Primary Spontaneous Pneumothorax was First Described by Laennec in 1819
Definitions
Primary Pneumothorax: spontaneous pneumothorax occurring in a patient without prior known underlying lung disease
However, Most Patients Believed to Have Primary Spontaneous Pneumothorax Actually Have Unrecognized Subpleural Blebs Which are the Likely Etiology of the Pneumothorax (Chest, 1990) [MEDLINE]
Secondary Pneumothorax: spontaneous pneumothorax occurring in a patient with known underlying lung disease
Demographics
Incidence
US (Males): approximately 7.4 cases per 100k population per year
US (Females): approximately 1.2 cases per 100k population per year
UK (Males): approximately 37 cases per 100k population per year
UK (Males): approximately 15.4 cases per 100k population per year
Risk Factors
Primary Spontaneous Pneumothorax
Tobacco Abuse (Smoking) (see Tobacco): predominant risk factor
In Large Swedish Case Series, Smoking Increased the Risk of a First Spontaneous Pneumothorax 9-Fold in Females and 22-Fold in Males (Chest, 1987) [MEDLINE]
Approximately 88% of Patients with Primary Spontaneous Pneumothorax Smoked
There was Dose-Response Relationship Between Smoking and the Risk of Primary Spontaneous Pneumothorax
Lifetime Risk of Primary Spontaneous Pneumothorax was 12% in Smokers, But Only 1/1000 in Never Smokers
Height
Height is a Risk Factor for Primary Spontaneous Pneumothorax (Am J Surg, 1964) [MEDLINE]
Low Body Mass Index (BMI)
Relationship of Primary Spontaneous Pneumothorax to Low Body Mass Index Has Been Reported (Eur Respir J, 2006)[MEDLINE]
Air Pollution
Clustered Cases Have Been Reported (Chest, 2007)[MEDLINE]
Atmospheric Pressure
Clustered Cases Have Been Reported (J Thorac Dis, 2010) [MEDLINE]
Pneumothorax recurrence is more common in pregnancy, poses risks to the mother and fetus, and requires close cooperation between chest physicians, obstetri- cians and thoracic surgeons (Grade C) (Thorax, 2010) [MEDLINE]
Physiology: inadvertent puncture of pleural space during procedure
Clinical Data
French Multi-Center, Randomized Trial Examining Complication Rates of Three Different Central Venous Catheter Insertion Sites (NEJM, 2015) [MEDLINE]: multi-center, randomized trial (n = 3471)
Subclavian CVC had 3x Higher Risk of Pneumothorax Requiring Chest Tube Insertion (1.5% of Cases), as Compared to Internal Jugular Sites (0.5% of cases)
Incidence of Barotrauma with Mechanical Ventilation in ARDS is Approximately 10% (NEJM, 2000) [MEDLINE] (Intensive Care Med, 2002) [MEDLINE] (NEJM, 2004) [MEDLINE]
Physiology: barotrauma
Ventilator Factors Which May Cause Alveolar Overdistention, Resulting in Alveolar Rupture
Positive-Pressure Ventilation Itself
High Tidal Volume
High Plateau Pressure (Pplat): this is the pressure which is most associated with the risk of barotrauma during mechanical ventilation in ARDS
High Peak Inspiratory Pressure (PIP)
High Positive End-Expiratory Pressure (PEEP)
Mode of Ventilation (Volume-Cycled vs Pressure-Cycled): does not appear to be associated with the risk of barotrauma (PLoS One, 2011) [MEDLINE] (Cochrane Database Syst Rev, 2015) [MEDLINE]
Disease Factors Which May Cause Alveolar Overdistention, Resulting in Alveolar Rupture
Acute Respiratory Distress Syndrome (ARDS): due to decreased lung compliance, resulting in increased alveolar pressure (Am J Respir Crit Care Med, 1995) [MEDLINE] (Intensive Care Med, 2004) [MEDLINE]
Asthma (see Asthma): due to dynamic hyperinflation, resulting in increased alveolar pressure (Intensive Care Med, 2004) [MEDLINE]
