

Definitions

Respiratory Failure (see Respiratory Failure)
- Definition
- Respiratory Failure is Defined as the Occurrence of One or Both of the Following
- Decreased pO2, as Predicted for the Patient’s Age (Hypoxemia)
- Increased pCO2 (Hypercapnia) in the Setting of a Normal Serum Bicarbonate
- A Normal Serum Bicarbonate is Specified Here Since a Primary Metabolic Alkalosis (with Increased Serum Bicarbonate) Would Be Expected to Result in a Normal Compensatory Increase in pCO2: this normal compensatory mechanism functions to maintain a normal serum pH and would not be considered “respiratory failure”
- Respiratory Failure is Defined as the Occurrence of One or Both of the Following
Hypoxemia (see Hypoxemia)
- Definition
- Hypoxemia is Defined a Decrease in Hemoglobin Oxygen Saturation (as Assessed by Pulse Oximetry: SaO2 or SpO2) or Decrease in Arterial pO2 (as Assessed by Arterial Blood Gas)
- Note that a Patient May Be Hypoxemic, But Not Be Hypoxic
- Example
- A Young Hypoxemic Patient Can Significantly Increase Their Cardiac Output to Maintain Tissue Oxygen Delivery
- Example
Hypoxia (see Hypoxemia)
- Definition
- Hypoxia is Defined as a State of Impaired Tissue Oxygenation
- Note that a Patient May Be Hypoxic, But Not Be Hypoxemic
- Example
- In Cyanide Intoxication, SaO2 Can Be Normal, But Tissues May Be Hypoxic (see Cyanide)
- Example
Anoxia
- Definition
- Anoxia is Defined as Complete Tissue Deprivation of Oxygen Supply
Hypercapnia (see Hypercapnia)
- Definition
- Hypercapnia is Defined as Increase in Arterial pCO2 (i.e. Increased Arterial Blood Partial Pressure of Carbon Dioxide) to >40 mm Hg
Acidemia
- Definition
- Acidemia is Defined as Decrease in Arterial pH < 7.40 (Due to Either Metabolic or Respiratory Acidosis)
- Note that a Patient Can Be Acidemic without having a Respiratory Acidosis
- Example
- Metabolic Acidosis Can Produce Acidemia without the Presence of a Respiratory Acidosis
- Example
Alkalemia
- Definition
- Alkalemia is Defined an Increase in Arterial pH to >7.40 (Due to Either Metabolic or Respiratory Alkalosis)
Acidosis
- Definition
- Acidosis is Defined as the Presence of an Acid-Producing Acid-Base Disturbance (with or without Concomitant Acidemia)
- Clinical Scenarios in Which an Acidosis is Present, But in Which the pH is Not Acidemic
- Presence of a Metabolic Acidosis May Not Necessarily Result in an Acidemic pH (pH <7.4), Since Respiratory Compensation (Hyperventilation) Occurs, Resulting in an Increase in the Serum pH
- Presence of a (Chronic) Respiratory Acidosis May Not Necessarily Result in an Acidemic pH (pH <7.4), Since Metabolic Compensation (Renal Bicarbonate Retention) Generally Occurs Over a Period of Days, Resulting in an Increase in the Serum pH
Alkalosis
- Definition
- Alkalosis is Defined as the Presence of an Alkali-Producing Acid-Base Disturbance (with or without Concomitant Alkalemia)
- Clinical Scenarios in Which an Alkalosis is Present, But in Which the pH is Not Alkalemic
- Presence of a Metabolic Alkalosis May Not Necessarily Result in an Alkelemic pH (pH >7.4), Since Respiratory Compensation (Hypoventilation) Occurs Rapidly, Resulting in a Decrease in the Serum pH
- Presence of a (Chronic) Respiratory Alkalosis May Not Necessarily Result in an Alkalemic pH (pH >7.4), Since Metabolic Compensation (Renal Bicarbonate Wasting) Generally Occurs Over a Period of Days, Resulting in a Decrease in the Serum pH
Respiratory Acidosis (see Respiratory Acidosis)
- Definition
- Respiratory Acidosis is Defined as a Disorder Which Results in Increase in Arterial pCO2 with an Associated Decrease in Arterial pH
- Note that a Patient Can Have a Respiratory Acidosis without Being Significantly Acidemic
- Example
- Via Normal Compensatory Mechanisms, Chronic Respiratory Acidosis Induces Metabolic (Predominantly Renal) Compensation (with a Increase in Serum Bicarbonate Over Time), Culminating in Minimal Acidemia
- Example
Terms
- PaO2: arterial pO2 (arterial oxygen tension)
- Usually Referred to Simply as pO2
- PAO2: alveolar PO2 (alveolar oxygen tension)
- SpO2: pulse oximetry, as determined by peripheral pulse oximeter (see Pulse Oximetry)
- SaO2: pulse oximetry, as determined by arterial blood gas co-oximeter (see Arterial Blood Gas)
Epidemiology
Demographics of Patients with Acute Hypoxemic, Hypercapnic Respiratory Failure
- Study of Patients with Acute Hypoxemic, Hypercapnic Respiratory Failure Requiring Intensive Care Unit (ICU) Admission (Am J Respir Crit Care Med, 2017) [MEDLINE]
- Presence of Comorbid Conditions
- Approximately 67% (52/78) of Patients Had Chronic Obstructive Pulmonary Disease (COPD): however, only 24% (19/78) had been previously diagnosed with COPD
- Patients without COPD were Predominantly Obese
- Severe Obstructive Sleep Apnea (OSA) was Present in 51% of COPD Patients and 81% of Non-COPD Patients
- Previously Undiagnosed Chronic Diastolic Congestive Heart Failure was Present in 44% of Cases
- Previously Undiagnosed Hypertension was Present in 67% of Cases
- Number of Comorbid Conditions
- More than 50% of the Patients Had ≥3 Comorbidities Which were Known to Precipitate Acute Hypoxemic, Hypercapnic Respiratory Failure
- Multiple Morbidities were Associated with Increased Hospital Length of Stay
- Prognosis
- Hospital Readmission or Death Occurred in 46% of Patients Over an Average of 3.5 mo After Discharge
- Presence of Comorbid Conditions
Classification Schemes for Respiratory Failure
Classification Based on the Predominant Gas Exchange Abnormality and Time of Onset
Type 1-Hypoxemic Respiratory Failure
- Subtypes

Type II-Hypoxemic, Hypercapnic Respiratory Failure)
- Subtypes: the accompanying pH depends on the level of serum bicarbonate (which is dependent on the duration of the hypercapnia)
- Acute Hypoxemic, Hypercapnic Respiratory Failure: pH may be more decreased (due to inadequate time for renal reabsorption of bicarbonate)
- Chronic Hypoxemic, Hypercapnic Respiratory Failure: pH generally normal or only slightly decreased (due to prolonged duration, allowing for renal reabsorption of bicarbonate)
Potential Clinical Exceptions to This Classification Scheme
- Exception: patient with prolonged, severe hypoxemia (initially classified as type I-acute hypoxemic respiratory failure), with the inability to maintain the required work of breathing, subsequently resulting in acute respiratory muscle fatigue with onset of acute hypercapnia (now classified as type II-hypercapnic/ventilatory failure) -> note that the classification of the patient’s respiratory failure changed during their clinical course
- Example: 50 y/o WM with history of COPD and AIDS, presenting with PCP and severe acute hypoxemia
