

Definition
- Pulmonary Infiltrates + Peripheral Eosinophilia (see Peripheral Eosinophilia)
Etiology
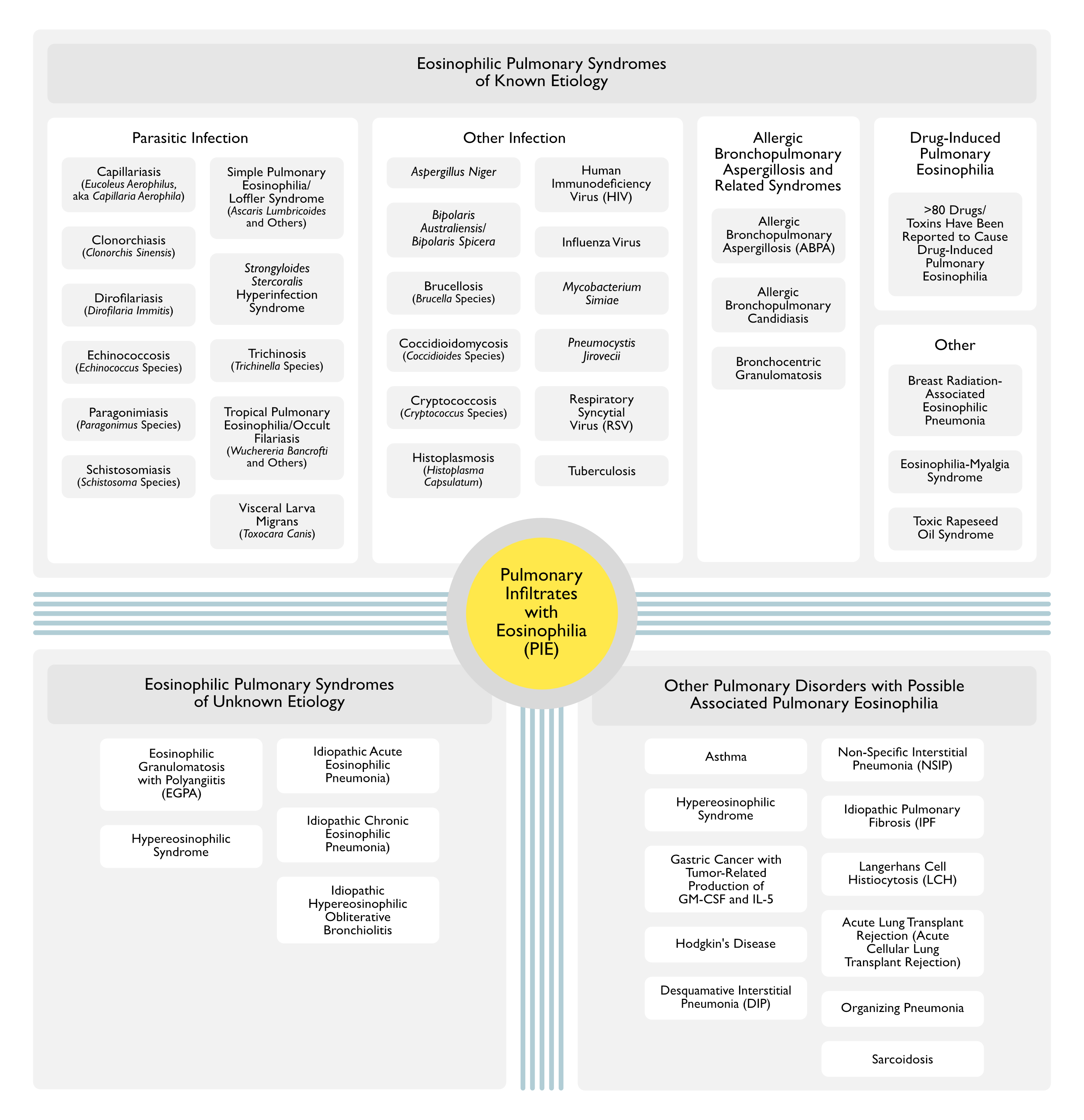
Eosinophilic Pulmonary Syndromes of Known Etiology
Parasitic Infection
- General Comments
- Parasite-Associated Eosinophilic Pneumonias Represent the Most Common Etiologies of Pulmonary Infiltrates with Eosinophilia Worldwide
- Capillaria Aerophila (see Capillariasis)
- Epidemiology
- Rare Etiology of Eosinophilic Pulmonary Infiltrates
- Epidemiology
- Clonorchis Sinensis (see Clonorchiasis)
- Epidemiology
- Rare Etiology of Eosinophilic Pulmonary Infiltrates
- Epidemiology
- Dirofilariasis (see Dirofilariasis)
- Clinical
- Eosinophilic Pulmonary Infiltrates
- Clinical
- Echinococcosis (see Echinococcosis)
- Paragonimiasis (see Paragonimiasis)
- Epidemiology
- Rare Etiology of Eosinophilic Pulmonary Infiltrates
- Epidemiology
- Schistosomiasis (see Schistosomiasis)
- Manifestations of Schistosomiasis in the Lung Vary Dependent on the Stage of Disease
- Early Acute Schistosomiasis: transient, multiple small pulmonary nodules with peripheral eosinophilia
- Chronic Schistosomiasis: embolization of ova in small arteries of the lung results in granuloma formation, occlusion and remodeling of pulmonary arteries, and further pulmonary hypertension mediared by portopulmonary hypertension
- Post-Treatment of Schistosomiasis: eosinophilic pneumonitis (lung shift, verminous pneumonia, reactionary Loffler-like pneumonitis) due to antigen release following treatment
- Manifestations of Schistosomiasis in the Lung Vary Dependent on the Stage of Disease
- Simple Pulmonary Eosinophilia (Loffler Syndrome) (see Simple Pulmonary Eosinophilia)
- Ascaris Lumbricoides (or Ascaris Suum): most common etiology of simple pulmonary eosinophilia (Loffler syndrome)
- Necator Americanus
- Ancylostoma Duodenale
- Ancylostoma Brazliense or Canium
- Entamoeba Histolytica
- Fasciola Hepatica
- Schistosomiasis (see Schistosomiasis)
- Manifestations of Schistosomiasis in the Lung Vary Dependent on the Stage of Disease
- Early Acute Schistosomiasis: transient, multiple small pulmonary nodules with peripheral eosinophilia
- Chronic Schistosomiasis: embolization of ova in small arteries of the lung results in granuloma formation, occlusion and remodeling of pulmonary arteries, and further pulmonary hypertension mediared by portopulmonary hypertension
- Post-Treatment of Schistosomiasis: eosinophilic pneumonitis (lung shift, verminous pneumonia, reactionary Loffler-like pneumonitis) due to antigen release following treatment
- Manifestations of Schistosomiasis in the Lung Vary Dependent on the Stage of Disease
- Strongyloides Stercoralis: simple pulmonary eosinophilia (Loffler syndrome) may occur when larvae migrate through the lungs after acute infection
