Nomenclature of Ventilator Modes Has Become Increasingly Complex
Proposals Have Been Made to Revise the Ventilator Naming Scheme (Respir Care, 2007) [MEDLINE]
Continuous Mandatory Ventilation (CMV)
Clinical Use
Currently, Continuous Mandatory Ventilation is Less Commonly Used in the US
Concept
Minute Ventilation is Entirely Determined by the Set Respiratory Rate and Set Tidal Volume
Due to Sedation/Paralysis/Coma/Lack of Incentive to Increase Minute Ventilation Above the Set Respiratory Rate and Tidal Volume, the Patient Does Not Initiate Any Breaths Above the Set Respiratory Rate (and Ventilator Does Not Deliver Any Breaths if Patient Attempts to Triggers a Breath)
Types of Breaths Delivered
Volume Control Breaths (Ventilator-Triggered)
Work of Breathing
Effectively Zero
Settings
Respiratory Rate (RR)
Tidal Volume (VT)
Monitor
Peak Airway Pressure (PIP)
Plateau Pressure (Pplat)
Recommendations for Patients with ARDS Associated with Sepsis (2016 Surviving Sepsis Guidelines; Intensive Care Med, 2017) [MEDLINE]
No Ventilator Mode is Recommended Over Another for Mechanical Ventilation in Patients with Sepsis
Volume Synchronized Intermittent Mandatory Ventilation is Commonly Used (Am J Respir Crit Care Med, 2000) [MEDLINE]
However, in a Study of Ventilation Practices in Patients with ARDS, the Use of Synchronized Intermittent Mandatory Ventilation (SIMV) Decreased from 1998 (11%) to 2004 (1.6%) (Am J Respir Crit Care Med, 2008) [MEDLINE]
Concept
Mode Which Uses a Set Respiratory Rate and Tidal Volume in Which the Ventilator-Initiated Breaths are Synchronized with the Patient’s Breaths
Patient-Triggered Breaths Occur Over the Set Rate (and These are at a Variable Tidal Volume, Depending on the Patient’s Respiratory Mechanics)
Types of Breaths
Volume Control Breaths (Ventilator-Triggered): ventilator breaths are synchronized with the patient inspiratory effort
Spontaneous Unsupported Breaths (Patient-Triggered): at whatever size the patient is able to generate
Work of Breathing
Highly Variable
If the Respiratory Rate is Set High and the Patient is Not Triggering Any Breaths, this Mode Functions Similar to Assist Control and the Patient’s Work of Breathing Will Be Very Low
If the Respiratory Rate is Set Low (or at Zero) and the Patient is Triggering Most or All of the Breaths, the Work of Breathing is Increased (and if Not Properly Monitored, the Patient May Rapidly Fatigue)
Settings
Respiratory Rate (RR)
Tidal Volume (VT)
Monitor
Peak Airway Pressure (PIP)
Plateau Pressure (Pplat)
Advantages
If the Respiratory Rate is Set Low, SIMV Allows the Patient to Maintain a Higher Degree of Respiratory Muscle Function (and Increased Work of Breathing), as Compared to Assist Control Ventilation
Work of Breathing Can Be Gradually Increased by Weaning Down the Set Respiratory Rate: this may be advantageous in postoperative settings, etc
Decreased Propensity to Develop Auto-PEEP, as Compared to Assist Control Ventilation
Disadvantages
Inappropriately Low Set Respiratory Rate May Result in the Patient Having a High Work of Breathing (with Resultant Fatigue)
Clinical Efficacy
SIMV May Decrease Dyssynchrony, Better Preserve Respiratory Muscle Function, Decrease Mean Airway Pressure, and Allow Greater Control Over the Level of Support, as Compared to Assist Control Ventilation (Am Rev Respir Dis, 1983) [MEDLINE]
Trial of Assist Control vs Synchronized Intermittent Mandatory Ventilation in Acute Respiratory Failure (without COPD) (Crit Care Med, 1989) [MEDLINE]
No Clear Clinical Difference Between Modes (Although Cardiac Output, Mean Arterial Blood Pressure, Pulmonary Capillary Wedge Pressure, and Oxygen Consumption were All Better When the Level of Support Provided by SIMV was <50%)
Study of Intermittent Mandatory Ventilation (Anesthesiology, 1994) [MEDLINE]
The Respiratory Neuromuscular System Poorly Adapts to Changing Respiratory Workloads Since Muscle Contraction During Lower Levels of IMV is Similar During Both Supported (Mandatory) and Unsupported (Spontaneous) Breaths
Recommendations for Patients with ARDS Associated with Sepsis (2016 Surviving Sepsis Guidelines; Intensive Care Med, 2017) [MEDLINE]
No Ventilator Mode is Recommended Over Another for Mechanical Ventilation in Patients with Sepsis
However, in a Study of Ventilation Practices in Patients with ARDS, the Use of Synchronized Intermittent Mandatory Ventilation (SIMV) Decreased from 1998 (11%) to 2004 (1.6%) (Am J Respir Crit Care Med, 2008) [MEDLINE]
Concept
Mode Which Uses a Set Respiratory Rate and Driving Pressure in Which the Ventilator-Initiated Breaths are Synchronized with the Patient’s Breaths
Patient-Triggered Breaths Occur Over the Set Rate (and These are at a Variable Tidal Volume, Depending on the Patient’s Respiratory Mechanics)
Types of Breaths
Pressure Control Breaths (Ventilator-Triggered): ventilator breaths are synchronized with the patient inspiratory effort
Spontaneous Unsupported Breaths (Patient-Triggered): at whatever size the patient is able to generate
Work of Breathing
Highly Variable
If the Respiratory Rate is Set High and the Patient is Not Triggering Any Breaths, this Mode Functions Similar to Assist Control and the Patient’s Work of Breathing Will Be Very Low
If the Respiratory Rate is Set Low (or at Zero) and the Patient is Triggering Most or All of the Breaths, the Work of Breathing is Increased (and if Not Properly Monitored, the Patient May Rapidly Fatigue)
Settings
Respiratory Rate (RR)
Driving Pressure (Delta P)
Monitor
Tidal Volume
Advantages
If the Respiratory Rate is Set Low, SIMV Allows the Patient to Maintain a Higher Degree of Respiratory Muscle Function (and Increased Work of Breathing), as Compared to Assist Control
Work of Breathing Can Be Gradually Increased by Weaning Down the Set Respiratory Rate: this may be advantageous in postoperative settings, etc
Disadvantages
Inappropriately Low Set Respiratory Rate May Result in the Patient Having a High Work of Breathing: which can result in fatigue
Recommendations for Patients with ARDS Associated with Sepsis (2016 Surviving Sepsis Guidelines; Intensive Care Med, 2017) [MEDLINE]
No Ventilator Mode is Recommended Over Another for Mechanical Ventilation in Patients with Sepsis
Volume Assist Control (Assist Control, AC) Ventilation
Clinical Use
Volume Assist Control (Assist Control) Ventilation is Commonly Used (Am J Respir Crit Care Med, 2000) [MEDLINE]
Concept
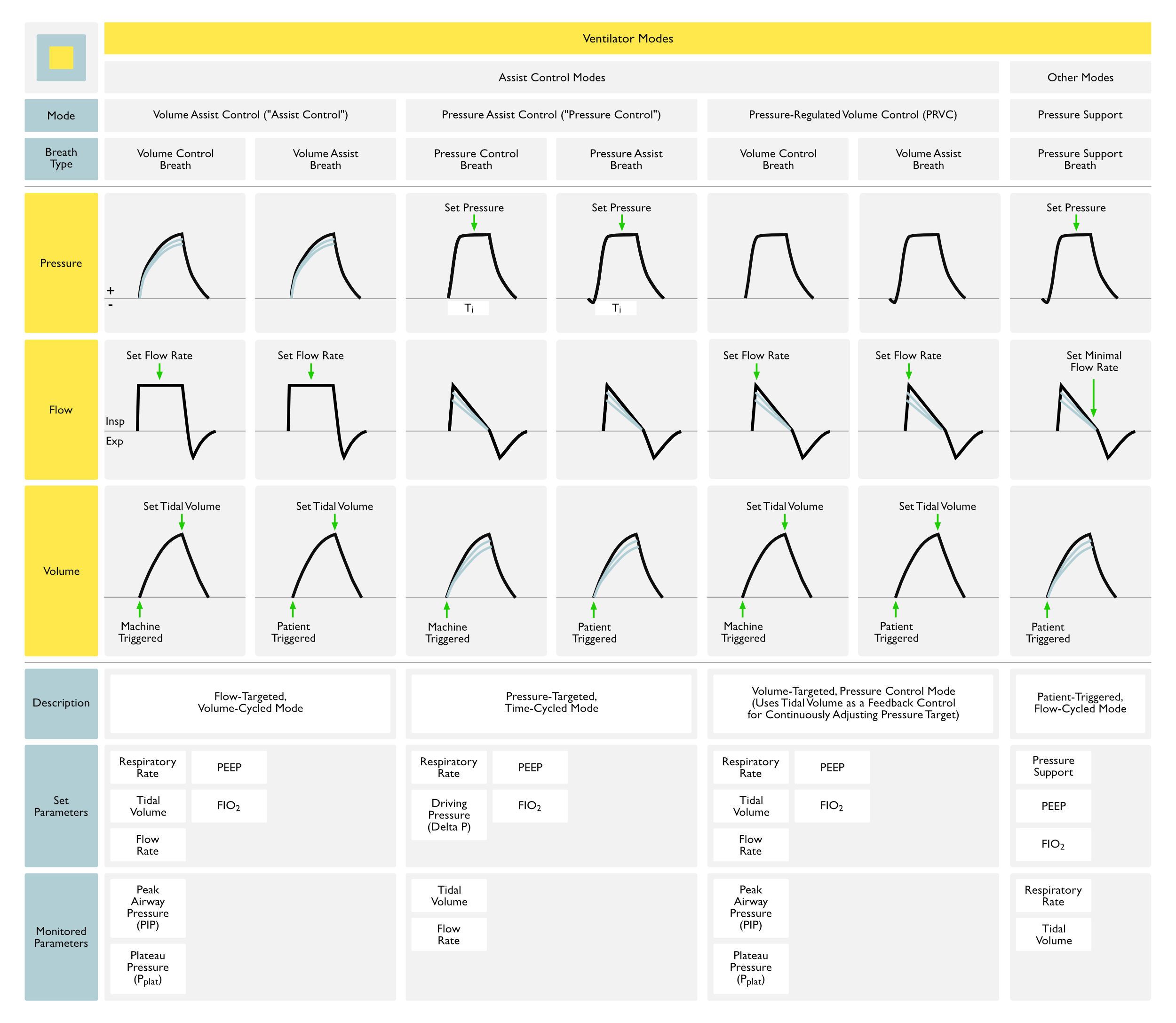
Flow-Targeted, Volume-Cycled Mode
Patient Can Trigger Additional Breaths Above the Set Respiratory Rate (with Each Breath Consisting of a Full Tidal Volume Breath)
Types of Breaths
Volume Control Breaths (Ventilator-Triggered)
Volume Assist Breaths (Patient-Triggered)
Work of Breathing
Very Low: most of the patient’s work of breathing in this mode (which is generally minimal) involves triggering ventilator-delivered breaths (if the patient is not triggering any breaths, their work of breathing is effectively zero)
Settings
Respiratory Rate (RR)
Tidal Volume (VT)
Flow Rate
PEEP
FIO2
I/E Ratio (Usually 1:2)
Monitor
Peak Airway Pressure (PIP)
Plateau Pressure (Pplat)
Advantages
Provides Guaranteed Delivery of the Desired Minute Ventilation (Due to a Set Tidal Volume and Set Respiratory Rate): this is useful if the patient is heavily sedated/paralyzed or apneic for other reasons
Disadvantages
Low Respiratory Muscle Workload May Result in Ventilator-Induced Diaphragmatic Dysfunction (VIDD)
Recommendations for Patients with ARDS Associated with Sepsis (2016 Surviving Sepsis Guidelines; Intensive Care Med, 2017) [MEDLINE]
No Ventilator Mode is Recommended Over Another for Mechanical Ventilation in Patients with Sepsis
Pressure Assist Control (Pressure Control, PC)
Concept
Pressure-Targeted, Time-Cycled Mode
Patient Can Trigger Additional Breaths Above the Set Respiratory Rate (with Each Breath Consisting of a Full Pressure Breath)
Types of Breaths
Pressure Control Breaths: machine triggered
Pressure Assist Breaths: patient triggered
Work of Breathing
Very Low: most of the patient’s work of breathing in this mode (which is generally minimal) involves triggering ventilator-delivered breaths (if the patient is nor triggering any breaths, their work of breathing is effectively zero)
Settings
Respiratory Rate (RR)
Delta P (Driving Pressure): since driving pressure is manually set, tidal volume that occurs will depend on lung/chest wall compliance
PEEP: typically initially set to +5
FIO2: typically initially set to 100% FIO2
Monitor
Tidal Volume (VT)
Advantages
Assuming No Change in Lung/Chest Wall Compliance, Provides Guaranteed Delivery of the Desired Minute Ventilation (Due to a Set Driving Pressure and Set Respiratory Rate): this is useful if the patient is heavily sedated/paralyzed or apneic for other reasons
Disadvantages
If Lung/Chest Wall Compliance Decreases During the Course of Ventilation (Due to Hemothorax, Pneumothorax, Pulmonary Edema), Tidal Volume Will Decrease: for this reason, tidal volumes need to be monitored closely in this mode (with ventilator alarms set accordingly)
Recommendations for Patients with ARDS Associated with Sepsis (2016 Surviving Sepsis Guidelines; Intensive Care Med, 2017) [MEDLINE]
