Weaning is the Process of Decreasing Ventilator Support and Increasing the Patient Work of Breathing
Weaning Can Range from an Abrupt Transition of the Workload from the Ventilator to the Patient (i.e. Extubation) to a Gradual Transition of the Workload from the Ventilator to the Patient (Pressure Support Trials with a Progressive Decrease in the Amount of Pressure Support)
Subsequently, After the Patient Manifests Successful Weaning During a Spontaneous Breathing Trial, Extubation Can Be Considered
Assessment of Patient Readiness to Wean
Clinicians Frequently Underestimate the Ability of Patients to Wean from the Ventilator
Studies Suggest that Many Patients were Successfully Extubated on the First Day that They were Assessed for Readiness to Extubate (Am J Respir Crit Care Med, 1994) [MEDLINE] (NEJM, 1995) [MEDLINE]
In Patients with Unplanned Extubation, Reintubation Rates were Only 56%, Suggesting that 44% of Patients Were Ready to Extubate at the Time (Am J Respir Crit Care Med, 2000) [MEDLINE]
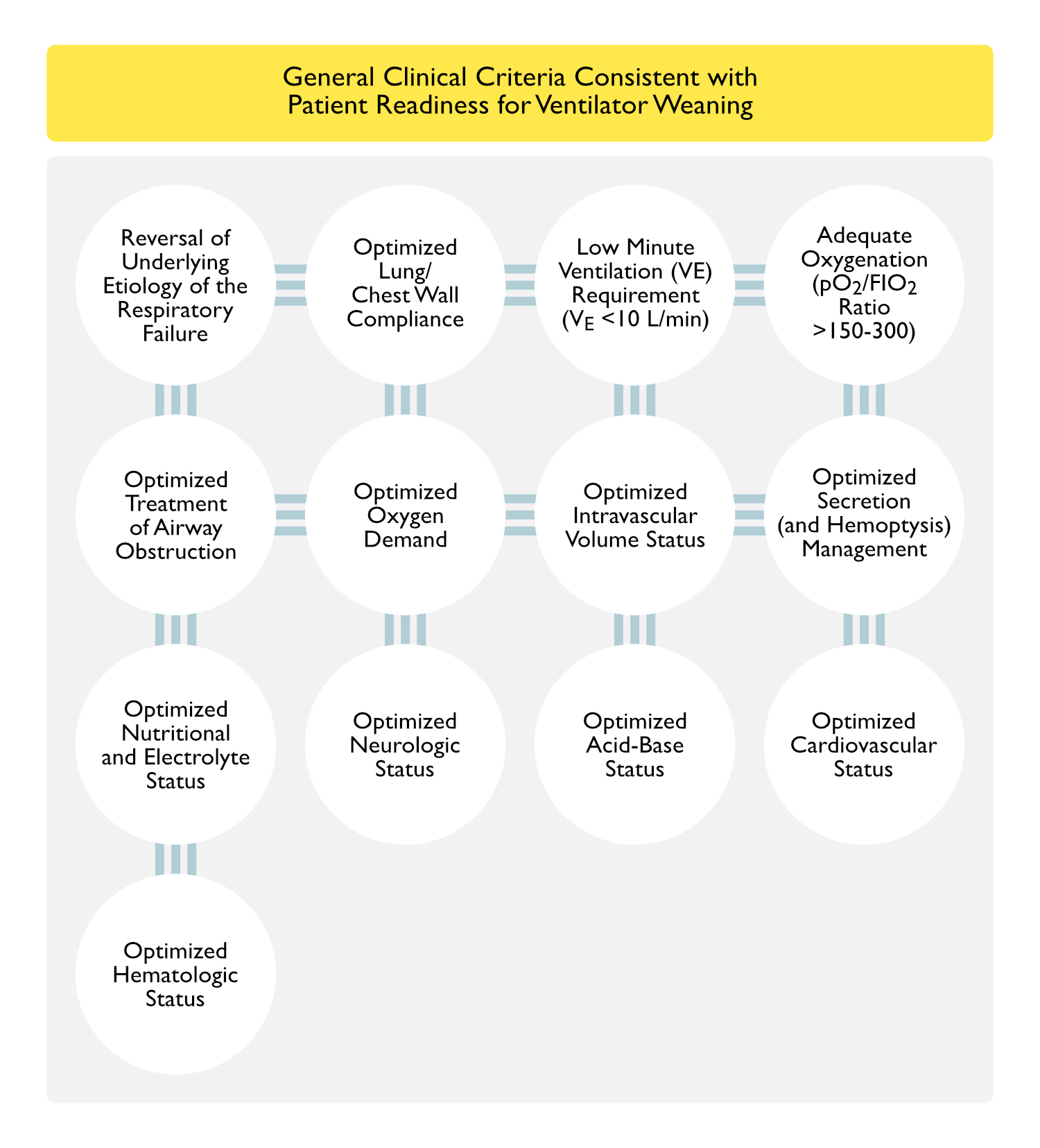
Clinical Criteria Consistent with Patient Readiness for Ventilator Weaning
General Clinical Criteria
Reversal of Underlying Etiology of the Respiratory Failure
Adequate Resolution of Particularly Cardiogenic Pulmonary Edema, Pneumonia, etc
Optimized Lung/Chest Wall Compliance
Absence of a Pulmonary Process Which Significantly Increases the Work of Breathing (Severe Pneumonia, Large Pleural Effusion, etc)
Absence of a Chest Wall/Abdominal Process Which Significantly Increases the Work of Breathing ((Abdominal Compartment Syndrome, Ascites, etc)
Low Minute Ventilation (VE) Requirement (Generally VE <10 L/min)
Adequate Oxygenation (Generally, pO2 >60 mm Hg on FIO2 ≤40%, pO2/FIO2 Ratio >150-300, PEEP ≤10 cm H2O)
Optimized Treatment of Airway Obstruction
Treated with Bronchodilators, Corticosteroids, etc
Optimized Oxygen Demand
Absence of Physiologic Processes Which Increase Oxygen Consumption (Fever, Anxiety, Agitation, etc)
Optimized Intravascular Volume Status
Extubation (Removal of Positive-Pressure Mechanical Ventilation) Results in an Effective Increase in Right-Sided Venous Return, Which May Exacerbate Congestive Heart Failure)
Optimized Secretion (and Hemoptysis) Management
Ability to Safely Manage Secretions (and Any Hemoptysis) Post-Extubation
Optimized Nutritional and Electrolyte Status
Absence of Severe Malnutrition Which Might Impair Respiratory Neuromuscular Function
Absence of Any Electrolyte Disturbance Which Might Impair Respiratory Neuromuscular Function (Hypokalemia, Hypophosphatemia, etc) or Mental Status (Hyponatremia, etc)
Optimized Neurologic Status
Adequate Mental Status to Allow the Patient to Follow Directions and Cough to Clear Secretions
Absence of Ongoing Sedative/Opiate Infusions
Absence of Recent Paralytic Use
Optimized Acid-Base Status
Absence of Metabolic Acidosis (Which Would Contribute to Excessive Work of Breathing Post-Extubation)
Absence of Metabolic Alkalosis (Which Would Decrease Respiratory Drive Post-Extubation)
Optimized Cardiovascular Status
Absence of Significant Tachycardia/Active Arrhythmias
Absence of Hypotension/Shock Which Requires Significant Amount of Vasopressors
Absence of Unstable Coronary Artery Disease with Myocardial Ischemia
Optimized Hematologic Status
Absence of Severe Anemia (Hb <7 g/dL in Patient without Ischemic Cardiovascular Disease or Hb <10 g/dL in Patient with Ischemic Cardiovascular Disease)
Criteria from Evidence-Based Guidelines for Weaning from the American College of Chest Physicians, American Association for Respiratory Care, and the American College of Critical Care Medicine (Chest, 2001) [MEDLINE]
Required Criteria
Cause of Respiratory Failure Has Improved
pO2/FIO2 Ratio ≥150 or SpO ≥90% on FIO4 ≤40% and PEEP ≤5 cm H2O
pH >7.25
Hemodynamic Stability (No or Low-Dose Vasopressor Requirement) without Myocardial Ischemia
Able to Initiate Respiratory Effort
Optional Criteria
Hemoglobin ≥7 g/dL
Core Temperature ≤38-38.5 Degrees C
Awake or Alert/Easily Arousable Mental Status
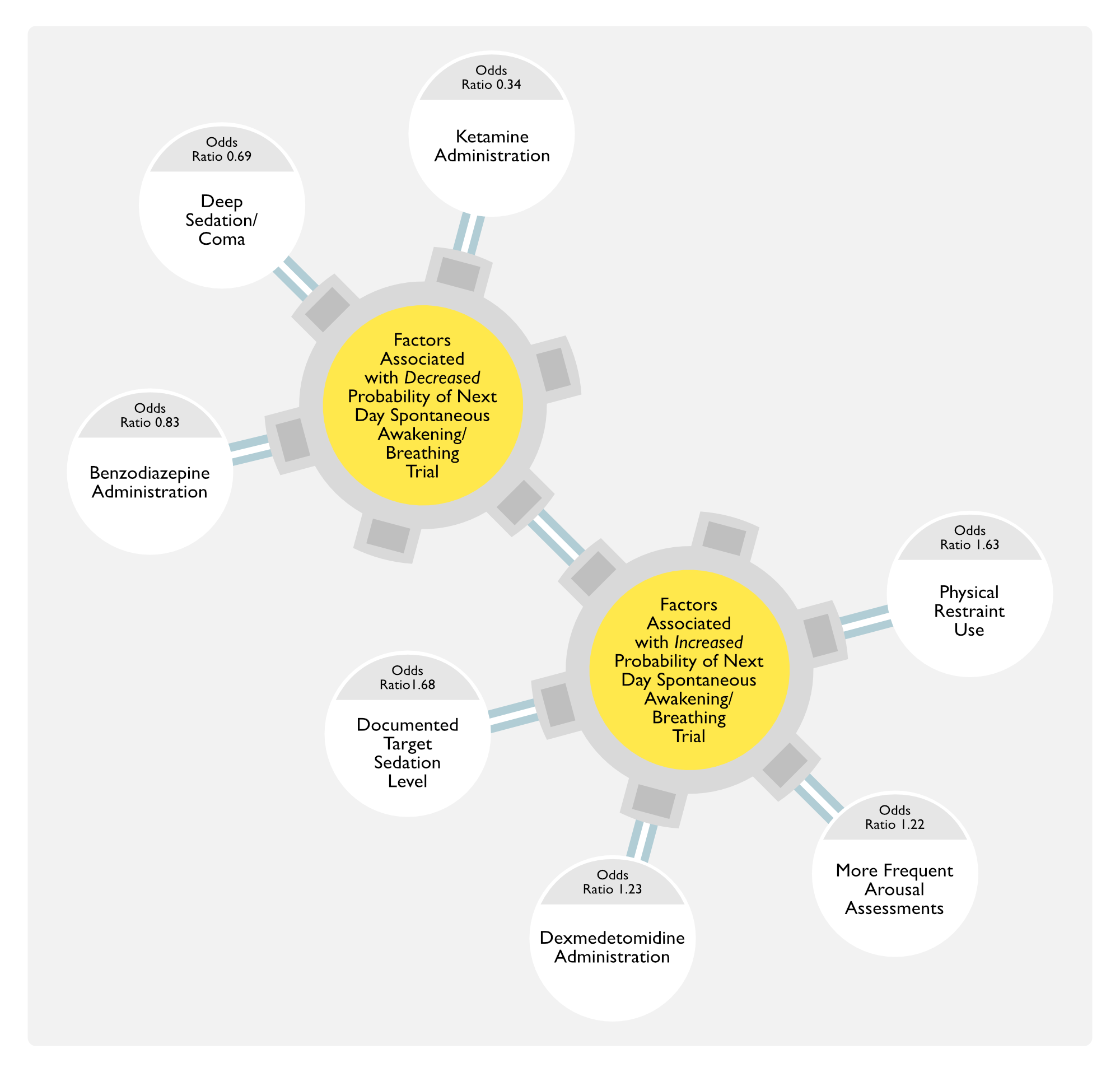
Prediction of Patient Undergoing a Spontaneous Awakening Trial/Spontaneous Breathing Trial
Study of Predictors of Patient Undergoing Next-Day Spontaneous Awakening Trial/Spontaneous Breathing Trial from National Quality Improvement Data (Chest, 2022) [MEDLINE]
Population Included Patients from 68 Intensive Care Units
Spontaneous Awakening Trial: n = 4,847
Spontaneous Breathing Trial: n = 4,936
Factors Associated with Higher Odds of a Next-Day Spontaneous Awakening Trial/Spontaneous Breathing Trial
Assessment of the Quality of Weaning Parameters for Predicting Weaning Success/Failure
Likelihood Ratios are Probably the Best Metric (Since They are Independent of the Pretest Probability of Weaning Success)
Positive Likelihood Ratio (Likelihood Ratio for Positive Results) = Sensitivity/1-Specificity
LR = 1-2 -> none/minimal
LR = 2-5 -> small
LR = 5-10 -> moderate
LR = >10 -> large
The Greater the Deviation of the Positive Likelihood Ratio is from 1, the More Powerful a Positive Test is as a Predictor of a Positive Outcome
Negative Likelihood Ratio (Likelihood Ratio for Negative Results) = 1-Sensitivity/Specificity
LR = 0.1-1 -> none/minimal
LR = 0.3-0.5 -> small
LR =0.1-0.3 -> moderate
LR = <0.1 -> large
The Greater the Deviation of the Negative Likelihood Ratio is from 1, the More Powerful a Negative Test is as a Predictor of a Negative Outcome
Positive and Negative Predictive Values are Generally Not Optimal Metrics for Assessing the Quality of a Weaning Predictor, Since They Vary According to the Pretest Probability (i.e. Prevalence) of Weaning Success in the Studied Population
Clinical Efficacy
Study of Prognostic Value of Daily Weaning Parameters (Intensive Care Med, 1999) [MEDLINE]: n = 216
Daily Weaning Parameters Had an 82% Accuracy for Predicting Successful Extubation
Daily Weaning Parameters Had a 73% Accuracy for Predicting In-Hospital Survival
Prognostic Value of Daily Weaning Parameters for Predicting Extubation Decreased Over Time
Passing Weaning Parameters Within 5 Days of Intubation: average time to extubation = 3 days
Passing Weaning Parameters After 10 Days of Intubation: average time to extubation = 8 days
Approximately 30% of Patients Failed Weaning Parameters, But Were Able to Be Successfully Extubated Anyway
Study of Conservative vs Liberal Transfusion Strategies on Mechanical Ventilation Outcomes (Chest, 2001) [MEDLINE]
Liberal Blood Transfusion Strategy (Maintaining Hb 10-12 g/dL) Did Not Decrease the Duration of Mechanical Ventilation in Critically Ill Patients
Retrospective Study of Impact of Transfusion Strategy on Mechanical Ventilation Outcomes (PLoS One, 2013) [MEDLINE]: n = 751 (138 were difficult to wean from mechanical ventilation)
Patients with Hemoglobin Level >10 g/dL were More Likely to Be Successfully Weaned from Mechanical Ventilation, as Compared to Patients with Hemoglobin <8 g/dL (Odds Ratio3.69; 95% CI: 1.22-11.15 for Hemoglobin 8-10 g/dL and Odds Ratio 4.16, 95% CI: 1.30-13.29 for Hemoglobin >10 g/dL)
Multivariate Analysis Demonstrated that the Odds Ratio for Weaning Success Remained Significant for Hemoglobin Levels 8-10 g/dL (Adjusted Odds Ratio 3.3; 95% CI: 1.07-10.15) with Borderline Significance for Hemoglobin Levels >10 g/dL (adjusted Odds Ratio 2.95, 95% CI: 0.88-9.96)
Randomized, Controlled Trial of Weaning Predictors (pO2/FIO2 Ratio, PEEP, Hemodynamic Stability, Mental Status, Cough) with RSBI-Dependent or RSBI-Independent Weaning (Crit Care Med, 2006) [MEDLINE]: n = 304
Overall Weaning Success: 59% (similar to other trials, suggesting no selection bias in the trial)
Including RSBI in a Protocol Prolonged the Weaning Time
RSBI Did Not Confer a Survival Benefit or Decrease the Incidence of Extubation Failure or Tracheostomy
Critique: study used a single RSBI threshold (rather than graded RSBI levels, as many clinicians might use)
Study of Cough Test and Diaphragmatic Ultrasound in Predicting Spontaneous Breathing Trial and Extubation Success (Crit Care, 2023) [MEDLINE]: n = 367
Equation for Prediction of Success of the Spontaneous Breathing Trial: (0.56 × Cough) – (0.13 × Diaphragmatic Contraction Velocity) + 0.25
When the Cutoff Point was ≥ 0.83, the Sensitivity for Success of the Spontaneous Breathing Trial was 91.5%, the Specificity was 22.1%, and the Overall Accuracy was 76.2%
Area Under the ROC Curve (AUC-ROC) was 0.63
Equation for Prediction of Success of Extubation: (5.7 × SBT) + (0.75 × Cough) – (0.25 × DCV) – 4.5
When the Cutoff Point was ≥ 1.25, the Sensitivity for Success of Extubation was 96.8%, the Specificity was 78.4%, and the Overall Accuracy was 91.5%
Study of the Effect of Sepsis on Weaning Outcomes in Patients Recovering from Respiratory Failure (Chest, 1997) [MEDLINE]
Patients with Respiratory Failure and Sepsis Breathe with a Higher Respiratory Rate/Tidal Volume Ratio, Have a Lower Maximal Inspiratory Pressure, and Tend to More Likely Encounter First Day Ventilator Weaning Failure, as Compared to Patients with Respiratory Failure without Sepsis
Severity of Illness on ICU Admission Could Explain Some of These Differences
Analysis of Prospective Cohort Study Evaluating the Impact of Fever on Ventilator Weaning in Patients with Acute Respiratory Distress Syndrome (Ann Am Thorac Soc, 2013) [MEDLINE]: n = 450 (from 13 ICU’s at 4 hospitals in Baltimore, Maryland)
Only 12% of Patients were Normothermic During the First 3 Days After Onset of Acute Respiratory Distress Syndrome
Fever was Associated with Delayed Liberation from Mechanical Ventilation
During the First Week Post-Acute Respiratory Distress Syndrome, Each Additional Day of Fever Resulted in a 33% Reduction in the Likelihood of Successful Ventilator Liberation (95% Confidence Interval for Adjusted Hazard Ratio, 0.57-0.78; P<0.001
Hypothermia was Associated with Delayed Liberation from Mechanical Ventilation and Increased Mortality Rate
Hypothermia was Independently Associated with Decreased Ventilator-Free Days (Hypothermia During Each of the First 3 Days: Reduction of 5.58 Days, 95% CI: -9.04 to -2.13; P = 0.002)
Hypothermia was Independently Associated with Increased Mortality (Hypothermia During Each of the First 3 Days: Relative Risk, 1.68; 95% CI: 1.06-2.66; P = 0.03)
Hemodynamic Stability
Clinical Efficacy
Randomized, Controlled Trial of Weaning Predictors (Crit Care Med, 2006) [MEDLINE]: n = 304
Study Assessed pO2/FIO2 Ratio, PEEP, Hemodynamic Stability, Mental Status, Cough, and RSBI with Randomization to RSBI-Dependent or Independent Weaning
Overall Weaning Success: 59% (similar to other trials)
Including RSBI in a Protocol Prolonged the Weaning Time
RSBI Did Not Confer a Survival Benefit or Decrease the Incidence of Extubation Failure or Tracheostomy
Critique: study used a single RSBI threshold (rather than graded RSBI levels, as many clinicians might use)
Mental Status
Clinical Efficacy
Prospective Cohort Study of Weaning Brain-Injured Patients (Am J Respir Crit Care Med, 2000) [MEDLINE]: n = 136
Approximately 73% of Patients were Extubated within 48 hrs of Meeting Readiness Criteria: the other 27% remained intubated for a meedian of 3 days (range: 2-19 days)
Practice Variation Existed After Stratifying for Differences in Glasgow Coma Scale Scores (10 vs 7, p<0.001) at Time of Meeting Readiness Criteria, Particularly for Comatose Patients
Median Hospital Charges were $29,057 Higher for Extubation Delay Patients (p<0.001)
Study of Predictors of Successful Extubation in Neurosurgical Patients (Am J Respir Crit Care Med, 2001) [MEDLINE]
Multivariate Analysis Demonstrated that Glasgow Coma Scale Score (GCS) (p<0.0001) and pO2/FIO2 Ratio (p<0.0001) Were Associated with Extubation Success
