Post-Intensive Care Syndrome (PICS): defined as the impairment of cognition, mental health, and physical function in a patient who has been cared for in an intensive care unit (Crit Care Med, 2012) [MEDLINE]
Post-Intensive Care Syndrome Constitutes New or Worsening Function in One or More of the Cognitive, Psychiatric, and Physical Domains After a Critical Illness
Definition Applies to Adult Patients Who Reside at Home, in Long-Term Acute Care (LTAC) Units, or Skilled Nursing Facilities (SNF)
Post-Intensive Care Syndrome Generally Excludes Patients Who Have Been Admitted with Traumatic Brain Injury (TBI) or Stroke
Post-Intensive Care Syndrome is Usually Identified in the Immediate Post-Critical Illness Period, But There is No Established Duration of Time After a Critical Illness Where Post-Intensive Care Syndrome Can or Cannot Occur
Post-Intensive Care Syndrome-Family (PICS-Family): defined as altered mental health of family member(s) of a patient who has been cared for in an intensive care unit (Crit Care Med, 2012) [MEDLINE]
Epidemiology
Scope of the Problem
In the United States, There are Approximately 5.7 Million Annual Intensive Care Unit Admissions
Approximately 4.8 Million of These Admissions Will Survive the Intensive Care Unit Stay (NEJM, 2000) [MEDLINE] (NEJM, 2001) [MEDLINE] (Crit Care Med, 2008) [MEDLINE] (Crit Care, 2013) [MEDLINE] (Am J Respir Crit Care Med, 2013) [MEDLINE] (NEJM, 2013) [MEDLINE]
Prevalence of Post-Intensive Care Syndrome (PICS)
At Last 50% of Intensive Care Unit Survivors Will Experience Some Component of Post-Intensive Care Unit Syndrome (Cognitive, Psychiatric, or Physical) (Crit Care, 2013) [MEDLINE] (Am J Respir Crit Care Med, 2013) [MEDLINE] (NEJM, 2013) [MEDLINE] (Lancet Respir Med, 2014) [MEDLINE] (Ann Am Thorac Soc, 2016) [MEDLINE] (Crit Care Med, 2018) [MEDLINE]
In an Observational Cohort Study of Survivors of Critical Illness Who Received Life Support in the Intensive Care Unit, Approximately 64% of Survivors Had Newly-Acquired Cognitive Impairment, Depression, and/or Disability in Activities of Daily Living (ADL’s) at Three Months (Ann Am Thorac Soc, 2016) [MEDLINE]
Approximately 56 % of Survivors Had Newly-Acquired Cognitive Impairment, Depression, and/or Disability in Activities of Daily Living (ADL’s) at 12 Months
In a Study Comparing 6-Month Outcomes of Survivors of COVID-19 vs Non-COVID-19 Critical Illness, at Six Months, New Disability was Identified in Approximately 33% of Survivors (Am J Respir Crit Care Med, 2022) [MEDLINE]
Incidence and Severity of Disability was Similar for Survivors of COVID-19-Related Critical Illness
Public Health Burden
In a Study of Intensive Care Survivors, Approximately 44% Required Visitation by Home Health Nurses (Crit Care, 2013) [MEDLINE]
A Negative Impact on Family Income was Reported by 33-50% of Intensive Care Survivors/Families of Intensive Care Survivors
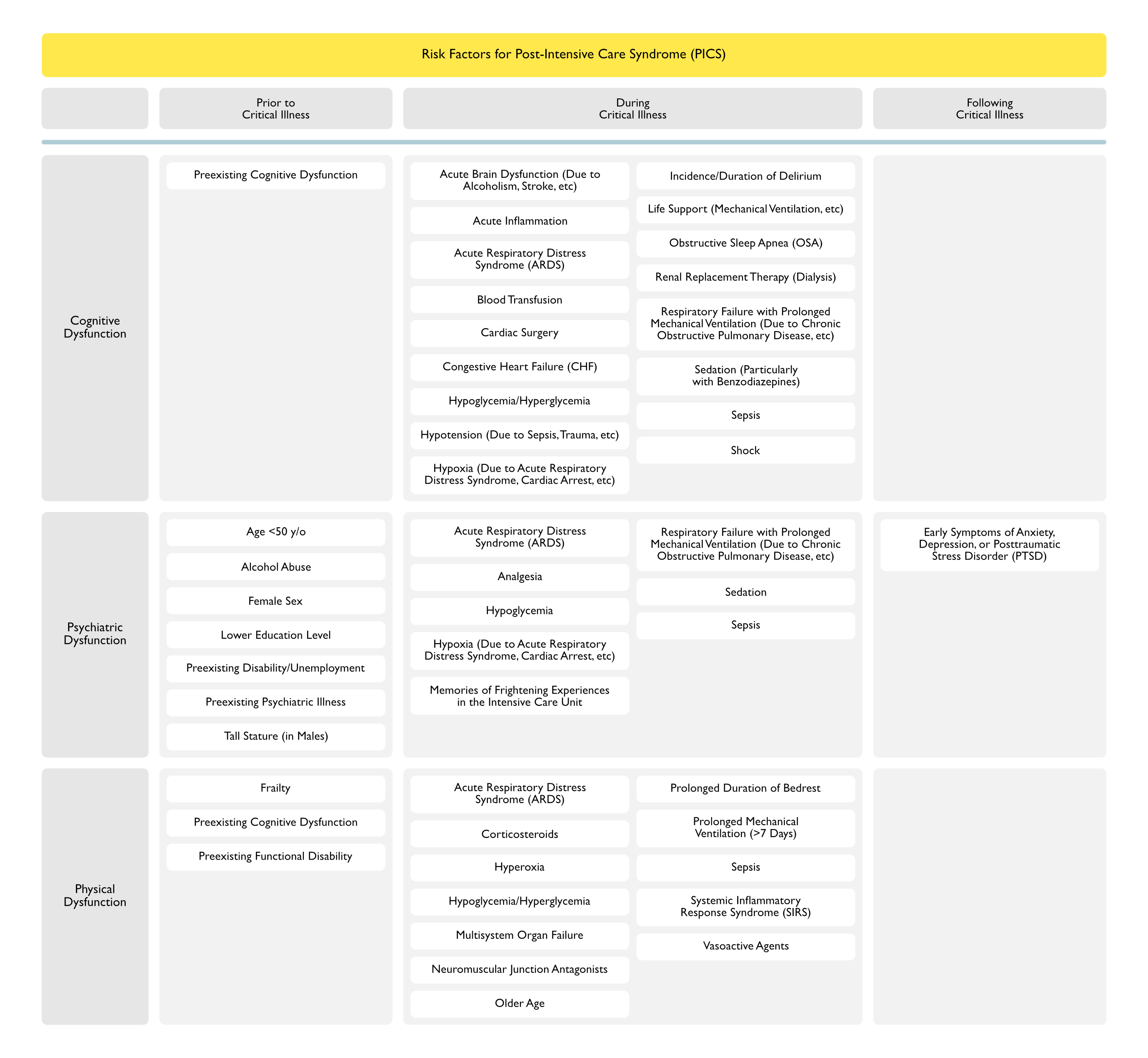
Risk Factors
Risk Factors for Cognitive Dysfunction (NEJM, 2013) [MEDLINE]
Risk Factors Prior to Critical Illness
Preexisting Cognitive Dysfunction
Poor Cognitive Reserve Prior to Critical Illness (Attributable to Older Age, Preexisting Cognitive Deficits, Premorbid Health Conditions, and/or the ApoE Genotype) is Associated with the Development of Cognitive Impairment (JAMA, 2011) [MEDLINE] (J Am Geriatr Soc, 2012) [MEDLINE] (Crit Care Med, 2012) [MEDLINE]
In Contrast, Attaining a Higher Level of Education (i.e. Having a Higher Level of Cognitive Reserve) is Associated with a Higher Probability of Being Free of Post-Intensive Care Syndrome at 3 and 12 Months (Crit Care Med, 2018) [MEDLINE]
Risk Factors During Critical Illness
Acute Brain Dysfunction (Due to Alcoholism, Stroke, etc)
Observational Studies of Acute Respiratory Distress Syndrome (ARDS) Survivors Indicate that Up to 73% Experience Moderate-Severe Cognitive Impairment Upon Discharge from the Intensive Care Unit (Am J Respir Crit Care Med, 1999) [MEDLINE] (Am J Respir Crit Care Med, 2005) [MEDLINE] (Am J Respir Crit Care Med, 2012) [MEDLINE]
Cognitive Dysfunction is Persistent at 1 Year (Present in 46-55% of Patients) and at 2 Years (Present in 47% of Patients)
BRAIN-ICU Study of Patients with Respiratory Failure or Shock in the Medical/Surgical Intensive Care Unit (NEJM, 2013) [MEDLINE]
Longer Duration of Delirium was Significantly Associated with Worse Global Cognition at 3 and 12 Months and Worse Executive Function at 3 and 12 Months
Use of Sedatives or Analgesics was Not Associated with Cognitive Impairment at 3 and 12 Months
In a Prospective Trial of Older Patients, as Compared with Survivors of Non-Sepsis Hospitalizations, Severe Sepsis Survivors were 3x More Likely to Develop Moderate-Severe Cognitive Impairment (Odds Ratio of 3.3; 95%: CI 1.5-7.3) (JAMA, 2010) [MEDLINE]
After Adjusting for Premorbid Cognitive Status, Sepsis Survivors Had a Higher Prevalence of Cognitive Dysfunction (16% vs 6%)
In a Study of Pneumonia and Cognitive Dysfunction, Small Subclinical Changes in Cognition Increased the Risk of Pneumonia (β = -0.02; P < 0.001) and Patients with Pneumonia were Subsequently at an Increased Risk of Dementia (Hazard Ratio of 2.24; 95% CI: 1.62-3.11]; P = 0.01) (Am J Respir Crit Care Med, 2013) [MEDLINE]
Glucocorticoids are Associated with a Decreased Risk for Posttraumatic Stress Disorder (PTSD) (Crit Care Med, 1999) [MEDLINE] (Biol Psychiatry, 2001) [MEDLINE] (Psychol Med, 2013) [MEDLINE]
Decreased Cortisol Levels May Play a Role in the Development of Posttraumatic Stress Disorder
Risk Factors for Physical Dysfunction
Intensive Care Unit (ICU)-Acquired Weakness (see Intensive Care Unit-Acquired Weakness) (NEJM, 2001) [MEDLINE] (JAMA, 2002) [MEDLINE] (NEJM, 2003) [MEDLINE] (Intensive Care Med, 2007) [MEDLINE] (Intensive Care Med, 2007) [MEDLINE] (Am J Respir Crit Care Med, 2007) [MEDLINE] (Chest, 2007) [MEDLINE] (JAMA, 2010) [MEDLINE] (NEJM, 2011) [MEDLINE] (Am J Respir Crit Care Med, 2012) [MEDLINE] (Crit Care Med, 2012) [MEDLINE] (J Am Geriatr Soc, 2012) [MEDLINE] (Crit Care Med, 2014) [MEDLINE] (Am J Respir Crit Care Med, 2014) [MEDLINE] (Am J Respir Crit Care Med, 2014) [MEDLINE] (Crit Care Med, 2014) [MEDLINE] (Intensive Care Med, 2015) [MEDLINE] (Crit Care Med, 2016) [MEDLINE] (Lancet Respir Med, 2017) [MEDLINE] (Chest, 2018) [MEDLINE]
Risk of Intensive Care Unit (ICU)-Acquired Weakness Appears to Be the Strongest for Neuromuscular Junction Antagonists When They are Used in the Setting of Sepsis
Systemic Inflammatory Response Syndrome (SIRS) (see Sepsis)