No Ventilator Mode is Recommended Over Another for Mechanical Ventilation in Patients with Sepsis
Pressure-Regulated Volume Control (PRVC)
History
1991: development of pressure-regulated volume control (and inclusion in the Siemens Servo 300 Ventilator)
PRVC was Developed to Address the Shortfall of Pressure Control Ventilation Where it Cannot Guarantee a Minimum Minute Ventilation in the Setting of Changing Lung Mechanics or Patient Effort
Concept
Volume-Targeted, Pressure Control Mode
PRVC Uses Tidal Volume as a Feedback Control for Continuously Adjusting the Pressure Target (and Inspiratory Time): it is a type of adaptive pressure control
PRVC Will Attempt to Deliver the Set Tidal Volume Using the Lowest Possible Pressure: it increases or decreases the pressure by +/- 3 cm H2O per breath
With Improved Respiratory Mechanics or Increased Respiratory Effort by the Patient, PRVC Will Deliver a Lower Inspiratory Pressure
If Patient Effort is Large Enough, the Tidal Volume Will Increase Despite a Lower Inspiratory Pressure
With Worsened Respiratory Mechanics or Decreased Respiratory Effort by the Patient, PRVC Will Deliver a Higher Inspiratory Pressure
Work of Breathing
Very Low
Commercial Availability
Maquet Servo-i Ventilator: known as Pressure-Regulated Volume Control (PRVC)
Drager Evita Ventilator: known as AutoFlow
Hamilton Galileo Ventilator: known as Adaptive Pressure Ventilation
Puritan Bennett 840 Ventilator: known as Volume Control+
Engstrom/General Electric Ventilator: known as Volume Targeted Pressure Control, Pressure Controlled Volume Guaranteed
Settings
Respiratory Rate (RR)
Tidal Volume (VT)
Flow Rate
PEEP
FIO2
Inspiratory Time: resulting in an I/E ratio (typically around 1:2)
Inspiratory Rise Time (Slope Percent): used on some PRVC ventilators to specify the speed at which to reach the peak pressure
Upper Pressure Alarm (Usually at 35-40 cm H2O): maximum delivered pressure should be 5 cm H2O below this
Monitor
Peak Airway Pressure (PIP)
Plateau Pressure (Pplat)
Advantages
Guaranteed Delivery of a Minimum Average Tidal Volume (Unless the Pressure Alarm is Set Too Low, So that the Target Tidal Volume is Not Delivered)
Guaranteed Ventilation at the (Minimum) Set Respiratory Rate
Decreased Peak Inspiratory Pressure (PIP), Theoretically Decreasing the Risk of Barotrauma: however, risk of barotrauma is most related to the plateau pressure (Pplat)
However, this Decrease is Relative to Volume Control, in Which the Peak Inspiratory Pressure is a Function of Both Resistance and Compliance and Would Be Expected to Be Higher (But Does Not Reflect the Actual Lung-Distending Pressure, the Plateau Pressure)
Decelerating Flow Pattern (Similar to Pressure Control) May Improve the Distribution of Ventilation
Can Better Meet Patient’s Inspiratory Flow Demands Since it Adapts to the Patient’s Airway Resistance and Compliance on a Breath by Breath Basis (i.e. Achieves Flow Synchrony)
Provides Automatic Weaning of Ventilator Support (Since the Inspiratory Pressure Decreases with Increasing Patient Effort): this can be an advantage or a disadvantage, depending on the desire for the patient to be exerting these efforts
Disadvantages
Ventilator May Potentially Increase the Pressure to a Dangerously High Level as it Attempts to Maintain the Set Tidal Volume
The Maximum Delivered Pressure is Limited to 5 cm H2O Below the Set High Pressure Alarm Limit
High Pressure Alarm Limit Should Be Set at 35-40 cm H20
Pressure Delivered is Dependent on the Tidal Volume Achieved During the Previous Breath
If the Patient Intermittently Makes a Significant Inspiratory Effort, it Can Result in Variable Tidal Volumes than Can Be Higher or Lower than the Set Tidal Volume
If a Patient Have a High Respiratory Drive (in the Setting of Severe Metabolic Acidosis, etc), PRVC Will Decrease the Inspiratory Pressure, Inappropriately Shifting the Workload to the Patient
Clinical Efficacy
Study Comparing Patient Comfort Between PRVC vs Pressure Support Ventilation (Respir Care, 2008) [MEDLINE]
PRVC was Less Comfortable than Pressure Support
Recommendations for Patients with ARDS Associated with Sepsis (2016 Surviving Sepsis Guidelines; Intensive Care Med, 2017) [MEDLINE]
No Ventilator Mode is Recommended Over Another for Mechanical Ventilation in Patients with Sepsis
Automode
Concept
Ventilator Automatically Switches Between PRVC and Volume Support Mode
When There is No Patient Effort, Ventilator Delivers PRVC Breaths
When There is Patient Effort, Ventilator Delivers Volume Support Breaths
Commercial Availability
Maquet Servo-i Ventilator
Recommendations for Patients with ARDS Associated with Sepsis (2016 Surviving Sepsis Guidelines; Intensive Care Med, 2017) [MEDLINE]
No Ventilator Mode is Recommended Over Another for Mechanical Ventilation in Patients with Sepsis
1994: adaptive support ventilation was first described by Laubscher (Int J Clin Monit Comput 1994) [MEDLINE] (IEEE Trans Biomed Eng 1994) [MEDLINE]
1998: adaptive support ventilation became commercially vvailable in Europe
2007: adaptive support ventilation became commercially available in the US
Concept
Assist Control, Pressure-Targeted, Time-Cycled Mode Which Utilizes Respiratory Mechanics to Automatically Set a Tidal Volume-Frequency Pattern to Achieve a Desired Minute Ventilation Using Pressure Control Breaths
The Ventilator Algorithm Uses an Equation to Mimimize the Work of Inspiration (Theoretically Decreasing Applied Forces to the Lungs)
Equation Utilizes an Expiratory Time Constant Obtained from the Expiratory Limb of the Flow-Volume Loop (on a Breath by Breath Basis) (Crit Care Med, 1995) [MEDLINE] (Intensive Care Med, 2000) [MEDLINE]
Patients with Long Expiratory Time Constant (COPD or Asthma Exacerbation) Will Receive a Higher Tidal Volume and Lower Respiratory Rate (Int J Artif Organs, 2004) [MEDLINE] (Intensive Care Med, 2008) [MEDLINE]
Patients with Short Expiratory Time Constant (Stiff Lungs Due to ARDS, etc or Stiff Chest Wall Due to Kyphoscoliosis, Morbid Obesity, Neuromuscular Disease, etc) Will Receive a Lower Tidal Volume and Higher Respiratory Rate (Int J Artif Organs, 2004) [MEDLINE] (Intensive Care Med, 2008) [MEDLINE]
Tidal Volume is Adjusted to Deliver Low Tidal Volumes (But High Enough Above the Dead Space Volume to Avoid Hypoventilation)
Exhalation Time is Adjusted to Avoid Gas Trapping
In a Patient without Respiratory Efforts (Paralyzed Patient, etc), Adaptive Support Ventilation Delivers Pressure Control Breaths
In a Patient with Respiratory Efforts, Adaptive Support Ventilation Delivers Pressure Support for the Triggered Breaths with Supplemental Pressure Control Breaths to Achieve the Desired Respiratory Rate
Commercial Availability
Hamilton Galileo Ventilator
Settings
Desired Minute Ventilation (VE)
Patient Height (Which is Used to Calculate the Ideal Body Weight, Which is Subsequently Used to Estimate Anatomic Dead Space, Approximately 2.2 mL/kg)
Patient Sex
Percent of Normal Predicted Minute Ventilation Goal
If the Patient Has Increased Minute Ventilation Requirements (Due to Sepsis, Increased Dead Space, etc), this Might Be Set >100%
During Weaning, this Would Typically Be Set <100%
FIO2
PEEP
Advantages
Adaptive Support Ventilation Can Be Used from Initial Support Through Weaning
Adapts to Changing Lung Mechanics
Provides Automatic Weaning
Less Need for Human Manipulation of the Ventilator
Improved Synchrony
Disadvantages
Providers May Be Unfamiliar with This Ventilator Modality
Clinical Efficacy
Randomized Trial of Adaptive Support Ventilation in Fast-Track Extubation Protocol in Cardiac Surgery Patients (Anesthesiology, 2001) [MEDLINE]
Weaning Protocol Based on Adaptive Support Ventilation was Predictable and May Accelerate Extubation in Fast-Track Cardiac Surgery Patients
Trial Comparing Adaptive Support Ventilation with Pressure Control Synchronous Intermittent Mandatory Ventilation (Crit Care Med, 2002) [MEDLINE]
Adaptive Support Ventilation Had Lower Inspiratory Load and Improved Synchrony
Randomized Trial of Adaptive Support Ventilation vs Pressure-Regulated Volume Control Ventilation with Automode in Weaning Patients After Cardiac Surgery (Anesthesiology, 2008) [MEDLINE]
Adaptive Support Ventilation was Associated with Earlier Extubation
Randomized Trial Comparing Adaptive Support Ventilation to Pressure Assist/Control Ventilation in Mechanically-Ventilated Adult Medical ICU Patients (Chest, 2015) [MEDLINE]: n = 229
Adaptive Support Ventilation Shortened the Duration of Weaning and Total Duration of Mechanical Ventilation with a Fewer Number of Manual Ventilator Settings
No Differences were Observed in Terms of 28-Day Weaning Success or Mortality Rate
Recommendations for Patients with ARDS Associated with Sepsis (2016 Surviving Sepsis Guidelines; Intensive Care Med, 2017) [MEDLINE]
No Ventilator Mode is Recommended Over Another for Mechanical Ventilation in Patients with Sepsis
Adjusts the Level of Pressure Support Required to Achieve a Set Tidal Volume, Based on the Inspiratory Effort by the Patient
Volume Support is Essentially Pressure Support with a Guaranteed Tidal Volume
Recommendations for Patients with ARDS Associated with Sepsis (2016 Surviving Sepsis Guidelines; Intensive Care Med, 2017) [MEDLINE]