- Exception: patient with increased work of breathing/increased minute ventilation (due to severe metabolic acidosis) without significant hypoxemia or hypercapnia -> note that such a patient may manifest imminent “respiratory failure”, although not technically fulfilling the criteria for either type I or type II respiratory failure
- Example: 30 y/o WM with severe diabetic ketoacidosis (pH 6.9/pCO2 20/pO2 65/bicarb 3 + RR 36)
Classification Based on Anatomic Site of Dysfunction
- Obstructive Lung Disease
- Example: Airway Tumors
- Example: Asthma
- Example: Chronic Obstructive Pulmonary Disease (COPD)
- Example: Mucous Plugging of Airway
- Alveolar Disease
- Example: Acute Lung Injury (ALI)/Adult Respiratory Distress Syndrome (ARDS)
- Example: Diffuse Alveolar Hemorrhage (DAH)
- Example: Pneumonia
- Example: Pulmonary Alveolar Proteinosis (PAP)
- Example: Pulmonary Edema
- Interstitial Lung Disease (ILD)
- Example: Acute Lung Injury (ALI)/Adult Respiratory Distress Syndrome (ARDS)
- Example: Hypersensitivity Pneumonitis (HP)
- Example: Idiopathic Pulmonary Fibrosis (IPF)
- Example: Viral Pneumonia
- Cardiac/Pulmonary Vascular Disease
- Example: Congestive Heart Failure (CHF)
- Example: Idiopathic Pulmonary Arterial Hypertension (IPAH)
- Example: Intracardiac Shunt
- Example: Intrapulmonary Shunt
- Example: Pulmonary Edema
- Example: Pulmonary Embolism
- Pleural Disease
- Example: Fibrothorax
- Example: Pleural Effusion
- Example: Pneumothorax
- Neuromuscular Disease
- Example: Guillain-Barre Syndrome (GBS)
- Example: Myastenia Gravis
- Example: Myopathy
Classification Based on Pathophysiologic Mechanism
- Decreased Inspired Oxygen Pressure
- ABG (typical)
- pCO2: Normal-Decreased
- pO2: Decreased
- ABG (typical)
- Acute Hypoventilation
- ABG (typical)
- pH: Decreased (acidemia)
- pCO2: Increased
- pO2: Decreased
- Serum Bicarbonate: Normal
- ABG (typical)
- Chronic Hypoventilation
- ABG (typical)
- pH: Near Normal
- pCO2: Increased
- pO2: Decreased
- Serum Bicarbonate: Increased
- ABG (typical)
- V/Q Mismatch
- ABG (typical)
- pCO2: Normal-Decreased
- pO2: Decreased
- ABG (typical)
- Shunt
- ABG (typical)
- pCO2: Normal-Decreased
- pO2: Decreased
- ABG (typical)
- Diffusion Impairment
- ABG (typical)
- pCO2: Normal-Decreased
- pO2: Decreased
- ABG (typical)
Etiology of Acute/Chronic Type I-Hypoxemic Respiratory Failure

Pseudohypoxemia
- Mechanism
- ABG Left at Room Temperature (Particularly with Elevated White Blood Cell Count), Resulting in In Vitro Oxygen Consumption by White Blood Cells in the Sample
- Diagnosis
- Arterial Blood Gas (ABG) (see Arterial Blood Gas): decreased pO2
Normal A-a Gradient Hypoxemia
Decreased Inspired PO2 (PiO2)
- Mechanism: decreased PiO2 results in decreased oxygen delivery to the alveoli (with decreased alveolar pO2)
- PiO2 = FIO2 x (Patm – PH20)
- Patm: atmospheric pressure
- PH20: partial pressure of water (equal to 47 mm Hg at 37 degrees C)
- PiO2 = FIO2 x (Patm – PH20)
- Etiology
- Fire in Enclosed Space
- High Altitude (with Decreased Barometric Pressure)
- Sea Level (0 ft): FIO2 = 21%, PIO2= 150, pATM = 760, pH2O = 47 (at 37 degree C)
- Denver (5280 ft): FIO2 = 21%, PIO2= 125, pATM = 640, pH2O = 47 (at 37 degree C)
- Inadvertent Administration of Low FIO2 During Mechanical Ventilation: due to circuit leak, clinician error, etc
Decreased Mixed Venous Oxygen Saturation
- Mechanism: blood returns to the right side of the heart in a severely deoxygenated state and cardiopulmonary system is incapable of re-oxygenating the blood
- Low Mixed Venous Oxygen Saturation Usually Only Results in Arterial Hypoxemia in the Setting of Coexistent Anemia, V/Q Mismatch, or Right-to-Left Shunt: these result in the impaired ability to re-oxygenate the blood
- Etiology
- Decreased Cardiac Output State/Cardiogenic Shock (see Cardiogenic Shock)
- Right Ventricular Dysfunction Due to Right Ventricular infarct (see Coronary Artery Disease)
- Acute Cor Pulmonale Due to Acute Pulmonary Embolism (see Acute Pulmonary Embolism)
- Tamponade (see Tamponade): unclear why this results in decreased mixed venous oxygen saturation
- Increased Tissue Oxygen Extraction
- Decreased Cardiac Output State/Cardiogenic Shock (see Cardiogenic Shock)
Elevated A-a Gradient Hypoxemia
Worsened V/Q Mismatch (Above Levels Observed as Part of Normal Physiology)
- Mechanism
- Worsening of V/Q Mismatch, Aabove the Levels Which are Observed as Part of Normal Human Physiology
- Etiology
- Acute Pulmonary Embolism (Acute PE) (see Acute Pulmonary Embolism)
- Predominant Mechanism is V/Q Mismatch
- Minor Mechanism is Shunt (Particularly Occurs Due to Coexistent Atelectasis)
- Atelectasis (see Atelectasis)
- Hemodialysis-Associated Hypoxemia (see Hemodialysis,)
- Interstitial Lung Disease (ILD) (see Interstitial Lung Disease)
- Leukostasis (see Leukostasis)
- Obstructive Lung Disease (see Obstructive Lung Disease)
- Asthma (see Asthma)
- Chronic Obstructive Pulmonary Disease (COPD) (see Chronic Obstructive Pulmonary Disease)
- Pneumonia
- Community-Acquired Pneumonia (CAP) (see Community-Acquired Pneumonia)
- Hospital-Acquired Pneumonia (HAP)/Ventilator-Associated Pneumonia (VAP) (see Hospital-Acquired Pneumonia and Ventilator-Associated Pneumonia
- Pulmonary Vascular Disease (see Pulmonary Hypertension)
- Acute Pulmonary Embolism (Acute PE) (see Acute Pulmonary Embolism)
Intrapulmonary Right-to-Left Shunt (see Intracardiac and Extracardiac Shunt)
- Mechanism
- Shunting of Unoxygenated Blood Through the Lung, Without Undergoing Oxygenation
- Since a Large Intrapulmonary Shunt Can Produce a Region of Near Zero V/Q Ratio, Intrapulmonary Shunt Really Represents the Most Extreme Form of V/Q Mismatch
- Shunt is Classically Characterized by Poor Response of pO2 (or SaO2) to the Administration of Supplemental Oxygen
- Quantification of Shunt Fraction: perform on 100% FIO2 for at least 20 min (to allow nitrogen washout)
- Qs/Qt = (CcO2-CaO2) / (CcO2-CvO2)
- PIO2 = FIO2 x pATM -> at sea level and on 100% FIO2, PIO2 = 760
- PAO2 = PIO2 – (PCO2 x 1.25) -> at sea level and on 100% FIO2, PAO2 = 760 – (PCO2 x 1.25)
- CcO2: end-capillary oxygen content = Hb x 1.39 + (0.003 x PAO2)
- CaO2: arterial oxygen content = Hb x SaO2 x 1.39 + (0.003 x PaO2)
- Use values from ABG
- CvO2: mixed venous oxygen content = Hb x SvO2 x 1.39 + (0.003 x PvO2)
- Use values from Swan-Ganz Catheter
- Normal Shunt Fraction: <5% (this accounts for the normal physiologic degree of anatomical shunt that exists, due to the bronchial and Thebesian circulations)
- Qs/Qt = (CcO2-CaO2) / (CcO2-CvO2)
- Etiology
- Acute Respiratory Distress Syndrome (ARDS) (see Acute Respiratory Distress Syndrome): due to physiologic intrapulmonary shunt
- Acute Pulmonary Embolism (PE) (see Acute Pulmonary Embolism)
- Epidemiology
- Case Report of a Patient with Platypnea-Orthodeoxia Due to Bilateral Lower Lobe Pulmonary Emboli (South Med J, 2011) [MEDLINE]
- Physiology
- Predominant Mechanism is V/Q Mismatch
