

Contraindications to Noninvasive Positive-Pressure Ventilation (NIPPV) (Am J Respir Crit Care Med, 2001) [MEDLINE]
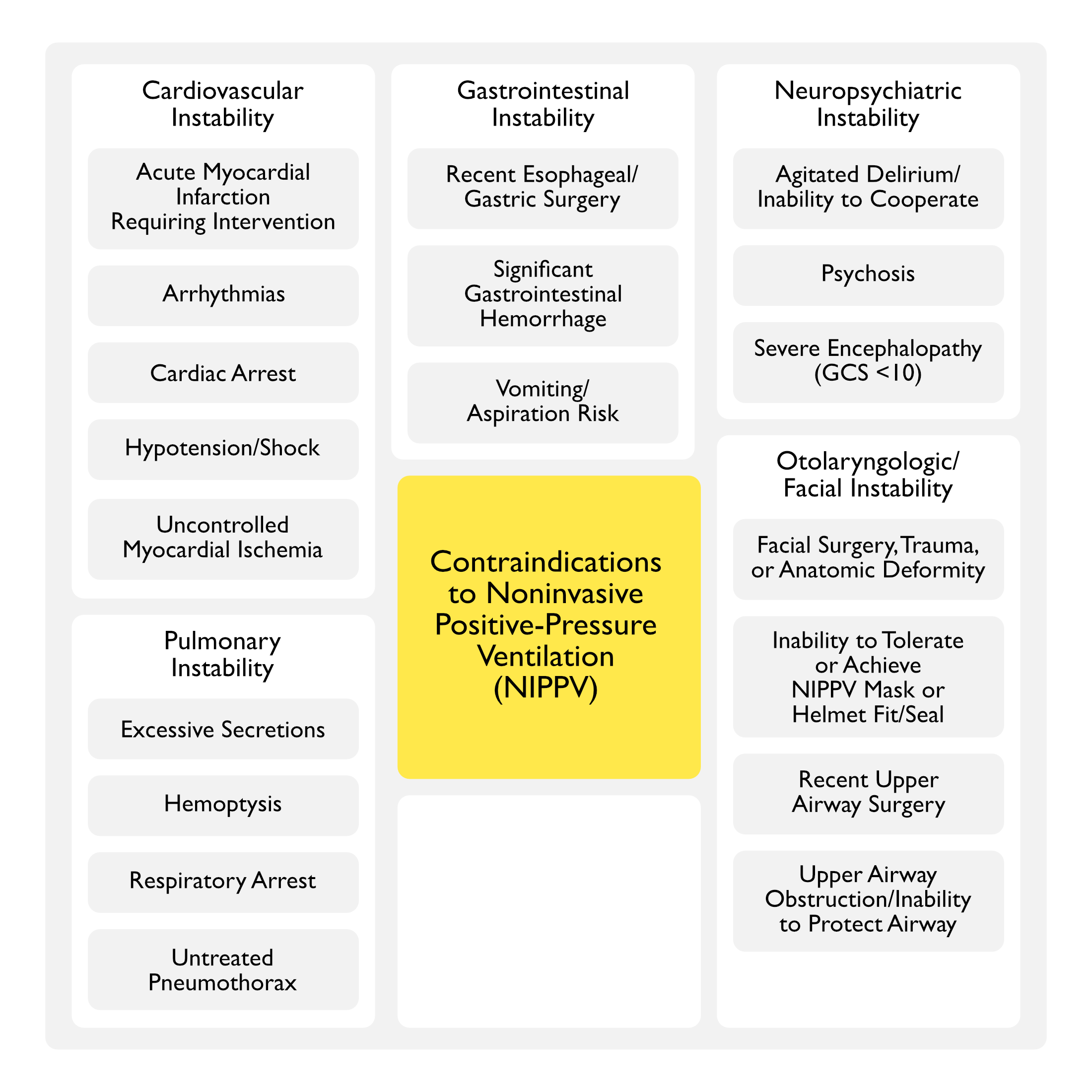
Cardiovascular Instability
- Acute Myocardial Infarction Requiring Intervention (see Coronary Artery Disease)
- Arrhythmias
- Cardiac Arrest (see Cardiac Arrest)
- Hypotension/Shock (see Hypotension)
- Uncontrolled Myocardial Ischemia (see Coronary Artery Disease)
Gastrointestinal Instability
- Recent Esophageal/Gastric Surgery (see Esophagectomy and Gastrectomy)
- Significant Gastrointestinal Hemorrhage (see Gastrointestinal Hemorrhage)
- Vomiting/Aspiration Risk (see Nausea and Vomiting)
Neuropsychiatric Instability
- Agitated Delirium/Inability to Cooperate (see Delirium)
- Psychosis (see Psychosis)
- Severe Encephalopathy (GCS <10) (see Obtundation/Coma)
Otolaryngologic/Facial Instability
- Facial Surgery, Trauma, or Anatomic Deformity
- Inability to Achieve NIPPV Mask/Helmet Fit/Seal
- Recent Upper Airway Surgery
- Upper Airway Obstruction/Inability to Protect Airway (see Obstructive Lung Disease)
Pulmonary Instability
- Excessive Secretions
- Hemoptysis (see Hemoptysis)
- Respiratory Arrest
- Untreated Pneumothorax (see Pneumothorax)

Physiology
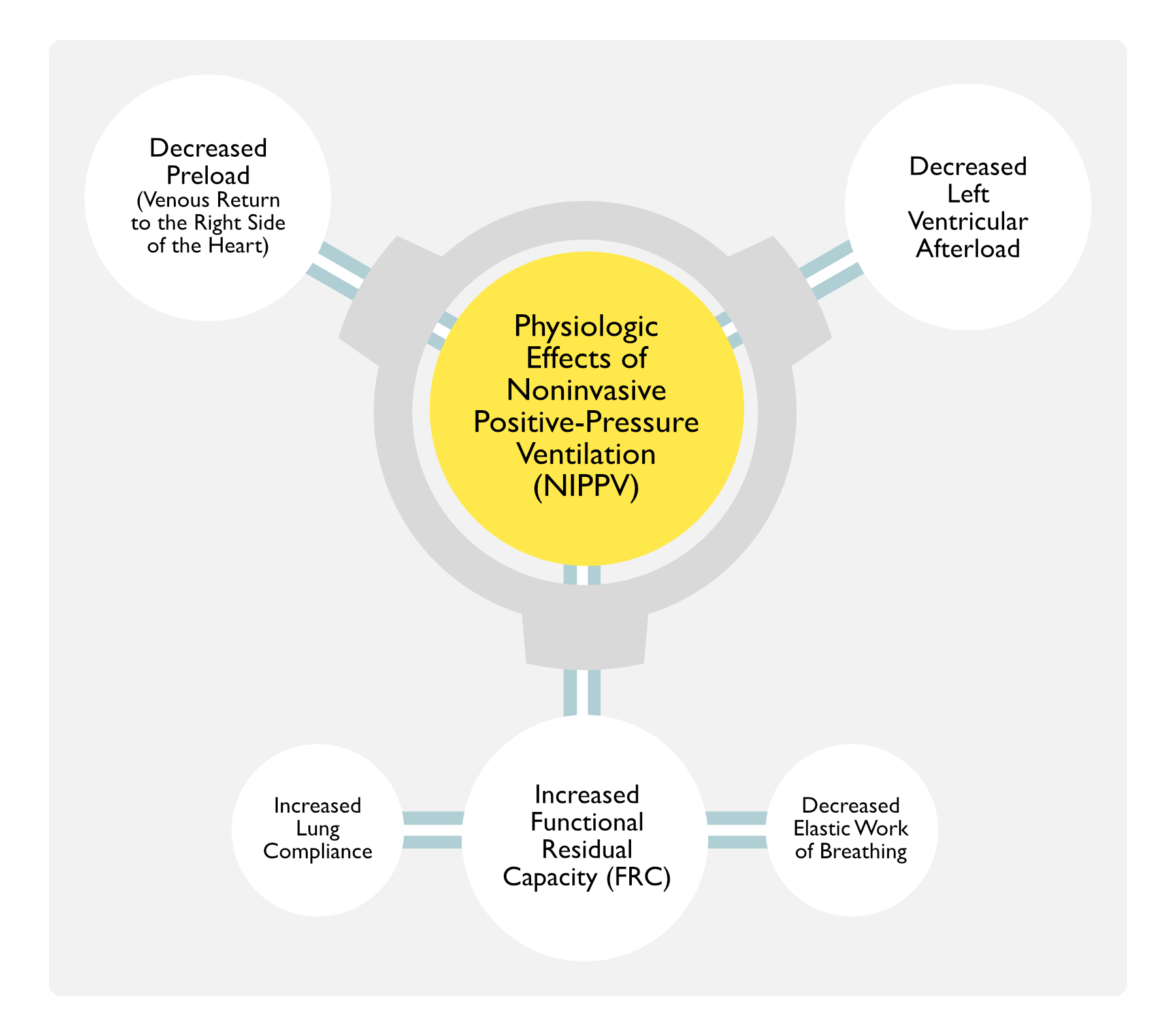
Physiologic Effects of Noninvasive Positive Pressure Ventilation (NIPPV)
- Increased Functional Residual Capacity (FRC)
- Resulting in Increased Lung Compliance and Decreased the Elastic Work of Breathing, Culminating in More Efficient Ventilation
- Decreased Preload (Venous Return to the Right Side of the Heart) (NEJM, 1991) [MEDLINE]
- Decreased Left Ventricular Afterload (NEJM, 1991) [MEDLINE]
Technique
Timing of Initiation of Noninvasive Positive Pressure Ventilation (NIPPV)
Pre-Hospital Initiation of Noninvasive Positive-Pressure Ventilation
- Systematic Review and Meta-Analysis of Pre-Hospital Initiation of NIPPV in Adults with Severe Respiratory Distress (Ann Emerg Med, 2014) [MEDLINE]: n = 632 (7 trials)
- Pre-Hospital Initiation of NIPPV for Respiratory Distress Decreased In-Hospital Mortality Rate (Relative Risk 0.58) and Need for Invasive Mechanical Ventilation (Relative Risk 0.37)
- There was No Difference in ICU Length of Stay or Hospital Length of Stay
- Systematic Review, Network Meta-Analysis, and Individual Patient Data Meta-Analysis of Pre-Hospital NIPPV in Acute Respiratory Failure (Acad Emerg Med, 2014) [MEDLINE]: n = 8 trials
- Pre-Hospital CPAP Decreased the Mortality Rate and Intubation Rate
- Pre-Hospital BiPAP Effect on Mortality Rate and Intubation was Uncertain

Hospital Initiation of Noninvasive Positive-Pressure Ventilation
- Initiate NIPPV as Soon as Possible
- Early Application of NIPPV Improved the Arterial Blood Gas and Decreased the Need for Intubation in Acute COPD Exacerbation (Chin Med J, 2005) [MEDLINE]
Site of Initiation of Noninvasive Positive Pressure Ventilation (NIPPV)
General Comments
- Clinical Monitoring of NIPPV is Best Accomplished in the ICU Setting (or Emergency Department)
- Some Facilities Allow for Short Duration Use of NIPPV in Other Less Monitored Settings
Clinical Efficacy
- Italian Study of the Use of NIPPV on Hospital Wards (Crit Care Med, 2016) [MEDLINE]
- Use of NIPPV on Hospital Wards Has Been Reported to Have Similar Mortality Rates as Those in the ICU
- Good Prognostic Factors
- Postoperative Respiratory Failure
- Poor Prognostic Factors
- Pneumonia with Hematologic Malignancy
- Solid Malignancy
- Do Not Resuscitate Status
- Italian Observational Study of Noninvasive Positive-Pressure Ventilation in Pneumonia Outside of the ICU (Eur J Intern Med, 2018) [MEDLINE]
- Outside of the ICU Setting, CPAP was Predominantly Used for Hypoxemic (Non-Hypercapnic) Respiratory Failure, While NIPPV was Predominantly Used for Hypoxemic, Hypercapnic Respiratory Failure
- Do Not Intubate (DNI) Order and Charlson Comorbidity Index (CCI) ≥3 were Independent Risk Factors for In-Hospital Mortality
Mask Interface
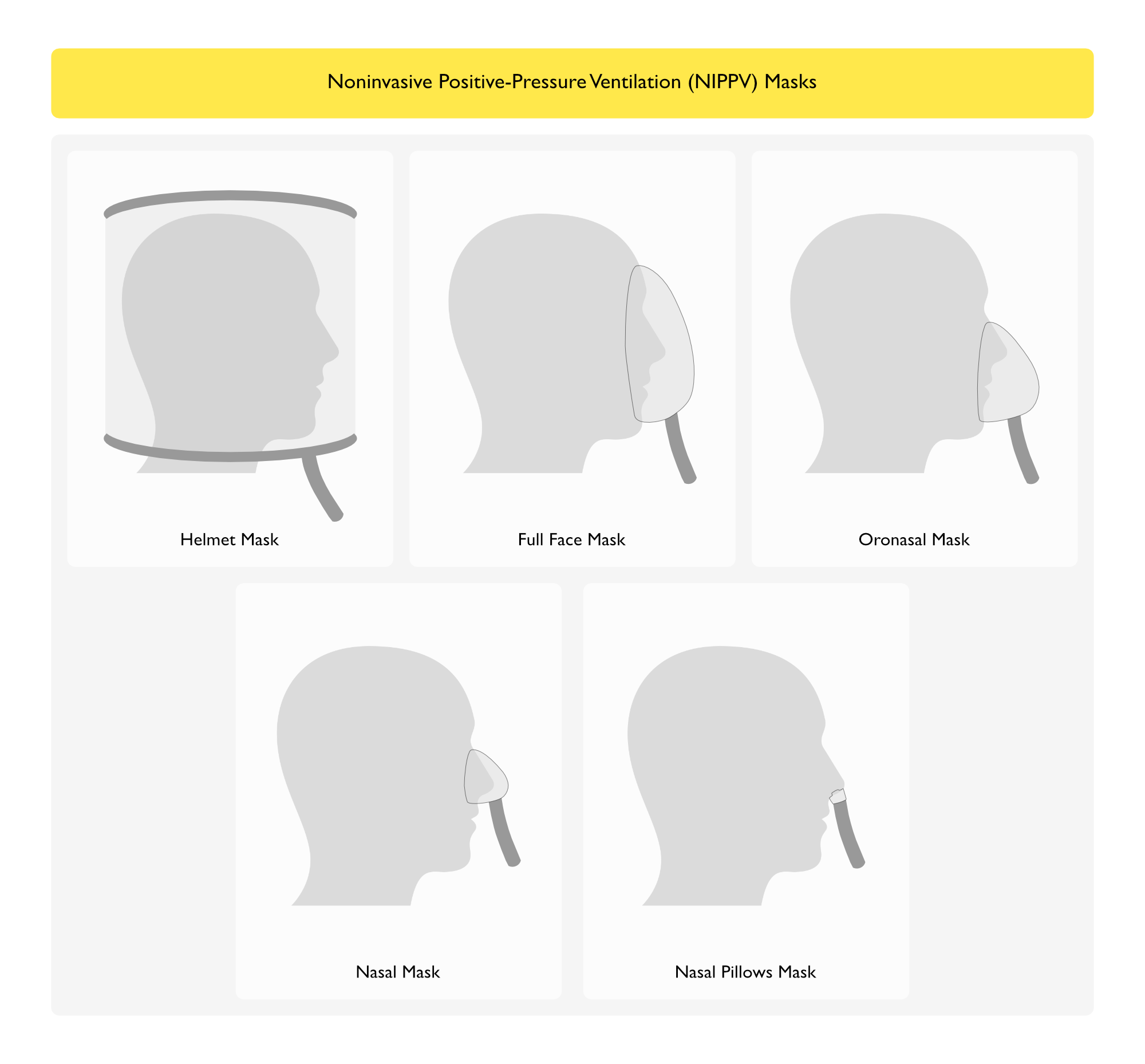
Types of Masks
- Oronasal Mask (Encompassing Both the Nose and Mouth)
- Most Commonly Used Initial Mask
- Advantages
- Higher Level of Ventilation than a Nasal Mask (Due to Less Oral Air Leak)
- Disadvantages
- Carbon Dioxide Rebreathing
- More Difficult to Monitor for Vomiting/Aspiration (as Compared to a Nasal Mask)
- Nasal Mask
- Advantages
- Produces Less Claustrophobia and a Higher Level of Comfort (as Compared to an Oronasal Mask): this may be beneficial for longer-term use
- Allows Expectoration
- Allows Speech
- Allows Oral Intake
- Easier Monitoring for Vomiting/Aspiration (as Compared to a Oronasal Mask)
- Disadvantages
- Air Leak: chin strap may be used to decrease the oral leak
- Due to Significant Airflow Resistance of Nasal Passages, the Selected Inspiratory Pressure Needs to Account for This When a Nasal Mask is Used
- Advantages
- Nasal Pillows
- Advantages
- Produces Less Claustrophobia and a Higher Level of Comfort (as Compared to an Oronasal Mask): this may be beneficial for longer-term use
- Allows Expectoration
- Allows Speech
- Allows Oral Intake
- Easier Monitoring for Vomiting/Aspiration (as Compared to a Oronasal Mask)
- Disadvantages
- Air Leak: chin strap may be used to decrease the oral leak
- Due to Significant Airflow Resistance of Nasal Passages, the Selected Inspiratory Pressure Needs to Account for This When a Nasal Mask is Used
- Advantages
- Full Face Mask (Encompassing the Nose, Mouth, and Eyes)
- Full Face Mask May Be Useful in Some Cases if the Oronasal Mask Fails (Crit Care Med, 2013) [MEDLINE]
- Helmet