No Ventilator Mode is Recommended Over Another for Mechanical Ventilation in Patients with Sepsis
Continuous Positive Airway Pressure (CPAP)
Clinical Utility
While Many Ventilators Use a “CPAP Mode”, During Which Pressure Support Ventilation is Added (So Called “CPAP/PS”), CPAP is Rarely Used Alone in the Modern Era for Spontaneous Breathing Trials
Concept
Maintains a Continuous Level of Pressure Throughout Inspiration
Indications
Weaning from Mechanical Ventilation
Recommendations for Patients with ARDS Associated with Sepsis (2016 Surviving Sepsis Guidelines; Intensive Care Med, 2017) [MEDLINE]
No Ventilator Mode is Recommended Over Another for Mechanical Ventilation in Patients with Sepsis
Pressure Support Ventilation (PSV)
Concept
Patient-Triggered, Flow-Cycled Mode
Inspiratory Pressure is Delivered by the Ventilator Until the Inspiratory Flow Decreases to a Predetermined Percentage of its Peak Value (Usually 25%)
Types of Breaths
Pressure Support Breaths (Patient-Triggered)
Work of Breathing
Variable (Depending on the Level of Pressure Support)
Patient’s Work of Breathing is Inversely Proportional to the Amount of Pressure Support Applied (i.e. High Pressure Support = Low Work of Breathing), Assuming that the Inspiratory Flow Rate is Sufficient to Meet the Patient Demand (Crit Care Med, 1997) [MEDLINE]
High Pressure Support Usually Results in a Higher Tidal Volume and Lower Respiratory Rate
Work of Breathing is Also Inversely Proportional to the Inspiratory Flow Rate, Such that Increasing the Inspiratory Flow Rate Shortens the Time Until Maximal Airway Pressure is Reached (Crit Care Med, 2003) [MEDLINE]
Indications
Ventilator Weaning
Settings
Pressure Support Level
The Required Pressure Support Level Depends on the Size of the Endotracheal Tube: resistance of the endotracheal tube is related to the endotracheal tube diameter and the inspiratory flow rate (Chest, 1988) [MEDLINE]
For 7.5-8.0 Endotracheal Tubes, Pressure Support of 5 cm H2O is Generally Considered Adequate to Overcome the Resistance of the Tube
For <7.0 Endotracheal Tube, Pressure Support ≥10 cm H20 May Be Required to Overcome the Resistance of the Tube (Anesthesiology, 1991) [MEDLINE]
Some Ventilators Have an Automatic Tube Compensation Mode, Which is a Type of Pressure Support Ventilation that Applies an Adequate Amount of Pressure to Overcome the Work of Breathing Imparted by the Endotracheal Tube (Which Can Vary from Breath to Breath)
Automatic Tube Compensation May Improve Tolerance of Spontaneous Breathing Trial Over CPAP Alone (Crit Care Med, 2006) [MEDLINE]
PEEP
FIO2
Monitor
Respiratory Rate (RR)
Tidal Volume (VT)
Index of Rapid Shallow Breathing (RSBI)
Advantages
Comfortable for Patient
Useful (and Commonly Used) for Ventilator Weaning
May Be Combined with Synchronized Intermittent Mandatory Ventilation (SIMV): SIMV breaths with most of the work of breathing performed by the ventilator and PS breaths with increasing amount of work performed by the patient (as pressure support levels are gradually decreased)
Disadvantages
Lack of Guaranteed Ventilation at a (Minimum) Set Respiratory Rate, Since the Patient Must Trigger All of the Breaths (Pressure Support Relies Entirely on the Patient’s Intrinsic Respiratory Drive)
When Used for Full Ventilatory Support, Pressure Support Ventilation Results in Poorer Sleep (as Compared to Assist Control Ventilation (Intensive Care Med, 2007) [MEDLINE]
As Compared to Assist Control Ventilation, Pressure Support Results in Greater Sleep Fragmentation, Less Stage 1 and 2 Non-Rapid Eye Movement (NREM) Sleep, More Wakefulness During the First Part of the Night, and Less Stage 3 and 4 NREM Sleep During the Second Part of the Night
When Used for Full Ventilatory Support, Pressure Support May Result in the Development of Central Sleep Apnea (CSA) During Sleep (see Central Sleep Apnea): may occur in patient on pressure support ventilation, due to sedation which depresses the central respiratory drive, critical illness itself, or hyperventilation (with hypocapnia)
Study of Ventilator Mode on Quality of Sleep (Am J Respir Crit Care Med, 2002) [MEDLINE]: n = 11
Inspiratory Assistance from Pressure Support Causes Hypocapnia, Which Combined with the Lack of a Backup Respiratory Rate and Wakefulness Drive Can Lead to Central Apneas and Sleep Fragmentation (Especially in Patients with Heart Failure)
When Used for Full Ventilatory Support, Pressure Support May Result in Ventilator Dyssynchrony (Which May Prolong the Duration of Mechanical Ventilation) (Chest, 1995) [MEDLINE] (Intensive Care Med, 2006) [MEDLINE]
Mechanisms Include Inspiratory Response Delays Caused by the Inspiratory Triggering Mechanisms and the Ventilator Demand Flow Characteristics, Mismatch Between the Patient’s cCompletion of the Inspiration and the Ventilator’s Criterion for Terminating Pressure Support; and Restriction of Expiration Due to Resistance from the Patient’s Airways, Endotracheal Tube, and/or Expiratory Valve
When Used for Full Ventilatory Support, High Levels of Pressure (≥20 cm H2O) are Required to Prevent Atelectasis and to Maintain a Stable Respiratory Pattern (Intensive Care Med, 1989) [MEDLINE] (Chest, 1990) [MEDLINE]
Higher Levels of Pressure Support (≥20 cm H2O) are Generally Less Comfortable for Patients, as Compared to Moderate Levels of Pressure Support (10-15 cm H2O) (Chest, 2004) [MEDLINE]
Pressure Support is Relatively Contraindicated in the Setting of Increased Airway Resistance (COPD or Asthma Exacerbation)
Due to Decreased Airflow Resulting in Termination of Inspiration After a Smaller than Optimal Tidal Volume Has Been Achieved (J Appl Physiol, 1985) [MEDLINE] (Chest, 1993) [MEDLINE]
Due to Pressure Support Not Preventing the Development of Auto-PEEP (Am J Respir Crit Care Med, 1995) [MEDLINE]
In This Setting, Selecting a Higher Percentage of the Peak Inspiratory Flow as the Trigger to Terminate Inspiration May Slightly Improve Auto-PEEP (Crit Care Med, 2007) [MEDLINE]
Clinical Efficacy-Weaning
Cochrane Database Systematic Review of Pressure Support vs T-Piece Weaning from Mechanical Ventilation in Adults (Cochrane Database Syst Rev, 2014) [MEDLINE]
Due to Low Quality Studies, the Effects on Weaning Success, ICU Mortality Rate, Reintubation Rate, ICU Length of Stay, and Pneumonia Rate were Imprecise
Pressure Support was More Effective than T-Piece for Successful Spontaneous Breathings Trials Among Patients with Simple Weaning
Based on 3 Trials, Pressure Support Use Shortened Weaning, While 1 Trial Demonstrated that T-Piece Use Shortened Weaning
Trial of Neurally Adjusted Ventilatory Assist vs Pressure Support (Crit Care Med, 2016) [MEDLINE]
In Patients Recovering from Acute Respiratory Failure, Levels of Neurally Adjusted Ventilatory Assist Between 0.5-2.5 cm H2O/μvolt are Comparable to Pressure Support Levels from 7-25 cm H2O in Terms of Respiratory Muscle Unloading
Neurally Adjusted Ventilatory Assist Provides Better Patient-Ventilator Interaction, But Can Be Sometimes Excessively Sensitive to Electrical Activity of the Diaphragm in Terms of Triggering
Comparative Trial of Pressure Support vs Proportional Assist Ventilation (Respir Care, 2017) [MEDLINE]
Mechanical Ventilation Dyssynchrony was Influenced by Patient Effort, Respiratory Mechanics, Ventilator Type, and Ventilation Mode
In Pressure Support Mode, Delayed Cycling was Associated with Shorter Effort in Obstructive Respiratory Mechanics Profiles, Whereas Premature Cycling was More Common with Longer Effort and a Restrictive Profile
Proportional Assist Ventilation-Plus (PAV+) Prevented Premature Cycling But Not Delayed Cycling, Especially in Obstructive Respiratory Mechanics Profiles, and it was Associated with a Lower Tidal Volume
Recommendations for Patients with ARDS Associated with Sepsis (2016 Surviving Sepsis Guidelines; Intensive Care Med, 2017) [MEDLINE]
No Ventilator Mode is Recommended Over Another for Mechanical Ventilation in Patients with Sepsis
1992: proportional assist ventilation was first developed by Younes (Am Rev Respir Dis, 1992) [MEDLINE] (Am Rev Respir Dis, 1992) [MEDLINE]
1999: proportional assist ventilation first became available in Europe
2006: proportional assist ventilation first became available in the US
Concept
Useful for a Spontaneously Breathing Patient with Normal Respiratory Drive
Proportional Assist Ventilation is Similar to Pressure Support Ventilation, Except that the Pressure Applied is a Function of the Patient Effort
Using the Servo, the Greater the Inspiratory Effort, the Greater the Increase in Applied Pressure
In Contrast, Pressure Support Ventilation Delivers a Constant Pressure Throughout Inspiration (as Pressure Controlled Breaths Via a Servo), Regardless of the Patient’s Inspiratory Effort
Pressure Rises to a Preset Level Which is Held Constant Until a Cycling Criterion is Met (Percent of the Maximum Inspiratory Flow is Reached): the inspiratory flow and tidal volume is the result of the patient’s inspiratory effort, the level of pressure applied, and the respiratory system mechanics
Indications
Ventilator Weaning
Commercial Availability
Puritan Bennett 840 Ventilator: known as proportional assist ventilation
Drager Ventilator: known as proportional pressure support
Settings