Chronic Obstructive Pulmonary Disease (COPD) (see Chronic Obstructive Pulmonary Disease): due to dynamic hyperinflation, resulting in increased alveolar pressure
Interstitial Lung Disease (ILD) (see Interstitial Lung Disease): due to decreased lung compliance, resulting in increased alveolar pressure (Intensive Care Med, 2004) [MEDLINE]
Langerhans Cell Histiocytosis (see Langerhans Cell Histiocytosis): due to cystic lung disease, resulting in escape of air
Noninvasive Positive-Pressure Ventilation Probably Has a Similar Mechanism of Barotrauma as Invasive Mechanical Ventilation, But the Rate of Barotrauma is Lower (Due to Use of Lower Pressures) (Rev Bras Ter Intensiva, 2008) [MEDLINE]
Inadvertent Extraluminal Positioning of the Tracheostomy Fenestration During Tracheostomy Placement: for this reason, fenestrated tracheostomies are typically not selected for initial percutaneous tracheostomy placement
Laceration of the Posterior Tracheal Wall
Clinical
Pneumothorax (see Pneumothorax): occurs in 0.6% of cases (Chest, 2004) [MEDLINE]
Air from Torn Alveolus Enters the Perivascular Interstitium, Dissecting Along the Bronchovascular Sheath into the Pulmonary Hila and Subsequently Into the Mediastinum, Causing Pneumomediastinum (in the Setting of Blunt Trauma to the Lung, This Tracking of Air Has Been Termed the “Macklin Effect”) (see Pneumomediastinum) (Chest, 2001) [MEDLINE]
From Pneumomediastinum, Air Can Dissect Upward into the Soft Tissues of the Neck (Causing Subcutaneous Emphysema), into the Pleural Spaces (Causing Pneumothorax on Either Side), Inferiorly into the Peritoneum (Causing Pneumoperitoneum), or Rarely, into the Pericardium (Causing Pneumopericardium)
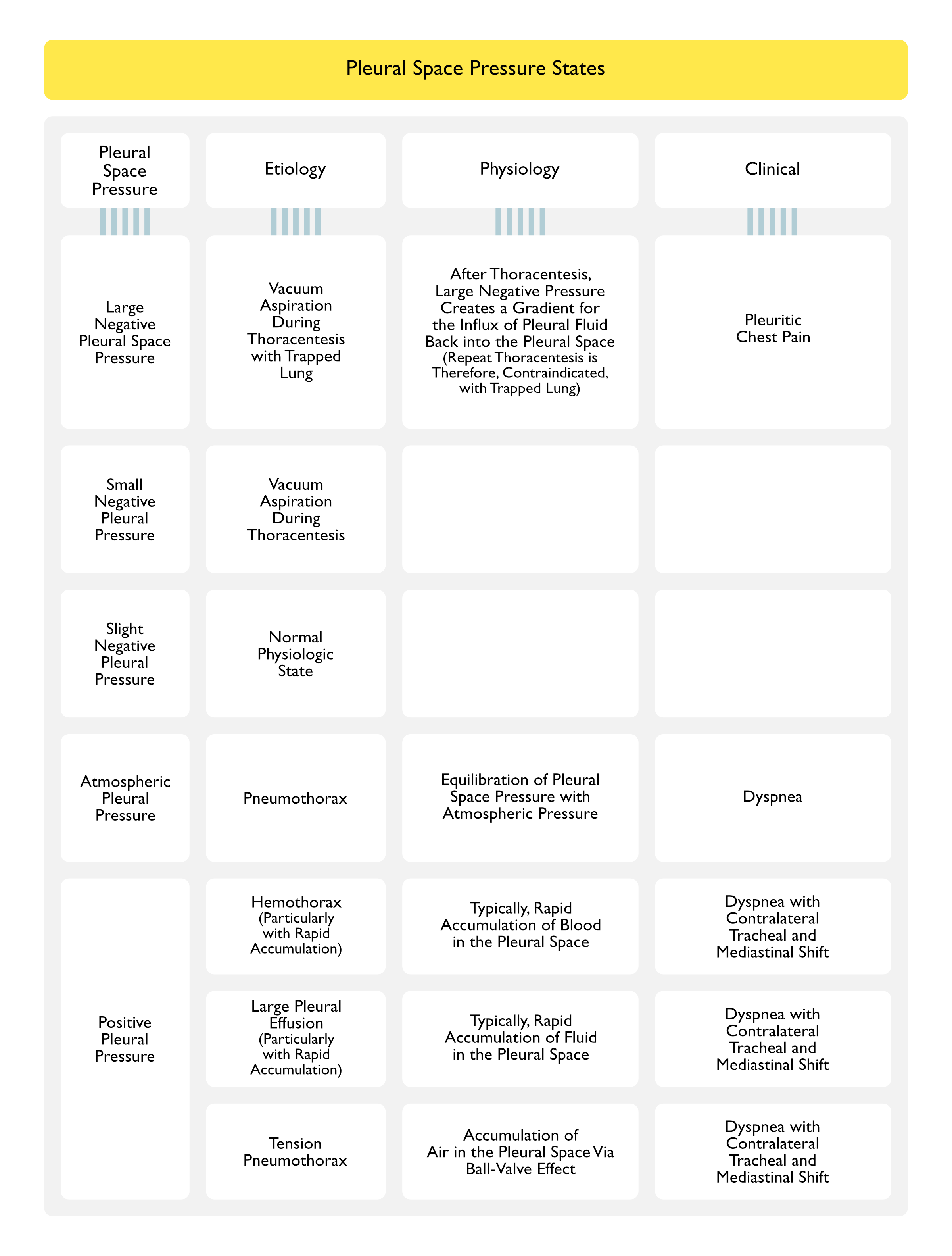
Etiologies of Various Pleural Space Pressure States
The Classically Observed Findings of Pneumothorax on Chest X-Ray (Apical White Visceral Pleural Line Which Appears Separated from the Parietal Pleura by Air) May Be Absent in Supine Patients (Especially in the Intensive Care Unit) (Postgrad Med J, 2000) [MEDLINE]
In the Supine Position, Air May Track Anteriorly or in the Subpulmonic Location
Findings
Apical White Visceral Pleural Line Which Appears Separated from the Parietal Pleura by Air: classical finding of pneumothorax on chest x-ray
Gas Outlining the Anterior Pleural Reflection or Anterloateral Border of the Mediastinum: due to air in the subpulmonic location
Deep Sulcus Sign: due to air in the subpulmonic location outlining the costophrenic sulcus
Double Diaphragm Sign: due to air in the subpulmonic location outlining the costophrenic sulcus
Continuous Diaphragm Sign (Diaphragm Appears as One Continuous Line Through Both the Left and Right Hemithorax): due to air in the subpulmonic location
Standard Upright Inspiratory Chest X-Ray is Recommended for the Initial Diagnosis of Pneumothorax, Rather than expiratory Chest X-Ray (Grade A)
The Widespread Adoption of Digital Imaging (Picture-Archiving Communication Systems, PACS) Requires Diagnostic Caution and Further Study Since the Presence of a Small Pneumothorax May Not Be Immediately Apparent on These Studies (Grade D)
Chest CT Scan is Recommended for Uncertain or Complex Cases (Grade D)
Size of Pneumothorax
In Defining a Management Strategy, the Degree of Clinical Compromise is More Important than the Size of a Pneumothorax (Grade D)
The Differentiation of Large vs Small Pneumothorax is the Presence of a Visible Rim of >2 cm Between the Lung Margin and the Chest Wall and is Easily Measured with Chest X-Ray (Grade D)
