

Epidemiology
History
- Noninvasive Positive-Pressure Ventilation (NIPPV) was First Utilized to Treat Acute Respiratory Failure Due to Chronic Obstructive Pulmonary Disease (COPD) in the Late 1980’s (NEJM, 1990) [MEDLINE]
Clinical Utilization
The Utilization of Noninvasive Positive-Pressure Ventilation (NIPPV) Has Increased Dramatically Over the Last 2-3 Decades
- Retrospective Study of the Utilization of NIPPV (from 1999-2003) (J Crit Care, 2008) [MEDLINE]
- Despite Meeting Established Indications (COPD, CHF), NIPPV was Used in Only 33.9% of Qualifying Patients During the Study Period (from 1999-2003)
- Study of Utilization of NIPPV in Eight Acute Care Hospitals in Massachusetts (Chest, 2014) [MEDLINE]
- Of the 548 Ventilator Starts, 61.5% were for Invasive Mechanical Ventilation and 38.5% were for NIPPV
- NIPPV Success Rate (Avoidance of Intubation While on NIPPV or within 48 hrs of Discontinuation) was 73.9
- Hospital Mortality Rate was Higher for Invasive Mechanical Ventilation than for NIPPV (30.3% vs 16.6%)

Indications to Prevent or Treat Acute Respiratory Failure
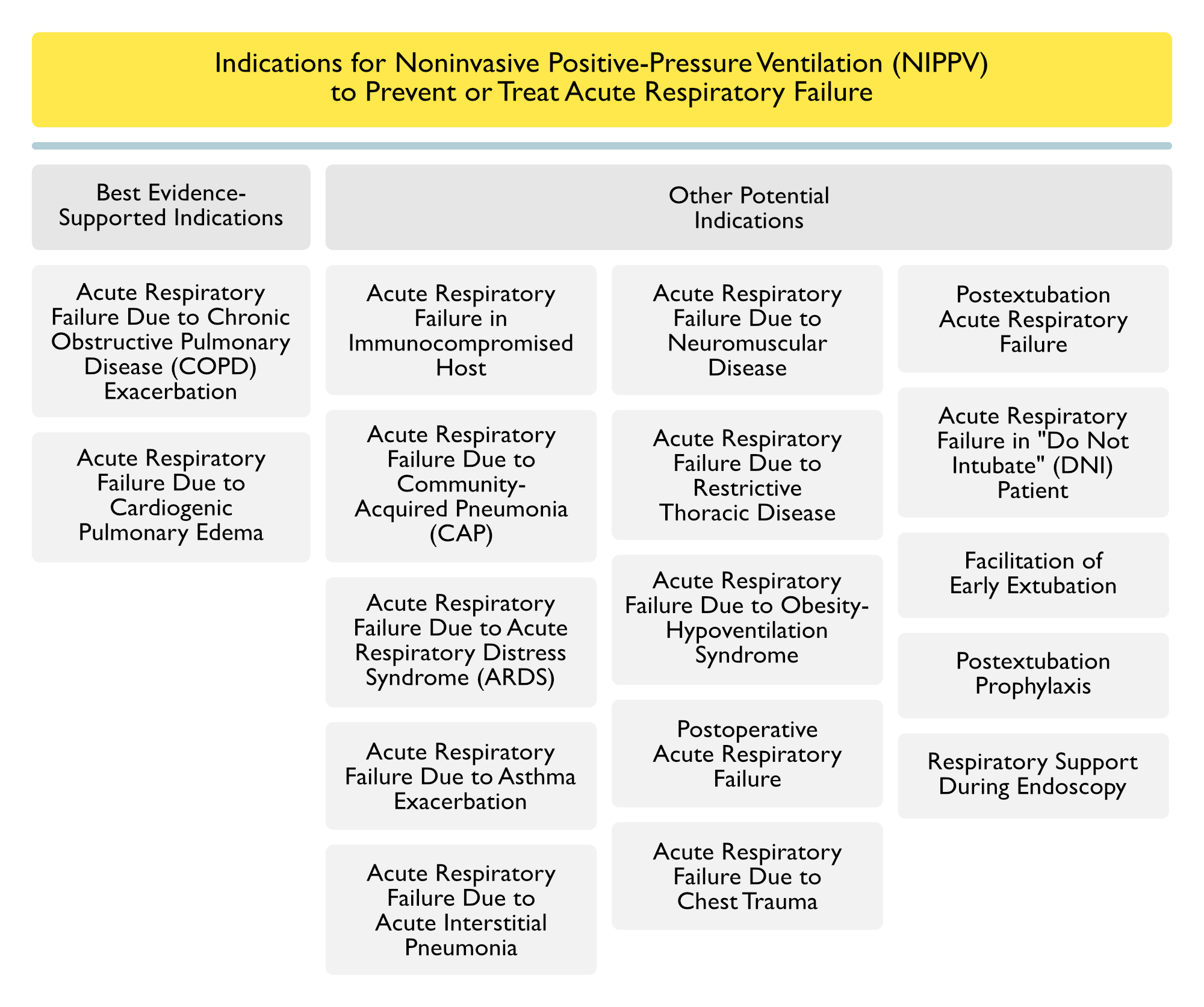
Acute Respiratory Failure Due to Chronic Obstructive Pulmonary Disease (COPD) (see Chronic Obstructive Pulmonary Disease)
Clinical Efficacy-Noninvasive Positive-Pressure Ventilation (NIPPV) in the Treatment of Chronic Obstructive Pulmonary Disease (COPD) Exacerbation
- Matched Case-Control Study of NIPPV in Acute Respiratory Failure in COPD Exacerbation and Cardiogenic Pulmonary Edema (JAMA, 2000) [MEDLINE]
- Use of NIPPV Instead of Mechanical Ventilation was Associated with a Decreased Risk of Nosocomial Infections, Decreased Antibiotic Use, Shorter ICU Length of Stay, and Decreased Mortality Rate
- Retrospective Study of Trends in NIPPV in COPD Exacerbation and Cardiogenic Pulmonary Edema (JAMA, 2003) [MEDLINE]
- Routine Use of NIPPV in Acute Respiratory Failure Due to Acute COPD Exacerbation or Cardiogenic Pulmonary Edema was Associated with Improved Survival and Decreased Risk of Nosocomial Infections (ICU-Acquired Pneumonia, etc)
- Study of Cost-Effectiveness of NIPPV in the Treatment of Acute Respiratory Failure Due to COPD Exacerbation (BMJ, 2003)[MEDLINE]
- NIPPV was Highly Cost Effective and Decreased Both Total Costs and Hospital Mortality Rate
- Systematic Review of NIPPV for Respiratory Failure Due to COPD Exacerbation (Cochrane Database Syst Rev, 2004) [MEDLINE]
- NIPPV Decreased Endotracheal Intubation, Treatment Failure and Mortality Rate in Respiratory Failure Due to COPD Exacerbation
- Systematic Review and Meta-Analysis of Trials Using NIPPV for Prevention or Treatment of Acute Respiratory Failure or as a Tool to Facilitate Early Extubation (Crit Care Med, 2015) [MEDLINE]: n = 78 trials
- Overall (in All Populations), NIPPV Decreased the Mortality Rate (at Longest F/U) with Relative Risk 0.73 (95% CI: 0.66–0.81) (p<0.001): number needed to treat = 19
- Chronic Obstructive Pulmonary Disease (COPD) Exacerbation (see Chronic Obstructive Pulmonary Disease)
- NIPPV Decreased Mortality Rate (at Longest F/U) with Relative Risk 0.56 (95% CI: 0.42-0.74) (p<0.001)
- Analysis of Utilization of NIPPV and Outcome from California State Inpatient Database (Ann Am Thorac Soc, 2017) [MEDLINE]: n = 22,706 hospitalizations with NIPPV as the initial ventilatory strategy
- Approximately 70% of Patients Who Received NIPPV Did Not Have an a Strong Evidence-Based Indication for NIPPV (COPD, CHF) (with Wide Institutional Variation)
- Patients with a Strong Evidence-Based Indication for NIPPV (COPD, CHF) Had a Lower Risk of NIPPV Failure
- Regardless of Admitting Diagnosis, Patients Admitted to Hospitals with Greater Use of Strong Evidence-Based Indications for NIPPV (COPD, CHF) Had a Lower Risk of NIPPV Failure: suggests a “hospital effect” that is synergistic with patient selection
- Even Patients without Strong Evidence-Based Indication for NIPPV (COPD, CHF) Benefited from Admission to Hospitals with Greater Use of Strong Evidence-Based Indications for NIPPV (COPD, CHF)
- Cochrane Database Systematic Review of Noninvasive Positive-Pressure Ventilation for Respiratory Failure Due to COPD Exacerbation (Cochrane Database Syst Rev, 2017) [MEDLINE]
- NIPPV is Beneficial as a First-Line Intervention (in Addition to Usual Care) in Decreasing the Mortality Rate and Intubation Rate in Patients with Hypercapnic Respiratory Failure Due to COPD Exacerbation
- Magnitude of Benefit is Similar for Mild Acidosis (pH 7.30-7.35) and More Severe Acidosis (pH <7.30) When NIPPV is Applied in the ICU or Ward Setting
- NIPPV is Beneficial as a First-Line Intervention (in Addition to Usual Care) in Decreasing the Mortality Rate and Intubation Rate in Patients with Hypercapnic Respiratory Failure Due to COPD Exacerbation

Clinical Efficacy-Combination of HELIOX + Noninvasive Positive-Pressure Ventilation (NIPPV) in the Treatment of Chronic Obstructive Pulmonary Disease (COPD) Exacerbation
- Small Study of Noninvasive Ventilation with Helium-Oxygen in Acute Respiratory Failure Associated with Chronic Obstructive Pulmonary Disease (Am J Respir Crit Care MED, 2000) [MEDLINE]
- HELIOX + NIPPV Decreased Airway Resistance and More Rapidly Improved Gas Exchange in the Setting of COPD Exacerbation
- Prospective Multicenter Trial of Helium-Oxygen vs Air-Oxygen Noninvasive Ventilation in Acute Respiratory Failure Due to Chronic Obstructive Pulmonary Disease (Crit Care Med, 2003) [MEDLINE]
- HELIOX + NIPPV Had No Benefit (in Terms of Intubation Rate, Mortality Rate, or Hospital Length of Stay) over NIPPV Alone in Randomized, Prospective Trial in COPD Exacerbation
- Meta-Analysis of Randomized Trials of HELIOX and Noninvasive Positive-Pressure Ventilation in the Treatment of Respiratory Due to COPD Exacerbation (Ann Intensive Care, 2017) [MEDLINE]
- Compared to Air-Oxygen, HELIOX Does Not Decrease the Rate of NIPPV Failure in Hypercapnic COPD Exacerbation
- HELIOX is Associated with a Lower Incidence of NIPPV-Related Adverse Events and a Shortening of ICU Length of Stay with No Increase in Hospital Cost
Recommendations (ERS/ATS Clinical Practice Guidelines for Noninvasive Ventilation for Respiratory Failure, 2017) (Eur Respir J, 2017) [MEDLINE]
- Background
- Bilevel NIPPV May Theoretically Be Considered in Acute COPD Exacerbation in the Following Clinical Settings
- Prevention of Acute Respiratory Acidosis in the Presence of COPD Exacerbation with Chronically Compensated Hypercapnia (with Normal pH)
- Prevention of Endotracheal Intubation/Invasive Mechanical Ventilation in the Setting of COPD Exacerbation with Respiratory Failure and Mild-Moderate Acidemia
- As an Alternative to Endotracheal Intubation/Invasive Mechanical Ventilation in the Setting of COPD Exacerbation with Respiratory Failure and Severe Acidemia
- As the Only Method of Ventilatory Support in the Setting of COPD Exacerbation with Respiratory Failure in Patients Who are Not Candidates for or Decline Invasive Mechanical Ventilation
- Bilevel NIPPV May Theoretically Be Considered in Acute COPD Exacerbation in the Following Clinical Settings
- Bilevel NIPPV is Not Recommended as a Preventative Treatment in COPD Exacerbation with Hypercapnia without Acidemia (i.e. Chronic Hypercapnia with Metabolic Compensation) (Conditional Recommendation, Low Certainty of Evidence)
- Bilevel NIPPV is Recommended for COPD Exacerbation and Acute/Acute on Chronic Hypoxemic, Hypercapnic Respiratory Failure and Acidemia (pH ≤7.35) (Strong Recommendation, High Certainty of Evidence)
- Bilevel NIPPV Should Be Considered with pH ≤7.35, pCO2 >45 mmHg, and Respiratory Rate >20–24 Despite Standard Medical Therapy
- There is No Lower Limit of pH Below Which a Trial of NIPPV is Contraindicated
- However, the Lower the pH, the Greater the Risk of Failure, Suggesting that the Patient Be Closely Monitored with Rapid Access to Endotracheal Intubation/Invasive Mechanical Ventilation (Should the Need Arise)
- A Trial of Bilevel NIPPV is Recommended in COPD Exacerbation and Acute/Acute on Chronic Respiratory Failure Who May Require Endotracheal Intubation/Invasive Mechanical Ventilation, Unless the Patient is Immediately Deteriorating (Strong Recommendation, Moderate Certainty of Evidence)
Recommendations (Japanese Respiratory Society Noninvasive Positive-Pressure Ventilation Guidelines, 2017) (Respir Investig, 2017) [MEDLINE]
- NIPPV Should Be Used for the Management of Acute Respiratory Failure Due to COPD Exacerbation (Level I Evidence, Grade A Recommendation)
- NIPPV is Useful When Weaning Patients with Complications from COPD from Invasive Mechanical Ventilation (Level I Evidence, Grade B Recommendation)
Acute Respiratory Failure Due to Cardiogenic Pulmonary Edema (see Cardiogenic Pulmonary Edema)
Physiology
- In Cardiogenic Pulmonary Edema CPAP NIPPV Improved Lung Compliance, Decreased Lung and Airway Resistance, Decreased Respiratory Muscle Effort, and Decreased Work of Breathing (Am J Respir Crit Care Med, 1997) [MEDLINE]
- CPAP NIPPV Decreased Negative Intrathoracic Pressure Swings, Resulting in Decreased Afterload (with No Increase in Cardiac Index or Stroke Volume) (Am J Respir Crit Care Med, 1997) [MEDLINE]
- However, Mean Transmural Filling Pressures Decreased Significantly with CPAP, Suggesting Improved Cardiac Performance
Clinical Efficacy
- Trial of CPAP in Cardiogenic Pulmonary Edema (NEJM, 1991) [MEDLINE]
- Positive-Pressure Mechanical Ventilation Decreased Venous Return to the Right Side of the Heart and Decreased Left Ventricular Afterload
- Matched Case-Control Study of NIPPV in Acute Respiratory Failure in COPD Exacerbation and Cardiogenic Pulmonary Edema (JAMA, 2000) [MEDLINE]
- Use of NIPPV Instead of Mechanical Ventilation was Associated with a Decreased Risk of Nosocomial Infections, Decreased Antibiotic Use, Shorter ICU Length of Stay, and Decreased Mortality Rate
- Retrospective Study of Trends in NIPPV in COPD Exacerbation and Cardiogenic Pulmonary Edema (JAMA, 2003) [MEDLINE]
- Routine Use of NIPPV in Acute Respiratory Failure Due to Acute COPD Exacerbation or Cardiogenic Pulmonary Edema was Associated with Improved Survival and Decreased Risk of Nosocomial Infections (ICU-Acquired Pneumonia, etc)
- Meta-Analyses/Systematic Reviews Indicated that Both CPAP and NIPPV Decreased Intubation and Mortality Rates (JAMA, 2005) [MEDLINE] (Crit Care, 2006) [MEDLINE] (Ann Emerg Med, 2006) [MEDLINE]
- However, Mortality Rate was Significantly Decreased in Only a Third of These Analyses
- Meta-Analysis of NIPPV in Cardiogenic Pulmonary Edema (Ann Intern Med, 2010) [MEDLINE]
- Continuous Positive Airway Pressure Decreased the Mortality Rate (RR 0.64 [95% CI, 0.44 to 0.92]) and Need for Intubation (RR 0.44 [CI, 0.32 to 0.60]), But Not the Incidence of New Myocardial Infarction (RR 1.07 [CI, 0.84 to 1.37])
- Systematic Review and Meta-Analysis of Trials Using NIPPV for Prevention or Treatment of Acute Respiratory Failure or as a Tool to Facilitate Early Extubation (Crit Care Med, 2015) [MEDLINE]: n = 78 trials
- Overall (in All Populations), NIPPV Decreased the Mortality Rate (at Longest F/U) with Relative Risk 0.73 (95% CI: 0.66–0.81) (p<0.001): number needed to treat = 19
- Congestive Heart Failure (CHF) Exacerbation (see Congestive Heart Failure)
- NIPPV Decreased Mortality Rate (at Longest Follow-Up) with Relative Risk 0.80 (95% CI: 0.65-0.99) (p = 0.04)
- Analysis of Utilization of NIPPV and Outcome from California State Inpatient Database (Ann Am Thorac Soc, 2017) [MEDLINE]: n = 22,706 hospitalizations with NIPPV as the initial ventilatory strategy
- Approximately 70% of Patients Who Received NIPPV Did Not Have an a Strong Evidence-Based Indication for NIPPV (COPD, CHF) (with Wide Institutional Variation)
- Patients with a Strong Evidence-Based Indication for NIPPV (COPD, CHF) Had a Lower Risk of NIPPV Failure
- Regardless of Admitting Diagnosis, Patients Admitted to Hospitals with Greater Use of Strong Evidence-Based Indications for NIPPV (COPD, CHF) Had a Lower Risk of NIPPV Failure: suggests a “hospital effect” that is synergistic with patient selection
- Even Patients without Strong Evidence-Based Indication for NIPPV (COPD, CHF) Benefited from Admission to Hospitals with Greater Use of Strong Evidence-Based Indications for NIPPV (COPD, CHF)
- Systematic Review and Meta-Analysis of NIPPV in the Treatment of Hypoxemic Respiratory Failure (J Crit Care, 2019) [MEDLINE]: n = 9 studies
- NIPPV Decreased Intubation Rate in Immunocompromised Patients (Cancer/Transplant)
- NIPPV Decreased Intubation Rate in Acute Pulmonary Edema
- NIPPV Decreased Intubation Rate in Community-Acquired Pneumonia (CAP)
- Effect of NIPPV in Respiratory Failure Due to Other Etiologies was Unclear
Recommendations (ERS/ATS Clinical Practice Guidelines for Noninvasive Ventilation for Respiratory Failure, 2017) (Eur Respir J, 2017) [MEDLINE]
- Bilevel NIPPV or CPAP is Recommended for Patients with Acute Respiratory Failure Due to Cardiogenic Pulmonary Edema in the Pre-Hospital Setting (Conditional Recommendation, Low Certainty of Evidence)
- Bilevel NIPPV or CPAP is Recommended for Patients with Acute Respiratory Failure Due to Cardiogenic Pulmonary Edema (Strong Recommendation, Moderate Certainty of Evidence)
Recommendations (Japanese Respiratory Society Noninvasive Positive Pressure Ventilation Guidelines, 2017) (Respir Investig, 2017) [MEDLINE]
- NIPPV (Particularly CPAP) Should Be Used as First-Line Treatment in Patients with Acute Cardiogenic Pulmonary Edema (Level I Evidence, Grade A Recommendation)
Acute Respiratory Failure in Immunocompromised Host
Immunocompromised Hosts
- Hematologic Malignancy
- Human Immunodeficiency Virus (HIV)/Acquired Immunodeficiency Syndrome (AIDS) (see Human Immunodeficiency Virus)
- Solid Organ Transplant
- Bone Marrow/Hematopoietic Stem Cell Transplant (HSCT) (see Hematopoietic Stem Cell Transplant)
Clinical Efficacy
- Prospective Randomized Study of NIPPV in Solid Orhan Transplant Patients with Acute Respiratory Failure (JAMA, 2000) [MEDLINE]
- NIPPV Decreased the Intubation Rate and ICU Mortality Rate with Respiratory Failure in Patients with Solid Organ Transplants
- Prospective, Randomized Trial of NIPPV vs Standard Care with Supplemental Oxygen Alone in Immunocompromised Patients with Acute Respiratory Failure (NEJM, 2001) [MEDLINE]
- Early NIPPV Decreased the Intubation Rate and Mortality Rate with Respiratory Failure in Patients with Hematologic Malignancy (Predominantly), Solid Organ Transplant, and AIDS
- Retrospective Study of NIPPV in Patients with Hematologic Malignancy and Respiratory Failure (Crit Care Med, 2008) [MEDLINE]
- Failure of NIPPV Occurred in 50% the Critically Ill Hematologic Malignancy Patients and is Associated with an Increased Mortality Rate
- Predictors of NIPPV Failure
- Respiratory Rate During NIPPV
- Longer Delay Between Admission and NIPPV Initiation
