

Definitions

Respiratory Failure (see Respiratory Failure)
- Definition
- Respiratory Failure is Defined as the Occurrence of One or Both of the Following
- Decreased pO2, as Predicted for the Patient’s Age (Hypoxemia)
- Increased pCO2 (Hypercapnia) in the Setting of a Normal Serum Bicarbonate
- A Normal Serum Bicarbonate is Specified Here Since a Primary Metabolic Alkalosis (with Increased Serum Bicarbonate) Would Be Expected to Result in a Normal Compensatory Increase in pCO2: this normal compensatory mechanism functions to maintain a normal serum pH and would not be considered “respiratory failure”
- Respiratory Failure is Defined as the Occurrence of One or Both of the Following
Hypoxemia (see Hypoxemia)
- Definition
- Hypoxemia is Defined a Decrease in Hemoglobin Oxygen Saturation (as Assessed by Pulse Oximetry: SaO2 or SpO2) or Decrease in Arterial pO2 (as Assessed by Arterial Blood Gas)
- Note that a Patient May Be Hypoxemic, But Not Be Hypoxic
- Example
- A Young Hypoxemic Patient Can Significantly Increase Their Cardiac Output to Maintain Tissue Oxygen Delivery
- Example
Hypoxia (see Hypoxemia)
- Definition
- Hypoxia is Defined as a State of Impaired Tissue Oxygenation
- Note that a Patient May Be Hypoxic, But Not Be Hypoxemic
- Example
- In Cyanide Intoxication, SaO2 Can Be Normal, But Tissues May Be Hypoxic (see Cyanide)
- Example
Anoxia
- Definition
- Anoxia is Defined as Complete Tissue Deprivation of Oxygen Supply
Hypercapnia (see Hypercapnia)
- Definition
- Hypercapnia is Defined as Increase in Arterial pCO2 (i.e. Increased Arterial Blood Partial Pressure of Carbon Dioxide) to >40 mm Hg
Acidemia
- Definition
- Acidemia is Defined as Decrease in Arterial pH < 7.40 (Due to Either Metabolic or Respiratory Acidosis)
- Note that a Patient Can Be Acidemic without having a Respiratory Acidosis
- Example
- Metabolic Acidosis Can Produce Acidemia without the Presence of a Respiratory Acidosis
- Example
Alkalemia
- Definition
- Alkalemia is Defined an Increase in Arterial pH to >7.40 (Due to Either Metabolic or Respiratory Alkalosis)
Acidosis
- Definition
- Acidosis is Defined as the Presence of an Acid-Producing Acid-Base Disturbance (with or without Concomitant Acidemia)
- Clinical Scenarios in Which an Acidosis is Present, But in Which the pH is Not Acidemic
- Presence of a Metabolic Acidosis May Not Necessarily Result in an Acidemic pH (pH <7.4), Since Respiratory Compensation (Hyperventilation) Occurs, Resulting in an Increase in the Serum pH
- Presence of a (Chronic) Respiratory Acidosis May Not Necessarily Result in an Acidemic pH (pH <7.4), Since Metabolic Compensation (Renal Bicarbonate Retention) Generally Occurs Over a Period of Days, Resulting in an Increase in the Serum pH
Alkalosis
- Definition
- Alkalosis is Defined as the Presence of an Alkali-Producing Acid-Base Disturbance (with or without Concomitant Alkalemia)
