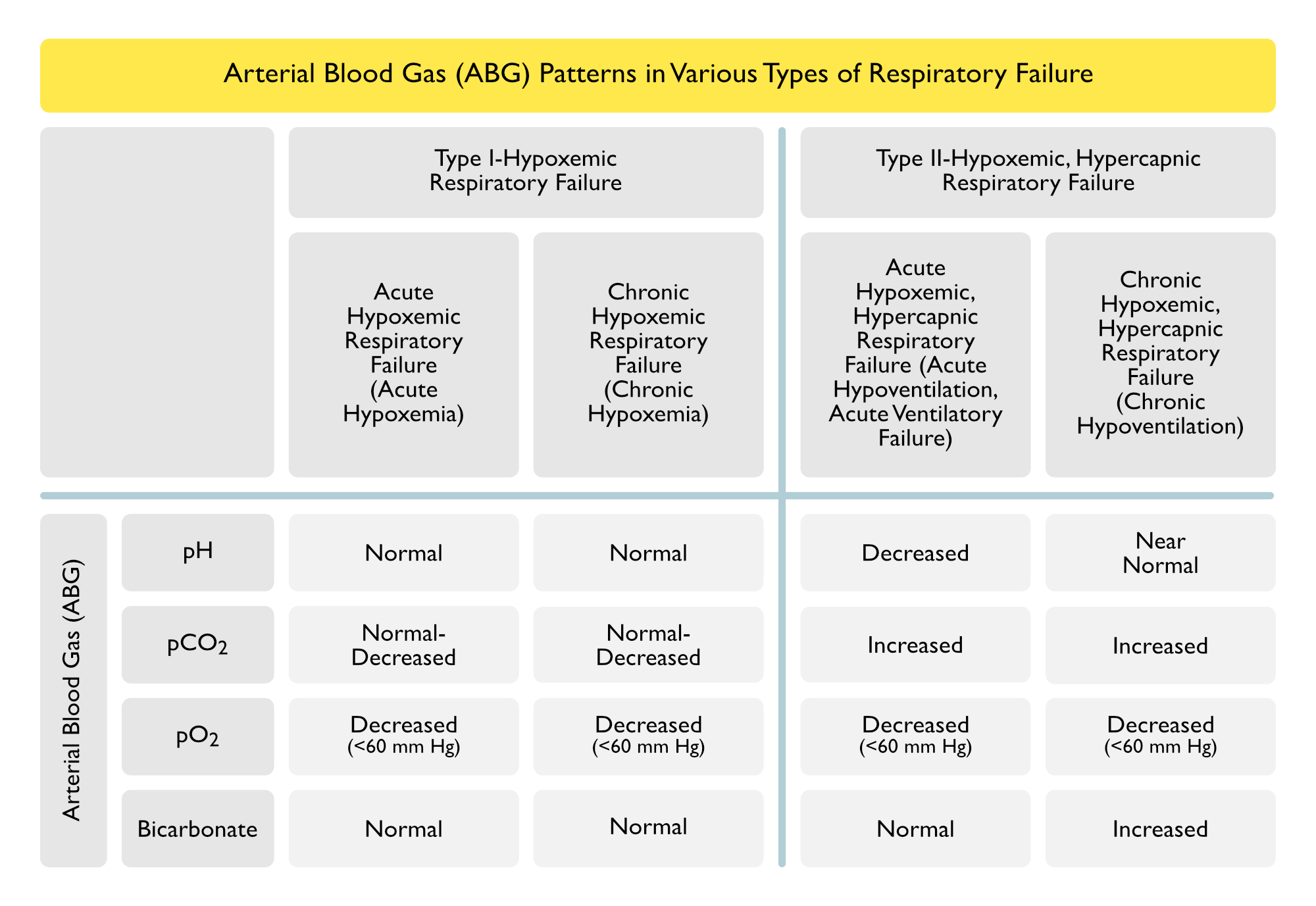
Arterial Blood Gas is an Essential Diagnostic Procedure in Respiratory Failure, as it Provides Information Regarding the Arterial pH, Arterial pCO2, Arterial pO2, and the Serum Bicarbonate
Pulse Oximetry Only Measures Oxygen Saturation and Does Not Provide the pH and pCO2 (the Latter Two of Which are Required to Diagnose Acidemia and Hypercapnia)
End-Tidal Carbon Dioxide (Capnography) (see Capnography)
Capnography May Be Used to Diagnose Hypercapnia
Transcutaneous Carbon Dioxide
Transcutaneous Carbon Dioxide Measurement May Be Used to Diagnose Hypercapnia
Thyroid Function Tests areUseful to Diagnose Both Hypothyroidism and Hyperthyroidism (see Hypothyroidism)
Diagnosis of Chronic Type II-Hypoxemic, Hypercapnic Respiratory Failure
Chemosensitivity Disorders
ABG: normal A-a gradient
PFT’s: normal spirometry and lung volumes (usually), normal MIP+MEP
Neuromuscular Disease
ABG: normal A-a gradient
PFT’s: restriction, decreased MIP+MEP
Upper Airway/Lower Airway/Chest Wall Disease
ABG: increased A-a gradient
PFT’s: restriction or obstruction, normal MIP+MEP
Clinical Manifestations
Practical Daily Assessment of Respiratory Failure
Acute Type II-Hypoxemic, Hypercapnic Respiratory Failure
Upper Airway/Proximal Tracheal Airway Obstruction
Characteristics of Upper Airway/Tracheal Obstruction
Role of Airway Diameter: progressive/gradual airway obstruction can be tolerated until upper airway/tracheal diameter reaches approximately 5-6 mm
Role of the Location of Airway Obstruction: impacts whether inspiratory and/or expiratory flows are more adversely affected by the obstructing lesion