- Need for Vasopressors or Renal Replacement Therapy
- Acute Respiratory Distress Syndrome (ARDS)
- French/Belgian Multicenter Randomized Trial of NIPPV in Immunocompromised Patients with Hypoxemic Acute Respiratory Failure in the ICU (JAMA, 2015) [MEDLINE]: n = 374
- Approximately 84.7% of the Immunocompromised Patients in the Trial Had Hematologic Malignancies or Solid Tumors
- Early NIPPV Did Not Decrease the 28-Day Mortality Rate, as Compared to Oxygen Therapy Alone
- No Differences in Duration of Mechanical Ventilation, ICU-Acquired Infections, ICU Length of Stay, or Hospital Length of Stay
- Systematic Review and Meta-Analysis of NIPPV in the Treatment of Hypoxemic Respiratory Failure (J Crit Care, 2019) [MEDLINE]: n = 9 studies
- NIPPV Decreased Intubation Rate in Immunocompromised Patients (Cancer/Transplant)
- NIPPV Decreased Intubation Rate in Acute Pulmonary Edema
- NIPPV Decreased Intubation Rate in Community-Acquired Pneumonia (CAP)
- Effect of NIPPV in Respiratory Failure Due to Other Etiologies was Unclear
Recommendations (ERS/ATS Clinical Practice Guidelines for Noninvasive Ventilation for Respiratory Failure, 2017) (Eur Respir J, 2017) [MEDLINE]
- Early NIPPV is Recommended for Respiratory Failure in Immunocompromised Hosts (Conditional Recommendation, Moderate Certainty of Evidence)
Recommendations (Japanese Respiratory Society Noninvasive Positive Pressure Ventilation Guidelines, 2017) (Respir Investig, 2017) [MEDLINE]
- NIPPV is Recommended as a First-Line Treatment for the Management of Immunocompromised Patients with Acute Respiratory Failure (Level II Evidence, Grade A Recommendation)
Acute Respiratory Failure Due to Community-Acquired Pneumonia (CAP)/Hospital-Acquired (HAP)/Ventilator-Associated Pneumonia (VAP) (see Community-Acquired Pneumonia and Hospital-Acquired Pneumonia and Ventilator-Associated Pneumonia)
Clinical Efficacy-Pneumonia (see Community-Acquired Pneumonia and Hospital-Acquired Pneumonia and Ventilator-Associated Pneumonia)
- NIPPV Has Been Reported to Both Increase the Mortality Rate or Decrease the Mortality Rate in Pneumonia (Thorax, 1995) [MEDLINE] (Am J Respir Crit Care Med, 1999) [MEDLINE]
- Latter Study Suggests that NIPPV Decreased Mortality Rate in Subset of Patients with COPD with Concomitant Pneumonia
- Systematic Review of NIPPV in Pneumonia (Cochrane Database Syst Rev, 2012) [MEDLINE]
- NIPPV Decreased the ICU Mortality Rate, Intubation Rate, ICU Length of Stay, and Duration of Intubation in Pneumonia
- Systematic Review and Meta-Analysis of Trials Using NIPPV for Prevention or Treatment of Acute Respiratory Failure or as a Tool to Facilitate Early Extubation (Crit Care Med, 2015) [MEDLINE]: n = 78 trials
- Overall (in All Populations), NIPPV Decreased the Mortality Rate (at Longest F/U) with Relative Risk 0.73 (95% CI: 0.66–0.81) (p<0.001): number needed to treat = 19
- Acute Respiratory Failure (Mixed Etiologies)
- NIPPV Decreased Mortality Rate (at Longest F/U) with Relative Risk 0.66 (95% CI: 0.54–0.80) (p<0.001)
- Study of Tidal Volume on NIPPV in De Novo Acute Hypoxemic Respiratory Failure (Crit Care Med, 2016) [MEDLINE]: n = 62 (82% of cases were due to pneumonia)
- Rationale: a low-moderate expired tidal volume can be difficult to achieve during NIPPV for de novo acute hypoxemic respiratory failure (i.e. respiratory failure not due to chronic lung disease or heart failure)
- A Low Exhaled Tidal Volume is Almost Impossible to Achieve in Patients Receiving NIPPV for De Novo Acute Hypoxemic Respiratory Failure
- High Exhaled Tidal Volume is Independently Associated with NIPPV Failure
- In Patients with Moderate-Severe Hypoxemia, Exhaled Tidal Volume >9.5 mL/kg Predicted Body Weight Accurately Predicted NIPPV Failure
- Systematic Review and Meta-Analysis of NIPPV in Acute Hypoxemic (Non-Hypercapnic) Respiratory Failure (Crit Care Med, 2017) [MEDLINE]: analysis excluded chronic obstructive pulmonary disease exacerbation and cardiogenic pulmonary edema patients
- NIPPV Decreased Intubation Rate and Mortality Rate in Acute Hypoxemia (Non-Hypercapnic) Respiratory Failure
- There was InSufficient Evidence to Recommend Bilevel Positive Airway Pressure or Helmet Due to the Limited Number of Trials Available
- Retrospective Review of NIPPV and Mortality in Pneumonia in Medicare Beneficiaries (Age >64 y/o) (Crit Care Med, 2017) [MEDLINE]
- Among Medicare Beneficiaries Hospitalized with Pneumonia Who Received Mechanical Ventilation, NIPPV Use was Not Associated with a Real-World Mortality Benefit (and with Wide Confidence Intervals, May Have Caused Harm)
- Systematic Review and Meta-Analysis of NIPPV in the Treatment of Hypoxemic Respiratory Failure (J Crit Care, 2019) [MEDLINE]: n = 9 studies
- NIPPV Decreased Intubation Rate in Immunocompromised Patients (Cancer/Transplant)
- NIPPV Decreased Intubation Rate in Acute Pulmonary Edema
- NIPPV Decreased Intubation Rate in Community-Acquired Pneumonia (CAP)
- Effect of NIPPV in Respiratory Failure Due to Other Etiologies was Unclear
Clinical Efficacy-Influenza (see Influenza Virus)
- Study of Risk Factors for NIPPV Failure in Patients with Respiratory Failure and Influenza (Respir Care, 2017) [MEDLINE]
- NIPPV Failure Rate was 56.8%
- Acute Physiology and Chronic Health Evaluation II (APACHE II) Score, Sequential Organ Failure Assessment (SOFA) Score, and Infiltrates on the Chest X-Ray were Higher in the NIPPV Failure Group, as Compared to the NIPPV Success Group
- ICU Mortality (38.4% vs 6.3%) was Higher (P < .001) in the NIPPV Failure Group, as Compared to the NIPPV Success Group
- Prospective Observational Study of NIPPV in Respiratory Failure and Influenza (Clin Microbiol Infect, 2013)
- NIPPV Failure Rate was 59.3%
- Success of NIPPV was Independently Associated with <2 Chest X-Ray Quadrant Opacities (OR 3.5) and No Vasopressor Requirement (OR 8.1)
- Among Patients with ≥ Chest X-Ray Quadrant Opacities, a SOFA Score ≤7 was Associated with a Higher Success Rate than SOFA Score >7 (OR 10.7)
Recommendations (ERS/ATS Clinical Practice Guidelines for Noninvasive Ventilation for Respiratory Failure, 2017) (Eur Respir J, 2017) [MEDLINE]
- Given the Uncertainty of Evidence, No Recommendations were Made Regarding the Use of NIPPV in Acute Respiratory Due to Pneumonia and/or Acute Respiratory Distress Syndrome (ARDS)
- Given the Uncertainty of Evidence, No Recommendations were Made Regarding the Use of NIPPV in Acute Respiratory Due to Viral Illness (Such as Influenza)
Recommendations (Japanese Respiratory Society Noninvasive Positive Pressure Ventilation Guidelines, 2017) (Respir Investig, 2017) [MEDLINE]
- The Use of NIPPV is Recommended for Management of Severe Pneumonia in Patients with COPD (Level II Evidence, Grade B Recommendation)
- It Remains Unclear Whether NIPPV is Useful for the Management of Severe Pneumonia in Patients without COPD (Level IV Evidence, Grade C2 Recommendation)
- Except for Mild Cases, NIPPV is Not Recommended for the Management of Severe Pneumonia Following an Influenza Infection (Level IV Evidence, Grade C2 Recommendation)
Acute Respiratory Failure Due to Acute Respiratory Distress Syndrome (ARDS) (see Acute Respiratory Distress Syndrome)
Clinical Efficacy-General
- Systematic Review and Meta-Analysis of Trials Using NIPPV for Prevention or Treatment of Acute Respiratory Failure or as a Tool to Facilitate Early Extubation (Crit Care Med, 2015) [MEDLINE]: n = 78 trials
- Overall (in All Populations), NIPPV Decreased the Mortality Rate (at Longest F/U) with Relative Risk 0.73 (95% CI: 0.66–0.81) (p<0.001): number needed to treat = 19
- Acute Respiratory Failure (Mixed Etiologies)
- NIPPV Decreased Mortality Rate (at Longest F/U) with Relative Risk 0.66 (95% CI: 0.54–0.80) (p<0.001)
- Study of Tidal Volume on NIPPV in De Novo Acute Hypoxemic Respiratory Failure (Crit Care Med, 2016) [MEDLINE]: n = 62 (82% of cases were due to pneumonia)
- Rationale: a low-moderate expired tidal volume can be difficult to achieve during NIPPV for de novo acute hypoxemic respiratory failure (i.e. respiratory failure not due to chronic lung disease or heart failure)
- A Low Exhaled Tidal Volume is Almost Impossible to Achieve in Patients Receiving NIPPV for De Novo Acute Hypoxemic Respiratory Failure
- High Exhaled Tidal Volume is Independently Associated with NIPPV Failure
- In Patients with Moderate-Severe Hypoxemia, Exhaled Tidal Volume >9.5 mL/kg Predicted Body Weight Accurately Predicted NIPPV Failure
- Trial Comparing Helmet vs Face Mask NIPPV in ARDS (JAMA, 2016) [MEDLINE]: single-center randomized, controlled trial
- Helmet NIPPV Decreased the Intubation Rate and 90-Day Mortality in ARDS, as Compared to Face Mask NIPPV
- Helmet NIPPV Increased Ventilator-Free Days, as Compared to Face Mask NIPPV
- NIPPV is Used Commonly in the Treatment of Patients with Respiratory Failure Due to ARDS
- Analysis of NIPPV Use in Patients with ARDS with Data from the LUNG SAFE Study (Am J Respir Crit Care Med, 2017) [MEDLINE]
- NIPPV was Used in 15% of ARDS Cases
- NIPPV was Associated with a Higher ICU Mortality Rate in ARDS Patients with a pO2/FiO2 Ratio <150 mm Hg
- Analysis of NIPPV Use in Patients with ARDS with Data from the LUNG SAFE Study (Am J Respir Crit Care Med, 2017) [MEDLINE]
- Systematic Review and Meta-Analysis Comparing High-Flow Nasal Cannula vs Standard Oxygen vs NIPPV in Acute Respiratory Failure (Chest, 2017) [MEDLINE]
- High-Flow Nasal Cannula and NIPPV Comparably Decreased the Intubation Rate in Acute Respiratory Failure, as Compared to Standard Oxygen Therapy in Acute Respiratory Failure
- Systematic Review and Meta-Analysis of NIPPV in Acute Hypoxemic (Non-Hypercapnic) Respiratory Failure (Crit Care Med, 2017) [MEDLINE]: analysis excluded chronic obstructive pulmonary disease exacerbation and cardiogenic pulmonary edema patients
- NIPPV Decreased Intubation Rate and Mortality Rate in Acute Hypoxemia (Non-Hypercapnic) Respiratory Failure
- There was InSufficient Evidence to Recommend Bilevel Positive Airway Pressure or Helmet Due to the Limited Number of Trials Available
- Meta-Analysis Examining High-Flow Nasal Cannula in Acute Hypoxemic Respiratory Failure (CMAJ, 2017) [MEDLINE]
- The Intubation Rate with High-Flow Nasal Cannula Oxygen was Lower than the Rate with Conventional Oxygen Therapy and Similar to the Rate with NIPPV in Patients with Acute Hypoxemic Respiratory Failure
- Systematic Review and Meta-Analysis of NIPPV in the Treatment of Hypoxemic Respiratory Failure (J Crit Care, 2019) [MEDLINE]: n = 9 studies
- NIPPV Decreased Intubation Rate in Immunocompromised Patients (Cancer/Transplant) with Hypoxemic Respiratory Failure
- NIPPV Decreased Intubation Rate in Acute Pulmonary Edema with Hypoxemic Respiratory Failure
- NIPPV Decreased Intubation Rate in Community-Acquired Pneumonia (CAP) with Hypoxemic Respiratory Failure
- Effect of NIPPV in Hypoxemic Respiratory Failure Due to Other Etiologies was Unclear
- National Cohort Study of Noninvasive Positive-Pressure Ventilation in Acute Respiratory Distress Syndrome (ARDS) (Crit Care Res Pract, 2019) [MEDLINE] NIPPV Success Group Had the Lowest Mortality Rate (4.9% [3.8-6.4]) and the Shortest LOS (7 Days [6.6-7.5])
- NIPPV Failure Rate was 21%
- Sepsis, Pneumonia, and Chronic Liver Disease were Associated with Higher Odds of NIPPV Failure (Adjusted Odds Ratio: 4.47, 2.65, and 2.23, Respectively)
Clinical Efficacy-Coronavirus Disease 2019 (see Coronavirus Disease 2019)
- Italian HENIVOT Trial of Helmet Noninvasive Ventilation vs High-Flow Nasal Cannula Oxygen in Moderate-Severe Acute Hypoxemic Respiratory Failure Due to COVID-19 Virus Infection (JAMA, 2021) [MEDLINE]: n = 110
- Rate of Endotracheal Intubation was Significantly Lower in the Helmet Group, as Compared to the High-Flow Nasal Cannula Oxygen Group (30% vs 51%; Difference, -21% [95% CI: -38% to -3%]; P = 0.03)
- Median Number of Days Free of Invasive Mechanical Ventilation within 28 Days was Significantly Higher in the Helmet Group, as Compared to the High-Flow Nasal Cannula Oxygen Group (28 [IQR, 13-28] vs 25 [IQR 4-28]; Mean Difference, 3 days [95% CI: 0-7]; P = 0.04)
- Median Days Free of Respiratory Support within 28 Days After Randomization were 20 (IQR, 0-25) in the Helmet Group and 18 (IQR, 0-22) in the High-Flow Nasal Cannula Oxygen Group (Mean Difference of 2 Days [95% CI: -2 to 6]; P = 0.26 -> Not Statistically Significant)
- In-Hospital Mortality Rate was 24% in the Helmet Group and 25% in the High-Flow Nasal Cannula Oxygen Group (Absolute Difference -1% [95% CI: -17% to 15%]; P > 0.99 -> Not Statistically Significant)
Recommendations (ERS/ATS Clinical Practice Guidelines for Noninvasive Ventilation for Respiratory Failure, 2017) (Eur Respir J, 2017) [MEDLINE]
- Given the Uncertainty of Evidence, No Recommendations were Made Regarding the Use of NIPPV in Acute Respiratory Due to Pneumonia and/or Acute Respiratory Distress Syndrome (ARDS)
Recommendations (Japanese Respiratory Society Noninvasive Positive Pressure Ventilation Guidelines, 2017) (Respir Investig, 2017) [MEDLINE]
- NIPPV Should Be Used Cautiously in ARDS (Level I Evidence, Grade C1 Recommendation)
- NIPPV is Recommended for the Management of Patients with Milder ARDS and Minor Extrapulmonary Organ Dysfunction (Level II Evidence, Grade B Recommendation)
Acute Respiratory Failure Due to Asthma (see Asthma)
Clinical Efficacy
- Study of NIPPV in Respiratory Failure Due to Asthma Exacerbation (Respirology, 2010) [MEDLINE]
- NIPPV Use in Asthma is Not Well-Defined, But Can Be Considered in Select Patients
- Systematic Review of NIPPV in Asthma Exacerbation (Cochrane Database Syst Rev, 2012) [MEDLINE]
- Use of NIPPV in Asthma Exacerbation Has Unclear Clinical Benefit
- Trial of Nebulization with Noninvasive Ventilation in the Treatment of Asthma Exacerbation (Respiratory Care, 2013) [MEDLINE]
- Coupling Nebulization and NIPPV During the Treatment of Asthma Exacerbation Did Not Improve Pulmonary Radio-Aerosol Deposition, But There was Clinical Improvement of Pulmonary Function
- Systematic Review and Meta-Analysis of Trials Using NIPPV for Prevention or Treatment of Acute Respiratory Failure or as a Tool to Facilitate Early Extubation (Crit Care Med, 2015) [MEDLINE]: n = 78 trials
- Asthma Exacerbation
- Data About Efficacy of NIPPV were Inconclusive
- Asthma Exacerbation
- Retrospective Study of NIPPV in Respiratory Failure Due to Asthma Exacerbation (Ann Am Thorac Soc, 2016) [MEDLINE]
- In Patients Hospitalized for Asthma Exacerbation with Respiratory Failure Requiring Ventilatory Support, >40% Received NIPPV
- Patients Treated with NIPPV Had Better Outcomes than Those Treated with Invasive Mechanical Ventilation
- Patients Treated with NIPPV Had Low Rates of NIPPV Failure, Suggesting that NIPPV was Being Selectively Used in Lower Risk Patients
Recommendations (ERS/ATS Clinical Practice Guidelines for Noninvasive Ventilation for Respiratory Failure, 2017) (Eur Respir J, 2017) [MEDLINE]
