In 1948, Graham First Described the Middle Lobe Syndrome in 12 Patients with Atelectasis and Nontuberculous Pneumonitis of the Right Middle Lobe (Postgrad Med, 1948) [MEDLINE]
These Cases Had Presumed (But Not Bronchoscopically–Proven) Airway Compression by Peribronchial Enlarged Lymph Nodes
In 1955, Effler and Ervin Published a Review on the Anatomic and Clinical Features of the Middle Lobe Syndrome (Am Rev Tuberc, 1955) [MEDLINE]
They Defined Middle Lobe Syndrome as a “Suppurative Process Which is Characterized by Recurrent Pneumonitis, Productive Cough, Recurrent Fever, and Frequent Hemoptyses”
They Stated “The Middle Lobe Syndrome Begins with a Phase of Obstructive Pneumonitis and Terminates with a Phase in Which There is Destruction of the Lung Parenchyma Distal to the Point of Obstruction”
In 1966, Culiner Described the Middle Lobe Syndrome as “Obstructive Atelectasis of This Lobe, with the Obstruction Being Attributed to Compression by Peribronchial Nodes” (Dis Chest, 1966) [MEDLINE]
Definition
Middle Lobe Syndrome is Most Consistently Defined in the Medical Literature as Recurrent or Chronic Right Middle Lobe Atelectasis (Collapse or Volume Loss) (see Atelectasis) (Postgrad Med, 1948) [MEDLINE] (Dis Chest, 1966) [MEDLINE] (Thorax, 1980) [MEDLINE] (Respiration, 2012) [MEDLINE]
A Similar Syndrome May Occur in the Lingula, Being Termed the “Lingula Syndrome” (Chest, 2004) [MEDLINE]
Epidemiology
Middle Lobe Syndrome is Considered to Be a Rare Clinical Entity, But its Epidemiology Has Not Been Well-Described in the Medical Literature (Thorax, 1980) [MEDLINE] (Respiration, 2012) [MEDLINE]
Middle Lobe Syndrome Has Been Described in Childen and Adults of Both Sexes
Middle Lobe Syndrome Has Been Described in Both Primary and Tertiary Care Settings
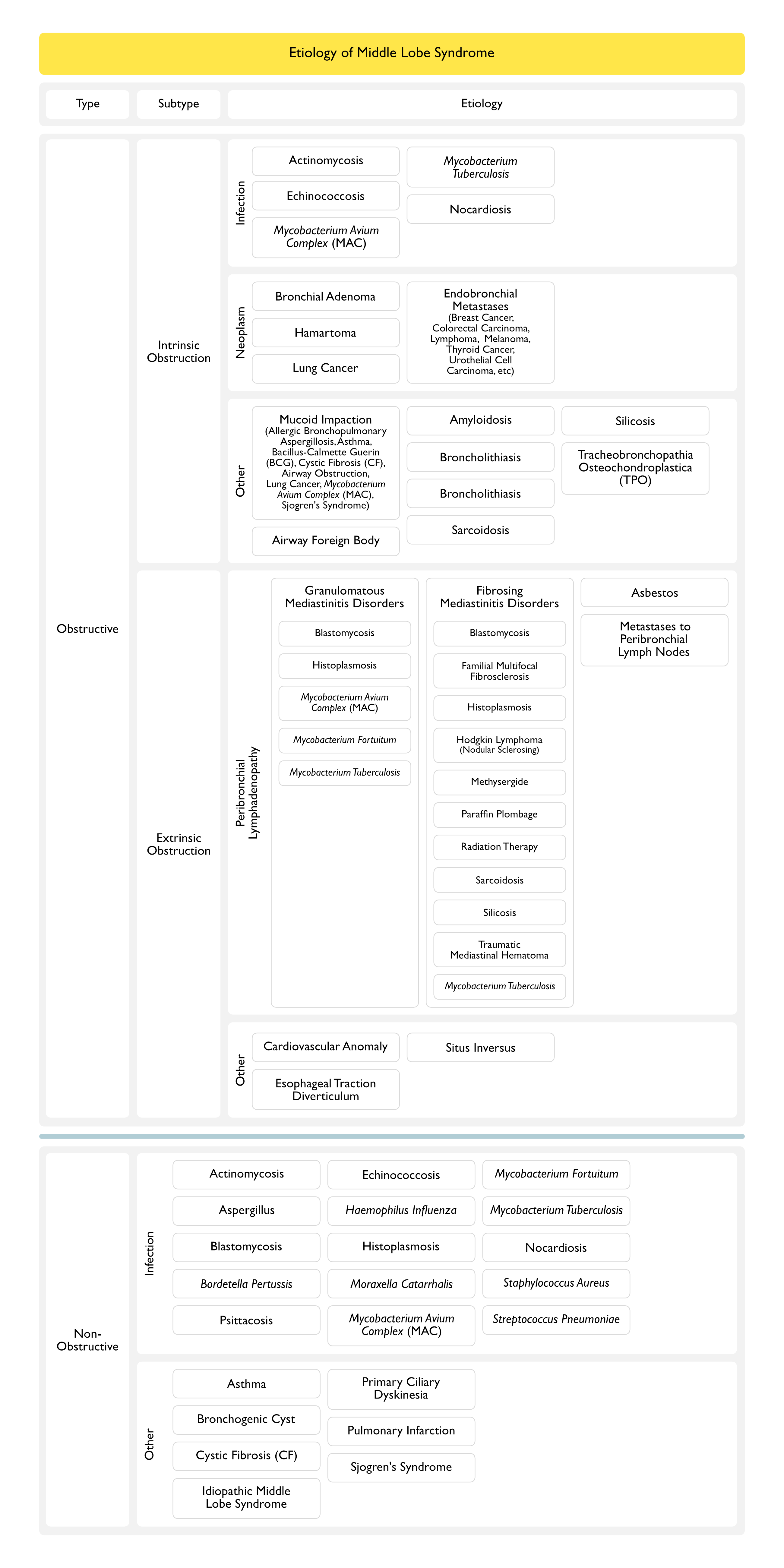
Non-Obstructive Middle Lobe Syndrome Appears to Be More Common than Obstructive Middle Lobe Syndrome (Clin Respir J, 2009) [MEDLINE]
Incidence
In a National Study from Iceland, the Incidence of Middle Lobe Syndrome Requiring Surgical Resection was Defined (JAMA, 1966) [MEDLINE]
Male: 1.43 milion males per year
Female: 2.94 milion females per year
Sex-Predominance
Middle Lobe Syndrome is More Common in Females
The F:M Ratio is 1.5-3.0 in Most Studies (Respiration, 2012) [MEDLINE]
Family History of Atopy
Family History of Atopy, Asthma, Chronic Obstructive Pulmonary Disease are Present in Up to 50% of Cases (Thorax, 1980) [MEDLINE] (Clin Respir J, 2009) [MEDLINE] (Respiration, 2012) [MEDLINE]
However, as Noted Below, Most Cases of Middle Lobe Syndrome Associated with Nontuberculous Mycobacteria Have a Patent Right Middle Lobe Bronchus (Dis Chest, 1966) [MEDLINE]
Endobronchial Submucosal “Pearls” May Be Seen in HIV Patients (Biopsy of These is Usually Positive for Acid-Fast Bacilli)
Mycobacterium Tuberculosis (Tuberculosis) (see Tuberculosis)
Neoplasms (Benign and Malignant) Account for Approximately 25% of Middle Lobe Syndrome Cases (Although Many Middle Lobe Syndrome Studies Have Excluded Patients with Identifiable Neoplasms) (Respiration, 2012) [MEDLINE]