Variable Extrathoracic Upper Airway Obstruction: adversely affects predominantly inspiratory flow (as inspiratory negative intraluminal pressures exacerbate the inspiratory airway narrowing, while expiratory positive intraluminal pressures splints the obstruction open)
Example: vocal cord paralysis -> inspiratory stridor with no expiratory obstruction
Variable Intrathoracic Upper Airway Obstruction: adversely affects predominantly expiratory flow (as inspiratory negative pressures decrease the inspiratory airway narrowing, while expiratory positive intrapleural pressures exacerbate the airway obstruction)
Example: tracheomalacia -> expiratory worsening of airway obstruction
Fixed Upper Airway Obstruction: adversely affects both inspiratory and espiratory flows
Complication by Negative Pressure Pulmonary Edema: negative pressure pulmonary edema may occur in cases with critical, acute upper airway obstruction (such as laryngospasm)
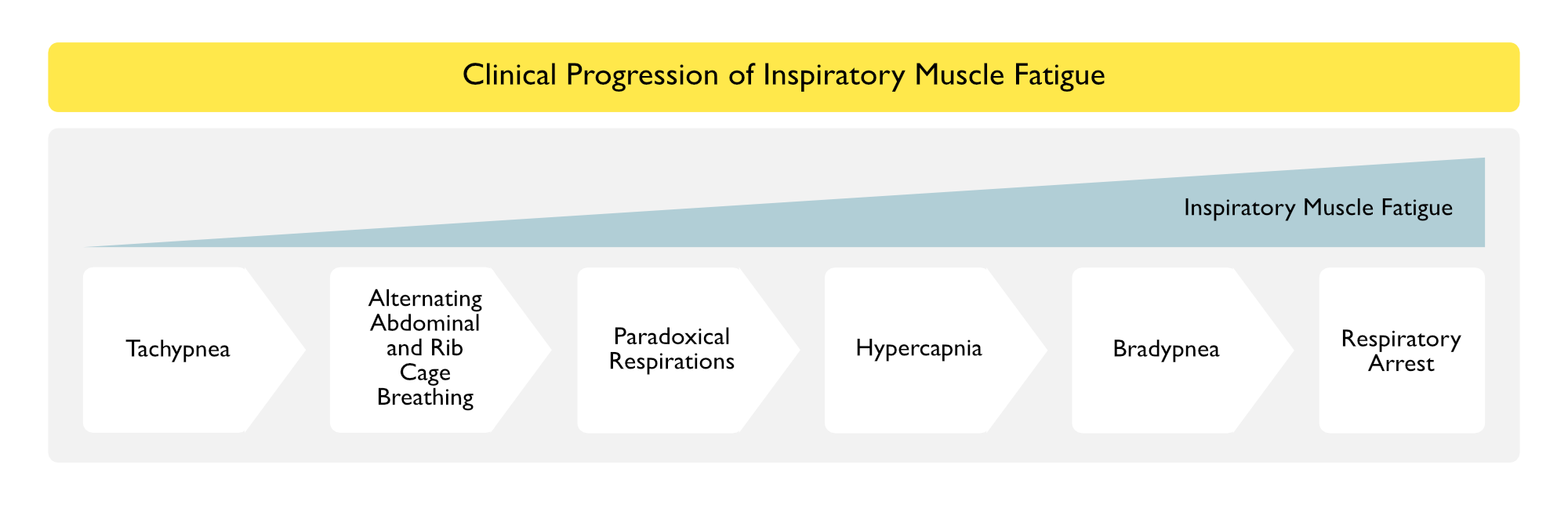
Clinical Manifestations of Inspiratory Muscle Fatigue
Patients with Acute Respiratory Failure Typically Progress Through a Defined Sequence of Clinical Stages (Am J Med, 1982) [MEDLINE]
Study Involved 12 Postextubation Patients with Intact Ventilatory Drive, But Decreased Ventilatory Output
6 of the Patients Manifested EMG Evidence of Inspiratory Muscle Fatigue
Importantly, the Stages were of Variable Duration and Some Patients Skipped Some Stages Altogether
Main Conclusion is that Respiratory Arrest is Typically Heralded by Preceding Clinical Events
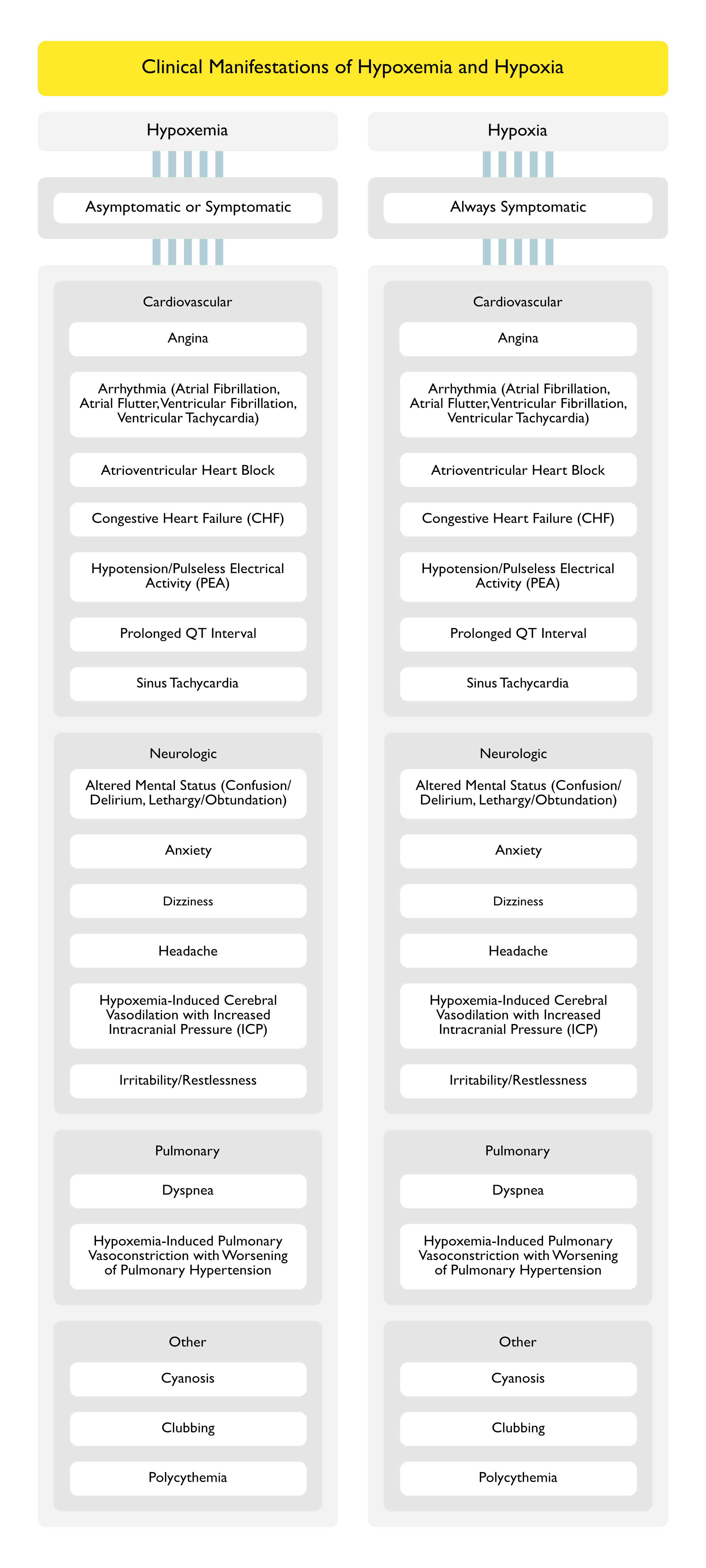
Clinical Manifestation of Hypoxemia (see Hypoxemia)
General Comments
Hypoxemia May Be Asymptomatic, Since Compensatory Mechanisms (Such as Increase in Cardiac Output, Increase in Hemoglobin) May Act to Maintain Tissue Oxygen Delivery and Avoid Hypoxic End-Organ Dysfunction