- Given the Uncertainty of Evidence, No Recommendations were Made Regarding the Use of NIPPV in the Treatment of Acute Respiratory Failure Associated with Asthma
Recommendations (Japanese Respiratory Society Noninvasive Positive Pressure Ventilation Guidelines, 2017) (Respir Investig, 2017) [MEDLINE]
- NIPPV Can Be Used for the Management of Acute Respiratory Failure Due to Asthma Exacerbation (Level II Evidence, Grade C1 Recommendation; Grade C2 Recommendation at Facilities with Limited Experience)
Respiratory Failure Due to Acute Interstitial Pneumonia
Clinical Efficacy
- Multicenter, Retrospective, Observational Study of of NIPPV in Respiratory Failure Associated with Diffuse Interstitial Lung Disease (BMC Pulm Med, 2014) [MEDLINE]: n = 60
- Pneumonia (42%) and Acute Exacerbation of Pulmonary Fibrosis (39%) were the Two Most Frequent Causes of Acute Respiratory Failure
- NIPPV Increased pO2/FIO2 Ratio in Pneumonia, But Not in Pulmonary Fibrosis
- NIPPV Failure Rate was 37%
Recommendations (Japanese Respiratory Society Noninvasive Positive Pressure Ventilation Guidelines, 2017) (Respir Investig, 2017) [MEDLINE]
- NIPPV Can Be Used for the Management of Acute Respiratory Failure Due to Interstitial Pneumonia (Level IV Evidence, Grade C1 Recommendation)
Acute Respiratory Failure Due to Neuromuscular Disease
Clinical Efficacy
- As of 2009 Review, There Were No Published Trials Using NIPPV in Acute Respiratory Failure Due to Neuromuscular Disease (Respir Care, 2009) [MEDLINE]
- However, NIPPV is the Preferred Treatment of Nocturnal Hypoventilation and Chronic Respiratory Failure in Neuromuscular Disease (Curr Opin Neurol, 2005) [MEDLINE] (Am J Respir Crit Care Med, 2013) [MEDLINE]
- Tracheostomy/Mechanical Ventilation is Required in Cases with Bulbar Dysfunction or Uncontrolled Aspiration
- However, NIPPV is the Preferred Treatment of Nocturnal Hypoventilation and Chronic Respiratory Failure in Neuromuscular Disease (Curr Opin Neurol, 2005) [MEDLINE] (Am J Respir Crit Care Med, 2013) [MEDLINE]
Clinical Efficacy-Myasthenia Gravis (see Myasthenia Gravis)
- Small Case Series Examining NIPPV in Acute Respiratory Failure Due to Myasthenia Gravis (Neurology, 2002) [MEDLINE]
- Presence of Hypercapnia (pCO2 >50 mm Hg) at Onset Predicted BiPAP Failure and Subsequent Intubation
- Study of Efficacy of NIPPV in Myasthenic Crisis (Arch Neurol, 2008) [MEDLINE]
- BiPAP was Effective for Acute Respiratory Failure in Patients with Myasthenia Gravis
- A BiPAP Trial Before the Development of Hypercapnia Can Prevent Intubation and Prolonged Mechanical Ventilation, Decreasing Pulmonary Complications, ICU Length of Stay, and Hospital Length of Stay
Clinical Efficacy-Guillain-Barre Syndrome (see Guillain-Barre Syndrome)
- Small Study of NIPPV in Acute Respiratory Failure Due to Guillain-Barre Syndrome (GBS) (Can J Neurol Sci, 2006) [MEDLINE]
- Until More Experience is Available, Authors Strongly Warned Against Using BiPAP in the Treatment of Deteriorating Guillain-Barre Syndrome Patients
Recommendations
- Acute Respiratory Failure
- NIPPV Has Undefined Role in Acute Respiratory Failure Due to Neuromuscular Disease
Acute Respiratory Failure Due to Restrictive Thoracic Disease
Clinical Efficacy
- Study of Noninvasive Positive-Pressure Ventilation in Acute (or Acute on Chronic) Respiratory Failure Associated with Kyphoscoliosis (Multidiscip Respir Med, 2012) [MEDLINE]: n = 62
- In the Subset of Patients without Sepsis, NIPPV Failure Rate was 38.1%
- In the Subset of Patients with Sepsis, NIPPV Failure was 84.6%
Recommendations (Japanese Respiratory Society Noninvasive Positive Pressure Ventilation Guidelines, 2017) (Respir Investig, 2017) [MEDLINE]
- NIPPV is Recommended as a First-Line Treatment in Patients with Exacerbation of Restrictive Thoracic Disease (Sequelae of Pulmonary Tuberculosis, Kyphoscoliosis) (Level IV Evidence, Grade A Recommendation)
Acute Respiratory Failure Due to Obesity-Hypoventilation Syndrome (OHS) (see Obesity-Hypoventilation Syndrome)
Clinical Efficacy
- Spanish Study of Effects of NIPPV in OHS (Chest, 2005) [MEDLINE]
- NIPPV was Effective for Acute Respiratory Failure Due to OHS, Providing a Significant Improvement in Clinical Status and Gas Exchange
- Spanish Study of NIPPV for Acute Hypercapnic Respiratory Failure Due to Obesity-Hypoventilation Syndrome (Am J Respir Crit Care Med, 2012) [MEDLINE]
- Patients with OHS Can Be Treated with NIPPV During an Episode of Acute Hypercapnic Respiratory Failure with Similar Efficacy and Better Outcomes than Patients with COPD
- Prospective Study of NIPPV in the Treatment of Morbidly Obese Patients with Obesity-Hypoventilation Syndrome and Acute Respiratory Failure (PLoS One, 2014) [MEDLINE]: n = 76 (with BMI >40 kg/m2)
- Factors Associated with Failure of NIPPV in this Population
- Pneumonia
- High Admission SOFA Score
- High Admission SAPS2 Score
- Factors Associated with Success of NIPPV
- Idiopathic Decompensation of OHS
- In Morbidly Obese Patients with Hypoxemic Acute Respiratory Failure, Multiple Organ Failure and Pneumonia were the Main Factors Associated with Failure of NIPPV and Death
- in Morbidly Obese Patients with Hypercapnic Acute Respiratory Failure, NIPPV Can Be Safely Used
- Factors Associated with Failure of NIPPV in this Population
- Review of Efficacy of Noninvasive Positive-Pressure Ventilation in Obese Patients (Adv Respir Med, 2017) [MEDLINE]
- More than Half of the Hypercapnic Patients with Decompensated OHS Exhibited a Delayed, But Successful, Response to NIPPV
- Review of the Use of Noninvasive Positive-Pressure Ventilation in Obese Patients Undergoing Bariatric Surgery (Minerva Chir, 2017) [MEDLINE]
- In the Perioperative Setting, NIPPV May Decrease Obesity-Related Comorbidities, Decreased Upper Airway Obstruction, Decrease Hypoventilation, Decrease Atelectasis, Improve Gas Exchange, Improve Respiratory Function, Relieve Dyspnea, and Decrease Work of Breathing
- Review of Noninvasive Positive-Pressure Ventilation in Obesity-Hypoventilation Syndrome (J Intensive Care Med, 2017) [MEDLINE]
- Authors Propose an Algorithm for the Management of OHS with Acute Hypoxemic Respiratory Failure
General Recommendations
- Obesity-Hypoventilation Syndrome with Acute Decompensation
- Bilevel Positive Airway Pressure (BPAP) is Recommended
Postoperative Acute Respiratory Failure
Clinical Efficacy-Respiratory Failure Following Lung Resection
- Small Randomized Trial of NIPPV in Respiratory Following Lung Resection (Am J Resp Crit Care Med, 2001) [MEDLINE]
- NIPPV Decreased Intubation Rate, Length of Stay, and Mortality Rate
- Systematic Review of NIPPV Following Lung Resection for Lung Cancer (Cochrane Database Syst Rev, 2015) [MEDLINE]
- No Benefit in Terms of Rate of Pulmonary Complications, Rate of Non-Pulmonary Complications, Post-Operative Antibiotic Use, Length of ICU Stay, Length of Hospital Stay, Rate of Intubation, Adverse Effects Related to NIPPV, and Mortality Rate
- Criticism: Quality of Evidence is Moderate, Low, and Very Low
- Systematic Review and Meta-Analysis of Trials Using NIPPV for Prevention or Treatment of Acute Respiratory Failure or as a Tool to Facilitate Early Extubation (Crit Care Med, 2015) [MEDLINE]: n = 78 trials
- Overall (in All Populations), NIPPV Decreased the Mortality Rate (at Longest F/U) with Relative Risk 0.73 (95% CI: 0.66–0.81) (p<0.001): number needed to treat = 19
- Postoperative Respiratory Failure
- NIPPV Decreased Mortality Rate (at Longest F/U) with Relative Risk 0.51 (95% CI: 0.28–0.92) (p=0.02)
Clinical Efficacy-Respiratory Failure Following Abdominal Surgery
- Systematic Review and Meta-Analysis of Trials Using NIPPV for Prevention or Treatment of Acute Respiratory Failure or as a Tool to Facilitate Early Extubation (Crit Care Med, 2015) [MEDLINE]: n = 78 trials
- Overall (in All Populations), NIPPV Decreased the Mortality Rate (at Longest F/U) with Relative Risk 0.73 (95% CI: 0.66–0.81) (p<0.001): number needed to treat = 19
- Postoperative Respiratory Failure
- NIPPV Decreased Mortality Rate (at Longest F/U) with Relative Risk 0.51 (95% CI: 0.28–0.92) (p=0.02)
- French Randomized NIVAS Trial of NIPPV in Respiratory Failure Following Abdominal Surgery (JAMA, 2016) [MEDLINE]: randomized, multi-center trial (n = 293); trial excluded patients who required immediate reintubation
- As Compared to Standard Oxygen Therapy, NIPPV Decreased the Rate of Endotracheal Intubation Within 7 Days
- NIPPV Increased the Number of Ventilator-Free Days
- NIPPV Decreased the Health Care-Associated Infection Rate
- No Difference in 90-Day Mortality Rate
- There Were No Significant Differences in Gas Exchange Between the Groups
- Criticism: Trial Had a Lower Than Expected Reintubation Rate
Clinical Efficacy-Respiratory Failure Following Cardiac Surgery
- Randomized Trial of NIPPV for Acute Respiratory Failure After Cardiac Surgery (Chin Med J (Engl) 2013;126:4463–9 [MEDLINE]: n = 95
- NIPPV Can Be Applied in Selected Patients with Acute Respiratory Failure After Cardiac Surgery to Decrease the Need for Reintubation and Improve Clinical Outcomes, as Compared with Conventional Treatment
- Pneumonia and a APACHE II Score >20 Might Be Independent Risk Factors for NIPPV Failure in this Group of Patients
Recommendations (ERS/ATS Clinical Practice Guidelines for Noninvasive Ventilation for Respiratory Failure, 2017) (Eur Respir J, 2017) [MEDLINE]
- NIPPV is Recommended for Patients with Acute Respiratory Failure in the Postoperative Setting (Conditional Recommendation, Moderate Certainty of Evidence)
Recommendations (Japanese Respiratory Society Noninvasive Positive Pressure Ventilation Guidelines, 2017) (Respir Investig, 2017) [MEDLINE]
- NIPPV May Be Useful for the Prevention and Treatment of Respiratory Complications During the Perioperative Period (Level II Evidence, Grade B Recommendation)
Recommendations from 2018 International Consensus Conference Regarding Nonsurgical Strategies to Reduce Mortality in Patients Undergoing Cardiac Surgery (J Cardiothorac Vasc Anesth, 2018) [MEDLINE]
- Recommended Perioperative Strategies Which May Decrease the Mortality Rate
- Low-Dose Preoperative and Early Postoperative Aspirin (Grade 2B): data from 2 RCT’s
- Strict Glycemic Control (2B): data from 3 RCT’s and 1 meta-analysis of RCT’s
- However, Authors Recommend Caution When Using this Strategy Because Hypoglycemic Episodes Might Increase the Mortality Rate
- High-Volume Surgeon (Grade 1C): data from 3 non-RCT’s
- Especially with Valve Procedures
- Prophylactic Intra-Aortic Balloon Pump (IABP) in High-Risk Patients Undergoing Coronary Artery Bypass Grafting (CABG) (Grade 2B): data from 1 RCT, 4 meta-analyses of RCT’s, and 1 meta-analysis of both RTC’s and non-RCT’s
- Levosimendan in Low Ejection Fraction Patients Undergoing CABG (Grade 1B): data from 1 RCT, 3 meta-analyses of RCT’s, 1 meta-analysis of RCT’s with subanalysis performed in cardiac surgery, and 2 meta-analyses of RCT’s involving mostly cardiac surgery studies
- Leukocyte-Depleted Packed Red Blood Cell Transfusion in Patients Requiring a High Number of Packed Red Blood Cell Units (Grade 2B): data from 2 RCT’s
- Postoperative Noninvasive Positive-Pressure Ventilation (NIPPV), Especially in Patients with Acute Respiratory Failure (Grade 2B): data from 1 RCT (Chin Med J-Engl, 2013) [MEDLINE] and 1 meta-analysis of RCT’s (Crit Care Resusc, 2013) [MEDLINE]
- Tranexamic Acid (Grade 2C): data from network meta-analysis including RCT’s and non-RCT’s
- VAC Therapy for Patients with Postoperative Deep Sternal Wound Infection (Grade 1C): data from 1 meta-analysis including non-RCT’s
- Volatile Anesthetic Agents (Desflurane, Isoflurane, and Sevoflurane) in Patients Undergoing CABG (Grade 2B): data from 2 meta-analysis of RCT’s and a metaregression
- Therapies Which May Increase the Mortality Rate
- Aprotinin (see Aprotinin)
Acute Respiratory Failure Due to Chest Trauma
Clinical Efficacy
- Randomized Trial of CPAP with Regional Anesthesia vs Intubation with Mechanical Ventilation (with PEEP) in Patients with Rib Fractures (Chest, 1990) [MEDLINE]: n = 69
- CPAP Strategy Decreased the Mean Duration of Treatment, ICU Length of Stay, Hospital Length of Stay, and Complication Rate, as Compared to Intubation with Mechanical Ventilation
- CPAP Strategy Decreased the Pneumonia Rate (14%), as Compared to Intubation with Mechanical Ventilation (48%)
- Comparative Study of CPAP vs Intermittent Positive-Pressure Ventilation (IPPV) in Patients with Flail Chest (Emerg Med J, 2005) [MEDLINE]
- Noninvasive CPAP with Patient-Controlled Analgesia (PCA) Resulted in Decreased Mortality and Decreased Nosocomial Infection Rate, But Similar Oxygenation and ICU Length Stay
- Randomized Trial of Noninvasive Positive-Pressure Ventilation vs Oxygen Therapy in Chest Trauma-Related Hypoxemia (Chest, 2010) [MEDLINE]
- NIPPV Decreased the Intubation Rate, as Compared to Oxygen Therapy
Recommendations (ERS/ATS Clinical Practice Guidelines for Noninvasive Ventilation for Respiratory Failure, 2017) (Eur Respir J, 2017) [MEDLINE]
- NIPPV is Recommended for Chest Trauma Patients with Acute Respiratory Failure (Conditional Recommendation, Moderate Certainty of Evidence)
Recommendations (Japanese Respiratory Society Noninvasive Positive Pressure Ventilation Guidelines, 2017) (Respir Investig, 2017) [MEDLINE]
- NIPPV Can Be Used for Patients with Acute Respiratory Failure Due to Thoracic Injury (Level II Evidence, Grade C1 Recommendation; Grade B Recommendation at Experienced Facilities)
Post-Extubation Acute Respiratory Failure
Background
- Extubation Failure Occurs After 5-20% of Planned and After 40-50% of Unplanned Extubations
- Extubation Failure is Associated with Increased Mortality Rate of 43% (vs 12% Mortality in Those with Successful Extubation)
Clinical Efficacy
- In COPD, NIPPV Decreased Reintubation Rate and ICU Length of Stay (Eur Respir J, 1998) [MEDLINE]
- In Randomized Trial (Which Excluded COPD Patients After the First Year of the Study, Due to Ethical Concerns), NIPPV Did Not Decrease Reintubation Rate, Duration of Mechanical Ventilation, Length of Hospital Stay, or Mortality (JAMA, 2002) [MEDLINE]
- In Study (with Only 10% COPD Patients), NIPPV Increased the Mortality Rate (NEJM, 2004) [MEDLINE]
- In this Study, the Longer Delay to Reintubation was Likely the Reason for the Observed Increase in Mortality Rate
- Also 25% of the Control Subjects were Crossed-Over to NIPPV When They Deteriorated and Met Criteria for Intubation: cross-overs had only only a 25% reintubation rate (which was half of that in the-to-treat NIPPV group), raising the concerns about the study design
- Meta-Analysis of NIPPV in Post-Extubation Respiratory Failure (Indian J Crit Care, 2013) [MEDLINE]
- Prophylactic NIPPV Improved Reintubation and Hospital Mortality Rates