Odds of Successful Extubation Increased by 39% with Each GCS Score Increment
GCS Score ≥8 at Extubation was Associated with Success in 75% of Cases, as Compared to 33% for a GCS Score <8 (p<0.0001)
Risk Factors for Extubation Failure Include Low Cough Peak Flow (≤60 L/min), Increased Endotracheal Secretions (Secretions >2.5 ml/hr), and Inability to Complete 4 Simple Tasks (Open Eyes, Follow with Eyes, Grasp Hand, Stick Out Tongue) (Intensive Care Med, 2004) [MEDLINE]
Failure Rate was 100% for Patients with All 3 Risk factors, as Compared to 3% for Those with 0 Risk Factors (RR=23.2; 95% CI: 3.2-167.2)
Presence of Any 2 of the Risk Factors had a Sensitivity of 71% and Specificity of 81% in Predicting Extubation Failure
Patients Who Failed a Trial of Extubation were 3.8x More Likely to Have Any 2 Risk Factors, as Compared to Those Who were Successful
Randomized, Controlled Trial of Weaning Predictors (Crit Care Med, 2006) [MEDLINE]: n = 304
Study Assessed pO2/FIO2 Ratio, PEEP, Hemodynamic Stability, Mental Status, Cough, and RSBI with Randomization to RSBI-Dependent or Independent Weaning
Overall Weaning Success: 59% (similar to other trials)
Including RSBI in a Protocol Prolonged the Weaning Time
RSBI Did Not Confer a Survival Benefit or Decrease the Incidence of Extubation Failure or Tracheostomy
Critique: study used a single RSBI threshold (rather than graded RSBI levels, as many clinicians might use)
French Study of Peak Cough Expiratory Flow as a Predictor of Extubation Success (Intensive Care Med, 2009) [MEDLINE]: n = 130
Inability to Cough on Command or a Peak Cough Expiratory Flow ≤35 l/min Predicted Extubation Failure with a Sensitivity of 79% and a Specificity of 71%
Risk of Extubation Failure was 24% for the Patients Who Did Not Cough on Command or with a Peak Cough Expiratory Flow ≤35 l/min and 3.5% for those with a Peak Cough Expiratory Flow >35 l/min (RR = 6.9 (95% CI: 2-24; P = 0.002)
Mean Peak Cough Flow of Patients Who Failed Extubation (36.3 +/- 15 L/min) was Significantly Lower than the One of Patients Who Succeeded (63.6 +/- 32 L/min) (P<0.001)
Measures of Oxygenation (as Measured by pO2/FIO2 Ratio, etc)
General Comments
While Oxygenation is a Critical Factor to Consider for Weaning/Extubation, it is a Relatively Poor Predictor of Weaning Success
Clinical Efficacy
Single-Center Retrospective Study of Weaning Criteria in Elderly (≥70 y/o) Patients (Crit Care Med, 1989) [MEDLINE]: n = 241
Parameters: spontaneous respiratory rate, tidal volume, minute ventilation, maximal inspiratory pressure (MIP), pH, pCO2, pO2, and pO2/FIO2 ratio
MIP and pH were Lower in the Unsuccessfully Weaned Group, Although the Mean Absolute Differences were Small (-32 vs -38 cm H2O and 7.42 vs. 7.44 cm H2O, respectively)
All Parameters Had Good Positive Predictive Value, But Poor Negative Predictive Value (≤22%) and Only Marginal Diagnostic Accuracy (58-86%)
However, the Pretest Probability of Weaning Success was Unusually High (90%) in this Study
Randomized, Controlled Trial of Weaning Predictors (Crit Care Med, 2006) [MEDLINE]: n = 304
Study Assessed pO2/FIO2 Ratio, PEEP, Hemodynamic Stability, Mental Status, Cough, and RSBI with Randomization to RSBI-Dependent or Independent Weaning
Overall Weaning Success: 59% (similar to other trials)
Including RSBI in a Protocol Prolonged the Weaning Time
RSBI Did Not Confer a Survival Benefit or Decrease the Incidence of Extubation Failure or Tracheostomy
Critique: study used a single RSBI threshold (rather than graded RSBI levels, as many clinicians might use)
Randomized, Controlled Trial of Ventilator Weaning Protocol ofr Mechanically-Ventilated Patients in the ICU (Lancet, 2008) [MEDLINE]: n = 336
Spontaneous Breathing Trials were Safe and Successful Even in Patients with Poorer Oxygenation (pO2/FIO2 Ratio 110-120)
Minute Ventilation (VE)
General Comments
Minute Ventilation Requirement is Inversely Correlated with the Efficiency of Carbon Dioxide Excretion by the Lungs
Minute Ventilation Requirements Can Be Increased by Factors Which Increase Metabolic Demand, Resulting in Increased Carbon Dioxide Production (Fever, etc) and the Presence of Decreased Bicarbonate Buffer (Due to Metabolic Acidosis)
Minute Ventilation Can Also Increase Due to Factors Which Increase Central Respiratory Drive (Agitation, Pain, Central Nervous System Disease, etc)
Clinical Efficacy
Systematic Review of Various Factors Predicting Successful Weaning (Chest, 2001) [MEDLINE]: n = 65 observational studies
Minute Ventilation
Minute Ventilation was a Poor Predictor of Weaning Outcome
After Pooling, Respiratory Rate of >38 Breaths/min Decreased the Probability of Successful Extubation
Maximal Inspiratory Pressure (MIP)
MIP Had a Low Sensitivity and Specificity in Predicting Weaning Success
After Pooling, Maximal Inspiratory Pressure (PImax) <0.3 (More Negative than -30 cm H2O) Had a Pooled Likelihood Ratio of 2.23 (95% CI: 1.15 to 4.34), Indicating that it Appeared to Marginally Increase the Likelihood of Successful Extubation
Rapid Shallow Breathing Index (RSBI)
Unpooled, RSBI Had Positive Likelihood Ratio of 1.66 -> indicates that there was small increase in the probability of weaning success in patients with a positive RSBI
Unpooled, RSBI Had Negative Likelihood Ratio of 0.11 -> indicates that there was a moderate increase in the probability of weaning failure in patients with a negative RSBI
After Pooling, RSBI of >100 Decreased the Probability of Successful Extubation
Based on Receiver Operator Curve for All of the Variables, None of the Variables Demonstrated More than Modest Accuracy in Predicting Weaning Outcome: may be related to the fact that clinicians have already considered the results when they choose patients for trials of weaning
Prospective Study of Weaning Parameters in Predicting Outcome from Ventilator Weaning (NEJM, 1991) [MEDLINE]
Pretest Probability of Weaning Success in Study Population: 60%
Sensitivity was the Highest for Maximal Inspiratory Pressure (Plmax) (1.00), Followed Closely by the Respiratory Rate/Tidal Volume Ratio (Rapid Shallow Breathing Index, RSBI) (0.97)
Specificity was the Highest for the Respiratory Rate/Tidal Volume Ratio (Rapid Shallow Breathing Index, RSBI) (0.64) and Lowest for Maximal Inspiratory Pressure (Plmax) (0.11)
Respiratory Rate/Tidal Volume Ratio (Rapid Shallow Breathing Index, RSBI) was the Best Predictor of Successful Weaning
Positive Likelihood Ratio for RSBI: 2.7 -> means that there was a small increase in the probability of weaning success with positive RSBI (<105)
Negative Likelihood Ratio for RSBI: 0.05 -> means that there was large increase in the probability of weaning failure with negative RSBI (≥105)
Maximal Inspiratory Pressure (Plmax) and the Respiratory Rate/Tidal Volume Ratio (Rapid Shallow Breathing Index, RSBI) were the Best Predictors of Failure
The Area Under the ROC Curve for the Respiratory Rate/Tidal Volume Ratio (Rapid Shallow Breathing Index, RSBI) (0.89) was Larger than that Under the Curves for the CROP Index (0.78, P<0.05), Maximal Inspiratory Pressure (Plmax) (0.61, P less than 0.001), and Minute Ventilation (VE) (0.40, P<0.001
Compliance Had a Poor Predictive Capacity
Study of Integrative Weaning Index (IWI) in Predicting Weaning Outcome (Crit Care, 2009) [MEDLINE]: n = 331
Integrative Weaning Index (IWI) = Static Compliance x Arterial Oxygen Saturation/Respiratory Rate/Tidal Volume
Integrative Weaning Index (IWI) Area Under the ROC Curves was Larger than that Under the Curves for the Respiratory Rate/Tidal Volume Ratio (0.96 vs 0.85, respectively; P = 0.003)
Integrative Weaning Index was the Best Predictive Performance Index for Weaning Outcome in the ICU Setting
Work of Breathing
General Comments
Work of Breathing Can Be Measured Using the Tidal Volume and Intrathoracic Pressure Generated by Respiratory Muscle Contraction (Using an Esophageal Balloon Measurement Device)
It is Unclear if Work of Breathing Measurements are Superior to Other Less Invasive Methods in Predicting Weaning Success
Clinical Efficacy
Study of Work of Breathing in Predicting Success of Weaning (Chest, 1988) [MEDLINE]: n = 17
Bedside Weaning Parameters are Associated with Weaning Success in Patients Requiring Brief Mechanical Ventilation
In Patients Requiring Prolonged Ventilation, Work of Breathing Measurements May Be a Better Predictor of Successful Weaning
Study of Work of Breathing in Predicting Weaning Outcome (Chest, 1995) [MEDLINE]
Measurement of Patient Work of Breathing was Less Accurate than Conventional Weaning Parameters and Clinical Judgement fro Predicting Successful Extubation
Study of Work of Breathing in Patients Failing Weaning from Mechanical Ventilation (Am J Respir Crit Care Med, 1997) [MEDLINE]
The Product of Inspiratory Pressure-Time Product and pCO2, an Index of Inefficient Carbon Dioxide Clearance, was More than Twice as High in the Failure Group than in the Success Group at the End of the Trial (p<0.0005)
Study of Tension-Time Index and Respiratory Rate/Tidal Volume Ratio in Predicting Weaning Success (Am J Respir Crit Care Med, 1998) [MEDLINE]
Tension-Time Index and the Respiratory Rate/Tidal Volume Ratio are the Major Pathophysiologic Determinants Underlying the Transition from Weaning Failure to Weaning Success
Study of Load Balance and Respiratory Rate/Tidal Volume Ratio in Predicting Weaning Success (Intensive Care Med, 2006) [MEDLINE]
Combination of Mean Paw/MIP and Respiratory Rate/Tidal Volume Ratio in a Simplified Discriminant Function is Useful in Predicting Weaning Outcome
Oxygen Cost of Breathing
General Comments
Oxygen Cost of Breathing is the Difference Between Oxygen Consumption While Breathing Spontaneously and Oxygen Consumption While Breathing on Mechanical Ventilation
Requires a Metabolic Cart to Measure (Although Non-Pulmonary Changes in Oxygen Consumption Can Complicate Measurement)
In Normal Subjects, Oxygen Cost of Breathing is <5% of Total Oxygen Consumption
In Patients Being Weaned (Especially Those Failing Weaning), Oxygen Cost of Breathing May Be >50% of Total Oxygen Consumption
Clinical Efficacy
Study of the Oxygen Cost of Breathing (Chest. 1988) [MEDLINE]
Sensitivity and Specificity of Increase in Oxygen Consumption (Delta VO2) and Respiratory Power Output (Wresp were Insufficient for Evaluation of Disease State and Weaning Decisions in Individual Patients
Airway Occlusion Pressure
General Comments
Measurement of Respiratory Drive Can Be Obtained by Occluding the Airway During Inspiration and Measuring the Airway Pressure Generated During the First 0.1 sec (P0.1) of the Occlusion
In Normal Subjects, P0.1 is <2 cm H2O
Patients Failing Weaning Have Higher P0.1 Values (Due to Elevated Inspiratory Drive)
Clinical Efficacy
Study of Airway Occlusion Pressure in Patients Failing Weaning (Am Rev Respir Dis, 1987) [MEDLINE]
Airway Occlusion Pressure >6 cm H2O Has Been Associated with Weaning Failure
Evaluation of Maximal Inspiratory Pressure (Pimax) and Airway Occlusion Pressure (P0.1) in Predicting Weaning Outcome (J Crit Care, 2009) [MEDLINE]
P0.1 (Area Under ROC 0.76) and P0.1/Pimax Ratio (Area Under ROC 0.78) were Moderately Accurate in Predicting Weaning Outcome
Pimax was Less Accurate in Predicting Weaning Outcome (Area Under ROC 0.52)
Maximal Inspiratory Pressure (MIP, PImax, or Pimax)
General Comments
Maximal Inspiratory Pressure is an Assessment of Inspiratory Muscle Strength
Measured Using a Manometer with an Occluded Airway
Measurement Can Be Problematic in a Spontaneously Breathing Patient, Often Underestimating the True MIP Due to Inadequate Patient Effort (Am Rev Respir Dis, 1990) [MEDLINE]