American Method: measure from apex of lung to the cupola (superior peak of thoracic cage)
British Method: interpleural distance at the level of the hilum
Accurate Pneumothorax Size Calculations are Best Achieved by Chest CT Scan (Grade C)
Chest CT May Be Necessary to Visualize Pneumothorax When Pneumothorax is Small (<500 mL), is Loculated, is Posteriorly-Located, or is Difficult to Visualize Due to Overlying Subcutaneous Emphysema
Chest CT Scan is Considered the Gold Standard for Detecting a Small Pneumothorax and for Size Estimation of a Pneumothorax (Respir Med, 2006) [MEDLINE]
Standard Upright Inspiratory Chest X-Ray is Recommended for the Initial Diagnosis of Pneumothorax, Rather than expiratory Chest X-Ray (Grade A)
The Widespread Adoption of Digital Imaging (PACS) Requires Diagnostic Caution and Further Study Since the Presence of a Small Pneumothorax May Not Be Immediately Apparent on These Studies (Grade D)
Chest CT Scan is Recommended for Uncertain or Complex Cases (Grade D)
Size of Pneumothorax
In Defining a Management Strategy, the Degree of Clinical Compromise is More Important than the Size of a Pneumothorax (Grade D)
The Differentiation of Large vs Small Pneumothorax is the Presence of a Visible Rim of >2 cm Between the Lung Margin and the Chest Wall and is Easily Measured with Chest X-Ray (Grade D)
American Method: measure from apex of lung to the cupola (superior peak of thoracic cage)
British Method: interpleural distance at the level of the hilum
Accurate Pneumothorax Size Calculations are Best Achieved by Chest CT Scan (Grade C)
Thoracentesis with Pleural Fluid Analysis (see Thoracentesis)
Pleural Fluid Eosinophilia: may be seen -> eosinophils appear within 3 days and peak at day 6
Sensitivity: very sensitive in detecting pneumothorax and can be repeated at bedside multiple times, noninvasively, and quickly (Crit Care Med, 2010) [MEDLINE]
Lung Sliding: normal finding, where the visceral pleura slides against the parietal pleura
In Pneumothorax, Lung Sliding is Absent
Lung Point Sign
In Pneumothorax, Lung Touches the Chest Wall Intermittently
Clinical Manifestations
Cardiovascular Manifestations
Hypotension: may occur with tension pneumothorax
xxxx
Pulmonary Manifestations
Unilateral or Bilateral Pneumothorax
Epidemiology
Pneumothorax is Not Usually Associated with Physical Exertion (Grade D) (Thorax, 2010) [MEDLINE]
Patients with Pre-Existing Lung Disease More Poorly Tolerate Pneumothorax (Grade D)
Physiology
XXXXX
Diagnosis
Unilateral Pneumothorax
Bilateral Pneumothorax: may occur in cases with “buffalo chest” (where mediastinum has been previously entered during prior mediastinal surgery, lung transplant, etc) (see Buffalo Chest)
Clinical
Symptoms in Primary Spontaneous Pneumothorax May Be Minimal or Absent (Thorax, 2010) [MEDLINE]
In Contrast, Symptoms are More Common in Secondary Spontaneous Pneumothorax, Even if the Pneumothorax is Relatively Small in Size (Grade D) (Thorax, 2010) [MEDLINE]
Severe Symptoms and Signs of Respiratory Distress Suggest the Presence of Tension Pneumothorax (Grade D) (Thorax, 2010) [MEDLINE]
Tension Pneumothorax is a Medical Emergency Which Requires Heightened Awareness in a Specific Range of Clinical Situations (Grade D) (Thorax, 2010) [MEDLINE]: see above
The Presence of Dyspnea Influences the Management Strategy (Grade D)
Dyspnea Indicates the Need for Active Intervention, as well as the Need for Supportive Treatment (Including Supplemental Oxygen Therapy) (Grade D)