- Therapeutic NIPPV Only Improved ICU Length of Stay, But Did Not Impact the Reintubation or Mortality Rate
- Meta-Analysis of NIPPV in Post-Extubation Respiratory Failure (Heart Lung, 2014) [MEDLINE]: n = 10 trials (n = 1382 patients)
- NIPPV Did Not Decrease the Reintubation Rate or Decreased ICU Mortality In Established Post-Extubation Respiratory Failure, as Compared to Standard Care
- Early Application of NIPPV Did Not Decrease the Reintubation Rate in Post-Extubation Respiratory Failure
- However, in the Planned Extubation Subgroup, NIPPV Decreased the Reintubation Rate, ICU Mortality Rate, and Hospital Mortality Rate
- Systematic Review and Meta-Analysis of Trials Using NIPPV for Prevention or Treatment of Acute Respiratory Failure or as a Tool to Facilitate Early Extubation (Crit Care Med, 2015) [MEDLINE]: n = 78 trials
- Overall (in All Populations), NIPPV Decreased the Mortality Rate (at Longest F/U) with Relative Risk 0.73 (95% CI: 0.66–0.81) (p<0.001): number needed to treat = 19
- Post-Extubation Acute Respiratory Failure
- NIPPV Did Not Decrease Mortality Rate (at Longest F/U) with Relative Risk 1.35 (9% CI: 0.78–2.35) (p=0.28)
- Retrospective Study of NIPPV in Unplanned Extubation (Respir Care, 2018) [MEDLINE]
- NIPPV After Unplanned Extubation Had Uncertain Efficacy, Especially When Provided as Rescue Management of Postextubation Respiratory Failure
Recommendations
- NIPPV Can be Selectively Used for Extubation Failure: NIPPV is beneficial in COPD and other hypercapnic conditions
- However, if NIPPV Fails to Rescue the Patient, Reintubation Should Be Performed without Delay
Recommendations (ERS/ATS Clinical Practice Guidelines for Noninvasive Ventilation for Respiratory Failure, 2017) (Eur Respir J, 2017) [MEDLINE]
- NIPPV is Not Recommended for Post-Extubation Acute Respiratory Failure (Conditional Recommendation, Low Certainty of Evidence)
Acute Respiratory Failure in “Do Not Intubate” (DNI) Patients
Clinical Efficacy
- Study of Outcomes of the Use of Noninvasive Positive-Pressure Ventilation in Do No Intubate (DNI) Patients (Crit Care Med, 2004) [MEDLINE]: n = 114
- Patients with Respiratory Failure and DNI Status Have High Mortality Rate When Treated with NIPPV (Only 43% of Patients Survived to Discharge)
- Factors Unassociated with Improved Survival to Discharge
- Age
- Gender
- Location in a Community vs Teaching Hospital
- Initial pH
- Initial pO2
- Factors Associated with Improved Survival to Discharge
- Higher Baseline pCO2
- Diagnosis (with Congestive Heart Failure Having Significantly Better Survival Rates than Those with Chronic Obstructive Pulmonary Disease, Cancer, Pneumonia, or Other Diagnoses)
- Strong Cough
- Awake Mental Status
- Study of Outcomes of the Use of Noninvasive Positive-Pressure Ventilation in Do No Intubate (DNI) Patients (Crit Care Med, 2005) [MEDLINE]: n = 131
- Hospital Mortality Varied by Diagnosis
- COPD: 37.5% hospital mortality rate
- Cardiogenic Pulmonary Edema: 39% hospital mortality rate
- Non-COPD Hypercapnic Respiratory Failure: 68% hospital mortality rate
- Postextubation Respiratory Failure: 77% hospital mortality rate
- Hypoxemic Respiratory Failure: 86% hospital mortality rate
- Advanced Cancer: 85% hospital mortality rate
- Score Based on Simplified Acute Physiology Score (SAPS) II and Serum Albumin Calculated Before NIPPV Predicted Hospital Outcome
- Hospital Mortality Varied by Diagnosis
- Review of Palliative NIPPV in Patients with Acute Respiratory Failure (Intensive Care Med, 2011)< [MEDLINE]
- NIPPV Has Been Extensively Used as a Pallative Treatment for Dyspnea
- Study of Noninvasive Positive-Pressure Ventilation in Very Elderly (≥80 y/o) Patients (Ann Intensive Care, 2012) [MEDLINE]: n = 376
- Hospital Mortality was Higher in Very Elderly Patients, as Compared to Younger Patients
- However, Hospital Mortality Did Not Differ When NIPPV was Used for Cardiogenic Pulmonary Edema, Acute on Chronic Respiratory Failure, and Postextubation Respiratory Failure
- 6-Month Mortality was 51% for Very Elderly Patients, 67% of DNI Patients, and 77% in Patients with NIPPV Failure Requiring Intubation
- Hospital Mortality was Higher in Very Elderly Patients, as Compared to Younger Patients
- Study of Noninvasive Positive-Pressure Ventilation in DNI Patients (Intensive Care Med, 2013) [MEDLINE]
- DNI Status was Present in 20% of Patients Who Received NIPPV
- DNI Patients Who were Alive on Day 90 Experienced No Decrease in Health-Related Quality of Life (HRQOL), as Compared to Baseline
- The Prevalences of Anxiety, Depression, and Post-Traumatic Stress Disorder (PTSD)-Related Symptoms in These Patients and Their Relatives were Similar to Those Seen After NIPPV as Used as Part of Full-Code Management
- Study of Sedation for Treatment of Agitation During Noninvasive Positive-Pressure Ventilation (BMC Pulm Med, 2015) [MEDLINE]
- Using RASS Score, Sedation During NIPPV in Proficient Hospitals May Be Favorably Used to Avoid NIPPV Failure in Agitated Patients, Eeven in Those Patients with Diseases with Poor Evidence for the Usefulness of NIPPV
- In DNI Patients with Agitation, 96% of Patients were Able to Continue NIPPV with Sedation
- Study of Noninvasive Positive-Pressure Ventilation in DNI Patients in the Emergency Department (PLoS One, 2016) [MEDLINE]
- Survival Rate was 49% Among DNI Patients for Whom NIV was Used as a Treatment in ED, and These Patients Did Not Experience a Decline in Health-Related Quality of Life (HRQOL) Throughout the Study
- NIPPV Did Not Provide Significant Relief of Symptoms in 59% of the Patients Who Received it for that Purpose
Recommendations (ERS/ATS Clinical Practice Guidelines for Noninvasive Ventilation for Respiratory Failure, 2017) (Eur Respir J, 2017) [MEDLINE]
- NIPPV is Suggested for Dyspneic Patients for Palliation in the Setting of Terminal Cancer or Other Terminal Conditions (Conditional Recommendation, Moderate Certainty of Evidence)
Recommendations (Japanese Respiratory Society Noninvasive Positive Pressure Ventilation Guidelines, 2017) (Respir Investig, 2017) [MEDLINE]
- NIPPV is Recommended for the Management of Acute Respiratory Failure in DNI and Elderly Patients with COPD or Cardiac Failure (Level of Evidence IV, Grade B Recommendation)
- There is Only Poor Evidence for the Effectiveness of NIPPV for the Management of Acute Respiratory Failure in DNI and Elderly Patients without COPD or Congestive Heart Failure (Level of Evidence IV, Grade C1 Recommendation)
- If No Improvement is Observed, the Aim of Treatment Should Be Alleviation of Dyspnea
- NIPPV Can Be Used as a Palliative Treatment for Respiratory Failure in Patients in the Terminal Phase of a Disease or with Malignant Tumor (Level II Evidence, Grade C1 Recommendation)
Facilitation of Early Extubation
Clinical Efficacy
- Systematic Review/Meta-Analysis of Early Extubation with Transition to NIPPV in Studies of Predominantly COPD Patients Demonstrates Decreased Mortality and Ventilator-Associated Pneumonia Rates (Cochrane Database Syst Rev, 2010) [MEDLINE]
- In 12 Studies with Predominantly COPD Patients, Postextubation NIPPV Decreased the Mortality Rate and Ventilator-Associated Pneumonia Rate
- Systematic Review and Meta-Analysis of Trials Using NIPPV for Prevention or Treatment of Acute Respiratory Failure or as a Tool to Facilitate Early Extubation (Crit Care Med, 2015) [MEDLINE]: n = 78 trials
- NIPPV Decreased the Mortality Rate in Patients Treated for Acute Respiratory Failure (Due to COPD Exacerbation, Pulmonary Edema, Postoperative Acute Respiratory Failure, and Mixed Etiologies)
- NIPPV Decreased the Mortality Rate When Used to Prevent Acute Respiratory Failure
- NIPPV Did Not Decrease the Mortality Rate When Used to Facilitate Early Extubation
- Cochrane Systematic Review of NIPPV as a Weaning Strategy in Adults with Acute Respiratory Failure (Population with Predominantly COPD) (CMAJ, 2014) [MEDLINE]: n= 16 trials (n = 994 patients)
- Most of Patients in Trials Had COPD
- NIPPV Decreased the Mortality Rate and Pneumonia Rate without Increasing the Risk of Weaning Failure or Reintubation
- In Subgroup Analysis, Mortality Benefits were Significantly Greater in Patients with COPD
- Systematic Review and Meta-Analysis of Trials Using NIPPV for Prevention or Treatment of Acute Respiratory Failure or as a Tool to Facilitate Early Extubation (Crit Care Med, 2015) [MEDLINE]: n = 78 trials
- Overall (in All Populations), NIPPV Decreased the Mortality Rate (at Longest F/U) with Relative Risk 0.73 (95% CI: 0.66–0.81) (p<0.001): number needed to treat = 19
- Facilitation of Early Extubation
- NIPPV Did Not Decrease the Mortality Rate (at Longest F/U) with Relative Risk 0.81 (95% CI: 0.51–1.30) (p=0.39)
- Pooled Analysis of Use of Postextubation NIPPV in High-Risk Patients (Chest, 2017) [MEDLINE]: n = 5 trials
- High-Risk Factors: COPD, CHF, hypercapnia, older age, and a higher severity of illness
- NIPPV was Favored Postextubation Over Standard Care in High-Risk Patients (RR, 1.14; 95% CI: 1.05-1.23)
- NIPPV was Significantly Better than Conventional Therapy for ICU Length of Stay (Mean Difference –2.48 Days; 95% CI, –4.03 to –0.93) and Short-Term Mortality (RR 0.37; 95% CI: 0.19-0.70)
- Trial of Early Extubation to Immediate NIPPV in Patients with Hypoxemic Respiratory Failure (Intensive Care Med, 2018) [MEDLINE]: n = 130
- In Highly Selected Hypoxemic Patients, Early Extubation Followed by Immediate NIPPV Decreased the Duration of Invasive Mechanical Ventilation without Affecting ICU Length of Stay
- Incidence of VAP, Rate of Patients Requiring Sedative Infusion, and Hospital Length of Stay were All Decreased in the Early Extubation Group, as Compared to Control
- No Difference was Observed in ICU or Hospital Mortality Rate, Number of Treatment Failures, Severe Events, and Tracheostomy Rate
- UK Randomized Breathe Trial of Early Extubation to NIPPV in General Population of Patients with Respiratory Failure (JAMA, 2018) [MEDLINE]: n = 364
- The Median Time to Liberation was 4.3 Days in the NIPPV Group vs 4.5 Days in the Invasive Ventilation Group (Adjusted Hazard Ratio, 1.1; 95% CI: 0.89-1.40)
- The NIPPV Group Received Less Invasive Ventilation (Median, 1 Day vs 4 Days; Incidence Rate Ratio, 0.6; 95% CI: 0.47-0.87) and Fewer Total Ventilator Days (Median, 3 Days vs 4 Days; Incidence Rate Ratio, 0.8; 95% CI: 0.62-1.0)
- There was No Significant Difference in Reintubation Rates, Tracheostomy Rates, or Mortality Rates
- Adverse Events Occurred in 24.7% of Patients in the NIPPV Group vs 25.8% of Patients in the Invasive Ventilation Group
- In Patients Requiring Mechanical Ventilation in Whom a Spontaneous Breathing Trial Had Failed, Early Extubation to NIPPV Did Not Shorten time to Liberation from Any Ventilation
- Systematic Review of Postextubation NIPPV in Patients with Respiratory Failure (Intensive Care Med, 2018) [MEDLINE]
- Postextubation NIPPV Decreased Hospital Mortality, Decreased VAP Incidence, and Decreased ICU Length of Stay
- Effect was Most Beneficial in Patients with COPD
- Small Randomized Trial of Early Extubation with Immediate Postextubation NIPPV in Highly-Selected Patients with Hypoxemic Respiratory Failure (Intensive Care Med, 2019) [MEDLINE]: n = 130
- In Highly-Selected Hypoxemic Patients, Early Extubation with Immediate Postextubation NIPPV Decreased Ventilator Days, But Did Not Impact ICU Length of Stay
- No Significant Difference in ICU Mortality, Hospital Mortality, Number of Treatment Failures, Severe Event Rate, or Tracheostomy Rate
General Recommendations
- Good Candidates for Early Extubation to NIPPV
- Abscence of Major Co-Morbidities
- Alertness
- Manageable Secretions
- Presence of COPD
- Poor Candidates for Early Extubation to NIPPV
- Cardiac/Hemodynamic Instability
- Facial/Upper Airway Abnormalities
- High FIO2 or PEEP Requirement
- Poor Cough
- Significant Secretions
Recommendations (ERS/ATS Clinical Practice Guidelines for Noninvasive Ventilation for Respiratory Failure, 2017) (Eur Respir J, 2017) [MEDLINE]
- NIPPV May Be Used to Facilitate Weaning from Mechanical Ventilation in Patients with Hypercapnic Respiratory Failure (Conditional Recommendation, Moderate Certainty of Evidence)
- No Recommendations are Made Regarding Using NIPPV to Facilitate Weaning from Mechanical Ventilation in Hypoxemic Patients
Recommendations (Japanese Respiratory Society Noninvasive Positive Pressure Ventilation Guidelines, 2017) (Respir Investig, 2017) [MEDLINE]
- NIPPV is Useful When Weaning Patients with Complications from COPD from Invasive Mechanical Ventilation (Level I Evidence, Grade B Recommendation)
Post-Extubation Prophylaxis
Clinical Efficacy
- Prospective Randomized Trial of Prophylactic NIPPV Following Thoracoabdominal Aortic Surgery (Chest, 2005) [MEDLINE]
- Prophylactic Post-Extubation NIPPV Decreased Pulmonary Morbidity and Length of Stay
- Randomized Trial of Early Prophylactic NIPPV in High-Risk Patients (Am J Respir Crit Care Med, 2006) [MEDLINE]
- In At-Risk Patients (with Risk Factors Such as Hypercapnia, Congestive Heart Failure, Ineffective Cough and Excessive Tracheobronchial Secretions, More Than One Failure of a Weaning Trial, More Than One Comorbid Condition, and Upper Airway Obstruction), Prophylactic NIPPV for First 48 hrs After Extubation Decreased Reintubation Rate and Mortality Rate
- Randomized Trial of Prophylactic NIPPV vs Usual Care in Extubated Patients Who were at Risk for Reintubation (Am J Respir Crit Care Med, 2006) [MEDLINE]
- Overall, NIPPV Decreased the Reintubation Rate and ICU Mortality Rate
- In the Subgroup of Chronically Hypercapnic Patients (Identified by the Presence of Hypercapnia with pCO2 ≥45 mm Hg During Spontaneous Breathing Trial), NIPPV Decreased the Reintubation Rate, ICU Mortality Rate, and 90-Day Mortality Rate
- Systematic Review and Meta-Analysis of Prophylactic NIPPV Following Abdominal Surgery (Ann Surg, 2008) [MEDLINE]
- Post-Abdominal Surgery, Prophylactic NIPPV (CPAP) Decreased Post-Operative Pulmonary Complications, Atelectasis, and Pneumonia
- Spanish Randomized Trial of Prophylactic NIPPV vs Usual Care in Extubated Chronically Hypercapnic Patients (Lancet, 2009) [MEDLINE]
- In Chronically Hypercapnic Patients, Early Prophylactic NIPPV After Extubation Decreased the Reintubation Rate and 90-Day Mortality Rate
- Meta-Analysis of NIPPV in Post-Extubation Respiratory Failure (Indian J Crit Care, 2013) [MEDLINE]
- Prophylactic NIPPV Improved Reintubation and Hospital Mortality Rates
- Therapeutic NIPPV Only Improved ICU Length of Stay, But Did Not Impact the Reintubation or Mortality Rate
- Meta-Analysis of NIPPV After Cardiac Surgery (Crit Care Resusc, 2013) [MEDLINE]: meta-analysis of 14 randomised trials
- NIV Appears to Be Effective in Reducing the Reintubation Rate, Hospital Length of Stay, and Mortality Rate After Cardiothoracic Surgery
