Recommendations (American College of Chest Physicians Evidence-Based Lung Cancer Guidelines, 3rd Edition) (Chest, 2013) [MEDLINE]
For Patient with >20 Pack-Year Smoking History or History of Lung Cancer, β-Carotene Supplementation is Not Recommended for the Primary/Secondary/Tertiary Chemoprevention of Lung Cancer (Grade 1A Recommendation)
β-Carotene Dose Used in Studies: 20-30 mg/day or 50 mg qOD
For Patient at Risk for Lung Cancer or History of Lung Cancer, Vitamin E, Retinoids, N-Acetylcysteine, Isotretinoin are Not Recommended for the Primary/Secondary/Tertiary Chemoprevention of Lung Cancer (Grade 1A Recommendation)
For Patient at Risk for Lung Cancer or History of Lung Cancer, Aspirin is Not Recommended for the Primary/Secondary/Tertiary Chemoprevention of Lung Cancer Outside of a Clinical Trial (Grade 1B Recommendation)
For Patient with a History of Early-Stage Lung Non-Small Cell Lung Cancer, Selenium is Not Recommended for the Tertiary Chemoprevention of Lung Cancer (Grade 1B Recommendation)
For Patient at Risk for Lung Cancer or History of Lung Cancer, Prostacyclin Analogs (Iloprost), Cyclooxygenase-2 Inhibitors (Celecoxib), and Anethole Dithiolethione are Not Recommended for the Primary/Secondary/Tertiary Chemoprevention of Lung Cancer Outside of a Clinical Trial (Grade 1B Recommendation)
For Patient at Risk for Lung Cancer or History of Lung Cancer, Inhaled Corticosteroids are Not Recommended for the Primary/Secondary/Tertiary Chemoprevention of Lung Cancer (Grade 1B Recommendation)
For Patient at Risk for Lung Cancer or History of Lung Cancer, Pioglitazone and Myoinositol are Not Recommended for the Primary/Secondary/Tertiary Chemoprevention of Lung Cancer Outside of a Clinical Trial (Grade 1B Recommendation)
For Patient at Risk for Lung Cancer, Tea Extract and Metformin are Not Recommended for the Primary/Secondary/Tertiary Chemoprevention of Lung Cancer Outside of a Clinical Trial (Grade 2C Recommendation)
Patients Who Continue to Smoke After a Diagnosis of Lung Cancer Double Their Risk of Dying (Oncology, 2010) [MEDLINE]
Recommendations for Current Smokers (American College of Chest Physicians Lung Cancer Practice Guidelines; Chest, 2013) [MEDLINE]
Current Smokers Undergoing Low-Dose Chest CT Screening Should Be Provided with Smoking Cessation Interventions (Including Counseling and Pharmacotherapy) (Grade 1B Recommendation)
Current Smokers with Smoking-Related Pulmonary Disease Should Receive Intensive Smoking Cessation Interventions (Grade 1B Recommendation)
Recommendations for Patients with Lung Cancer (American College of Chest Physicians Lung Cancer Practice Guidelines; Chest, 2013) [MEDLINE]
In Lung Cancer Patients Undergoing Surgery, Perioperative Smoking Cessation Pharmacotherapy is Recommended to Improve the Abstinence Rate (Grade 1B Recommendation)
In Lung Cancer Patients Undergoing Surgery for Whom Smoking Cessation Pharmacotherapy is Contraindicated or Refused, Cessation Counseling Alone is Recommended During the Perioperative Period (Grade 2C Recommendation)
In Lung Cancer Patients Undergoing Surgery, the Timing of Cessation Does Not Appear to Increase the Risk of Postoperative Complications (Grade 2C Recommendation)
Cessation Interventions Should Begin in the Preoperative Period
In Lung Cancer Patients Attempting Cessation in Conjunction with Surgical Interventions Counseling and Pharmacotherapy are Recommended as the Outset of Surgical Intervention (Grade 1B Recommendation)
In Lung Cancer Patients Undergoing Chemotherapy, Smoking Cessation Interventions (Counseling and Pharmacotherapy) Improve Abstinence Rates (Grade 1B Recommendation)
In Lung Cancer Patients with Depressive Symptoms, Smoking Cessation with Bupropion is Recommended to Improve Abstinence Rate, Depressive Symptoms, and Quality of Life (Grade 2B Recommendation)
In Lung Cancer Patients for Whom Smoking Cessation Pharmacotherapy is Contraindicated or Refused, Cessation Counseling Alone is Recommended as a Method to Improve the Abstinence Rate (Grade 2B Recommendation)
In Lung Cancer Patients Undergoing Radiotherapy, Smoking Cessation Interventions (Counseling and Pharmacotherapy) are Recommended (Grade 1C Recommendation)
Treatment of Non-Small Cell Lung Cancer
General Considerations
Patient Expectations Regarding Chemotherapy
Cancer Care Outcomes Research and Surveillance (CanCORS) Study About Patient Expectations (NEJM, 2012) [MEDLINE]
Metastatic Lung Cancer: 69% of patients did not understand that chemotherapy was not at all likely to cure their cancer
Metastatic Colon Cancer: 81% of patients did not understand that chemotherapy was not at all likely to cure their cancer
Level of education, functional status, and the patient’s role in decision making were not associated with the inaccurate beliefs about chemotherapy
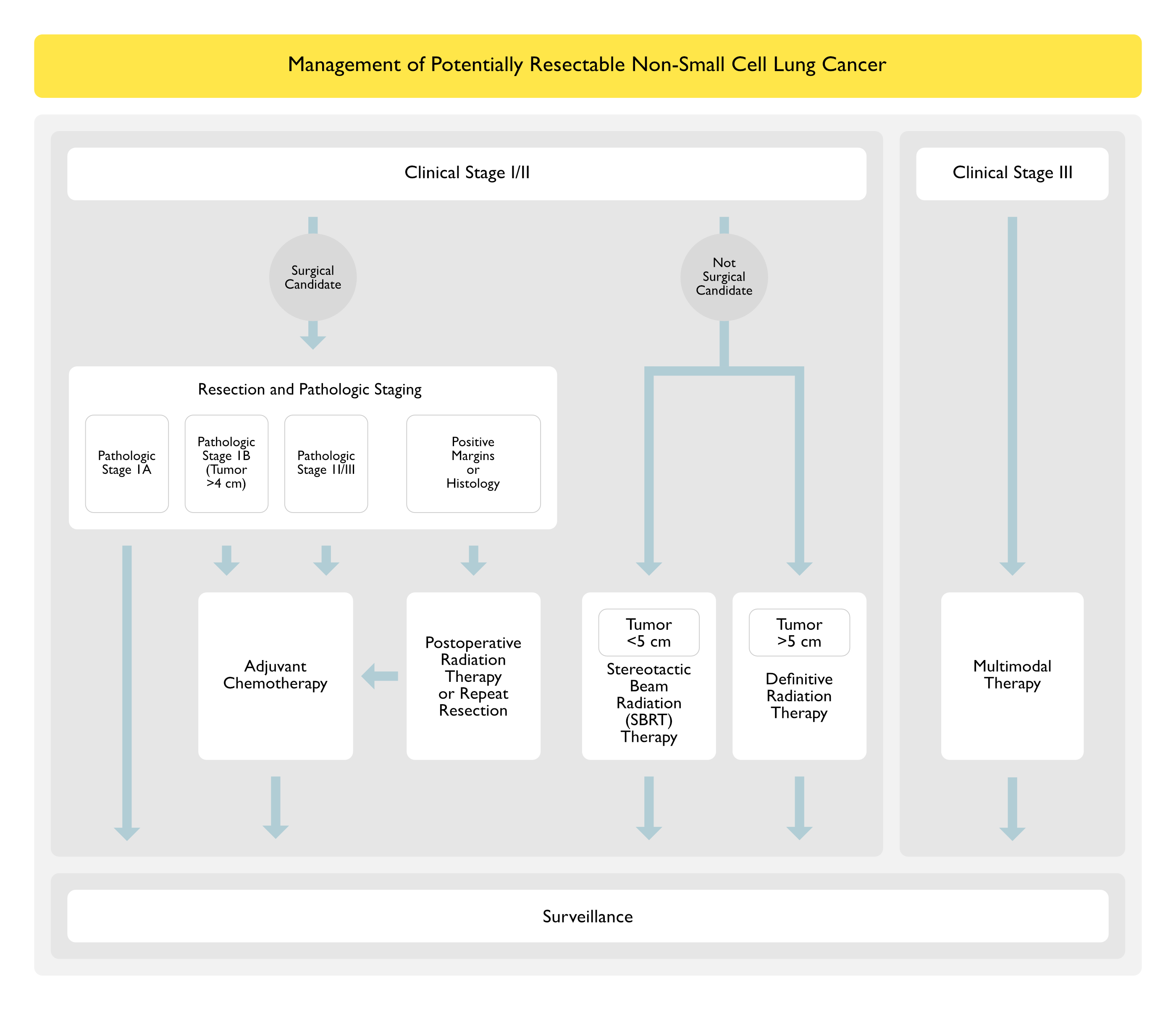
Stage I Non-Small Cell Lung Cancer
Surgical Resection
Surgical Resection is First-Line Therapy for Stage I Non-Small Cell Lung Cancer
Radiation Therapy
Radiation May Be Used For Patients Who are Not Surgical Candidates