The Size of the Pneumothorax Determines the Rate of Resolution and is a Relative Indication for Active Intervention (Grade D)
In Defining a Management Strategy, the Degree of Clinical Compromise is More Important than the Size of a Pneumothorax (Grade D)
Distinction Between Primary Spontaneous Pneumothorax and Secondary Spontaneous Pneumothorax Should Be Made at the Time of Diagnosis to Guide Appropriate Management (Grade D)
Supplemental Oxygen (100% FIO2) Creates a Nitrogen Gradient from the Pleural Space to the Alveoli and Increases the Rate of Pneumothorax Resolution by Approximately 4 to 6-Fold (BMJ, 1971) [MEDLINE] (Pediatrics, 1963) [MEDLINE]
In the Absence of Supplemental Oxygen Therapy, the Normal Rate of Absorption is 1.25 Percent of the Volume of the Pneumothorax Per 24 hrs
Patients with Primary Spontaneous Pneumothorax or Secondary Spontaneous Pneumothorax and Significant Dyspnea Associated with Any Size of Pneumothorax Should Undergo Active Intervention (Grade A)
Chest Tube is Usually Required for Tension or Bilateral Pneumothorax Who Should Be Admitted to the Hospital (Grade D)
Observation is the Treatment of Choice for Small Primary Spontaneous Pneumothorax without Significant Dyspnea (Grade B)
Selected Asymptomatic Patients with a Large Primary Spontaneous Pneumothorax May Be Managed by Observation Alone (Grade A)
Patients with a Small Primary Spontaneous Pneumothorax without Dyspnea Should Be Considered for Discharge with Early Outpatient Follow-Up (Grade D)
These Patients Should Also Be Advised to Return in the Event of Worsening Dyspnea (Grade D)
Needle Aspiration is as Effective as Large-Bore (>20 F) Chest Tube and May Be Associated with Decreased Need for Hospitalization and Decreased Hospital Length of Stay (Grade A)
Needle Aspiration Should Not Be Repeated Unless There were Technical Difficulties (Grade B)
Following Failed Needle Aspiration, Small-Bore (<14F) Chest Tube Insertion is Recommended (Grade A)
Large-Bore Chest Tube is Not Required for Pneumothorax (Grade D)
Suction
Suction Should Not Be Routinely Employed (Grade B)
*Caution is Required Because of the Risk of Re-Expansion Pulmonary Edema (Grade B)
High-Volume, Low-Pressure Suction Systems are Recommended (Grade C)
Pulmonary Consultation
Referral to a Pulmonary Physician Should Be Made within 24 h of Hospital Admission (Grade C)
Complex Chest Tube Management is Best Effected in Areas Where Specialist Medical and Nursing Expertise is Available (Grade D)
Thoracic Surgical Consultation
In Cases of Persistent Air Leak or Failure of the Lung to Reexpand, an Early Thoracic Surgical Consultation (within (3-5 Days) Should Be Obtained (Grade C)
Surgical Approach
Open Thoracotomy and Pleurectomy Remain the Procedure with the Lowest Recurrence Rate (Approximately 1%) for Difficult or Recurrent Pneumothorax (Grade A)
Video-Assisted Thoracoscopic Surgery (VATS) with Pleurectomy and Pleural Abrasion is Better Tolerated, But Has a Higher Recurrence Rate of Approximately 5% (Grade A)
Surgical Chemical Pleurodesis is Best Achieved by Using 5g of Sterile Graded Talc, with Which the Complications of Adult Respiratory Distress Syndrome and Empyema are Rare (Grade A)
Disposition and Follow-Up
Patients Should Be Advised to Return to the Hospital if Increasing Dyspnea Develops (Grade D)
All Patients Should Be Followed Up by Pulmonary Physician Until Full Resolution (Grade D)
Air Travel Should Be Avoided Until Full Resolution (Grade C)