- Helmet May Be Used in Some Cases if the Oronasal Mask Fails
- Advantages
- Allows Speech
- Allows Drinking Through a Straw
- Allows Reading
- Disadvantages
- Carbon Dioxide Rebreathing (Which is Typically Compensated for by Increased Flow Rates) (Intensive Care Med, 2003) [MEDLINE] (Intensive Care Med, 2008) [MEDLINE]
- High Noise Level (Which May Cause Hearing Damage) (Intensive Care Med, 2004) [MEDLINE]
- Patient-Ventilator Dyssynchrony (Due to Delayed Triggering and Cycling) (Intensive Care Med, 2007) [MEDLINE]
- Less Relief of Inspiratory Effort
Clinical Efficacy
- Prospective Case Series of Nasal NIPPV for Hypercapnic Respiratory Failure Due to COPD (Crit Care Med, 1994) [MEDLINE]
- Patients who Failed Nasal NIPPV Had a Higher Severity of Illness and They were Unable to Minimize Oral Leak (Due to of Lack of Teeth, Secretions, or Respiratory Pattern) and Coordinate with the Ventilator
- Randomized Trial of NIPPV Masks in Chronic Hypercapnic Respiratory Failure (Crit Care Med, 2000) [MEDLINE]
- Overall, the Nasal Mask was Better Tolerated than the Nasal Plugs or Full-Face Mask
- pCO2 was Lower with the Full-Face Mask or Nasal Plugs than with the Nasal Mask
- Minute Ventilation was Higher (Due to increased Tidal Volume) with the Full-Face Mask than with the Nasal Mask
- No Differences were Observed in Tolerance to Ventilation, ABG, or Breathing Pattern Using Assist Control or Pressure-Assisted Modes
- Prospective Pilot Study of Helmet NIPPV (Crit Care Med, 2002) [MEDLINE]
- Helmet Interface Had Better Tolerance and Fewer Complications (Skin Necrosis, Gastric Distension, Eye Irritation) than Face Mask NIPPV
- Multicenter Randomized Trial of Helmet NIPPV (Intensive Care Med, 2002) [MEDLINE]
- Helmet Interface Decreased Skin Breakdown and Increased Patient Comfort, as Compared to Face Mask NIPPV
- Study of Helmet NIPPV in COPD Exacerbation (Anesthesiology, 2004) [MEDLINE]
- Helmet was Less Efficient at Decreasing pCO2, as Compared to Face Mask NIPPV in COPD Exacerbation
- Randomized Trial of NIPPV Masks in Acute Hypercapnic Respiratory Failure (Crit Care Med, 2009) [MEDLINE]
- Mask Failure (Need for Mask Change Due to Oral Air Leak) Occurred More Commonly in the Nasal Mask Group, as Compared to the Face Mask Group
- Face Mask Group Had Higher Lower Respiratory Comfort and Higher Complications, as Compared to the Nasal Mask Group
- Trial of Rescue Therapy Switching to a Total Face Mask in “Do Not Intubate” Patients with Acute Respiratory Failure (Crit Care Med, 2013) [MEDLINE]
- In Patients with Acute Hypercapnic Respiratory Failure, for Whom Escalation to Intubation Would Be Deemed Inappropriate, Switching to a Total Face Mask Can Be Used as Last Resort Therapy When Face Mask-Delivered NIPPV Has Failed to Reverse the Acute Respiratory Failure (Especially in the Setting of Prolonged NIPPV with Risk of Facial Pressure Sores)
- Trial Comparing Helmet vs Face Mask NIPPV in ARDS (JAMA, 2016) [MEDLINE]: single-center randomized, controlled trial
- Helmet NIPPV Decreased the Intubation Rate and 90-Day Mortality in ARDS, as Compared to Face Mask NIPPV
- Helmet NIPPV Increased Ventilator-Free Days, as Compared to Face Mask NIPPV
Ventilator Mode and Settings
Ventilator Modes
- General Comments
- Use of a Standard ICU Ventilator or Bilevel-Type Ventilator is Strongly Recommended Over a Portable Ventilator for Several Reasons
- Ability to Monitor Closely (with Alarms) to Rapidly Detect a Mask Leak or Patient Disconnection
- Ability to Deliver a Precise and High Oxygen Concentration
- Ability to Deliver Time-Limited Pressure Support Modes of Ventilation
- Separate Inspiratory and Expiratory Tubing to Minimize Carbon Dioxide Rebreathing
- Use of a Standard ICU Ventilator or Bilevel-Type Ventilator is Strongly Recommended Over a Portable Ventilator for Several Reasons
- Assist Control (AC)
- Advantage
- Guarantees a Minimum Minute Ventilation
- Advantage
- Bilevel Positive Airway Pressure (BPAP)
- Commonly Used
- Related Terminology
- “BiPAP”: specific type of BPAP delivered by a portable ventilator manufactured by the Respironics Corporation
- “BIPAP”: specific type of BPAP delivered by a ventilator made by the Drager Medical Company
- Bilevel-Type NIPPV Ventilator with an Oxygen Blender and Waveform Display
- Examples
- Philips Respironics V60 Ventilator
- Examples
- Conventional Ventilator
- Continuous Positive Airway Pressure (CPAP)
- Commonly Used to Treat Cardiogenic Pulmonary Edema
- Pressure Support Ventilation (PSV)
- Advantages
- Maximizes Patient Comfort
- Maximizes Patient-Ventilator Synchrony
- Advantages
- Proportional Assist Ventilation (PAV)
Clinical Efficacy-Chronic Obstructive Pulmonary Disease (COPD) Exacerbation
- Assist Control (AC) NIPPV Has Been Demonstrated to Decrease the Work of Breathing More than Pressure Support Ventilation (PSV) NIPPV, But PSV is Better Tolerated (Intensive Care Med, 1993) [MEDLINE] (Chest, 1997) [MEDLINE]
- Bilevel Positive Airway Pressure (BPAP) Has Been Demonstrated to Result in Improved Gas Exchange and Work of Breathing, as Compared tp Pressure Support Ventilation (PSV) (Am J Respir Crit Care Med, 1994) [MEDLINE] (Chest, 2000) [MEDLINE]
Clinical Efficacy-Cardiogenic Pulmonary Edema
- Meta-Analysis of NIPPV Modalities in Cardiogenic Pulmonary Edema (Lancet, 2006) [MEDLINE]: n = 23 trials
- Bilevel Positive Airway Pressure (BPAP) and Continuous Positive Airway Pressure (CPAP) Had Similar Mortality Rates
- Prospective Randomized Trial of NIPPV Modalities in Cardiogenic Pulmonary Edema (Intensive Care Med, 2011) [MEDLINE]