Stereotactic Body Radiation Therapy (SBRT): single or very limited number of high-dose fractions to a radiographically discrete treatment volume by using multiple convergent beams -> preferred for tumors <5 cm
Preferred Radiotherapy Technique for the Definitive Management of Peripheral Stage I Lesions
Conventionally Fractionated Radiation Therapy: for patients who are not surgical candidates and whose tumor is too large for SBRT
Radiofrequency Ablation (RFA): unclear role at this time
Cryoablation: unclear role at this time
Post-Operative Adjuvant Chemotherapy
Stage IB: adjuvant chemotherapy may have a role
Clinical Stage I/II with Mediastinal Lymph Node Involvement in Surgical Specimen (Pathologic Stage IIIA): adjuvant chemotherapy improves survival
Stage II Non-Small Cell Lung Cancer
Surgical Resection
Surgical Resection is First-Line Therapy for Stage II Non-Small Cell Lung Cancer
Radiation Therapy: for patients who are not surgical candidates
Stereotactic Body Radiation Therapy (SBRT): single or very limited number of high-dose fractions to a radiographically discrete treatment volume by using multiple convergent beams
Preferred radiotherapy technique for the definitive management of peripheral stage I lesions
Conventionally Fractionated Radiation Therapy: for patients who are not surgical candidates and whose tumor is too large for SBRT (>5 cm)
Radiofrequency Ablation (RFA): unclear role at this time
Cryoablation: unclear role at this time
Photodynamic Therapy: may be used as primary treatment in selected patients with superficial airway lesions
Post-Operative Adjuvant Chemotherapy: improves survival in patients with pathologic stage II disease
Stage III Non-Small Cell Lung Cancer
Surgical Resection
Stage III (N0-1): surgical resection is generally indicated
Stage IIIA (T3 N1): surgical resection, followed by adjuvant chemotherapy (for those with completely resected disease)
Have better prognosis than stage IIIA disease associated with mediastinal (N2) nodal involvement
Adjuvant chemotherapy (platinum-based doublet regimens) prolongs overall survival in patients with completely resected stage III disease
Superior Sulcus (Pancoast) Tumor with Hilar Lymph Node Involvement (T3-4 N1 M0) or without Hilar Lymph Node Involvement (T3-4 N0 M0): usually treated with chemoradiotherapy, followed by surgery
Stage IIIA (T4 N0-1): since resectable T4 N0-1 lesions are uncommon, most T4 lesions are best treated with definitive chemoradiotherapy
Patients with involvement of the carina/superior vena cava/vertebral body may benefit from surgery with a multimodal treatment approach
Radiation Therapy: definitive radiation therapy is indicated for patients who are not surgical candidates
Stereotactic Body Radiation Therapy (SBRT): single or very limited number of high-dose fractions to a radiographically discrete treatment volume by using multiple convergent beams -> preferred for tumors <5 cm
Conventionally Fractionated Radiation Therapy: for patients who are not surgical candidates and whose tumor is too large for SBRT (>5 cm)
Radiofrequency Ablation (RFA): unclear role at this time
Post-Operative Radiation Therapy: role is uncertain
Indications
Patients with Inadequate Lymph Node Sampling in Whom Mediastinal Node Involvement was Suspected But Not Confirmed: the use of post-operative radiation therapy in this case should not be prioritized over adjuvant chemotherapy
Patients with Involvement of Multiple Stations of Involved N2 Lymph Nodes
Patients with Positive Resection Margins
Mediastinal (N2-3) Lymph Node Disease: concurrent chemoradiotherapy is recommended
For Patients with Potentially Resectable Disease: unclear if surgical resection offers a benefit over chemoradiotherapy alone
For Patients with Unresectable Disease: concurrent chemoradiotherapy alone
Prophylactic Cranial Irradiation: not indicated (although patients with stage III disease are at high risk for brain metastases)
Stage IV Non-Small Cell Lung Cancer
Squamous Cell Lung Cancer
Preferred Therapy
Platinum-Based (Usually Cisplatin) Combination Chemotherapy (see Cisplatin): 4-6 cycles
Progression During or After Initial Therapy with a Platinum-Based Regimen
Subsequent Maintenance Therapy: after initial 4-6 cycles (and in the absence of disease progression), maintenance therapy has been demonstrated to prolong progression-free survival and overall survival
KEYNOTE-024 Trial of Pembrolizumab in Previously-Untreated Advanced PD-L1-Positive Non-Small Cell Lung Cancer Patients without EGFR/ALK Mutations (NEJM, 2016) [MEDLINE]
Pembrolizumab in PD-L1-Positive Non-Small Cell Lung Cancer (with PD-L1 Expression on ≥50% Cells) Improved Progression-Free and Overall Survival, with Fewer Adverse Effects than Platinum-Based Chemotherapy
Non-Squamous Cell Lung Cancer
Preferred Therapy with Driver Mutations Absent
Platinum-Cased (Usually Cisplatin) Combination Chemotherapy: see Cisplatin): 4-6 cycles
May Supplement with Bevacizumab (Avastin) (see Bevacizumab)