In Contrast, Hypoxia is Defined as a State of Impaired Tissue Oxygenation and is Always Symptomatic (See Definition Above)
Sleep-Disordered Breathing is Associated with an Increased Risk of Nocturnal Ventricular Arrhythmias (Am J Respir Crit Care Med, 2006) [MEDLINE]
In Patients with Heart Failure and Sleep Apnea, Treatment with CPAP Eliminates Sleep-Disordered Breathing and Decreases Ventricular Irritability (Circulation, 2000) [MEDLINE]
Hypoxemia Has Been Demonstrated to Prolong the QT Interval During Sleep in Patients with Coronary Artery Disease (CAD) (Chest, 1982) [MEDLINE]
Nocturnal Hypoxemia Has Been Demonstrated to Prolong the QT Interval in Patients with Chronic Obstructive Pulmonary Disease (COPD) (NEJM, 1982) [MEDLINE]
Acute Hypoxia Has Been Demonstrated to Prolong the QT Interval in Normal Subjects (Am J Cardiol, 2003) [MEDLINE]
Severe Obstructive Sleep Apnea Has Been Demonstrated to Prolong the QTc Interval in Patients with Congenital Long QT Syndrome (Independent of Age, Sex, BMI, Use of β-Blockers, and History of Syncope), Which is a Biomarker for Sudden Cardiac Death (Sleep, 2015) [MEDLINE] (see Obstructive Sleep Apnea)
Severity of Obstructive Sleep Apnea (as Represented by the Apnea-Hypoxia Index and Apnea Index During Sleep) is Directly Related to the Degree of QT Prolongation in This Population
The Obstructive Sleep Apnea-Related Increase in the QT May Be Mediated by Hypoxic Episodes (Typically Immediately Following the Apnea), Sympathetic Activation (During the Apnea), and/or Vagal Bradyarrhythmias (During the Apnea)
Hypercapnia-Associated Decreased Diaphragmatic Contractility: this decrease in diaphragmatic contractility may contribute further to the development of respiratory failure