Diving Should Be Permanently Avoided Unless the Patient Has Undergone Bilateral Surgical Pleurectomy and Has Normal Lung Function and Chest CT Scan Postoperatively (Grade C)
Recommendations (European Respiratory Society Task Force Statement-Diagnosis and Treatment of Primary Spontaneous Pneumothorax, 2015) (Eur Respir J, 2015)[MEDLINE]
Indications for Definitive Management of Primary Spontaneous Pneumothorax
Second Episode of Primary Spontaneous Pneumothorax
Patients with Primary Spontaneous Pneumothorax or Secondary Spontaneous Pneumothorax and Significant Dyspnea Associated with Any Size of Pneumothorax Should Undergo Active Intervention (Grade A)
All Patients with Secondary Spontaneous Pneumothorax Should Be Admitted to Hospital for at Least 24 hrs and Receive Supplemental Oxygen (Grade D)
Most Patients with Secondary Spontaneous Pneumothorax Will Require Insertion of a Small-Bore Chest Tube (Grade B)
Pulmonary Consultation
All Patients Require Early Referral to a Pulmonary Physician (Grade D)
Suction
Suction Should Not Be Routinely Employed (Grade B)
*Caution is Required Because of the Risk of Re-Expansion Pulmonary Edema (Grade B)
High-Volume, Low-Pressure Suction Systems are Recommended (Grade C)
Thoracic Surgical Consultation
Patients with a Persistent Air Leak Should Be Discussed with a Thoracic Surgeon at 48 hrs (Grade B)
In Cases of Persistent Air Leak or Failure of the Lung to Reexpand, an Early Thoracic Surgical Consultation (within (3-5 Days) Should Be Obtained (Grade C)
Medical Pleurodesis May Be Appropriate for Inoperable Patients (Grade D)
Medical Chemical Pleurodesis Can Control Difficult or Recurrent Pneumothoraces (Grade A), But, Since Surgical Options are More Effective, it Should Only Be Used if a Patient is Either Unwilling or Unable to Undergo Surgery (Grade B)
Medical Chemical Pleurodesis for Pneumothorax Should Only Be Performed by a Pulmonary Physician (Grade C)
Patients with Secondary Spontaneous Pneumothorax Can Be Considered for Outpatient Management with a Heimlich Valve (Grade D)
Surgical Approach
Open Thoracotomy and Pleurectomy Remain the Procedure with the Lowest Recurrence Rate (Approximately 1%) for Difficult or Recurrent Pneumothorax (Grade A)
Video-Assisted Thoracoscopic Surgery (VATS) with Pleurectomy and Pleural Abrasion is Better Tolerated, But Has a Higher Recurrence Rate of Approximately 5% (Grade A)
Surgical Chemical Pleurodesis is Best Achieved by Using 5g of Sterile Graded Talc, with Which the Complications of Adult Respiratory Distress Syndrome and Empyema are Rare (Grade A)
Disposition and Follow-Up
Patients Should Be Advised to Return to the Hospital if Increasing Dyspnea Develops (Grade D)
All Patients Should Be Followed Up by Pulmonary Physician Until Full Resolution (Grade D)
Air Travel Should Be Avoided Until Full Resolution (Grade C)
Diving Should Be Permanently Avoided Unless the Patient Has Undergone Bilateral Surgical Pleurectomy and Has Normal Lung Function and Chest CT Scan Postoperatively (Grade C)
The modern and less invasive strategies of simple observation and aspiration are usually effective during pregnancy, with elective assisted delivery and regional anaesthesia at or near term (Grade C)
A corrective surgical procedure (VATS) should be considered after delivery (Grade D)
The combination of pneumothorax and HIV infection requires early intercostal tube drainage and surgical referral, in addition to appropriate treatment for HIV and PJP infection (Grade C)