One-Way Valve Devices with Prolonged Occlusion (20-25 sec) May Improve the Measurement
MIP Assesses Only the Respiratory Muscle Strength, But Does Not Assess the Inspiratory Load Placed on the Muscles
Clinical Efficacy
Study of Bedside Weaning Parameters in Predicting Ventilator Weaning (Chest, 1973) [MEDLINE]
MIP Greater than -30 cm H20 (More Negative) was Associated with Weaning Success
MIP Less than -20 cm H2O (Less Negative) was Associated with Weaning Failure
Prospective Study of Weaning Parameters in Predicting Outcome from Ventilator Weaning (NEJM, 1991) [MEDLINE]
Pretest Probability of Weaning Success in Study Population: 60%
Sensitivity was the Highest for Maximal Inspiratory Pressure (Plmax) (1.00), Followed Closely by the Respiratory Rate/Tidal Volume Ratio (Rapid Shallow Breathing Index, RSBI) (0.97)
Specificity was the Highest for the Respiratory Rate/Tidal Volume Ratio (Rapid Shallow Breathing Index, RSBI) (0.64) and Lowest for Maximal Inspiratory Pressure (Plmax) (0.11)
Respiratory Rate/Tidal Volume Ratio (Rapid Shallow Breathing Index, RSBI) was the Best Predictor of Successful Weaning
Positive Likelihood Ratio for RSBI: 2.7 -> means that there was a small increase in the probability of weaning success with positive RSBI (<105)
Negative Likelihood Ratio for RSBI: 0.05 -> means that there was large increase in the probability of weaning failure with negative RSBI (≥105)
Maximal Inspiratory Pressure (Plmax) and the Respiratory Rate/Tidal Volume Ratio (Rapid Shallow Breathing Index, RSBI) were the Best Predictors of Failure
The Area Under the ROC Curve for the Respiratory Rate/Tidal Volume Ratio (Rapid Shallow Breathing Index, RSBI) (0.89) was Larger than that Under the Curves for the CROP Index (0.78, P<0.05), Maximal Inspiratory Pressure (Plmax) (0.61, P less than 0.001), and Minute Ventilation (VE) (0.40, P<0.001
Compliance Had a Poor Predictive Capacity
Systematic Review of Various Factors Predicting Successful Weaning (Chest, 2001) [MEDLINE]: n = 65 observational studies
Minute Ventilation
Minute Ventilation was a Poor Predictor of Weaning Outcome
After Pooling, Respiratory Rate of >38 Breaths/min Decreased the Probability of Successful Extubation
Maximal Inspiratory Pressure (MIP)
MIP Had a Low Sensitivity and Specificity in Predicting Weaning Success
After Pooling, Maximal Inspiratory Pressure (PImax) <0.3 (More Negative than -30 cm H2O) Had a Pooled Likelihood Ratio of 2.23 (95% CI: 1.15 to 4.34), Indicating that it Appeared to Marginally Increase the Likelihood of Successful Extubation
Rapid Shallow Breathing Index (RSBI)
Unpooled, RSBI Had Positive Likelihood Ratio of 1.66 -> indicates that there was small increase in the probability of weaning success in patients with a positive RSBI
Unpooled, RSBI Had Negative Likelihood Ratio of 0.11 -> indicates that there was a moderate increase in the probability of weaning failure in patients with a negative RSBI
After Pooling, RSBI of >100 Decreased the Probability of Successful Extubation
Based on Receiver Operator Curve for All of the Variables, None of the Variables Demonstrated More than Modest Accuracy in Predicting Weaning Outcome: may be related to the fact that clinicians have already considered the results when they choose patients for trials of weaning
Evaluation of Maximal Inspiratory Pressure (Pimax) and Airway Occlusion Pressure (P0.1) in Predicting Weaning Outcome (J Crit Care, 2009) [MEDLINE]
P0.1 (Area Under ROC 0.76) and P0.1/Pimax Ratio (Area Under ROC 0.78) were Moderately Accurate in Predicting Weaning Outcome
Pimax was Less Accurate in Predicting Weaning Outcome (Area Under ROC 0.52)
Observational Prospective Study of Time Inspiratory Effort (TIE), the Integrative Weaning Index (IWI), and Rapid Shallow Breathing Index (RSBI) in Predicting Weaning Outcome (J Intensive Care Med, 2015) [MEDLINE]: n = 103
TIE Index is the Maximal Inspiratory Pressure and the Occlusion Time Required to Reach it
TIE Had the Largest Area Under the Receiver Operating Curve of All the Indices
Gastric Mucosal Acidosis
General Comments
Since Blood Flow May Be Diverted from the Splanchnic Bed to the Respiratory Muscles During Weaning (Especially During Weaning Failure, Resulting in Gastric Mucosal Ischemia), Measurement of Gastric Mucosal Acidosis May Be Useful
Measurement Requires a Nasogastric Tube
Clinical Efficacy
Study of Gastric Mucosal Acidosis in Weaning Failure (Ann Intern Med, 1993) [MEDLINE]: n = 29
Gastrointestinal Acidosis May Be an Early Sign of Weaning Failure
Uruguayan Prospective Clinical Study of Gastric Mucosal Acidosis in Weaning Patients (Crit Care Med, 2001) [MEDLINE]
Weaning Failure was Associated with Gastric Intramucosal Acidosis
Diaphragmatic Ultrasound
General Comments
Using B-Mode or M-Mode Ultrasound, Diaphragmatic Function Can Be Assessed to Determine the Probability of Weaning Success
Clinical Efficacy
Study of Diaphragmatic Ultrasound in Predicting Weaning Success (Crit Care Med, 2011) [MEDLINE]
Less than 10 mm of Diaphragmatic Descent, or Paradoxical Diaphragmatic Ascent During Inspiration was Associated with Longer Ventilator Weaning Time
Study of Diaphragmatic Ultrasound in Predicting Weaning Success (Thorax, 2014) [MEDLINE]: n = 63
Diaphragmatic Thickening Fraction of >30% was Associated with a Sensitivity 88%, Specificity of 71%, Positive-Predictive Value of 91%, and Negative-Predictive Value of 63% for Predicting Extubation Success
Systematic Review and Meta-Analysis of Diaphragmatic Ultrasound in Predicting Weaning Success (Chest, 2017) [MEDLINE]: n = 1,071 (19 studies)
Both Diaphragmatic Thickening Fraction (Pooled Odds Ratio = 21) and Diaphragmatic Excursion (Pooled Odds Ratio = 10) Predicted Weaning Outcome
Study of Diaphragmatic Ultrasound and Rapid Shallow Breathing Index (RSBI) in Predicting Weaning Success (J Intensive Care, 2018) [MEDLINE]
The Combination of Diaphragmatic Ultrasound and Rapid Shallow Breathing Index (RSBI Increased Accuracy of Predicting Weaning Outcome
Study of Cough Test and Diaphragmatic Ultrasound in Predicting Spontaneous Breathing Trial and Extubation Success (Crit Care, 2023) [MEDLINE]: n = 367
Equation for Prediction of Success of the Spontaneous Breathing Trial: (0.56 × Cough) – (0.13 × Diaphragmatic Contraction Velocity) + 0.25
When the Cutoff Point was ≥ 0.83, the Sensitivity for Success of the Spontaneous Breathing Trial was 91.5%, the Specificity was 22.1%, and the Overall Accuracy was 76.2%
Area Under the ROC Curve (AUC-ROC) was 0.63
Equation for Prediction of Success of Extubation: (5.7 × SBT) + (0.75 × Cough) – (0.25 × DCV) – 4.5
When the Cutoff Point was ≥ 1.25, the Sensitivity for Success of Extubation was 96.8%, the Specificity was 78.4%, and the Overall Accuracy was 91.5%
Area Under the ROC Curve (AUC-ROC) was 0.91
Rapid Shallow Breathing Index (RSBI)
Clinical Use
Rapid Shallow Breathing Index (RSBI) is the Most Commonly Used Weaning Parameter/Predictor
Rationale
Patients with High Work of Breathing (and Highest Risk to Fail Weaning and Extubation) Tend to Breathe at High Respiratory Rates with Low Tidal Volumes
Based on Studies of the Clinical Performance of RSBI, a Negative RSBI (RSBI >105) is Better at Identifying Patients Who Will Fail Weaning than a Positive RSBI (RSBI <105) is at Identifying Patients Who Can Be Successfully Weaned
For This Reason, RSBI is Best Utilized to Assess a Patient Who Has Already Been Deemed Stable Enough by Clinical Criteria to Undergo a Spontaneous Breathing Trial, But in Whom There is a Concern as to Whether the Patient Will Succeed with Weaning
RSBI Can Then Identify a Patient Who May Be at High Risk of Weaning Failure to Avoid the Risks of a Failed Spontaneous Breathing Trial in Such a Patient
Technique
RSBI Has Been Traditionally Performed Using One Minute Independent Breathing Trial on CPAP 0 with Pressure Support 0
Original Study Used a Handheld Spirometer to Measure the RSBI (NEJM, 1991) [MEDLINE]
At the End of One Minute, Calculate the Average Respiratory Rate/Average Tidal Volume
Measuring the RSBI While on Ventilator Support: this will result in lower values than those measured on no ventilator support
Use of Pressure Support Ventilation and/or PEEP as Low as 5 cm H2O Influenced the RSBI, While FIO2 Did Not Impact the RSBI (Intensive Care Med, 2008) [MEDLINE]
RSBI is Impacted by the Level of Ventilatory Support, But is Relatively Unaffected by the Technique Used to Determine the Breathing Pattern and the Time of Day at Which it is Measured (Respir Care, 2009) [MEDLINE]
Measuring the RSBI on Ventilators with Flow Triggering: this will result in lower values than those measured on venetilators without flow triggering
Values Measured Through the Ventilator with CPAP-5 cm H2O were Much Lower than the Values Measured with a Handheld Spirometer and Even RSBI Values Measured with CPAP-0 cm H2O were Significantly Lower (Due to Base Flow Delivered by Some Ventilators) (J Crit Care, 2012) [MEDLINE]
RSBI Values were Lower (Approximately 17% Lower) on Ventilators with Flow Triggering (Due to the Base Flow) (J Intensive Care Med, 2015) [MEDLINE]
Measuring RSBI in a Patient with Dynamic Hyperinflation (Due to COPD, Asthma, etc)
Unmeasured Inspiratory Efforts on the Ventilator (Due to the Ventilator Not Sensing These and Properly Triggering) Can Falsely Decrease the RSBI (Am J Respir Crit Care Med, 2000) [MEDLINE]
Factors Which Can Increase the RSBI
Small Diameter Endotracheal Tube (Am J Respir Crit Care Med, 1996) [MEDLINE]
Prospective Study of Weaning Parameters in Predicting Outcome from Ventilator Weaning (NEJM, 1991) [MEDLINE]
Pretest Probability of Weaning Success in Study Population: 60%
Sensitivity was the Highest for Maximal Inspiratory Pressure (Plmax) (1.00), Followed Closely by the Respiratory Rate/Tidal Volume Ratio (Rapid Shallow Breathing Index, RSBI) (0.97)
Specificity was the Highest for the Respiratory Rate/Tidal Volume Ratio (Rapid Shallow Breathing Index, RSBI) (0.64) and Lowest for Maximal Inspiratory Pressure (Plmax) (0.11)
Respiratory Rate/Tidal Volume Ratio (Rapid Shallow Breathing Index, RSBI) was the Best Predictor of Successful Weaning
Positive Likelihood Ratio for RSBI: 2.7 -> means that there was a small increase in the probability of weaning success with positive RSBI (<105)
Negative Likelihood Ratio for RSBI: 0.05 -> means that there was large increase in the probability of weaning failure with negative RSBI (≥105)
Maximal Inspiratory Pressure (Plmax) and the Respiratory Rate/Tidal Volume Ratio (Rapid Shallow Breathing Index, RSBI) were the Best Predictors of Failure
The Area Under the ROC Curve for the Respiratory Rate/Tidal Volume Ratio (Rapid Shallow Breathing Index, RSBI) (0.89) was Larger than that Under the Curves for the CROP Index (0.78, P<0.05), Maximal Inspiratory Pressure (Plmax) (0.61, P less than 0.001), and Minute Ventilation (VE) (0.40, P<0.001
Compliance Had a Poor Predictive Capacity
Systematic Review of Various Factors Predicting Successful Weaning (Chest, 2001) [MEDLINE]: n = 65 observational studies
Minute Ventilation
Minute Ventilation was a Poor Predictor of Weaning Outcome
After Pooling, Respiratory Rate of >38 Breaths/min Decreased the Probability of Successful Extubation
Maximal Inspiratory Pressure (MIP)
MIP Had a Low Sensitivity and Specificity in Predicting Weaning Success
After Pooling, Maximal Inspiratory Pressure (PImax) <0.3 (More Negative than -30 cm H2O) Had a Pooled Likelihood Ratio of 2.23 (95% CI: 1.15 to 4.34), Indicating that it Appeared to Marginally Increase the Likelihood of Successful Extubation
Rapid Shallow Breathing Index (RSBI)
Unpooled, RSBI Had Positive Likelihood Ratio of 1.66 -> indicates that there was small increase in the probability of weaning success in patients with a positive RSBI