- Continuous Positive Airway Pressure (CPAP) and Pressure Support Ventilation (PSV) Had Similar Mortality Rates and Intubation Rates
- Pressure Support Ventilation (PSV) Resulted in More Rapid Resolution of Respiratory Distress
Clinical Efficacy-Mixed Etiologies of Acute Respiratory Failure
- Pressure Support Ventilation (PSV) NIPPV and Proportional Assist Ventilation (PAV) NIPPV Have Been Demonstrated to Be Comparable (Am J Respir Crit Care Med, 2001) [MEDLINE] (Crit Care Med, 2002) [MEDLINE] (Intensive Care Med, 2003) [MEDLINE]
Clinical Efficacy-Tidal Volume
- Study of Tidal Volume on NIPPV in De Novo Acute Hypoxemic Respiratory Failure (Crit Care Med, 2016) [MEDLINE]: n = 62 (82% of cases were due to pneumonia)
- Rationale: a low-moderate expired tidal volume can be difficult to achieve during NIPPV for de novo acute hypoxemic respiratory failure (i.e. respiratory failure not due to chronic lung disease or heart failure)
- A Low Exhaled Tidal Volume is Almost Impossible to Achieve in Patients Receiving NIPPV for De Novo Acute Hypoxemic Respiratory Failure
- High Exhaled Tidal Volume is Independently Associated with NIPPV Failure
- In Patients with Moderate-Severe Hypoxemia, Exhaled Tidal Volume >9.5 mL/kg Predicted Body Weight Accurately Predicted NIPPV Failure
General Recommendations
- The Best Clinical Outcomes are Achieved in NIPPV with the Use of Assist Control (AC), Pressure Support Ventilation (PSV), or Bilevel Positive Airway Pressure (BPAP) Modes
Settings for Bilevel Positive Airway Pressure (BPAP)
- Initial Settings
- Start with Low Pressures (Typically 8/4 cm H2O or 10/4 cm H2O) to Allow the Patient to Acclimate and Then Subsequently Gradually Ramp the Pressure Up to Optimize Lung Volumes
- Inspiratory Flow Rate
- Adjust the “Rise Time” (Inspiratory Flow Rate) to Patient Comfort
- COPD Patients Typically Prefer Shorter Inspiratory Times (Higher Inspiratory Flow Rates), Which Allow for Longer Expiratory Times
- Backup Respiratory Rate
- Can Be Used
- Oxygen Delivery
- Bilevel Devices without an Oxygen Blender: maximum FIO2 that can be achieved is 45-50%
- Bilevel Device with an Oxygen Blender: necessary when higher FIO2 is required
- Humidification
- Humidifier is Routinely Used to Decrease Work of Breathing and Enhance Patient Tolerance
- Humidification is Recommended Since NIPPV Delivers Air with Low Relative Humidity, Especially with a High Inspiratory Pressure (Respir Care, 2007) [MEDLINE]
- Humidifier is Routinely Used to Decrease Work of Breathing and Enhance Patient Tolerance
Monitoring of Noninvasive Positive Pressure Ventilation (NIPPV)
General Comments
- Clinical Monitoring is Crucial (Especially Early in the Application of NIPPV)
Monitor for Air Leaks
- Proper Mask Fit and Monitoring for Air Leaks from the Mask are Critical
Monitor Patient Tolerance
- Routine Monitoring of Patient Tolerance and Providing Encouragement/Assurance to the Patient are Critical to Ensure Patient Compliance
Gas Exchange Monitoring
- Serial Arterial Blood Gas (ABG) (see Arterial Blood Gas): routinely used
- Continuous Pulse Oximetry (see Pulse Oximetry): routinely used
- Continuous Capnography (see Capnography): may be used
Sedation
General Comments
- Sedation May Be Used Judiciously to Facilitate Patient Cooperation with NIPPV
- Sedation with Non-Respiratory Depressants May Be Useful
- Dexmedetomidine (Precedex) (see Dexmedetomidine)
- Sedation with Non-Respiratory Depressants May Be Useful
Clinical Efficacy
- Randomized Trial of Dexmedetomidine vs Midazolam in Acute Respiratory Failure (Due to Acute COPD Exacerbation) Treated with NIPPV (Curr Ther Res Clin Exp, 2010) [MEDLINE]
- Dexmedetomidine and Midazolam are Both Effective Sedatives for Patients Requiring NIPPV
- Dexmedetomidine Required Fewer Adjustments in Dosing to Maintain Adequate Sedation, as Compared with Midazolam
- Study of Dexmedetomidine vs Midazolam in Acute Respiratory Failure (Due to Cardiogenic Pulmonary Edema) Treated with NIPPV (Intern Med, 2012) [MEDLINE]
- In Acute Cardiogenic Pulmonary Edema, Dexmedetomidine Resulted in Improved Level of Sedation, Shortened the Duration of Mechanical Ventilation, Shortened the Length of ICU Stay, and Decreased the Risk of Nosocomial Pneumonia, as Compared to Midazolam
- Small Randomized Pilot Study of Dexmedetomidine During Noninvasive Ventilation for Patients with Acute Respiratory Failure (Chest, 2014) [MEDLINE]
- Initiating Dexmedetomidine Soon After NIPPV for Acute Respiratory Failure Neither Improves Tolerance Nor Maintains Sedation at a Desired Goal
- Spanish Study of Use of Sedatives and Analgesics During NIPPV (Intensive Care Med, 2015) [MEDLINE]
- Slightly <20% of Patients Received Analgesics or Sedatives During NIPPV and These Individually Did Not Impact Outcome
- Simultaneous Use of Analgesics and Sedatives During NIPPV was Associated with an Increased NIPPV Failure Rate
- Study of Sedation for Treatment of Agitation During Noninvasive Positive-Pressure Ventilation (BMC Pulm Med, 2015) [MEDLINE]
- Using RASS Score, Sedation During NIPPV in Proficient Hospitals May Be Favorably Used to Avoid NIPPV Failure in Agitated Patients, Even in Those Patients with Diseases with Poor Evidence for the Usefulness of NIPPV
Predictors of Successful Noninvasive Positive-Pressure Ventilation (NIPPV)
Clinical Efficacy
- Study of Factors Associated with NIPPV Success
- Illness-Related Factors
- Presence of COPD or Cardiogenic Pulmonary Edema
- Lack of Pneumonia or ARDS
- APACHE II Score <29 (X)
- Minimal Secretions
- Adequate Neurologic Status (Glasgow Coma at least 15) (X)
- Patient-Related Factors
- Dentate + Compatible Facial Structure with Minimal Air Leakage Around Mask