Airway Type (Endotracheal Tube vs Tracheostomy)
Airway Size (Inner Diameter)
Percentage of Work Supported (Assist Range: 5-95%)
Tidal Volume Limit
Pressure Limit
Expiratory Sensitivity: this parameter tells the ventilator at what flow to end the inspiration (since, normally, as inspiration ends, flow should stop)
Advantages
Decreased Work of Breathing
Improved Synchrony
Adapts to Changing Respiratory Mechanics and Patient Effort
Decreased Need for Ventilator Manipulation
Decreased Need for Sedation
Similar Hemodynamic Profile to Pressure Support Ventilation
Disadvantages
All Breaths are Spontaneous (Similar to Pressure Support)
Not Useful in a Patient with Decreased Respiratory Drive
The Patient Controls the Timing and Size of the Breath
While There are No Preset Volume, Pressure, or Flow Goals, Safety Limits Can Be Set for the Volume and Pressure
Not Useful in a Patient with Large Air Leak (Due to a Bronchopleural Fistula, etc)
Cautious Use in Patient with Airway Obstruction/Dynamic Hyperinflation (as the Ventilator May Not Sense the Prolonged Exhalation)
Cautious Use in Patient with High Ventilatory Drive (as the Ventilator May Overestimate the Respiratory System Mechanics and May Provide Overassistance, Even if the Patient Has Stopped Inspiration)
Clinical Efficacy
Trial Comparing Proportional Assist Ventilation to Pressure Support Ventilation (J Appl Physiol, 1996) [MEDLINE]
Proportional Assist Ventilation Decreased the Work of Breathing More than Pressure Support Ventilation
Trial Comparing Proportional Assist Ventilation to Pressure Support Ventilation in COPD Patients (Intensive Care Med, 1999) [MEDLINE]
Proportional Assist Ventilation Decreased the Work of Breathing More than Pressure Support Ventilation
Trial Comparing Proportional Assist Ventilation to Pressure Support Ventilation (Am J Respir Crit Care Med, 2000) [MEDLINE]
Proportional Assist Ventilation Decreased the Work of Breathing More than Pressure Support Ventilation
Study of the Effects of Pressure Support and Proportional Assist Ventilation in Hypercapnic COPD Patients with Acute Respiratory Failure (Respiration, 2003) [MEDLINE]
In Hypercapnic COPD Patients with Acute Respiratory Failure, Pressure Support May Cause Missing Efforts, Whereas Proportional Assist Ventilation May Cause “Runaway” Phenomenon, Due to Distinct Patient-Ventilator Interactions
However, These Phenomenon Do Not Limit the Improvement in Arterial Blood Gases with the Use of Both Modes
Trial Comparing Proportional Assist Ventilation to Pressure Support Ventilation (Intensive Care Med, 2006) [MEDLINE]
Proportional Assist Ventilation Decreased the Work of Breathing More than Pressure Support Ventilation
Trial of Pressure Support and Proportional Assist Ventilation in Patients with ARDS (Anesthesiology, 2006)[MEDLINE]
In Patients with ARDS Due to Sepsis, Respiratory Rate and Cardiac Index were Slightly Higher, as Compared to Pressure-Support Ventilation
Tidal Volumes were Variable, But within the Lung Protective Range (6-8 mL/kg with Plateau Pressure <30 cm H2O)
Trial of Pressure Support and Proportional Assist Ventilation in Mechanically-Ventilated Patients (Crit Care Med, 2007) [MEDLINE]
Proportional Assist Ventilation was More Efficacious than Pressure Support Ventilation in Terms of Matching Ventilatory Requirements with Ventilator Assistance, Resulting in Less Patient-Ventilator Dyssynchrony and Better Quality of Sleep
Trial of Pressure Support and Proportional Assist Ventilation in Mechanically-Ventilated Critically Ill Patients (Intensive Care Med, 2008) [MEDLINE]
Tidal Volumes were Variable, But within the Lung Protective Range (6-8 mL/kg with Plateau Pressure <30 cm H2O)
Proportional Assist Ventilation Increase Synchrony, as Compared to Pressure Support
Recommendations for Patients with ARDS Associated with Sepsis (2016 Surviving Sepsis Guidelines; Intensive Care Med, 2017) [MEDLINE]
No Ventilator Mode is Recommended Over Another for Mechanical Ventilation in Patients with Sepsis
Inverse Ratio Ventilation (IRV)
Concept
While Not a Ventilator Mode, this is a Ventilatory Strategy (Employed During Volume-Limited or Pressure-Limited Ventilation) with the Induction of Inspiratory Time > Expiratory Time (i.e. Inversion of the I:E Ratio)
Inverse Ratio Ventilation Strategy is Most Commonly Used in Conjunction with Pressure Ventilation (as Pressure Control-Inverse Ratio Ventilation), But There is No Clinical Difference Between its Use with Either of Volume-Cycled or Pressure-Cycled Ventilation (Chest, 2000) [MEDLINE]
The Clinical Goal is to Increase the Mean Airway Pressure to Potentially Improve Oxygenation
Indications
Refractory Hypoxemia in the Setting of ARDS
Technique
Inverse Ratio Ventilation Usually Requires Heavy Sedation with Paralysis to Facilitate Inversion of the Ratio (Since the Ratio is Typically Uncomfortable for the Patient)
Use of Inverse Ratio Ventilation with Volume-Cycled Ventilation
With a Ramp Wave Flow Pattern: peak inspiratory flow rate is initially set at least 4x higher than the minute ventilation and then slowly decreased until the inspiratory time exceeds the expiratory time
With a Square Wave Flow Pattern: end-inspiratory pause is added (usually 0.2 sec) and then slowly increased until the inspiratory time exceeds the expiratory time
Use of Inverse Ratio Ventilation with Pressure-Cycled Ventilation
Gradually Increase the I:E Ratio Until the Inspiratory Time Exceeds the Expiratory Time
When Inverse Ratio Ventilation is Used with Pressure Control, this Strategy Will Assure that a Maximal Plateau Pressure Will Not Be Exceeded (Protecting Against Ventilator-Induced Lung Injury and Barotrauma)
While Unproven, Development of Auto-PEEP May Be Less Common with Pressure Control-Inverse Ratio Ventilation than it is with Volume Control-Inverse Ratio Ventilation (Intensive Care Med, 1992) [MEDLINE]
Disadvantages
Development of Auto-PEEP (with Consequences Including Barotrauma, Hypotension, etc) (Chest, 1988) [MEDLINE]
Development of Barotrauma (Independent of the Development of Auto-PEEP)
Risk of Pneumothorax Has Been Reported to Be as High as 29% (Despite the Presence of Auto-PEEP) (Crit Care Med, 1995) [MEDLINE]
Clinical Efficacy
Observational Study of Pressure Control-Inverse Ratio Ventilation in Severe Adult Respiratory Failure (Chest, 1988) [MEDLINE]: n = 31
IRV was Associated with a Significant Increase in the Mean Airway Pressure and the pO2 (from 69 to 80 mm Hg), Despite a Decrease in PEEP
Study of Effects of Inverse Ratio Ventilation on Hemodynamics and Pulmonary Parameters (Chest, 1992) [MEDLINE]
IRV is Usually Well-Tolerated Hemodynamically
Trial of IRV in ARDS (Crit Care Med, 2001) ([MEDLINE]
In ARDS, Extending the End-Inspiratory Pause without Inducing a Clinically Significant Increase in PEEPi, Does Not Consistently Improve Arterial Oxygenation But Enhances Carbon Dioxide Elimination
Recommendations for Patients with ARDS Associated with Sepsis (2016 Surviving Sepsis Guidelines; Intensive Care Med, 2017) [MEDLINE]
No Ventilator Mode is Recommended Over Another for Mechanical Ventilation in Patients with Sepsis
Alveolar Recruitment is Maximized by the High Continuous Positive Airway Pressure During the P high Phase (Crit Care Med, 1987) [MEDLINE] (Crit Care Med, 1987) [MEDLINE]
The Transition from P high to P low Deflates the Lungs and Results in the Elimination of Carbon Dioxide
The Difference Between P high and P low is the Driving Pressure
Airway Pressure Release Ventilation Allows the Patient to Breathe Spontaneously While Receiving High Airway Pressure with an Intermittent Pressure Release
Historically, Airway Pressure Release Ventilation Has Been Viewed as “Alternating Levels of CPAP”: this gave rise to the P high, P low, etc terminology for settings
Confusion Exists in the Literature Regarding the Distinction Between APRV and Bi-Level Ventilation
Review of 50 Published Studies Noted that 78% of Them Described APRV, While 22% Described Bi-Level Ventilation (Intensive Care Med, 2008) [MEDLINE]
Both Modes Allow Unrestricted Spontaneous Breathing During and Between the Mandatory Breaths
Differences
APRV Uses Extreme I:E Ratios (>2:1), While Bi-Level Ventilation Usually Does Not
APRV Usually Keeps the Duration of T low at ≤1.5 sec, While Bi-Level Ventilation Has No Restriction on T low (Consequently, Bi-Level Ventilation Allows More Spontaneous Breaths to Occur at P low)
APRV Results in Higher Mean Airway Pressure, But Lower Minute Ventilation (VE) than Bi-Level Ventilation
In Intermittent Mandatory Airway Pressure Release Ventilation (IMPRV), Cyclic Inflations and Deflations are Synchronized to Occur After Every Few Spontaneous Breaths (Intensive Care Med, 1992) [MEDLINE]
Obstructive Lung Disease (COPD or Asthma Exacerbation) or High Minute Ventilation Requirement
Due to Increased Risk of Hyperinflation, High Alveolar Pressure, and Pulmonary Barotrauma
Physiology
Time Ratio
Airway Pressure Release Ventilation Time Ratios Reported in Literature: 1:1 to 9:1
The Greater the Percentage of the Total Time Spent at High Pressure (80-95%), the Greater the Alveolar Recruitment
The Lesser the Percentage of the Total Time Spent at Low Pressure (Usually 0.2-0.8 sec in Adults), the Less Alveolar De-Recruitment Occurs