Specific Treatment of Pneumothorax Associated with Cystic Fibrosis (CF) (see xxxx)
Nonsmoking, non-alpha 1-antitrypsin deficiency-induced emphysema in nonsmokers with healed spontaneous pneumothorax, identified by computed tomography of the lungs. Chest. 1993;103(2):433 [MEDLINE]
Spontaneous pneumothorax. N Engl J Med. 2000;342(12):868 [MEDLINE]
De l’auscultation mediate, ou traité du diagnostic des maladies des poumons et du coeur, fondé principalement sur ce nouveau moyen d’exploration [On mediate auscultation, or treatise on the diseases of the lungs and heart, based principally on this new method of investigation]. Paris, Brosson and Chaudé, 1819.
SPONTANEOUS PNEUMOTHORAX. SUGGESTED ETIOLOGY AND COMPARISON OF TREATMENT METHODS. Am J Surg. 1964 Dec;108:772-6 [MEDLINE]
Smoking and the increased risk of contracting spontaneous pneumothorax. Chest. 1987 Dec;92(6):1009-12 [MEDLINE]
Pulmonary hazards of smoking marijuana as compared with tobacco. N Engl J Med 1988; 318: 347–351 [MEDLINE]
Pneumothorax in polysubstance-abusing marijuana and tobacco smokers: three cases. J Subst Abuse 1993; 5: 183–186 [MEDLINE]
Large lung bullae in marijuana smokers. Thorax. 2000 Apr;55(4):340-2 [MEDLINE]
Simplified stepwise management of primary spontaneous pneumothorax: a pilot study. Eur Respir J. 2006 Mar;27(3):470-6 [MEDLINE]
Emphysema and secondary pneumothorax in young adults smoking cannabis. Eur J Cardiothorac Surg 2007; 32: 834–838 [MEDLINE]
Atmospheric pressure influences the risk of pneumothorax: beware of the storm! Chest. 2007 Jun;131(6):1877-82 [MEDLINE]
Air pollution, weather variations and primary spontaneous pneumothorax. J Thorac Dis. 2010 Mar;2(1):9-15 [MEDLINE]
Incidence of pulmonary barotrauma in a medical ICU. Crit Care Med. 1983;11(2):67 [MEDLINE]
The effects of ventilatory pattern on hyperinflation, airway pressures, and circulation in mechanical ventilation of patients with severe air-flow obstruction. Am Rev Respir Dis. 1987 Oct;136(4):872-9 [MEDLINE]
Mean airway pressure: physiologic determinants and clinical importance–Part 2: Clinical implications. Crit Care Med. 1992;20(11):1604 [MEDLINE]
Risk factors for morbidity in mechanically ventilated patients with acute severe asthma. Am Rev Respir Dis. 1992;146(3):60 [MEDLINE]
Continuous venous air embolism in patients receiving positive end-expiratory pressure. Am Rev Respir Dis. 1993;147(4):1034 [MEDLINE]
Mechanisms of ventilator-induced lung injury. Crit Care Med. 1993;21(1):131 [MEDLINE]
Peak airway pressure: why the fuss? Chest. 1994;105(1):242 [MEDLINE]
Frequency and importance of barotrauma in 100 patients with acute lung injury. Crit Care Med. 1995;23(2):272 [MEDLINE]
Clinical risk factors for pulmonary barotrauma: a multivariate analysis. Am J Respir Crit Care Med. 1995;152(4 Pt 1):1235 [MEDLINE]
The relation of pneumothorax and other air leaks to mortality in the acute respiratory distress syndrome. N Engl J Med. 1998;338(6):341 [MEDLINE]
International consensus conferences in intensive care medicine: Ventilator-associated Lung Injury in ARDS. This official conference report was cosponsored by the American Thoracic Society, The European Society of Intensive Care Medicine, and The Societéde Réanimation de Langue Française, and was approved by the ATS Board of Directors, July 1999. Am J Respir Crit Care Med. 1999;160(6):2118 [MEDLINE]
The Macklin effect: a frequent etiology for pneumomediastinum in severe blunt chest trauma. Chest. 2001 Aug;120(2):543-7 [MEDLINE]
