Pleural space normally contains 75% macrophages + 23% lymphocytes
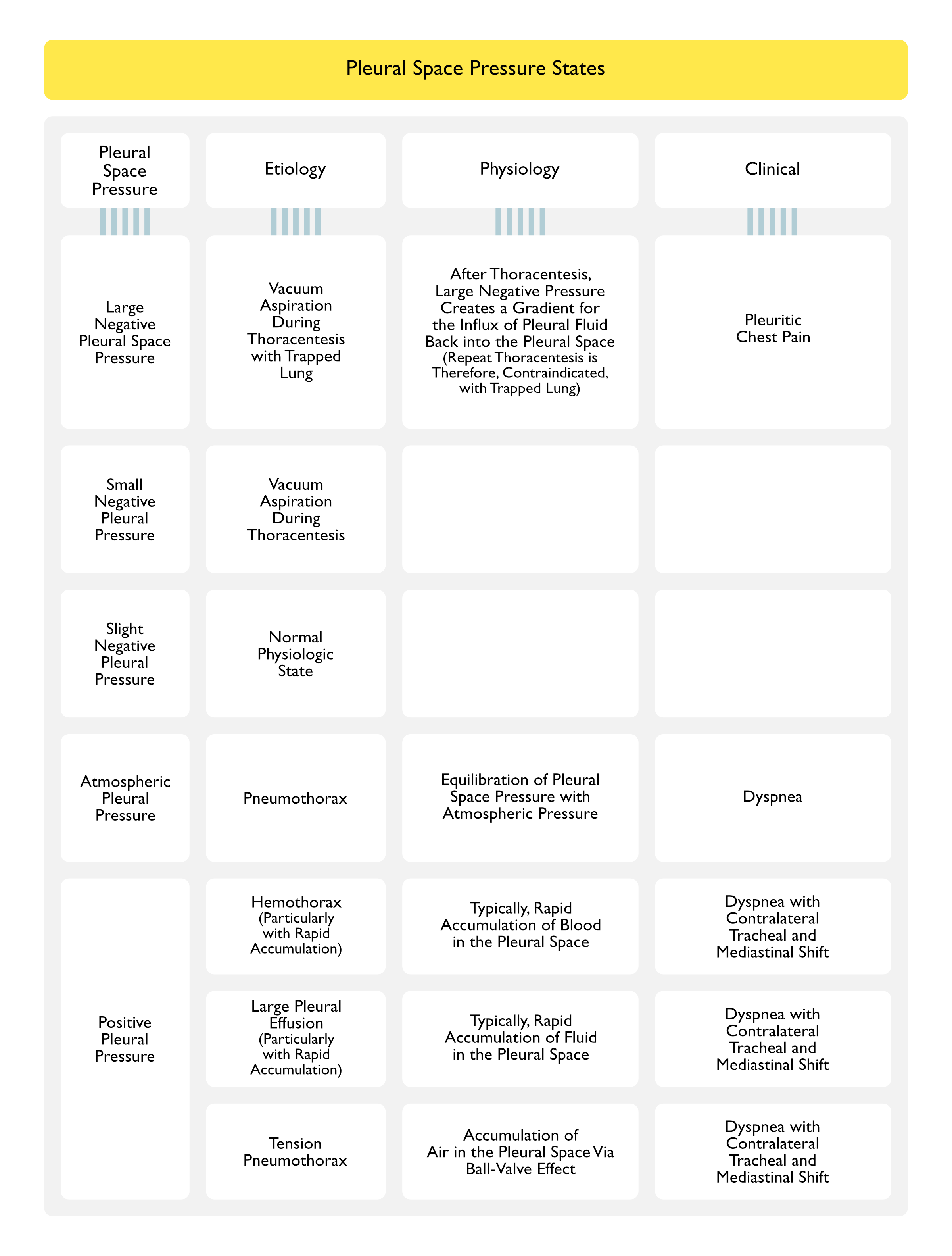
Etiologies of Various Pleural Space Pressure States
CXR Findings
Typical CXR Finding = Pleural Effusion with Contralateral Shift of Mediastinum
CXR Finding in Presence of Trapped Lung, Fixed Mediastinum, or Co-Existent Atelectasis = Pleural Effusion with Ipsilateral Shift of Mediastinum (or Midline Mediastinum)
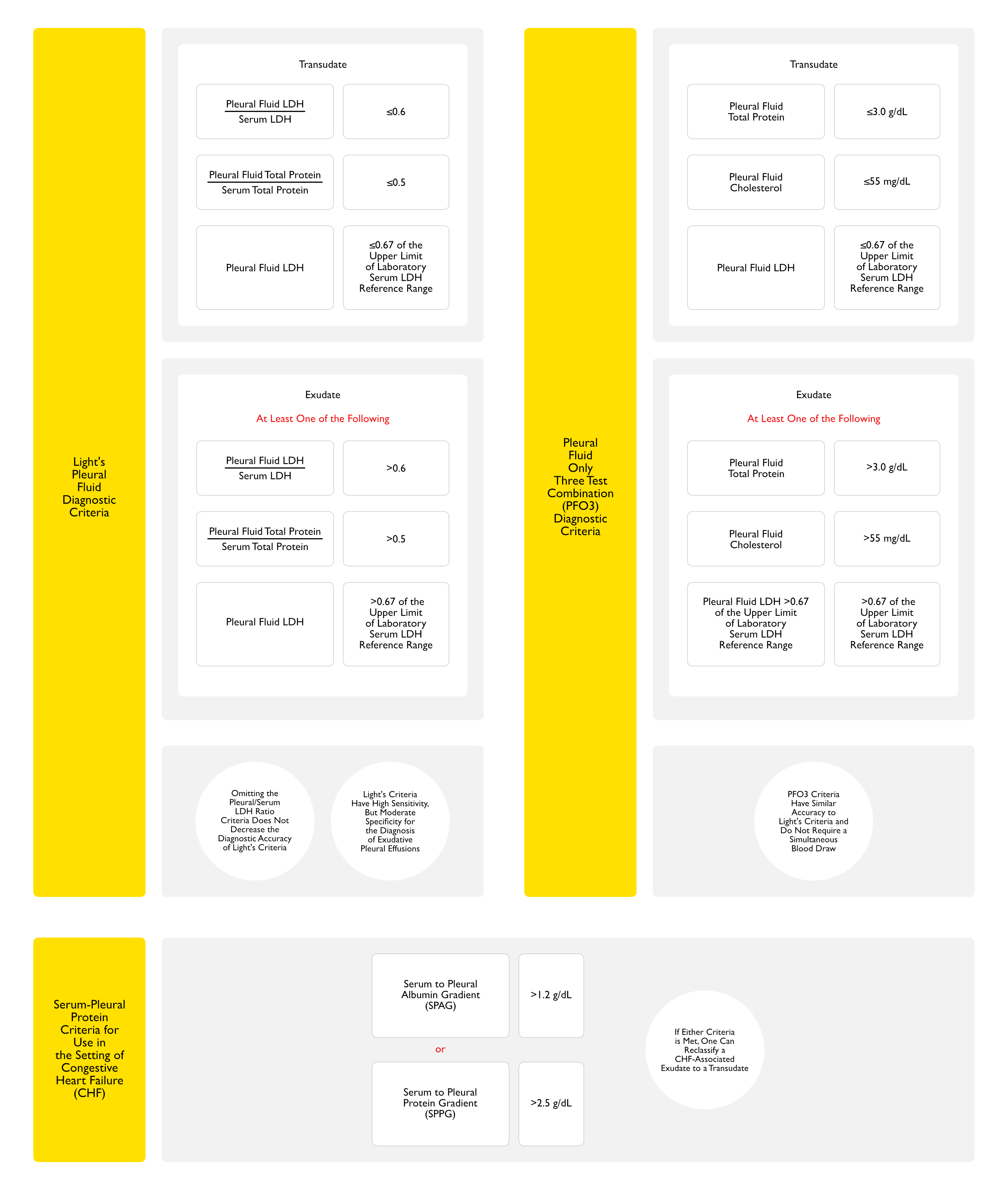
Pleural Fluid Criteria
General Comments
Pleural Fluid <0.67 of Upper Limit of Laboratory Normal Value and the Pleural/Serum Total Protein Ratio are Both Necessary from Light’s Criteria
However, Omitting the Pleural/Serum LDH Ratio Criteria Does Not Decrease Diagnostic Accuracy of Light’s Criteria
Cut-Off Values for LDH and Total Protein Ratios
Since there is not a discrete cut-off between values of LDH and total protein, the specified cut-off values give high sensitivity but lower specificity (ie: you will detect all true exudates, but you may misclassify some transudates as exudates, as in diuresed congestive heart failure cases)
Pleural LDH <66% of Upper Limit of Normal Range for Serum LDH
Pleural Cholesterol <55-60 mg/L
Pleural/Serum Cholesterol Ratio: normal
Serum-Pleural Albumin Gradient (SPAG) >1.2 g/dL
If the Pleural Fluid Clinically Appears to Be a Transudate and SPAG >1.2, But Light’s Criteria Suggest an Exudate, the Fluid Can Be Assumed to be a Transudate (Albumin is Lower Molecular Weight than Other Proteins and Crosses Capillary Walls More Readily)
General Comments: pleural effusion is considered exudative if it meets any one of the following criteria, although LDH ratio and total protein ratio are the best criteria
LDH Ratio >0.6