- Systematic Review and Meta-Analysis of Trials Using NIPPV for Prevention or Treatment of Acute Respiratory Failure or as a Tool to Facilitate Early Extubation (Crit Care Med, 2015) [MEDLINE]: n = 78 trials
- Overall (in All Populations), NIPPV Decreased the Mortality Rate (at Longest F/U) with Relative Risk 0.73 (95% CI: 0.66–0.81) (p<0.001): number needed to treat = 19
- Prevention of Acute Respiratory Failure
- Overall, NIPPV Decreased Mortality Rate (at Longest F/U) with Relative Risk 0.64 (95% CI: 0.46–0.90) (p=0.01)
- In the Prevention of Post-Extubation Respiratory Failure, NIPPV Decreased Mortality Rate with Relative Risk 0.65 (0.44–0.96) (p=0.03)
- In Prevention of Post-Extubation Respiratory Failure in High-Risk Patients, NIPPV Decreased Mortality Rate with Relative Risk 0.64 (0.43–0.97) (p=0.03)
- In Prevention of Post-Extubation Respiratory Failure in Unselected Patients, NIPPV Did Not Decrease Mortality Rate with Relative Risk 0.53 (0.04–6.50) (p=0.61)
- In the Prevention of Postoperative Respiratory Failure, NIPPV Did Not Decrease Mortality Rate with Relative Risk 0.81 (0.26–2.53) (p=0.72)
- In the Prevention of Postoperative Respiratory Failure Following Lung Surgery, NIPPV Did Not Decrease Mortality Rate with Relative Risk 0.55 (0.19–1.64) (p=0.29)
- In the Prevention of Postoperative Respiratory Failure in Obese Patients, Data About Efficacy of NIPPV were Inconclusive
- Retrospective Study of NIPPV in Unplanned Extubation (Respir Care, 2018) [MEDLINE]
- NIPPV After Unplanned Extubation Had Uncertain Efficacy, Especially When Provided as Rescue Management of Postextubation Respiratory Failure
Recommendations (ERS/ATS Clinical Practice Guidelines for Noninvasive Ventilation for Respiratory Failure, 2017) (Eur Respir J, 2017) [MEDLINE]
- NIPPV is Recommended to Prevent Post-Extubation Respiratory Failure in High-Risk Patients (Age >65 y/o and/or Underlying Cardiopulmonary Disease) (Conditional Recommendation, Low Certainty of Evidence)
- NIPPV is Not Recommended to Prevent Post-Extubation Respiratory Failure in Non-High-Risk Patients (Conditional Recommendation, Very Low Certainty of Evidence)
Recommendations (Japanese Respiratory Society Noninvasive Positive Pressure Ventilation Guidelines, 2017) (Respir Investig, 2017) [MEDLINE]
- NIPPV May Be Useful for the Prevention and Treatment of Respiratory Complications During the Perioperative Period (Level II Evidence, Grade B Recommendation)
Recommendations (American College of Chest Physicians/American Thoracic Society Clinical Practice Guideline for Liberation from Mechanical Ventilation in Critically Ill Adults) (Chest, 2017) [MEDLINE]
- Management of Patients at High Risk for Post-Extubation Respiratory Failure
- For Patients at High Risk for Extubation Failure (Hypercapnia, COPD, Congestive Heart Failure, or Other Serious Comorbidities) Who Have Been Receiving Mechanical Ventilation for >24 hrs, and Who Have Passed a Spontaneous Breathing Trial, Extubation to Preventative NIPPV is Recommended (Strong Recommendation, Moderate Quality of Evidence)
- Apply NIPPV Immediately After Extubation to Maximize the Outcome Benefit
- For Patients at High Risk for Extubation Failure (Hypercapnia, COPD, Congestive Heart Failure, or Other Serious Comorbidities) Who Have Been Receiving Mechanical Ventilation for >24 hrs, and Who Have Passed a Spontaneous Breathing Trial, Extubation to Preventative NIPPV is Recommended (Strong Recommendation, Moderate Quality of Evidence)
Respiratory Support During Endoscopic Procedures
Clinical Efficacy
- Prospective, Randomized Trial of Comparing High-FLow Nasal Cannula vs NIPPV During Bronchoscopy in Patients with Hypoxemia (Crit Care, 2014) [MEDLINE]
- NIPPV was Superior to HFNC in Terms of Oxygenation Before, During, and After Bronchoscopy in Patients with Moderate-Severe Hypoxemia
- Small Case Series of NIPPV During Deep Sedation for a Percutaneous Left Atrial Appendage Closure Procedure (Can J Anaesth, 2016) [MEDLINE]
- Deep Sedation with NIPPV May Be Used (Instead of General Anesthesia) for Patients Requiring Prolonged Transesophageal Echocardiogram for Noninvasive Cardiac Procedures
Indications to Treat Chronic Respiratory Failure
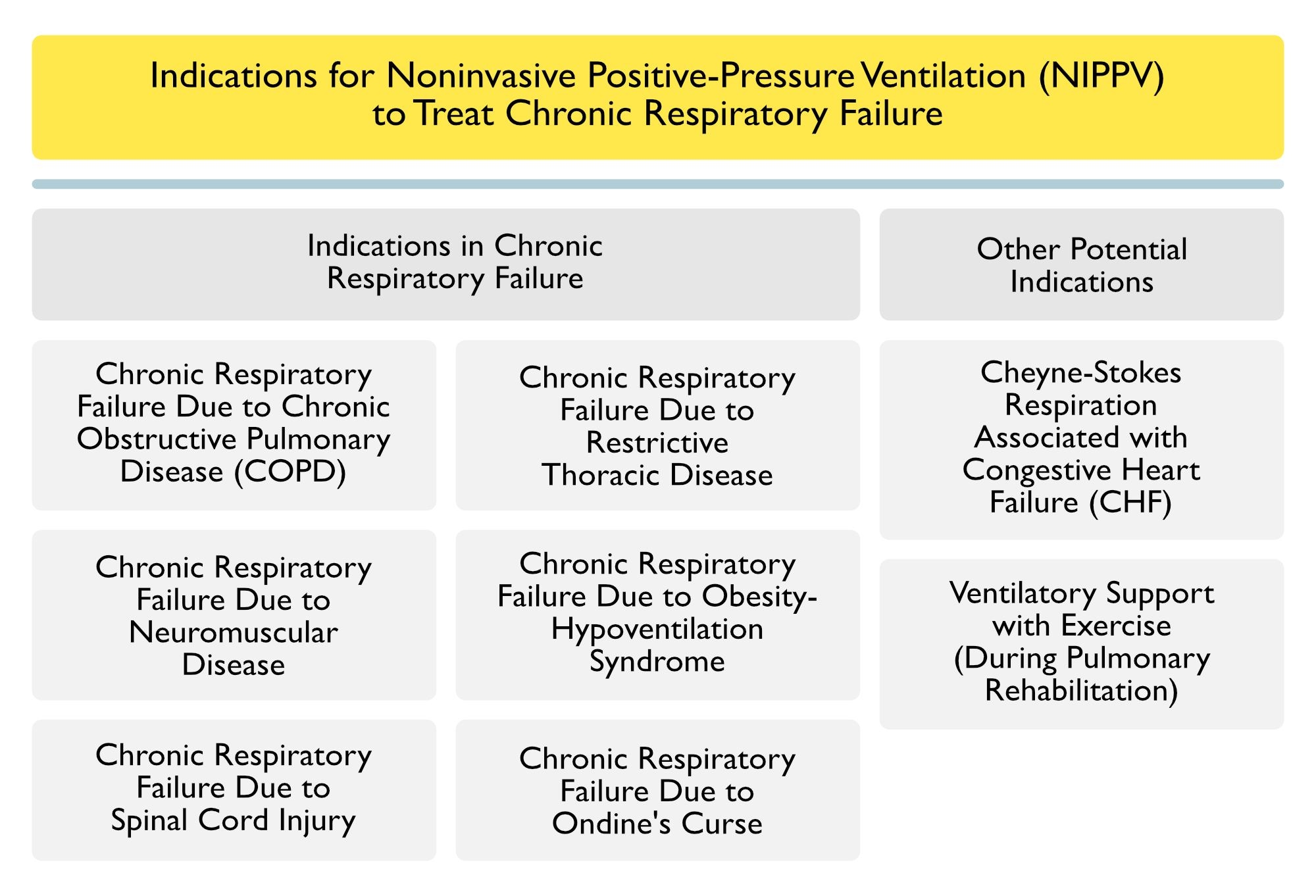
Chronic Respiratory Failure Due to Chronic Obstructive Pulmonary Disease (COPD) (see Chronic Obstructive Pulmonary Disease)
Clinical Efficacy
- AVCAL Study of NIPPV in Stable Hypercapnic COPD (Thorax, 2009) [MEDLINE]
- Nocturnal NIPPV Improved Survival in Stable Oxygen-Dependent Hypercapnic COPD, But Worsened Quality of Life
- Study of High Pressure vs High Intensity NIPPV in Stable Hypercapnic COPD (Int J Chron Obstruct Pulmon Dis, 2012) [MEDLINE]
- There was No Additional Benefit (in Terms of Nighttime Adherence or Other Parameters) of Addition of High Backup Rate to High-Pressure NIPPV
- High Pressure Component is the Predominant Determinant of Adequate Treatment of Hypercapnic COPD
- There was No Additional Benefit (in Terms of Nighttime Adherence or Other Parameters) of Addition of High Backup Rate to High-Pressure NIPPV
- Cochrane Database Systematic Review of Nocturnal NIPPV in Stable COPD (Cochrane Database Syst Rev, 2013) [MEDLINE]
- Nocturnal-NIPPV at Home for at Least 3 Months in Hypercapnic Patients with Stable COPD Had No Consistent Clinically or Statistically Significant Effect on Gas Exchange, Exercise Tolerance, Health-Related Quality of Life, Lung Function, Respiratory Muscle Strength or Sleep Efficiency
- Meta-Analysis of the 2 New Long-Term Studies Did Not Demonstrate Significant Improvement in Arterial Blood Gas, Health-Related Quality of Life, or Lung Function After 12 Months of NIPPV
- However, the Small Sample Sizes of the Studies Preclude a Definite Conclusion Regarding the Effects of NIPPV in COPD
- German Trial of NIPPV in Chronic Stable Hypercapnic COPD (Lancet Respir Med, 2014) [MEDLINE]
- The Addition of Long-Term NIPPV to Standard Treatment Improved Survival in Hypercapnic COPD When NIPPCV is Targeted to Significantly Decease the Hypercapnia
- UK Randomized Trial of Home Noninvasive Ventilation Following COPD Exacerbation (JAMA, 2017) [MEDLINE]: n = 166
- Exclusion Criteria: obesity (BMI >35), obstructive sleep apnea syndrome, or other cause of respiratory failure
- In COPD Patients with Persistent Hypercapnia Following an Acute COPD Exacerbation, Adding Home Noninvasive Ventilation to Home Oxygen Therapy Prolonged the Time to Hospital Readmission or Death within 12 Months
- The 12-Month Risk of Readmission or Death was 63.4% in the Home Oxygen Plus Home Noninvasive Ventilation Group vs 80.4% in the Home Oxygen Alone Group (Absolute Risk Reduction of 17%; 95% CI: 0.1%-34.0%)
General Indications for Nocturnal NIPPV in Chronic Obstructive Pulmonary Disease (COPD)
- Daytime Hypercapnia (pCO2 >52 mm Hg) and Sleep-Associated Desaturation (SpO2 ≤88% for ≥5 min Out of 2 hrs of Nocturnal Sleep) Despite the Use of Supplemental Oxygen at ≥2 L/min
- Following an Acute COPD Exacerbation Which Necessitated the Use of Continuous NIPPV During the Hospitalization
Recommendations (Canadian Thoracic Society Clinical Practice Guideline for Home Mechanical Ventilation, 2011) (Can Respir J, 2011) [MEDLINE]
- The Use of Long-Term NIPPV Cannot Be Widely Recommended in Patients with Stable COPD (Grade 1B Recommendation)
- Long-Term NIPPV in COPD Should Only Be Considered on an Individual Basis
- One Subgroup of COPD Patients in Which Long-Term NIPPV Could Be Considered are Those with Severe Hypercapnia (pCO2 >55 mm Hg) Experiencing Repeated Episodes of Acute Hypercapnic Respiratory Failure Who Require In-Hospital Ventilatory Support (Grade 2C Recommendation)
- However, Definitive Evidence of Efficacy of Long-Term NIPPV in this Subset of Patients Awaits Future Study
- One Subgroup of COPD Patients in Which Long-Term NIPPV Could Be Considered are Those with Severe Hypercapnia (pCO2 >55 mm Hg) Experiencing Repeated Episodes of Acute Hypercapnic Respiratory Failure Who Require In-Hospital Ventilatory Support (Grade 2C Recommendation)
- The Overlap Syndrome, and Concomitant COPD and OSA Syndrome, Should Be Differentiated from Chronic Respiratory Failure Which is Solely Due to Advanced COPD. (Grade 1C Recommendation)
Recommendations (Japanese Respiratory Society Noninvasive Positive Pressure Ventilation Guidelines, 2017) (Respir Investig, 2017) [MEDLINE]
- NIPPV May Be Used in Patients with COPD in Whom NIPPV is Indicated (Level I Evidence, Grade C1 Recommendation)
Chronic Respiratory Failure Due to Neuromuscular Disease
Clinical Efficacy-General
- Review of Use of NIPPV in Chronic Respiratory Failure Associated with Neuromuscular Disease (Chest, 2006) [MEDLINE]
- Nocturnal NIPPV Has Multiple Suggested Physiologic Effects
- Improvement of Ventilatory Mechanics
- Rest of Fatigued Respiratory Muscles, Resulting in Improved Strength and Endurance
- Enhanced Ventilatory Sensitivity to Carbon Dioxide (Thorax, 2005) [MEDLINE]
- Improvement in Sleep Stage Distribution, Resulting in Increased Chemosensitivity and Enhance Sleep Quality
- Nocturnal NIPPV is Believed to Prolong Survival in Chronic Respiratory Failure Associated with Neuromuscular Disease
- Nocturnal NIPPV Has Multiple Suggested Physiologic Effects
Clinical Efficacy-Duchenne’s Muscular Dystrophy (see Duchenne’s Muscular Dystrophy)
- Small Study of NIPPV in Duchenne’s Muscular Dystrophy (Am J Phys Med Rehabil, 2014) [MEDLINE]
- NIPPV Prolonged Survival without Resorting to Tracheotomy (and without Hospitalization)
Clinical Efficacy-Amyotrophic Lateral Sclerosis (ALS) (see Amyotrophic Lateral Sclerosis)
- Cochrane Database Systematic Review of Mechanical Ventilation in ALS (Cochrane Database Syst Rev, 2013) [MEDLINE]
- Evidence from a Single Randomized Trial of NIPPV (N = 41) Suggests that it Significantly Prolonged Survival and Improved or Maintained Quality of Life in ALS
- Survival and Some measures of Quality of Life were Significantly Improved in the Subgroup with Better Bulbar Function, But Not in Those with Severe Bulbar Impairment
Recommendations
- Acute Respiratory Failure
- NIPPV Has Undefined Role in Acute Respiratory Failure Due to Neuromuscular Disease
- NIPPV is the Preferred Treatment of Nocturnal Hypoventilation and Chronic Respiratory Failure in Neuromuscular Disease
Recommendations (Canadian Thoracic Society Clinical Practice Guideline for Home Mechanical Ventilation, 2011) (Can Respir J, 2011) [MEDLINE]
- Duchenne’s Muscular Dystrophy (see Duchenne’s Muscular Dystrophy)
- Monitoring
- Educate Patient and Assess for Symptoms Consistent with Chronic Hypoventilation (Including Disturbed Sleep, Excessive Daytime Somnolence, Morning Headache, and Weight Loss (Grade 1C Recommendation)
- Measure Vital Capacity (VC), Maximal Inspiratory Pressure (MIP), Maximal Expiratory Pressure (MEP), Peak Cough Flow (PCF), and Daytime Oxyhemoglobin Saturation by Pulse Oximetry at Least Annually (Grade 1C Recommendation)
- If VC <40% Predicted, Should Also Assess the Awake pCO2 with Arterial Blood Gas or Capnography (Grade 1C Recommendation)
- If There are Symptoms Consistent with Nocturnal Hypoventilation or Other Forms of Sleep-Disordered Breathing, Should Assess Ventilation During Sleep (Grade 1C Recommendation)
- In the Absence of Such Symptoms, Periodic Screening for Sleep-Disordered Breathing Should Be Considered Once FEV1 or FVC <40% Predicted (Grade 1C Recommendation)
- Treatment
- In Patients with Daytime Hypercapnia 9pCO2 >45 mm Hg) or Documented Nocturnal Hypercapnia and the Presence of Symptoms Consistent with Hypoventilation, Nocturnal NIPPV is Recommended (Grade 1B Recommendation)
- In Patients with Major Nocturnal Hypoxemia (Even if Asymptomatic), Nocturnal NIPPV is Recommended (Grade 2C Recommendation)
- When Bilevel Ventilation is Used, Backup Respiratory Rate is Recommended During Sleep to Decrease the Work of Breathing Associated with Breath Initiation (Grade 1C Recommendation)
- The Decision to Transition from Nocturnal NIPPV to Daytime Ventilation Should Be Individualized by Careful Evaluation of Patient Factors (Symptoms, Bulbar Involvement, Patient Preference) and Available Resources (Grade 1B Recommendation)
- In Patients Requiring Daytime Ventilation, Mouthpiece Ventilation Should Be Strongly Considered as an Alternative to Invasive Tracheostomy (Grade 1B Recommendation)
- With Declining VC, Lung Volume Recruitment Maneuvers Should Be Introduced (Grade 1C Recommendation)
- When Peak Cough Flow <270 L/min, Secretion Clearance Assistance Should Be Initiated (Grade 1C Recommendation)
- Monitoring
Recommendations (Japanese Respiratory Society Noninvasive Positive Pressure Ventilation Guidelines, 2017) (Respir Investig, 2017) [MEDLINE]
- NIPPV Should Be Used as a First-Line Treatment in Patients with Chronic Respiratory Failure Due to Neuromuscular Disease (Level II Evidence, Grade B Recommendation)
- NIPPV Should Not Be Used if There is a Significant Decline in Pharyngeal and Laryngeal Function and it is Difficult to Maintain Airway Clearance (Level II evidence, Grade D Recommendation)
Chronic Respiratory Failure Due to Spinal Cord Injury (SCI) (see Chronic Spinal Cord Injury)
Recommendations (Canadian Thoracic Society Clinical Practice Guideline for Home Mechanical Ventilation, 2011) (Can Respir J, 2011) [MEDLINE]
- Protocols for Weaning with Progressive Ventilator-Free Breathing (PVFB) Should Be Considered for Appropriate Patients with Tetraplegia Who are Ventilator-Dependent (Grade 1C Recommendation)
- Each Patient Must Be Individually Evaluated for the Need for Long-Term Ventilation Either Acutely or in Follow-Up (Grade 1C Recommendation)
- NIPPV is Preferable to Invasive Ventilation (Grade 1C Recommendation)
- Phrenic Nerve Pacing is Recommended in Selected Patients as an Alternative to Positive-Pressure Ventilation Alone (Grade 2C Recommendation)
- Regular Airway Clearance Techniques (Lung Volume Recruitment/LVR), Manually-Assisted Coughing/MAC) etc), Clinical Assessment and Ongoing Monitoring of Pulmonary Function is Recommended to Ensure Adequate Airway Clearance (Grade 1C Recommendation)
- In the Long Term, Individuals with SCI Require Regular Monitoring to Identify the Development of Sleep-Disordered Breathing or Respiratory Failure and Evaluate the Need for NIPPV (Consensus Recommendation)
Chronic Respiratory Failure Due to Restrictive Thoracic Disease
Clinical Efficacy
- Study of Nocturnal NIPPV in Patients with Hypercapnic Respiratory Failure Associated with Restrictive Thoracic Disease (Thorax, 2005) [MEDLINE]
- Increased Ventilatory Response to Carbon Dioxide is the Predominant Mechanism Responsible for Improved Daytime Hypercapnia in Patients Treated with Nocturnal NIPPV for Hypercapnic Respiratory Failure Due to Restrictive Thoracic Disease
- Increased Respiratory Muscle Strength (Sniff Esophageal Pressure, Sniff Nasal Pressure) Correlated with Decreases in Epworth Sleepiness Score: possibly indicating an increase in the ability to activate inspiratory muscles, rather than an improvement in contractility