Subsequent Maintenance Therapy: after initial 4-6 cycles (and in the absence of disease progression), maintenance therapy has been demonstrated to prolong progression-free survival and overall survival
KEYNOTE-024 Trial of Pembrolizumab in Previously-Untreated Advanced PD-L1-Positive Non-Small Cell Lung Cancer Patients without EGFR/ALK Mutations (NEJM, 2016) [MEDLINE]
Pembrolizumab in PD-L1-Positive Non-Small Cell Lung Cancer (with PD-L1 Expression on ≥50% Cells) Improved Progression-Free and Overall Survival, with Fewer Adverse Effects than Platinum-Based Chemotherapy
Other Special Clinical Circumstances in Stage IV Non-Small Cell Lung Cancer
Stage IV Disease with an Isolated Metastasis (Brain, Adrenal)
May Benefit from Resection of Metastasis and Aggressive Therapy of the Primary Tumor
Central Airway Involvement
May Benefit from Radiation Therapy, Rigid Bronchoscopy/Airway Stenting, or Brachytherapy
Zoledronate Significantly Decreases the Incidence of Skeletal Related Events in Patients with Bone Metastases from Non-Small Cell Lung Cancer and Other Solid Tumors
However, Zoledronate Does Not Improve Progression-Free Survival or Overall Survival in Stage III NSCLC
Specific Treatment of Lepidic Predominant Adenocarcinoma (Bronchioloalveolar Carcinoma)
General Approach
Due to Variability in Clinical Behavior (Which Can Range from Subcentimeter Ground-Glass Opacities Which are Growing at a Barely Perceptible Rate Over Years in Both Lungs to Extensive Confluent Lobar Infiltrates Which Cause a Debilitating Productive Cough with Bronchorrhea and Rapid Progression to Respiratory Failure), Assessment of the Pace of Disease is Critical Prior to Treatment (Clin Adv Hematol Oncol, 2014) [MEDLINE]
In Indolent Cases, Lepidic-Predominant-Adenocarcinoma Can Manifest Doubling Times Which are Measured in Years (Radiology, 2007) [MEDLINE] (Acad Radiol, 2011) [MEDLINE] (Am J Respir Crit Care Med, 2012) [MEDLINE]
Bronchioloalveolar Carcinoma May Have Epidermal Growth Factor Receptor (EGFR) or May Have a a Translocation in the Gene for Anaplastic Lymphoma Kinase (ALK) or May Have No Actionable Gene Target (Clin Adv Hematol Oncol, 2014) [MEDLINE]
Surgical Resection
In a Small Retrospective Series of Patients with Bronchioloalveolar Carcinoma, Early-Stage Non-Mucinous Bronchioloalveolar Carcinoma Had an Excellent Prognosis, While Mucinous Bronchioloalveolar Carcinoma Generally Had a Poor Prognosis (J Thorac Oncol, 2010) [MEDLINE]: n = 40
Early Stages (IA+IB) Non-Mucinous Bronchioloalveolar Carcinoma Had a 5-Year Overall Survival Rate of 91% (5-Year Overall Survival Rate was 100% for Stage IA Cases)
However, in Cases with Pneumonic-Like Bronchioloalveolar Carcinoma (All Mucinous), 71% of Cases Died of Recurrent/Progressive Disease
Clinical Stage 1A Ground Glass Opacity-Predominant Adenocarcinomas Exhibited Low-Grade Malignancy and Had an Extremely Favorable Prognosis with Wedge Resection (for T1a Tumors) or Segmentectomy (for T1b Tumors) (Chest, 2014) [MEDLINE]
Lepidic Adenocarcinoma Had a Good Prognosis and Could Be Amenable to Sublobar Resection Instead of Standard Lobectomy (J Thorac Dis, 2016) [MEDLINE]
Palliative Surgical Resection
Some Patients with Pneumonic Bronchioloalveolar Carcinoma (Clinically Appearing Similar to Lobar Pneumonia) May Benefit from Palliative Surgical Resection to Relieve Symptoms of Dyspnea (Due to Bronchorrhea and/or Shunt) (Br J Radiol. 2001) [MEDLINE]
Lung Transplant Has Been Used in Patients with Small Case Series of Patients with Multifocal Bronchioloalveolar Carcinoma or a Pneumonic Pattern of Diffuse Disease (Clin Adv Hematol Oncol, 2014) [MEDLINE]
Chemotherapy
xxxxxx
Management of Bronchorrhea in Adenocarcinoma-Lepidic Type Lung Cancer (Bronchioloalveolar Carcinoma) (see Bronchorrhea)
Nebulized Indomethacin (see Indomethacin): 25 mg in 2 ml NS (pH adjusted to 7.4 qith Na2CO3)
Corticosteroids (see Corticosteroids): decrease mucous hypersecretion
Nebulized Furosemide (Lasix) (see Furosemide): 20 mg in 2 ml NS TID
Macrolides (see Macrolides): decrease bacteria (LPS is known to stimulate goblet cell secretion)
Special Clinical Treatment Issues and Recommendations (American College of Chest Physicians Evidence-Based Clinical Practice Guidelines, 3rd Edition) (Chest, 2013) [MEDLINE]
Pancoast Tumor
Tissue Diagnosis Should Be Obtained Prior to Treatment of Pancoast Tumor (Grade 1C Recommendation)
In Pancoast Tumor Being Considered for Curative-Intent Surgical Resection, MRI of the Thoracic Inlet and Brachial Plexus is Recommended to Characterize Possible Tumor Invasion of Vascular Structures or the Extradural Space (Grade 1C Recommendation)
In Pancoast Tumor Being Considered for Curative-Intent Surgical Resection, Invasive Mediastinal Staging and Extrathoracic Imaging (Head CT/Brain MRI and Either Whole-Body PET or Abdominal CT with Bone Scan) are Recommended (Grade 1C Recommendation)
Involvement of Mediastinal Nodes and/or Metastatic Disease is a Contraindication to Resection
In Potentially-Resectable Pancoast Tumor and Good Performance Status, Preoperative Concurrent Chemoradiotherapy is Recommended (Grade 2B Recommendation)