- Strongyloides Stercoralis Hyperinfection Syndrome (see Strongyloides Stercoralis)
- Epidemiology
- Occurs in 20% of Patients Hospitalized with Strongyloidiasis and Coexisting Chronic Lung Disease (COPD, Asthma, etc)
- Diagnosis
- Rhabditiform Larvae May Be Recovered Via Bronchoalveolar Lavage, Bronchial Wash, or Sputum Sample
- Clinical
- Epidemiology
- Trichinosis (see Trichinosis)
- Epidemiology
- Rare Etiology of Eosinophilic Pulmonary Infiltrates
- Epidemiology
- Tropical Pulmonary Eosinophilia (Occult Filariasis) (see Tropical Pulmonary Eosinophilia)
- Wuchereria Bancrofti
- Brugia Malayi
- Brugia Timori
- Visceral Larva Migrans (see Visceral Larva Migrans)
- Toxocara Canis
Other Infection
- Aspergillus Niger (see Aspergillus)
- Epidemiology
- Case Reports of Eosinophilic Pneumonia
- Epidemiology
- Bipolaris Australiensis
- Epidemiology
- Case Reports of Eosinophilic Pneumonia
- Epidemiology
- Bipolaris Spicera
- Epidemiology
- Case Reports of Eosinophilic Pneumonia
- Epidemiology
- Brucellosis (see Brucellosis)
- Epidemiology
- Case Reports of Eosinophilic Pneumonia [Eosinophilia and pneumonitis in chronic brucellosis: a report of two cases. Ann Intern Med. 1942;16:995-1001]
- Epidemiology
- Coccidioidomycosis (see Coccidioidomycosis)
- Clinical
- Pronounced Peripheral Eosinophilia May Be an Early Indicator of Dissemination
- Clinical
- Cryptococcosis (see Cryptococcosis)
- Epidemiology
- Case Reports of Eosinophilic Pneumonia (South Med J, 1995) [MEDLINE]
- Epidemiology
- Histoplasmosis (see Histoplasmosis)
- Human Immunodeficiency Virus (HIV) (see Human Immunodeficiency Virus)
- Influenza Virus (see Influenza Virus)
- Epidemiology
- May Produce Eosinophilic Pneumonia in Some Cases
- Epidemiology
- Mycobacterium Simiae (see Mycobacterium Simiae)
- Epidemiology
- Case Reports of Eosinophilic Pneumonia (NEJM, 1989) [MEDLINE]
- Epidemiology
- Pneumocystis Jirovecii (PJP) (see Pneumocystis Jirovecii)
- Epidemiology: BAL eosinophilia has been reported in HIV-associated cases
- Respiratory Syncytial Virus (RSV) (see Respiratory Syncytial Virus)
- Epidemiology
- May Produce Eosinophilic Pneumonia in Some Cases
- Epidemiology
- Tuberculosis (see Tuberculosis)
- Epidemiology
- May Produce Eosinophilic Pneumonia in Some Cases
- Epidemiology
Allergic Bronchopulmonary Aspergillosis and Related Syndromes
- Allergic Bronchopulmonary Aspergillosis (ABPA) (see Allergic Bronchopulmonary Aspergillosis)
- Allergic Bronchopulmonary Candidiasis (see Candida)
- Bronchocentric Granulomatosis (BCG) (see Bronchocentric Granulomatosis)
Drug-Induced Pulmonary Eosinophilia (see Drug-Induced Pulmonary Eosinophilia)
- More Than 80 Drugs/Toxins Have Been Reported to Cause Drug-Induced Pulmonary Eosinophilia
Other