If the Time Spent at Low Pressure is Too Short, Expiration Will Be Incomplete and Auto-PEEP Will Develop
However, Some APRV Regimens Use P Low of 0 cm H2O with the Required Development of Auto-PEEP
There is a Theoretical Concern About Developing Auto-PEEP, Since (Unlike Applied PEEP Which Distributes Evenly) Auto-PEEP Distributes Predominantly to Lung Units with the Highest Airway Resistance and Lowest Compliance (Chest, 1995) [MEDLINE]
Lung Units with Partially Obstructed Airways and Atelectatic Lung Units Will Consequently Have Higher PEEP than the Set P low
Clinical Determinants of Tidal Volume
Driving Pressure
Lung/Chest Wall Compliance (Which Includes the Airway Resistance)
Timing and Duration of Pressure Release
Clinical Determinants of Oxygenation (pO2)
FIO2
Amount of P high
Time Spent at T high
Clinical Determinants of Ventilation (pCO2)
Driving Pressure or Delta P (P high – P low)
Larger Delta P = More Volume Per Release = More CO2 Excretion Per Release
Patient’s Spontaneous Breathing
While Spontaneous Breathing May Occur at Both P high and P low, it Typically Occurs During the P high Phase (Due to the Short Duration of Time Spent at P low)
Technique
Ventilator Settings/Terminology
P high is the Upper Pressure Level
P low or PEEP is the Lower Pressure Level
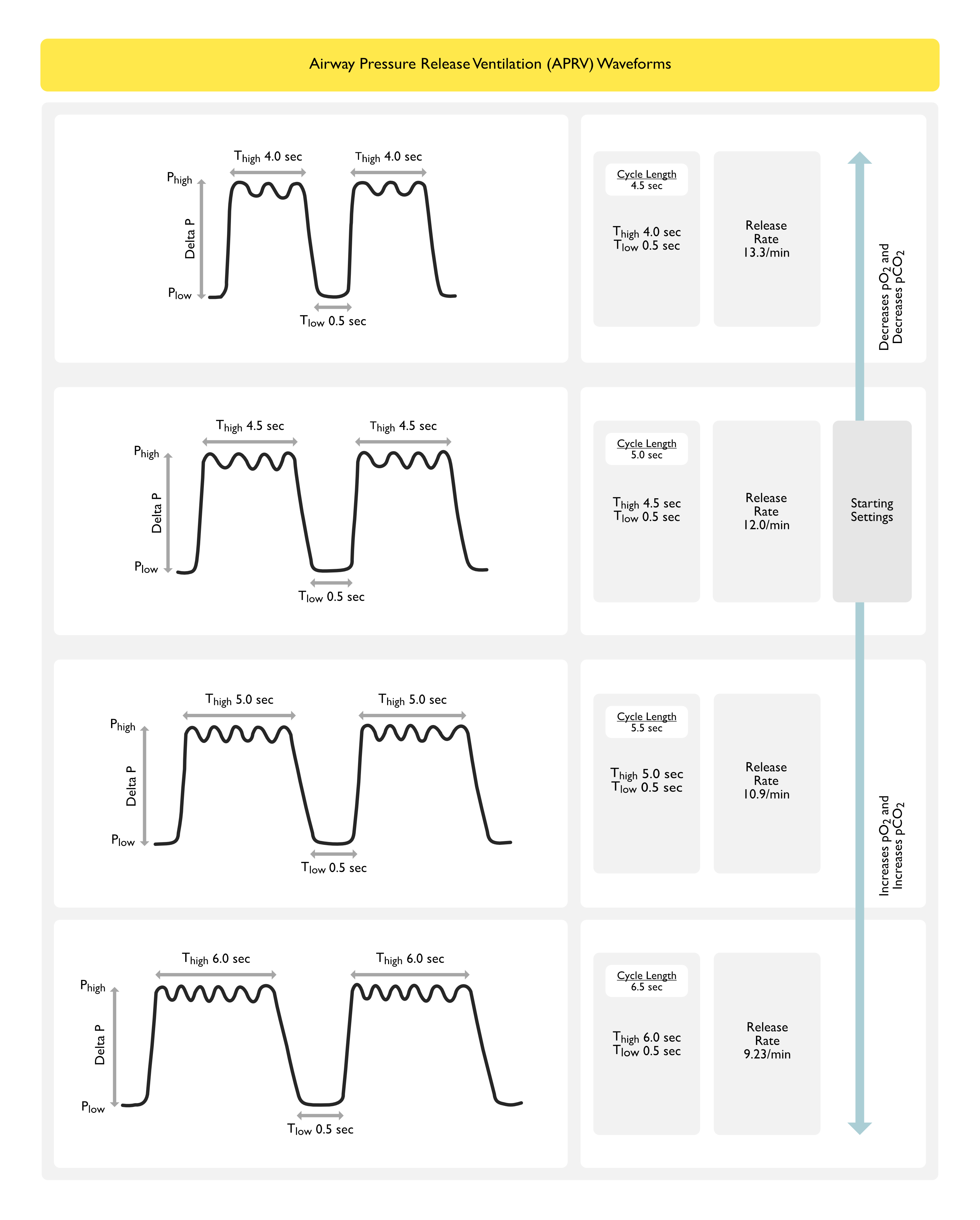
T high is the Time Spent at P high
T low is the Time Spent at T low
Release Rate is the Number of Cycles (or Releases) Per Minute: increasing the release rate will decrease the pCO2
T high 4.0 sec + T low 0.5 sec (cycle length = 4.5 sec) -> release rate = 13.3/min
T high 4.5 sec + T low 0.5 sec (cycle length = 5.0 sec) -> release rate = 12.0/min
T high 5.0 sec + T low 0.5 sec (cycle length = 5.5 sec) -> release rate = 10.9/min
T high 6.0 sec + T low 0.5 sec (cycle length = 6.5 sec) -> release rate = 9.23/min
General Approach is to Ventilate the Lung on the Steep Portion of the Pressure-Volume Curve (Where Mean Lung Volume and Pressures are Adequate for Oxygenation and Ventilation and the Tidal Volume Lies Between the Lower and Upper Inflection Points of the Curves)
This Strategy Improves Lung Compliance, Venous Admixture, and pO2 in ARDS
This Strategy Also Protects the Lung in ARDS by Avoiding Collapse During Expiration (Atelectrauma) and Stretch-Related Lung Injury During Inspiration (Volutrauma, Barotrauma)
Sedation Should Be Minimized (Although, Some Sedation is Usually Required)
Paralytics Should Be Avoided, Since Using Paralytics Will Eliminate the Spontaneous Breaths (One of the Purported Benefits of APRV)
Initial Settings
No Consensus Exists with How to Set the Initial APRV Parameters: both of the following approaches are probably grossly equivalent
Approach #1: use short T low + P low of 0 cm H2O -> prolongs I:E ratio and creates auto-PEEP
Approach #2: use longer T low (to eliminate auto-PEEP) + higher P low (to avoid alveolar collapse)
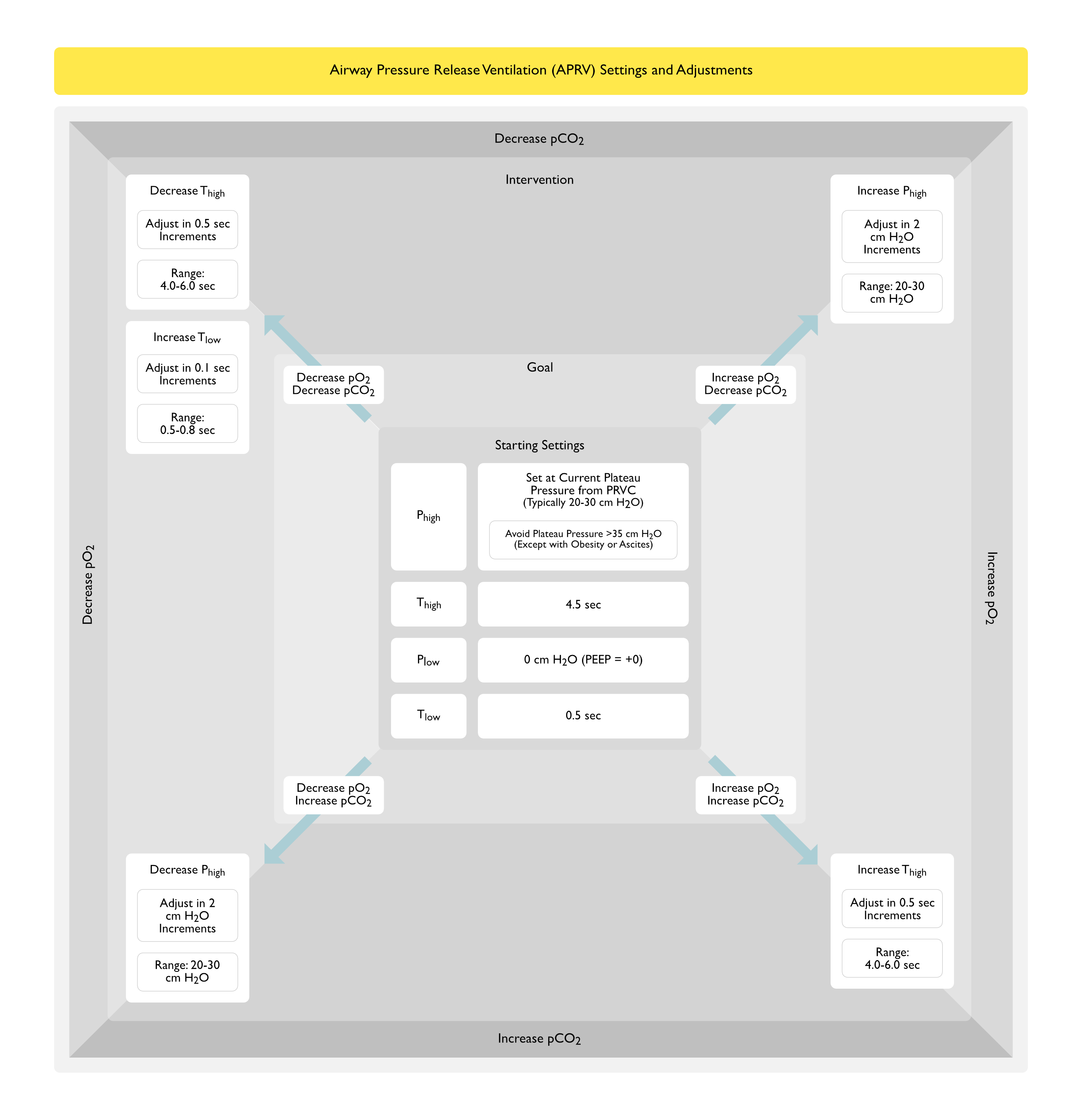
Initial P high is Set Using the Plateau Pressure of the Current Volume-Controlled Mode (Preferably 20-30 cm H2O)
Target Tidal Volume Should Be Approximately 6 ml/kg PBW
Avoid Using P high >35 cm H2O, Unless the Patient Has Obesity/Ascites/etc
Initial P low Should Be Set at 0 cm H2O
Initial T high Should Be Set at 4.5 sec
Initial T low Should Be Set at 0.5 sec
Subsequent Changes
Wait 4-6 hrs for Clinical Response After a Change in Ventilator Settings
To Increase pO2
Increase FIO2
Increase P high (Adjust in 2 cm H2O Increments, Range: 20-30 cm H2O)
Increase T high (Adjust in 0.5 sec Increments, Range: 4.0-6.0 sec): this will decrease the release rate
Decrease T low: note that as the T high:T low ratio increases, auto-PEEP can develop (which will decrease effective delta P and VT)
Lung Recruitment Maneuvers
To Decrease pO2
Decrease FIO2
Decrease T high: this will increase the release rate
Increase T low (Adjust in 0.1 sec Increments, Range: 0.5-0.8 sec): this will increase the time spent at release
To Decrease pCO2
Increase P high (Adjust in 2 cm H2O Increments, Usual Range: 20-30 cm H2O): this will increase the delta P (P high – P low)
Decrease T high (Adjust in 0.5 sec Increments): this will increase the release rate
Increase T low (Adjust in 0.1 sec Increments, Range: 0.5-0.8 sec): this will increase the time spent at release
Optimize Spontaneous Breathing*
To Increase pCO2
Increase T high (Adjust in 0.5 sec Increments, Range: 4.0-6.0 sec): this will decrease the release rate
Decrease P high (Adjust in 2 cm H2O Increments, Usual Range: 20-30 cm H2O): this will decrease the delta P (P high – P low) and may undesirably decrease the pO2
Advantages
Alveolar Recruitment Due to High Airway Pressure and Diaphragmatic Contraction During Spontaneous Breathing
Improved Oxygenation, as Spontaneous Breaths Allow More Even Distribution of Ventilation (Decreasing Intrapulmonary Shunt)
Preservation of Spontaneous Breathing
With Spontaneous Breathing, APRV is Better Tolerated than Inverse Ratio Ventilation (Without the Need for Deep Sedation/Paralysis)
However, in the Absence of Spontaneous Breathing (i.e. During Paralysis), APRV is Functionally Equivalent to Inverse Ratio Ventilation (Due to the Relatively Long Times Spent at High Pressure)
No Significant Impact on Intracranial Pressure in the Setting of Traumatic Brain Injury and ARDS (J Crit Care, 2019) [MEDLINE]
Disadvantages
Risk of Volutrauma Due to Spontaneous Breathing During High Pressure (with Concomitant generation of Large Tidal Volumes and Large Negative Pleural Pressure Swings)
Increased Work of Breathing
Increased Energy Expenditure Due to Patient Taking Spontaneous Breaths
Clinical Efficacy
Trial of APRV vs Pressure Control Ventilation in Trauma Patients with ARDS (Am J Respir Crit Care Med, 2001) [MEDLINE]: n = 30
APRV was Associated with Increased Respiratory System Compliance, Increased Arterial pO2, Increased Cardiac Index, Increased Oxygen Delivery, Decreased Venous Admixture (QVA/QT), and Decreased Oxygen Extraction
Pressure Control Ventilation was Associated with Decreased Respiratory System Compliance, Decreased Arterial pO2, Decreased Cardiac Index, Decreased Oxygen Delivery, Increased Venous Admixture (QVA/QT), Increased Need for Sufentanil/Midazolam/Norepinephrine/Dobutamine
APRV was Associated with a Shorter Duration of Ventilatory Support and ICU Length of Stay
No Difference in Mortality Rates
Large Randomized Controlled Trial of APRV (Acta Anaesthesiol Scand, 2004) [MEDLINE]: RCT (n = 58) comparing APRV with SIMV with PS (study was terminated early for futility)
No 28-Day or 1-Year Mortality Benefit
No Difference in Ventilator-Free Days at 28 Days
However, Proning was Used in Both Arms and its Effects May Have Overshadowed the Potential Effects of APRV in this Study
Randomized Trial of APRV in Adult Trauma Patients with Respiratory Failure (J Trauma, 2010) [MEDLINE]: n= 63
For Adult Trauma Patients Requiring Mechanical Ventilation >72 hrs, APRV Had a Similar Safety Profile as Low Tidal Volume Ventilation
Trends for APRV Patients to Have Increased Ventilator Days, ICU Length of Stay, and Ventilator-Associated Pneumonia May Be Explained by Initial Higher Acute Physiology and Chronic Health Evaluation II Scores
Retrospective Review of APRV in Trauma Patients (J Trauma Acute Care Surg, 2012) [MEDLINE]
After Controlling for Confounding Factors, APRV Mode Increased the Number of Ventilator Days in Trauma Patients
Animal Study of APRV in Traumatized Pigs with Combined Brain and Lung Trauma (J Trauma Acute Care Surg, 2015) [MEDLINE]
Microdialysis Data Suggested a Trend Toward Increased Cerebral Ischemia Associated with APRV Over Time
Trial of APRV vs Standard Low Tidal Volume Ventilation in ARDS (Intensive Care Med, 2017) [MEDLINE]: n = 148
Early Application of APRV in ARDS Improved Oxygenation, Improved Respiratory System Compliance, Decreased Pplat, Decreased Duration of Mechanical Ventilation, and Decreased the ICU Length of Stay
Prospective Randomized Intermountain Trial of Low Tidal vs Traditional APRV and Volume Control Ventilation Protocols (Crit Care Med, 2018) [MEDLINE]: n = 246 planned (study stopped early because of low enrollment and inability to consistently achieve tidal volumes <6.5 mL/kg in the low tidal volume-airway pressure release ventilation arm)
APRV Often Resulted in Release Volumes >12 mL/kg Despite a Protocol Targeting Low Tidal Volume Ventilation
Current APRV Protocols are Unable to Achieve Consistent and Reproducible Delivery of Low Tidal Volume Ventilation Goals
Systematic Review and Meta-Analysis of APRV in Acute Hypoxemic Respiratory Failure (Ann Intensive Care, 2019) [MEDLINE]: n = 330 (5 RCT’s)
Evidence was Low Quality with Moderate Heterogeneity
APRV was Associated with a Higher Number of Ventilator-Free Days at Day 28
APRV was Associated with a Lower Hospital Mortality Rate
APRV was Not Associated with Any Negative Hemodynamic Impact or Increased Risk of Barotrauma
Recommendations for Patients with ARDS Associated with Sepsis (2016 Surviving Sepsis Guidelines; Intensive Care Med, 2017) [MEDLINE]
No Ventilator Mode is Recommended Over Another for Mechanical Ventilation in Patients with Sepsis
Ventilator Mode in Which the Electrical Discharge from the Diaphragm (i.e. Diaphragmatic Excitation = EAdi) is Used to Trigger a Ventilator-Delivered Breath (Respir Care, 2011) [MEDLINE]