- Prospective Study of Kyphoscoliosis Patients Treated with Home Mechanical Ventilation vs Oxygen (Chest, 2006) [MEDLINE]: n = 244
- As Compared to Long-Term Oxygen Therapy Alone, Patients Treated with Home Mechanical Ventilation Had Better Survival, Even When Adjusting for Age, Gender, Concomitant Respiratory Disease, and Arterial Blood Gas Levels, with a Hazard Ratio of 0.30 (95% Confidence Interval, 0.18 to 0.51)
- Study of Predictors of Mortality in Patients with Chest Wall Disease Treated with Noninvasive Positive-Pressure Ventilation (Respir Med, 2010) [MEDLINE]: n = 110
- In Patients with Chest Wall Disease, pCO2 ≥50 mm Hg at 1 Month After Starting Home NIPPV and the Presence of Comorbid Conditions (Charlson Index ≥3) are Risk Factors for Mortality
Recommendations (Canadian Thoracic Society Clinical Practice Guideline for Home Mechanical Ventilation, 2011) (Can Respir J, 2011) [MEDLINE]
- Kyphoscoliosis
- Patients with Kyphoscoliosis Should Undergo Periodic Spirometry Testing and if FVC is <50%, Ongoing Review and Assessment for Evidence of Hypercapnic Respiratory Failure Should Be Instituted (Grade 1C Recommendation)
- Long-Term Nocturnal NIPPV Should Be Offered to All Patients with Kyphoscoliosis Who Have Developed Chronic Hypoxemic, Hypercapnic Respiratory Failure (Grade of recommendation 1B)
- Patients with hypoxemia but without hypercapnia may be managed cautiously with oxygen therapy alone while monitoring for development of hypercapnia (Grade 1C Recommendation)
- Oxygen Therapy Can Be Added to NIPPV, if Considered Necessary for Unresponsive Oxygen Desaturation (Grade 1C Recommendation)
- Methods to Assist Secretion Clearance Should Be Initiated When Peak Cough Flow is <270 L/min (Grade 1C Recommendation)
Recommendations (Japanese Respiratory Society Noninvasive Positive Pressure Ventilation Guidelines, 2017) (Respir Investig, 2017) [MEDLINE]
- Long-Term NIPPV Should Be Implemented in Patients with Restrictive Thoracic Disease in Whom the Use of NIPPV is Indicated (Level IV Evidence, Grade A Recommendation)
Chronic Respiratory Failure Due to Obesity-Hypoventilation Syndrome (OHS) (see Obesity-Hypoventilation Syndrome)
Clinical Efficacy
- Study of NIPPV in Obesity-Hypoventilation Syndrome (Chest, 2001) [MEDLINE]
- NIPPV Improved Clinical Symptoms and Respiratory Failure in Obesity-Hypoventilation Syndrome to a Similar Degree to that Reported for Other Diseases with Established Indications (Such as Kyphoscoliosis)
- Post-Hoc Analysis of Supplemental Oxygen in OHS (J Clin Sleep Med, 2016) [MEDLINE]
- After 2 Months of Follow-Up, Chronic Supplemental Oxygen Therapy Resulted in Marginal Changes that were Insufficient to Consider it as Beneficial or Deleterious
- Because Supplemental Oxygen Therapy Did Not Increase Hospital Resource Utilization, Authors Recommended Prescribing Supplemental Oxygen Therapy to Patients with OHS Who Meet Criteria with Close Monitoring
- Randomized Trial of Continuous Positive Airway Pressure (CPAP) vs Noninvasive Positive-Pressure Ventilation (NIPPV) in OHS (Thorax, 2017) [MEDLINE]: n = 60
- In Newly Diagnosed Severe OHS, Bilevel Positive Airway Pressure (BPAP) and CPAP Resulted in Similar Improvements in Ventilatory Failure, Health-Related Quality of Life (HRQOL), and Adherence
- Baseline pCO2 Predicted Persistent Ventilatory Failure on Treatment
- Long-Term Studies are Required to Determine Whether these Treatments Have Different Cost-Effectiveness or Impact on Mortality
- Nutrition and Exercise Rehabilitation in Obesity Hypoventilation (NERO) Pilot Study (Thorax, 2018) [MEDLINE]: n = 37
- A 3 Month Comprehensive Rehabilitation Program, in Addition to NIPPV, Resulted in iImproved Weight Loss, Exercise Capacity, and Quality of Life (QOL) at the end of the Rehabilitation Period, But These Effects Were Not Retained at 12 Months, in Part, Due to the Limited Retention of Patients in the Study at 12 Months
General Recommendations
- Obesity-Hypoventilation Syndrome with Coexistent Obstructive Sleep Apnea
- Continuous Positive Airway Pressure (CPAP) is Initially Recommended
- If the Patient is Intolerant of CPAP, Bilevel Positive Airway Pressure (BPAP) is Recommended
- If BPAP is Not Tolerated, Average Volume-Assured Pressure Support (or Volume-Cycled Ventilation) is Recommended
- Obesity-Hypoventilation Syndrome with Sleep-Associated Hypoventilation (without Frank Obstructive Sleep Apneas)
- Bilevel Positive Airway Pressure (BPAP) is Initially Recommended
- Obesity-Hypoventilation Syndrome with Acute Decompensation
- Bilevel Positive Airway Pressure (BPAP) is Recommended
Recommendations (Canadian Thoracic Society Clinical Practice Guideline for Home Mechanical Ventilation, 2011) (Can Respir J, 2011) [MEDLINE]
- NIPPV is the Treatment of Choice for OHS (Grade of 1A Recommendation)
- In Patients with OHS Who Have Minor Nocturnal Hypoxemia and No Nocturnal Hypercappnia, CPAP is a Reasonable Initial Therapy Provided that Follow-Up is Arranged Within 1-3 Months to Evaluate Response to Therapy (Grade of 1B Recommendation)
- When Access to More than One Device (Bilevel PAP or CPAP) is Limited, Bilevel Therapy is Recommended (Grade 1C Recommendation)
- In Patients with OHS Who Experience Significant Nocturnal Hypoxemia or Nocturnal Hypercapnia, Bilevel PAP Remains the Therapy of Choice (Grade 1B Recommendation)
- Polysomnography is Useful for Titrating and Confirming Efficacy of Bilevel Pressures (Grade 1C Recommendation)
Recommendations (Japanese Respiratory Society Noninvasive Positive Pressure Ventilation Guidelines, 2017) (Respir Investig, 2017) [MEDLINE]
- CPAP Should Be Used as a First-Line Treatment in Patients with Obesity-Hypoventilation Syndrome (Level III Evidence, Grade B Recommendation)
- If CPAP Therapy is Ineffective, Bilevel PAP Should Be Initiated (Level III Evidence, Grade C1 Recommendation)
Chronic Respiratory Failure Due to Ondine’s Curse (see Ondine’s Curse)
Etiology of Ondine’s Curse
- Congenital Central Hypoventilation Syndrome (C-CHS) (see xxxx): most common etiology of Ondine’s Curse
- Late-Onset Central Hypoventilation Syndrome (LO-CHS)
- Rapid-Onset Obesity with Hypothalamic Dysfunction, Hypoventilation, and Autonomic Dysregulation (ROHHAD) Syndrome
Recommendations (Canadian Thoracic Society Clinical Practice Guideline for Home Mechanical Ventilation, 2011) (Can Respir J, 2011) [MEDLINE]
- The Diagnosis of Central Hypoventilation Syndrome in Adults with Less Severe Hypoventilation is Best Made by Standard Polysomnography with the Addition of Transcutaneous Carbon Dioxide or Early Morning Arterial pCO2 (Grade 1C Recommendation)
- Once the Diagnosis of Central Hypoventilation Syndrome is Established, it is Strongly Recommended that Acquired Causes Should Be Excluded by Brainstem Magnetic Resonance Imaging (Grade 1C Recommendation)
- Patients with Central Hypoventilation Syndrome and No Known Acquired Cause Should Undergo Genetic Screening for the PHOX2B Gene Mutation (Grade 1C Recommendation)
- For Patients Confirmed to Harbor the PHOX2B Gene Mutation, First-Degree Relatives Should Be Offered Genetic Testing and Screening for Hypoventilation (Grade 1C Recommendation)
- Central Hypoventilation Syndrome Patients Who Require Only Nocturnal Ventilatory Support May Be Managed by NIPPV with a Backup Rate or Diaphragmatic Pacing (Grade 1C Recommendation)
- Severe Central Hypoventilation Syndrome, Mainly Seen in Congenital Central Hypoventilation Syndrome, Requires Continuous Invasive Ventilatory Support, But Daytime Diaphragmatic Pacing Can Markedly Improve Mobility and, as the Child Matures, NIPPV May Suffice (Grade 1C Recommendation)
Chronic Cheyne-Stokes Respiration (CSR) Due to Congestive Heart Failure (CHF)
Clinical Efficacy
- Randomized SERVE-HF Trial of Adaptive Servo-Ventilation for Central Sleep Apnea in Systolic Heart Failure (NEJM, 2015) [MEDLINE]: n = 1325 (with left ventricular ejection fraction ≤45%, apnea-hypopnea index/AHI) of ≥15 events per hour, and a predominance of central events)
- Adaptive Servo Ventilation Had No Significant Effect on the Primary End Point in Patients Who Had Heart Failure with Reduced Ejection Fraction and Predominantly Central Sleep Apnea, But All-Cause and Cardiovascular Mortality were Both Increased with This Therapy
Recommendations (Japanese Respiratory Society Noninvasive Positive Pressure Ventilation Guidelines, 2017) (Respir Investig, 2017) [MEDLINE]
- For CHF Patients with Cheyne-Stokes Respiration (CSR), CPAP Should Be First Initiated if Indicated (Level I Evidence, Grade B Recommendation)
- If CPAP Therapy is Ineffective, Active Servo Ventilation (ASV) Should Be Used (Level II Evidence, Grade B Recommendation)
- If CPAP Therapy is Ineffective, Bilevel PAP Should Be Used (Level III Evidence, Grade C1 Recommendation)
- If Positive-Pressure Ventilation is Ineffective or Not Tolerated, Oxygen Therapy Should Be Considered (Level II Evidence, Grade C1 Recommendation)
Need for Ventilatory Support During Exercise (During Pulmonary Rehabilitation) (see Pulmonary Rehabilitation)
Clinical Efficacy
- Analysis of Noninvasive Positive-Pressure During Pulmonary Rehabilitation in Patients with End-Stage Lung Disease Awaiting Lung Transplantation (Respiration, 2018) [MEDLINE]
- While Awaiting Lung Transplantation, Patients Treated with Nocturnal NIPPV Had an Increased Benefit of Pulmonary Rehabilitation, as Compared to Patients without Nocturnal NIPPV
Recommendations (Japanese Respiratory Society Noninvasive Positive Pressure Ventilation Guidelines, 2017) (Respir Investig, 2017) [MEDLINE]
- The Use of NPPV During Exercise Increases Exercise Duration and Intensity, Particularly in Patients with Severe Impairment of Pulmonary Function (Level II Evidence, Grade B Recommendation)
- Combining Exercise Rehabilitation with the Use of NPPV During Sleep is Effective for Improving Exercise Tolerance in Patients with Severely Impaired Pulmonary Function (Level II Evidence, Grade B Recommendation)
References
General
- International Consensus Conferences in Intensive Care Medicine: noninvasive positive pressure ventilation in acute Respiratory failure Am J Respir Crit Care Med. 2001 Jan;163(1):283-91 [MEDLINE]
- Effect of varying the pressurisation rate during noninvasive pressure support ventilation. Eur Respir J. 2004 Feb;23(2):314-20 [MEDLINE]
- Utilization of noninvasive ventilation in acute care hospitals: a regional survey. Chest. 2006;129(5):1226 [MEDLINE]
- Increased use of noninvasive ventilation in French intensive care units. Intensive Care Med. 2006;32(11):1747 [MEDLINE]
- Noninvasive ventilation in acute respiratory failure. Crit Care Med. 2007;35:2402-2407 [MEDLINE]
- Missed opportunities for noninvasive positive pressure ventilation: a utilization review. J Crit Care. 2008;23(1):111 [MEDLINE]
- Clinical practice guidelines for the use of noninvasive positive-pressure ventilation and noninvasive continuous positive airway pressure in the acute care setting. CMAJ. 2011 Feb 22; 183(3): E195–E214; doi: 10.1503/cmaj.100071 [MEDLINE]
- Patient-ventilator interaction during noninvasive ventilation. Respir Care. 2011 Feb;56(2):153-65; discussion 165-7. doi: 10.4187/respcare.01049 [MEDLINE]
- Clinical practice guidelines for the use of noninvasive positive-pressure ventilation and noninvasive continuous positive airway pressure in the acute care setting. CMAJ. 2011 Feb 22;183(3):E195-214. doi: 10.1503/cmaj.100071 [MEDLINE]
- Noninvasive ventilation: practical advice. Curr Opin Crit Care. 2013 Feb;19(1):1-8. doi: 10.1097/MCC.0b013e32835c34a5 [MEDLINE]
- Noninvasive ventilation for acute respiratory failure: a review of the literature and current guidelines. Intern Emerg Med. 2012 Dec;7(6):539-45. doi: 10.1007/s11739-012-0856-z [MEDLINE]
- Noninvasive ventilation and survival in acute care settings: a comprehensive systematic review and metaanalysis of randomized controlled trials. Crit Care Med. 2015 Apr;43(4):880-8. doi: 10.1097/CCM.0000000000000819 [MEDLINE]
- Official ERS/ATS clinical practice guidelines: noninvasive ventilation for acute respiratory failure. Eur Respir J. 2017 Aug 31;50(2). pii: 1602426. doi: 10.1183/13993003.02426-2016 [MEDLINE]
- The Japanese Respiratory Society Noninvasive Positive Pressure Ventilation (NPPV) Guidelines (second revised edition). Respir Investig. 2017 Jan;55(1):83-92. doi: 10.1016/j.resinv.2015.11.007 [MEDLINE]
Indications
Acute Respiratory Failure Due to Chronic Obstructive Pulmonary Disease (COPD) Exacerbation (see Chronic Obstructive Pulmonary Disease)
- Reversal of acute exacerbations of chronic obstructive lung disease by inspiratory assistance with a face mask. N Engl J Med. 1990;323:1523-1530 [MEDLINE]
- Noninvasive ventilation for acute exacerbations of chronic obstructive pulmonary disease. N Engl J Med. 1995 Sep 28;333(13):817-22 [MEDLINE]
- Noninvasive ventilatory support does not facilitate recovery from acute respiratory failure in chronic obstructive pulmonary disease. Eur Respir J. 1996 Jun;9(6):1240-5 [MEDLINE]
- Acute respiratory failure in patients with severe community-acquired pneumonia. A prospective randomized evaluation of noninvasive ventilation. Am J Respir Crit Care Med. 1999 Nov;160(5 Pt 1):1585-91 [MEDLINE]
- Noninvasive ventilation with helium-oxygen in acute exacerbations of chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2000 Apr;161(4 Pt 1):1191-200 [MEDLINE]
- Early use of non-invasive ventilation for acute exacerbations of chronic obstructive pulmonary disease on general respiratory wards: a multicentre randomised controlled trial. Lancet. 2000 Jun 3;355(9219):1931-5 [MEDLINE]
- Association of noninvasive ventilation with nosocomial infections and survival in critically ill patients. JAMA 2000; 284: 2361–2367 [MEDLINE]
- Non-invasive positive pressure ventilation to treat respiratory failure resulting from exacerbations of chronic obstructive pulmonary disease: Cochrane systematic review and meta-analysis. BMJ. 2003 Jan 25;326(7382):185 [MEDLINE]
- Cost effectiveness of ward based non-invasive ventilation for acute exacerbations of chronic obstructive pulmonary disease: economic analysis of randomised controlled trial. BMJ 2003; 326: 956–961 [MEDLINE]
- Secular trends in nosocomial infections and mortality associated with noninvasive ventilation in patients with exacerbation of COPD and pulmonary edema. JAMA 2003; 290: 2985–2991 [MEDLINE]
- Which patients with acute exacerbation of chronic obstructive pulmonary disease benefit from noninvasive positive-pressure ventilation? A systematic review of the literature. Ann Intern Med. 2003 Jun 3;138(11):861-70 [MEDLINE]
- Acute applications of noninvasive positive pressure ventilation. Chest 2003;124:699–713 [MEDLINE]
- Helium-oxygen versus air-oxygen noninvasive pressure support in decompensated chronic obstructive disease: A prospective, multicenter study. Crit Care Med. 2003 Mar;31(3):878-84 [MEDLINE]
