Endotracheal Intubation with Invasive Mechanical Ventilation
Advantages
Presence of Endotracheal Tube Allows Protection of Upper Airway and Access to Lower Airways (Via Bronchoscopy, etc) to Facilitate Sampling and Clearance)
Disadvantages
Less Physiologic, as Compared to Normal Respiratory Physiologic Function
Requires Close Monitoring of Pressure and Volume Being Utilized to Avoid Lung Injury
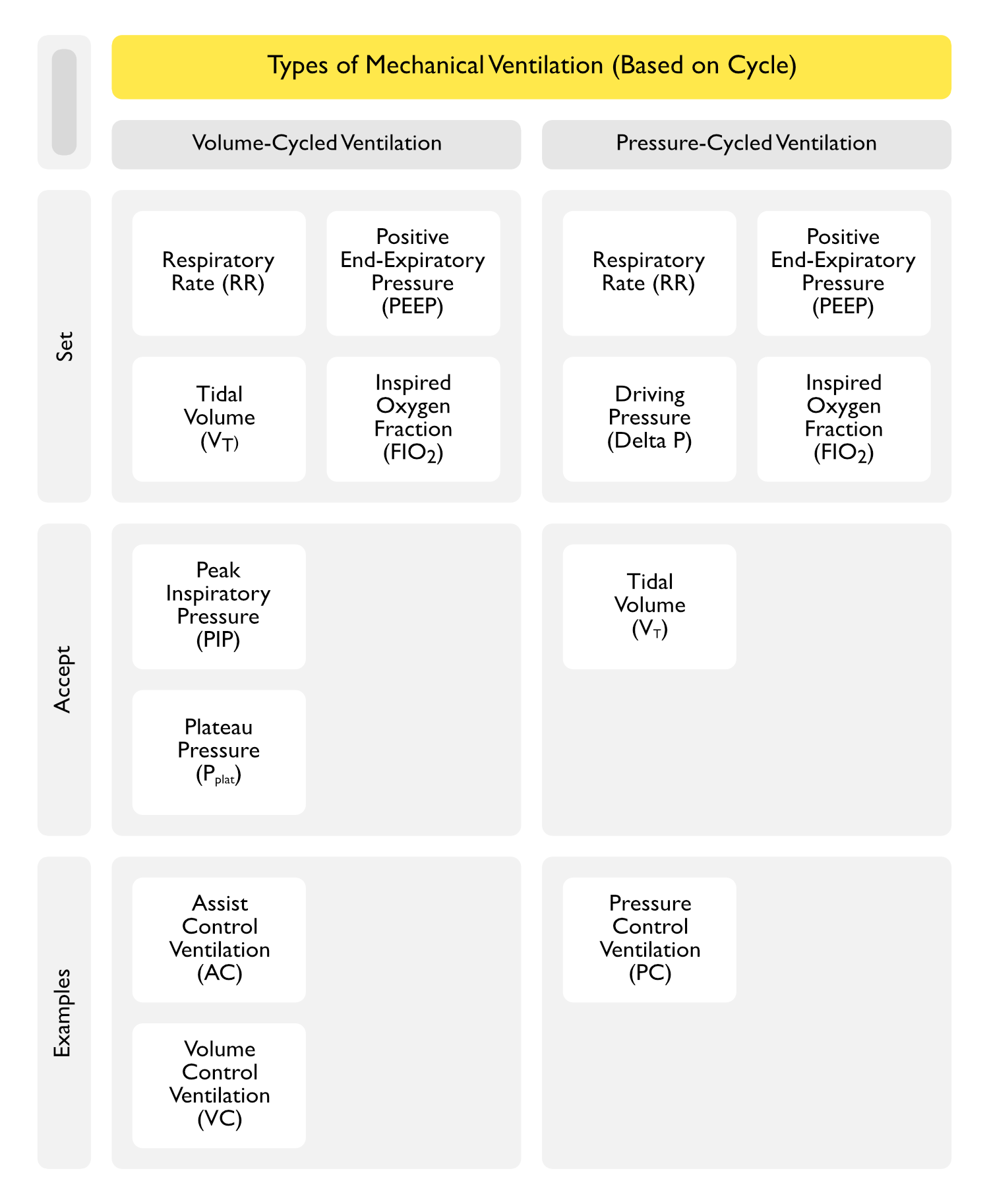
Volume-Cycled vs Pressure-Cycled Ventilation
Volume-Cycled Ventilation
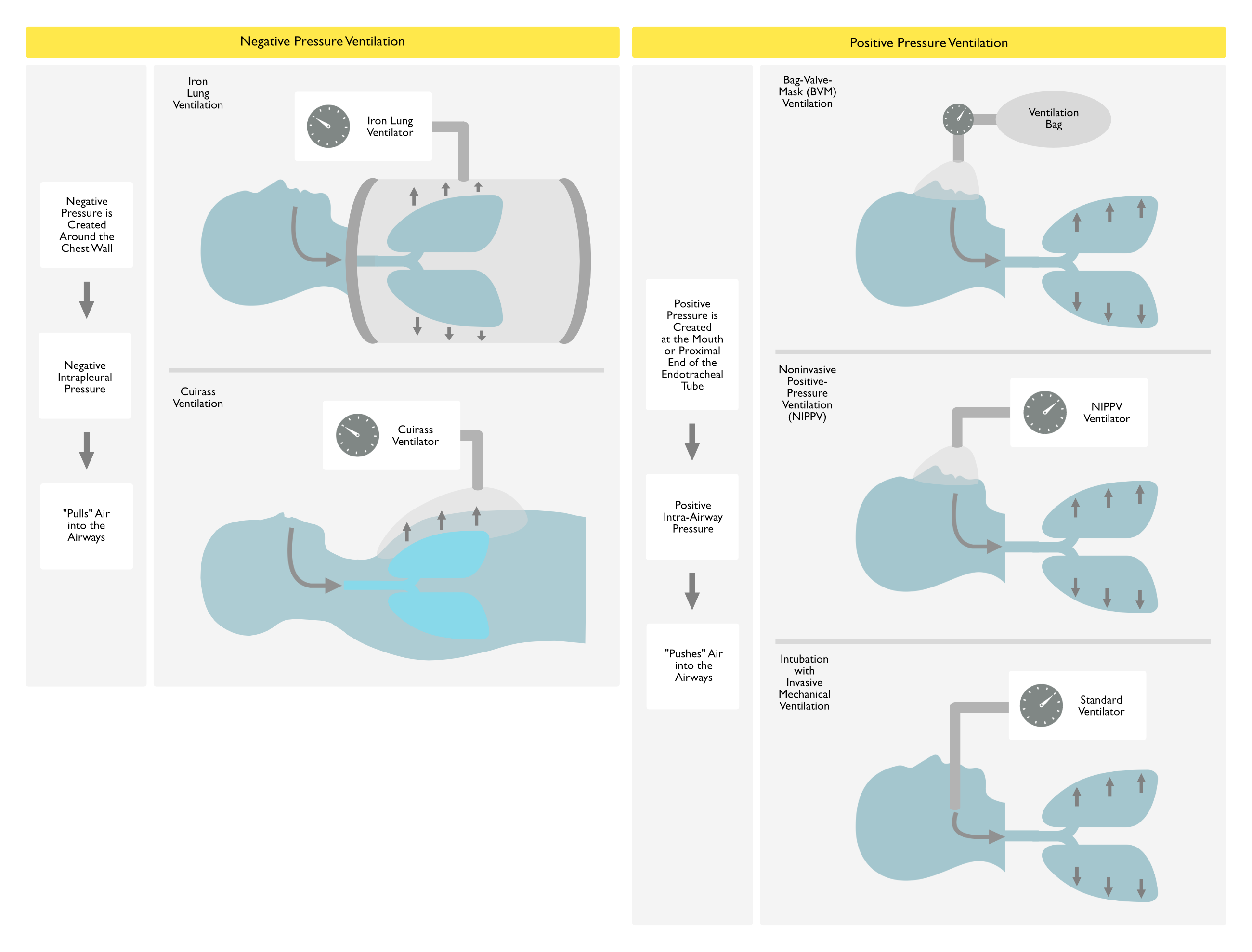
Mechanism of Delivery: delivers a pre-determined volume (VT) at a set inspiratory flow rate and respiratory rate (RR), allowing exhalation when volume is reached (resultingly, airway pressure is determined by lung mechanics or patient effort)
Advantages
Providers are More Familiar with Volume-Cycled Ventilator Modes, Facilitating Troubleshooting
Decreased Lung Compliance (Pneumothorax, etc) During Volume-Cycled Ventilation Results in Easily Recognizable Increase in Peak Inspiratory Pressure (PIP)
Disadvantages
Inappropriately Large Tidal Volume (VT) May Result in High Peak Inspiratory Pressure (PIP) and Increased Plateau Pressure (Pplat), the Latter of Which is Most Associated with an Increased Risk of Barotrauma)
Mechanism of Delivery: delivers a pre-determined pressure (resultingly, VT is determined by lung mechanics or patient effort)
Advantages
Increased Patient Comfort
Disadvantages
Providers are Less Familiar with Volume-Cycled Ventilator Modes, Complicating Troubleshooting
Decreased Lung Compliance (Pneumothorax, etc) During Pressure-Cycled Ventilation Results in a Less Recognizable Decrease in Tidal Volume (VT)
Examples of Pressure-Cycled Ventilation Modes
Pressure-Control (PC)
Pressure Support (PS)
Clinical Efficacy: data suggest no significant differences in work of breathing, mortality rate, or oxygenation between volume-cycled vs pressure-cycled ventilation
Randomized Trial of Volume-Cycled vs Pressure-Cycled Ventilation in Severe Respiratory Failure (Crit Care Med, 1994) [MEDLINE]
Early Initiation of Pressure-Limited Ventilation was Associated with Lower Peak Airway Pressure and More Rapid Clinical Improvement in Static Thoracic Compliance than Volume-Cycled Ventilation
Prospective, Observational Study of Pressure-Cycled vs Volume-Cycled Ventilation in ARDS (Chest, 2002) [MEDLINE]
Pressure Control Ventilation Generated Lower Peak Pressures and May Have Homogenized Gas Distribution and Avoided Regional Overdistention