Vasoactive Agents
Physiology
XXXX
xxx
Diagnosis
XXXXX
xxx
Clinical Manifestations
General Comments
Post-Intensive Care Syndrome (PICS) is Considered to Be Distinct from (Post-Hospital Syndrome (Hospitalization-Associated Disability) (Ann Intern Med, 1993) [MEDLINE] (JAMA, 2011) [MEDLINE] (NEJM, 2013) [MEDLINE]
While Post-Hospital Syndrome (Especially in Older Patients) Can Be Associated with a Variety of Transient Functional Disabilities (Typically Lasting Days-Weeks), the Clinical Manifestations of Post-Intensive Care Syndrome (PICS) are More Wide-Ranging and are Typically Persistent
Cognitive Manifestations
General Comments
Cognitive Impairment Occurs in Approximately 25% of Intensive Care Unit Survivors (Chest, 2003) [MEDLINE] (Crit Care Med, 2003) [MEDLINE] (Intensive Care Med, 2004) [MEDLINE] (Anaesthesia, 2005) MEDLINE] (Chest, 2006) [MEDLINE] (Crit Care Med, 2010) [MEDLINE] (NEJM, 2012) [MEDLINE] (Am J Respir Crit Care Med, 2012) [MEDLINE] (Semin Respir Crit Care Med, 2012) [MEDLINE] (Ann Am Thorac Soc, 2013) [MEDLINE] (Am J Respir Crit Care Med, 2013) [MEDLINE]
Some Studies Report the Incidence of Cognitive Impairment in Intensive Care Unit Survivors to Be as High as 78%
BRAIN-ICU Study of Patients with Respiratory Failure or Shock in the Medical/Surgical Intensive Care Unit (NEJM, 2013) [MEDLINE]: n = 821
Delirium Developed in 74% of Cases During Hospital Stay
Outcomes At 3 Months
40% of Patients Had Impaired Global Cognition Scores that Were 1.5 Standard Deviations (SD) Below the Population Mean, Similar to Scores for Patients with Moderate Traumatic Brain Injury
26% of Patients Had Scores 2 Standard Deviations (SD) Below the Population Mean (Similar to Scores for Patients with Mild Alzheimer’s Disease)
Outcomes At 12 Months
Similar Persistent Cognitive Dysfunction Occurs as in Those with Moderate Traumatic Brain Injury
Similar Persistent Cognitive Dysfunction Occurs as in Those with Mild Alzheimer’s Disease
Impact of Duration of Delirium
Longer Duration of Delirium was Significantly Associated with Worse Global Cognition at 3 and 12 Months and Worse Executive Function at 3 and 12 Months
Impact of Sedative Use
Use of Sedatives or Analgesics was Not Associated with Cognitive Impairment at 3 and 12 Months
Cognitive Dysfunction was Also Independent of Age, Pre-Existing Cognitive Impairment, Presence or Severity of Coexisting Conditions, and Organ Failure During Intensive Care Unit Stay
Clinical Features
General Comments
Severity of Post-Intensive Care Cognitive Impairment Varies from Mild to Severe
Cognitive Impairment Can Range from Subtle Difficulties in Accomplishing Complex Executive Tasks to Profound Inability to Perform Activities of Daily Living (ADL’s)
Alteration in Attention
Alteration in Executive Function
Memory and Executive Function are the Most Commonly Affected Domains (Anaesthesia, 2005) [MEDLINE]
Dysfunctional Memory and/or Executive Function Frequently Impair Individuals from Engaging in Purposeful, Goal-Directed Behaviors Necessary for Effective Daily Functioning and Complex Cognition
Since These Functions are Also Critical to Effectively Carry Out a Discharge Plan, Inability to Perform the Functions Below Can Further Delay Recovery
Appointment Scheduling and Maintenance
Adherence to Dietary Restrictions
Medication Compliance
Alteration in Memory
Memory and Executive Function are the Most Commonly Affected Domains (Anaesthesia, 2005) [MEDLINE]
Dysfunctional Memory and/or Executive Function Frequently Impair Individuals from Engaging in Purposeful, Goal-Directed Behaviors Necessary for Effective Daily Functioning and Complex Cognition
Since These Functions are Also Critical to Effectively Carry Out a Discharge Plan, Inability to Perform the Functions Below Can Further Delay Recovery
Appointment Scheduling and Maintenance
Adherence to Dietary Restrictions
Medication Compliance
Alteration in Mental Processing Speed
Alteration in Visuo-Spatial Function
Communication Difficulties
Impaired Cognition Can Also Contribute to Communication Difficulties Frequently Observed in Patients Admitted to Rehabilitation Following a Critical Illness
Cognitive Impairment is Frequently Unrecognized Due to Patient Communication Difficulties and Because Screening and Formalized Testing are Not Routinely Performed (Crit Care Med, 2003) [MEDLINE] (Chest, 2003) [MEDLINE]
Long-Term Prognosis
While Cognitive Dysfunction May Improve Over the First 6-12 Months, Data from the BRAIN-ICU Study Suggests that Most Improvements are Small and Cognitive Impairment Persists for Years (NEJM, 2013) [MEDLINE]
In Addition, Impaired Cognition is Particularly Associated with Psychiatric Dysfunction, Decreased Quality of Life, and the Inability to Return to Work
Psychiatric Manifestations
General Comments
Psychiatric Illness is Common in Intensive Care Unit Survivors (Crit Care Med, 2011) [MEDLINE] (Am J Respir Crit Care Med, 2012) [MEDLINE] (Am J Respir Crit Care Med, 2012) [MEDLINE] (Chest, 2013) [MEDLINE] (JAMA, 2014) [MEDLINE] (Am J Respir Crit Care Med, 2016) [MEDLINE]
Risk of Psychiatric Illness Ranges from 1-62% (with the Highest Rates Generally Reported in Acute Respiratory Distress Syndrome Survivors)
In a National Database Registry Study of Acute Respiratory Distress Syndrome Survivors, 1% of Patients Had a New Psychiatrist-Diagnosed Psychological Disorder (Most Commonly Anxiety or Depression) (JAMA, 2014) [MEDLINE]
Approximately 19% of Patients Received ≥1 Prescriptions for Psychoactive Medications
Systematic Reviews of Observational Cohorts Reported Higher Rates of Psychiatric Illness in Intensive Care Unit Survivors (Psychiatry, 2008) [MEDLINE] (Intensive Care Med, 2009) [MEDLINE] (Am J Respir Crit Care Med, 2016) [MEDLINE]
Incidence of Depression Symptoms was 28%
Incidence of Posttraumatic Stress Disorder Symptoms was 22%
Longitudinal Cohort Study of Depression, Posttraumatic Stress Disorder, and Functional Disability in Intensive Care Survivors from the BRAIN-ICU Study (Lancet Respir Med, 2014) [MEDLINE]: n = 821
At 3 Months
Approximately 37% of Patients Reported at Least Mild Depression (Depression was Mainly Due to Somatic Symptoms, Rather than Cognitive-Affective Symptoms)
Depressive Symptoms were Common Even in Patients without a History of Depression (Occurred in 30% of These Patients at 3 Months)
Approximately 7% of Patients Reported Posttraumatic Stress Disorder at 3 Months
Approximately 32% of Patients were Disabled in Their Activities of Daily Living (ADL’s)