Unpooled, RSBI Had Negative Likelihood Ratio of 0.11 -> indicates that there was a moderate increase in the probability of weaning failure in patients with a negative RSBI
After Pooling, RSBI of >100 Decreased the Probability of Successful Extubation
Based on Receiver Operator Curve for All of the Variables, None of the Variables Demonstrated More than Modest Accuracy in Predicting Weaning Outcome: may be related to the fact that clinicians have already considered the results when they choose patients for trials of weaning
Bayesian Analysis of RSBI in Predicting Weaning Outcome (Intensive Care Med, 2006) [MEDLINE]
Much of the Heterogeneity in Performance of RSBI Can Be Explained by Variation in Pretest Probability of Successful Weaning Outcome (Which May Be Secondary to Spectrum and Test-Referral Bias)
Average Sensitivity of 0.87 indicates that RSBI) is a Reliable Screening Test for Successful Weaning
Randomized, Controlled Trial of Weaning Predictors (Crit Care Med, 2006) [MEDLINE]: n = 304
Study Assessed pO2/FIO2 Ratio, PEEP, Hemodynamic Stability, Mental Status, Cough, and RSBI with Randomization to RSBI-Dependent or Independent Weaning
Overall Weaning Success: 59% (similar to other trials)
Including RSBI in a Protocol Prolonged the Weaning Time
RSBI Did Not Confer a Survival Benefit or Decrease the Incidence of Extubation Failure or Tracheostomy
Critique: study used a single RSBI threshold (rather than graded RSBI levels, as many clinicians might use)
Observational Prospective Study of Time Inspiratory Effort (TIE), the Integrative Weaning Index (IWI), and Rapid Shallow Breathing Index (RSBI) in Predicting Weaning Outcome (J Intensive Care Med, 2015) [MEDLINE]: n = 103
TIE Index is the Maximal Inspiratory Pressure and the Occlusion Time Required to Reach it
TIE Had the Largest Area Under the Receiver Operating Curve of All the Indices
Study of Diaphragmatic Ultrasound and Rapid Shallow Breathing Index (RSBI) in Predicting Weaning Success (J Intensive Care, 2018) [MEDLINE]
The Combination of Diaphragmatic Ultrasound and Rapid Shallow Breathing Index (RSBI Increased Accuracy of Predicting Weaning Outcome
Inspiratory Effort Quotient (IEQ)
General Comments
IEQ = [(0.75VT/Cdyn) x (TI/TTOT)]/MIP
VT = Tidal volume
Cdyn = dynamic compliance
TI = inspiratory time
TTOT = respiratory duty cycle
MIP = maximal inspiratory pressure
Clinical Efficacy
Study of Weaning Predictors (Am Rev Respir Dis, 1986) [MEDLINE]
IEQ May Predict Weaning Outcome
CROP Index (Compliance, Rate, Oxygenation, Pressure)
General Comments
CROP Index = [Cdyn * MIP * (PaO2/PAO2)]/R
Cdyn = dynamic compliance
MIP = maximal inspiratory pressure
pO2/PAO2 = ratio of arterial pO2 to alveolar pO2
R = respiratory rate
Clinical Efficacy
Prospective Study of Weaning Parameters in Predicting Outcome from Ventilator Weaning (NEJM, 1991) [MEDLINE]
Pretest Probability of Weaning Success in Study Population: 60%
Sensitivity was the Highest for Maximal Inspiratory Pressure (Plmax) (1.00), Followed Closely by the Respiratory Rate/Tidal Volume Ratio (Rapid Shallow Breathing Index, RSBI) (0.97)
Specificity was the Highest for the Respiratory Rate/Tidal Volume Ratio (Rapid Shallow Breathing Index, RSBI) (0.64) and Lowest for Maximal Inspiratory Pressure (Plmax) (0.11)
Respiratory Rate/Tidal Volume Ratio (Rapid Shallow Breathing Index, RSBI) was the Best Predictor of Successful Weaning
Maximal Inspiratory Pressure (Plmax) and the Respiratory Rate/Tidal Volume Ratio (Rapid Shallow Breathing Index, RSBI) were the Best Predictors of Failure
The Area Under the ROC Curve for the Respiratory Rate/Tidal Volume Ratio (Rapid Shallow Breathing Index, RSBI) (0.89) was Larger than that Under the Curves for the CROP Index (0.78, P<0.05), Maximal Inspiratory Pressure (Plmax) (0.61, P less than 0.001), and Minute Ventilation (VE) (0.40, P<0.001
Compliance Had a Poor Predictive Capacity
CORE Index (Compliance, Oxygenation, Respiration, Effort)
General Comments
CORE Index = [Cdyn * (MIP/P0.1) * (PaO2/PAO2)]/R
Cdyn = dynamic compliance
P0.1 = airway occlusion pressure 0.1 sec after the start of inspiratory flow
MIP = maximal inspiratory pressure
pO2/PAO2 = ratio of arterial pO2 to alveolar pO2
R = respiratory rate
Clinical Efficacy
Study of CORE Index (vs CROP Index, Airway Occlusion Pressure, and RSBI) in Predicting Ventilator Weaning (Respir Care, 2011) [MEDLINE]: n = 47
CORE Index was the Most Accurate Predictor of Weaning Success/Failure
CORE Index Positive Likelihood Ratio was 20 and Negative Likelihood Ratio was 0
Weaning Index (WI)
General Comments
WI = PTI x (VE40/VTsb)
PTI = modified pressure time index (time integral of respiratory muscle pressure, which quantifies ventilatory endurance)
VE40 = minute ventilation needed to bring pCO2 to 40 mmHg (estimate of the efficiency of gas exchange, which quantifies ventilatory endurance)
VTsb = tidal volume during spontaneous breathing
Clinical Efficacy
Study of Weaning Index (WI) (Am Rev Respir Dis, 1991) [MEDLINE]; n = 38
Using a threshold of 4 min-1, WI was Highly Accurate in Predicting Weaning Outcome
Integrative Weaning Index (IWI)
General Comments
IWI = [(Cst,rs) x SaO2]/[f/VT]
Cst,rs = static compliance (Cst,rs)
SaO2 = arterial oxygen saturation
f = respiratory rate
VT = tidal volume
Difficult to Measure in Spontaneously Breathing Patient
Clinical Efficacy
Study of Integrative Weaning Index (IWI) in Predicting Weaning Outcome (Crit Care, 2009) [MEDLINE]: n = 331
Integrative Weaning Index (IWI) = Static Compliance x Arterial Oxygen Saturation/Respiratory Rate/Tidal Volume
Integrative Weaning Index (IWI) Area Under the ROC Curves was Larger than that Under the Curves for the Respiratory Rate/Tidal Volume Ratio (0.96 vs 0.85, respectively; P = 0.003)
Integrative Weaning Index was the Best Predictive Performance Index for Weaning Outcome in the ICU Setting
Observational Prospective Study of Time Inspiratory Effort (TIE), the Integrative Weaning Index (IWI), and Rapid Shallow Breathing Index (RSBI) in Predicting Weaning Outcome (J Intensive Care Med, 2015) [MEDLINE]: n = 103
TIE Index is the Maximal Inspiratory Pressure and the Occlusion Time Required to Reach it
TIE Had the Largest Area Under the Receiver Operating Curve of All the Indices
Bedrest During Critical Illness Adversely Impacts Musculoskeletal, Cardiovascular, Respiratory, and Immune System Function, Slowing Recovery
Immobility-Related Complications (Muscular Atrophy, Decubitus Ulcers, Venous Thromboembolism, etc) are Common in ICU Patients
Profound Weakness is Common (and May Be Persistent for Months-Years) in ICU Survivors
Weakness is Associated with Decreased Post-ICU Survival (Am J Respir Crit Care Med, 2014) [MEDLINE]
Clinical Efficacy
Pooled Meta-Analysis of Early Mobilization Data in Mechanically Ventilated Patients (Am J Respir Crit Care Med, 2017) [MEDLINE]
Early Mobilization Decreased the Duration of Mechanical Ventilation (Mean Difference, 2.7 Fewer Days; 95% CIL 1.19–4.21)
Early Mobilization Patients were More Likely to Be Able to Walk at Discharge (64% vs. 41.4%; RR, 1.56; 95% CI: 1.15–2.10)
There was No Impact on Mortality Rate, ICU Length of Stay, Ability to Walk at ICU Discharge, 6-Minute Walk Distance or Ventilator-Free Days
Trials Did Not Provide Adequate Details to Assess Adverse Events
Recommendations (American Thoracic Society/American College of Chest Physicians Clinical Practice Guideline for Liberation from Mechanical Ventilation in Critically Ill Adults) (Am J Respir Crit Care Med, 2017) [MEDLINE]
For Acutely Hospitalized Adults Who Have Been Mechanically Ventilated for >24 hrs, Protocolized Early Mobilization is Recommended (Conditional Recommendation, Low Certainty of Evidence)
Protocol May Be Implemented by Nurse, Physical Therapist, or Other Clinician
Safety of Weaning
Clinical Efficacy
Study of Large-Scale Respiratory Therapist-Driven Weaning Protocol (Am J Respir Crit Care Med, 1999) [MEDLINE]: n = 1,067
Weaning Trials were Associated with Low Complication Rates (<0.1%)
Study of the Impact of Weaning Failure on Diaphragmatic Function (Am J Respir Crit Care Med, 2003) [MEDLINE]
Weaning Failure was Not Associated with Low-Frequency Diaphragmatic Fatigue (Which Can Impair Future Weaning Attempts), Although Many Patients Demonstrated Diaphragmatic Weakness
Observational Study of Weaning Outcomes (Eur Respir J, 2010) [MEDLINE]
No Difference in Mortality Between Patients Who Passed Their First Spontaneous Breathing Trial, as Compared to Patients Who Failed Their First Breathing Trial
General Measures to Address for Weaning
Ensure Upright Posture
Upright Posture is Generally Preferred to Advantage the Diaphragm Mechanically (Especially in Patients with Diaphragmatic Paresis/Paralysis)
Optimize Bronchodilation
Clinical Efficacy
Small Study of the Effects of Albuterol on the Work of Breathing During Weaning from Mechanical Ventilation (Am Rev Respir Dis, 1991) [MEDLINE]
Decreased Work of Breathing was More Likely to Occur in Patients with the Largest Bronchodilating Effect of Albuterol at Baseline
Ensure Upper and Lower Airway Secretion Clearance
Clinical Efficacy
However, Suctioning of Lower Airways Should Be Performed in Advance of a Spontaneous Breathing Trial, Since Recent Suctioning Can Increase the RSBI (to >100) for Up to 5 min (Respir Care, 2009) [MEDLINE]
Inspiratory Muscle Training
Unproven Therapy
Clinical Efficacy
Systematic Review of Inspiratory Muscle Training in Mechanically-Ventilated Patients (J Physiother, 2015) [MEDLINE]
Inspiratory Muscle Training for Selected Patients in the ICU Facilitates Ventilator Weaning, with Potential Reductions in Length of Stay and the Duration of Noninvasive Positive-Pressure Ventilation (NIPPV) After Extubation
Weaning Protocols
Rationale
Weaning Protocols were Developed to Expedite the Performance of Daily Spontaneous Breathing Trials (and Avoiding Prolonged Unnecessary Mechanical Ventilation)
Clinical Efficacy
Effect of Daily Sedation Vacation and Spontaneous Breathing Trials (NEJM, 1996) [MEDLINE]
Daily Spontaneous Breathing Trials Decreased the Duration of Mechanical Ventilation, Decreased the Cost of Intensive Care, and Decrease Complication Rates
Randomized, Controlled Trial of Protocol-Drive vs Physician-Directed Weaning (Crit Care Med, 1997) [MEDLINE]
Protocol-Guided Weaning (Performed by Nurses and Respiratory Therapists) is Safe and Led to Extubation More Rapidly than Physician-Directed Weaning
Study of Large-Scale Respiratory Therapist-Driven Weaning Protocol (Am J Respir Crit Care Med, 1999) [MEDLINE]: n = 1,067
Weaning Trials were Associated with Low Complication Rates (<0.1%)
Randomized, Controlled Trial of Weaning Predictors (Crit Care Med, 2006) [MEDLINE]: n = 304
Study Assessed pO2/FIO2 Ratio, PEEP, Hemodynamic Stability, Mental Status, Cough, and RSBI with Randomization to RSBI-Dependent or Independent Weaning
Overall Weaning Success: 59% (similar to other trials)
Including RSBI in a Protocol Prolonged the Weaning Time
RSBI Did Not Confer a Survival Benefit or Decrease the Incidence of Extubation Failure or Tracheostomy
Critique: study used a single RSBI threshold (rather than graded RSBI levels, as many clinicians might use)
Randomized, Controlled Awakening and Breathing Controlled (ABC) Trial (Lancet, 2008) [MEDLINE]: n = 336
Patients were Screened Daily for Adequate Oxygenation (SpO2 >88% on FiO2 <50% and PEEP ≤8 cm H2O), Hemodynamic Stability, and Any Spontaneous Inspiratory Effort During a 5 min Period, Absence of Agitation, Absence of Myocardial Ischemia, and Absence of Increased Intracranial Pressure
Weaning Predictors were Not Measured