- Clinical Scenarios in Which an Alkalosis is Present, But in Which the pH is Not Alkalemic
- Presence of a Metabolic Alkalosis May Not Necessarily Result in an Alkelemic pH (pH >7.4), Since Respiratory Compensation (Hypoventilation) Occurs Rapidly, Resulting in a Decrease in the Serum pH
- Presence of a (Chronic) Respiratory Alkalosis May Not Necessarily Result in an Alkalemic pH (pH >7.4), Since Metabolic Compensation (Renal Bicarbonate Wasting) Generally Occurs Over a Period of Days, Resulting in a Decrease in the Serum pH
Respiratory Acidosis (see Respiratory Acidosis)
- Definition
- Respiratory Acidosis is Defined as a Disorder Which Results in Increase in Arterial pCO2 with an Associated Decrease in Arterial pH
- Note that a Patient Can Have a Respiratory Acidosis without Being Significantly Acidemic
- Example
- Via Normal Compensatory Mechanisms, Chronic Respiratory Acidosis Induces Metabolic (Predominantly Renal) Compensation (with a Increase in Serum Bicarbonate Over Time), Culminating in Minimal Acidemia
- Example
Terms
- PaO2: arterial pO2 (arterial oxygen tension)
- Usually Referred to Simply as pO2
- PAO2: alveolar PO2 (alveolar oxygen tension)
- SpO2: pulse oximetry, as determined by peripheral pulse oximeter (see Pulse Oximetry)
- SaO2: pulse oximetry, as determined by arterial blood gas co-oximeter (see Arterial Blood Gas)

Etiology of Hypercapnia/Respiratory Acidosis (see Hypercapnia)
- See Hypercapnia (see Hypercapnia)
Physiology
Normal Acid-Base Physiology
Normal Compensatory Responses to Respiratory Acidosis
Initial Acute Response to Respiratory Acidosis (Which is Relatively Modest) is Generated by a Variety of pH Buffering Molecules Present in All of the Body Fluid Compartments (i.e. Total Body Buffering)
- Reactions with These Molecules Cause the Serum Bicarbonate to Increase within Minutes
Chronic Compensation for Respiratory Acidosis (Which is Comparatively Larger) is Mediated Via the Kidney
- Renal Compensatory Response Begins Soon After the Onset of Respiratory Acidosis, But Requires 3-5 Days to Complete
- Kidney Increases Acid Excretion in the Form of Titratable Acid and Ammonium Ion, Which Generates Additional Bicarbonate
- Renal Tubular Bicarbonate Reabsorption is Also Increased, Which Maintains a Higher Serum Bicarbonate Concentration
- The Normal Compensatory Response to Chronic Respiratory Acidosis is that for Each 10 mm Hg Increase in pCO2, the Serum Bicarbonate Concentration Increases by about 3.5-5.0 mEq/L
- This Eventually Results in a Serum pH Which is Slightly Acidemic (Since Compensation is Incomplete and Corrects the pH Back Toward a Normal pH, But Not Completely Back to a Normal pH)