Trial of Pressure-Cycled vs Volume-Cycled Ventilation in Acute Respiratory Failure (Eur Respir J, 2002) [MEDLINE]
No Difference in Work of Breathing and Gas Exchange (at a Fixed Tidal Volume and Peak Inspiratory Flow)
Variables Involved in Positive-Pressure Ventilation
Trigger (What Initiates the Breath)
Patient Effort (Detected as Either a Pressure or Flow Change): this is the trigger for patient-initiated breaths
Set Machine Timer at a Set Respiratory Rate: this is the trigger for ventilator-initiated breaths
Target (What Controls Gas Delivery During the Breath)
Set Flow Rate (Such as the Peak Inspiratory Flow Rate)
Set Inspiratory Pressure
Cycle (What Terminates the Breath)
Set Tidal Volume
Set Inspiratory Time
Set Flow Rate
Airway Pressure: may be used a backup safety cycle variable in some cases
Trigger
General Comments
Trigger Should Be Set to Allow the Patient to Easily Trigger the Initiation of a Breath (Anesthesiology, 1988) [MEDLINE]
Pressure Triggering: patient attempting to initiate a breath results in a negative airway pressure with sensing by the demand valve
Trigger Sensitivity is Typically Set at -1 to -3 cm H2O): ventilator-assisted breaths will be initiated when the alveolar pressure decreases to 1-3 cm H2O below atmospheric pressure
Pressure Triggering May Be Used in AC and SIMV Modes
Problems with Pressure Triggering
Trigger Sensitivity Set Too High (i.e -1 cm H2O) May Result in the Inappropriate Triggering in Response to Cardiac Oscillations, Patient Movement, Water Moving in the Ventilator Tubing, etc
Trigger Sensitivity Set Too Low (i.e. -4 cm H2O) May Result in Increased Work of Breathing or a Delay for the Patient to Trigger a Breath (and Therefore, Dyssynchrony)
Presence of Auto-PEEP Impairs Pressure Triggering (and Therefore, Can Produce Dyssynchrony), Since the Patient Needs to First Overcome the Positive End-Expiratory Pressure to Trigger the Breath
Flow Triggering: uses monitoring of a continuous flow of gas through the ventilator circuit, such that when the patient attempts to initiate a breath with generation of negative airflow, the ventilator breath is initiated when the return flow is less than the delivered flow
Trigger Sensitivity is Typically set at 2L/min
Flow Triggering May Be Used in CPAP, PS, AC, and SIMV Modes
Flow Triggering