- Minor Mechanism is Shunt (Particularly Occurs Due to Coexistent Atelectasis)
- Epidemiology
- Atelectasis (see Atelectasis): due to physiologic intrapulmonary shunt
- Hepatopulmonary Syndrome (see Hepatopulmonary Syndrome): due to anatomic intrapulmonary shunt (which often increases with the patient in an upright position, resulting in orthodeoxia/platypnea)
- Intralobar Pulmonary Sequestration (see Pulmonary Sequestration): one reported case of this resulting in an anatomic intrapulmonary shunt
- Pneumonia: due to physiologic intrapulmonary shunt
- Community-Acquired Pneumonia (CAP) (see Community-Acquired Pneumonia)
- Hospital-Acquired Pneumonia (HAP) and Ventilator-Associated Pneumonia (VAP) (see Hospital-Acquired Pneumonia and Ventilator-Associated Pneumonia)
- Pulmonary Arteriovenous Malformation (AVM) (see Pulmonary Arteriovenous Malformation (AVM)): due to anatomic intrapulmonary shunt
Intracardiac Right-to-Left Shunt (see Intracardiac and Extracardiac Shun)
- Mechanism
- Shunting of Unoxygenated Blood from the Right to the Left Side of the Heart, Bypassing the Pulmonary Vascular Bed
- Etiology
- Acute Pulmonary Embolism (Acute PE) with Right to Left Shunt (see Acute Pulmonary Embolism): acutely increased pulmonary artery pressure may result in new or exacerbated right to left shunt through a pre-existing PFO, etc
- Atrial Septal Defect with Right to Left Shunt (see Atrial Septal Defect)
- Patent Ductus Arteriosus with Right to Left Shunt (see Patent Ductus Arteriosus)
- Patent Foramen Ovale with Right to Left Shunt (see Patent Foramen Ovale)
- Tetralogy of Fallot with Right to Left Shunt (see Tetralogy of Fallot): VSD + pulmonary artery stenosis
- Ventricular Septal Defect (VSD) with Right to Left Shunt (see Ventricular Septal Defect)
Diffusion Limitation
- Mechanism
- Limitation of Oxygen Exchange Across the Pulmonary Alveolar-Capillary Membrane
- Thickening of the Alveolar-Capillary Membrane (Associated with Interstitial Fibrosis, Cryptogenic Organizing Pneumonia, ARDS, Asbestos Exposure, etc) Results in Inadequate Red Blood Cell Transit Time in the Pulmonary Circulation, Not Allowing Adequate Equilibration of pO2 Between the Alveolar Gas and Pulmonary Capillary Blood
- Note: diffusion limitation is absent in normal subjects at rest
- Limitation of Oxygen Exchange Across the Pulmonary Alveolar-Capillary Membrane
- Etiology
- Heavy Exercise
- Due to Increased Cardiac Output (with Transient Pulmonary Interstitial Fluid Accumulation) with Decreased Time Available for Oxygen Diffusion
- Effect of Hypoxia: humans will freqently demonstrate diffusion limitation in setting of normoxia, but almost all will demonstrate diffusion limitation in setting of hypoxia
- Race Horses Develop Diffusion Limitation During Severe Exercise (Explaining the Common Practice of Administering Furosemide Prior to Races, with the Goal of Decreasing the Accumulation of High Cardiac Output-Associated Interstitial Pulmonary Edema)
- Severe Interstitial Lung Disease with Exercise (see Interstitial Lung Disease)
- Due to Increased Cardiac Output with Decreased time Available for Oxygen Diffusion Combined with Thickening of the Alveolar-Capillary Membrane
- Heavy Exercise
Etiology of Type II-Hypoxemic, Hypercapnic Respiratory Failure

Acute Type II-Hypoxemic, Hypercapnic Respiratory Failure
Disorders with Decreased Ventilatory Drive
- Metabolic Alkalosis (see Metabolic Alkalosis)
- Mechanism
- Elevated Serum Bicarbonate Increases the Serum pH, Resulting in a Physiologic Decrease in the Central Respiratory Drive
- Mechanism
- Chemosensitivity Disorders
- Carotid Body Dysfunction (see Carotid Body Dysfunction)
- Bilateral Carotid Endarterectomy with Inadvertent Destruction of Peripheral Chemoreceptors (see Carotid Endarterectomy)
- Clinical: decreased hypoxic ventilatory response and a slight increase in the resting arterial pCO2
- Carotid Body Resection (Glomectomy) (see Carotid Body Resection)
- Epidemiology: historically used a treatment for asthma and dyspnea in severe COPD
- Bilateral Carotid Endarterectomy with Inadvertent Destruction of Peripheral Chemoreceptors (see Carotid Endarterectomy)
- Hypercapnia (“CO2 Narcosis”) (see Hypercapnia)
- Mechanism: worsens central hypoventilation
- Hypothyroidism (see Hypothyroidism)
- Mechanism: combination of decreased central respiratory drive, phrenic neuropathy, and respiratory muscle myopathy
- Clinical: manifests as both inspiratory and expiratory muscle weakness
- Carotid Body Dysfunction (see Carotid Body Dysfunction)
- Acute Brainstem Disease
- Autonomic Insufficiency Syndrome (Dysautonomia) (see Autonomic Insufficiency Syndrome)
- Brainstem Abscess (see Brain Abscess)
- Brainstem Encephalitis (see Encephalitis)
- Brainstem Hemorrhage (see Intracerebral Hemorrhage)
- Brainstem Cerebrovascular Accident (CVA) (see Ischemic Cerebrovascular Accident)
- Brainstem Multiple Sclerosis (see Multiple Sclerosis)
- Brainstem Neoplasm
- Brainstem Poliomyelitis (see Poliomyelitis)
- Brainstem Sarcoidosis (see Sarcoidosis)
- Hypogonadism with Testosterone Administration (see Hypogonadism)
- Obesity Hypoventilation Syndrome (OHS) (see Obesity Hypoventilation Syndrome)
- Mechanism: combination of chest wall restriction and decreased central respiratory drive
- Prader-Willi Syndrome (see Prader-Willi Syndrome)
- Mechanism: impaired hypoxic/hypercapnic ventilatory drive
- Primary Alveolar Hypoventilation Syndrome (Ondine’s Curse) (see Primary Alveolar Hypoventilation Syndrome)
- Pharmacologic Central Respiratory Depression
- Opiates (see Opiates)
- Benzodiazepines (see Benzodiazepines)
- Barbiturates (see Barbiturates)
- Etomidate (Amidate) (see Etomidate)
- General Anesthesia (see General Anesthesia)
- Intoxications
- Propylene Glycol Intoxication (see Propylene Glycol)
- Tricyclic Antidepressant Intoxication (see Tricyclic Antidepressants)
- Ketamine (Ketalar) (see Ketamine): respiratory depression may occur with rapid administration or overdosage
- Propofol (Diprivan) (see Propofol)
- Starvation
- Physiology
- Decreased Hypoxic Ventilatory Response: decreases approximately 40% in normal subjects after 10 days of 500 kcal/day dietary restriction (NEJM, 1976) [MEDLINE]
- Little Change in Hypercapnic Ventilatory Response
- Physiology
Disorders with Decreased Ventilatory Output (Despite Increased Ventilatory Effort) Due to Neuromuscular Disease
- Acute Spinal Cord Disease
- High Cervical (Above C3) or Low-Mid Cervical (C3-C8) Spinal Cord Disease (see Cervical Spinal Cord Disease)
- Atlantoaxial Subluxation/Instability (see Atlantoaxial Instability)
- Cervical Disk Disease with Cord Compression
- Cervical Osteoarthritis
- Cervical Space-Occupying Lesions
- Cervical Echinococcal Cyst (see Echinococcosis)
- Cervical Epidural Abscess (see Spinal Epidural Abscess)
- Cervical Gumma (see Syphilis)