When a Deflection in the EAdi Signal Greater than the Set Threshold (Usually >0.5 μvolts) is Detected by a Sensor in a Gastric Tube Catheter, a Ventilator Breath is Delivered
Degree of Assist is Proportional to the Amplitude of the EAdi Signal and the Set Assist Level
Set Assist Level is Determined with the Assist Level Being Increased to Achieve a Comfortable and Consistent Tidal Volume and an EAdi Signal Which Remains Flat
Neuroventilator Coupling (Time Between a Spontaneous Diaphragmatic Effort and the Delivery of a Ventilator Breath) is Faster with NAVA than with Conventional Ventilator Modes
Advantages
XXXX
Disadvantages
Requires the Patient to Have an Intact Respiratory Drive
Clinical Efficacy
French Prospective Study of NAVA vs Pressure Support in Spontaneously Breathing Acute Respiratory Failure Patients in the ICU (Intensive Care Med, 2011) [MEDLINE]: n= 22
NAVA Decreased Ventilator Dyssynchrony
Trial of NAVA vs Proportional Assist Ventilation (Crit Care, 2015) [MEDLINE]: n = 16
NAVA vs Proportional Assist Ventilation Both Prevented Overdistention, Improved Neuromechanical Coupling, Improved the Variability of the Respiratory Pattern, and Decrease Ventilator Dyssynchrony
Trial of Neurally Adjusted Ventilatory Assist vs Pressure Support (Crit Care Med, 2016) [MEDLINE]
In Patients Recovering from Acute Respiratory Failure, Levels of Neurally Adjusted Ventilatory Assist Between 0.5-2.5 cm H2O/μvolt are Comparable to Pressure Support Levels from 7-25 cm H2O in Terms of Respiratory Muscle Unloading
Neurally Adjusted Ventilatory Assist Provides Better Patient-Ventilator Interaction, But Can Be Sometimes Excessively Sensitive to Electrical Activity of the Diaphragm in Terms of Triggering
French Multicenter Randomized Trial of NAVA vs Pressure Support Ventilation in the Early Phase of Ventilator Weaning (Intensive Care Med, 2016) [MEDLINE]: n = 125
NAVA Did Not Increase the Probability of Remaining in a Partial Ventilatory Mode (Either NAVA or Pressure Support) throughout the First 48 hrs
NAVA Did Not Increase Ventilator-Free Days at Day 28 or the 28-Day Mortality Rate
NAVA Decreased Ventilator Dyssynchrony
NAVA Resulted in Less Frequent Application of Postextubation Noninvasive Mechanical Ventilation
Recommendations for Patients with ARDS Associated with Sepsis (2016 Surviving Sepsis Guidelines; Intensive Care Med, 2017) [MEDLINE]
No Ventilator Mode is Recommended Over Another for Mechanical Ventilation in Patients with Sepsis
Ventilation Mode Employing the Use of High Respiratory Rates
Technique
General Comments: all techniques utilize respiratory rates >100 breaths/min
Conventional Mechanical Ventilation with Small Tidal Volumes and Rapid Respiratory Rates
Chest Wall Oscillation
High-Frequency Percussive Ventilation (HFPV): flow-regulated, pressure-limited, and time-cycled ventilator that delivers a series of high-frequency small volumes (at 200-900 cycles/min) in a successive stepwise stacking pattern
High-Frequency Jet Ventilation
High-Frequency Oscillation Ventilation (HFOV): most widely used type of high-frequency ventilation used in adult critical care -> delivers a small tidal volume by oscillating a bias gas flow in the airway
Clinical Efficacy
Randomized, Controlled Multicenter Oscillatory Ventilation For Acute Respiratory Distress Syndrome Trial) MOAT Trial of High-Frequency Oscillation Ventilation (Am J Respir Crit Care Med, 2002) [MEDLINE]
While the Study was Not Powered to Evaluate Mortality Differences, But an Insignificant Trend Toward Improved Overall 30-Day Mortality Rate in the High-Frequency Oscillation Ventilation Group, as Compared with the Conventional Ventilation Group (37% vs 52% 30-Day Mortality, p=0.098)
There Were No Significant Difference Between Groups in New or Worsening Barotrauma, Endotracheal Tube Obstruction, or Adverse Hemodynamic Effects
Retrospective Chart Review of High-Frequency Oscillation Ventilation for Rescue Therapy in Medical-Surgical ICU Patients (Chest, 2004) [MEDLINE]: n = 156
High-Frequency Oscillation Ventilation Had Beneficial Effects on pO2/FIO2 Ratios and Oxygenation Index
30-Day Mortality Rate was 61.7%
Pneumothorax Rate was 21.8%
Canadian Clinical Trials Group OSCILLATE High-Frequency Oscillation Study in ARDS (NEJM, 2013) [MEDLINE]
In Adults with Moderate-to-Severe ARDS, Early Application of High-Frequency Oscillation Ventilation (as Compared with a Ventilation Strategy of Low Tidal Volume and High PEEP) Did Not Decrease and May Increase, the In-Hospital Mortality Rate
Recommendations (American Thoracic Society/European Society of Intensive Care Medicine/Society of Critical Care Medicine Clinical Practice Guidelines for Mechanical Ventilation in ARDS) (Am J Respir Crit Care Med, 2017) [MEDLINE]
High Frequency Ventilation is Not Routinely Recommended in Moderate-Severe ARDS (Strong Recommendation, Moderate-High Confidence)
Recommendations for Patients with ARDS Associated with Sepsis (2016 Surviving Sepsis Guidelines; Intensive Care Med, 2017) [MEDLINE]
No Ventilator Mode is Recommended Over Another for Mechanical Ventilation in Patients with Sepsis
Esophageal Pressure-Guided Mechanical Ventilation
Rationale
Pressures
Esophageal Pressure is a Surrogate for Pleural Pressure
Optimal Level of PEEP Maintains Oxygenation, While Preventing Lung Injury Due to Repeated Alveolar Collapse and Overdistention
In Patients with Low Pleural Pressure, PEEP Can Be Maintained Low to Keep Transpulmonary Pressure Low
In Patients with High Pleural Pressure (Where Underinflation May Cause Hypoxemia), PEEP Can Be Increased to Maintain a Positive Transpulmonary Pressure Which Might Improve Aeration and Oxygenation without Causing Overdistention
Stress Index
Rationale: stress index calculation allows determination of the optimal PEEP
Technique
Software-Derived Dimensionless Value Obtained During a Constant Flow Breath Reflecting the Shape of the Airway Pressure vs Time Curve
Requires Absence of Patient Effort
Optimal Stress Index is a Straight Diagonal (i.e. 1.0): reflecting unchanging compliance throughout the breath
Alternatively, if recruitment/derecruitment is occurring during the breath, the stress index curve is concave bowing upward (low compliance early, followed by high compliance later in the breath) -> stress index <1
Alternatively, if overdistention is occurring during the breath, the stress index curve is concave bowing downward (high compliance early, followed by low compliance later in the breath) -> stress index >1
Clinical Efficacy
EPVent Pilot Study Using Transpulmonary Pressure (NEJM, 2008) [MEDLINE]
Esophageal Pressure was Used as a Surrogate for Pleural Pressure
PEEP Levels were Set to Maintain End-Expiratory Transpulmonary Pressure Between 0-10 cm H2O and End-Inspiratory Transpulmonary Pressure to <25 cm H2O, Based on a Sliding Scale Using the Patient's pO2 and FIO2
Transpulmonary Pressure was Used to Determine the Optimal Level of PEEP Based on Lung and Chest Wall Mechanics
pH was Maintained Between 7.30-7.45
pO2 was Maintained Between 55-120 mm Hg
As Compared to Standard Care, a Ventilator Strategy Using Esophageal Pressures to Estimate Transpulmonary Pressure Improved Oxygenation and Respiratory System Compliance and Had a Trend Toward a Decreased Mortality Rate
Study of Stress Index (Using Airway Pressure vs Time) to Decrease Injurious Ventilation (as Assessed by CT Scanning Measures of Ventilator-Induced Lung Injury) in ARDS (Anesthesiology, 2013) [MEDLINE]
Injurious Ventilation was Most Associated with Pplat,rs >25 cm H2O and Stress Index >1.05
Pplat,rs = plateau pressure for the respiratory system (inspiratory)
Stress Index = dimensionless number obtained during a constant flow breath which describes the shape of airway pressure vs time curve and the shape of the transpulmonary pressure (PL) vs time curve
Recommendations for Patients with ARDS Associated with Sepsis (2016 Surviving Sepsis Guidelines; Intensive Care Med, 2017) [MEDLINE]
No Ventilator Mode is Recommended Over Another for Mechanical Ventilation in Patients with Sepsis
Recommendations for Patients with ARDS Associated with Sepsis (2016 Surviving Sepsis Guidelines; Intensive Care Med, 2017) [MEDLINE]
No Ventilator Mode is Recommended Over Another for Mechanical Ventilation in Patients with Sepsis
References
Ventilator Modes
General
Randomized, prospective trial of pressure-limited versus volume-controlled ventilation in severe respiratory failure. Crit Care Med. 1994;22(1):22 [MEDLINE]
How is mechanical ventilation employed in the intensive care unit? An international utilization review. Am J Respir Crit Care Med. 2000;161(5):1450 [MEDLINE]
Characteristics and outcomes in adult patients receiving mechanical ventilation: a 28-day international study. JAMA. 2002;287(3):345 [MEDLINE]
Classification of ventilator modes: update and proposal for implementation. Respir Care 2007; 52:301–323 [MEDLINE]
Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016. Intensive Care Med. 2017 Jan 18. doi: 10.1007/s00134-017-4683-6 [MEDLINE]
Continuous Mandatory Ventilation (CMV)
Patient comfort during pressure support and volume controlled continuous mandatory ventilation. Respir Care 2008; 53:897-902 [MEDLINE]