Those Passing Screening were Initiated on a Spontaneous Breathing Trial (without Ventilator Assistance)
Over 50% of Patients Initiated on a Spontaneous Breathing Trial Tolerated the Trial
Paired Daily Sedation Vacation and Spontaneous Breathing Trial Decreased the Duration of Mechanical Ventilation, Decreased ICU/Hospital Length of Stay, and Decreased the Mortality Rate
Patients in the Intervention Group Spent More Days Breathing without Ventilatory Assistance During the 28-day Study, as Compared to the Control Group (14.7 days vs 11.6 days; mean difference 3.1 Days, 95% CI 0.7 to 5.6; p=0.02)
Patients in the Intervention Group Had Less ICU Days, as Compared to the Control Group (9.1 Days vs 12.9 Days; p=0.01)
Patients in the Intervention Group Left the Hospital Earlier, as Compared to the Control Group (Median Time in the Hospital 14.9 Days vs 19.2 Days; p=0.04)
More Patients in the Intervention Group Self-Extubated, as Compared to the Control Group (16 Patients vs 6 Patients; 6.0% Difference, 95% CI: 0.6% to 11.8%; p=0.03)
Number of Patients Who Required Reintubation After Self-Extubation was Similar Between the Intervention and Control Groups (5 Patients vs 3 Patients; 1.2% difference, 95% CI: -5.2% to 2.5%; p=0.47
Reintubation Rate was Similar Between the Intervention and Control Groups (13.8% vs 12.5%; 1.3% difference, 95% CI: -8.6% to 6.1%; p=0.73)
At Any Point During the Year after Enrollment, Patients in the Intervention Group were Less Likely to Die than were the Patients in the Control Group (HR 0.68, 95% CI: 0.50 to 0.92; p=0.01)
For Every 7 Patients Treated with the Intervention, 1 Life was Saved (Number Needed to Treat was 7.4 (95% CI: 4.2 to 35.5)
Spontaneous Breathing Trials were Safe and Successful Even in Patients with Poorer Oxygenation (pO2/FIO2 Ratio 110-120)
Prospective Observational Cohort Study of Mechanical Ventilation Practices from 1998 to 2004 (349 ICU’s in 23 Countries) (Am J Respir Crit Care Med, 2008) [MEDLINE]
From 1998 to 2004, More Patients were Extubated After Their First Attempt of Spontaneous Breathing (77 vs 62%, P<0.001), Perhaps Suggesting that Clinicians were More Commonly Performing Daily Spontaneous Breathing Trials (Possibly with Weaning Protocols)
WEAN Study of Automated Weaning (Am J Respir Crit Care Med, 2013) [MEDLINE]: n = 92
As Compared with a Standardized Weaning Protocol, Automated Weaning was Associated with Promising Outcomes
Automated Closed Loop Systems May Result in Decreased Weaning Duration, Decreased Ventilation, and Decreased ICU Length of Stay
Reductions are More Likely to Occur in Mixed or Medical ICU Populations
Cochrane Database Systematic Review of Automated Weaning in Postoperative Adults (Cochrane Database Syst Rev, 2014) [MEDLINE]
Inadequate Evidence
Study of Standardized Weaning Protocols from Mechanical Ventilation in Critically Ill Adults (Cochrane Database Syst Rev, 2014) [MEDLINE]: n = 17 trials
Standardized Weaning Protocols Decrease the Duration of Mechanical Ventilation, Weaning Duration, and ICU Length of Stay
Weaning Protocols Decreased the Duration of Mechanical Ventilation by 26%, as Compared to Usual Care (n = 14 trials, 95% CI: 13% to 37%, P=0.0002)
Reductions were most likely to occur in medical, surgical and mixed ICUs, but not in neurosurgical ICUs
Weaning Protocols Decreased the Duration of Weaning by 70% (n = 8 trials, 95% CI: 27% to 88%, P=0.009)
Weaning Protocols Decreased ICU Length of Stay by 11% (n = 9 trials, 95% CI: 3% to 19%, P=0.01
Cochrane Database Systematic Review of Factors Which Impact the Use of Weaning Protocols in Adults and Children (Cochrane Database Syst Rev, 2016) [MEDLINE]: n = 267 (11 studies)
Factors Related to Weaning Protocol Development and Implementation
Need for Continual Staff Training and Development
Clinical Experience as this Promotes Perceived Competence and Confidence to Wean
Vulnerability of Weaning to Disparate Interprofessional Working
Understanding of Protocols as Militating Against a Necessary Proactivity in Clinical Practice
Perceived Nursing Scope of Practice and Professional Risk
ICU Structure and Processes of Care
Ability of Protocols to Act as a Prompt for Shared Care and Consistency in Weaning Practice
Maximizing the Use of Protocols through Visibility and Ease of Implementation
Ability of Protocols to Act as a Framework for Communication with Parents
Pooled Meta-Analysis of Weaning Protocol Data in Mechanically Ventilated Patients (Am J Respir Crit Care Med, 2017) [MEDLINE]
Ventilator Weaning Protocols Decreased the Duration of Mechanical Ventilation by Approximately 25 hrs (95% CI, 12.5–35.5 Hours)
Ventilator Weaning Protocols Decreased ICU Length of Stay by 0.96 Days (95% CI: 0.24–1.7 Days)
Ventilator Weaning Protocols Did Not Impact the Mortality Rate (22.3 vs 22.2%; Odds Ratio 1.02; 95% CI: 0.82–1.26)
Ventilator Weaning Protocols Did Not Impact the Reintubation Rate (10.6 vs 11.9%; Odds Ratio 0.74; 95% CI: 0.44–1.23)
Weaning Protocols Did Not Impact Adverse Event Rates
In Subgroup Analyses, Personnel-Driven and Computer-Driven Protocols Had Similar Effects, as Compared to Management without a Ventilator Weaning Protocols
International Study of Weaning Practice (Ann Am Thorac Soc, 2018) [MEDLINE]
Most Providers Screened Patients Once Daily to Identify Spontaneous Breathing Trial Candidates (Regional Range, 70.0-95.6%)
Most Providers Used Pressure Support Alone (Range, 31.0-71.7%) or with Spontaneous Breathing Trials (Range, 35.7-68.1%)
To Conduct Spontaneous Breathing Trials, Most Providers Used Pressure Support with Positive End-Expiratory Pressure (Range, 56.5-72.3%) and T-Piece (Range 8.9-59.5%)
Less than 50% of ICU’s Outside of North America Have Written Directives to Conduct Spontaneous Breathing Trials
Recommendations (American Thoracic Society/American College of Chest Physicians Clinical Practice Guideline for Liberation from Mechanical Ventilation in Critically Ill Adults) (Am J Respir Crit Care Med, 2017) [MEDLINE]
Ventilator Weaning Protocols are Recommended for Acutely Ill Hospitalized Adults Who Have Been Mechanically Ventilated for >24 hrs (Conditional Recommendation, Low Certainty of Evidence)
Endotracheal Intubation Can Result in Laryngeal Edema, Especially in Patients Who Have Been Intubated for >36 hrs (Anesthesiology, 1992) [MEDLINE]
Incidence of Postextubation Stridor Has Been Reported to Be Between 6-37% (J Evid Based Med, 2011) [MEDLINE]
Identification of Laryngeal Edema Prior to Extubation is Useful to Decrease the Risk of Reintubation
Since Direct Visualization of the Vocal Cords is Difficult with the Endotracheal Tube in Place, Endotracheal Tube Cuff Leak Testing is Used as a Surrogate Indicator for the Presence of Laryngeal Edema
Technique
General Concept
Endotracheal Tube Cuff Leak (with the Cuff Deflated) Indicates the Presence of Airflow Around the Endotracheal Tube, Suggesting Adequate Space Between the Airway and the Endotracheal Tube
Lack of Leak (i.e. Lack of Space) May Be Suggestive of Laryngeal Edema, Laryngeal Injury, Secretions Laryngeal Stenosis, or a Large Endotracheal Tube within a Small Airway
Types of Leak Tests
Qualitative Endotracheal Tube Cuff Leak Test
Deflation of Endotracheal Tube Cuff with Subsequent Listening for an Air Leak (Either with or without a Stethoscope Over the Trachea)
Quantitative Endotracheal Tube Cuff Leak Test
Deflation of Endotracheal Tube Cuff with Subsequent Measurement of the Amount of Air Leak Via the Ventilator (Difference Between the Inspired and Expired Tidal Volumes During Volume-Cycled Ventilation)
Generally Accepted Threshold for Adequate Air Leak: >110 mL (or >24% of the Delivered Tidal Volume) (Crit Care Med, 2006) [
False-Positive Endotracheal Tube Cuff Leak Test: can occur in cases with late post-extubation upper airway edema
False-Negative Endotracheal Tube Cuff Leak Test: can occur with large ETT with crusted secretions
Clinical Efficacy
Systematic Review and Meta-Analysis of Cuff Leak Testing for the Diagnosis of Airway Obstruction in Adults (Intensive Care Med, 2009) [MEDLINE]
Overall Incidence of Upper Airway Obstruction: 6.9%
A Positive Cuff Leak Test (Absence of Leak) Should Alert the Clinician of a High Risk of Upper Airway Obstruction
Pooled Sensitivity was 0.56 (95% CI: 0.48-0.63), the Specificity was 0.92 (95% CI: 0.90-0.93)
Positive Likelihood Ratio was 5.90 (95% CI: 4.00-8.69) and the Negative Likelihood Ratio was 0.48 (95% CI: 0.33-0.72)
Diagnostic Odds Ratio was 18.78 (95% CI: 7.36-47.92
Area Under the Curve of the Summary Receiver Operator Characteristic (SROC) was 0.92 (95% CI: 0.89-0.94)
Systematic Review of Cuff Leak Testing for Predicting Postextubation Airway Complications (J Evid Based Med, 2011) [MEDLINE]
Cuff Leak Testing Accurately Predicts Which Adult Patients are at High Risk of Postextubation Airway Complications
Median Diagnostic Odds Ratios for Predicting Postextubation Laryngeal Edema and Reintubation were 18.16 (Range: 3.54-356.00) and 10.80 (Range: 2.74-1665.00), Respectively
Accuracy of the Cuff Leak Test Varied with the Methods, Duration of Intubation, and Study Population
Study of Endotracheal Tube Cuff Leak Testing for the Prediction of Postextubation Stridor (J Intensive Care Med, 2019) [MEDLINE]: n = 34
Postextubation Stridor Occurred in <10% of Unselected Critically Ill Patients
Postextubation Stridor Patients More Frequently Required Reintubation (17.6% vs 7.9%, P = .041), Prolonged Duration of Mechanical Ventilation (6 vs 5 Days, P = .029), and Longer ICU Length of Stay (12 vs 7.5 Days, P = .018)
However, ICU Mortality was Similar in Both Groups (2.9% vs 7.0%, P = .61)
Four Endotracheal Tube Cuff Leak Tests Had Poor Diagnostic Accuracy (Sensitivities Ranged from 27-46%, Specificities from 70-88%, Positive Predictive Values from 14-19%, and Negative Predictive Values from 92-93%)
Simulated Study of Cuff Leak Testing (Am J Respir Crit Care Med, 2017) [MEDLINE]
Cuff Leak Test–Guided Management Decreased Both the Reintubation Rate (2.4 vs 4.2%; RR, 0.58; 95% CI: 0.40–0.83) and Postextubation Stridor Rate (4.0 vs 6.7%; RR, 0.60; 95% CI: 0.47–0.77)
Cuff Leak Test–Guided Management Resulted in More Unnecessarily Delayed Extubations (9.2% Absolute Increase)
Cuff Leak Test–Guided Management Had No Effect on the Duration of Mechanical Ventilation
Recommendations (American Thoracic Society/American College of Chest Physicians Clinical Practice Guideline for Liberation from Mechanical Ventilation in Critically Ill Adults) (Am J Respir Crit Care Med, 2017) [MEDLINE]
Cuff Leak Test in Should Be Performed in Mechanically Ventilated Adults Who Meet Extubation Criteria and are Deemed to Be High Risk for Postextubation Stridor (Conditional Recommendation, Very Low Certainty of Evidence)
Criteria for High Risk
Female Sex
Traumatic Intubation
Intubation for >6 Days
Large Endotracheal Tube
Reintubated after an Unplanned Extubation
For Adults Who Have Failed a Cuff Leak Test But are Otherwise Ready for Extubation, Administering Systemic Steroids for >4 hrs Before Extubation is Recommended (Conditional Recommendation, Moderate Certainty of Evidence)
Weaning Modalities
Modalities
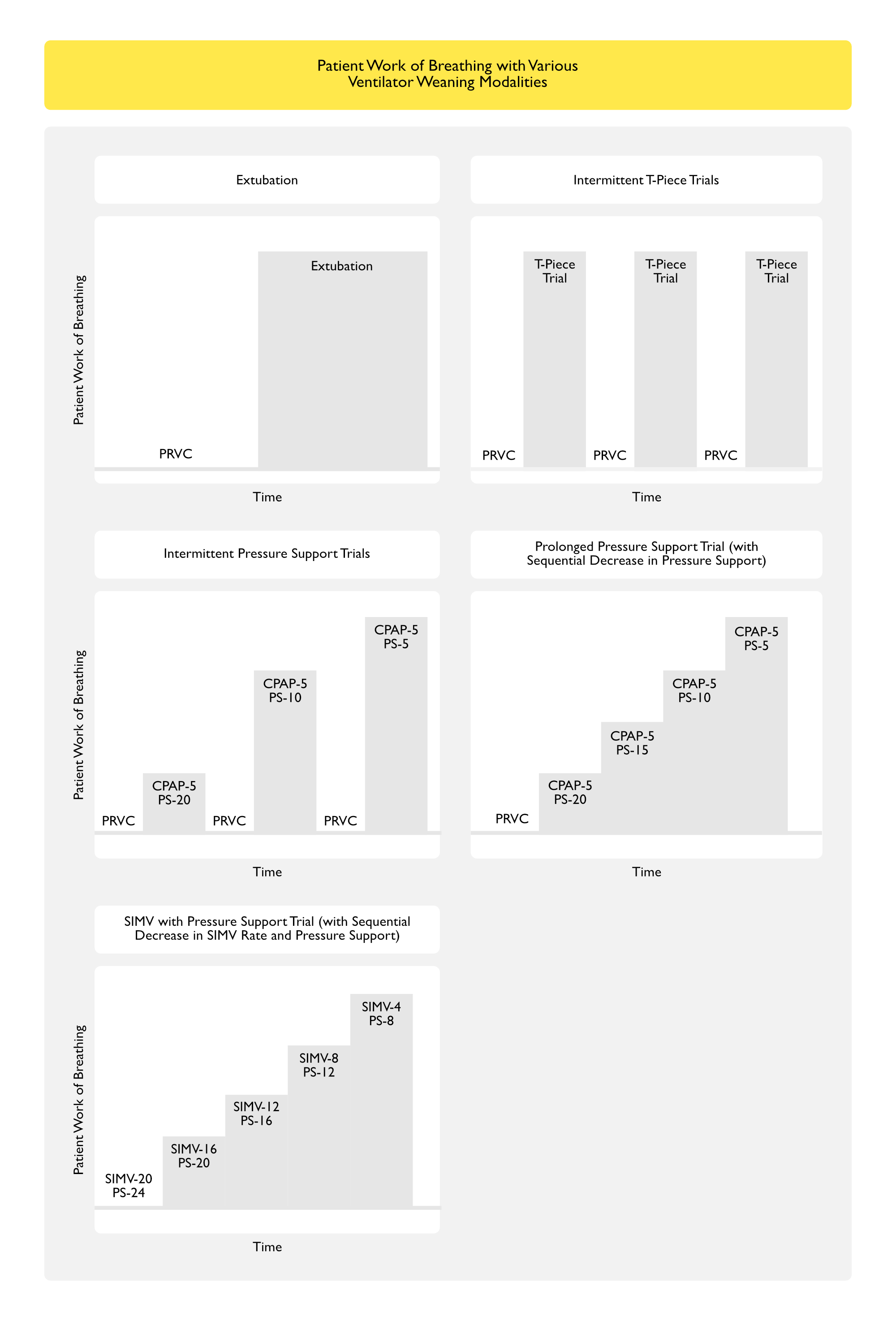
Extubation
Although Not Really Considered a Modality of Ventilator “Weaning” Per Se, Extubation (Liberation from the Ventilator) Transfers All of the Work of Breathing from the Ventilator to the Patient
Advantages
Simple and Useful for a Patient with Minimal Cardiopulmonary Disease (Especially in the Postoperative Setting When the Effects of General Anesthesia Have Resolved)
Disadvantages
Abruptly Transfers the Work of Breathing (and Requirement to Maintain a Patent Airway and Secretion Clearance) to the Patient