Total Protein Ratio >0.5
Pleural LDH >66% of Upper Limit of Normal Range for Serum LDH
Pleural Cholesterol >55-60 mg/dL
Pleural/Serum Cholesterol Ratio: elevated
Serum-Pleural Albumin Gradient (SPAG) <1.2 g/dl
If the Pleural Fluid Clinically Appears to Be a Transudate and SPAG >1.2, But Light’s Criteria Suggest an Exudate, the Fluid Can Be Assumed to be a Transudate (Albumin is Lower Molecular Weight than Other Proteins and Crosses Capillary Walls More Readily)
Post-Cardiac Surgery Pleural Effusion (see Post-Cardiac Surgery Pleural Effusion, [[Post-Cardiac Surgery Pleural Effusion]]): 50% of cases are hemorrhagic (Chest, 2009) [MEDLINE]
Pus in the pleural space (with or without a positive gram stain)
Pleural Fluid pH
Routine measurement of pleural pH is recommended only in patients with parapneumonic effusions
Technique: collect blood aerobically in heparinized syringe (similar to ABG collection technique)
Sample left open to air (or with sir bubble in the syringe) can have increase in pH due to loss of CO2 into the air
In general, pleural fluid pH correlates with pleural fluid glucose [Potts DE, Willcox MA, Good JTJ, et al: The acidosis of low-glucose pleural effusions. Am Rev Respir Dis 1978; 117:665-671]
Pleural Fluid Cholesterol
Cholesterol is always very high (>200 mg/dL) in Pseudochylothorax
Pleural Fluid Triglycerides
Trig >100 mg/dL: diagnoses chylothorax (chylothorax fluid clears with addition of ethyl ether)
Trig <50 mg/dL: rules out chylothorax
Trig 50-110 mg/dL: perform lipoprotein analysis for chylomicrons to diagnose chylothorax
Typically increased in pleural fluid within 2 hrs of perforation
Pancreatico-Pleural Fistula: pleural fluid amylase is typically very high (>4000 IU/mL)
Malignancy