- Non-invasive positive pressure ventilation for treatment of respiratory failure due to exacerbations of chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2004;(1):CD004104 [MEDLINE]
- Noninvasive positive-pressure ventilation to treat hypercapnic coma secondary to respiratory failure. Chest. 2005;127:952-960 [MEDLINE]
- A chart of failure risk for noninvasive ventilation in patients with COPD exacerbation. Eur Respir J. 2005 Feb;25(2):348-55 [MEDLINE]
- Noninvasive positive pressure ventilation in patients with acute exacerbations of COPD and varying levels of consciousness. Chest. 2005;128:1657-1666 [MEDLINE]
- Non-invasive ventilation in chronic obstructive pulmonary disease patients: Helmet versus facial mask. Intensive Care Med 2007;33:74–81 [MEDLINE]
- Noninvasive ventilation and survival in acute care settings: a comprehensive systematic review and metaanalysis of randomized controlled trials. Crit Care Med. 2015 Apr;43(4):880-8. doi: 10.1097/CCM.0000000000000819 [MEDLINE]
- Evidence-based Utilization of Noninvasive Ventilation and Patient Outcomes. Ann Am Thorac Soc. 2017 Nov;14(11):1667-1673. doi: 10.1513/AnnalsATS.201703-208OC [MEDLINE]
- Non-invasive ventilation for the management of acute hypercapnic respiratory failure due to exacerbation of chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2017 Jul 13;7:CD004104. doi: 10.1002/14651858.CD004104.pub4 [MEDLINE]
- Noninvasive ventilation with helium-oxygen mixture in hypercapnic COPD exacerbation: aggregate meta-analysis of randomized controlled trials. Ann Intensive Care. 2017 Dec;7(1):59. doi: 10.1186/s13613-017-0273-6 [MEDLINE]
Acute Respiratory Failure Due to Cardiogenic Pulmonary Edema/Congestive Heart Failure (CHF) Exacerbation (see Congestive Heart Failure)
- Acute left ventricular dysfunction during unsuccessful weaning from mechanical ventilation. Anesthesiology. 1988 Aug;69(2):171-9 [MEDLINE]
- Ventilatory and hemodynamic effects of continuous positive airway pressure in left heart failure. Am J Respir Crit Care Med. 1997 Feb;155(2):500-5 [MEDLINE]
- Association of noninvasive ventilation with nosocomial infections and survival in critically ill patients. JAMA 2000; 284: 2361–2367 [MEDLINE]
- Secular trends in nosocomial infections and mortality associated with noninvasive ventilation in patients with exacerbation of COPD and pulmonary edema. JAMA 2003; 290: 2985–2991 [MEDLINE]
- Randomized, prospective trial of oxygen, continuous positive airway pressure, and bilevel positive airway pressure by face mask in acute cardiogenic pulmonary edema. Crit Care Med. 2004;32(12):2407-2415 [MEDLINE]
- Noninvasive ventilation in acute cardiogenic pulmonary edema. JAMA 2005; 294: 3124-3130 [MEDLINE]
- Efficacy and safety of non-invasive ventilation in the treatment of acute cardiogenic pulmonary edema: a systematic review and meta-analysis. Crit Care 2006; 10:R69 [MEDLINE]
- The use of noninvasive ventilation in emergency department patients with acute cardiogenic pulmonary edema: a systematic review. Ann Emerg Med 2006; 48:260-269 [MEDLINE]
- Effect of non-invasive positive pressure ventilation (NIPPV) on mortality in patients with acute cardiogenic pulmonary oedema: a meta-analysis. Lancet. 2006 Apr 8;367(9517):1155-63 [MEDLINE]
- Noninvasive ventilation in acute cardiogenic pulmonary edema. N Engl J Med. 2008;359(2):142-151 [MEDLINE]
- Meta-analysis: noninvasive ventilation in acute cardiogenic pulmonary edema. Ann Intern Med 2010;152(9):590-600 [MEDLINE]
- Noninvasive ventilation and survival in acute care settings: a comprehensive systematic review and metaanalysis of randomized controlled trials. Crit Care Med. 2015 Apr;43(4):880-8. doi: 10.1097/CCM.0000000000000819 [MEDLINE]
- Evidence-based Utilization of Noninvasive Ventilation and Patient Outcomes. Ann Am Thorac Soc. 2017 Nov;14(11):1667-1673. doi: 10.1513/AnnalsATS.201703-208OC [MEDLINE]
- Noninvasive ventilation in acute hypoxemic respiratory failure: A systematic review and meta-analysis. J Crit Care. 2019 Feb;49:84-91. doi: 10.1016/j.jcrc.2018.10.012 [MEDLINE]
Acute Respiratory Failure in Immunocompromised Host
- Noninvasive ventilation for treatment of acute respiratory failure in patients undergoing solid organ transplantation: a randomized trial. JAMA 2000; 283:2239-2240 [MEDLINE]
- Noninvasive ventilation in immunosuppressed patients with pulmonary infiltrates, and acute respiratory failure. N Engl J Med 2001; 344:481-487 [MEDLINE]
- Predictors of noninvasive ventilation failure in patients with hematologic malignancy and acute respiratory failure. Crit Care Med. 2008;36(10):2766 [MEDLINE]
- Effect of Noninvasive Ventilation vs Oxygen Therapy on Mortality Among Immunocompromised Patients With Acute Respiratory Failure: A Randomized Clinical Trial. JAMA. 2015 Oct 27;314(16):1711-9. doi: 10.1001/jama.2015.12402 [MEDLINE]
- Noninvasive ventilation in acute hypoxemic respiratory failure: A systematic review and meta-analysis. J Crit Care. 2019 Feb;49:84-91. doi: 10.1016/j.jcrc.2018.10.012 [MEDLINE]
Acute Respiratory Failure Due to Pneumonia
- Non-invasive mechanical ventilation in acute respiratory failure due to chronic obstructive pulmonary disease: correlates for success. Thorax 1995 Jul;50(7):755-7 [MEDLINE]
- Acute respiratory failure in patients with severe community-acquired pneumonia. A prospective randomized evaluation of noninvasive ventilation. Am J Respir Crit Care Med 1999; 60(5 Pt 1):1585-91 [MEDLINE]
- Oxygen therapy for pneumonia in adults. Cochrane Database Syst Rev. 2012 [MEDLINE]
- Early non-invasive ventilation treatment for severe influenza pneumonia. Clin Microbiol Infect. 2013 Mar;19(3):249-56. doi: 10.1111/j.1469-0691.2012.03797.x [MEDLINE]
- Noninvasive ventilation and survival in acute care settings: a comprehensive systematic review and metaanalysis of randomized controlled trials. Crit Care Med. 2015 Apr;43(4):880-8. doi: 10.1097/CCM.0000000000000819 [MEDLINE]
- Failure of Noninvasive Ventilation for De Novo Acute Hypoxemic Respiratory Failure: Role of Tidal Volume. Crit Care Med. 2016 Feb;44(2):282-90. doi: 10.1097/CCM.0000000000001379 [MEDLINE]
- Noninvasive Ventilation in Acute Hypoxemic Nonhypercapnic Respiratory Failure: A Systematic Review and Meta-Analysis. Crit Care Med. 2017 Jul;45(7):e727-e733. doi: 10.1097/CCM.0000000000002361 [MEDLINE]
- Association Between Noninvasive Ventilation and Mortality Among Older Patients With Pneumonia. Crit Care Med. 2017 Mar;45(3):e246-e254. doi: 10.1097/CCM.0000000000002076 [MEDLINE]
- Risk Factors for Noninvasive Ventilation Failure in Critically Ill Subjects With Confirmed Influenza Infection. Respir Care. 2017 Oct;62(10):1307-1315. doi: 10.4187/respcare.05481 [MEDLINE]
- Noninvasive ventilation in acute hypoxemic respiratory failure: A systematic review and meta-analysis. J Crit Care. 2019 Feb;49:84-91. doi: 10.1016/j.jcrc.2018.10.012 [MEDLINE]
Acute Respiratory Failure Due to Acute Respiratory Distress Syndrome (ARDS)
- The use of non-invasive ventilation for life-threatening asthma attacks: Changes in the need for intubation. Respirology. 2010 May;15(4):714-20. doi: 10.1111/j.1440-1843.2010.01766.x [MEDLINE]
- Non-invasive positive pressure ventilation for treatment of respiratory failure due to severe acute exacerbations of asthma. Cochrane Database Syst Rev 2012 Dec 12; 12:CD004360. doi: 10.1002/14651858.CD004360.pub4 [MEDLINE]
- Noninvasive Ventilation Coupled With Nebulization During Asthma Crises: A Randomized Controlled Trial. Respiratory Care February 1, 2013 vol. 58 no. 2 241-249 [MEDLINE]
- Noninvasive ventilation and survival in acute care settings: a comprehensive systematic review and metaanalysis of randomized controlled trials. Crit Care Med. 2015 Apr;43(4):880-8. doi: 10.1097/CCM.0000000000000819 [MEDLINE]
- Effect of Noninvasive Ventilation Delivered by Helmet vs Face Mask on the Rate of Endotracheal Intubation in Patients With Acute Respiratory Distress Syndrome: A Randomized Clinical Trial. JAMA. 2016;315(22):2435 [MEDLINE]
- Failure of Noninvasive Ventilation for De Novo Acute Hypoxemic Respiratory Failure: Role of Tidal Volume. Crit Care Med. 2016 Feb;44(2):282-90. doi: 10.1097/CCM.0000000000001379 [MEDLINE]
- Can High-flow Nasal Cannula Reduce the Rate of Endotracheal Intubation in Adult Patients With Acute Respiratory Failure Compared With Conventional Oxygen Therapy and Noninvasive Positive Pressure Ventilation?: A Systematic Review and Meta-analysis. Chest. 2017;151(4):764 [MEDLINE]
- Effect of high-flow nasal cannula oxygen therapy in adults with acute hypoxemic respiratory failure: a meta-analysis of randomized controlled trials. CMAJ. 2017;189(7):E260 [MEDLINE]
- Noninvasive Ventilation of Patients with Acute Respiratory Distress Syndrome. Insights from the LUNG SAFE Study. Am J Respir Crit Care Med. 2017 Jan 1;195(1):67-77. doi: 10.1164/rccm.201606-1306OC [MEDLINE]
- Noninvasive Ventilation in Acute Hypoxemic Nonhypercapnic Respiratory Failure: A Systematic Review and Meta-Analysis. Crit Care Med. 2017 Jul;45(7):e727-e733. doi: 10.1097/CCM.0000000000002361 [MEDLINE]
- Effect of Helmet Noninvasive Ventilation vs High-Flow Nasal Oxygen on Days Free of Respiratory Support in Patients With COVID-19 and Moderate to Severe Hypoxemic Respiratory Failure: The HENIVOT Randomized Clinical Trial. JAMA. 2021 May 4;325(17):1731-1743. doi: 10.1001/jama.2021.4682 [MEDLINE]
- Outcomes of Noninvasive Positive Pressure Ventilation in Acute Respiratory Distress Syndrome and Their Predictors: A National Cohort. Crit Care Res Pract. 2019 Sep 18;2019:8106145. doi: 10.1155/2019/8106145. eCollection 2019 [MEDLINE]
Acute Respiratory Failure Due to Asthma Exacerbation (see Asthma)
- Outcomes of Noninvasive and Invasive Ventilation in Patients Hospitalized with Asthma Exacerbation. Ann Am Thorac Soc. 2016 Jul;13(7):1096-104 [MEDLINE]
Acute Respiratory Failure Due to Interstitial Pneumonia
- Non-invasive mechanical ventilation in patients with diffuse interstitial lung diseases. BMC Pulm Med. 2014 Dec 5;14:194. doi: 10.1186/1471-2466-14-194 [MEDLINE]
Acute Respiratory Failure Due to Neuromuscular Disease
- BiPAP in acute respiratory failure due to myasthenic crisis may prevent intubation. Neurology. 2002 Nov 26;59(10):1647-9 [MEDLINE]
- Mechanisms of improvement of respiratory failure in patients with restrictive thoracic disease treated with non-invasive ventilation. Thorax. 2005;60(9):754 [MEDLINE]
- Recent advances in respiratory care for neuromuscular disease. Chest. 2006;130(6):1879 [MEDLINE]
- Noninvasive Ventilation for Patients Presenting With Acute Respiratory Failure: The Randomized Controlled Trials. Respir Care 2009;54(1):116-124 [MEDLINE]
- Respiratory function assessment and intervention in neuromuscular disorders. Curr Opin Neurol. 2005 Oct;18(5):543-7 [MEDLINE]
- Update on respiratory management of critically ill neurologic patients. Curr Neurol Neurosci Rep 2005; 5:476–482 [MEDLINE]
- BiPAP in early guillain-barré syndrome may fail. Can J Neurol Sci. 2006 Feb;33(1):105-6 [MEDLINE]
- Noninvasive ventilation in myasthenic crisis. Arch Neurol. 2008 Jan;65(1):54-8. doi: 10.1001/archneurol.2007.1 [MEDLINE]
- Pulmonary issues in patients with chronic neuromuscular disease. Am J Respir Crit Care Med Vol 187, Iss. 10, pp 1046-1055, May 15, 2013 [MEDLINE]
- Noninvasive ventilation for neuromuscular respiratory failure: when to use and when to avoid. Curr Opin Crit Care. 2016 Apr;22(2):94-9. doi: 10.1097/MCC.0000000000000284 [MEDLINE]
Acute Respiratory Failure Due to Restrictive Thoracic Disease
- Invasive and noninvasive ventilation in the emergency department. Emerg Med Clin North Am. 2012 May;30(2):421-49, ix. doi: 10.1016/j.emc.2011.10.008 [MEDLINE]
- Management of kyphoscoliosis patients with respiratory failure in the intensive care unit and during long term follow up. Multidiscip Respir Med. 2012 Sep 21;7(1):30. doi: 10.1186/2049-6958-7-30 [MEDLINE]
Acute Respiratory Failure Due to Obesity-Hypoventilation Syndrome (OHS) (see Obesity-Hypoventilation Syndrome)
- Short-term and long-term effects of nasal intermittent positive pressure ventilation in patients with obesity-hypoventilation syndrome. Chest. 2005;128(2):587 [MEDLINE]
- Noninvasive ventilation in acute hypercapnic respiratory failure caused by obesity hypoventilation syndrome and chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2012 Dec;186(12):1279-85 [MEDLINE]
- Determinants of noninvasive ventilation success or failure in morbidly obese patients in acute respiratory failure. PLoS One. 2014;9(5):e97563 [MEDLINE]
- Predictors of noninvasive ventilation failure in critically ill obese patients: a brief narrative review. Adv Respir Med. 2017;85(5):264-270. doi: 10.5603/ARM.a2017.0044 [MEDLINE]
- Obesity and perioperative noninvasive ventilation in bariatric surgery. Minerva Chir. 2017 Jun;72(3):248-264. doi: 10.23736/S0026-4733.17.07310-2 [MEDLINE]
- Noninvasive Ventilation in the Critically Ill Patient With Obesity Hypoventilation Syndrome: A Review. J Intensive Care Med. 2017 Aug;32(7):421-428. doi: 10.1177/0885066616663179 [MEDLINE]
Postoperative Acute Respiratory Failure
- Noninvasive ventilation reduces mortality in acute respiratory failure following lung resection. Am J Respir Crit Care Med. 2001 Oct 1;164(7):1231-5 [MEDLINE]
- Effects of non-invasive ventilation on reintubation rate: A systematic review and meta-analysis of randomised studies of patients undergoing cardiothoracic surgery. Crit Care Resusc 2013;15:220–7 [MEDLINE]
- Efficacy and safety of noninvasive positive pressure ventilation in the treatment of acute respiratory failure after cardiac surgery. Chin Med J (Engl) 2013;126:4463–9 [MEDLINE]
- Non-invasive positive pressure ventilation for prevention of complications after pulmonary resection in lung cancer patients. Cochrane Database Syst Rev. 2015 Sep 25;9:CD010355. doi: 10.1002/14651858.CD010355.pub2 [MEDLINE]
- Noninvasive ventilation and survival in acute care settings: a comprehensive systematic review and metaanalysis of randomized controlled trials. Crit Care Med. 2015 Apr;43(4):880-8. doi: 10.1097/CCM.0000000000000819 [MEDLINE]
- NIVAS Trial. Effect of Noninvasive Ventilation on Tracheal Reintubation Among Patients With Hypoxemic Respiratory Failure Following Abdominal Surgery: A Randomized Clinical Trial. JAMA. 2016 Apr 5;315(13):1345-53. doi: 10.1001/jama.2016.2706 [MEDLINE]
- Nonsurgical Strategies to Reduce Mortality in Patients Undergoing Cardiac Surgery: An Updated Consensus Process. J Cardiothorac Vasc Anesth. 2018 Feb;32(1):225-235. doi: 10.1053/j.jvca.2017.06.017 [MEDLINE]
Acute Respiratory Failure Due to Chest Trauma
- Treatment of multiple rib fractures. Randomized controlled trial comparing ventilatory with nonventilatory management. Chest 1990; 97: 943–948 [MEDLINE]
- A comparative study of continuous positive airway pressure (CPAP) and intermittent positive pressure ventilation (IPPV) in patients with flail chest. Emerg Med J 2005; 22: 325–329 [MEDLINE]