- Patient Ability to Tolerate
- Clinical Assessment-Related Factors
- RR < 30 (X)
- pH > 7.30 (X)
- pO2/FIO2 Ratio >146 After First Hour (In Hypoxemic Respiratory Failure)
- Good Synchronization with NIPPV
- Good Response to NIPPV Within First 1-2 Hrs
- Decreased RR
- Improved pO2 + Decreased pCO2
- Improved pH
- (X) Presence of All Four in COPD Patients at Baseline: 94% Success Rate
- (X) Presence of All Four After 2 Hrs: 97% Success Rate
- Illness-Related Factors
- Prospective Study of Factors Predicting Success of NIPPV in Patients with Respiratory Failure Associated with Chronic Obstructive Pulmonary Disease (Chest, 2000) [MEDLINE]
- Good Level of Consciousness at the Beginning of NIPPV and Improvement in pH, pCO2, and Level of Consciousness Values After 1 hr of NIPPV were Associated with Successful Responses to NIPPV in COPD Patients with Acute Hypercapnic Respiratory Failure
- Predictors of Success in Noninvasive Positive-Pressure Ventilation (International Consensus Conferences in Intensive Care Medicine: Noninvasive Positive-Pressure Ventilation in Acute Respiratory Failure, 2001) (Am J Respir Crit Care Med, 2001) [MEDLINE]
- Ability to Cooperate
- Better Neurologic Function
- Improvement in Gas Exchange, Heart Rate, and Respiratory Rate within 2 hrs After Starting NIPPV
- Less Air Leak (with Intact Dentition, etc)
- Lower Acuity of Illness (Lower APACHE Score)
- Moderate Acidemia (pH 7.10-7.35)
- Moderate Hypercapnia (pCO2 45-92 mm Hg)
- Younger Age
- Study of Risk Factors for NIPPV Failure in COPD (Eur Respir J, 2005) [MEDLINE]
- Risk Factors for NIPPV Failure (at Admission)
- APACHE II ≥29: odds ratio 3.30
- GCS ≤11: odds ratio 4.40
- GCS 12-14: odds ratio 2.29
- pH <7.25: odds ratio 1.97
- pH 7.25-7.29: odds ratio 1.08
- RR ≥35: odds ratio 2.66
- RR 30-34: odds ratio 1.83
- Risk Factors for NIPPV Failure (at 2 hrs)
- APACHE II ≥29: odds ratio 4.79
- GCS ≤11: odds ratio 5.16
- GCS 12-14: odds ratio 1.93
- pH <7.25: odds ratio 21.02
- pH 7.25-7.29: odds ratio 2.92
- RR ≥35: odds ratio 4.95
- RR 30-34: odds ratio 2.67
- Risk Factors for NIPPV Failure (at Admission)
- Study of Factors Predicting Failure of Noninvasive Positive-Pressure Ventilation (Med Intensiva, 2016) [MEDLINE]: n = 410
- Overall Failure Rate was 50% (with Overall Mortality Rate of 33%)
- Failure Rate in Patients with Hypoxemic Respiratory Failure: 74%
- Failure Rate in Postextubation Respiratory Failure: 54%
- Failure Rate in Hypercapnic Respiratory Failure without COPD: 31%
- Failure Rate in Respiratory Failure Due to COPD Exacerbation: 27%
- Failure Rate in Respiratory Failure Due to Cardiogenic Pulmonary Edema: 21%
- Factors Associated with Failure
- Etiology of Respiratory Failure
- Serum Bilirubin at the Start
- APACHE II Score
- Radiological Findings
- Need for Sedation to Tolerate NIPPV
- Change in Level of Consciousness
- pO2/FIO2 Ratio
- Respiratory Rate
- Heart Rate
- Overall Failure Rate was 50% (with Overall Mortality Rate of 33%)
- Post-Hoc Analysis of Randomized Trial Studying the Predictors of Successful Noninvasive Positive-Pressure Ventilation Treatment for Acute Respiratory Failure (Crit Care Med, 2018) [MEDLINE]
- Respiratory Rate ≥30 Breaths/min (One Hour After Treatment Initiation) was a Predictor of Intubation When Using Standard Oxygen Therapy (Odds Ratio, 2.76; 95% CI, 1.13-6.75; p = 0.03), But Not When Using High-Flow Nasal Cannula or Noninvasive Positive-Pressure Ventilation
- pO2/FIO2 Ratio <200 mm Hg and a Tidal Volume >9 mL/kg Predicted Body Weight (One Hour After Treatment Initiation) were the Two Strongest Predictors of Intubation When Using Noninvasive Positive-Pressure Ventilation (Adjusted Odds Ratio, 4.26; 95% CI, 1.62-11.16; p = 0.003 and Adjusted Odds Ratio, 3.14; 95% CI, 1.22-8.06; p = 0.02, Respectively)
- Tidal Volume >9 mL/kg Predicted Body Weight Predicted 90-Day Mortality
Impact of Noninvasive Positive-Pressure Ventilation (NIPPV) on Infection Rates
Clinical Efficacy
- Study of NIPPV Impact on Complication Rates in the Treatment of Acute Hypoxemic Respiratory Failure (NEJM, 1998) [MEDLINE]
- NIPPV Decreased the Pneumonia and Sinusitis Complication Rates, as Compared to Invasive Mechanical Ventilation
- NIPPV Decreased the Duration of Ventilation and the ICU Length of Stay, as Compared to Invasive Mechanical Ventilation
- French Case Control Study of NIPPV on Nosocomial Infection Rates in the Treatment of Respiratory Failure Due to COPD Exacerbation or Cardiogenic Pulmonary Edema (JAMA, 2000) [MEDLINE]
- Use of NIPPV Instead of Invasive Mechanical Ventilation was Associated with a Decreased Risk of Nosocomial Infections, Decreased Antibiotic Use, Decreased Length of ICU Stay, and Decreased Mortality Rate
Adverse Effects/Complications
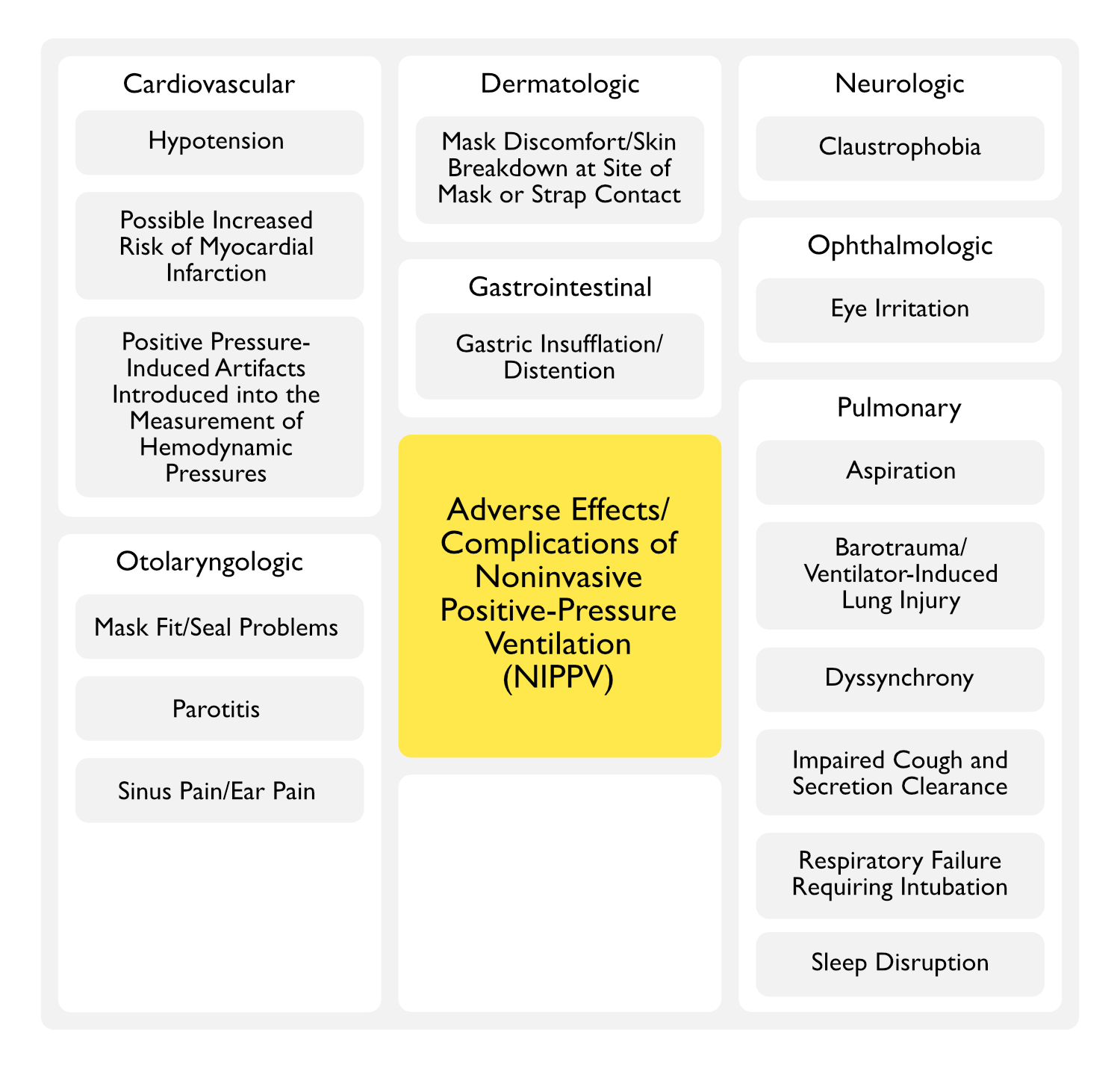
Cardiovascular Adverse Effects/Complications
Hypotension
- Mechanisms
- Positive-Pressure Ventilation Increases Intrathoracic and Right Atrial Pressure, Resulting in Decreased Venous Return to the Right Side of the Heart and, Consequently, Decreased Right Ventricular Cardiac Output
- Effect of Positive-Pressure Ventilation is Accentuated by the Presence of Hypovolemia (Anesthesiology, 1975) [MEDLINE]
- Positive-Pressure Ventilation Causes Alveolar Inflation with Compression of the Pulmonary Vascular Bed, Resulting in Increased Pulmonary Vascular Resistance (PVR), and Consequently, Decreased Right Ventricular Output (Crit Care Med, 2010) [MEDLINE]
- Passive Leg Raise Maneuver Has Been Demonstrated to Increase Central Blood Volume and Mitigate this Effect (Crit Care Med, 2010) [MEDLINE]