In Patient Undergoing Resection of a Pancoast Tumor, Every Effort Be Made to Achieve a Complete Resection (Grade 1B Recommendation)
In Patient Undergoing Resection of a Pancoast Tumor, Resection Consisting of a Lobectomy (Instead of a Non-Anatomic Wedge Resection), as Well as the Involved Chest Wall Structures is Suggested (Grade 2C Recommendation)
In Patient with an Unresectable, Non-Metastatic Pancoast Tumor Who Has Good Performance Status, Definitive Concurrent Chemotherapy and Radiotherapy are Suggested (Grade 2C Recommendation)
In Patient with Pancoast Tumor Who is Not a Candidate for Curative-Intent Treatment, Palliative Radiotherapy is Suggested (Grade 2B Recommendation)
Tumor Invading the Chest Wall
With NSC Lung Cancer Invading the Chest Wall Being Considered for Curative-Intent Surgical Resection, Invasive Mediastinal Staging and Extrathoracic Imaging (Head CT/Brain MRI and Either Whole-Body PET or Abdominal CT with Bone Scan) are Suggested (Grade 2C Recommendation)
With NSC Lung Cancer Invading the Chest Wall, Involvement of Mediastinal Nodes and/or Metastatic Disease Represent a Contraindication to Resection, and Definitive Chemoradiotherapy is Suggested (Grade 2C Recommendation)
At the Time of Resection of a Tumor Invading the Chest Wall, Every Effort Should Be Made to Achieve a Complete Resection (Grade 1B Recommendation)
Central T4 N0-1 M0 Tumor
With Clinical T4 N0-1 M0 NSC Lung Cancer Being Considered for Curative Resection, Extrathoracic Imaging (Head CT/Brain MRI and Either Whole-Body PET or Abdominal CT with Bone Scan) is Recommended (Grade 1C Recommendation)
Metastatic Disease Represents a Contraindication to Resection
With Clinical T4 N0-1 M0 NSC Lung Cancer without Distant Metastases Being Considered for Curative Resection, Invasive Mediastinal Staging Should Be Performed (Grade 2C Recommendation)
Mediastinal Nodal Involvement Represents a Contraindication to Primary Resection
Preoperative Chemotherapy and Resection has Resulted in Long-Term Survival in Experienced Centers in Patients with Mediastinal Nodal Involvement
With Clinical T4 N0-1 M0 NSC Lung Cancer Being Considered for Curative Resection, Resection Should Only Be Performed at a Specialized Center (Grade 2C Recommendation)
Second Primary Lung Cancer
With Two Foci Typical of a Primary Lung Cancer (Solid Spiculated Masses that are Either Proven or Suspected Lung Cancer), Identification of These as Second Primary Lung Cancers (Either Synchronous or Metachronous) Should be Based on the Judgment of a Multidisciplinary Team, Taking into Account Clinical, Radiologic, and Tumor Cytologic/Histologic Features (Grade 2C Recommendation)
With Two Primary NSC Lung Cancers (Synchronous or Metachronous) Being Considered for Curative Surgical Resection, Invasive Mediastinal Staging and Extrathoracic Imaging (Head CT/Brain MRI and Either Whole-Body PET or Abdominal CT with Bone Scan) are Recommended (Grade 1B Recommendation)
Mediastinal Nodal Involvement is a Contraindication and/or Metastatic Disease is a Contraindication to Resection
In Patients Not Initially Suspected of Having a Second Focus of Lung Cancer Who is Found Intraoperatively to Have a Second Lung Cancer in a Different Lobe, Resection of Each Lesion is Suggested, Provided the Patient has Adequate Pulmonary Reserve and there is No N2 Nodal Involvement (Grade 2C Recommendation)
Additional Tumor Nodules in the Same Lobe (T3Satell)
With Suspected or Proven Lung Cancer and an Additional (Suspected) Tumor Nodule within the Same Lobe, No Further Diagnostic Work-Up of the Additional Nodule is Recommended (Grade 1B)
With an Additional (Suspected) Tumor Nodule within the Same Lobe as a Suspected or Proven Primary Lung Cancer, Mediastinal Staging and Extrathoracic Imaging (Head CT/Brain MRI and Either Whole-Body PET or Abdominal CT with Bone Scan) Should Be Dictated by the Primary Lung Cancer Alone and Not Modified by the Presence of the Additional Lesion (Grade 1C)
With NSC Lung Cancer and an Additional Focus of Lung Cancer within the Same Lobe (and No Mediastinal or Distant Metastases), Resection Via a Lobectomy is Recommended (Grade 1B)
Ipsilateral Different Lobe Tumor Nodules (T4Ipsi Nod)
In Suspected or Proven NSC Lung Cancer with Ipsilateral Different Lobe Tumor Nodule(s), Multidisciplinary Team Should Reasonably Exclude the Possibility that this Represents a Benign Lesion or a Synchronous Primary Lung Cancer (Taking into Account Clinical, Radiologic, and Tumor Cytologic/Histologic Features) (Grade 1C Recommendation)
With Ipsilateral Different Lobe Tumor Nodule(s), Extrathoracic Imaging (Head CT/Brain MRI and Either Whole-Body PET or Abdominal CT with Bone Scan) is Recommended (Grade 2C Recommendation)
Presence of Distant Metastases Indicates that the Pulmonary Nodule Most Likely Represents Metastatic (M1b) Disease
With Ipsilateral Different Lobe Tumor Nodule(s), Invasive Mediastinal Staging Should Be Performed (Grade 2C Recommendation)
Mediastinal Nodal Involvement is a Contraindication to Curative-Intent Treatment