Flow Triggering Decreases Work of Breathing in CPAP and During Spontaneous Breaths in SIMV (Crit Care Med, 1989) [MEDLINE] (Crit Care Med, 1994) [MEDLINE] (Am J Respir Crit Care Med, 1995) [MEDLINE] (Crit Care Med, 2000) [MEDLINE]
Flow Triggering Decreases Work of Breathing During IMV (Crit Care Med, 1994) [MEDLINE]
Flow Triggering Decreases Work of Breathing During PS (Am J Respir Crit Care Med, 1998) [MEDLINE]
Flow Triggering Does Not Decrease the Work of Breathing During AC (Am J Respir Crit Care Med, 1998) [MEDLINE]
Tidal Volume
Clinical Efficacy-Tidal Volume Setting in Patients without Acute Respiratory Distress Syndrome (ARDS)
Randomized IMPROVE Trial Examining Intraoperative Low Tidal Volume Ventilation in Patients Undergoing Major Abdominal Surgery (NEJM, 2013) [MEDLINE]
Intraoperative Low Tidal Volume Ventilation (6-8 mL/kg PBW, PEEP 6-8 cm H2O, Recruitment Maneuvers q30 min) was Associated with Decreased Adverse Pulmonary/Extrapulmonary Events, Decreased Need for Mechanical Ventilation and Decreased Hospital Length of Stay in Intermediate and High-Risk Patients Undergoing Major Abdominal Surgery
Lung Protective Strategy Did Not Decrease the Development of ARDS or Impact the Mortality Rate
Meta-Analysis of Low Tidal Volume Ventilation in Non-ARDS Patients (JAMA, 2012) [MEDLINE]: n= 2,822 (20 studies)
Low Tidal Volume Ventilation Decreased the Development of Lung Injury and Decreased the Mortality Rate
Systematic Review of Low Tidal Volume Ventilation in Non-ARDS Patients (Crit Care Med, 2015) [MEDLINE]
Meta-Analysis of Low Tidal Volume Ventilation in Patients without ARDS (Intensive Care Med, 2014) [MEDLINE]
Use of Lower Tidal Volumes in Patients without ARDS at the Onset of Mechanical Ventilation Could Be Associated with a Shorter Duration of Ventilation
Use of Lower Tidal Volumes Seems No to Affect Sedation or Analgesia Needs, But This Must Be Confirmed in a Robust, Well-Powered Randomized Controlled Trial
Meta-Analysis of Efficacy of Intraoperative Low Tidal Volume Ventilation in Preventing Postoperative Pulmonary Complications (Ann Surg, 2016) [MEDLINE]: n = 1054 (16 studies)
Intraoperative Low Tidal Volume Ventilation in Conjunction with PEEP and Recruitment Maneuvers Improved Clinical Pulmonary Outcomes (Atelectasis, Lung Infection, Acute Lung Injury) and Decreased Hospital Length of Stay in Otherwise Healthy Patients Undergoing General Surgery
PReVENT Trial Comparing Low (7 mL/kg PBW) vs Intermediate (9 mL/kg PBW) Tidal Volume Ventilation in ICU Patients at Risk for ARDS (JAMA, 2018) [MEDLINE]: n = 961 (6 centers)