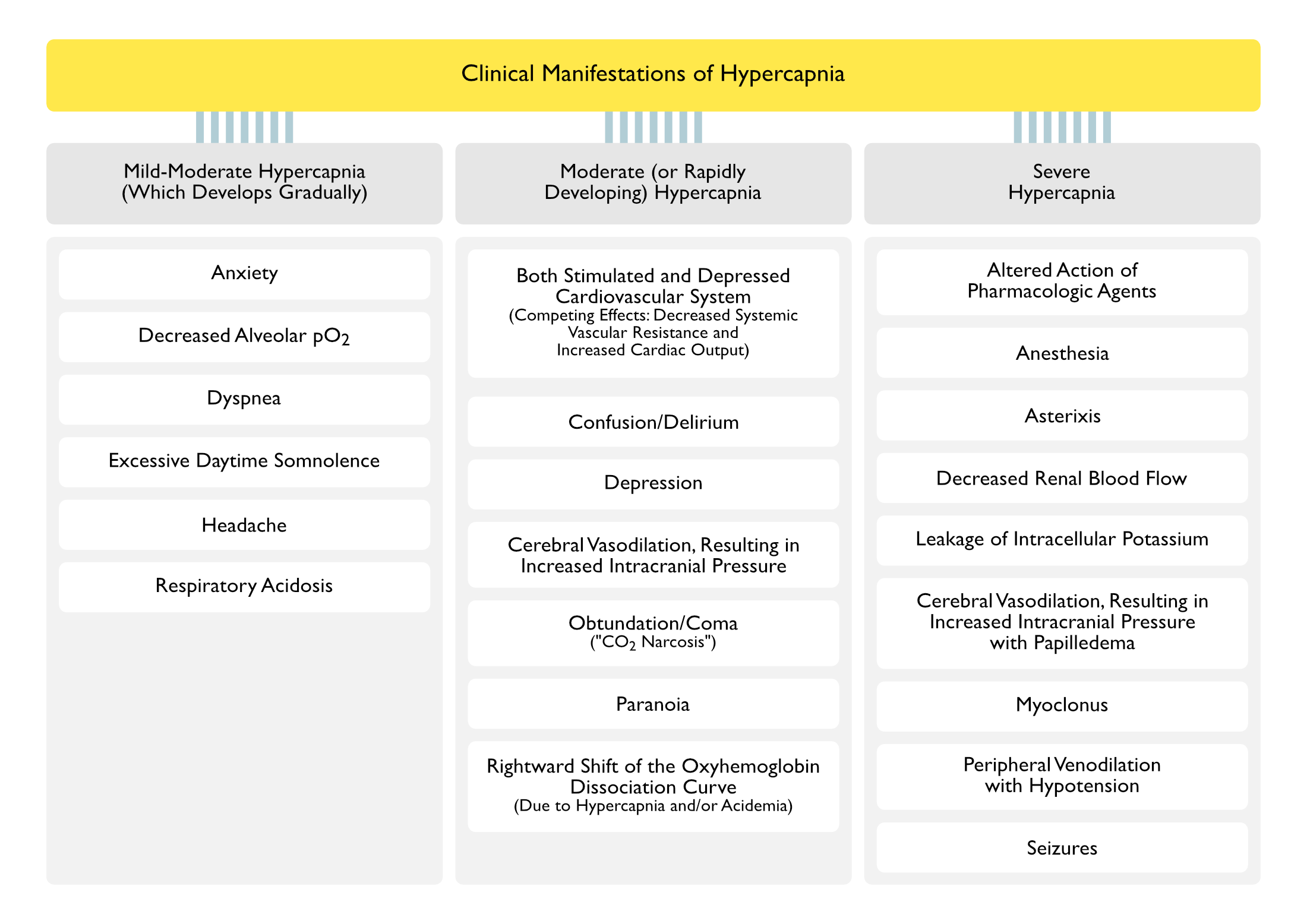
Subsequently, There is Development of Decreased Respiratory Drive, Leading to Worsening Hypercapnia with Depressed Mental Status (“CO2 Narcosis”)
These Later Effects are Mediated Via Increased Brain Glutamine, Increased Brain γ-Aminobutyric Acid (GABA), Decreased Brain Glutamate, and Decreased Brain Aspartate
Rightward Shift of the Oxyhemoglobin Dissociation Curve (Due to Hypercapnia and/or Acidemia): this results in increased oxygen release at the tissues (Bohr Effect)
Decreased Hemoglobin Affinity for Oxygen in the Lungs (with Decreased Oxygen Loading) and Increased Oxygen Unloading at the Tissues (Bohr Effect)
Severe Hypercapnia
Altered Action of Pharmacologic Agents
Due to Intracellular Acidosis, Not Due to the Hypercapnia Itself
Clinicians are Generally Poor at Recognizing the Clinical Signs of Respiratory Failure
In a Study of Clinical Assessment of Patients Requiring CPR, Physicians were Poor at Recognizing a Lack of Respiratory Effort (Ann Emerg Med, 1999) [MEDLINE]
Approximately 89.7% of Emergency Personnel Accurately Recognized Failure of Respiratory Effort
Approximately 84.5% of Physicians Accurately Recognized Failure of Respiratory Effort
Approximately 78.4% of Medical Students Accurately Recognized Failure of Respiratory Effort
In a Study of Automated Graphical Assessment of Respiratory Activity During Endoscopy, Visual Recognition of Changes Respiratory Activity (Which Might Precede the Development of Hypoxemia) was Poor (Gastrointest Endosc, 2002) [MEDLINE]
Capnography was an Excellent Indicator of Respiratory Rate, as Compared to Auscultation (r = 0.967, p < 0.001)
Fifty Four Episodes of Apnea or Disordered Respiration Occurred in 28 Patients (Mean Duration: 70.8 sec)