With Ipsilateral Different Lobe Tumor Nodule(s) (and No Mediastinal or Distant Metastases), Resection of Each Lesion is Suggested, Provided the Patient Has Adequate Pulmonary Reserve (Grade 1B Recommendation)
Contralateral Lobe Tumor Nodules (M1aContr Nod)
With Contralateral Lobe Tumor Nodule(s), Invasive Mediastinal Staging and Extrathoracic Imaging (Head CT/Brain MRI and Either Whole-Body PET or Abdominal CT with Bone Scan) are Recommended (Grade 2C Recommendation)
Involvement of Mediastinal Nodes and/or Metastatic Disease is a Contraindication to Curative-Intent Treatment
With Contralateral Lobe Tumor Nodule(s) and No Mediastinal or Distant Mets, Resection of Each Lesion is Suggested, Provided the Patient Has Adequate Pulmonary Reserve (Grade 2C Recommendation)
Multifocal Lung Cancer
With Multiple Lesions Which are at Least Partially Ground Glass and are Suspected to Be Malignant, These Should Be Classified as Multifocal Lung Cancer (MFLC) (Grade 2C Recommendation)
In Suspected/Proven Multifocal Lung Cancer with a Negative Clinical Evaluation and Normal Mediastinum by CT, Distant and Mediastinal Staging are Not Considered Routinely Necessary (Grade 2C Recommendation)
In Suspected/Proven Multifocal Lung Cancer, Curative-Intent Treatment Should Be Pursued (Grade 2C Recommendation)
In Suspected/Proven Multifocal Lung Cancer, Sublobar Resection of All Lesions Suspected of Being Malignant Should Be Performed, if Feasible (Grade 2C Recommendation)
Isolated Brain Metastasis
In Isolated Brain Metastasis from NSC Lung Cancer Being Considered for Curative-Intent Surgical Resection, Invasive Mediastinal Staging and Extrathoracic Imaging (Head CT/Brain MRI and Either Whole-Body PET or Abdominal CT with Bone Scan) are Suggested (Grade 2C Recommendation)
Involvement of Mediastinal Nodes and/or Metastatic Disease is a Contraindication to Resection
With No Other Sites of Metastases and a Synchronous Resectable N0-1 Primary NSC Lung Cancer, Resection or Radiosurgical Ablation of an Isolated Brain Metastasis is Recommended (as Well as Resection of the Primary Tumor) (Grade 1C Recommendation)
With No Other Sites of Metastases and a Previously Completely Resected Primary NSC Lung Cancer (Metachronous Presentation), Resection or Radiosurgical Ablation of an Isolated Brain Metastasis is Recommended (Grade 1C Recommendation)
Following Curative Resection of an Isolated Brain Metastasis, Adjuvant Whole-Brain Radiotherapy is Suggested (Grade 2B Recommendation)
Adjuvant Chemotherapy is Reasonable with a Good Performance Status with the Goal of Decreasing the Incidence of Brain Recurrences, Although No Studies Have Specifically Addressed This
Following Curative Resection of an Isolated Brain Metastasis, Adjuvant Chemotherapy is Suggested (Grade 2B Recommendation)
Adjuvant Chemotherapy is Reasonable with a Good Performance Status, Although No Studies Have Specifically Addressed This
Isolated Adrenal Metastasis
In Isolated Adrenal Metastasis from NSC Lung Cancer Being Considered for Curative-Intent Surgical Resection, Invasive Mediastinal Staging and Extrathoracic Imaging (Head CT/Brain MRI and Either Whole-Body PET or Abdominal CT with Bone Scan) are Suggested (Grade 2C Recommendation)
Involvement of Mediastinal Nodes and/or Distant Metastatic Disease is a Contraindication to Resection
With a Synchronous Resectable N0-1 Primary NSC Lung Cancer and an Isolated Adrenal Metastasis with No Other Sites of Metastases, Resection of the Primary Tumor and the Adrenal Metastasis is Recommended (Grade 1C Recommendation)
With No Other Sites of Metastases and a Previously Completely Resected Primary NSC Lung Cancer (Metachronous Presentation), Resection of an Isolated Adrenal Metastasis is Recommended (Grade 1C Recommendation)
Following Curative Resection of an Isolated Adrenal Metastasis, Adjuvant Chemotherapy is Suggested (Grade 2B Recommendation)
Adjuvant Chemotherapy is Reasonable with a Good Performance Status, Although No Studies Have Specifically Addressed This
Surgical Considerations
Clinical Efficacy
Systematic Review of Randomized and Non-Randomized Trials of Video-Assisted Thoracoscopic Surgery (VATS) Lobectomy for Early-Stage Non-Small-Cell Lung Cancer (J Clin Oncol, 2009) [MEDLINE]
No Differences in Post-Op Air Leak, Arrhythmias, Pneumonia, Mortality, or Local Recurrence as Compared to Open Lobectomy
VATS Had a Lower 5-Year Mortality Rate than Open Lobectomy
Comparison of VATS and Open Thoracotomy (Ann Thorac Surg, 2010) [MEDLINE]
VATS Had Higher Rate of Intraoperative Complications than Open Lobectomy
No Difference in Short-Term Mortality Rate, Length of Stay, and Hospitalization Cost
There was a Socioeconomic Disparity (in Terms of Annual Income) Between VATS and Open Thoracotomy Patients
Treatment of Small Cell Lung Cancer
General Considerations
General Comments
Small Cell Lung Cancer is Usually Very Responsive to Chemotherapy
Patient Expectations Regarding Chemotherapy
Cancer Care Outcomes Research and Surveillance (CanCORS) Study About Patient Expectations (NEJM, 2012) [MEDLINE]