Non-Obstructive Middle Lobe Syndrome is Characterized by Absence of Demonstrable Right Middle Lobe Bronchus Obstruction by Bronchoscopy
Non-Obstructive Cases May Also Manifest Pathology in the Lingula on the Left Side (“Lingula Syndrome”) (Chest, 2004) [MEDLINE]
Non-Obstructive Middle Lobe Syndrome Commonly Manifests as Recurrent Pneumonia in Association with Asthma, Bronchitis, or Cystic Fibrosis (JAMA, 1966) [MEDLINE] (J Maine Med Assoc, 1972) [MEDLINE] (Arch Dis Child, 1992) [MEDLINE]
Most Cases of Middle Lobe Syndrome Associated with Nontuberculous Mycobacteria Have a Patent Right Middle Lobe Bronchus (Dis Chest, 1966) [MEDLINE]
In 1992, the “Lady Windermere Syndrome” was Described in a Series of Female Patients (n = 29) with MAC Infection Initially in Middle Lobe or Lingular Distributions (in the Absence of Airway Obstruction or Predisposing Pulmonary Disease) (Chest, 1992) [MEDLINE]
Lady Windermere was a Fastidious Female Character in the Victorian-Era (1892) Oscar Wilde Play, “Lady Windermere’s Fan”
The Authors Hypothesized that Voluntary Suppression of Cough May Have Led to the Development of Nonspecific Inflammation in the Poorly-Draining Middle Lobe or Lingula, Upon Which MAC Infection then Occurred
Predominantly Seen in Pediatric Cases with History of Asthma or Atopy
In a Series of Asthmatic Children with Middle Lobe Syndrome, Haemophilus Influenzae and Streptococcus Pneumoniae were the Predominant Organisms Recovered (see Haemophilus Influenzae and Streptococcus Pneumoniae) (Arch Dis Child, 1992) [MEDLINE]
Non-Obstructive Middle Lobe Syndrome (Characterized by an Absence of Airway Obstruction by Chest CT and/or Bronchoscopy) Accounts for the Majority of Middle Lobe Syndrome Cases (Respiration, 2012) [MEDLINE]
Non-Obstructive Type May Also Occur in Other Lobes of the Lung, Most Commonly the Lingula
Right Middle Lobe Bronchus Has a Narrow Diameter, Long Length, and an Acute Takeoff Angle, Creating Poor Conditions for Drainage (and Poor Clearance of Mucous)
Right Middle Lobe Bronchus Typically Has a “Fish-Mouth” Configuration (as Does the Lingular Bronchus)
Embryologic Factors
Early in Embryologic Development, the Smaller Left Endodermal Bud is Directed More Laterally than the Caudally-Located Right Endodermal Bud, Resulting in Asymmetry of the Mainstem Bronchi
Later in Embryologic Development, the Right Main Lung Bud Forms Three Lung Buds and the Left Lung Bud Forms Only Two Buds (Corresponding to the Later Pulmonary Lobes)
Right Middle Has Relatively Poor Collateral Ventilation (as Compared to the Upper Lobes)
Right Middle Lobe is Anatomically Surrounded by Two Fissures (with Scant Parenchymal Bridges), Which Impedes Collateral Ventilation (Similar Anatomic Features Occur in the Lingula)
Poor Right Middle Lobe Collateral Ventilation (Especially in Patients with Complete Fissures) and Relative Anatomical Isolation Decrease the Probability of Reinflation Once Atelectasis Has Occurred (Radiology, 1983) [MEDLINE]
Right Middle Lobe Has a Greater Ratio of Pleural Surface to Nonpleural Surface, as Compared to the Upper Lobes