- Noninvasive ventilation reduces intubation in chest trauma-related hypoxemia: a randomized clinical trial. Chest 2010; 137: 74–80 [MEDLINE]
Facilitation of Early Extubation
- Noninvasive positive pressure ventilation as a weaning strategy for intubated adults with respiratory failure. Cochrane Database Syst Rev. 2003;(4):CD004127[MEDLINE]
- Use of non-invasive ventilation to wean critically ill adults off invasive ventilation: meta-analysis and systematic review. BMJ. 2009 May 21;338:b1574. doi: 10.1136/bmj.b1574 [MEDLINE]
- Noninvasive positive pressure ventilation as a weaning strategy for intubated adults with respiratory failure. Cochrane Database Syst Rev. 2010 Aug 4;(8):CD004127. doi: 10.1002/14651858.CD004127.pub2 [MEDLINE]
- Noninvasive ventilation as a weaning strategy for mechanical ventilation in adults with respiratory failure: a Cochrane systematic review. CMAJ. 2014 Feb 18;186(3):E112-22. doi: 10.1503/cmaj.130974 [MEDLINE]
- Noninvasive ventilation and survival in acute care settings: a comprehensive systematic review and metaanalysis of randomized controlled trials. Crit Care Med. 2015 Apr;43(4):880-8. doi: 10.1097/CCM.0000000000000819 [MEDLINE]
- An Official American Thoracic Society/American College of Chest Physicians Clinical Practice Guideline: Liberation from Mechanical Ventilation in Critically Ill Adults. Chest. 2017 Jan;151(1):166-180. doi: 10.1016/j.chest.2016.10.036 [MEDLINE]
- Non-invasive ventilation as a strategy for weaning from invasive mechanical ventilation: a systematic review and Bayesian meta-analysis. Intensive Care Med. 2018;44(12):2192 [MEDLINE]
- Early extubation followed by immediate noninvasive ventilation vs. standard extubation in hypoxemic patients: a randomized clinical trial. Intensive Care Med. 2018 Dec 10. doi: 10.1007/s00134-018-5478-0 [MEDLINE]
- Effect of Protocolized Weaning With Early Extubation to Noninvasive Ventilation vs Invasive Weaning on Time to Liberation From Mechanical Ventilation Among Patients With Respiratory Failure: The Breathe Randomized Clinical Trial. JAMA. 2018 Nov 13;320(18):1881-1888. doi: 10.1001/jama.2018.13763 [MEDLINE]
- Early extubation followed by immediate noninvasive ventilation vs. standard extubation in hypoxemic patients: a randomized clinical trial. Intensive Care Med. 2019;45(1):62 [MEDLINE]
Post-Extubation Prophylaxis
- Nasal-continuous positive airway pressure reduces pulmonary morbidity and length of hospital stay following thoracoabdominal aortic surgery. Chest. 2005 Aug;128(2):821-8 [MEDLINE]
- Early noninvasive ventilation averts extubation failure in patients at risk: a randomized trial. Am J Respir Crit Care Med. 2006 Jan 15;173(2):164-70. Epub 2005 Oct 13 [MEDLINE]
- Continuous positive airway pressure for treatment of respiratory complications after abdominal surgery: a systematic review and meta-analysis. Ann Surg. 2008 Apr;247(4):617-26. doi: 10.1097/SLA.0b013e3181675829 [MEDLINE]
- Non-invasive ventilation after extubation in hypercapnic patients with chronic respiratory disorders: randomised controlled trial. Lancet. 2009 Sep 26;374(9695):1082-8. doi: 10.1016/S0140-6736(09)61038-2. Epub 2009 Aug 12 [MEDLINE]
- Noninvasive ventilation to prevent respiratory failure after extubation in high-risk patients. Crit Care Med. 2005 Nov;33(11):2465-70 [MEDLINE]
- Effects of non-invasive ventilation on reintubation rate: A systematic review and meta-analysis of randomised studies of patients undergoing cardiothoracic surgery. Crit Care Resusc 2013;15:220–7 [MEDLINE]
- Noninvasive ventilation and survival in acute care settings: a comprehensive systematic review and metaanalysis of randomized controlled trials. Crit Care Med. 2015 Apr;43(4):880-8. doi: 10.1097/CCM.0000000000000819 [MEDLINE]
- Easily identified at-risk patients for extubation failure may benefit from noninvasive ventilation: a prospective before–after study. Crit Care 2016; 20: 48 [MEDLINE]
- An Official American Thoracic Society/American College of Chest Physicians Clinical Practice Guideline: Liberation from Mechanical Ventilation in Critically Ill Adults. Chest. 2017 Jan;151(1):166-180. doi: 10.1016/j.chest.2016.10.036 [MEDLINE]
- Effect of Noninvasive Ventilation After Unplanned Extubation. Respir Care. 2018 Nov 6. pii: respcare.06328. doi: 10.4187/respcare.06328 [MEDLINE]
Extubation Failure
- Effect of failed extubation on the outcome of mechanical ventilation. Chest. 1997 Jul;112(1):186-92 [MEDLINE]
- Unplanned extubation: risk factors of development and predictive criteria for reintubation. Crit Care Med. 1998 Jun;26(6):1049-53 [MEDLINE]
- Noninvasive pressure support ventilation in COPD patients with postextubation hypercapnic respiratory insufficiency. Eur Respir J. 1998 Jun;11(6):1349-53 [MEDLINE]
- Noninvasive positive-pressure ventilation for postextubation respiratory distress: a randomized controlled trial. JAMA. 2002 Jun 26;287(24):3238-44 [MEDLINE]
- Noninvasive positive-pressure ventilation for respiratory failure after extubation. N Engl J Med. 2004 Jun 10;350(24):2452-60 [MEDLINE]
- Early noninvasive ventilation averts extubation failure in patients at risk: a randomized trial. Am J Respir Crit Care Med. 2006 Jan 15;173(2):164-70. Epub 2005 Oct 13 [MEDLINE]
- Risk factors for extubation failure in patients following a successful spontaneous breathing trial. Chest. 2006;130(6):1664-1671 [MEDLINE]
- Non-invasive ventilation after extubation in hypercapnic patients with chronic respiratory disorders: randomised controlled trial. Lancet. 2009 Sep 26;374(9695):1082-8. doi: 10.1016/S0140-6736(09)61038-2. Epub 2009 Aug 12 [MEDLINE]
- The role of non-invasive positive pressure ventilation in post-extubation respiratory failure: An evaluation using meta-analytic techniques. Indian J Crit Care Med. 2013 Jul;17(4):253-61. doi: 10.4103/0972-5229.118477 [MEDLINE]
- The efficacy of noninvasive ventilation in managing postextubation respiratory failure: a meta-analysis. Heart Lung. 2014 Mar-Apr;43(2):99-104. doi: 10.1016/j.hrtlng.2014.01.002 [MEDLINE]
- Noninvasive ventilation and survival in acute care settings: a comprehensive systematic review and metaanalysis of randomized controlled trials. Crit Care Med. 2015 Apr;43(4):880-8. doi: 10.1097/CCM.0000000000000819 [MEDLINE]
Acute Respiratory Failure in “Do Not Intubate” (DNI) Patients
- Outcomes of patients with do-not-intubate orders treated with noninvasive ventilation. Crit Care Med. 2004 Oct;32(10):2002-7 [MEDLINE]
- Noninvasive positive pressure ventilation reverses acute respiratory failure in select “do-not-intubate” patients. Crit Care Med. 2005 Sep;33(9):1976-82 [MEDLINE]
- Palliative noninvasive ventilation in patients with acute respiratory failure. Intensive Care Med. 2011 Aug;37(8):1250-7. doi: 10.1007/s00134-011-2263-8. Epub 2011 Jun 9 [MEDLINE]
- Results of noninvasive ventilation in very old patients. Ann Intensive Care. 2012 Feb 21;2(1):5. doi: 10.1186/2110-5820-2-5 [MEDLINE]
- Noninvasive mechanical ventilation in patients having declined tracheal intubation. Intensive Care Med. 2013 Feb;39(2):292-301. doi: 10.1007/s00134-012-2746-2 [MEDLINE]
- Role of sedation for agitated patients undergoing noninvasive ventilation: clinical practice in a tertiary referral hospital. BMC Pulm Med. 2015 Jul 13;15:71. doi: 10.1186/s12890-015-0072-5 [MEDLINE]
- The Role of Noninvasive Ventilation in Patients with “Do Not Intubate” Order in the Emergency Setting. PLoS One. 2016 Feb 22;11(2):e0149649. doi: 10.1371/journal.pone.0149649. eCollection 2016 [MEDLINE]
Respiratory Support During Endoscopic Procedures
- Continuous positive airway pressure during fiberoptic bronchoscopy in hypoxemic patients. A randomized double-blind study using a new device. Am J Respir Crit Care Med 2000; 162: 1063–1067 [MEDLINE]
- Noninvasive positive-pressure ventilation vs. conventional oxygen supplementation in hypoxemic patients undergoing diagnostic bronchoscopy. Chest 2002; 121: 1149–1154 [MEDLINE]
- Mask adaptor – a novel method of positive pressure ventilation during propofol deep sedation for upper GI endoscopy. Gastrointest Endosc 2008; 68: 127–131 [MEDLINE]
- Non-invasive ventilation-aided transesophageal echocardiography in high-risk patients: a pilot study. Eur J Echocardiogr 2010; 11: 554–556 [MEDLINE]
- Anesthetic management of transcatheter aortic valve implantation with transaxillary approach. J Cardiothorac Vasc Anesth 2011; 25: 437–443 [MEDLINE]
- Non-invasive ventilation during upper endoscopies in adult patients. A systematic review. Minerva Anestesiol 2013; 79: 683–694 [MEDLINE]
- Utility of noninvasive ventilation in high-risk patients during endoscopic retrograde cholangiopancreatography. Lung India 2014; 31: 331–335 [MEDLINE]
- High-flow nasal cannula oxygen versus non-invasive ventilation in patients with acute hypoxaemic respiratory failure undergoing flexible bronchoscopy – a prospective randomised trial. Crit Care 2014; 18: 712 [MEDLINE]
- Prolonged transesophageal echocardiography during percutaneous closure of the left atrial appendage without general anesthesia: the utility of the Janus mask. Can J Anaesth 2016; 63: 962–965 [MEDLINE]
Chronic Respiratory Failure Due to Chronic Obstructive Pulmonary Disease (COPD) (see Chronic Obstructive Pulmonary Disease)
- Clinical indications for noninvasive positive pressure ventilation in chronic respiratory failure due to restrictive lung disease, COPD, and nocturnal hypoventilation–a consensus conference report. Chest. 1999 Aug;116(2):521-34 [MEDLINE]
- AVCAL Study. Nocturnal non-invasive nasal ventilation in stable hypercapnic COPD: a randomised controlled trial. Thorax. 2009;64(7):561 [MEDLINE]
- Guidelines for non-invasive and invasive mechanical ventilation for treatment of chronic respiratory failure. Published by the German Society for Pneumology (DGP). Pneumologie. 2010 Oct;64(10):640-52 [MEDLINE]
- Noninvasive positive pressure ventilation for stable outpatients: CPAP and beyond. Cleve Clin J Med. 2010 Oct;77(10):705-14 [MEDLINE]
- High pressure versus high intensity noninvasive ventilation in stable hypercapnic chronic obstructive pulmonary disease: a randomized crossover trial. Int J Chron Obstruct Pulmon Dis. 2012;7:811 [MEDLINE]
- Nocturnal non-invasive positive pressure ventilation for stable chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2013 [MEDLINE]
- Non-invasive positive pressure ventilation for the treatment of severe stable chronic obstructive pulmonary disease: a prospective, multicentre, randomised, controlled clinical trial. Lancet Respir Med. 2014;2(9):698 [MEDLINE]
- Effect of Home Noninvasive Ventilation With Oxygen Therapy vs Oxygen Therapy Alone on Hospital Readmission or Death After an Acute COPD Exacerbation: A Randomized Clinical Trial. JAMA. 2017;317(21):2177 [MEDLINE]
- Non-invasive Positive Airway Pressure in Obesity Hypoventilation Syndrome and Chronic Obstructive Pulmonary Disease: Present and Future Perspectives. COPD. 2017 Aug;14(4):418-428. doi: 10.1080/15412555.2017.1317730 [MEDLINE]
Chronic Respiratory Failure Due to Neuromuscular Disease
- Mechanisms of improvement of respiratory failure in patients with restrictive thoracic disease treated with non-invasive ventilation. Thorax. 2005;60(9):754 [MEDLINE]
- Recent advances in respiratory care for neuromuscular disease. Chest. 2006;130(6):1879 [MEDLINE]
- Respiratory function assessment and intervention in neuromuscular disorders. Curr Opin Neurol. 2005 Oct;18(5):543-7 [MEDLINE]
- Pulmonary issues in patients with chronic neuromuscular disease. Am J Respir Crit Care Med Vol 187, Iss. 10, pp 1046-1055, May 15, 2013 [MEDLINE]
- Mechanical ventilation for amyotrophic lateral sclerosis/motor neuron disease. Cochrane Database Syst Rev. 2013 Mar 28;(3):CD004427. doi: 10.1002/14651858.CD004427.pub3 [MEDLINE]
- Duchenne muscular dystrophy: life prolongation by noninvasive ventilatory support. Am J Phys Med Rehabil. 2014 Jul;93(7):595-9. doi: 10.1097/PHM.0000000000000074 [MEDLINE]
Chronic Respiratory Failure Due to Obesity-Hypoventilation Syndrome (OHS) (see Obesity-Hypoventilation Syndrome)
- The obesity hypoventilation syndrome can be treated with noninvasive mechanical ventilation. Chest. 2001;119(4):1102 [MEDLINE]
- The obesity hypoventilation syndrome. Am J Med. 2005;118(9):948 [MEDLINE]
- The Effect of Supplemental Oxygen in Obesity Hypoventilation Syndrome. J Clin Sleep Med. 2016 Oct 15;12(10):1379-1388 [MEDLINE]
- Non-invasive Positive Airway Pressure in Obesity Hypoventilation Syndrome and Chronic Obstructive Pulmonary Disease: Present and Future Perspectives. COPD. 2017 Aug;14(4):418-428. doi: 10.1080/15412555.2017.1317730 [MEDLINE]
- CPAP or non-invasive ventilation in obesity hypoventilation syndrome: does it matter which one you start with? Thorax. 2017 May;72(5):398-399. doi: 10.1136/thoraxjnl-2016-209607 [MEDLINE]
- A randomised controlled trial of CPAP versus non-invasive ventilation for initial treatment of obesity hypoventilation syndrome. Thorax. 2017 May;72(5):437-444. doi: 10.1136/thoraxjnl-2016-208559 [MEDLINE]
- Nutrition and Exercise Rehabilitation in Obesity hypoventilation syndrome (NERO): a pilot randomised controlled trial. Thorax. 2018 Jan;73(1):62-69. doi: 10.1136/thoraxjnl-2016-209826 [MEDLINE]
Chronic Respiratory Failure Due to Restrictive Thoracic Disease
- Noninvasive ventilatory support during sleep improves respiratory failure in kyphoscoliosis. Chest. 1988 Oct;94(4):811-5 [MEDLINE]
- Survival of patients with kyphoscoliosis receiving mechanical ventilation or oxygen at home. Chest. 2006 Dec;130(6):1828-33 [MEDLINE]
- Predictors of mortality in chest wall disease treated with noninvasive home mechanical ventilation. Respir Med. 2010 Dec;104(12):1843-9. doi: 10.1016/j.rmed.2010.08.013 [MEDLINE]
- Home mechanical ventilation: a Canadian Thoracic Society clinical practice guideline. Can Respir J. 2011 Jul-Aug;18(4):197-215 [MEDLINE]
- Efficacy of noninvasive volume targeted ventilation in patients with chronic respiratory failure due to kyphoscoliosis. Adv Exp Med Biol. 2015;838:53-8. doi: 10.1007/5584201468 [MEDLINE]
Chronic Respiratory Failure Due to Cheyne-Stokes Respiration (CSR) Due to Congestive Heart Failure (CHF) (see xxxx and xxxx)
- SERVE-HF Trial. Adaptive Servo-Ventilation for Central Sleep Apnea in Systolic Heart Failure. N Engl J Med. 2015 Sep 17;373(12):1095-105. doi: 10.1056/NEJMoa1506459 [MEDLINE]
- Sleep-disordered Breathing in Heart Failure. Eur Cardiol. 2015 Dec;10(2):89-94. doi: 10.15420/ecr.2015.10.2.89 [MEDLINE]
Need for Ventilatory Support During Exercise (During Pulmonary Rehabilitation) (see Pulmonary Rehabilitation)
- Impact of Nocturnal Noninvasive Ventilation on Pulmonary Rehabilitation in Patients with End-Stage Lung Disease Awaiting Lung Transplantation. Respiration. 2018;95(3):161-168. doi: 10.1159/000484056 [MEDLINE]