- Cervical Spinal Cord Hematoma (Hematomyelia) (see Spinal Cord Hematoma)
- Cervical Tumor
- Cervical Spinal Cord Infarction (see Spinal Cord Infarction)
- Cervical Spine Trauma with Cord Injury
- Diastematomyelia (Bony Spur in Spinal Canal, Which May Compress the Cervical Spinal Cord)
- Post-Cervical Cordotomy: procedure done to achieve pain control may damage ascending and descending tracts
- Spondylolisthesis/Cervical Spondylosis
- Syringomelia (Cavitation of Central Spinal Cord) (see Syringomelia)
- Thoracic Outlet Syndrome (see Thoracic Outlet Syndrome)
- Transverse Myelitis (see Transverse Myelitis)
- Cervical Root Disease (see Cervical Root Disease)
- Cervical Osteoarthritis (with Bilateral C3-C5 Involvement)
- Cervical Spine Manipulation (with Bilateral C3-C5 Involvement)
- Cervical Mass Lesion (with Bilateral C3-C5 Involvement)
- Herpes Zoster (with Bilateral C3-C5 Involvement) (see Varicella-Zoster Virus)
- Multiple Sclerosis (with Bilateral C3-C5 Involvement) (see Multiple Sclerosis)
- Neuralgic Amyotrophy (with Bilateral C3-C5 Involvement): usually affects the brachial plexus
- High Cervical (Above C3) or Low-Mid Cervical (C3-C8) Spinal Cord Disease (see Cervical Spinal Cord Disease)
- Acute Motor Neuron Disease
- Amyotrophic Lateral Sclerosis (ALS) (see Amyotrophic Lateral Sclerosis)
- Mechanism: upper and lower motor neuron disease
- Acute Ventilatory Failure May Be the Initial Presentation of ALS
- Kennedy Disease
- Epidemiology: age of onset from adolescence-old age in males
- Mechanism: X-linked lower motor neuron disease due to androgen receptor mutation
- Poliomyelitis (see Poliomyelitis)
- Post-Polio Syndrome (see Poliomyelitis)
- Primary Lateral Sclerosis
- Mechanism: upper motor neuron disease
- Progressive Muscular Atrophy (PMA)
- Mechanism: lower motor neuron disease
- Spinal Muscular Atrophies
- Mechanism: lower motor neuron disease
- Strychnine Intoxication (see Strychnine)
- Survival of Motor Neuron (SMN) Protein-Associated Spinal Muscular Atrophy (All Involve Gene Defect of the Survival of Motor Neuron Protein)
- Werdnig-Hoffman Disease (Type 1): lower motor neuron disease with onset at 0-6 mo
- Type 2 Survival of Motor Neuron Protein-Associated Spinal Muscular Atrophy: lower motor neuron disease with onset at 7-18 mo
- Kugelberg-Welander Disease (Type 3): lower motor neuron disease with onset at >18 mo
- Adult-Onset (Type 4) Survival of Motor Neuron Protein-Associated Spinal Muscular Atrophy: lower motor neuron disease with adult onset
- Tetanus (see Tetanus)
- Mechanism: damaged upper motor neurons can no longer inhibit lower motor neurons
- Amyotrophic Lateral Sclerosis (ALS) (see Amyotrophic Lateral Sclerosis)
- Acute Peripheral Neuropathy (see Phrenic Neuropathy)
- Infection/Toxin
- Alcoholic Neuropathy (see Alcoholic Neuropathy)
- Buckthorn Berry Intoxication (see Buckthorn Berry Intoxication)
- Diphtheria (see Diphtheria)
- Lyme Disease (see Lyme Disease)
- Neurotoxic Shellfish Poisoning (see Neurotoxic Shellfish)
- Physiology: ingestion of brevetoxin-contaminated bivalve shellfish
- Clinical: descending paralysis (similar to botulism and in contrast to ascending paralysis seen in Guillain-Barre syndrome and tick paralysis)
- Paralytic Shellfish Poisoning (see Paralytic Shellfish)
- Physiology: ingestion of saxitoxin-contaminated bivalve mollusks (cockles, salt and fresh water mussels, butter/little neck clams, scallops, oysters), gastropod mollusks (whelk, abalone, snails), crustaceans (dungeness crabs, shrimp, lobster), and zooplanktivorous fish (atlantic salmon, herring, mackerel)
- Clinical: descending paralysis (similar to botulism and in contrast to ascending paralysis seen in Guillain-Barre syndrome and tick paralysis)
- Poisonous Lizard Bite (see Poisonous Lizard Bite)
- Rabies (see Rabies): ascending paralysis (may mimic that of Guillian-Barre syndrome)
- Widow Spider Bite (see Widow Spider Bite)
- Other
- Acute Intermittent Porphyria (see Acute Intermittent Porphyria)
- Chronic Inflammatory Demyelinating Polyneuropathy (see Chronic Inflammatory Demyelinating Polyneuropathy)
- Critical Illness Polyneuropathy (see ICU-Acquired Weakness)
- Diabetic Neuropathy (see Diabetic Neuropathy)
- Guillain-Barre Syndrome (GBS) (see Guillain-Barre Syndrome)
- Epidemiology
- GBS is the Most Common Etiology of Acute Paralysis and Neuromuscular Ventilatory Failure Presenting to Acute Care Hospitals
- Clinical
- Approximately 33% of Cases Develop Acute Ventilatory Failure
- May Be Acute or Subacute
- Ascending Paralysis (Similar to Tick Paralysis)
- Hypothyroidism (see Hypothyroidism)
- Mechanism: combination of decreased central respiratory drive, phrenic neuropathy, and respiratory muscle myopathy
- Clinical: manifests as both inspiratory and expiratory muscle weakness
- Idiopathic Peripheral Neuropathy
- Mediastinal/Esophageal Surgical Injury or Traumatic Injury of Bilateral Phrenic Nerves
- Epidemiology
- Phrenic Nerve Injury Occurs in 2-20% of Open Heart Surgery Cases
- L>R Sided Injury
- Mechanisms
- Cold Cardioplegia
- Dissection of Left Internal Mammary Artery (LIMA)
- Stretching of Phrenic Nerve
- Multiple Sclerosis (see Multiple Sclerosis)
- Neurofibromatosis (see Neurofibromatosis)
- Epidemiology: case report of bilateral diaphragmatic paralysis
- Systemic Lupus Erythematosus (SLE) (see Systemic Lupus Erythematosus)
- Physiology: neuropathy with vasculitis of phrenic nerves and myopathy
- Acute Neuromuscular Junction Disease (Involving the Respiratory Muscles)
- Myasthenia Gravis (MG) (see Myasthenia Gravis)
- Clinical: acute ventilatory failure may be the initial presentation of myasthenia gravis
- Lambert-Eaton Myasthenic Syndrome (LEMS) (see Lambert-Eaton Myasthenic Syndrome)
- Botulism (see Botulism)
- Physiology: botulinum toxin blocks acetylcholine release at neuromuscular junction
- Clinical: descending paralysis (similar to paralytic-neurotoxic shellfish poisoning)
- Tick Paralysis (see Tick Paralysis)
- Physiology: toxin probably impairs acetylcholine mobilization at motor nerve terminal
- Clinical: ascending paralysis (Similar to Guillain-Barre Syndrome)
- Snake Bite: due to various types of neurotoxins in venom
- Mojave Rattlesnake (Crotalus Scutulatus) (see Rattlesnake Bite): Fasciculin toxin (destroys acetylcholinesterase, resulting in tetany)
- Cobra/King Cobra: α-neurotoxins (inhibition at acetylcholine receptor)
- Sea Snake: α-neurotoxins (inhibition at acetylcholine receptor)
- Mamba: Fasciculin toxin (destroys acetylcholinesterase, resulting in tetany) and Dendrotoxin (blocks ion channels -> blocks nerve transmission)
- Organophosphate/Carbamate Intoxication (see Organophosphates-Carbamates) (PLoS Med, 2008) [MEDLINE]
- VX Nerve Agent (see VX Nerve Agent)
- Pharmacologic Neuromuscular Junction Antagonists