External work output and force generation during synchronized intermittent mechanical ventilation. Effect of machine assistance on breathing effort. Am Rev Respir Dis. 1988;138(5):1169 [MEDLINE]
Assist control versus synchronized intermittent mandatory ventilation during acute respiratory failure. Crit Care Med. 1989;17(7):607 [MEDLINE]
Regulation of inspiratory neuromuscular output during synchronized intermittent mechanical ventilation. Anesthesiology. 1994;80(1):13 [MEDLINE]
Influence of pressure and flow-triggered synchronous intermittent mandatory ventilation on inspiratory muscle work. Crit Care Med. 1994;22(12):1933 [MEDLINE]
Synchronized intermittent mandatory ventilation with and without pressure support ventilation in weaning patients with COPD from mechanical ventilation. Chest. 1994;105(4):1204 [MEDLINE]
Evolution of mechanical ventilation in response to clinical research. Am J Respir Crit Care Med. 2008;177(2):17 [MEDLINE]
Assist Control (AC) Ventilation
Assist control versus synchronized intermittent mandatory ventilation during acute respiratory failure. Crit Care Med. 1989;17(7):607 [MEDLINE]
Pressure-Regulated Volume Control (PRVC) Ventilation
Patient comfort during pressure support and volume controlled continuous mandatory ventilation. Respir Care 2008; 53:897-902 [MEDLINE]
Adaptive Support Ventilation (ASV)
Automatic selection of tidal volume, respiratory frequency and minute ventilation in intubated ICU patients as start up procedure for closed-loop controlled ventilation. Int J Clin Monit Comput 1994; 11:19-30 [MEDLINE]
An adaptive lung ventilation controller. IEEE Trans Biomed Eng 1994; 699. 41:51–59 [MEDLINE]
Simple method to measure total expiratory time constant based on the passive expiratory flow-volume curve. Crit Care Med. 1995;23(6):1117 [MEDLINE]
Expiratory time constants in mechanically ventilated patients with and without COPD. Intensive Care Med. 2000;26(11):1612 [MEDLINE]
Adaptive support ventilation for fast tracheal extubation after cardiac surgery: a randomized controlled study. Anesthesiology 2001; 95:1339–1345 [MEDLINE]
Adaptive support ventilation. Respir Care Clin North Am 2001; 7:425–440 [MEDLINE]
Patient ventilator interactions during partial ventilatory support: a preliminary study comparing the effects of adaptive support ventilation with synchronized intermittent mandatory ventilation plus inspiratory pressure support. Crit Care Med 2002; 30:801–807 [MEDLINE]
Adaptive support ventilation (ASV). Minerva Anestesiol 2002; 68:365–368 [MEDLINE]
Automatic “respirator/weaning” with adaptive support ventilation: the effect on duration of endotracheal intubation and patient management. Anesth Analg 2003; 97:1743–1750 [MEDLINE]
Evaluation of adaptive support ventilation in paralysed patients and in a physical lung model. Int J Artif Organs. 2004;27(8):709 [MEDLINE]
Randomized controlled trial comparing adaptive-support ventilation with pressure-regulated volume-controlled ventilation with automode in weaning patients after cardiac surgery. Anesthesiology 2008; 109:81–87 [MEDLINE]
Automatic selection of breathing pattern using adaptive support ventilation. Intensive Care Med. 2008;34(1):75 [MEDLINE]
A randomized controlled trial comparing the ventilation duration between adaptive support ventilation and pressure assist/control ventilation in medical patients in the ICU. Chest. 2015 Jun;147(6):1503-1509. doi: 10.1378/chest.14-2599 [MEDLINE]
Pressure Support Ventilation (PSV)
Respiratory function during pressure support ventilation. Chest. 1986;89(5):677 [MEDLINE]
Pressure support compensation for inspiratory work due to endotracheal tubes and demand continuous positive airway pressure. Chest. 1988;93(3):499 [MEDLINE]
Determinants and limits of pressure-preset ventilation: a mathematical model of pressure control. J Appl Physiol (1985). 1989;67(3):1081 [MEDLINE]
Comparison of pressure support ventilation and assist control ventilation in patients with acute respiratory failure. Intensive Care Med. 1989;15(6):364 [MEDLINE]
Efficacy of pressure support ventilation dependent on extravascular lung water. Chest. 1990;97(6):1412 [MEDLINE]
Inspiratory pressure support compensates for the additional work of breathing caused by the endotracheal tube. Anesthesiology. 1991;75(5):739 [MEDLINE]
Patient and ventilator work of breathing and ventilatory muscle loads at different levels of pressure support ventilation. [MEDLINE]
Decreasing imposed work of the breathing apparatus to zero using pressure-support ventilation. Crit Care Med. 1993;21(9):1333 [MEDLINE]
Mechanical ventilation. American College of Chest Physicians’ Consensus Conference. Chest. 1993;104(6):1833 [MEDLINE]
An analysis of desynchronization between the spontaneously breathing patient and ventilator during inspiratory pressure support. Chest. 1995;107(5):1387 [MEDLINE]
Variability of patient-ventilator interaction with pressure support ventilation in patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 1995;152(1):12 [MEDLINE]
Patient-ventilator flow dyssynchrony: flow-limited versus pressure-limited breaths. Crit Care Med. 1997;25(10):1671 [MEDLINE]
Effect of ventilator mode on sleep quality in critically ill patients. Am J Respir Crit Care Med. 2002;166(11):1423 [MEDLINE]
Effect of different inspiratory rise time and cycling off criteria during pressure support ventilation in patients recovering from acute lung injury. Crit Care Med. 2003;31(11):2604 [MEDLINE]
Assessment of physiologic variables and subjective comfort under different levels of pressure support ventilation. Chest. 2004;126(3):85 [MEDLINE]
Patient-ventilator asynchrony during assisted mechanical ventilation. Intensive Care Med. 2006;32(10):1515 [MEDLINE]
Assist-control ventilation vs. low levels of pressure support ventilation on sleep quality in intubated ICU patients. Intensive Care Med. 2007;33(7):1148 [MEDLINE]
Extubation outcome following a spontaneous breathing trial with automatic tube compensation versus continuous positive airway pressure. Crit Care Med. 2006;34(3):682 [MEDLINE]
Effect of different cycling-off criteria and positive end-expiratory pressure during pressure support ventilation in patients with chronic obstructive pulmonary disease. Crit Care Med. 2007;35(11):2547 [MEDLINE]
Pressure support versus T-tube for weaning from mechanical ventilation in adults. Cochrane Database Syst Rev. 2014 May 27;(5):CD006056. doi: 10.1002/14651858.CD006056.pub2 [MEDLINE]
Comparison Between Neurally Adjusted Ventilatory Assist and Pressure Support Ventilation Levels in Terms of Respiratory Effort. Crit Care Med. 2016 Mar;44(3):503-11. doi: 10.1097/CCM.0000000000001418 [MEDLINE]
Influences of Duration of Inspiratory Effort, Respiratory Mechanics, and Ventilator Type on Asynchrony With Pressure Support and Proportional Assist Ventilation. Respir Care. 2017 May;62(5):550-557. doi: 10.4187/respcare.05025 [MEDLINE]
Proportional Assist Ventilation (PAV)
Proportional assist ventilation, a new approach to ventilatory support. Theory. Am Rev Respir Dis 1992; 145:114-120 [MEDLINE]
Proportional assist ventilation. Results of an initial clinical trial. Am Rev Respir Dis 1992; 145:121-129 [MEDLINE]
Patient ventilator interaction during acute hypercapnia: pressure support vs. proportional assist ventilation. J Appl Physiol 1996; 81:426-436 [MEDLINE]
Proportional assist versus pressure support ventilation: effects on breathing pattern and respiratory work of patients with chronic ob- structive pulmonary disease. Intensive Care Med 1999; 25:790-798 [MEDLINE]
Compensation for increase in respiratory workload during mechanical ventilation. Pressure support versus proportional assist ventilation. Am J Respir Crit Care Med 2000; 161:819–826 [MEDLINE]
Effect of different levels of pressure support and proportional assist ventilation on breathing pattern, work of breathing and gas exchange in mechanically ventilated hypercapnic COPD patients with acute respiratory failure. Respiration 2003; 70:355-361 [MEDLINE]
Respiratory load compensation during mechanical ventilation-proportional assist ventilation with load-adjustable gain factors versus pressure support. Intensive Care Med 2006; 32:692-699 [MEDLINE]
Short-term cardiorespiratory effects of proportional assist and pressure support ventilation in patients with acute lung injury/acute respiratory distress syndrome. Anesthesiology 2006; 105:703-708 [MEDLINE]
Patient ventilator interaction and sleep in mechanically ventilated patients: pressure support versus proportional assist ventilation. Crit Care Med 2007; 35:1048-1054 [MEDLINE]
Proportional assist ventilation with load-adjustable gain factors in critically ill patients: comparison with pressure support. Intensive Care Med 2008; 34:2026-2034 [MEDLINE]
Proportional assist ventilation and neurally adjusted ventilatory assist-better approaches to patient ventilator synchrony? Clin Chest Med 2008; 29:329-342 [MEDLINE]
Influences of Duration of Inspiratory Effort, Respiratory Mechanics, and Ventilator Type on Asynchrony With Pressure Support and Proportional Assist Ventilation. Respir Care. 2017 May;62(5):550-557. doi: 10.4187/respcare.05025 [MEDLINE]
Inverse Ratio Ventilation (IRV)