Collateral Ventilation in the Right Middle Lobe of Young Normal Subjects is Characterized by High Resistance and a Long-Time Constant, Relative to the Upper Lobes (Am Rev Respir Dis, 1978) [MEDLINE]
Infection in the Right Middle Lobe
Inflammation in the Right Middle Lobe
Therapy
Medical Management is the Typically the Preferred Therapy
Association of Middle Lobe Syndrome with the Development of Bronchiectasis (see Bronchiectasis)
Recurrent or Chronic Right Middle Lobe Syndrome May Result in Bronchiectasis
Due to Recurrent and/or Chronic Infection/Inflammation
Bronchiectasis Occurs in 50% of Cases (Respiration, 2012) [MEDLINE]
On the Posteroanterior Chest X-Ray, There is Obscuration of the Right Heart Border (Because the Medial Segment of the Right Middle Lobe is Adjacent to the Right Atrium)
On the Lateral Chest X-Ray, There is Triangle of Increased Density Between the Minor Fissure and the Lower Half of the Major Fissure
Chest CT Scan is Useful to Evaluate Bronchial Patency, Assess for Lymphadenopathy, Assess for Calcifications, and Detect Other Etiologies of Extrinsic Right Middle Lbe Airway Compression (Radiology, 1983) [MEDLINE]
In One Histopathologic Study of Right Middle Lobe Syndrome Cases Cured Surgically (n = 60), 60% Had Chronic Suppurative Infection, 33% Had Neoplasm, and 7% Had Tuberculosis (Med Interne, 1982) [MEDLINE]
May Be Recurrent (Requiring Multiple Courses of Antibiotics, Bronchodilators, etc)
Right Middle Lobectomy May Be Required in Some Cases
Cases with Obstructive Right Middle Lobe Syndrome are More Amenable to Surgical Intervention
Indications for Right Middle Lobectomy
Resistant/Complex Cases (Which are Unresponsive to Medical Therapy) and Who Have Proven Right Middle Lobe Bronchial Obstruction (Clin Respir J, 2009) [MEDLINE]
Resistant/Complex Cases with Chronic Atelectasis (>6 Months) Despite Medical Therapy: especially if patient has associated debilitating symptoms (such as persistent cough, fever, failure to thrive, etc)
Recurrent Hemoptysis, Not Amenable to Interventional Radiology Angioembolization (see Hemoptysis)
Presence of Malignancy (or Concern for Underlying Malignancy) in Right Middle Lobe
Surgical Approach
Video-Assisted Thoracoscopic Approach is Feasible for the Surgical Management of Middle Lobe Syndrome in Selected Patients with No Severe Calcified Lymph Nodes Surrounding the Hilus Pulmonis (World J Surg, 2017) [MEDLINE]
The middle lobe syndrome; a review of the anatomic and clinical features. Am Rev Tuberc 1955;71:775–784 [MEDLINE]
Middle-lobe syndrome. N Engl J Med. 253:489-495 1955 [MEDLINE]
The right middle lobe syndrome, a non-obstructive complex. Dis Chest 1966;50:57–66 [MEDLINE]
Chronic middle lobe infection. Factors responsible for its development. Ann Thorac Surg 1966;2:612–616 [MEDLINE]
Right middle lobe syndrome in children. JAMA 1966;197:8–14 [MEDLINE]
Middle lobe disease. South Med J 1967;60:1029–1032 [MEDLINE]
Middle lobe syndrome in asthmatic children. J Maine Med Assoc 1972;63:46–48 [MEDLINE]
Collateral ventilation and the middle lobe syndrome. Am Rev Respir Dis 1978;118: 305–310 [MEDLINE]