- Aminoglycosides (see Aminoglycosides): usually clinically relevant only in the presence of other neuromuscular junction disease
- Anticholinergics (see Anticholinergic Agents): usually clinically relevant only in the presence of other neuromuscular disease
- Fluoroquinolones (see Fluoroquinolones): usually clinically relevant only in the presence of other neuromuscular disease
- Procainamide (see Procainamide): usually clinically relevant only in the presence of other neuromuscular disease
- Polymyxin B (see Polymyxins): usually clinically relevant only in the presence of other neuromuscular disease
- Sodium Colistimethate (aka Colistin, Polymyxin E) (see Polymyxins): usually clinically relevant only in the presence of other neuromuscular disease
- Paralytics: Succinylcholine, Aminosteroid Non-Depolarizing Blockers (Pancuronium, Vecuronium, etc), Benzylisoquinolone Non-Depolarizing Blockers (Atracurium, etc)
- Myasthenia Gravis (MG) (see Myasthenia Gravis)
- Acute Myopathy/Muscle Dysfunction (Involving Respiratory Muscles) (see Myopathy)
- Periodic Paralysis Syndromes
- Hyperkalemic Periodic Paralysis (see Hyperkalemic Periodic Paralysis)
- Hypokalemic Periodic Paralysis (see Hypokalemic Periodic Paralysis)
- Thyrotoxic Periodic Paralysis (see Thyrotoxic Periodic Paralysis)
- Rheumatologic
- Mixed Connective Tissue Disease (see Mixed Connective Tissue Disease)
- Polydermatomyositis (see Polydermatomyositis)
- Systemic Lupus Erythematosus (SLE) (see Systemic Lupus Erythematosus): neuropathy and myopathy
- Electrolyte-Related
- Hyperkalemia (see Hyperkalemia): may cause respiratory muscle weakness
- Hypomagnesemia (see Hypomagnesemia)
- Hypophosphatemia (see Hypophosphatemia)
- Other
- Bilateral Diaphragmatic Paralysis (see Bilateral Diaphragmatic Paralysis)
- Critical Illness Polymyopathy (see ICU-Acquired Weakness)
- Necrotizing Myopathy from Steroids and Neuromuscular Junction Antagonists
- Hyperthyroidism (see Hyperthyroidism)
- Clinical: proximal and distal myopathy with both inspiratory and expiratory muscle weakness
- Hypothyroidism (see Hypothyroidism)
- Mechanism: combination of decreased central respiratory drive, phrenic neuropathy, and respiratory muscle myopathy
- Clinical: manifests as both inspiratory and expiratory muscle weakness
- Periodic Paralysis Syndromes
Disorders with Decreased Ventilatory Output (Despite Increased Ventilatory Effort) Due to Excessive Ventilatory Demand
- Acute Upper Airway Obstruction (with Increased Work of Breathing) (see Obstructive Lung Disease)
- Bilateral Vocal Fold Immobility (BVFI) (see Bilateral Vocal Fold Immobility) (Select Etiologies Shown)
- Cricoarytenoid Arthritis (see Cricoarytenoid Arthritis)
- Laryngeal Inflammation
- Laryngospasm (see Laryngospasm)
- Neurologic Disease/Dysfunction Involving the Vocal Folds (Select Etiologies Shown)
- Altered Mental Status with Inability to Protect Upper Airway
- Airway Obstruction Occurs Due to Tongue Prolapse into the Posterior Pharynx and/or Decreased Soft Palate Muscular Tone
- Amyotrophic Lateral Sclerosis (ALS) (see Amyotrophic Lateral Sclerosis)
- Idiopathic Bilateral Vocal Cord Paralysis
- Paradoxical Vocal Fold Motion (Vocal Cord Dysfunction) (see Paradoxical Vocal Fold Motion)
- Intubation Injury to Vocal Folds
- Mechanical/Iatrogenic Injury to Vocal Folds
- Other Upper Airway Disease (see Obstructive Lung Disease)
- Croup (see Croup): typically acute
- Infection (Select Etiologies Shown)
- Deep Neck Infection (see Deep Neck Infection): typically acute
- Peritonsillar Abscess (see Peritonsillar Abscess): involving peritonsillar space
- Pretracheal Abscess (see Pretracheal Abscess): involving pretracheal space
- Retropharyngeal Abscess (see Retropharyngeal Abscess): involving retropharyngeal space
- Submandibular Space Abscess/Ludwig’s Angina (see Ludwig’s Angina): involving submandibular space
- Miscellaneous (Select Etiologies Shown)
- Anaphylaxis (see Anaphylaxis): typically acute
- Angioedema (see Angioedema): typically acute
- Bilateral Vocal Fold Immobility (BVFI) (see Bilateral Vocal Fold Immobility) (Select Etiologies Shown)
- Acute Obstructive Lung Disease (with Increased Work of Breathing) (see Obstructive Lung Disease)
- Acute Tracheobronchial Obstruction
- Tracheobronchial Infection
- Tracheobronchial Neoplasm
- Extrinsic Tracheobronchial Compression
- Other Tracheobronchial Obstructive Process
- Asthma Exacerbation (see Asthma)
- Bronchiectasis Exacerbation (see Bronchiectasis)
- Chronic Obstructive Pulmonary Disease (COPD) Exacerbation (see Chronic Obstructive Pulmonary Disease)
- Cystic Fibrosis Exacerbation (see Cystic Fibrosis)
- Acute Tracheobronchial Obstruction
- Acute Parenchymal Lung Disease (with Increased Work of Breathing)
- Acute Respiratory Distress Syndrome (ARDS) (see Acute Respiratory Distress Syndrome)
- Aspiration Pneumonia (see Aspiration Pneumonia)
- Cardiogenic Pulmonary Edema (see Congestive Heart Failure)
- Diffuse Alveolar Hemorrhage (DAH) (see Diffuse Alveolar Hemorrhage)
- Idiopathic Pulmonary Fibrosis (IPF) (see Idiopathic Pulmonary Fibrosis)
- Acute Ventilatory Failure May Be Manifested as the End-Stage of IPF or More Commonly, in Conjunction with Pneumonia, Surgery, or Other Illness
- In End-Stage IPF Requiring Mechanical Ventilation, Lung Compliance Has Been Noted to Be Significantly Decreased
- Pneumonia (see Pneumonia)
- Acute Pleural or Chest Wall Disease (with Increased Work of Breathing)
- Ankylosing Spondylitis (see Ankylosing Spondylitis)
- Chest Wall Trauma
- Fibrothorax (see Fibrothorax)
- Flail Chest (see Flail Chest,)
- Hemothorax (see Pleural Effusion-Hemothorax)
- Kyphoscoliosis (see Kyphoscoliosis)
- Large Pleural Effusion (see Pleural Effusion-Transudate and Pleural Effusion-Exudate)
- Large Pneumothorax (see Pneumothorax)
- Obesity Hypoventilation Syndrome (OHS) (see Obesity Hypoventilation Syndrome)
- Mechanism: combination of chest wall restriction and decreased central respiratory drive
- Pectus Excavatum (see Pectus Excavatum)
- Post-Thoracoplasty (see Thoracoplasty)
- Severe Abdominal Distention
- Ascites (see Ascites)
- Abdominal Compartment Syndrome (see Abdominal Compartment Syndrome)
- Pregnancy (see Pregnancy)
- Increased Dead Space Ventilation (Increased VD/VT Ratio)
- Acute Respiratory Distress Syndrome (ARDS) (see Acute Respiratory Distress Syndrome): very low V/Q and/or intrapulmonary shunt
- End-Stage Interstitial Lung Disease (ILD) (see Interstitial Lung Disease)
- Mechanism
- Due to Increased Physiologic Dead Space
- Mechanism
- Hyperinflation States
- Asthma Exacerbation (see Asthma): very high V/Q with dynamic hyperinflation
- COPD Exacerbation (see Chronic Obstructive Pulmonary Disease): very high V/Q with dynamic hyperinflation
- Pulmonary Hyperinflation (Excessive Exogenous PEEP or Auto-PEEP): generalized pulmonary hypoperfusion
- Pulmonary Vascular Disease (Severe)