Metastatic Lung Cancer: 69% of patients did not understand that chemotherapy was not at all likely to cure their cancer
Metastatic Colon Cancer: 81% of patients did not understand that chemotherapy was not at all likely to cure their cancer
Level of Education, Functional Status, and the Patient’s Role in Decision-Making were not Associated with the Inaccurate Beliefs About Chemotherapy
General Treatment Recommendations
Recommendations-Stage I Disease (Which is Amenable to Surgical Resection) (Chest, 2013) [MEDLINE]
In Patient with Clinical Stage I Small Cell Lung Cancer, Surgical Resection is Recommended Over Non-Surgical Treatment (Grade 2C Recommendation)
In Patient with Stage I Small Cell Lung Cancer Who Has Undergone Curative-Intent Surgical Resection, Platinum-Based Adjuvant Chemotherapy is Recommended (Grade 1C Recommendation)
Recommendations-Role of Radiotherapy (Chest, 2013) [MEDLINE]
In Patient with Limited-Stage Small Cell Lung Cancer, Early Chemoradiotherapy with Accelerated Hyper-Fractionated Radiotherapy (Twice Daily) Concurrent with Platinum-Based Chemotherapy is Recommended (Grade 1B Recommendation)
In Patient with Either Limited or Extensive-Stage Small Cell Lung Cancer Who Achieve as Partial/Complete Response to Initial Therapy, Prophylactic Cranial Irradiation is Recommended (Grade 1B Recommendation): regimen of 25 Gy in 10 daily fractions has the largest amount of supporting safety and efficacy data
In Patient with Extensive-Stage Small Cell Lung Cancer Who Has Completed Chemotherapy and Achieved a Complete Response Outside the Chest and Partial/Complete Response in the Chest, Course of Consolidation Thoracic Radiotherapy is Suggested (Grade 2C Recommendation)
Recommendations-Role of Chemotherapy (Chest, 2013) [MEDLINE]
In Patient with Either Limited or Extensive-Stage Small Cell Lung Cancer, 4-6 Cycles of Platinum-Based Chemotherapy (Cisplatin, Carboplatin) + Either Etoposide or Irinotecan is Recommended Over Other Regimens (Grade 1A Recommendation)
In Patient with Relapsed or Refractory Small Cell Lung Cancer, Administration of a Second-Line, Single Agent Chemotherapy is Recommended (Grade 1B Recommendation)
Reinitiation of the Previous First-Line Chemotherapy Regimen is Recommended in Patient Who Relapse >6 mo After Completion of Initial Chemotherapy
In Elderly Patient with Limited-Stage Small Cell Lung Cancer and Good Performance Status (ECOG 0-2), Combined Platinum-Based Chemotherapy and Thoracic Radiotherapy is Recommended (Grade 2B Recommendation): patient should be followed closely for toxicity
In Elderly Patient with Extensive-Stage Small Cell Lung Cancer and Good Performance Status (ECOG 0-2), Carboplatin-Based Chemotherapy is Recommended (Grade 2A Recommendation)
In Elderly Patient with Small Cell Lung Cancer and Poor Performance Status, Treatment with Chemotherapy is Suggested if the Poor Performance Status is Due to the Small Cell Lung Cancer (Grade 2C Recommendation)
Approved as Single-Agent for Recurrent Small Cell Lung Cancer: 20% response rate
Usually Used with Palliative Intent
Adverse Effects: myelosuppression
Prognosis
Overall Survival Rates (American College of Chest Physicians Lung Cancer Guidelines; Chest, 2013) [MEDLINE]
Overall 5-Year Survival Rate for Lung Cancer (2001-2007): 16.3%
Historically, 5-Year Survival Rate from Lung Cancer (1975-1977) was 12.3%
Survival Rate Varies by Stage at the Time of Diagnosis
Local Disease: 52% survival
Regional Disease: 24% survival
Distant Disease: 4% survival
Stage at Diagnosis Accounts for the Most Significant Variation in Prognosis
Factors Associated with Poorer Survival in Lung Cancer
African-American Race
Male Sex
Older Age
Non-Small Cell Lung Cancer
Prognostic Factors in Non-Small Cell Lung Cancer
TNM Stage at Time of Diagnosis: best predictor of prognosis
Performance Status
Factors Associated with Worse Survival
Anorexia
Poor Performance Status
Weight Loss
Ethnicity
African-American Ethnicity: African-American race is not believed to be an independent predictor of poorer survival (when multivariate analysis accounted for performance status and weight loss)
Asian Ethnicity: Asians with lung cancer have better survival than caucasians (probably due to significantly higher prevalence of EGFR mutations, which is amenable to therapy)
Histologic Subtype: there are conflicting results as to whether the distinction between adenocarcinoma and squamous cell carcinoma affects prognosis
Degree of Differentiation: although some studies indicate that poorly differentiated tumors have a worse prognosis, studies regarding the impact of degree of differentiation are conflicting
Degree of Lymphatic Vessel Invasion: associated with worse survival
Degree of Microscopic Vascular Invasion: associated with worse survival
Occult Lymph Node Metastases (Detected by Immunohistochemistry): negative impact on outcome in stage I disease
Intense Lymphocytic Infiltration: associated with improved survival
High PET Standardized Uptake Value: associated with worse survival (and possibly predict response to chemotherapy)