Relationship between ventilatory settings and barotrauma in the acute respiratory distress syndrome. Intensive Care Med. 2002;28(4):406 [MEDLINE]
Airway pressures and early barotrauma in patients with acute lung injury and acute respiratory distress syndrome. Am J Respir Crit Care Med. 2002;165(7):978 [MEDLINE]
Pneumothorax associated with long-term non-invasive positive pressure ventilation in Duchenne muscular dystrophy. Neuromuscul Disord. 2004 Jun;14(6):353-5 [MEDLINE]
Incidence, risk factors and outcome of barotrauma in mechanically ventilated patients. Intensive Care Med. 2004;30(4):612 [MEDLINE]
Pneumothorax: an important complication of non-invasive ventilation in neuromuscular disease. Neuromuscul Disord. 2004 Jun;14(6):351-2 [MEDLINE]
Occurrence of pneumothorax during noninvasive positive pressure ventilation through a helmet. J Clin Anesth. 2007 Dec;19(8):632-5 [MEDLINE]
[Evaluation of the incidence of pneumothorax and background of patients with pneumothorax during noninvasive positive pressure ventilation]. Nihon Kokyuki Gakkai Zasshi. 2008 Nov;46(11):870-4 [MEDLINE]
Benefits and complications of noninvasive mechanical ventilation for acute exacerbation of chronic obstructive pulmonary disease. Rev Bras Ter Intensiva. 2008 Jun;20(2):184-9 [MEDLINE]
Neuromuscular blockers in early acute respiratory distress syndrome. N Engl J Med. 2010;363(12):1107 [MEDLINE]
Pressure and volume limited ventilation for the ventilatory management of patients with acute lung injury: a systematic review and meta-analysis. PLoS One. 2011;6(1):e14623 [MEDLINE]
Neuromuscular blocking agents in acute respiratory distress syndrome: a systematic review and meta-analysis of randomized controlled trials. Crit Care. 2013 Mar;17(2):R43 [MEDLINE]
Pressure-controlled versus volume-controlled ventilation for acute respiratory failure due to acute lung injury (ALI) or acute respiratory distress syndrome (ARDS). Cochrane Database Syst Rev. 2015;1:CD008807 [MEDLINE]
Bilateral hydrothorax and cardiac tamponade after right subclavian vein catheterization. A case report. Korean J Anesthesiol. 2010 Dec;59 Suppl:S211-7. doi: 10.4097/kjae.2010.59.S.S211 [MEDLINE]
Intravascular Complications of Central Venous Catheterization by Insertion Site. N Engl J Med. 2015 Sep 24;373(13):1220-9. doi: 10.1056/NEJMoa1500964 [MEDLINE]
Other
Pneumothorax secondary to septic pulmonary emboli in tricuspid endocarditis. Thorax. 1992 Dec;47(12):1080-1 [MEDLINE]
Emphysema and pneumothorax after percutaneous tracheostomy: case reports and an anatomic study. Chest. 2004;125(5):1805 [MEDLINE]
Minimally invasive parathyroidectomy complicated by pneumothoraces: a report of 4 cases. J Surg Educ. 2007 Mar-Apr;64(2):101-7; discussion 113 [MEDLINE]
Pneumothorax in the critically ill patient. Chest 2012; 141:1098-1105 [MEDLINE]
Diagnosis
Computed tomography in the etiologic assessment of idiopathic spontaneous pneumothorax. Chest. 1990;98(2):341 [MEDLINE]
Radiology in heart disease. Br Med J 1933; 2:594 [MEDLINE]
A bedside ultrasound sign ruling out pneumothorax in the critically ill. Lung sliding. Chest 1995;108(5):1345-1348 [MEDLINE]
The comet-tail artifact: An ultrasound sign of alveolar-interstitial syndrome. Am J Respir Crit Care Med 1997; 156:1640-1646 [MEDLINE]
The comet-tail artifact, an ultrasound sign ruling out pneumothorax. Intensive Care Med 1999; 25:383–388 [MEDLINE]
Diagnosis of pneumothorax in critically ill adults. Postgrad Med J. 2000;76(897):399 [MEDLINE]