- Acute Pulmonary Embolism (Severe) (see Acute Pulmonary Embolism): localized pulmonary hypoperfusion with increased physiologic dead space
- Air Embolism (see Air Embolism): venous air ambolism -> localized pulmonary hypoperfusion with increased physiologic dead space
- Sickle Cell Acute Chest Syndrome (see Sickle Cell Disease)
- Shallow Breathing: due to anatomic dead space
- Shock States
- Cardiogenic Shock (see Cardiogenic Shock): generalized pulmonary hypoperfusion
- Hypovolemic Shock (see Hypovolemic Shock): generalized pulmonary hypoperfusion
- Ventilation During Cardiopulmonary Resuscitation (CPR) (see Cardiopulmonary Resuscitation): generalized pulmonary hypoperfusion
- Increased Carbon Dioxide Production: disorders which increase carbon dioxide production are usually not the primary or sole etiology of hypercapnia (since the usual response to increased pCO2 is to increase minute ventilation), but they can be contributors in patients with decreased ventilatory reserve (patients with chronic lung disease, respiratory muscle weakness, other conditions which increase the VD/VT ratio, etc)
- Inflammation/Hypermetabolism
- Corticosteroids (see Corticosteroids): due to catabolic state
- Exercise
- Fever (see Fever)
- Metabolic Acidosis (see Metabolic Acidosis-General)
- Burns (see Burns)
- Severe Trauma
- Sepsis (see Sepsis): due to catabolic state
- Thyrotoxicosis (see Hyperthryoidism)
- Muscle Activity
- Shivering
- Tetany
- Seizures (see Seizures)
- Malignant Hyperthermia (see Malignant Hyperthermia)
- Excessive Caloric Intake/Overfeeding
- Excessive Caloric Intake (see Enteral Nutrition): especially carbohydrates (which generate more carbon dioxide per calorie than fats)
- Inflammation/Hypermetabolism
- Exogenous Carbon Dioxide Inhalation
- Carbon Dioxide Rebreathing
- Industrial/Laboratory Accident
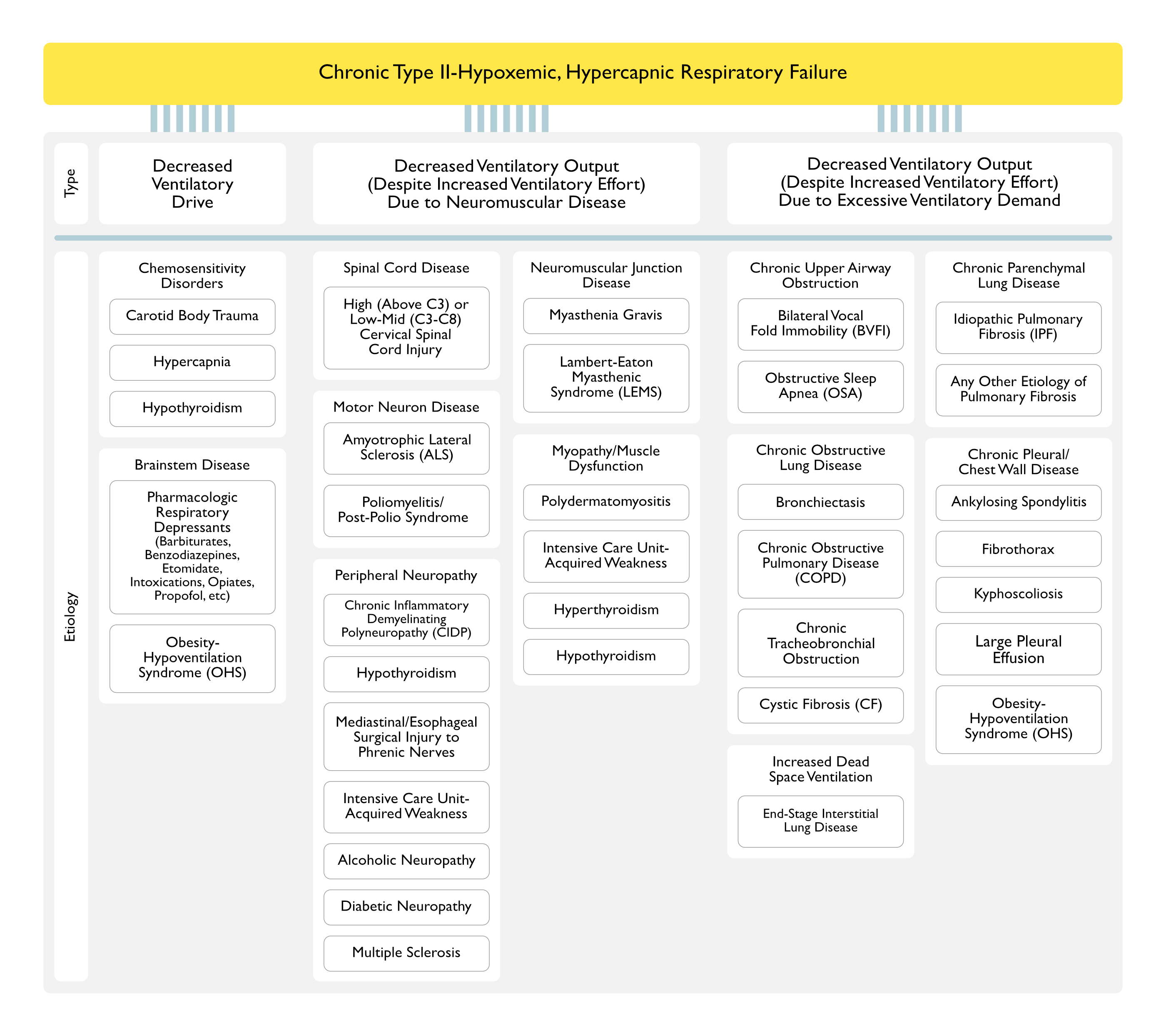
Chronic Type II-Hypoxemic, Hypercapnic Respiratory Failure
Disorders with Decreased Ventilatory Drive
- Metabolic Alkalosis (see Metabolic Alkalosis)
- Mechanism
- Elevated Serum Bicarbonate Increases the Serum pH, Resulting in a Physiologic Decrease in the Central Respiratory Drive
- Mechanism
- Chemosensitivity Disorders
- Carotid Body Dysfunction (see Carotid Body Dysfunction)
- Bilateral Carotid Endarterectomy with Inadvertent Destruction of Peripheral Chemoreceptors (see Carotid Endarterectomy)
- Clinical: decreased hypoxic ventilatory response and a slight increase in the resting arterial pCO2
- Carotid Body Resection (Glomectomy) (see Carotid Body Resection)
- Epidemiology: historically used a treatment for asthma and dyspnea in severe COPD
- Bilateral Carotid Endarterectomy with Inadvertent Destruction of Peripheral Chemoreceptors (see Carotid Endarterectomy)
- Central Sleep Apnea (see Central Sleep Apnea)
- Chronic Mountain Sickness (Monge Disease) (see Chronic Mountain Sickness)
- Mechanism: loss of ventilatory acclimatization to high altitude-associated hypoxia, leading to central hypoventilation
- Hypercapnia (“CO2 Narcosis”) (see Hypercapnia
- Mechanism: worsens central hypoventilation
- Hypothyroidism (see Hypothyroidism)
- Mechanism: combination of decreased central respiratory drive, phrenic neuropathy, and respiratory muscle myopathy
- Clinical: manifests as both inspiratory and expiratory muscle weakness
- Carotid Body Dysfunction (see Carotid Body Dysfunction)
- Chronic Brainstem Disease
- Autonomic Insufficiency Syndrome (Dysautonomia) (see Autonomic Insufficiency Syndrome)
- Brainstem Abscess (see Brain Abscess)
- Brainstem Encephalitis (see Encephalitis)
- Brainstem Intracerebral Hemorrhage (Hemorrhagic Cerebrovascular Accident) (see Intracerebral Hemorrhage)
- Brainstem Ischemic Cerebrovascular Accident (CVA) (see Ischemic Cerebrovascular Accident)
- Brainstem Multiple Sclerosis (see Multiple Sclerosis)
- Brainstem Neoplasm
- Brainstem Poliomyelitis (see Poliomyelitis)
- Brainstem Sarcoidosis (see Sarcoidosis)
- Hypogonadism with Testosterone Administration (see Hypogonadism)
- Obesity Hypoventilation Syndrome (OHS) (see Obesity Hypoventilation Syndrome)
- Mechanism: combination of chest wall restriction and decreased central respiratory drive
- Prader-Willi Syndrome (see Prader-Willi Syndrome
- Mechanism: impaired hypoxic/hypercapnic ventilatory drive
- Primary Alveolar Hypoventilation Syndrome (Ondine’s Curse) (see Primary Alveolar Hypoventilation Syndrome)
- Pharmacologic Central Respiratory Depression
- Opiates (see Opiates)
- Benzodiazepines (see Benzodiazepines)
- Barbiturates (see Barbiturates)
- Starvation
- Physiology
- Decreased Hypoxic Ventilatory Response: decreases approximately 40% in normal subjects after 10 days of 500 kcal/day dietary restriction (NEJM, 1976) [MEDLINE]
- Little Change in Hypercapnic Ventilatory Response
- Physiology
Disorders with Decreased Ventilatory Output (Despite Increased Ventilatory Effort) Due to Neuromuscular Disease
- Spinal Cord Disease
- High Cervical (Above C3) or Low-Mid Cervical (C3-C8) Spinal Cord Disease (see Cervical Spinal Cord Disease)
- Atlantoaxial Subluxation/Instability (see Atlantoaxial Instability)
- Cervical Disk Disease with Cord Compression
- Cervical Osteoarthritis
- Cervical Space-Occupying Lesions
- Cervical Echinococcal Cyst (see Echinococcosis)
- Cervical Epidural Abscess (see Spinal Epidural Abscess)
- Cervical Gumma (see Syphilis)
- Cervical Spinal Cord Hematoma (Hematomyelia) (see Spinal Cord Hematoma)
- Cervical Tumor
- Cervical Spinal Cord Infarction (see Spinal Cord Infarction)
- Cervical Spine Trauma with Cord Injury
- Diastematomyelia (Bony Spur in Spinal Canal, Which May Compress the Cervical Spinal Cord)
- Post-Cervical Cordotomy: procedure done to achieve pain control may damage ascending and descending tracts
- Spondylolisthesis/Cervical Spondylosis
- Syringomelia (Cavitation of Central Spinal Cord) (see Syringomelia)
- Thoracic Outlet Syndrome (see Thoracic Outlet Syndrome)
- Transverse Myelitis (see Transverse Myelitis)
- Cervical Root Disease (see Cervical Root Disease)
- Cervical Osteoarthritis (with Bilateral C3-C5 Involvement)
- Cervical Spine Manipulation (with Bilateral C3-C5 Involvement)
- Cervical Mass Lesion (with Bilateral C3-C5 Involvement)
- Herpes Zoster (with Bilateral C3-C5 Involvement) (see Varicella-Zoster Virus)
- Multiple Sclerosis (with Bilateral C3-C5 Involvement) (see Multiple Sclerosis)
- Neuralgic Amyotrophy (with Bilateral C3-C5 Involvement): usually affects the brachial plexus
- High Cervical (Above C3) or Low-Mid Cervical (C3-C8) Spinal Cord Disease (see Cervical Spinal Cord Disease)
- Motor Neuron Disease
- Amyotrophic Lateral Sclerosis (ALS) (see Amyotrophic Lateral Sclerosis)
- Mechanism: upper and lower motor neuron disease
- Clinical: acute ventilatory failure may be the initial presentation of ALS