EGFR Receptor Mutations: these patients are usually highly responsive to EGFR tyrosine kinase inhibitors (erlotinib, gefitinib, afatinib) and have a far better prognosis than those without EGFR mutations
EGFR Receptor Mutations are Associated with Lung Adenocarcinoma (Which More Frequently Affects Never Smokers, Women, and/or of Patients of Asian Ethnicity)
ROS1/ALK Mutations: these patients are highly responsive to crizotinib
ROS1/ALK Mutations are More Frequent in Non-Smokers or Former Smokers and Occur at a Younger Age
Co-Morbidity: 3-year survival rates in stage I disease are worse with increasing co-morbidity
Socioeconomic Status: lower socioeconomic status is associated with worse prognosis in lung cancer
Race-Related Differences in Lung Cancer Prognosis Tend to Diminish When Adjusted for Socioeconomic Status
Hospital Case Volume: patients operated on for non-small cell lung cancer at hospitals which perform large numbers of procedures have lower peri-operative mortality rates than those operated on at lower volume institutions
Hospital Volume Also Affects 5-Year Survival
Survival Rate in Non-Small Cell Lung Cancer
Survival with Adenocarcinoma In Situ (AIS) or Minimally Invasive Adenocarcinoma (MIA)
5-Year Survival with Complete Resection: near 100% (J Thorac Oncol, 2011) [MEDLINE]
5-Year Survival Based on Clinical Stage (IASLC Lung Cancer Staging Project: Proposals for Revision of the TNM Stage Groupings in the Forthcoming (Eighth) Edition of the TNM Classification for Lung Cancer) (J Thorac Oncol, 2016) [MEDLINE]
Clinical Stage IA1 5-Year Survival: 92%
Clinical Stage IA2 5-Year Survival: 83%
Clinical Stage IA1 5-Year Survival: 77%
Clinical Stage IB 5-Year Survival: 68%
Clinical Stage IIA 5-Year Survival: 60%
Clinical Stage IIB 5-Year Survival: 53%
Clinical Stage IIIA 5-Year Survival: 36%
Clinical Stage IIIB 5-Year Survival: 26%
Clinical Stage IIIC 5-Year Survival: 13%
Clinical Stage IVA 5-Year Survival: 10%
Clinical Stage IVB 5-Year Survival: 0%
5-Year Survival Based on Pathologic Stage (Note that the Survival Based on Pathologic Stage is Higher Than That Based on the Clinical Stage) (IASLC Lung Cancer Staging Project: Proposals for Revision of the TNM Stage Groupings in the Forthcoming (Eighth) Edition of the TNM Classification for Lung Cancer) (J Thorac Oncol, 2016) [MEDLINE]
Pathologic Stage IA1 5-Year Survival: 90%
Pathologic Stage IA2 5-Year Survival: 85%
Pathologic Stage IA1 5-Year Survival: 80%
Pathologic Stage IB 5-Year Survival: 73%
Pathologic Stage IIA 5-Year Survival: 65%
Pathologic Stage IIB 5-Year Survival: 56%
Pathologic Stage IIIA 5-Year Survival: 41%
Pathologic Stage IIIB 5-Year Survival: 24%
Pathologic Stage IIIC 5-Year Survival: 12%
Small Cell Lung Cancer
Prognostic Factors in Small Cell Lung Cancer
Extent of Disease at Presentation: most important prognostic factor
Survival Rate in Small Cell Lung Cancer
Limited Stage Disease: median survival is 15-20 mo
5-Year Survival: 10-13%
Extensive Stage Disease: median survival is 8-13 mo
5-Year Survival: 1-2%
Social Determinants of Health
xxx
The Impact of Social Determinants of Health on Textbook Oncological Outcomes and Overall Survival in Locally Advanced Non-Small Cell Lung Cancer. Published:September 19, 2023; DOI:https://doi.org/10.1016/j.xjon.2023.09.013
Objectives
Textbook oncological outcome (TOO) is a composite metric for surgical outcomes, including non-small cell lung cancer (NSCLC). We hypothesized that social determinants of health (SDH) can affect both TOO achievement and the overall survival (OS) of surgically resected NSCLC with pathological nodal disease.
Methods
We queried the NCDB (2010-2017) for pre-operative-therapy-naïve lobectomies for NSCLC with tumor size<7 cm and pathological N1/N2. Socio-economic factors comprised SDH scores, where SDH-negative (-) was considered if SDH ≥2(disadvantage), otherwise SDH was positive(+). TOO+ was defined as R0 resection, ≥5 lymph nodes resected, hospital stay<75th percentile, no 30-day mortality, adjuvant chemotherapy initiation ≤3 months, and no unplanned readmission. If one of these parameters was not achieved, the case was considered TOO-.
Results
Of 11,274 patients, 48% of cases were TOO+ and 38% were SDH+. 15% of patients were SDH- and were (aOR: 0.85, CI:0.78-0.92) less likely to achieve TOO+ than SDH+ patients. After accounting for confounders, TOO+ patients had 22% lower overall mortality than TOO- patients (aHR:0.78, CI:0.73-0.82). On the other hand, SDH- remained an independently significant risk factor, reducing survival by 24% compared to SDH+ (aHR:1.24, CI:1.17-1.32). The impact of SDH on OS was significant for both TOO+ and TOO- patients: SDH+/TOO+ had the best OS and SDH-/TOO- patients had the worst OS.
Conclusions
SDH score has a significant association with TOO achievement and TOO-driven overall post-treatment survival in lobectomy-resected NSCLC patients with postoperative pathologic N1/N2 nodal metastasis. Addressing SDH is important to optimize care and long-term survival of this patient population.