If the Patient is Unable to Tolerate this Increase in Work of Breathing, Extubation Failure Can Occur Precipitously
Pressure Support (PS) Weaning
Generally, Pressure Support Ventilation is Considered the Preferred Method of Ventilator Weaning (Chest, 2017) [MEDLINE]
Advantages
Allows Either Intermittent or Continuous Trials with the Pressure Support Level Adjusted According to the Patient’s Need
Gradual Increase in Work of Breathing May Be Useful in Patients with Unstable Coronary Artery Disease or Other Underlying Cardiopulmonary Limitations
Presence of Ventilator Alarms to Alert Provider to High Respiratory Rate and/or Low Tidal Volume
Easily Used in Respiratory Therapist-Driven Weaning Protocols
Disadvantages
An Inappropriately Low Level of Set Pressure Support Can Result in Respiratory Muscle Fatigue (Manifested by Low Spontaneous Tidal Volumes and Tachypnea), Recurrent Weaning Failure, and Patient Distress
This is Especially True in the Case of a Small Diameter Endotracheal Tube (≤7 mm), Which Generally Requires a Pressure Support of 7-10 cm H20 to Overcome the Resistance of the Endotracheal Tube Alone
Automatic Tube Compensation (ATC)
Available on Draeger Ventilators, ATC Compensates for the Endotracheal Tube Resistance
CPAP Weaning
Less Commonly Used in Modern Weaning Protocols
Advantages
Simple Method to Determine Readiness for Extubation
Presence of Ventilator Alarms to Alert Provider to High Respiratory Rate and/or Low Tidal Volume
T-Piece Weaning
Advantage
Simple Method (with Longstanding Clinical Experience) to Determine Readiness for Extubation
Disadvantages
Intermittent T-Piece Trials Provide No Ventilatory Support to the Patient (Patient Assumes Full Work of Breathing Plus the Resistance of the Endotracheal Tube During the Trial)
Inability to Maintain the Work of Breathing Required During the Trial Can Result in Abrupt (or Recurrent) Weaning Failure
T-Piece Trials are Not Indicated for Patients with Small Endotracheal Tubes (≤7 mm), Due to the Increased Endotracheal Tube Resistance
Lack of Ventilator Alarms to Alert Provider to High Respiratory Rate and/or Low Tidal Volume
Synchronized Intermittent Mandatory Ventilation (SIMV) with Pressure Support Weaning
Less Commonly Used in Modern Weaning Protocols
Advantages
Presence of Ventilator Alarms to Alert Provider to High Respiratory Rate and/or Low Tidal Volume
Disadvantages
Adjustment of Both the SIMV Backup Rate and Pressure Support Level Can Be Complicated and Vary Between Providers
Patient Work of Breathing with Various Ventilator Weaning Modes
Clinical Efficacy-Ventilator Weaning Modality
Study of T-Piece vs CPAP (5 cm H2O) for Weaning (Chest, 1991) [MEDLINE]
No Difference in Reintubation Rate
Comparative Trial of T-Piece, Intermittent Mandatory Ventilation (IMV) and Pressure Support (PS) Ventilator Weaning (Am J Respir Crit Care Med, 1994) [MEDLINE]: n = 109 patients who failed an initial spontaneous breathing trial
After Failing an Initial Spontaneous Breathing Trial, Patients were Randomized to Groups
After Excluding Patients Whose Weaning was Terminated for Complications Unrelated to the Weaning Process, Pressure Support Weaning Failure was Lowest (8%), as Compared to T-Piece and SIMV Weaning (p<0.025)
Spanish Randomized Trial of T-Piece (Once Daily or Two-Three Times Daily), Synchronized Intermittent Mandatory Ventilation (SIMV) and Pressure Support (PS) Ventilator Weaning (NEJM, 1995) [MEDLINE]: n = 130 patients who failed an initial spontaneous breathing trial
After Failing an Initial Spontaneous Breathing Trial, Patients were Randomized to Groups
Once Daily Spontaneous Breathing Trials with T-Piece
Multiple (2-3) Times Daily Spontaneous Breathing Trials with T-Piece
Once Daily Trial of Spontaneous Breathing with T-Piece Led to Extubation 3x More Quickly than Intermittent Mandatory Ventilation Weaning and Twice as Quickly as Pressure Support Weaning
Multiple (2-3) Daily Spontaneous Breathing Trials with T-Piece and Daily Spontaneous Breathing Trials with T-Piece were Equally Effective
Trial of T-Piece vs Pressure Support Ventilation Weaning (Am J Respir Crit Care Med, 1997) [MEDLINE]
No Difference Between Spontaneous Breathing Trials with Pressure Support Ventilation or T-Piece
Study of the Contribution of the Endotracheal Tube to Breathing Workload (Am J Respir Crit Care Med, 1998) [MEDLINE]
Work of Breathing was the Same Through a T-Piece and Following Extubation
Study of Automatic Tube Compensation, Pressure Support Ventilation, and T-Piece for Weaning (Acta Anaesthesiol Scand, 2002) [MEDLINE]
No Difference Between the Weaning Modes
Randomized Crossover Trial of Work of Breathing with Weaning Modes (Crit Care Med, 2000) [MEDLINE]
No Differences in the Work of Breathing During Spontaneous Breathing Trials Using a T-Piece, Low Level Pressure Support, or CPAP
In Fact, the Work of Breathing was Higher After Removal of the Endotracheal Tube than with Any of the Spontaneous Breathing Trial Methods: suggests that the endotracheal tube contribution to work of breathing is relatively small, in comparison to work of breathing with airway (which is possibly edematous) after extubation
Randomized, Prospective Trial of T-Piece vs Pressure Support Weaning (Croat Med J, 2004) [MEDLINE]
In Patients with Weaning Difficulties, Pressure Support Ventilation with 8 cm H2O was a More Successful Weaning Method than T-Piece
Study of Automatic Tube Compensation vs CPAP for Weaning (Crit Care Med, 2006) [MEDLINE]
No Difference in the Rate of Reintubation
Study of Crossover to Pressure Support Weaning in Patients Failing T-Piece Weaning (Intensive Care Med, 2006) [MEDLINE]
In Patients Failing a 30 min T-Piece Trial, Conversion to Pressure Support Ventilation (at 7 cm H2O) For an Additional 30 min Resulted in Weaning Success in 68% of Patients
Data Suggest that Endotracheal Tube Resistance May Contribute to Weaning Failure
Randomized, Controlled Trial of Automatic Tube Compensation vs Pressure Support Ventilation for Weaning (Crit Care, 2009) [MEDLINE]
No Difference in the Rate of Reintubation
Cochrane Database Systematic Review of Pressure support vs T-Piece for Ventilator Weaning in Adults (Cochrane Database Syst Rev, 2014) [MEDLINE]
Low Quality Data from Existing Studies
However, Pressure Support Ventilation was More Effective than T-Piece for Successful Spontaneous Breathing Trials Among Patients with Simple Weaning
Based on the Findings of Single Trials, Three Studies Presented a Shorter Weaning Duration in the Group undergoing Pressure Support Spontaneous Breathing Trials, However a Fourth Study Found a Shorter Weaning Duration with a T-Piece
Chinese Comparative Study of Pressure Support Ventilation vs T-Piece to Determine the Threshold RSBI During Spontaneous Breathing Trials (Am J Med Sci, 2014) [MEDLINE]: n = 208
The Threshold values of RSBI (75 for Pressure Support Ventilation and 100 for T-Piece) were the Most Accurate for Predicting Successful Weaning
Methods Had Comparable Weaning Success Rates (Pressure Support Ventilation: 83.9%, T-Piece: 78.3%)
Systematic Review and Meta-Analysis of Weaning Modalities with Pressure Augmentation (Pressure Support with 5-8 cm H2O or Automatic Tube Compensation) or without Pressure Augmentation (T-Piece or CPAP) (Chest, 2017) [MEDLINE]: n = 4 trials
Conducting the Spontaneous Breathing Trial with Pressure Augmentation (Pressure Support) was More Likely to Be Successful (84.6% vs 76.7%; RR, 1.11; 95% CI: 1.02-1.18), Produced a Higher Rate of Extubation Success (75.4% vs 68.9%; RR, 1.09; 95% CI: 1.02-1.18), and was Associated with a Trend Toward Lower ICU Mortality Rate (8.6% vs 11.6%; RR, 0.74; 95% CI: 0.45-1.24)
French Multicenter, Open-Label TIP-EX Trial Comparing Pressure-Support Ventilation (CPAP 0 cm H2O and PS 8 cm H2O) or T-Piece for Spontaneous Breathing Trials in Patients at High-Risk for Extubation Failure (>65 y/o or with Chronic Cardiopulmonary Disease) (NEJM, 2022) [MEDLINE]: n = 969
At Day 28, There were No Differences in Ventilator-Free Days Between the PS Group (Median 27; Interquartile Range: 24-27) and the T-Piece Group 27 (Interquartile Range: 23-27) (Difference: 0 days; 95% CI: -0.5 to 1; P = 0.31)
Extubation was Performed within 24 hrs in 77.7% of Patients in the PS Group and in 72.2% of Patients in the T-Piece Group (Difference: 5.5 Percentage Points; 95% CI: 0.01 to 10.9)
Extubation was Performed within 7 Days in 97.7% of Patients in the PS Group and 94.4% of Patients in the T-Piece Group (Difference: 3.3 Percentage Points; 95% CI: 0.8 to 5.9)
Reintubation was Performed in 14.9% of Patients in the PS Group and 13.6% of Patients in the T-Piece Group (Difference 1.3 Percentage Points; 95% CI: -3.1 to 5.8)
Cardiac or Respiratory Arrest was a Reason for Reintubation in 9 Patients (3 in the PS Group and 6 in the T-piece Group)
Recommendations (American College of Chest Physicians/American Thoracic Society Clinical Practice Guideline for Liberation from Mechanical Ventilation in Critically Ill Adults) (Chest, 2017) [MEDLINE]
Weaning Modality
For Acutely Hospitalized Patients Ventilated >24 hrs, Initial Spontaneous Breathing Trial Should Be Conducted with Inspiratory Pressure Augmentation (Pressure Support Ventilation of 5-8 cm H2O), Rather than with T-piece or CPAP (Conditional Recommendation, Moderate-Quality Evidence)
Duration of Weaning Trials
Background
Weaning Trials are Typically 30-120 min in Length
Trials of 30 min are Generally Adequate to Determine Patient Tolerance, Although Longer Trials Can Be Used in Some Cases to Assess Patient Endurance
Weaning Trials Should Be Terminated at the First Signs of Failure: prolonged weaning trials should be avoided to avoid fatigue, which may impair performance during future weaning trials
Clinical Efficacy
Multicenter Study of Weaning Trial Length (Am J Respir Crit Care Med, 1999) [MEDLINE]
T-Piece Weaning Trials of 30 or 120 min were Comparable in Terms of Rate of Weaning Failure and Reintubation
Prospective, Multicenter, Randomized Trial of Spontaneous Breathing vs Pressure Support in COPD Patients Requiring Ventilation >15 Days and Failing T-Piece Trials (Am J Respir Crit Care Med, 2001) [MEDLINE]
No Significant Difference were Found in Weaning Success Rate (73% vs 77% in the Pressure Support and Spontaneous Breathing Group, Respectively), Mortality Rate (11.5% vs 7.6%), Duration of Ventilatory Assistance (181 +/- 161 vs 130 +/- 106 h), Duration of Long-Term Weaning Units (33 +/- 12 vs 35 +/- 19 d), or Total Hospital Stay
Median Time to Spontaneous Breathing Trial Failure was 120 min
Multicenter, Cohort Study of Central Venous Saturation in Difficult to Wean Patients (Crit Care Med, 2010) [MEDLINE]
Central Venous Saturation was an Early and Independent Predictor of Extubation Failure in Difficult to Wean Patients
Rest After Weaning Trial
Rationale
Rest Between Weaning Trials is Critical to Facilitate Patient Recovery and Avoid Fatigue
Patients are Standardly Returned to Their Prior Ventilator Settings (Which Presumably Supplies a High Level of Ventilatory Support)
Rest After a Successful Weaning Trial, Prior to Extubation is Also Recommended: see the following section
Clinical Efficacy
Spanish Randomized Multicenter Trial of Reconnection to the Ventilator for 1 Hour of Rest After a Successful Spontaneous Breathing Trial, Prior to Extubation (Intensive Care Med, 2017) [MEDLINE]: n = 470
One Hours Rest (on the Ventilator) After a Successful Spontaneous Breathing Trial Decreased the 48-hr Reintubation Rate (5%), as Compared to the Control Group (14%)
Multivariable Regression Model Demonstrated that the Variables Independently Associated with Reintubation Rate were Rest [Odds Ratio 0.34 (95%CI: 0.17-0.68)], APACHE II [Odds Ratio 1.04 (95% CI: 1.002-1.077)], and Days of Mechanical Ventilation Before Spontaneous Breathing Trial [Odds Ratio 1.04 (95% CI: 1.001-1.073)]