- Positive-Pressure Ventilation Causes Alveolar Inflation with Compression of the Pulmonary Vascular Bed, Resulting in Increased Pulmonary Vascular Resistance (PVR, and Consequently, Shift of the Intraventricular Septum Toward the Left (with Impaired Diastolic Left Ventricular Filling), Culminating in Decreased Left Ventricular Cardiac Output
- Interaction Between Airway Pressures and Thoracic Structures
- Hemodynamic Effects of Positive-Pressure Ventilation are Due to Transmission of the Airway Pressure to the Adjacent Thoracic Structures
- Transmission is Greatest When There is Low Chest Wall Compliance (Due to Fibrothorax, etc) or High Chest Wall Compliance (Due to COPD, etc)
- Transmission is Least When There is High Chest Wall Compliance (Due to Sternotomy, etc) or Low Lung Compliance (Due to ARDS, Pulmonary Edema, etc)
- Hemodynamic Effects of Positive-Pressure Ventilation are Due to Transmission of the Airway Pressure to the Adjacent Thoracic Structures
- Positive-Pressure Ventilation Increases Intrathoracic and Right Atrial Pressure, Resulting in Decreased Venous Return to the Right Side of the Heart and, Consequently, Decreased Right Ventricular Cardiac Output
Increased Risk of Myocardial Infarction (see Coronary Artery Disease)
- Epidemiology
- Meta-Analysis of CPAP and BPAP NIPPV in Cardiogenic Pulmonary Edema (Crit Care, 2006) [MEDLINE]
- Based on Limited Data, There was an Insignificant Trend Toward an Increase in New Acute Myocardial Infarction in Patients Treated with BiPAP (RR 2.10, 95% CI 0.91-4.84; P = 0.08; I2 = 25.3%)
- Meta-Analysis of NIPPV in Cardiogenic Pulmonary Edema (Lancet, 2006) [MEDLINE]
- Weak Evidence of an Increased Incidence of New Acute Myocardial Infarction with BPAP vs CPAP was Observed (1.49, 0.92-2.42, p=0.11)
- Meta-Analysis of CPAP and BPAP NIPPV in Cardiogenic Pulmonary Edema (Crit Care, 2006) [MEDLINE]
Positive Pressure-Induced Artifacts Introduced into the Measurement of Hemodynamic Pressures
- Mechanism
- Airway Pressure Transmission to Thoracic Structures, Resulting in Artifactual Elevation of Hemodynamic Pressure Measurements
- This Occurs Because (by Convention) Most Hemodynamic Pressures (Such as the Pulmonary Capillary Wedge Pressure) are Assessed at End-Expiration (When Positive End-Expiratory Pressure/PEEP is the Predominant Determinant of Airway Pressure)
- Airway Pressure Transmission to Thoracic Structures, Resulting in Artifactual Elevation of Hemodynamic Pressure Measurements
- Clinical
- Positive End-Expiratory Pressure (PEEP) Artifactually Elevates the Pulmonary Capillary Wedge Pressure (PCWP)
- Correction of PEEP Consists of Subtracting Approximately One Half of the PEEP Level from the PCWP if the Lung Compliance is Normal (or One Quarter of the PEEP Level if the Lung Compliance is Decreased) (J Appl Physiol Respir Environ Exerc Physiol, 1982) [MEDLINE]
- Correction of the PCWP for the Amount of PEEP Can More Accurately Done Using the Index of Transmission (Crit Care Med, 2000) [MEDLINE]
- Index of Transmission = (End Inspiratory PCWP – End Expiratory PCWP) / (Plateau Pressure – Total PEEP)
- Transmural PCWP = End-Expiratory PCWP – (Index of Transmission x Total PEEP)
- This Estimation Can Be Unreliable if the Respiratory Variation of the PCWP is Greater than that of the Pulmonary Arterial Pressure Tracing
- Positive End-Expiratory Pressure (PEEP) May Also Artifactually Elevate the Central Venous Pressure (CVP)
- Positive End-Expiratory Pressure (PEEP) Artifactually Elevates the Pulmonary Capillary Wedge Pressure (PCWP)
Dermatologic Adverse Effects/Complications
Mask Discomfort/Skin Breakdown at Site of Mask or Strap Contact
- Epidemiology
- Common with Prolonged Use of NIPPV
Gastrointestinal Adverse Effects/Complications
Gastric Insufflation/Distention
- Epidemiology
- Frequent
- Clinical
- Not Typically Severe
- Use of Nasogastric Tube is Usually Not Required and, if Used, May Worsen the Mask Seal
- Not Typically Severe
Ophthalmologic Adverse Effects/Complications
Eye Irritation
- Epidemiology
- May Occur with Use of a Full Face Mask
Otolaryngologic Adverse Effects/Complications
Mask Fit/Seal Problems
- Modest Mask Leaks are Common
- Air Leak from Mask May Require Mask Adjustment
Parotitis (see Parotitis)
- Epidemiology
- Has Been Reported (J Intensive Care Med, 2016) [MEDLINE]
Sinus Pain/Ear Pain
- Physiology
- Due to Excessive Air Pressure
Pulmonary Adverse Effects/Complications
Aspiration (see Aspiration Pneumonia)
- Epidemiology
- May Occur
Barotrauma and Ventilator-Induced Lung Injury
- Epidemiology
- Noninvasive Positive-Pressure Ventilation Probably Has a Similar Mechanism of Barotrauma as Invasive Mechanical Ventilation, But the Rate of Barotrauma is Lower (Due to Use of Lower Pressures) (Rev Bras Ter Intensiva, 2008) [MEDLINE]
- Physiology
- Mechanical Ventilation Itself Increases the Risk of Barotrauma by Causing Alveolar Overdistention, Resulting in Alveolar Rupture
- Anatomic Path of Air Dissection
- Air from Torn Alveolus Enters the Perivascular Interstitium, Dissecting Along the Bronchovascular Sheath into the Pulmonary Hila and Subsequently Into the Mediastinum, Causing Pneumomediastinum (in the Setting of Blunt Trauma to the Lung, This Tracking of Air Has Been Termed the “Macklin Effect”) (see Pneumomediastinum) (Chest, 2001) [MEDLINE]
- From Pneumomediastinum, Air Can Dissect Upward into the Soft Tissues of the Neck (Causing Subcutaneous Emphysema), into the Pleural Spaces (Causing Pneumothorax on Either Side), Inferiorly into the Peritoneum (Causing Pneumoperitoneum), or Rarely, into the Pericardium (Causing Pneumopericardium)