- Note that Since Renal Compensation is Tightly Regulated, Administering Exogenous Bicarbonate in the Setting of Chronic Respiratory Acidosis and Relatively Normal Renal Function Results in Urinary Excretion of the Excess Alkali without a Further Increase in the Serum Bicarbonate Concentration
Diagnosis
Arterial Blood Gas (ABG) (see Arterial Blood Gas)
- Required for the Diagnosis of Hypercapnia/Respiratory Acidosis (see Hypercapnia)
Clinical Manifestations of Hypercapnia/Respiratory Acidosis (see Hypercapnia)
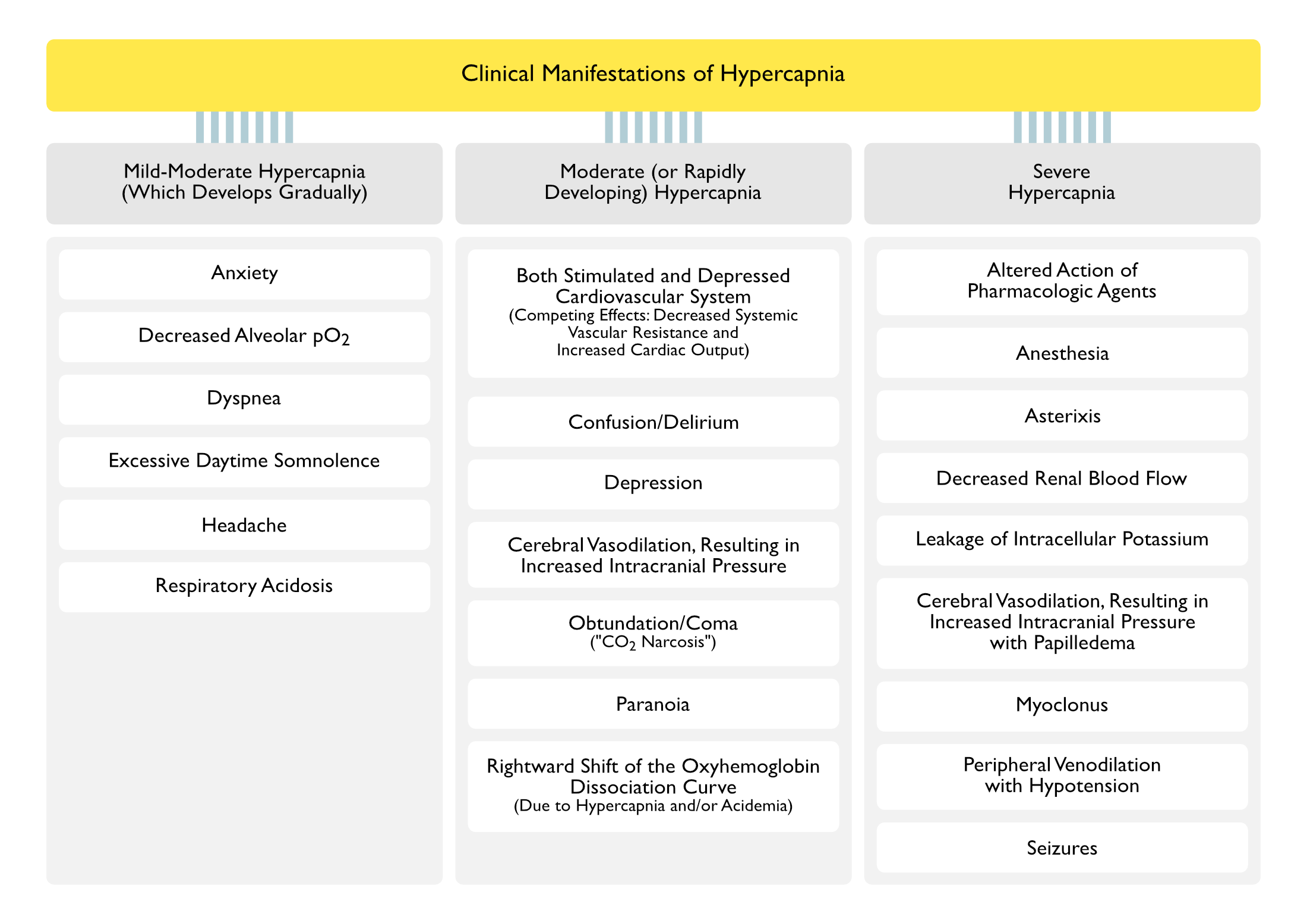
Cardiopulmonary Manifestations
- Acid-Base and Gas Exchange Abnormalities
- Decreased Alveolar pO2 (see Hypoxemia)
- Respiratory Acidosis (see Respiratory Acidosis)
- Arrhythmias
- Decreased Diaphragmatic Contractility
- May Result in Respiratory Failure (see Respiratory Failure)
- Decreased Myocardial Contractility
- May Result in Congestive Heart Failure (CHF) (see Congestive Heart Failure)
- Decreased Renal Blood Flow
- May Occur with pCO2 >150 mm Hg
- Dyspnea (see Dyspnea)
- Mechanisms
- Hypercapnia-Associated Decreased Diaphragmatic Contractility
- May Result in Respiratory Failure (see Respiratory Failure)
- Hypercapnia-Associated Decreased Myocardial Contractility
- May Result in Congestive Heart Failure (CHF) (see Congestive Heart Failure)
- Hypercapnia-Associated Acidemia, Resulting in Stimulation of Central and Peripheral Chemoreceptors
- Hypercapnia-Induced Increase in Respiratory Drive (Early), Then Decreased Respiratory Drive (Later)
- Hypercapnia-Associated Decreased Diaphragmatic Contractility
- Mechanisms
- Early Increased Respiratory Drive, Later Decreased Respiratory Drive
- Leakage of Intracellular Potassium
- May Occur with pCO2 >150 mm Hg
- Peripheral Venodilation with Hypotension (see Hypotension)
- May Occur with Severe Hypercapnia
- Rightward Shift of the Oxyhemoglobin Dissociation Curve (Due to Hypercapnia and/or Acidemia)
- Decreased Hemoglobin Affinity for Oxygen in the Lungs (with Decreased Oxygen Loading) and Increased Oxygen Unloading at the Tissues (Bohr Effect)
Neurologic Manifestations
- Altered Mental Status (see Altered Mental Status)
- Confusion (see Confusion)
- May Occur with Moderate (or Rapidly Developing) Hypercapnia
- Delirium (see Delirium)
- May Occur with Moderate (or Rapidly Developing) Hypercapnia
- Obtundation/Coma (“CO2 Narcosis”) (see Obtundation/Coma)
- Acute Hypercapnia Initially Increases the Respiratory Drive (with Associated Hyperventilation) (Anesthesiology, 1960) [MEDLINE] (NEJM, 1984) [MEDLINE]
- Later, Acute Hypercapnia Decreases the Respiratory Drive, Leading to Worsening Hypercapnia with Depressed Mental Status (“CO2 Narcosis”)
- Normal (Normocapnic) Patients Generally Do Not Develop Altered Mental Status Until the pCO2 Exceeds 75-80 mm Hg
- Chronically Hypercapnic Patients Generally Do Not Develop Altered Mental Status Until the pCO2 Exceeds 90-100 mm Hg