Only 50% of the Apnea or Disordered Respiration Episodes were Detected by Pulse Oximetry and None were Detected by Visual Assessment (p < 0.0010)
Chronic Type II-Hypoxemic, Hypercapnic Respiratory Failure
Consequences of Hypoventilation-Associated Sleep-Disordered Breathing
However, Provider Should Judiciously Use Supplemental Oxygen in Patients with Type II-Hypoxemic, Hypercapnic Respiratory Failure: generally titrated to achieve SpO2 90-94%
Risk Factors for Oxygen-Induced Worsening of Hypercapnia in Chronically Hypercapnic Patients with COPD (Am J Med, 1978) [MEDLINE]
History of Baseline Hypercapnia with/without Oxygen Administration
Low Initial pH (<7.33) and/or Low Arterial pO2
Mechanisms by Which Supplemental Oxygen May Worsen Hypercapnia
Gastric Decontamination Techniques: may be used in select sedative overdoses (and generally only in an intubated patient, where the risk of aspiration has been minimized
Evaluation/Treatment of Concomitant Sleep-Disordered Breathing/Obstructive Sleep Apnea (OSA): if present
In Retrospective Study of 54 Morbidly Obese Patients (Mean BMI: 44), 87% of Whom Had Concomitant OSA, Chronic Nocturnal Nasal NIPPV Improved Gas Exchange, Dyspnea, and Sleepiness (Chest, 2005) [MEDLINE]
Evaluation/Treatment of Concomitant Congestive Heart Failure (CHF): if present
Weight Loss
Management of Chest Trauma
In Subset of Chest Trauma Patients with Persistent Hypoxemia, NIPPV Has Been Demonstrated to Decrease the Need for Intubation and Shorten Hospital Length of Stay (Chest, 2010) [MEDLINE]
References
Clinical
Effects of carbon dioxide on the cardiovascular system. Anesthesiology. 1960;21:652 [MEDLINE]
Effect of carbon dioxide on diaphragmatic function in human beings. N Engl J Med. 1984;310(14):874 [MEDLINE]