Isolated middle lobe atelectasis: aetiology, pathogenesis, and treatment of the so-called middle lobe syndrome. Thorax 1980;35:449–452 [MEDLINE]
Traction diverticula of the esophagus in the middle lobe syndrome. Can Med Assoc J 124:1320-1322, 1981 [MEDLINE]
Pathology of the middle lobe syndromes. A histopathological and pathogenetic analysis of sixty surgically-cured cases. Med Interne 1982;20: 73–8 [MEDLINE]
Middle lobe syndrome: diagnosis and management. Ann Thorac Surg 1982;33:28–31 [MEDLINE]
Middle lobe syndrome. Ann Thorac Surg 1983;35:679–686 [MEDLINE]
Right middle lobe syndrome in children. Int J Pediatr Otorhinolaryngol 1987;13:11–23 [MEDLINE]
Infection with Mycobacterium avium complex in patients without predisposing conditions. N Engl J Med. 1989 Sep 28;321(13):863-8 [MEDLINE]
Mycobacterium avium complex pulmonary disease presenting as an isolated lingular or middle lobe pattern. The Lady Windermere syndrome. Chest. 1992 Jun;101(6):1605-9 [MEDLINE]
Right middle lobe syndrome caused by Mycobacterium fortuitum in a patient with human immunodeficiency virus infection. South Med J 1992; 85:767–769 [MEDLINE]
Role of infection in the middle lobe syndrome in asthma. Arch Dis Child 1992;67:592–594 [MEDLINE]
Allergic bronchopulmonary aspergillosis with middle lobe syndrome and allergic Aspergillus sinusitis. Eur Respir J. 1993 Jun;6(6):917-8 [MEDLINE]
Middle lobe syndrome: a clinicopathological study of 21 patients. Hum Pathol 1995;26: 302–307 [MEDLINE]
Outcome after right middle lobe syndrome. Chest 1995;108:150–15 [MEDLINE]
Case report: Blastomyces dermatitidis as a cause of middle lobe syndrome. Am J Med Sci 1996; 312:191–193 [MEDLINE]
Middle lobe syndrome. Am Fam Physician 1996;53:2547– 2550 [MEDLINE]
The right middle-lobe syndrome–a case report and review of the literature. S Afr Med J. 1997 Feb;87(2):178-9 [MEDLINE]
Right middle lobe atelectasis associated with endobronchial silicotic lesions. Arch Pathol Lab Med 2000;124:1619–1622 [MEDLINE]
Improvement in right lung atelectasis (middle lobe syndrome) following administration of low-dose roxithromycin. Respiration 2001;68: 210–214 [MEDLINE]
Sarcoidosis with multiple organ involvement emerging as Lofgren’s syndrome. Intern Med 2003;42: 534–537 [MEDLINE]
Resection of the right middle lobe and lingula in children for middle lobe/lingula syndrome. Chest 2004;125:38–42 [MEDLINE]
Congenital anomalies of the tracheobronchial tree, lung, and mediastinum: embryology, radiology, and pathology. Radiographics 2004;24:e17 [MEDLINE]
Middle lobe syndrome in children with asthma: review of 56 cases. J Asthma 2004;41:411–417 [MEDLINE]
The role of timely intervention in middle lobe syndrome in children. Chest 2005;128: 2504–2510 [MEDLINE]
A case of Mycobacterium avium complex pulmonary disease in an immunocompetent host. South Med J. 2005;98(10):1036-1038 [MEDLINE]
Middle lobe syndrome as the pulmonary manifestation of primary Sjogren’s syndrome. Med J Aust 2006;184:294–295 [MEDLINE]
Bronchial hyperresponsiveness, atopy, and bronchoalveolar lavage eosinophils in persistent middle lobe syndrome. Pediatr Pulmonol 2006;41:805–811 [MEDLINE]