Approximately 26% of Patients were Disabled in Their Instrumental Activities of Daily Living (IADL’s)
After Adjusting for Covariates, Younger Age was Associated with a Probability of Worse Posttraumatic Stress Disorder
At 12 Months
Approximately 33% of Patients Reported at Least Mild Depression (Depression was Mainly Due to Somatic Symptoms, Rather than Cognitive-Affective Symptoms)
Depressive Symptoms were Common Even in Patients without a History of Depression (Occurred in 29% of These Patients at 12 Months)
Approximately 7% of Patients Reported Posttraumatic Stress Disorder at 12 Months
Approximately 27% of Patients were Disabled in Their Activities of Daily Living (ADL’s)
Approximately 23% of Patients were Disabled in Their Instrumental Activities of Daily Living (IADL’s)
After Adjusting for Covariates, Younger Age was Associated with a Probability of Worse Posttraumatic Stress Disorder
In an Observational Study, the Incidence of Posttraumatic Stress Disorder in Intensive Care Unit Survivors was 10% at Both 3 and 12 Months Post-Hospitalization (Am J Respir Crit Care Med, 2016) [MEDLINE]
Clinical Features
General Comments
Psychiatric Morbidity After Critical Illness is Often Disabling and is Associated with Decreased Quality of Life for Both the Patient and Their Family
Intensive Care Unit-Acquired Weakness is the Most Common Type of Physical Impairment in Intensive Care Survivors (JAMA, 2002) [MEDLINE] (NEJM, 2013) [MEDLINE] (Lancet Respir Med, 2014) [MEDLINE] (Crit Care Med, 2014) [MEDLINE] (Am J Respir Crit Care Med, 2014) [MEDLINE]
Intensive Care Unit (ICU)-Acquired Weakness Occurs in ≥25% of Patients
One Multicenter Study Reported that 64% of Intensive Care Survivors Had Mobility Problems at 6 Months (Crit Care, 2013) [MEDLINE]
Approximately 73% of Intensive Care Survivors Had Moderate or Severe Pain at 12 Months
Approximately 26% of Intensive Care Survivors Had Care Needs >50 hrs Per Week (80% of Which was Provided by Family Members)
Longitudinal Cohort Study of Depression, Posttraumatic Stress Disorder, and Functional Disability in Intensive Care Survivors from the BRAIN-ICU Study (Lancet Respir Med, 2014) [MEDLINE]: n = 821
At 3 Months
Approximately 37% of Patients Reported at Least Mild Depression (Depression was Mainly Due to Somatic Symptoms, Rather than Cognitive-Affective Symptoms)
Depressive Symptoms were Common Even in Patients without a History of Depression (Occurred in 30% of These Patients at 3 Months)
Approximately 7% of Patients Reported Posttraumatic Stress Disorder at 3 Months
Approximately 32% of Patients were Disabled in Their Activities of Daily Living (ADL’s)
Approximately 26% of Patients were Disabled in Their Instrumental Activities of Daily Living (IADL’s)
After Adjusting for Covariates, Younger Age was Associated with a Probability of Worse Posttraumatic Stress Disorder
At 12 Months
Approximately 33% of Patients Reported at Least Mild Depression (Depression was Mainly Due to Somatic Symptoms, Rather than Cognitive-Affective Symptoms)
Depressive Symptoms were Common Even in Patients without a History of Depression (Occurred in 29% of These Patients at 12 Months)
Approximately 7% of Patients Reported Posttraumatic Stress Disorder at 12 Months
Approximately 27% of Patients were Disabled in Their Activities of Daily Living (ADL’s)
Approximately 23% of Patients were Disabled in Their Instrumental Activities of Daily Living (IADL’s)
After Adjusting for Covariates, Younger Age was Associated with a Probability of Worse Posttraumatic Stress Disorder
In Acute Respiratory Distress Syndrome (ARDS) Survivors, Lung Function May Be Compromised for as Long as 5 Years (Am J Respir Crit Care Med, 2003) [MEDLINE] (NEJM, 2003) [MEDLINE] (NEJM, 2011) [MEDLINE]
The Most Common Deficit is Decreased Diffusion Capacity for Carbon Monoxide (DLCO)
Other Deficits Include Spirometric Defects and Restriction
In Most Acute Respiratory Distress Syndrome (ARDS) Survivors, Spirometry and Lung Volumes Normalize by 6 Months and Diffusion Capacity Normalize by 5 Years (Am J Respir Crit Care Med, 2003) [MEDLINE] (NEJM, 2003) [MEDLINE] (NEJM, 2011) [MEDLINE]
Weight Loss is Especially Common in Patients Receiving Mechanical Ventilation, Who Often Receive <60% of Their Daily Prescribed Energy Requirements as a Result of Tube Feeding Intolerance, Delays, or Interruptions (JPEN J Parenter Enteral Nutr, 2003) [MEDLINE]
In One Study of Acute Respiratory Distress Syndrome (ARDS) Survivors, Patients Lost 18% of Their Baseline Body Weight (with Weight Gain to Near Normal Levels by 12 Months) (NEJM, 20003) [MEDLINE]
Although the Relationship is Unproven, Malnutrition Likely Contributes to the Development of Subjective Weakness and Decrease in Exercise Capacity
Additionally, Postextubation Swallowing Dysfunction May Contribute to Further Deficits in Caloric Intake (and a Requirement for Enteral/Parenteral Nutrition)
Sleep Disturbance
Epidemiology
Sleep Disturbance is Common Following Critical Illness
Systematic Review of Sleep Disturbance Following Critical Illness (Ann Am Thorac Soc, 2017) [MEDLINE]: n = 22 studies
Subjective Questionnaire Studies Demonstrated a 50-66.7% (Within 1 Month), 34-64.3% (>1-3 Months), 22-57% (>3-6 Months), and 10-61% (>6 Months) Prevalence of Abnormal Sleep After Hospital Discharge
Of the Studies Assessing Multiple Time Points, Four of the Five Questionnaire Studies and Five of Five Polysomnography Studies Demonstrated Improved Aspects of Sleep Over Time
Prehospital Risk Factors
Chronic Comorbidity
Preexisting Sleep Abnormality
In-Hospital Risk Factors
In-Hospital Sleep Disturbance
Intensive Care Unit Acute Stress Symptoms
Pain Medication Use
Severity of Acute Illness
Sleep Disturbance was Frequently Associated with Postdischarge Psychological Comorbidities and Impaired Quality of Life
Contractures/Impaired Limb Function
Epidemiology
Joint Contractures Can Develop as a Consequence of Prolonged Immobility
XXX
In One Study of Intensive Care Survivors (After Admission for ≥14 Days), 34% of Patients Had a Functionally Significant Contracture at Intensive Care Unit Discharge (CMAJ, 2008) [MEDLINE]
In Most Patients, This Limitation Persisted Throughout the Hospitalization
The Most Commonly Affected Joints are the Elbow and Ankle, Followed by the Hip and Knee
Use of Glucocorticoids were a Protective Factor in This Study
In One Study of Contractures in Intensive Care Survivors (After Admission for ≥3 Days), 47% of Patients Had Upper Limb Dysfunction at 6 Months (Crit Care Med, 2018) [MEDLINE]
Long-Term Prognosis