- Breast Radiation-Associated Eosinophilic Pneumonia (see Radiation Therapy)
- Clinical
- Chronic Eosinophilic Pneumonia
- Clinical
- Eosinophilia-Myalgia Syndrome (see Eosinophilia-Myalgia Syndrome)
- Physiology
- Due to Contaminated L-Tryptophan (see L-Tryptophan)
- Physiology
- Toxic Rapeseed Oil Syndrome (see Contaminated Rapeseed Oil)
- Physiology
- Due to Contaminated Rapeseed Oil
- Physiology
Eosinophilic Pulmonary Syndromes of Unknown Etiology
- Eosinophilic Granulomatosis with Polyangiitis (EGPA, Churg-Strauss Syndrome) (see Eosinophilic Granulomatosis with Polyangiitis)
- Clinical
- Pneumonia-Like Presentation (with Fleeting Patchy Alveolar or Nodular Infiltrates) May Occur in 30% of Cases
- Clinical
- Hypereosinophilic Syndrome (see Hypereosinophilic Syndrome)
- Idiopathic Acute Eosinophilic Pneumonia (IAEP) (see Acute Eosinophilic Pneumonia)
- Idiopathic Chronic Eosinophilic Pneumonia (ICEP) (see Chronic Eosinophilic Pneumonia)
- Idiopathic Hypereosinophilic Obliterative Bronchiolitis (see Idiopathic Hypereosinophilic Obliterative Bronchiolitis)
Other Pulmonary Disorders with Possible Associated Pulmonary Eosinophilia
- Asthma (see Asthma)
- Eosinophilic Bronchitis (see Eosinophilic Bronchitis)
- Clinical
- Chronic Cough with Sputum Eosinophilia (About 40%)
- Normal Lung Function with Absence of Bronchial Hyperreactivity: although it may evolve over time into either fixed airflow obstruction without asthma or into true asthma
- Absence of Eosinophilic Pneumonia
- Clinical
- Gastric Cancer with Tumor-Related Production of GM-CSF and IL-5 (see Gastric Cancer)
- Epidemiology
- Case Report
- Epidemiology
- Hodgkin’s Disease (see Hodgkins Disease)
- Idiopathic Interstitial Pneumonias
- Desquamative Interstitial Pneumonia (DIP) (see Desquamative Interstitial Pneumonia)
- Mild BAL Eosinophilia May Occur in Some Cases
- Non-Specific Interstitial Pneumonia (NSIP) (see Non-Specific Interstitial Pneumonia)
- Mild BAL Eosinophilia May Occur in Some Cases
- Desquamative Interstitial Pneumonia (DIP) (see Desquamative Interstitial Pneumonia)
- Idiopathic Pulmonary Fibrosis (IPF) (see Idiopathic Pulmonary Fibrosis): mild BAL eosinophilia may occur in some cases
- Langerhans Cell Histiocytosis (LCH) (see Langerhans Cell Histiocytosis)
- Diagnosis
- Pulmonary Pathologic Lesions are Nodules (with Bronchiolocentric Stellate Shape) with Langerhans Cells and Variable Numbers of Eosinophils, Plasma Cells, and Lymphocytes
- Eosinophils are Usually Present in the Initial, Active Stage of the Disease: they contribute to the eosinophilic granuloma
- Eosinophils are Numerous in 25% of Cases: usually located at the periphery of the lesions
- Eosinophils are Rare or Absent at the Chronic Stage of the Disease
- Diagnosis
- Lung Transplant (see Lung Transplant)