References
Chemoprevention
Chemoprevention of lung cancer: Diagnosis and management of lung cancer, 3rd ed: American College of Chest Physicians evidence-based clinical practice guidelines. Chest. 2013 May;143(5 Suppl):e40S-60S. doi: 10.1378/chest.12-2348 [MEDLINE]
Treatment
General
Cytoreductive antitumor activity of PF-2341066, a novel inhibitor of anaplastic lymphoma kinase and c-Met, in experimental models of anaplastic large-cell lymphoma. Mol Cancer Ther 2007;6:3314-3322 [MEDLINE]
Treatment of non-small cell lung cancer, stage IIIB: ACCP evidence-based clinical practice guidelines (2nd edition). Chest. 2007 Sep;132(3 Suppl):266S-276S [MEDLINE]
Clinical features and outcome of patients with non-small-cell lung cancer who harbor EML4-ALK. J Clin Oncol 2009;27:42-47 [MEDLINE]
Systematic review and meta-analysis of randomized and nonrandomized trials on safety and efficacy of video-assisted thoracic surgery lobectomy for early-stage non-small-cell lung cancer. J Clin Oncol 2009; 27: 2553–62 [MEDLINE]
Video-assisted thoracoscopic versus open thoracotomy lobectomy in a cohort of 13,619 patients. Ann Thorac Surg 2010; 89: 1563–70 [MEDLINE]
A single institution-based retrospective study of surgically treated bronchioloalveolar adenocarcinoma of the lung: clinicopathologic analysis, molecular features, and possible pitfalls in routine practice. J Thorac Oncol. 2010;5(6):830-836 [MEDLINE]
Non-small-cell lung cancer. Lancet. 2011 Nov 12;378(9804):1727-40. doi: 10.1016/S0140-6736(10)62101-0. Epub 2011 May 10 [MEDLINE]
The impact of genomic changes on treatment of lung cancer. Am J Respir Crit Care Med. 2013 Oct 1;188(7):770-5. doi: 10.1164/rccm.201305-0843PP [MEDLINE]
Executive Summary: Diagnosis and management of lung cancer, 3rd ed: American College of Chest Physicians evidence-based clinical practice guidelines. Chest. 2013 May;143(5 Suppl):7S-37S. doi: 10.1378/chest.12-2377 [MEDLINE]
Special treatment issues in non-small cell lung cancer: Diagnosis and management of lung cancer, 3rd ed: American College of Chest Physicians evidence-based clinical practice guidelines. Chest. 2013 May;143(5 Suppl):e369S-99S. doi: 10.1378/chest.12-2362 [MEDLINE]
The utility of the proposed IASLC/ATS/ERS lung adenocarcinoma subtypes for disease prognosis and correlation of driver gene alterations. Lung Cancer, 2013. 81(3):371–376 [MEDLINE]
Update on immune checkpoint inhibitors in lung cancer. Cancer Control 2014;21:80-89 [MEDLINE]
Crizotinib in ROS1-rearranged non-small-cell lung cancer. N Engl J Med. 2014 Nov 20;371(21):1963-71. doi: 10.1056/NEJMoa1406766. Epub 2014 Sep 27 [MEDLINE]
Appropriate sublobar resection choice for ground glass opacity- dominant clinical stage IA lung adenocarcinoma: wedge resection or segmentectomy. Chest 2014;145:66-71 [MEDLINE]
Feasibility of segmental resection in non-small-cell lung cancer with ground-glass opacity. Eur J Cardiothorac Surg 2014;46:375-9; discussion 379 [MEDLINE]
Anatomical thoracoscopic segmentectomy for lung cancer. en Thorac Cardiovasc Surg. 2014 Oct;62(10):586-93 [MEDLINE]
Managing multifocal bronchioloalveolar carcinoma/lepidic predominant adenocarcinoma: changing rules for an evolving clinical entity. Clin Adv Hematol Oncol. 2014 Sep;12(9):593-600 [MEDLINE]
Using multiplexed assays of oncogenic drivers in lung cancers to select targeted drugs. JAMA. 2014 May 21;311(19):1998-2006. doi: 10.1001/jama.2014.3741 [MEDLINE]
PDQ Adult Treatment Editorial Board. Non-Small Cell Lung Cancer Treatment (PDQ®): Health Professional Version. 2016 Jul 7. In: PDQ Cancer Information Summaries [Internet]. Bethesda (MD): National Cancer Institute (US); 2002-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK65865/
KEYNOTE-024 Trial. Pembrolizumab versus Chemotherapy for PD-L1-Positive Non-Small-Cell Lung Cancer. N Engl J Med. 2016, Oct 8 [MEDLINE]
Selumetinib for the treatment of non-small cell lung cancer. Expert Opin Investig Drugs. 2017 Aug;26(8):973-984 [MEDLINE]
Prognosis
Lung Cancer Incidence and Mortality with Extended Follow-up in the National Lung Screening Trial. J Thorac Oncol. 2019 Oct;14(10):1732-1742. doi: 10.1016/j.jtho.2019.05.044 [MEDLINE]
Psychosocial
Talking with patients about dying. N Engl J Med 2012;367:1651-1652 [MEDLINE]
Patients’ expectations about effects of chemotherapy for advanced cancer. N Engl J Med 2012;367:1616-1625.2 [MEDLINE]
Smoking Cessation
Smoking cessation: an integral part of lung cancer treatment. Oncology. 2010;78(5-6): 289-301 [MEDLINE]
Treatment of tobacco use in lung cancer: Diagnosis and management of lung cancer, 3rd ed: American College of Chest Physicians evidence-based clinical practice guidelines. Chest. 2013 May;143(5 Suppl):e61S-77S. doi: 10.1378/chest.12-2349 [MEDLINE]
Small Cell Lung Cancer
Small cell lung cancer: past, present, and future. Curr Oncol Rep. 2010 Sep;12(5):327-34. doi: 10.1007/s11912-010-0120-5 [MEDLINE]
Advances in the treatment of small-cell lung cancer. Semin Respir Crit Care Med. 2011 Feb;32(1):94-101. doi: 10.1055/s-0031-1272873. Epub 2011 Apr 15 [MEDLINE]
Systemic therapy for small cell lung cancer. J Natl Compr Canc Netw 2013;11(7):780-787 [MEDLINE]
Treatment of small cell lung cancer: Diagnosis and management of lung cancer, 3rd ed: American College of Chest Physicians evidence-based clinical practice guidelines. Chest. 2013 May;143(5 Suppl):e400S-19S. doi: 10.1378/chest.12-2363 [MEDLINE]
Advances in pharmacotherapy of small cell lung cancer. Expert Opin Pharmacother. 2014 Nov;15(16):2385-96. doi: 10.1517/14656566.2014.957180. Epub 2014 Sep 26 [MEDLINE]