As Compared to Cognitive/Psychiatric Dysfunction, Physical Dysfunction Following Critical Illness is More Likely to Improve (Particularly Over the First 12 Months)
Prospective Multicenter Study of Intensive Care Unit Survivors (Crit Care Med, 2014) [MEDLINE]: n = 222
Approximately 36% of Patients Had Physical Dysfunction on Discharge Which Improved Over the First 12 to 24 Months (14% and 9%, Respectively
Rate of Improvement May Also Be More Prolonged in Those with Physiologically Documented Polyneuropathy/Polymyopathy and in Those Receiving Prolonged Mechanical Ventilation (Crit Care Med, 2003) [MEDLINE] (Crit Care Med, 2014) [MEDLINE]
ABCDEF Bundle (Crit Care, 2010) [MEDLINE] (Curr Opin Crit Care, 2011) [MEDLINE] (Am J Respir Crit Care Med, 2017) [MEDLINE] (Am J Respir Crit Care Med, 2017) [MEDLINE] (Crit Care Med, 2019) [MEDLINE]
ABCDEF Bundle Components
Awakening and Breathing Coordination with Daily Sedative Interruption and Ventilator Liberation Practices (Lancet, 2008) [MEDLINE]
Delirium Monitoring and Management (JAMA, 2001) [MEDLINE] (Intensive Care Med, 2001) [MEDLINE]
Early Ambulation in the Intensive Care Unit (When Feasible) (Crit Care Med, 2008) [MEDLINE] (Lancet, 2009) [MEDLINE] (Chest, 2014) [MEDLINE] (Lancet, 2016) [MEDLINE]
Family Empowerment/Engagement
Clinical Efficacy
French IPREA Cluster-Randomized Controlled Trial of a Tailored Multicomponent Program to Decrease Discomfort in Critically Ill Patients (Intensive Care Med, 2017) [MEDLINE]: n = 398 (experimental) and 360 (control) from 34 French intensive care units
Tailored Multicomponent Program Decreased Self-Perceived Discomfort in Adult Critically Ill Patients, as Compared to Standard Care
IPREA-AQVAR Tailored Multicomponent Program for Discomfort Reduction in Critically Ill Patients (Intensive Care Med, 2019) [MEDLINE]: n = 344 exposed (to program) and 475 unexposed (to program)
Tailored Multicomponent Program May Decrease Posttraumatic Stress Disorder (PTSD) in Intensive Care Survivors at 1 Year
Large Trial of ABCDEF Bundle in Adults in the Intensive Care Unit (Crit Care Med, 2019)[MEDLINE]; n = 15,226
Complete ABCDEF bundle performance was associated with lower likelihood of seven outcomes
Hospital death within 7 days (Adjusted Hazard Ratio 0.32; CI: 0.17-0.62)
next-day mechanical ventilation (Adjusted Odds Ratio 0.28; CI: 0.22-0.36)
Coma (Adjusted Odds Ratio 0.35; CI: 0.22-0.56)
Delirium (Adjusted Odds Ratio0.60; CI: 0.49-0.72)
physical restraint use (Adjusted Odds Ratio 0.37; CI: 0.30-0.46)
discharge to a facility other than home (Adjusted Odds Ratio 0.64; CI: 0.51-0.80)
Consistent dose-response relationship between higher proportional bundle performance and improvements in each of the above-mentioned clinical outcomes (all p<0.002)
Significant Pain was More Frequently Reported as Bundle Performance Proportionally Increased (p = 0.0001)
Intensive Care Unit (ICU) Diaries
Intensive Care Unit Diaries Can Foster the Formation of Factual Memories Experienced by Patient During Their Intensive Care Unit Stay
Small Prospective or Randomized Studies Have Demonstrated that the Use of an Intensive Care Unit Diary Maintained Prospectively During the Patient’s Intensive Care Unit Stay by Family Members, Health Care Providers (or Both) Decreases the Symptoms of Posttraumatic Stress Disorder (PTSD) (Crit Care, 2010) [MEDLINE] (Crit Care Med, 2012) [MEDLINE] (Crit Care Med, 2014) [MEDLINE] (Crit Care Med, 2018) [MEDLINE]
Randomized Controlled Trial of Intensive Care Unit Diaries on the Development of Posttraumatic Stress Disorder Symptoms in Patients Receiving Mechanical Ventilation (JAMA, 2019) [MEDLINE]
In Patients Who Received Mechanical Ventilation in the Intensive Care Unit, the Use of an Intensive Care Unit Diary Filled in by Clinicians and Family Members Did Not Significantly Decrease the Number of Patients Who Reported Significant Posttraumatic Stress Disorder (PTSD) Symptoms at 3 Months
Early Ambulation/Physical Therapy
Clinical Efficacy
Secondary Analysis of Early Mobilization in Mechanically-Ventilated Intensive Care Unit Patients (Chest, 2014) [MEDLINE]: n = 104
On Logistic Regression Analysis, Early Mobilization and Increasing Insulin Dose Prevented the Incidence of Intensive Care Unit (ICU)-Acquired Weakness (Odds Ratio of 0.18; P = 0.001 and Odds Ratio of 0.001, P = .011; Respectively), Independent of Known Risk Factors for Weakness
Early Mobilization Also Significantly Decreased Insulin Requirements to Achieve Similar Glycemic Goals, as Compared with Control Patients (0.07 Units/kg/day vs 0.2 Units/kg/day, P < 0.001)
Pooled Meta-Analysis of Early Mobilization Data in Mechanically Ventilated Patients (Am J Respir Crit Care Med, 2017) [MEDLINE]
Early Mobilization Decreased the Duration of Mechanical Ventilation (Mean Difference 2.7 Fewer Days; 95% CIL 1.19–4.21)
Early Mobilization Patients were More Likely to Be Able to Walk at Discharge (64% vs. 41.4%; RR, 1.56; 95% CI: 1.15–2.10)
There was No Impact on Mortality Rate, ICU Length of Stay, Ability to Walk at ICU Discharge, 6-Minute Walk Distance or Ventilator-Free Days
Trials Did Not Provide Adequate Details to Assess Adverse Events
Recommendations
American Thoracic Society/American College of Chest Physicians Clinical Practice Guideline: Liberation from Mechanical Ventilation in Critically Ill Adults. Rehabilitation Protocols, Ventilator Liberation Protocols, and Cuff Leak Tests (Am J Respir Crit Care Med, 2017) [MEDLINE]
XXXX
American Thoracic Society/American College of Chest Physicians Clinical Practice Guideline: Liberation from Mechanical Ventilation in Critically Ill Adults (Am J Respir Crit Care Med, 2017) [MEDLINE]
XXXX
Society of Critical Care Medicine Clinical Practice Guidelines for the Prevention and Management of Pain, Agitation/Sedation, Delirium, Immobility, and Sleep Disruption in Adult Patients in the ICU (Crit Care Med, 2018) [MEDLINE]
XXXX
Cognitive Therapy
xxxx
Optimization of Glucose Management
Use of Insulin Protocols to Maintain Normoglycemia Have Been Demonstrated to Decrease the Rate of Intensive Care Unti (ICU)-Acquired Weakness (Am J Respir Crit Care Med, 2007) [MEDLINE] (Chest, 2014) [MEDLINE]
However, the Potential Benefit of Intensive Insulin Therapy Must Be Carefully Weighed Against the Long-Term Neuropsychological Harm Associated with Hypoglycemia in the Critically Ill
Glucocorticoid Administration Has Been Demonstrated to Decrease the Risk of Posttraumatic Stress Disorder (PTSD) (Crit Care Med, 1999) [MEDLINE] (Biol Psychiatry, 2001) [MEDLINE] (Psychol Med, 2013) [MEDLINE]