- Anatomic Path of Air Dissection
- Ventilator-Induced Lung Injury Has Been Observed in Moderate-Severe ARDS Patients Treated with NIPPV (Ann Transl Med, 2017) [MEDLINE]
- Low Tidal Volumes May Be Difficult to Achieve in Acute Hypoxemic Respiratory Failure Treated with NIPPV (Crit Care Med, 2016) [MEDLINE]
- In Patients with Moderate-Severe Hypoxemia, Tidal Volume >9.5 mL/kg Predicted Body Weight Accurately Predicted NIPPV Failure: high tidal volume was independently associated with NIPPV failure
- Mechanical Ventilation Itself Increases the Risk of Barotrauma by Causing Alveolar Overdistention, Resulting in Alveolar Rupture
- Clinical
- Clinical Worsening of Lung Injury
- Pneumothorax (see Pneumothorax)
Dyssynchrony
- Epidemiology
- Dyssynchrony is Common in NIPPV (Intensive Care Med, 2009) [MEDLINE]
- Physiology
- Leak is Believed to Play a Major Role in the Development of Dyssynchrony (Intensive Care Med, 2009)[MEDLINE]
- Treatment
- Pressure Support Ventilation (PSV) is Believed to Decrease Dyssynchrony (and Bilevel Positive Airway Pressure/BPAP Likely is Similar)
- Proportional Assist Ventilation (PAV) May Be an Alternative in a Patient Who Experiences Dyssynchrony on BPAP or PSV
- While Proportional Assist Ventilation (PAV) is More Comfortable and Better Tolerated than Pressure Support Ventilation (PSV), There Have Been No Demonstrated Differences in Mortality or Intubation Rates (Am J Respir Crit Care Med, 2001) [MEDLINE] (Crit Care Med, 2002) [MEDLINE] (Intensive Care Med, 2003) [MEDLINE]
- If an Air Leak is Present, a Time-Cycled Expiratory Trigger is Superior to a Flow-Cycled Expiratory Trigger (in Terms of Synchrony) (Intensive Care Med, 1999) [MEDLINE]: only specific ventilators are capable of delivering time-limited pressure support ventilation (PSV)
Impaired Cough and Secretion Clearance
- Expectoration May Be Facilitated by Using a Nasal Interface (Instead of a Full Face Mask, Oronasal Mask, etc)
- Early Bronchoscopy May Be Used in Some Cases to Clear Airway Secretions (Crit Care, 2010) [MEDLINE]
- In Patients with COPD Exacerbation or Bronchiectasis, High-frequency Chest Wall Oscillation or Intrapulmonary Percussive Ventilation (IPV) May Be Used to Mobilize Secretions (Crit Care, 2005) [MEDLINE] (Crit Care Med, 2006) [MEDLINE]
- In Patient with Neuromuscular Disease, But Intact Bulbar Function, NIPPV with Mechanical Cough Assistance (In-Exsufflator) or Manual Cough Assistance (Breath-Stacking Technique) May Be Useful to Enhance Secretion Clearance
Respiratory Failure Requiring Intubation
- Clinical Efficacy
- Systematic Review of Noninvasive Positive Pressure Ventilation in COPD Exacerbation (Cochrane Database Syst Rev, 2004) [MEDLINE]
- Noninvasive Positive Pressure Ventilation Has Clinical Benefit (Decreased Mortality Rate, Decreased Need for Intubation, Decreased Complications Associated with Treatment, and Decreased Length of Hospital Stay), in Addition to Usual Care, in the Management of COPD Exacerbation
- Intubation Rate with Noninvasive Positive Pressure Ventilation Had a Relative Risk of 0.41 (95% CI 0.33, 0.53), as Compared to Standard Care
- Meta-Analysis Noninvasive Positive Pressure Ventilation in Acute Cardiogenic Pulmonary Edema (Ann Intern Med, 2010) [MEDLINE]
- Continuous Positive Airway Pressure Decreased the Mortality Rate with a Relative Risk of 0.64 (95% CI, 0.44 to 0.92)
- Continuous Positive Airway Pressure Decreased the Intubation Rate with a Relative Risk of 0.44 (95% CI, 0.32 to 0.60]
- Single-Center Retrospective Study of Failure of Noninvasive Positive-Pressure Ventilation in Acute Respiratory Failure (Ann Intensive Care, 2015) [MEDLINE]
- In a Propensity-Adjusted Multivariate Regression Analysis (Corrected for Presence of Pneumonia or ARDS and Adjusted for Factors Known to Increase Intubation Complications), NIPPV Failure Resulted in Increased Odds of a Composite Complication of Intubation (2.20; CI 1.14-4.25)
- When a Composite Complication Occurred, the Unadjusted Odds of Death in the ICU were 1.79 (95% CI 1.03-3.12)
- Systematic Review of Noninvasive Positive Pressure Ventilation in COPD Exacerbation (Cochrane Database Syst Rev, 2004) [MEDLINE]
Sleep Disruption
- Recommendations (Society of Critical Care Medicine Clinical Practice Guidelines for the Prevention and Management of Pain, Agitation/Sedation, Delirium, Immobility, and Sleep Disruption in Adult Patients in the ICU) (Crit Care Med, 2018) [MEDLINE]
- In Patient Requiring Noninvasive Positive-Pressure Ventilation (NIPPV), Either an NIPPV-Dedicated Ventilator or a Standard ICU Ventilator May Be Used for Critically Ill Adults to Improve Sleep (Conditional Recommendation, Very Low Quality of Evidence)
References
Contraindications
- Noninvasive positive-pressure ventilation to treat hypercapnic coma secondary to respiratory failure. Chest. 2005;127(3):952 [MEDLINE]
- Noninvasive positive pressure ventilation in patients with acute exacerbations of COPD and varying levels of consciousness. Chest. 2005;128(3):1657 [MEDLINE]
Physiology
- Treatment of severe cardiogenic pulmonary edema with continuous positive airway pressure delivered by face mask. N Engl J Med. 1991;325(26):1825 [MEDLINE]
Technique
General
- Noninvasive ventilation in critically ill patients. Crit Care Clin 2015; 31:435 – 457 [MEDLINE]
- Noninvasive ventilation in acute respiratory failure: which recipe for success? Eur Respir Rev. 2018 Jul 11;27(149). pii: 180029. doi: 10.1183/16000617.0029-2018 [MEDLINE]
Timing of Initiation