Improved oxygenation and lower peak airway pressure in severe adult respiratory distress syndrome. Treatment with inverse ratio ventilation. Chest. 1986;89(2):211 [MEDLINE]
Pressure controlled inverse ratio ventilation in severe adult respiratory failure. Chest. 1988;94(4):755 [MEDLINE]
Pressure control inverse ratio ventilation as a method to reduce peak inspiratory pressure and provide adequate ventilation and oxygenation. Chest. 1989;95(5):1081 [MEDLINE]
Cardiorespiratory effects of pressure controlled inverse ratio ventilation in severe respiratory failure. Chest. 1989;96(6):1356 [MEDLINE]
The use of pressure-controlled inverse ratio ventilation in the surgical intensive care unit. J Trauma. 1991;31(9):1211 [MEDLINE]
Effects of inverse ratio ventilation on cardiorespiratory parameters in severe respiratory failure. Chest. 1992;102(5):1556 [MEDLINE]
Open up the lung and keep the lung open. Intensive Care Med. 1992;18(6):319 [MEDLINE]
Cardiorespiratory effects of pressure-controlled ventilation with and without inverse ratio in the adult respiratory distress syndrome. Chest. 1993;104(3):871 [MEDLINE]
Should inverse ratio ventilation be used in adult respiratory distress syndrome? Am J Respir Crit Care Med. 1994;149(5):1354 [MEDLINE]
Long-term effects of two different ventilatory modes on oxygenation in acute lung injury. Comparison of airway pressure release ventilation and volume-controlled inverse ratio ventilation. Am J Respir Crit Care Med. 1994;149(6):1550 [MEDLINE]
Pressure-controlled, inverse ratio ventilation that avoids air trapping in the adult respiratory distress syndrome. Crit Care Med. 1995;23(2):279 [MEDLINE]
Beneficial effects of the “open lung approach” with low distending pressures in acute respiratory distress syndrome. A prospective randomized study on mechanical ventilation. Am J Respir Crit Care Med. 1995;152(6 Pt 1):1835 [MEDLINE]
Inverse ratio ventilation (I/E = 2/1) in acute respiratory distress syndrome: a six-hour controlled study. Am J Respir Crit Care Med. 1997;155(5):1637 [MEDLINE]
Prospective randomized trial comparing pressure-controlled ventilation and volume-controlled ventilation in ARDS. For the Spanish Lung Failure Collaborative Group. Chest. 2000;117(6):1690 [MEDLINE]
Extending inspiratory time in acute respiratory distress syndrome. Crit Care Med. 2001;29(1):40 [MEDLINE]
The outcome of early pressure-controlled inverse ratio ventilation on patients with severe acute respiratory distress syndrome in surgical intensive care unit. Am J Surg. 2002;183(2):151 [MEDLINE]
Airway Pressure Release Ventilation (APRV)
Airway pressure release ventilation: a new concept in ventilatory support. Crit Care Med. 1987;15(5):459 [MEDLINE]
Airway pressure release ventilation. Crit Care Med. 1987;15(5):462 [MEDLINE]
Airway pressure release ventilation during acute lung injury: a prospective multicenter trial. Crit Care Med. 1991;19(10):1234 [MEDLINE]
Continuous positive airway pressure (CPAP) vs. intermittent mandatory pressure release ventilation (IMPRV) in patients with acute respiratory failure. Intensive Care Med. 1992;18(2):69 [MEDLINE]
The effects of applied vs auto-PEEP on local lung unit pressure and volume in a four-unit lung model. Chest. 1995 Oct;108(4):1073-9 [MEDLINE]
Spontaneous breathing during ventilatory support improves ventilation-perfusion distributions in patients with acute respiratory distress syndrome. Am J Respir Crit Care Med. 1999;159(4 Pt 1):1241 [MEDLINE]
Airway pressure release ventilation increases cardiac performance in patients with acute lung injury/adult respiratory distress syndrome. Crit Care. 2001;5(4):221 [MEDLINE]
Long-term effects of spontaneous breathing during ventilatory support in patients with acute lung injury. Am J Respir Crit Care Med. 2001;164(1):43 [MEDLINE]
Effects of spontaneous breathing during airway pressure release ventilation on renal perfusion and function in patients with acute lung injury. Intensive Care Med. 2002;28(10):1426 [MEDLINE]
Influence of different release times on spontaneous breathing pattern during airway pressure release ventilation. Intensive Care Med. 2002;28(12):1742 [MEDLINE]
Lung recruitment maneuvers in acute respiratory distress syndrome and facilitating resolution. Crit Care Med. 2003;31(4 Suppl):S265 [MEDLINE]
Lung computed tomography during a lung recruitment maneuver in patients with acute lung injury. Intensive Care Med. 2003;29(2):218 [MEDLINE]
Airway pressure release ventilation as a primary ventilatory mode in acute respiratory distress syndrome. Acta Anaesthesiol Scand. 2004;48(6):722-31 [MEDLINE]
Other approaches to open-lung ventilation: Airway pressure release ventilation. Crit Care Med. 2005 Mar;33(3 Suppl):S228-40 [MEDLINE]
Preliminary experience with airway pressure release ventilation in a trauma/surgical intensive care unit. J Trauma. 2005;59(1):71 [MEDLINE]
Does airway pressure release ventilation offer important new advantages in mechanical ventilatory support? Resp Care. 2007;52:452-460
Airway pressure release and biphasic intermittent positive airway pressure ventilation: are they ready for prime time? J Trauma. 2007;62(5):1298 [MEDLINE]
Airway pressure release ventilation and biphasic positive airway pressure: a systemic review of definitional criteria. Intensive Care Med 2008;34(10):1766-1773 [MEDLINE]
A randomized prospective trial of airway pressure release ventilation and low tidal volume ventilation in adult trauma patients with acute respiratory failure. J Trauma. 2010;69(3):501-510 [MEDLINE]
Comparison of APRV and BIPAP in a mechanical model of ARDS (abstract). Respir Care 2010;55(11): 1516
Airway pressure release ventilation: what do we know? Respir Care. 2012 Feb;57(2):282-92 [MEDLINE]
Compared to conventional ventilation, airway pressure release ventilation may increase ventilator days in trauma patients. J Trauma Acute Care Surg. 2012 Aug;73(2):507-10 [MEDLINE]
Lung protective ventilation (ARDSNet) versus airway pressure release ventilation: ventilatory management in a combined model of acute lung and brain injury. J Trauma Acute Care Surg. 2015 Feb;78(2):240-9; discussion 249-51. doi: 10.1097/TA.0000000000000518 [MEDLINE]
Early application of airway pressure release ventilation may reduce the duration of mechanical ventilation in acute respiratory distress syndrome. Intensive Care Med. 2017;43(11):1648 [MEDLINE]
Experimental study of airway pressure release ventilation in the treatment of acute respiratory distress syndrome. Exp Ther Med. 2017 Sep;14(3):1941-1946. doi: 10.3892/etm.2017.4718 [MEDLINE]
Randomized Feasibility Trial of a Low Tidal Volume-Airway Pressure Release Ventilation Protocol Compared With Traditional Airway Pressure Release Ventilation and Volume Control Ventilation Protocols. Crit Care Med. 2018;46(12):1943 [MEDLINE]
APRV for ARDS: the complexities of a mode and how it affects even the best trials. J Thorac Dis. 2018;10(Suppl 9):S1058 [MEDLINE]
Airway pressure release ventilation during acute hypoxemic respiratory failure: a systematic review and meta-analysis of randomized controlled trials. Ann Intensive Care. 2019 Apr 4;9(1):44. doi: 10.1186/s13613-019-0518-7 [MEDLINE]
Airway pressure release ventilation does not increase intracranial pressure in patients with traumatic brain injury with poor lung compliance. J Crit Care. 2019 Apr;50:118-121. doi: 10.1016/j.jcrc.2018.11.034 [MEDLINE]
Neurally Adjusted Ventilatory Assist (NAVA)
Neurally adjusted ventilatory assist: a ventilation tool or a ventilation toy? Respir Care. 2011 Mar;56(3):327-35 [MEDLINE]
Neurally adjusted ventilatory assist and proportional assist ventilation both improve patient-ventilator interaction. Crit Care. 2015;19:56 [MEDLINE]
Neurally adjusted ventilatory assist as an alternative to pressure support ventilation in adults: a French multicentre randomized trial. Intensive Care Med. 2016;42(11):1723 [MEDLINE]
Comparison Between Neurally Adjusted Ventilatory Assist and Pressure Support Ventilation Levels in Terms of Respiratory Effort. Crit Care Med. 2016 Mar;44(3):503-11. doi: 10.1097/CCM.0000000000001418 [MEDLINE]
High-Frequency Oscillatory Ventilation (HFOV)
High-frequency oscillatory ventilation for acute respiratory distress syndrome in adults: a randomized, controlled trial. Am J Respir Crit Care Med. 2002 Sep 15;166(6):801-8 [MEDLINE]
High-frequency oscillatory ventilation in adults: the Toronto experience. Chest. 2004 Aug;126(2):518-27 [MEDLINE]
Esophageal Pressure-Guided Mechanical Ventilation
Airway pressure-time curve profile (stress index) detects tidal recruitment/hyperinflation in experimental acute lung injury. Crit Care Med. 2004 Apr;32(4):1018-27 [MEDLINE]
EPVent Study. Mechanical ventilation guided by esophageal pressure in acute lung injury. N Engl J Med 2008; 359:2095– 2104 [MEDLINE]
Accuracy of plateau pressure and stress index to identify injurious ventilation in patients with acute respiratory distress syndrome. Anesthesiology. 2013 Oct;119(4):880-9. doi: 10.1097/ALN.0b013e3182a05bb8 [MEDLINE]
The application of esophageal pressure measurement in patients with respiratory failure. Am J Respir Crit Care Med 2014; 189:520–531 [MEDLINE]
The assessment of transpulmonary pressure in mechanically ventilated ARDS patients. Intensive Care Med 2014; 40:1670–1678 [MEDLINE]