Approximately 10% of malignant effusions (due to non-pancreatic malignancy) have mildly elevated pleural amylase
Pleural amylase in these cases is of the salivary isoenzyme type
Pleural Fluid Adenosine Deaminase (ADA)
ADA is released from activated lymphocytes
ADA is >45 U/mL in almost all patients with TB pleuritis
However, elevated ADA can also seen in empyema, lymphoma, leukemia, and RA
ADA may be less useful in Asians
ADA is a sensitive marker for TB pleuritis even in the setting of HIV [Baba K, Hoosen AA, Langeland N, et al: Adenosine deaminase activity is a sensitive marker for the diagnosis of tuberculous pleuritis in patients with very low CD4 counts. PLoS One 2008; 3:e2788]
Pleural Fluid ANA
Pleural Fluid ANA: positive at >1:40 titer
High Negative Predictive Value for Diagnosis of Lupus Pleuritis: positive pleural ANA is present in all cases of lupus pleuritis -> negative pleural ANA suggest that lupus pleuritis is not the etiology of the effusion
Low Specificity for Diagnosis of Lupus Pleuritis: positive pleural ANA can also be seen in 11-27% of other effusions -> importantly, neither the titer of ANA, ratio between pleural and serum ANA, nor pattern of staining increase the specificity of the pleural ANA test for lupus pleuritis
Pleural/serum ANA ratio is >1 (with pleural ANA >1:160) in SLE
Pleural Fluid RF
Pleural titer >1:320 is seen in RA (this is usually higher than the concomitant serum titer)
However, these tests have low sensitivity, often comparable to that of cultures alone
References
Baba K, Hoosen AA, Langeland N, et al: Adenosine deaminase activity is a sensitive marker for the diagnosis of tuberculous pleuritis in patients with very low CD4 counts. PLoS One 2008; 3:e2788