- Early use of non-invasive positive pressure ventilation for acute exacerbations of chronic obstructive pulmonary disease: a multicentre randomized controlled trial. Chin Med J (Engl). 2005;118(24):2034 [MEDLINE]
- Time of non-invasive ventilation. Intensive Care Med. 2006;32(3):361 [MEDLINE]
- Use and outcomes of noninvasive positive pressure ventilation in acute care hospitals in Massachusetts. Chest. 2014;145(5):964 [MEDLINE]
- Prehospital noninvasive ventilation for acute respiratory failure: systematic review, network meta-analysis, and individual patient data meta-analysis. Acad Emerg Med. 2014;21(9):960 [MEDLINE]
- Effect of out-of-hospital noninvasive positive-pressure support ventilation in adult patients with severe respiratory distress: a systematic review and meta-analysis. Ann Emerg Med. 2014 May;63(5):600-607.e1 [MEDLINE]
Site of Initiation
- Long-Term Survival Rate in Patients With Acute Respiratory Failure Treated With Noninvasive Ventilation in Ordinary Wards. Crit Care Med. 2016;44(12):2139 [MEDLINE]
- Non-invasive positive pressure ventilation in pneumonia outside Intensive Care Unit: An Italian multicenter observational study. Eur J Intern Med. 2018 Oct 24. pii: S0953-6205(18)30388-1. doi: 10.1016/j.ejim.2018.09.025 [MEDLINE]
Mask Interface
- Nasal mechanical ventilation for hypercapnic respiratory failure in chronic obstructive pulmonary disease: determinants of success and failure. Crit Care Med. 1994;22(8):1253 [MEDLINE]
- Physiologic evaluation of noninvasive mechanical ventilation delivered with three types of masks in patients with chronic hypercapnic respiratory failure. Crit Care Med. 2000;28(6):1785 [MEDLINE]
- Evaluation of patient skin breakdown and comfort with a new face mask for non-invasive ventilation: a multi-center study. Intensive Care Med. 2002;28(3):278 [MEDLINE]
- New treatment of acute hypoxemic respiratory failure: noninvasive pressure support ventilation delivered by helmet–a pilot controlled trial. Crit Care Med. 2002;30(3):602 [MEDLINE]
- Head helmet versus face mask for non-invasive continuous positive airway pressure: a physiological study. Intensive Care Med. 2003;29(10):1680 [MEDLINE]
- Noise exposure during noninvasive ventilation with a helmet, a nasal mask, and a facial mask. Intensive Care Med. 2004;30(9):1755 [MEDLINE]
- Noninvasive positive pressure ventilation using a helmet in patients with acute exacerbation of chronic obstructive pulmonary disease: a feasibility study. Anesthesiology. 2004;100(1):16 [MEDLINE]
- Non-invasive ventilation in chronic obstructive pulmonary disease patients: helmet versus facial mask. Intensive Care Med. 2007;33(1):74 [MEDLINE]
- Helmet ventilation and carbon dioxide rebreathing: effects of adding a leak at the helmet ports. Intensive Care Med. 2008;34(8):1461 [MEDLINE]
- Interface strategy during noninvasive positive pressure ventilation for hypercapnic acute respiratory failure. Crit Care Med. 2009 Jan;37(1):124-31 [MEDLINE]
- Rescue therapy by switching to total face mask after failure of face mask-delivered noninvasive ventilation in do-not-intubate patients in acute respiratory failure. Crit Care Med. 2013;41(2):481 [MEDLINE]
- Effect of Noninvasive Ventilation Delivered by Helmet vs Face Mask on the Rate of Endotracheal Intubation in Patients With Acute Respiratory Distress Syndrome: A Randomized Clinical Trial. JAMA. 2016;315(22):2435 [MEDLINE]
Ventilator Modes
- Non-invasive modalities of positive pressure ventilation improve the outcome of acute exacerbations in COLD patients. Intensive Care Med. 1993;19(8):450 [MEDLINE]
- Physiologic effects of positive end-expiratory pressure and mask pressure support during exacerbations of chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 1994;149(5):1069 [MEDLINE]
- Comparative physiologic effects of noninvasive assist-control and pressure support ventilation in acute hypercapnic respiratory failure. Chest. 1997;111(6):1639 [MEDLINE]
- Predicting the result of noninvasive ventilation in severe acute exacerbations of patients with chronic airflow limitation. Chest. 2000;117(3):828 [MEDLINE]
- Noninvasive proportional assist ventilation for acute respiratory insufficiency. Comparison with pressure support ventilation. Am J Respir Crit Care Med. 2001;164(9):1606 [MEDLINE]
- Noninvasive proportional assist ventilation compared with noninvasive pressure support ventilation in hypercapnic acute respiratory failure. Crit Care Med. 2002;30(2):323 [MEDLINE]
- Noninvasive pressure support versus proportional assist ventilation in acute respiratory failure. Intensive Care Med. 2003;29(7):1126 [MEDLINE]
- New things are not always Better: proportional assist ventilation vs. pressure support ventilation. Intensive Care Med. 2003;29(7):1038 [MEDLINE]
- Effect of non-invasive positive pressure ventilation (NIPPV) on mortality in patients with acute cardiogenic pulmonary oedema: a meta-analysis. Lancet. 2006 Apr 8;367(9517):1155-63 [MEDLINE]
- Non-invasive pressure support ventilation and CPAP in cardiogenic pulmonary edema: a multicenter randomized study in the emergency department. Intensive Care Med. 2011;37(2):249 [MEDLINE]
- Clinical Practice Guidelines for the Prevention and Management of Pain, Agitation/Sedation, Delirium, Immobility, and Sleep Disruption in Adult Patients in the ICU. Crit Care Med. 2018;46(9):e825 [MEDLINE]
Tidal Volume
- Failure of Noninvasive Ventilation for De Novo Acute Hypoxemic Respiratory Failure: Role of Tidal Volume. Crit Care Med. 2016 Feb;44(2):282-90. doi: 10.1097/CCM.0000000000001379 [MEDLINE]
Settings
- Efficacy of a heated passover humidifier during noninvasive ventilation: a bench study. Respir Care. 2007;52(1):38 [MEDLINE]