Checking for breathing: evaluation of the diagnostic capability of emergency medical services personnel, physicians, medical students, and medical laypersons. Ann Emerg Med. 1999;34(6):720 [MEDLINE]
Automated graphic assessment of respiratory activity is superior to pulse oximetry and visual assessment for the detection of early respiratory depression during therapeutic upper endoscopy. Gastrointest Endosc. 2002;55(7):826 [MEDLINE]
Treatment
The J. Burns Amberson Lecture. The management of acute respiratory failure in chronic bronchitis and emphysema. Am Rev Respir Dis. 1967;96(4):626 [MEDLINE]
Hypercapnia during oxygen therapy in acute exacerbations of chronic respiratory failure. Hypothesis revisited. Lancet. 1977;2(8036):483 [MEDLINE]
Controlled oxygen administration in acute respiratory failure in chronic obstructive pulmonary disease: a reappraisal. Am J Med. 1978;65(6):896 [MEDLINE]
Severe hypercapnia after low-flow oxygen therapy in patients with neuromuscular disease and diaphragmatic dysfunction. Mayo Clin Proc. 1995;70(4):327 [MEDLINE]
Standards for the diagnosis and treatment of patients with COPD: a summary of the ATS/ERS position paper. Eur Respir J. 2004;23(6):932 [MEDLINE]
Initial oxygen management in patients with an exacerbation of chronic obstructive pulmonary disease. QJM. 2005;98(7):499 [MEDLINE]
The effects of oxygen therapy in patients presenting to an emergency department with exacerbation of chronic obstructive pulmonary disease. Med J Aust. 2007;186(5):235 [MEDLINE]
Extracorporeal carbon dioxide removal: the future of lung support lies in the history. Blood Purif. 2012;34(2):94-106 [MEDLINE]
BTS guideline for oxygen use in adults in healthcare and emergency settings. Thorax. 2017;72(Suppl 1):ii1 [MEDLINE]