However, Despite This Observation, Glucocorticoids Should Not Be Administered Solely for This Indication
Treatment
Physical Rehabilitation
Physical rehabilitation Decreases cognitive impairment and psychiatric morbidity, as well as improve physical function (Crit Care Med, 2003) [MEDLINE] (Lancet, 2009) [MEDLINE] (Am J Respir Crit Care Med, 2012) [MEDLINE] (Crit Care Med, 2015) [MEDLINE]
Prognosis
Critical Illness is Associated with Subsequent Decreased Health-Related Quality of Life (HRQOL)
Health-Related Quality of Life (HRQOL) is Significantly Lower in Critical Illness and in Their Family Members
Prospective Observational Trial of Intensive Care Survivors (Chest, 2002) [MEDLINE]
Although Patients Who Develop Acute Organ Dysfunction are at Risk for Late Adverse Outcomes, Their Risk is Due Predominantly to Poor Baseline Status Prior to Illness and Not Due to the Organ Dysfunction Per Se
Systematic Review of Intensive Care Survivors (Crit Care Med, 2010) [MEDLINE]: n = 53 studies (from 10 centers)
Study Demonstrated Lower Quality of Life, as Compared with Age and Sex-Matched Controls
Prospective Longitudinal Multicenter Trial of Intensive Care Survivors (Crit Care, 2010) [MEDLINE]
A Large Proportion of the Decrease in the Health Related Quality of Life After Being in the Intensive Care Unit is Attributable to Preexisting Disease
Critical Illness is Associated with a Subsequent Increased Risk of Post-Intensive Care Unit Rehospitalization
Risk of Rehospitalization is Increased After Critical Illness and the Risk Persists for Years (Crit Care Med, 2015) [MEDLINE]
Critical Illness is Associated with a Subsequent Increased Mortality Rate
Mortality Risk is Elevated in Patients After Critical Illness (JAMA, 2010) [MEDLINE] (Crit Care Med, 2013) [MEDLINE] (Crit Care Med, 2013) [MEDLINE] (Am J Respir Crit Care Med, 2014) [MEDLINE] (Am J Respir Crit Care Med, 2016) [MEDLINE]
Risk is Highest in the First 3-6 Months After an Intensive Care Unit Admission
National Registry Database Study of Mortality Risk in Intensive Care Survivors (Crit Care Med, 2013) [MEDLINE]: n = 9,000
One/Two/Three Year Mortality Rates: 13%/19%/28%
As Compared with Elective and Cardiac Surgical Patients, Medical Patients and Those with Cancer Had Higher Mortality Rates (Hazard Ratios 1.4 and 1.9, Respectively)
Increased Mortality Risk is Likely Related to Preexisting Illnesses, New Impairments, and/or a Decline in Preexisting Organ Dysfunction and Impairments, Which Predispose to the Development of Acute Illness
Subgroups at Highest Mortality Risk After Critical Illness (JAMA, 1997) [MEDLINE] (JAMA, 2010) [MEDLINE] (Crit Care Med, 2013) [MEDLINE] (Crit Care Med, 2013) [MEDLINE] (Crit Care, 2016) [MEDLINE]
Disposition from Medical Intensive Care Unit (as Opposed to Patients from Surgical Intensive Care Unit)
Disposition to Skilled Nursing Facility or Long-Term Acute Care Facility
Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. N Engl J Med. 2000;342(18):1301 [MEDLINE]
Early goal-directed therapy in the treatment of severe sepsis and septic shock. N Engl J Med. 2001;345(19):1368 [MEDLINE]
Variation in critical care services across North America and Western Europe. Crit Care Med. 2008 Oct;36(10):2787-93, e1-9 [MEDLINE]
Improving long-term outcomes after discharge from intensive care unit: report from a stakeholders’ conference. Crit Care Med. 2012 Feb;40(2):502-9 [MEDLINE]
An exploration of social and economic outcome and associated health-related quality of life after critical illness in general intensive care unit survivors: a 12-month follow-up study. Crit Care. 2013 May;17(3):R100 [MEDLINE]
Physical and cognitive performance of patients with acute lung injury 1 year after initial trophic versus full enteral feeding. EDEN trial follow-up. Am J Respir Crit Care Med. 2013 Sep;188(5):567-76 [MEDLINE]
BRAIN-ICU Study. Long-term cognitive impairment after critical illness. N Engl J Med. 2013;369(14):1306 [MEDLINE]
Epidemiology
An exploration of social and economic outcome and associated health-related quality of life after critical illness in general intensive care unit survivors: a 12-month follow-up study. Crit Care. 2013 May;17(3):R100 [MEDLINE]
Physical and cognitive performance of patients with acute lung injury 1 year after initial trophic versus full enteral feeding. EDEN trial follow-up. Am J Respir Crit Care Med. 2013 Sep;188(5):567-76 [MEDLINE]
BRAIN-ICU Study. Long-term cognitive impairment after critical illness. N Engl J Med. 2013;369(14):1306 [MEDLINE]
Depression, post-traumatic stress disorder, and functional disability in the BRAIN-ICU study: a longitudinal cohort study. Lancet Respir Med. 2014;5:369 [MEDLINE]
Resilience in survivors of critical illness in the context of the survivors’ experience and self-reported neuropsychological and physical function. Ann Am Thorac Soc. 2016 Aug;13(8):1351-60 [MEDLINE]
Co-Occurrence of Post-Intensive Care Syndrome Problems Among 406 Survivors of Critical Illness. Crit Care Med. 2018;46(9):1393 [MEDLINE]
Risk Factors
General
Improving long-term outcomes after discharge from intensive care unit: report from a stakeholders’ conference. Crit Care Med 2012; 40:502. DOI: 10.1097/CCM.0b013e318232da75 [MEDLINE]
Society of Critical Care Medicine’s International Consensus Conference on Prediction and Identification of Long-Term Impairments After Critical Illness. Crit Care Med 2020; 48:1670. DOI: 10.1097/CCM.0000000000004586 [MEDLINE]
Cognitive
Neuropsychological sequelae and impaired health status in survivors of severe acute respiratory distress syndrome. Am J Respir Crit Care Med. 1999;160(1):50 [MEDLINE]
Underrecognition of preexisting cognitive impairment by physicians in older ICU patients. Chest. 2003 Dec;124(6):2267-74 [MEDLINE]
Six-month neuropsychological outcome of medical intensive care unit patients. Crit Care Med. 2003;31(4):1226 [MEDLINE]
Clinical identification of cognitive impairment in ICU survivors: insights for intensivists. Intensive Care Med. 2004;30(11):1997 [MEDLINE]
Two-year cognitive, emotional, and quality-of-life outcomes in acute respiratory distress syndrome. Am J Respir Crit Care Med. 2005;171(4):340 [MEDLINE]
Prolonged cognitive dysfunction in survivors of critical illness. Anaesthesia. 2005;60(9):847 [MEDLINE]
Prolonged cognitive dysfunction in survivors of critical illness. Anaesthesia. 2005;60(9):847 [MEDLINE]
Long-term neurocognitive function after critical illness. Chest. 2006 Sep;130(3):869-78 [MEDLINE]