Study Design
Randomized Patients Not Expected to Be Extubated within 24 hrs (Majority were Randomized within 1 hr of Start of Mechanical Ventilation)
Low Tidal Volume Group Used Higher Tidal Volume (7 mL/kg PBW) than in Other Similar Studies (Which Generally Used 6 mL/kg PBW), Because Pressure Support was Used More Frequently in this Group
By Day 1, 58% of Patients in the Low Tidal Volume Group were Receiving Pressure Support Ventilation (Which Allowed Large Spontaneous Tidal Volumes if the Patients were on Minimal Ventilatory Support)
On Day 1, 59% of Patient in the Low Tidal Volume Group Received a Tidal Volume >6 mL/kg PBW and 14% of Patients Received a Tidal Volume >9.5 mL/kg PBW
On Days 1 and 2, Respectively, Estimates Suggest that Only 25% of Patients in the Intermediate Tidal Volume Group Received Tidal Volumes >10 mL/kg PBW
In ICU Patients without ARDS, There was No Difference Between Low Tidal Volume Ventilation Strategy (7 mL/kg PBW) and Intermediate Tidal Volume Ventilation Strategy (9 mL/kg PBW), in Terms of Ventilator-Free Days at Day 28
In ICU Patients without ARDS, There was No Difference Between Low Tidal Volume Ventilation Strategy (7 mL/kg PBW) and Intermediate Tidal Volume Ventilation Strategy (9 mL/kg PBW), in Terms of ICU Length of Stay, Hospital Length of Stay, 90-Day Mortality, Incidence of ARDS, Incidence of Pneumonia, Incidence of Severe Atelectasis, and Incidence of Pneumothorax
Possible Explanations for Lack of Effect of the Low Tidal Volume Ventilation Strategy
The Low Tidal Volume Ventilation Strategy was Associated with Respiratory Acidosis, Which Might Have Influenced the Duration of Ventilation
Driving Pressure in the Intermediate Volume Ventilation Strategy was Still within a Protective Range for Patients without ARDS
Critique
Some Experts Have Suggested that the PReVENT Trial Demonstrates that a Negative Trial May Be the Result of Inadequate Separation Between Interventions
Spanish Randomized iPROVE Trial of Multiple Ventilation Strategies in Patients Undergoing Abdominal Surgery (Lancet Respir Med, 2018) [MEDLINE]: n = 1,012
Strategies: individualized intraoperative ventilation with individualized PEEP after a lung recruitment maneuver plus individualized postoperative CPAP, individualized intraoperative ventilation plus postoperative CPAP, and standard intraoperative ventilation plus postoperative CPAP, or standard intraoperative ventilation plus standard postoperative oxygen therapy