The “lung point”: an ultrasound sign specific to pneumothorax. Intensive Care Med 2000; 26:1434-1440 [MEDLINE]
Ultrasonic examination: an alternative to chest radiography after central venous catheter insertion? Am J Respir Crit Care Med. 2001;164(3):403-405 [MEDLINE]
Video-assisted thoracic surgery for primary spontaneous hemopneumothorax. Eur J Cardiothorac Surg. 2004;26(5):893 [MEDLINE]
Ultrasound diagnosis of occult pneumothorax. Crit Care Med 2005; 33(6):1231-1238 [MEDLINE]
Ultrasound comet-tail images: a marker of pulmonary edema: a comparative study with wedge pressure and extravascular lung water. Chest 2005;127(5):1690-1695 [MEDLINE]
Comparison between two methods for estimating pneumothorax size from chest x-rays. Respir Med 2006;100:1356e9 [MEDLINE]
Pleural ultrasonography. Clin Chest Med 2006; 27:215-227 [MEDLINE]
Clinical review: bedside lung ultrasound in critical care practice. Crit Care 2007; 11:205 [MEDLINE]
Relevance of lung ultrasound in the diagnosis of acute respiratory failure: the BLUE protocol. Chest 2008;134(1):117-125 [MEDLINE]
A-lines and B-lines: lung ultrasound as a bedside tool for predicting pulmonary artery occlusion pressure in the critically ill. Chest. 2009;136(4):1014-1020 [MEDLINE]
Pleural procedures and thoracic ultrasound: British Thoracic Society Pleural Disease Guideline. Thorax 2010; 65(Suppl 2):ii61-ii76 [MEDLINE]
Ultrasound localization of central vein catheter and detection of postprocedural pneumothorax: an alternative to chest radiography. Crit Care Med. 2010;38(2):533 [MEDLINE]
Thoracic Ultrasonography for the Pulmonary Specialist. Chest 2011; 140(5):1332–1341 [MEDLINE]
Sonographic diagnosis of pneumothorax. Intensive Care Med 2011; 37:224-232 [MEDLINE]
Clinical applications of bedside ultrasonography in internal and emergency medicine. Intern Emerg Med 2011 Jun;6(3):195-201. doi: 10.1007/s11739-010-0424-3. Epub 2010 Aug 3 [MEDLINE]
Can chest ultrasonography substitute standard chest radiography for evaluation of acute dyspnea in the emergency department? Chest 2011; 139(5):1140-1147 [MEDLINE]
Lung ultrasound in the ICU: From diagnostic instrument to respiratory monitoring tool. Minerva Anestesiol 2012; 78:1282-1296 [MEDLINE]
Lung ultrasound in the critically ill. Ann Intensive Care. 2014;4:1 [MEDLINE]
Bedside ultrasonography for the intensivist. Crit Care Clin. 2015 Jan;31(1):43-66. doi: 10.1016/j.ccc.2014.08.003. Epub 2014 Oct 3 [MEDLINE]
Treatment
SPONTANEOUS ALVEOLAR RUPTURE AT BIRTH. Pediatrics. 1963 Nov;32:816-24 [MEDLINE]
Oxygen therapy for spontaneous pneumothorax. BMJ 1971;4:86e8 [MEDLINE]
Management of spontaneous pneumothorax: an American College of Chest Physicians Delphi consensus statement. Chest. 2001;119(2):590 [MEDLINE]
Management of spontaneous pneumothorax. Clin Chest Med. 2006 Jun;27(2):369-81 [MEDLINE]
Management of spontaneous pneumothorax: state of the art. Eur Respir J. 2006 Sep;28(3):637-50 [MEDLINE]
Deviation from published guidelines in the management of primary spontaneous pneumothorax in Australia. Intern Med J. 2008 Jan;38(1):64-7 [MEDLINE]
Management of spontaneous pneumothorax: British Thoracic Society Pleural Disease Guideline 2010. Thorax. 2010;65 Suppl 2:ii18 [MEDLINE]
ERS task force statement: diagnosis and treatment of primary spontaneous pneumothorax. Eur Respir J. 2015 Aug;46(2):321-35 [MEDLINE]
Prognosis
Recurrence of primary spontaneous pneumothorax. Thorax. 1997;52(9):805 [MEDLINE]
Factors related to recurrence of spontaneous pneumothorax. Respirology. 2005;10(3):378 [MEDLINE]