Long-term cognitive impairment and functional disability among survivors of severe sepsis. JAMA. 2010;304(16):1787 [MEDLINE]
Delirium as a predictor of long-term cognitive impairment in survivors of critical illness. Crit Care Med. 2010;38(7):1513 [MEDLINE]
Association of plasma beta-amyloid level and cognitive reserve with subsequent cognitive decline. JAMA. 2011;305(3):261 [MEDLINE]
Presepsis depressive symptoms are associated with incident cognitive impairment in survivors of severe sepsis: a prospective cohort study of older Americans. J Am Geriatr Soc. 2012 Dec;60(12):2290-6. [MEDLINE]
Medical and economic implications of cognitive and psychiatric disability of survivorship. Semin Respir Crit Care Med. 2012 Aug;33(4):348-56 [MEDLINE]
Bidirectional relationship between cognitive function and pneumonia. Am J Respir Crit Care Med. 2013 Sep;188(5):586-92 [MEDLINE]
The adult respiratory distress syndrome cognitive outcomes study: long-term neuropsychological function in survivors of acute lung injury. Am J Respir Crit Care Med. 2012;185(12):1307 [MEDLINE]
Cognitive trajectories after postoperative delirium. N Engl J Med. 2012;367(1):30 [MEDLINE]
Medical and economic implications of cognitive and psychiatric disability of survivorship. Semin Respir Crit Care Med. 2012 Aug;33(4):348-56 [MEDLINE]
In-hospital acute stress symptoms are associated with impairment in cognition 1 year after intensive care unit admission. Ann Am Thorac Soc. 2013 Oct;10(5):450-7 [MEDLINE]
Co-Occurrence of Post-Intensive Care Syndrome Problems Among 406 Survivors of Critical Illness. Crit Care Med. 2018;46(9):1393 [MEDLINE]
Psychiatric
The effect of stress doses of hydrocortisone during septic shock on posttraumatic stress disorder and health-related quality of life in survivors. Crit Care Med. 1999 Dec;27(12):2678-83 [MEDLINE]
The effect of stress doses of hydrocortisone during septic shock on posttraumatic stress disorder in survivors. Biol Psychiatry. 2001 Dec;50(12):978-85 [MEDLINE]
Posttraumatic stress disorder in general intensive care unit survivors: a systematic review. Gen Hosp Psychiatry. 2008;30(5):421 [MEDLINE]
Depression in general intensive care unit survivors: a systematic review. Intensive Care Med. 2009 May;35(5):796-809 [MEDLINE]
Long-term complications of critical care. Crit Care Med. 2011 Feb;39(2):371-9. [MEDLINE]
Depressive symptoms and impaired physical function after acute lung injury: a 2-year longitudinal study. Am J Respir Crit Care Med. 2012;185(5):517 [MEDLINE]
The adult respiratory distress syndrome cognitive outcomes study: long-term neuropsychological function in survivors of acute lung injury. Am J Respir Crit Care Med. 2012;185(12):1307 [MEDLINE]
Post-traumatic stress disorder symptoms after acute lung injury: a 2-year prospective longitudinal study. Psychol Med. 2013;43(12):2657 [MEDLINE]
Posttraumatic stress disorder in survivors of acute lung injury: evaluating the Impact of Event Scale-Revised. Chest. 2013 Jul;144(1):24-31 [MEDLINE]
Depression, post-traumatic stress disorder, and functional disability in the BRAIN-ICU study: a longitudinal cohort study. Lancet Respir Med. 2014;5:369 [MEDLINE]
Psychiatric diagnoses and psychoactive medication use among nonsurgical critically ill patients receiving mechanical ventilation. JAMA. 2014 Mar;311(11):1133-42 [MEDLINE]
Incidence and Risk Factors for Intensive Care Unit-related Post-traumatic Stress Disorder in Veterans and Civilians. Am J Respir Crit Care Med. 2016;193(12):1373 [MEDLINE]
Physical
Paresis acquired in the intensive care unit: a prospective multicenter study. JAMA. 2002;288(22):2859 [MEDLINE]
Nutrition support in the critical care setting: current practice in canadian ICUs–opportunities for improvement? JPEN J Parenter Enteral Nutr. 2003 Jan;27(1):74-83 [MEDLINE]
Pulmonary function and health-related quality of life in survivors of acute respiratory distress syndrome. Am J Respir Crit Care Med. 2003;167(5):690 [MEDLINE]
One-year outcomes in survivors of the acute respiratory distress syndrome. N Engl J Med. 2003;348(8):683 [MEDLINE]
Neuromuscular dysfunction acquired in critical illness: a systematic review. Intensive Care Med. 2007 Nov;33(11):1876-91 [MEDLINE]
Joint contracture following prolonged stay in the intensive care unit. CMAJ. 2008;178(6):691 [MEDLINE]
Functional disability 5 years after acute respiratory distress syndrome. N Engl J Med. 2011;364(14):1293 [MEDLINE]
Long-term cognitive impairment after critical illness. N Engl J Med. 2013;369(14):1306 [MEDLINE]
Depression, post-traumatic stress disorder, and functional disability in the BRAIN-ICU study: a longitudinal cohort study. Lancet Respir Med. 2014;5:369 [MEDLINE]
Physical complications in acute lung injury survivors: a two-year longitudinal prospective study. Crit Care Med. 2014;42(4):849 [MEDLINE]
Acute outcomes and 1-year mortality of intensive care unit-acquired weakness. A cohort study and propensity-matched analysis. Am J Respir Crit Care Med. 2014;190(4):410 [MEDLINE]
Risk factors for physical impairment after acute lung injury in a national, multicenter study. Am J Respir Crit Care Med. 2014;189(10):1214. [MEDLINE]
An official American Thoracic Society Clinical Practice guideline: the diagnosis of intensive care unit-acquired weakness in adults. Am J Respir Crit Care Med. 2014;190(12):1437 [MEDLINE]
Neuromuscular Blocking Agents and Neuromuscular Dysfunction Acquired in Critical Illness: A Systematic Review and Meta-Analysis. Crit Care Med. 2016 Nov;44(11):2070-2078. doi: 10.1097/CCM.0000000000001839 [MEDLINE]
Sleep Disturbance after Hospitalization and Critical Illness: A Systematic Review. Ann Am Thorac Soc. 2017;14(9):1457 [MEDLINE]
Shoulder Impairment Following Critical Illness: A Prospective Cohort Study. Crit Care Med. 2018;46(11):1769 [MEDLINE]
Clinical
General
Hazards of hospitalization of the elderly. Ann Intern Med. 1993;118(3):219 [MEDLINE]
Hospitalization-associated disability: “She was probably able to ambulate, but I’m not sure”. JAMA. 2011;306(16):1782 [MEDLINE]
Post-hospital syndrome–an acquired, transient condition of generalized risk. N Engl J Med. 2013 Jan;368(2):100-2 [MEDLINE]
Cognitive
Neuropsychological sequelae and impaired health status in survivors of severe acute respiratory distress syndrome. Am J Respir Crit Care Med. 1999;160(1):50 [MEDLINE]
Underrecognition of preexisting cognitive impairment by physicians in older ICU patients. Chest. 2003 Dec;124(6):2267-74 [MEDLINE]
Six-month neuropsychological outcome of medical intensive care unit patients. Crit Care Med. 2003;31(4):1226 [MEDLINE]