Ventilation Strategy Did Not Impact the Postoperative Complication Rate
Recommendations-Tidal Volume Setting in Patients without Acute Respiratory Distress Syndrome (ARDS)
Lung-Protective Ventilation Strategy with Low Tidal Volume Ventilation (6-8 mL/kg PBW) and Low Plateau Pressure (<30 cm H2O) is Probably Recommended
Clinical Efficacy-Tidal Volume Setting in Patients with Acute Respiratory Distress Syndrome (ARDS) (see Acute Respiratory Distress Syndrome)
The Acute Respiratory Distress Syndrome Network (ARDSNet) Multicenter Randomized Trial Comparing High Tidal Volume (12 mL/kg PBW and Plateau Pressure <50 cm H2O) with Low Tidal Volume (6 mL/kg PBW and Plateau Pressure <30 cm H2O) Ventilation (NEJM, 2000) [MEDLINE]: n = 861
Trial was Stopped Prematurely Due to Mortality Benefit and Increased Ventilator-Free Days in Low Tidal Volume Ventilation Group
Low Tidal Volume Group Had Decreased Mortality Rate (31%), as Compared to High Tidal Volume Group (39.8%)
However, Tidal Volumes Between 6 and 12 mL/g PBW were Not Studied
Low Tidal Volume Group Had Increased Ventilator-Free Days During the First 28 Days (12 +/- 11), as Compared to the High Tidal Volume Group (10 +/- 11)
Mean Tidal Volumes Achieved on Days 1-3 in Low Tidal Volume Group were Lower (6.2 +/- 0.8 mL/kg PBW), as Compared to High Tidal Volume Group (11.8 +/- 0.8 mL/kg PBW)
Mean Plateau Pressures Achieved in Low Tidal Volume Group were Lower (25 +/- 6 cm H2O), as Compared to High Tidal Volume Group (33 +/- 8 cm H2O)
Arterial pCO2 was 4-7 mm Hg Higher in Low Tidal Volume Group, But pCO2 Never Exceeded 44 mm Hg: this is likely not clinically significant
FIO2 was Higher in the Low Tidal Volume Group on Days 1 and 3, Becoming Equivalent by Day 7: this suggests that the institution of low tidal volumes resulted in a transient worsening of oxygenation
Auto-PEEP was Higher in the Low Tidal Volume Group (Who Had Higher Respiratory Rates), Although the Difference in Median Auto-PEEP was <1 cm H2O: this is likely not clinically significant (Crit Care Med, 2005) [MEDLINE]
Review of Animal/Human Data from ARDS Clinical Trials Network (and Original Data) Examining if There is a Safe Upper Limit of Plateau Pressure in ARDS (Am J Respir Crit Care Med, 2005)
Authors Could Not Identify a Safe Upper Limit for Plateau Pressure in ARDS
Study of Sedative Use During Low Tidal Volume Ventilation (Crit Care Med, 2005) [MEDLINE]