- Kennedy Disease
- Epidemiology: age of onset from adolescence-old age in males
- Mechanism: X-linked lower motor neuron disease due to androgen receptor mutation
- Poliomyelitis (see Poliomyelitis)
- Post-Polio Syndrome (see Poliomyelitis)
- Primary Lateral Sclerosis
- Mechanism: upper motor neuron disease
- Progressive Muscular Atrophy (PMA)
- Mechanism: lower motor neuron disease
- Spinal Muscular Atrophies
- Mechanism: lower motor neuron disease
- Strychnine Intoxication (see Strychnine)
- Survival of Motor Neuron (SMN) Protein-Associated Spinal Muscular Atrophy (All Involve Gene Defect of the Survival of Motor Neuron Protein)
- Werdnig-Hoffman Disease (Type 1): lower motor neuron disease with onset at 0-6 mo
- Type 2 Survival of Motor Neuron Protein-Associated Spinal Muscular Atrophy: lower motor neuron disease with onset at 7-18 mo
- Kugelberg-Welander Disease (Type 3): lower motor neuron disease with onset at >18 mo
- Adult-Onset (Type 4) Survival of Motor Neuron Protein-Associated Spinal Muscular Atrophy: lower motor neuron disease with adult onset
- Tetanus (see Tetanus)
- Mechanism: damaged upper motor neurons can no longer inhibit lower motor neurons
- Amyotrophic Lateral Sclerosis (ALS) (see Amyotrophic Lateral Sclerosis)
- Peripheral Neuropathy (see Phrenic Neuropathy)
- Infection/Toxin
- Alcoholic Neuropathy (see Alcoholic Neuropathy)
- Buckthorn Berry Intoxication (see Buckthorn Berry Intoxication)
- Diphtheria (see Diphtheria)
- Lyme Disease (see Lyme Disease)
- Neurotoxic Shellfish Poisoning (see Neurotoxic Shellfish)
- Physiology: ingestion of brevetoxin-contaminated bivalve shellfish
- Clinical: descending paralysis (similar to botulism and in contrast to ascending paralysis seen in Guillain-Barre syndrome and tick paralysis)
- Paralytic Shellfish Poisoning (see Paralytic Shellfish)
- Physiology: ingestion of saxitoxin-contaminated bivalve mollusks (cockles, salt and fresh water mussels, butter/little neck clams, scallops, oysters), gastropod mollusks (whelk, abalone, snails), crustaceans (dungeness crabs, shrimp, lobster), and zooplanktivorous fish (atlantic salmon, herring, mackerel)
- Clinical: descending paralysis (similar to botulism and in contrast to ascending paralysis seen in Guillain-Barre syndrome and tick paralysis)
- Poisonous Lizard Bite (see Poisonous Lizard Bite)
- Rabies (see Rabies)
- Clinical: ascending paralysis (may mimic that of Guillian-Barre syndrome)
- Widow Spider Bite (see Widow Spider Bite)
- Other
- Acute Intermittent Porphyria (see Acute Intermittent Porphyria)
- Chronic Inflammatory Demyelinating Polyneuropathy (CIDP) (see Chronic Inflammatory Demyelinating Polyneuropathy)
- Critical Illness Polyneuropathy (see ICU-Acquired Weakness)
- Diabetic Neuropathy (see Diabetic Neuropathy)
- Guillain-Barre Syndrome (GBS) (see Guillain-Barre Syndrome)
- Epidemiology
- GBS is the Most Common Etiology of Acute Paralysis and Neuromuscular Ventilatory Failure Presenting to Acute Care Hospitals
- Clinical
- Approximately 33% of Cases Develop Acute Ventilatory Failure
- May Be Acute or Subacute
- Ascending Paralysis (Similar to Tick Paralysis)
- Hypothyroidism (see Hypothyroidism)
- Mechanism: combination of decreased central respiratory drive, phrenic neuropathy, and respiratory muscle myopathy
- Clinical: manifests as both inspiratory and expiratory muscle weakness
- Idiopathic Peripheral Neuropathy
- Mediastinal/Esophageal Surgical Injury or Traumatic Injury of Bilateral Phrenic Nerves
- Epidemiology
- Phrenic Nerve Injury Occurs in 2-20% of Open Heart Surgery Cases
- L>R Sided Injury
- Mechanisms
- Cold Cardioplegia
- Dissection of Left Internal Mammary Artery (LIMA)
- Stretching of Phrenic Nerve
- Multiple Sclerosis (see Multiple Sclerosis)
- Neurofibromatosis (see Neurofibromatosis)
- Epidemiology: case report of bilateral diaphragmatic paralysis
- Systemic Lupus Erythematosus (SLE) (see Systemic Lupus Erythematosus)
- Physiology: neuropathy with vasculitis of phrenic nerves and myopathy
- Neuromuscular Junction Disease (Involving the Respiratory Muscles)
- Myasthenia Gravis (MG) (see Myasthenia Gravis)
- Clinical: acute ventilatory failure may be the initial presentation of myasthenia gravis
- Lambert-Eaton Myasthenic Syndrome (LEMS) (see Lambert-Eaton Myasthenic Syndrome)
- Botulism (see Botulism)
- Physiology: botulinum toxin blocks acetylcholine release at neuromuscular junction
- Clinical: descending paralysis (similar to paralytic-neurotoxic shellfish poisoning)
- Tick Paralysis (see Tick Paralysis)
- Physiology: toxin probably impairs acetylcholine mobilization at motor nerve terminal
- Clinical: ascending paralysis (Similar to Guillain-Barre Syndrome)
- Organophosphate/Carbamate Intoxication (see Organophosphates-Carbamates) (PLoS Med, 2008) [MEDLINE]
- Pharmacologic Neuromuscular Junction Antagonists
- Aminoglycosides (see Aminoglycosides): usually clinically relevant only in the presence of other neuromuscular junction disease
- Anticholinergic Agents (see Anticholinergic Agents): usually clinically relevant only in the presence of other neuromuscular disease
- Fluoroquinolones (see Fluoroquinolones): usually clinically relevant only in the presence of other neuromuscular disease
- Procainamide (see Procainamide): usually clinically relevant only in the presence of other neuromuscular disease
- Polymyxin B (see Polymyxins): usually clinically relevant only in the presence of other neuromuscular disease
- Sodium Colistimethate (aka Colistin, Polymyxin E) (see Polymyxins): usually clinically relevant only in the presence of other neuromuscular disease
- Myasthenia Gravis (MG) (see Myasthenia Gravis)
- Acute Myopathy/Muscle Dysfunction (Involving Respiratory Muscles) (see Myopathy
- Periodic Paralysis Syndromes
- Hyperkalemic Periodic Paralysis (see Hyperkalemic Periodic Paralysis)
- Hypokalemic Periodic Paralysis (see Hypokalemic Periodic Paralysis)
- Thyrotoxic Periodic Paralysis (see Thyrotoxic Periodic Paralysis)
- Rheumatologic
- Mixed Connective Tissue Disease (see Mixed Connective Tissue Disease)
- Polydermatomyositis (see Polydermatomyositis)
- Systemic Lupus Erythematosus (SLE) (see Systemic Lupus Erythematosus): neuropathy and myopathy
- Electrolyte-Related
- Hyperkalemia (see Hyperkalemia): may cause respiratory muscle weakness
- Hypomagnesemia (see Hypomagnesemia)
- Hypophosphatemia (see Hypophosphatemia)
- Other
- Bilateral Diaphragmatic Paralysis (see Bilateral Diaphragmatic Paralysis)
- Critical Illness Polymyopathy (see ICU-Acquired Weakness)
- Necrotizing Myopathy from Steroids and Neuromuscular Junction Antagonists
- Hyperthyroidism (see Hyperthyroidism)
- Clinical: proximal and distal myopathy with both inspiratory and expiratory muscle weakness
- Hypothyroidism (see Hypothyroidism)