Clinical identification of cognitive impairment in ICU survivors: insights for intensivists. Intensive Care Med. 2004;30(11):1997 [MEDLINE]
Prolonged cognitive dysfunction in survivors of critical illness. Anaesthesia. 2005;60(9):847 [MEDLINE]
Two-year cognitive, emotional, and quality-of-life outcomes in acute respiratory distress syndrome. Am J Respir Crit Care Med. 2005;171(4):340 [MEDLINE]
Prolonged cognitive dysfunction in survivors of critical illness. Anaesthesia. 2005;60(9):847 [MEDLINE]
Long-term neurocognitive function after critical illness. Chest. 2006 Sep;130(3):869-78 [MEDLINE]
Long-term cognitive impairment and functional disability among survivors of severe sepsis. JAMA. 2010;304(16):1787 [MEDLINE]
Delirium as a predictor of long-term cognitive impairment in survivors of critical illness. Crit Care Med. 2010;38(7):1513 [MEDLINE]
Association of plasma beta-amyloid level and cognitive reserve with subsequent cognitive decline. JAMA. 2011;305(3):261 [MEDLINE]
Presepsis depressive symptoms are associated with incident cognitive impairment in survivors of severe sepsis: a prospective cohort study of older Americans. J Am Geriatr Soc. 2012 Dec;60(12):2290-6. [MEDLINE]
Medical and economic implications of cognitive and psychiatric disability of survivorship. Semin Respir Crit Care Med. 2012 Aug;33(4):348-56 [MEDLINE]
The adult respiratory distress syndrome cognitive outcomes study: long-term neuropsychological function in survivors of acute lung injury. Am J Respir Crit Care Med. 2012;185(12):1307 [MEDLINE]
Cognitive trajectories after postoperative delirium. N Engl J Med. 2012;367(1):30 [MEDLINE]
Medical and economic implications of cognitive and psychiatric disability of survivorship. Semin Respir Crit Care Med. 2012 Aug;33(4):348-56 [MEDLINE]
Bidirectional relationship between cognitive function and pneumonia. Am J Respir Crit Care Med. 2013 Sep;188(5):586-92 [MEDLINE]
In-hospital acute stress symptoms are associated with impairment in cognition 1 year after intensive care unit admission. Ann Am Thorac Soc. 2013 Oct;10(5):450-7 [MEDLINE]
Co-Occurrence of Post-Intensive Care Syndrome Problems Among 406 Survivors of Critical Illness. Crit Care Med. 2018;46(9):1393 [MEDLINE]
Psychiatric
The effect of stress doses of hydrocortisone during septic shock on posttraumatic stress disorder and health-related quality of life in survivors. Crit Care Med. 1999 Dec;27(12):2678-83 [MEDLINE]
The effect of stress doses of hydrocortisone during septic shock on posttraumatic stress disorder in survivors. Biol Psychiatry. 2001 Dec;50(12):978-85 [MEDLINE]
Posttraumatic stress disorder in general intensive care unit survivors: a systematic review. Gen Hosp Psychiatry. 2008;30(5):421 [MEDLINE]
Depression in general intensive care unit survivors: a systematic review. Intensive Care Med. 2009 May;35(5):796-809 [MEDLINE]
Long-term complications of critical care. Crit Care Med. 2011 Feb;39(2):371-9. [MEDLINE]
Depressive symptoms and impaired physical function after acute lung injury: a 2-year longitudinal study. Am J Respir Crit Care Med. 2012;185(5):517 [MEDLINE]
The adult respiratory distress syndrome cognitive outcomes study: long-term neuropsychological function in survivors of acute lung injury. Am J Respir Crit Care Med. 2012;185(12):1307 [MEDLINE]
Post-traumatic stress disorder symptoms after acute lung injury: a 2-year prospective longitudinal study. Psychol Med. 2013;43(12):2657 [MEDLINE]
Posttraumatic stress disorder in survivors of acute lung injury: evaluating the Impact of Event Scale-Revised. Chest. 2013 Jul;144(1):24-31 [MEDLINE]
Depression, post-traumatic stress disorder, and functional disability in the BRAIN-ICU study: a longitudinal cohort study. Lancet Respir Med. 2014;5:369 [MEDLINE]
Psychiatric diagnoses and psychoactive medication use among nonsurgical critically ill patients receiving mechanical ventilation. JAMA. 2014 Mar;311(11):1133-42 [MEDLINE]
Incidence and Risk Factors for Intensive Care Unit-related Post-traumatic Stress Disorder in Veterans and Civilians. Am J Respir Crit Care Med. 2016;193(12):1373 [MEDLINE]
Physical
Paresis acquired in the intensive care unit: a prospective multicenter study. JAMA. 2002;288(22):2859 [MEDLINE]
Nutrition support in the critical care setting: current practice in canadian ICUs–opportunities for improvement? JPEN J Parenter Enteral Nutr. 2003 Jan;27(1):74-83 [MEDLINE]
Pulmonary function and health-related quality of life in survivors of acute respiratory distress syndrome. Am J Respir Crit Care Med. 2003;167(5):690 [MEDLINE]
One-year outcomes in survivors of the acute respiratory distress syndrome. N Engl J Med. 2003;348(8):683 [MEDLINE]
Neuromuscular dysfunction acquired in critical illness: a systematic review. Intensive Care Med. 2007 Nov;33(11):1876-91 [MEDLINE]
Joint contracture following prolonged stay in the intensive care unit. CMAJ. 2008;178(6):691 [MEDLINE]
Functional disability 5 years after acute respiratory distress syndrome. N Engl J Med. 2011;364(14):1293 [MEDLINE]
Long-term cognitive impairment after critical illness. N Engl J Med. 2013;369(14):1306 [MEDLINE]
Depression, post-traumatic stress disorder, and functional disability in the BRAIN-ICU study: a longitudinal cohort study. Lancet Respir Med. 2014;5:369 [MEDLINE]
Physical complications in acute lung injury survivors: a two-year longitudinal prospective study. Crit Care Med. 2014;42(4):849 [MEDLINE]
Acute outcomes and 1-year mortality of intensive care unit-acquired weakness. A cohort study and propensity-matched analysis. Am J Respir Crit Care Med. 2014;190(4):410 [MEDLINE]
Risk factors for physical impairment after acute lung injury in a national, multicenter study. Am J Respir Crit Care Med. 2014;189(10):1214. [MEDLINE]
An official American Thoracic Society Clinical Practice guideline: the diagnosis of intensive care unit-acquired weakness in adults. Am J Respir Crit Care Med. 2014;190(12):1437 [MEDLINE]
Neuromuscular Blocking Agents and Neuromuscular Dysfunction Acquired in Critical Illness: A Systematic Review and Meta-Analysis. Crit Care Med. 2016 Nov;44(11):2070-2078. doi: 10.1097/CCM.0000000000001839 [MEDLINE]
Sleep Disturbance after Hospitalization and Critical Illness: A Systematic Review. Ann Am Thorac Soc. 2017;14(9):1457 [MEDLINE]
Shoulder Impairment Following Critical Illness: A Prospective Cohort Study. Crit Care Med. 2018;46(11):1769 [MEDLINE]
Prevention