Bronchial anthracofibrosis and tuberculosis presenting as a middle lobe syndrome. Prim Care Respir J 2008;17:51–55 [MEDLINE]
Endobronchial tuberculosis presenting as right middle lobe syndrome: clinical characteristics and bronchoscopic findings in 22 cases. Yonsei Med J 2008;49:615–619 [MEDLINE]
Bronchiectasis. Radiol Clin North Am 2009;47:289–306 [MEDLINE]
Chyloptysis with right middle lobe syndrome complicated postoperatively by chylothorax: an unusual cause of right middle lobe syndrome. Can Respir J 2009;16:e1–e2 [MEDLINE]
Middle lobe syndrome: a nationwide study on clinicopathological features and surgical treatment. Clin Respir J 2009;3:77–81 [MEDLINE]
Thoracoscopic lobectomy as a treatment option for persistent middle lobe syndrome in children. J Pediatr Int 2010;52:79–81 [MEDLINE]
Middle lobe syndrome: a review of clinicopathological features, diagnosis and treatment. Respiration. 2012;84(1):80-6 [MEDLINE]
Middle lobe syndrome in children today. Pediatr Respir Rev 2014 Jun;15(2):188-93. doi: 10.1016/j.prrv.2014.01.002 [MEDLINE]
Ten years’ experience in surgical treatment of right middle lobe syndrome. Ann Thorac Cardiovasc Surg. 2015;21(4):354-8. doi: 10.5761/atcs.oa.14-00273 [MEDLINE]
Middle lobe syndrome: a singularly rare presentation of complicated pulmonary hydatid disease. BMJ Case Rep. 2016 Apr 4;2016. pii: bcr2016214670. doi: 10.1136/bcr-2016-214670 [MEDLINE]
Endobronchial Silicosis and Tuberculosis Presenting as the Right Middle Lobe Syndrome. J Bronchology Interv Pulmonol. 2016 Oct;23(4):e35-e37 [MEDLINE]
Middle lobe syndrome: An exceptional presentation of concomitant lepidic adenocarcinoma and bronchial anthracofibrosis. Monaldi Arch Chest Dis. 2017 Dec 19;87(3):864. doi: 10.4081/monaldi.2017.864 [MEDLINE]
Tracheobronchopathia osteochondroplastica – a 61-year-old female with middle lobe syndrome Adv Respir Med. 2017;85(3):158-160. doi: 10.5603/ARM.2017.0027 [MEDLINE]
Middle lobe syndrome: an intriguing presentation of tracheobronchial amyloidosis. BMJ Case Rep. 2017 May 22;2017. pii: bcr-2017-219480. doi: 10.1136/bcr-2017-219480 [MEDLINE]
A Comparative Study of Video-Assisted Thoracic Surgery with Thoracotomy for Middle Lobe Syndrome. World J Surg. 2017 Mar;41(3):780-784. doi: 10.1007/s00268-016-3777-6 [MEDLINE]
Infectious Causes of Right Middle Lobe Syndrome. Cancer Control. 2017 Jan;24(1):60-65 [MEDLINE]
Image Diagnosis: Endobronchial Tuberculosis Masquerading as an Endobronchial Tumor with Presentation as Middle Lobe Syndrome. Perm J. 2017;21. pii: 16-006. doi: 10.7812/TPP/16-006 [MEDLINE]
A Comparative Study of Video-Assisted Thoracic Surgery with Thoracotomy for Middle Lobe Syndrome. World J Surg. 2017 Mar;41(3):780-784. doi: 10.1007/s00268-016-3777-6 [MEDLINE]
Middle lobe syndrome: An exceptional presentation of concomitant lepidic adenocarcinoma and bronchial anthracofibrosis. Monaldi Arch Chest Dis. 2017 Dec 19;87(3):864. doi: 10.4081/monaldi.2017.864 [MEDLINE]
Non-Obstructive Middle Lobe Syndrome: An Unusual Cause of Recurrent Pneumonia in an Elderly Woman. Eur J Case Rep Intern Med. 2018 Jan 31;5(1):000737. doi: 10.12890/2017_000737. eCollection 2018 [MEDLINE]