Age, Reason for Admission, and Type and Duration of Spontaneous Breathing Trial were Not Associated with Reintubation Rate
Weaning Success
Prediction of Weaning Success
Clinical Efficacy
Diaphragmatic Atrophy Can Be Identified by Diaphragmatic Ultrasound (Thorax, 2014)[MEDLINE]
Diaphragmatic Thickening Can Predict Weaning Success
Diaphragmatic Atrophy (Due to Abnormally Low Inspiratory Effort) Which Develops During Mechanical Ventilation (As Assessed by Diaphragmatic Ultrasound) Decreased the Probability of Liberation from Mechanical Ventilation (Adjusted Hazard Ratio, 0.69; 95% CI: 0.54-0.87; Per 10% Decrease), Prolonged ICU Length of Stay (Adjusted Duration Ratio, 1.71; 95% CI: 1.29-2.27), and Increased the Risk of Complications (Adjusted Odds Ratio, 3.00; 95% CI: 1.34-6.72) (Am J Respir Crit Care Med, 2018) [MEDLINE]
Increased Diaphragmatic Thickness (Due to Excessive Inspiratory Effort) Also Predicted Prolonged Mechanical Ventilation (Adjusted Duration Ratio, 1.38; 95% CI: 1.00-1.90)
Patients with Thickening Fraction 15-30% (Similar to Breathing at Rest) During the First 3 Days Had the Shortest Duration of Mechanical Ventilation
Reduction of duration and cost of mechanical ventilation in an intensive care unit by use of a ventilator management team. Crit Care Med 1991; 19:1278-1284
Effect of failed extubation on the outcome of mechanical ventilation. Chest. 1997;112(1):186 [MEDLINE]
Liberation from mechanical ventilation: a decade of progress. Chest 1998; 114:886-901
Noninvasive mechanical ventilation in the weaning of patients with respiratory failure due to chronic obstructive pulmonary disease: a randomized, controlled trial. Ann Intern Med 1998; 128:721-728
The prognostic significance of passing a daily screen of weaning parameters. Intensive Care Med. 1999;25(6):581 [MEDLINE]
Criteria for weaning from mechanical ventilation. Evid Rep Technol Assess (Summ). 2000 [MEDLINE]
Introduction to systematic reviews of weaning from mechanical ventilation. Chest 2001; 120(suppl):396S-399S
Systematic reviews of the evidence base for ventilator weaning. Chest 2001; 120(suppl):396S-482S
Trials of miscellaneous interventions to wean from mechanical ventilation. Chest 2001; 120(suppl):438S-444S
Trials comparing alternative weaning modes and discontinuation assessments. Chest 2001; 120(suppl):425S-437S
Evidence-based guidelines for weaning and discontinuing ventilatory support: a collective task force facilitated by the American College of Chest Physicians; the American Association for Respiratory Care; and the American College of Critical Care Medicine. Chest. 2001;120(6 Suppl):375S [MEDLINE]
Weaning patients from the ventilator. N Engl J Med. 2012 Dec 6;367(23):2233-9. doi: 10.1056/NEJMra1203367 [MEDLINE]
Official Executive Summary of an American Thoracic Society/American College of Chest Physicians Clinical Practice Guideline: Liberation from Mechanical Ventilation in Critically Ill Adults. Am J Respir Crit Care Med. 2017 Jan 1;195(1):115-119. doi: 10.1164/rccm.201610-2076ST [MEDLINE]
An Official American Thoracic Society/American College of Chest Physicians Clinical Practice Guideline: Liberation from Mechanical Ventilation in Critically Ill Adults. Rehabilitation Protocols, Ventilator Liberation Protocols, and Cuff Leak Tests. Am J Respir Crit Care Med. 2017 Jan 1;195(1):120-133. doi: 10.1164/rccm.201610-2075ST [MEDLINE]
Liberation From Mechanical Ventilation in Critically Ill Adults: Executive Summary of an Official American College of Chest Physicians/American Thoracic Society Clinical Practice Guideline. Chest. 2017 Jan;151(1):160-165. doi: 10.1016/j.chest.2016.10.037 [MEDLINE]
An Official American Thoracic Society/American College of Chest Physicians Clinical Practice Guideline: Liberation from Mechanical Ventilation in Critically Ill Adults. Chest. 2017 Jan;151(1):166-180. doi: 10.1016/j.chest.2016.10.036 [MEDLINE]
International Practice Variation in Weaning Critically Ill Adults from Invasive Mechanical Ventilation. Ann Am Thorac Soc. 2018;15(4):494 [MEDLINE]
Prediction of Patient Undergoing a Spontaneous Awakening Trial/Spontaneous Breathing Trial
Factors Associated With Spontaneous Awakening Trial and Spontaneous Breathing Trial Performance in Adults With Critical Illness: Analysis of a Multicenter, Nationwide, Cohort Study. Chest. 2022 Sep;162(3):588-602. doi: 10.1016/j.chest.2022.01.018 [MEDLINE]
Weaning Parameters
Anemia
Do blood transfusions improve outcomes related to mechanical ventilation? Chest. 2001;119(6):1850 [MEDLINE]
Hemoglobin levels and weaning outcome of mechanical ventilation in difficult-to-wean patients: a retrospective cohort study. PLoS One. 2013;8(8):e73743 [MEDLINE]
Cough
A randomized, controlled trial of the role of weaning predictors in clinical decision making. Crit Care Med. 2006;34(10):2530 [MEDLINE]
Utilization of spontaneous breathing trial, objective cough test, and diaphragmatic ultrasound results to predict extubation success: COBRE-US trial. Crit Care. 2023 Oct 31;27(1):414. doi: 10.1186/s13054-023-04708-y [MEDLINE]
Fever
The effect of sepsis on breathing pattern and weaning outcomes in patients recovering from respiratory failure. Chest. 1997;112(2):472 [MEDLINE]
Fever is associated with delayed ventilator liberation in acute lung injury. Ann Am Thorac Soc. 2013;10(6):608 [MEDLINE]
Hemodynamic Stability
A randomized, controlled trial of the role of weaning predictors in clinical decision making. Crit Care Med. 2006;34(10):2530 [MEDLINE]
Mental Status
Implications of extubation delay in brain-injured patients meeting standard weaning criteria. Am J Respir Crit Care Med. 2000;161(5):1530 [MEDLINE]
Predictors of successful extubation in neurosurgical patients. Am J Respir Crit Care Med. 2001;163(3 Pt 1):658 [MEDLINE]
Neurologic status, cough, secretions and extubation outcomes. Intensive Care Med. 2004;30(7):1334 [MEDLINE]
Interest of an objective evaluation of cough during weaning from mechanical ventilation. Intensive Care Med. 2009;35(6):1090 [MEDLINE]
Measures of Oxygenation (as Measured by pO2/FIO2 Ratio, etc)
Evaluation of conventional criteria for predicting successful weaning from mechanical ventilatory support in elderly patients. Crit Care Med. 1989;17(9):858 [MEDLINE]
Efficacy and safety of a paired sedation and ventilator weaning protocol for mechanically ventilated patients in intensive care (Awakening and Breathing Controlled trial): a randomised controlled trial. Lancet. 2008 Jan 12;371(9607):126-34 [MEDLINE]
Minute Ventilation
Predicting success in weaning from mechanical ventilation. Chest. 2001;120(6 Suppl):400S [MEDLINE]
Compliance (Lung and Chest Wall)
A prospective study of indexes predicting the outcome of trials of weaning from mechanical ventilation. N Engl J Med. 1991;324(21):1445 [MEDLINE]
A new integrative weaning index of discontinuation from mechanical ventilation. Crit Care. 2009;13(5):R152 [MEDLINE]
Work of Breathing
Comparison of standard weaning parameters and the mechanical work of breathing in mechanically ventilated patients. Chest. 1988;94(2):232 [MEDLINE]
Work of breathing as a weaning parameter in mechanically ventilated patients. Chest. 1995;108(4):1018 [MEDLINE]
Pathophysiologic basis of acute respiratory distress in patients who fail a trial of weaning from mechanical ventilation. Am J Respir Crit Care Med. 1997;155(3):906 [MEDLINE]
The tension-time index and the frequency/tidal volume ratio are the major pathophysiologic determinants of weaning failure and success. Am J Respir Crit Care Med. 1998;158(2):378 [MEDLINE]
The combination of the load/force balance and the frequency/tidal volume can predict weaning outcome. Intensive Care Med. 2006;32(5):684 [MEDLINE]
Oxygen Cost of Breathing
The oxygen cost of breathing in patients with cardiorespiratory disease. Am Rev Respir Dis. 1982;126(1):9 [MEDLINE]
Metabolic and respiratory changes during weaning from mechanical ventilation. Chest. 1987;92(6):979 [MEDLINE]
Oxygen uptake during weaning from mechanical ventilation. Chest. 1988;94(6):1148 [MEDLINE]
Airway Occlusion Pressure
Airway occlusion pressure. An important indicator for successful weaning in patients with chronic obstructive pulmonary disease. Am Rev Respir Dis. 1987;135(1):107 [MEDLINE]
Prediction of successful ventilator weaning using airway occlusion pressure and hypercapnic challenge. Chest. 1987;91(4):496 [MEDLINE]
Airway occlusion pressure and breathing pattern as predictors of weaning outcome. Am Rev Respir Dis. 1993;148(4 Pt 1):860 [MEDLINE]
A prospective, blinded evaluation of indexes proposed to predict weaning from mechanical ventilation. Intensive Care Med. 2004;30(5):830 [MEDLINE]
Evaluation of maximal inspiratory pressure, tracheal airway occlusion pressure, and its ratio in the weaning outcome. J Crit Care. 2009;24(3):441 [MEDLINE]
Maximal Inspiratory Pressure (MIP, PImax, or Pimax)
Bedside criteria for discontinuation of mechanical ventilation. Chest. 1973;63(6):1002 [MEDLINE]
Maximal inspiratory pressure is not a reliable test of inspiratory muscle strength in mechanically ventilated patients. Am Rev Respir Dis. 1990;142(3):529 [MEDLINE]
Predicting success in weaning from mechanical ventilation. Chest. 2001;120(6 Suppl):400S [MEDLINE]
Evaluation of a new index of mechanical ventilation weaning: the timed inspiratory effort. J Intensive Care Med. 2015;30(1):37 [MEDLINE]
Gastric Mucosal Acidosis
Gastric intramural pH as a predictor of success or failure in weaning patients from mechanical ventilation. Ann Intern Med. 1993;119(8):794 [MEDLINE]
Gastric intramucosal pH and intraluminal PCO2 during weaning from mechanical ventilation. Crit Care Med. 2001;29(1):70 [MEDLINE]
Diaphragmatic Ultrasound
Diaphragm dysfunction assessed by ultrasonography: influence on weaning from mechanical ventilation. Crit Care Med. 2011;39(12):2627 [MEDLINE]
Diaphragm ultrasound as a predictor of successful extubation from mechanical ventilation. Thorax. 2014 May;69(5):423-7 [MEDLINE]
Diaphragm and Lung Ultrasound to Predict Weaning Outcome: Systematic Review and Meta-Analysis. Chest. 2017;152(6):1140 [MEDLINE]
Use of diaphragm thickening fraction combined with rapid shallow breathing index for predicting success of weaning from mechanical ventilator in medical patients. J Intensive Care. 2018;6:6 [MEDLINE]
Utilization of spontaneous breathing trial, objective cough test, and diaphragmatic ultrasound results to predict extubation success: COBRE-US trial. Crit Care. 2023 Oct 31;27(1):414. doi: 10.1186/s13054-023-04708-y [MEDLINE]
Rapid Shallow Breathing Index (RSBI)
A prospective study of indexes predicting the outcome of trials of weaning from mechanical ventilation. N Engl J Med. 1991;324(21):1445 [MEDLINE]
Influence of gender and endotracheal tube size on preextubation breathing pattern. Am J Respir Crit Care Med. 1996;154(6 Pt 1):1647 [MEDLINE]
Physiologic determinants of ventilator dependence in long-term mechanically ventilated patients. Am J Respir Crit Care Med. 2000;161(4 Pt 1):1115 [MEDLINE]
Variable performance of weaning-predictor tests: role of Bayes’ theorem and spectrum and test-referral bias. Intensive Care Med. 2006;32(12):2002 [MEDLINE]
A randomized, controlled trial of the role of weaning predictors in clinical decision making. Crit Care Med. 2006;34(10):2530 [MEDLINE]
Effect of pressure support ventilation and positive end expiratory pressure on the rapid shallow breathing index in intensive care unit patients. Intensive Care Med. 2008;34(3):505 [MEDLINE]
Variation in the rapid shallow breathing index associated with common measurement techniques and conditions. Respir Care. 2009;54(11):1462 [MEDLINE]