- Mechanism: combination of decreased central respiratory drive, phrenic neuropathy, and respiratory muscle myopathy
- Clinical: manifests as both inspiratory and expiratory muscle weakness
- Periodic Paralysis Syndromes
Disorders with Decreased Ventilatory Output (Despite Increased Ventilatory Effort) Due to Excessive Ventilatory Demand
- Progressive Upper Airway Obstruction (with Increased Work of Breathing) (see Obstructive Lung Disease)
- Bilateral Vocal Fold Immobility (BVFI) (see Bilateral Vocal Fold Immobility)
- Cricoarytenoid Arthritis (see Cricoarytenoid Arthritis)
- Laryngeal Inflammation
- Neurologic Disease/Dysfunction Involving the Vocal Folds (Vocal Cord Paralysis)
- Developmental Abnormality or Neoplasm the Involving Vocal Folds
- Intubation Injury to Vocal Folds
- Mechanical/Iatrogenic Injury to Vocal Folds
- Surgical Injury to Vocal Folds
- Other Upper Airway Disease (see Obstructive Lung Disease)
- Infection
- Coccidioidomycosis (see Coccidioidomycosis): typically mild upper airway obstruction
- Cryptococcosis (see Cryptococcosis): typically mild upper airway obstruction
- Histoplasmosis (see Histoplasmosis): typically mild upper airway obstruction
- Syphilis (see Syphilis)
- Neurologic
- Essential Tremor (see Essential Tremor): typically mild upper airway obstruction
- Parkinson’s Disease (see Parkinson’s Disease): may cause acute upper airway obstruction in the postoperative setting or progressive upper airway dysfunction
- Miscellaneous
- Congenital Small Cricoid Cartilage: typically progressive
- Esophageal Foreign Body: extrinsic compression of upper airway, typically progressive
- Langerhans Cell Histiocytosis (see Langerhans Cell Histiocytosis): typically mild upper airway obstruction
- Laryngeal Cyst/Laryngocele: typically mild upper airway obstruction
- Laryngeal Rheumatoid Nodule (see Rheumatoid Arthritis): typically progressive
- Macroglossia: typically mild upper airway obstruction
- Nasal Polyps (see Nasal Polyps): typically mild upper airway obstruction
- Obstructive Sleep Apnea (OSA) (see Obstructive Sleep Apnea): may cause acute upper airway obstruction in the postoperative setting
- Thermal Injury/Burns of Upper Airway (see Smoke Inhalation): thermal injury is usually supraglottic (typically, laryngeal injury) and may be acute
- Thyromegaly/Goiter (see Goiter): typically progressive
- Tracheal Cyst: typically progressive
- Tracheobronchomalacia (see Tracheobronchomalacia): typically progressive
- Tonsillar/Adenoid Enlargement: typically progressive
- Unilateral Vocal Cord Paralysis (see Unilateral Vocal Fold Immobility): typically mild upper airway obstruction
- Infection
- Bilateral Vocal Fold Immobility (BVFI) (see Bilateral Vocal Fold Immobility)
- Obstructive Lung Disease (with Increased Work of Breathing) (see Obstructive Lung Disease)
- Bronchiectasis (see Bronchiectasis)
- Chronic Obstructive Pulmonary Disease (COPD) (see Chronic Obstructive Pulmonary Disease)
- Chronic Tracheobronchial Obstruction
- Tracheobronchial Infection
- Tracheobronchial Neoplasm
- Extrinsic Tracheobronchial Compression
- Other Tracheobronchial Obstructive Process
- Cystic Fibrosis (CF) (see Cystic Fibrosis)
- Increased Dead Space Ventilation (Increased VD/VT Ratio)
- End-Stage Interstitial Lung Disease (ILD) (see Interstitial Lung Disease)
- Mechanism
- Due to Increased Physiologic Dead Space
- Mechanism
- End-Stage Interstitial Lung Disease (ILD) (see Interstitial Lung Disease)
- Parenchymal Lung Disease (with Increased Work of Breathing)
- Any Etiology of Pulmonary Fibrosis
- Progressive Massive Fibrosis (PMF) (see Progressive Massive Fibrosis)
- Recurrent Diffuse Alveolar Hemorrhage (DAH) (see Diffuse Alveolar Hemorrhage)
- Idiopathic Pulmonary Fibrosis (IPF) (see Idiopathic Pulmonary Fibrosis)
- Acute Ventilatory Failure May Be Manifested as the End-Stage of IPF or More Commonly, in Conjunction with Pneumonia, Surgery, or Other Illness
- In End-Stage IPF Requiring Mechanical Ventilation, Lung Compliance Has Been Noted to Be Significantly Decreased
- Any Etiology of Pulmonary Fibrosis
- Pleural or Chest Wall Disease (with Increased Work of Breathing)
- Ankylosing Spondylitis (see Ankylosing Spondylitis)
- Fibrothorax (see Fibrothorax)
- Flail Chest (see Flail Chest)
- Kyphoscoliosis (see Kyphoscoliosis)
- Large Pleural Effusion (see Pleural Effusion-Transudate and Pleural Effusion-Exudate)
- Obesity Hypoventilation Syndrome (OHS) (see Obesity Hypoventilation Syndrome)
- Mechanism: combination of chest wall restriction and decreased central respiratory drive
- Pectus Excavatum (see Pectus Excavatum)
- Post-Thoracoplasty (see Thoracoplasty)
- Severe Abdominal Distention
Etiology of Respiratory Failure in Pregnancy (see Pregnancy)

References
General
- The continuous inhalation of oxygen in cases of pneumonia otherwise fatal, and in other diseases. Boston Med J 1890;123:481-5
- Clinical semi-starvation: depression of hypoxic ventilatory response. N Engl J Med. 1976;295(7):358 [MEDLINE]
- Clinical manifestations of inspiratory muscle fatigue. Am J Med. 1982 Sep;73(3):308-16 [MEDLINE]
- The spectrum of intermediate syndrome following acute organophosphate poisoning: a prospective cohort study from Sri Lanka. PLoS Med. 2008 Jul 15;5(7):e147. doi: 10.1371/journal.pmed.0050147 [MEDLINE]
- Short-term and long-term effects of nasal intermittent positive pressure ventilation in patients with obesity-hypoventilation syndrome. Chest. 2005 Aug;128(2):587-94 [MEDLINE]
- Noninvasive ventilation reduces intubation in chest trauma-related hypoxemia: a randomized clinical trial. Chest. 2010 Jan;137(1):74-80. doi: 10.1378/chest.09-1114. Epub 2009 Sep 11 [MEDLINE]
- High-flow oxygen administration by nasal cannula for adult and perinatal patients. Respir Care 2013;58:98-122
- Nasal high-flow versus Venturi mask oxygen therapy after extubation: effects on oxygenation, comfort, and clinical outcome. Am J Respir Crit Care Med 2014;190:282-8
- Transnasal humidified rapid-insufflation ventilatory exchange (THRIVE): a physiological method of increasing apnoea time in patients with difficult airways. Anaesthesia 2015;70:323-9 [MEDLINE]
- FLORALI Study. High-flow oxygen through nasal cannula in acute hypoxemic respiratory failure. N Engl J Med 2015. DOI: 10.1056/NEJMoa1503326 [MEDLINE]
- Saving lives with high-flow nasal oxygen. N Engl J Med. 2015 Jun 4;372(23):2225-6. doi: 10.1056/NEJMe1504852 [MEDLINE]
- High-flow nasal cannula oxygen therapy in adults. J Intensive Care. 2015 Mar 31;3(1):15. doi: 10.1186/s40560-015-0084-5. eCollection 2015 [MEDLINE]
- Comorbidities and Subgroups of Patients Surviving Severe Acute Hypercapnic Respiratory Failure in the Intensive Care Unit. Am J Respir Crit Care Med. 2017;196(2):200 [MEDLINE]
Etiology
- Acute Respiratory Failure in Pregnancy. Crit Care Clin. 2024 Apr;40(2):353-366. doi: 10.1016/j.ccc.2024.01.005 [MEDLINE]