- These Later Effects are Mediated Via Increased Brain Glutamine, Increased Brain γ-Aminobutyric Acid (GABA), Decreased Brain Glutamate, and Decreased Brain Aspartate
- Confusion (see Confusion)
- Anesthesia (see Anesthesia)
- May Occur with pCO2 >200 mm Hg
- Anxiety (see Anxiety)
- May Occur with Mild-Moderate Hypercapnia (Which Develops Gradually
- Asterixis (see Asterixis)
- May Occur with Severe Hypercapnia
- Depression (see Depression)
- May Occur with Moderate (or Rapidly Developing) Hypercapnia
- Excessive Daytime Somnolence (see Excessive Daytime Somnolence)
- May Occur with Mild-Moderate Hypercapnia (Which Develops Gradually
- Headache (see Headache)
- May Occur with Mild-Moderate Hypercapnia (Which Develops Gradually
- Increased Intracranial Pressure (ICP) (see Increased Intracranial Pressure) (Anesthesiology, 1960) [MEDLINE] (NEJM, 1984) [MEDLINE]
- Hypercapnia Causes Cerebral Vasodilation with Increased Cerebral Blood Flow
- The Increased Cerebral Blood Flow May Undesirably Potentiate Neurologic Injury in Traumatic Brain injury (TBI), etc (see Traumatic Brain injury)
- Papilledema May Occur with Severe Hypercapnia (see Papilledema)
- Hypercapnia Causes Cerebral Vasodilation with Increased Cerebral Blood Flow
- Myoclonus (see Myoclonus)
- May Occur with Severe Hypercapnia
- Paranoia (see Paranoia)
- May Occur with Moderate (or Rapidly Developing) Hypercapnia
- Seizures (see Seizures)
- May Occur with Severe Hypercapnia
Manifestations Due to the Acidosis Itself
- Altered Action of Pharmacologic Agents
- Intracellular Acidosis Potentiates the Effect of Neuromuscular Junction Antagonists (Cisatracurium, Rocuronium, etc) (see Neuromuscular Junction Antagonists)
- Cardiovascular Instability/Cardiac Arrest (see Cardiac Arrest)
- Central Nervous System Depression
- Decreased Calcium Binding to Albumin (with Increase Serum Ionized Calcium Levels) (see Hypercalcemia)
- Hyperkalemia Due to Extracellular Shift of Potassium (see Hyperkalemia)
- Hypotension/Pulseless Electrical Activity (PEA) (see Hypotension and Pulseless Electrical Activity)
- Due to Decreased Systemic Vascular Resistance (SVR)
Treatment
Noninvasive Positive-Pressure Ventilation (NIPPV) (see Noninvasive Positive-Pressure Ventilation)
- See Noninvasive Positive-Pressure Ventilation
Invasive Mechanical Ventilation (see Invasive Mechanical Ventilation-General)
- See Invasive Mechanical Ventilation-General
References
General
- Effects of carbon dioxide on the cardiovascular system. Anesthesiology. 1960;21:652 [MEDLINE]
Etiology
- Causes of and compensations for hypoxemia and hypercapnia. Compr Physiol. 2011 Jul;1(3):1541-53. doi: 10.1002/cphy.c091007 [MEDLINE]
- Oxygen-induced hypercapnia in COPD: myths and facts. Crit Care. 2012 Oct 29;16(5):323. doi: 10.1186/cc11475 [MEDLINE]
- Effects of hypercapnia on the lung. J Physiol. 2017 Apr 15;595(8):2431-2437. doi: 10.1113/JP273781 [MEDLINE]