Physiologic impact of closed-system endotracheal suctioning in spontaneously breathing patients receiving mechanical ventilation. Respir Care. 2009;54(3):367 [MEDLINE]
Comparison of 3 different methods used to measure the rapid shallow breathing index. J Crit Care. 2012 Aug;27(4):418.e1-6 [MEDLINE]
The effect of flow trigger on rapid shallow breathing index measured through the ventilator. J Intensive Care Med. 2015;30(2):103 [MEDLINE]
Evaluation of a new index of mechanical ventilation weaning: the timed inspiratory effort. J Intensive Care Med. 2015;30(1):37 [MEDLINE]
Use of diaphragm thickening fraction combined with rapid shallow breathing index for predicting success of weaning from mechanical ventilator in medical patients. J Intensive Care. 2018;6:6 [MEDLINE]
Inspiratory Effort Quotient (IEQ)
Is weaning an art or a science? Am Rev Respir Dis. 1986;134(6):1107 [MEDLINE]
CROP Index (Compliance, Rate, Oxygenation, Pressure)
A prospective study of indexes predicting the outcome of trials of weaning from mechanical ventilation. N Engl J Med. 1991;324(21):1445 [MEDLINE]
CORE Index (Compliance, Oxygenation, Respiration, Effort)
Preliminary evaluation of a new index to predict the outcome of a spontaneous breathing trial. Respir Care. 2011 Oct;56(10):1500-5 [MEDLINE]
Weaning Index (WI)
Evaluation of a new weaning index based on ventilatory endurance and the efficiency of gas exchange. Am Rev Respir Dis. 1991;144(3 Pt 1):531 [MEDLINE]
Integrative Weaning Index (IWI)
A new integrative weaning index of discontinuation from mechanical ventilation. Crit Care. 2009;13(5):R152 [MEDLINE]
Evaluation of a new index of mechanical ventilation weaning: the timed inspiratory effort. J Intensive Care Med. 2015;30(1):37 [MEDLINE]
Technique
General
Ventilator Weaning and Extubation. Crit Care Clin. 2024 Apr;40(2):391-408. doi: 10.1016/j.ccc.2024.01.007 [MEDLINE]
Prolonged Mechanical Ventilation, Weaning, and the Role of Tracheostomy. Crit Care Clin. 2024 Apr;40(2):409-427. doi: 10.1016/j.ccc.2024.01.008 [MEDLINE]
Rapid disuse atrophy of diaphragm fibers in mechanically ventilated humans. N Engl J Med 2008; 358(13):1327-1335 [MEDLINE]
Estimation of inspiratory muscle pressure in critically ill patients. Intensive Care Med 2010; 36(4):648-655 [MEDLINE]
Ventilator-induced diaphragmatic dysfunction. Curr Opin Crit Care 2010; 16(1):19-25 [MEDLINE]
Early mobilization in the intensive care unit: a systematic review. Cardiopulm Phys Ther J 2012;23:5–13 [MEDLINE]
Diaphragm weakness in mechanically ventilated critically ill patients. Crit Care 2013;17:R120 [MEDLINE]
Acute skeletal muscle wasting in critical illness. JAMA 2013;310:1591–1600 [MEDLINE]
Physiotherapy in intensive care: an updated systematic review. Chest 2013;144:825–847 [MEDLINE]
Interventions to improve the physical function of ICU survivors: a systematic review. Chest 2013;144:1469–1480 [MEDLINE]
Acute outcomes and 1-year mortality of intensive care unit-acquired weakness: a cohort study and propensity-matched analysis. Am J Respir Crit Care Med 2014;190: 410–420 [MEDLINE]
An environmental scan for early mobilization practices in U.S. ICUs. Crit Care Med 2015;43:2360–2369 [MEDLINE]
An Official American Thoracic Society/American College of Chest Physicians Clinical Practice Guideline: Liberation from Mechanical Ventilation in Critically Ill Adults. Rehabilitation Protocols, Ventilator Liberation Protocols, and Cuff Leak Tests. Am J Respir Crit Care Med 2017 [MEDLINE]
Safety of Weaning
Large scale implementation of a respiratory therapist-driven protocol for ventilator weaning. Am J Respir Crit Care Med. 1999;159(2):439 [MEDLINE]
Is weaning failure caused by low-frequency fatigue of the diaphragm? Am J Respir Crit Care Med. 2003;167(2):120 [MEDLINE]
Incidence and outcome of weaning from mechanical ventilation according to new categories. Eur Respir J. 2010;35(1):88 [MEDLINE]
General Measures During Weaning
Effects of albuterol inhalation on the work of breathing during weaning from mechanical ventilation. Am Rev Respir Dis. 1991;144(1):95 [MEDLINE]
Inspiratory Muscle Training
Inspiratory muscle training facilitates weaning from mechanical ventilation among patients in the intensive care unit: a systematic review. J Physiother. 2015;61(3):125 [MEDLINE]
Weaning Protocols
Effect on the duration of mechanical ventilation of identifying patients capable of breathing spontaneously. N Engl J Med 1996; 335:1864-1869 [MEDLINE]
A randomized, controlled trial of protocol-directed versus physician-directed weaning from mechanical ventilation. Crit Care Med. 1997 Apr;25(4):567-74 [MEDLINE]
Large scale implementation of a respiratory therapist-driven protocol for ventilator weaning. Am J Respir Crit Care Med. 1999;159(2):439 [MEDLINE]
A randomized, controlled trial of the role of weaning predictors in clinical decision making. Crit Care Med. 2006;34(10):2530 [MEDLINE]
Efficacy and safety of a paired sedation and ventilator weaning protocol for mechanically ventilated patients in intensive care (Awakening and Breathing Controlled trial): a randomised controlled trial. Lancet. 2008 Jan 12;371(9607):126-34 [MEDLINE]
Evolution of mechanical ventilation in response to clinical research. Am J Respir Crit Care Med. 2008;177(2):170 [MEDLINE]
Automating the weaning process with advanced closed-loop systems. Intensive Care Med. 2008 Oct;34(10):1757-65 [MEDLINE]
Wean earlier and automatically with new technology (the WEAN study). A multicenter, pilot randomized controlled trial. Am J Respir Crit Care Med. 2013;187(11):1203 [MEDLINE]
Automated versus non-automated weaning for reducing the duration of mechanical ventilation for critically ill adults and children. Cochrane Database Syst Rev. 2013 Jun 6;(6):CD009235. doi: 10.1002/14651858.CD009235.pub2 [MEDLINE]
Protocolized versus non-protocolized weaning for reducing the duration of mechanical ventilation in critically ill adult patients. Cochrane Database Syst Rev. 2014 Nov 6;11:CD006904. doi: 10.1002/14651858.CD006904.pub3 [MEDLINE]
Automated weaning and spontaneous breathing trial systems versus non-automated weaning strategies for discontinuation time in invasively ventilated postoperative adults. Cochrane Database Syst Rev. 2014 Feb 13;(2):CD008639. doi: 10.1002/14651858.CD008639.pub2 [MEDLINE]
Factors that impact on the use of mechanical ventilation weaning protocols in critically ill adults and children: a qualitative evidence-synthesis. Cochrane Database Syst Rev. 2016 Oct 4;10:CD011812 [MEDLINE]
Endotracheal Tube Cuff Leak Testing
Evaluation of risk factors for laryngeal edema after tracheal extubation in adults and its prevention by dexamethasone: a placebo-controlled, double-blind, multicenter study. Anesthesiology 1992;77:245–251 [MEDLINE]
Association between reduced cuff leak volume and postextubation stridor. Chest. 1996;110(4):1035 [MEDLINE]
Trials of corticosteroids to prevent post-extubation airway complications. Chest. 2001 Dec;120(6 Suppl):464S-8S [MEDLINE]
The cuff leak test to predict failure of tracheal extubation for laryngeal edema. Intensive Care Med. 2002;28(9):1267 [MEDLINE]
Post-extubation stridor in intensive care unit patients. Risk factors evaluation and importance of the cuff-leak test. Intensive Care Med. 2003;29(1):69 [MEDLINE]
How to identify patients with no risk for postextubation stridor? J Crit Care. 2004;19(1):23 [MEDLINE]
The endotracheal tube cuff-leak test as a predictor for postextubation stridor. Respir Care. 2005;50(12):1632 [MEDLINE]
Risk factors evaluation and the cuff leak test as predictors for postextubation stridor. J Med Assoc Thai. 2008;91(5):648 [MEDLINE]
Cuff-leak test for the diagnosis of upper airway obstruction in adults: a systematic review and meta-analysis. Intensive Care Med 2009;35:1171–1179 [MEDLINE]
Cuff-leak test for predicting postextubation airway complications: a systematic review. J Evid Based Med 2011;4:242–254 [MEDLINE]
Cuff Leak Test for the Diagnosis of Post-Extubation Stridor. J Intensive Care Med. 2019 May;34(5):391-396. doi: 10.1177/0885066617700095 [MEDLINE]
Weaning Modalities
Patient and ventilator work of breathing and ventilatory muscle loads at different levels of pressure support ventilation. Chest 1991; 100:531-533 [MEDLINE]
Positive end-expiratory pressure vs T-piece. Extubation after mechanical ventilation. Chest. 1991;100(6):1655 [MEDLINE]
Comparison of three methods of gradual withdrawal from ventilatory support during weaning from mechanical ventilation. Am J Respir Crit Care Med 1994; 150:896-903 [MEDLINE]
A comparison of four methods of weaning patients from mechanical ventilation. N Engl J Med 1995; 332:345-350 [MEDLINE]
Tidal volume maintenance during weaning with pressure support. Am J Respir Crit Care Med. 1995;152(3):1034 [MEDLINE]
Extubation outcome after spontaneous breathing trials with T-tube or pressure support ventilation. The Spanish Lung Failure Collaborative Group. Am J Respir Crit Care Med. 1997;156(2 Pt 1):459-465 [MEDLINE]
Contribution of the endotracheal tube and the upper airway to breathing workload. Am J Respir Crit Care Med. 1998;157(1):23 [MEDLINE]
Prediction of post-extubation work of breathing. Crit Care Med. 2000;28(5):1341 [MEDLINE]
Extubation after breathing trials with automatic tube compensation, T-tube, or pressure support ventilation. Acta Anaesthesiol Scand. 2002;46(8):973 [MEDLINE]
Comparison of pressure support and T-tube weaning from mechanical ventilation: randomized prospective study. Croat Med J. 2004;45(2):162 [MEDLINE]
Weaning from mechanical ventilation with pressure support in patients failing a T-tube trial of spontaneous breathing. Intensive Care Med. 2006;32(1):165 [MEDLINE]
Extubation outcome following a spontaneous breathing trial with automatic tube compensation versus continuous positive airway pressure. Crit Care Med. 2006;34(3):682 [MEDLINE]
Prediction of extubation outcome: a randomised, controlled trial with automatic tube compensation vs. pressure support ventilation. Crit Care. 2009;13(1):R21 [MEDLINE]
Pressure support versus T-tube for weaning from mechanical ventilation in adults. Cochrane Database Syst Rev. 2014 May 27;(5):CD006056. doi: 10.1002/14651858.CD006056.pub2 [MEDLINE]
Comparison of pressure support ventilation and T-piece in determining rapid shallow breathing index in spontaneous breathing trials. Am J Med Sci. 2014 Oct;348(4):300-5 [MEDLINE]
TIP-EX Trial. Spontaneous-Breathing Trials with Pressure-Support Ventilation or a T-Piece. N Engl J Med. 2022 Nov 17;387(20):1843-1854. doi: 10.1056/NEJMoa2209041 [MEDLINE]
Duration of Weaning Trials
Effect of spontaneous breathing trial duration on outcome of attempts to discontinue mechanical ventilation. Spanish Lung Failure Collaborative Group. Am J Respir Crit Care Med. 1999;159(2):512 [MEDLINE]
Comparison of two methods for weaning patients with chronic obstructive pulmonary disease requiring mechanical ventilation for more than 15 days. Am J Respir Crit Care Med. 2001;164(2):225 [MEDLINE]
Central venous saturation is a predictor of reintubation in difficult-to-wean patients. Crit Care Med. 2010 Feb;38(2):491-6 [MEDLINE]
Rest After Weaning Trial
Reconnection to mechanical ventilation for 1 h after a successful spontaneous breathing trial reduces reintubation in critically ill patients: a multicenter randomized controlled trial. Intensive Care Med. 2017;43(11):1660 [MEDLINE]
Weaning Success
Diaphragm ultrasound as a predictor of successful extubation from mechanical ventilation. Thorax. 2014 May;69(5):423-7 [MEDLINE]
Mechanical Ventilation-induced Diaphragm Atrophy Strongly Impacts Clinical Outcomes. Am J Respir Crit Care Med. 2018;197(2):204 [MEDLINE]