- Acute Lung Transplant Rejection (Acute Cellular Lung Transplant Rejection) (see Acute Lung Transplant Rejection): peripheral eosinophilia may occur with/without pulmonary infiltrates (as acute rejection may be detected by surveillance bronchoscopy with transbronchial biopsy prior to the development of pulmonary infiltrates)
- Organizing Pneumonia (see Cryptogenic Organizing Pneumonia)
- Diagnosis
- Mild BAL Eosinophilia May Occur in Some Cases (Usually <20%)
- Diagnosis
- Sarcoidosis (see Sarcoidosis)
- Diagnosis
- Peripheral Eosinophilia (and Tissue Eosinophilia) May Be Present, But are Usually Mild
- Diagnosis
Diagnosis
Complete Blood Count (CBC) (see Complete Blood Count)
- Peripheral Eosinophilia (see Peripheral Eosinophilia)
- May Be Present in the Disorders Noted Above to a Variable Extent
- Definition of Peripheral Eosinophilia: absolute eosinophil count >500 eosinophils/μL
- Definition of Peripheral Hypereosinophilia: absolute eosinophil count >1500 eosinophils/μL on two examinations at least 1 mo apart and/or tissue hypereosinophilia
- Effect of Corticosteroids on Peripheral Eosinophilia: course of corticosteroids typically results in a decrease in peripheral eosinophilia
High-Resolution Chest CT (see High-Resolution Chest Computed Tomography)
- Useful to Differentiate the Diseases Above
Bronchoscopy (see Bronchoscopy)
Bronchoalveolar Lavage (BAL)
- Although Pathologic Examination of the Lung is the Gold Standard for Diagnosing Eosinophilic Pneumonia, BAL is a Widely-Accepted Noninvasive Surrogate of Lung Biopsy for Diagnosis in Patients with High-Resolution Features of Eosinophilic Pneumonia
- However, No Study Has Definitely Established a Correlation Between the Presence of BAL Eosinophilia and the Finding of Eosinophilic Pneumonia on Lung Pathology
- BAL Eosinophil Percentage in Various Disease States
- Normal: BAL eosinophil <1%
- BAL Eosinophilia 3-40% (and Especially Between 3-9%): may be found in various disorders
- BAL Eosinophilia >40%: found predominantly in patients with chronic eosinophilic pneumonia
- BAL Eosinophil Percentage Proposed Cut-Off Values
- Diagnosis of Idiopathic Acute Eosinophilic Pneumonia: BAL Eosinophilia >25%
- Diagnosis of Idiopathic Chronic Eosinophilic Pneumonia: BAL Eosinophilia >40%
Transbronchial Biopsy (TBB)
- xxx
Video-Assisted Thoracoscopic Surgery (VATS) with Lung Biopsy
- May Be Required in Unusual Cases
References
- Eosinophilia and pneumonitis in chronic brucellosis: a report of two cases. Ann Intern Med. 1942;16:995-1001
- Acute eosinophilic pneumonia as a reversible cause of noninfectious respiratory failure. N Engl J Med. 1989;321:569-574 [MEDLINE]
- Cryptococcal pneumonia simulating chronic eosinophilic pneumonia. South Med J. 1995;88:845-846 [MEDLINE]