Sedation
- Sedation during noninvasive mechanical ventilation with dexmedetomidine or midazolam: A randomized, double-blind, prospective study. Curr Ther Res Clin Exp. 2010 Jun;71(3):141-53. doi: 10.1016/j.curtheres.2010.06.003 [MEDLINE]
- Dexmedetomidine versus midazolam for the sedation of patients with non-invasive ventilation failure. Intern Med. 2012;51(17):2299-305 [MEDLINE]
- Efficacy and safety of early dexmedetomidine during noninvasive ventilation for patients with acute respiratory failure: a randomized, double-blind, placebo-controlled pilot study. Chest. 2014 Jun;145(6):1204-1212. doi: 10.1378/chest.13-1448 [MEDLINE]
- Impact of sedation and analgesia during noninvasive positive pressure ventilation on outcome: a marginal structural model causal analysis. Intensive Care Med. 2015 Sep;41(9):1586-600 [MEDLINE]
- Role of sedation for agitated patients undergoing noninvasive ventilation: clinical practice in a tertiary referral hospital. BMC Pulm Med. 2015 Jul 13;15:71. doi: 10.1186/s12890-015-0072-5 [MEDLINE]
Predictors of Successful Noninvasive Positive-Pressure Ventilation
- Predicting the result of noninvasive ventilation in severe acute exacerbations of patients with chronic airflow limitation. Chest. 2000;117(3):828 [MEDLINE]
- A chart of failure risk for noninvasive ventilation in patients with COPD exacerbation. Eur Respir J. 2005 Feb;25(2):348-55 [MEDLINE]
- Effectiveness and predictors of failure of noninvasive mechanical ventilation in acute respiratory failure. Med Intensiva. 2016 Jan-Feb;40(1):9-17. doi: 10.1016/j.medin.2015.01.007 [MEDLINE]
- Predictors of Intubation in Patients With Acute Hypoxemic Respiratory Failure Treated With a Noninvasive Oxygenation Strategy. Crit Care Med. 2018 Feb;46(2):208-215. doi: 10.1097/CCM.0000000000002818 [MEDLINE]
Impact of Noninvasive Positive-Pressure Ventilation on Infection
- A comparison of noninvasive positive-pressure ventilation and conventional mechanical ventilation in patients with acute respiratory failure. N Engl J Med. 1998;339(7):429 [MEDLINE]
- Association of noninvasive ventilation with nosocomial infections and survival in critically ill patients. JAMA. 2000;284(18):2361 [MEDLINE]
Adverse Effects/Complications
Increased Risk of Myocardial Infarction
- Effect of non-invasive positive pressure ventilation (NIPPV) on mortality in patients with acute cardiogenic pulmonary oedema: a meta-analysis. Lancet. 2006;367(9517):1155 [MEDLINE]
- A comparison of continuous and bi-level positive airway pressure non-invasive ventilation in patients with acute cardiogenic pulmonary oedema: a meta-analysis. Crit Care. 2006;10(2):R49 [MEDLINE]
Otolaryngologic
- Acute Parotitis as a Complication of Noninvasive Ventilation. J Intensive Care Med. 2016 Sep;31(8):561-3 [MEDLINE]
Barotrauma
- The Macklin effect: a frequent etiology for pneumomediastinum in severe blunt chest trauma. Chest. 2001 Aug;120(2):543-7 [MEDLINE]
- Relationship between ventilatory settings and barotrauma in the acute respiratory distress syndrome. Intensive Care Med. 2002;28(4):406 [MEDLINE]
- Pneumothorax associated with long-term non-invasive positive pressure ventilation in Duchenne muscular dystrophy. Neuromuscul Disord. 2004 Jun;14(6):353-5 [MEDLINE]
- Pneumothorax: an important complication of non-invasive ventilation in neuromuscular disease. Neuromuscul Disord. 2004 Jun;14(6):351-2 [MEDLINE]
- Occurrence of pneumothorax during noninvasive positive pressure ventilation through a helmet. J Clin Anesth. 2007 Dec;19(8):632-5 [MEDLINE]
- [Evaluation of the incidence of pneumothorax and background of patients with pneumothorax during noninvasive positive pressure ventilation]. Nihon Kokyuki Gakkai Zasshi. 2008 Nov;46(11):870-4 [MEDLINE]
- Benefits and complications of noninvasive mechanical ventilation for acute exacerbation of chronic obstructive pulmonary disease. Rev Bras Ter Intensiva. 2008 Jun;20(2):184-9 [MEDLINE]
- Failure of noninvasive ventilation for de novo acute hypoxemic respiratory failure: role of tidal volume. Crit Care Med 2016; 44: 282–290 [MEDLINE]
- High-flow nasal oxygen therapy and noninvasive ventilation in the management of acute hypoxemic respiratory failure. Ann Transl Med 2017; 5: 297 [MEDLINE]
Dyssynchrony
- Patient-ventilator asynchrony during noninvasive ventilation: the role of expiratory trigger. Intensive Care Med. 1999;25(7):662 [MEDLINE]
- NIPPV: patient-ventilator synchrony, the difference between success and failure? Intensive Care Med. 1999;25(7):645 [MEDLINE]
- Patient-ventilator asynchrony during non-invasive ventilation for acute respiratory failure: a multicenter study. Intensive Care Med. 2009;35(5):840 [MEDLINE]
Failure of Noninvasive Positive-Pressure Ventilation
- Failed noninvasive positive-pressure ventilation is associated with an increased risk of intubation-related complications. Ann Intensive Care. 2015 Mar 6;5:4. doi: 10.1186/s13613-015-0044-1. eCollection 2015 [MEDLINE]
Impaired Cough and Secretion Clearance
- Intrapulmonary percussive ventilation in acute exacerbations of COPD patients with mild respiratory acidosis: a randomized controlled trial [ISRCTN17802078]. Crit Care 2005; 9: R382–R389 [MEDLINE]
- Intrapulmonary percussive ventilation improves the outcome of patients with acute exacerbation of chronic obstructive pulmonary disease using a helmet. Crit Care Med 2006; 34: 2940–2945 [MEDLINE]
- Early fiberoptic bronchoscopy during non-invasive ventilation in patients with decompensated chronic obstructive pulmonary disease due to community-acquired-pneumonia. Crit Care 2010; 14: R80 [MEDLINE]