Delirium in mechanically ventilated patients: validity and reliability of the confusion assessment method for the intensive care unit (CAM-ICU). JAMA. 2001;286(21):2703 [MEDLINE]
Intensive Care Delirium Screening Checklist: evaluation of a new screening tool. Intensive Care Med. 2001;27(5):859 [MEDLINE]
Impact of intensive insulin therapy on neuromuscular complications and ventilator dependency in the medical intensive care unit. Am J Respir Crit Care Med. 2007;175(5):480 [MEDLINE]
Efficacy and safety of a paired sedation and ventilator weaning protocol for mechanically ventilated patients in intensive care (Awakening and Breathing Controlled trial): a randomised controlled trial. Lancet. 2008;371(9607):126 [MEDLINE]
Early intensive care unit mobility therapy in the treatment of acute respiratory failure. Crit Care Med. 2008 Aug;36(8):2238-43 [MEDLINE]
Early physical and occupational therapy in mechanically ventilated, critically ill patients: a randomised controlled trial. Lancet. 2009;373(9678):1874 [MEDLINE]
Liberation and animation for ventilated ICU patients: the ABCDE bundle for the back-end of critical care. Crit Care. 2010;14(3):157 [MEDLINE]
Intensive care diaries reduce new onset post traumatic stress disorder following critical illness: a randomised, controlled trial. Crit Care. 2010;14(5):R168 [MEDLINE]
Sedation, delirium and mechanical ventilation: the ‘ABCDE’ approach. Curr Opin Crit Care. 2011 Feb;17(1):43-9 [MEDLINE]
Impact of an intensive care unit diary on psychological distress in patients and relatives. Crit Care Med. 2012 Jul;40(7):2033-40 [MEDLINE]
Rehabilitation interventions for postintensive care syndrome: a systematic review. Crit Care Med. 2014;42(5):1263 [MEDLINE]
Impact of early mobilization on glycemic control and ICU-acquired weakness in critically ill patients who are mechanically ventilated. Chest. 2014;146(3):583 [MEDLINE]
Impact of early mobilization on glycemic control and ICU-acquired weakness in critically ill patients who are mechanically ventilated. Chest. 2014;146(3):583 [MEDLINE]
Early, goal-directed mobilisation in the surgical intensive care unit: a randomised controlled trial. Lancet. 2016;388(10052):1377 [MEDLINE]
An Official American Thoracic Society/American College of Chest Physicians Clinical Practice Guideline: Liberation from Mechanical Ventilation in Critically Ill Adults. Rehabilitation Protocols, Ventilator Liberation Protocols, and Cuff Leak Tests. Am J Respir Crit Care Med. 2017;195(1):120 [MEDLINE]
Official Executive Summary of an American Thoracic Society/American College of Chest Physicians Clinical Practice Guideline: Liberation from Mechanical Ventilation in Critically Ill Adults. Am J Respir Crit Care Med. 2017;195(1):115 [MEDLINE]
IPREA Trial. A tailored multicomponent program to reduce discomfort in critically ill patients: a cluster-randomized controlled trial. Intensive Care Med. 2017;43(12):1829 [MEDLINE]
Preventing Posttraumatic Stress in ICU Survivors: A Single-Center Pilot Randomized Controlled Trial of ICU Diaries and Psychoeducation. Crit Care Med. 2018;46(12):1914 [MEDLINE]
Staged Implementation of Awakening and Breathing, Coordination, Delirium Monitoring and Management, and Early Mobilization Bundle Improves Patient Outcomes and Reduces Hospital Costs. Crit Care Med. 2019;47(7):885 [MEDLINE]
Effect of an ICU Diary on Posttraumatic Stress Disorder Symptoms Among Patients Receiving Mechanical Ventilation: A Randomized Clinical Trial. JAMA. 2019;322(3):229 [MEDLINE]
Caring for Critically Ill Patients with the ABCDEF Bundle: Results of the ICU Liberation Collaborative in Over 15,000 Adults. Crit Care Med. 2019;47(1):3 [MEDLINE]
IPREA-AQVAR Trial. Tailored multicomponent program for discomfort reduction in critically ill patients may decrease post-traumatic stress disorder in general ICU survivors at 1 year. Intensive Care Med. 2019;45(2):223 [MEDLINE]
Treatment
Rehabilitation after critical illness: a randomized, controlled trial. Crit Care Med. 2003 Oct;31(10):2456-61 [MEDLINE]
Early physical and occupational therapy in mechanically ventilated, critically ill patients: a randomised controlled trial. Lancet. 2009;373(9678):1874 [MEDLINE]
Improving post-intensive care unit neuropsychiatric outcomes: understanding cognitive effects of physical activity. Am J Respir Crit Care Med. 2012 Dec;186(12):1220-8 [MEDLINE]
Cooccurrence of and remission from general anxiety, depression, and posttraumatic stress disorder symptoms after acute lung injury: a 2-year longitudinal study. Crit Care Med. 2015;43(3):642 [MEDLINE]
Prognosis
Magnitude and duration of the effect of sepsis on survival. Department of Veterans Affairs Systemic Sepsis Cooperative Studies Group. JAMA. 1997 Apr;277(13):1058-63 [MEDLINE]
Does acute organ dysfunction predict patient-centered outcomes? Chest. 2002 Jun;121(6):1963-71 [MEDLINE]
Persistent neuromuscular and neurophysiologic abnormalities in long-term survivors of prolonged critical illness. Crit Care Med. 2003;31(4):1012 (Crit Care Med, 2003) [MEDLINE]
Three-year outcomes for Medicare beneficiaries who survive intensive care. JAMA. 2010 Mar;303(9):849-56 [MEDLINE]
Quality of life after intensive care: a systematic review of the literature. Crit Care Med. 2010 Dec;38(12):2386-400 [MEDLINE]
Pre-existing disease: the most important factor for health related quality of life long-term after critical illness: a prospective, longitudinal, multicentre trial. Crit Care. 2010;14(2):R67 [MEDLINE]
Mortality after hospital discharge in ICU patients. Crit Care Med. 2013 May;41(5):1229-36 [MEDLINE]
Determinants of mortality after hospital discharge in ICU patients: literature review and Dutch cohort study. Crit Care Med. 2013 May;41(5):1237-51 [MEDLINE]
Acute outcomes and 1-year mortality of intensive care unit-acquired weakness. A cohort study and propensity-matched analysis. Am J Respir Crit Care Med. 2014;190(4):410 [MEDLINE]
Early and late unplanned rehospitalizations for survivors of critical illness. Crit Care Med. 2015 Feb;43(2):430-8 [MEDLINE]
Five-Year Mortality and Hospital Costs Associated with Surviving Intensive Care. Am J Respir Crit Care Med. 2016;194(2):198 [MEDLINE]
Factors Associated with Functional Recovery among Older Intensive Care Unit Survivors. Am J Respir Crit Care Med. 2016;194(3):299 [MEDLINE]
Long-term outcomes and healthcare utilization following critical illness–a population-based study. Crit Care. 2016;20:76 [MEDLINE]
Comparison of 6-Month Outcomes of Survivors of COVID-19 versus Non-COVID-19 Critical Illness. Am J Respir Crit Care Med. 2022;205(10):1159 [MEDLINE]