Low Tidal Volume Ventilation Does Not Result in Increased Use of Sedatives, Opiates, or Paralytics
Meta-Analysis of Low Tidal Volume and Limited Airway Pressure or Higher PEEP in ALI/ARDS (Ann Intern Med, 2009) [MEDLINE]
Decreased Mortality with Routine Use of Low Tidal Volume, But Not High PEEP Ventilation, in Unselected Patients with ARDS or Acute Lung Injury
High PEEP May Help to Prevent Life-Threatening Hypoxemia in Selected Patients
Systematic Review of Pressure/Volume-Limited Strategies (PLoS One, 2011) [MEDLINE]: the ARDS Network trial [MEDLINE] contributed 21.4% of the weight toward the summary estimate of effect in this analysis
Pressure/Volume-Limited Strategies Decrease Mortality Rate and are Associated with Increased Use of Paralytics
Cochrane Database Review of Lung Protective Ventilation Strategies in ARDS (Cochrane Database Syst Rev, 2013) [MEDLINE]
Lung Protective Strategies (Low Tidal Volume or Plateau Pressure <30 cm H2O) Decrease Mortality
Trial Examining Predictors of Ventilator-Induced Lung Injury in ARDS (Anesthesiology, 2013) [MEDLINE]
Rationale: stress index describes the shape of the airway pressure-time curve profile and may indicate tidal recruitment or tidal overdistension (convex downward pressure curve indicates initial low compliance with better compliance later in the breath due to recruitment, while convex upward curve indicates overdistention -> optimal curve is straight diagonal initial pressure waveform)
Plateau Pressure Partitioned to the Respiratory System (Pplat,Rs) >25 cm H20 and Stress Index Partitioned to the Respiratory System (SI,Rs) >1.05 were Most Associated with Injurious Ventilation
Systematic Review/Meta-Analysis of Morbidity/Mortality in Post-Operative Acute Lung Injury (Lancet Respir Med, 2014) [MEDLINE]
Lung Protective Mechanical Ventilation Strategies (Applied During Surgery) Decrease the Incidence of Post-Operative Acute Lung Injury, But Do Not Decrease the Mortality Rate
Study of Contribution of Driving Pressure to Mortality in ARDS (NEJM, 2015) [MEDLINE]: study used data from 9 prior randomized trials
Rationale: lower tidal volume, lower plateau pressure, and higher PEEP are all believed to decrease mechanical stresses on the lung in ARDS (which can induce ventilator-associated lung injury)
However, There is an Uncertainty When Optimizing One Component Adversely Affects Another (Example: Increasing PEEP May Undesirably Increase the Plateau Pressure), Which this Study Attempted to Address
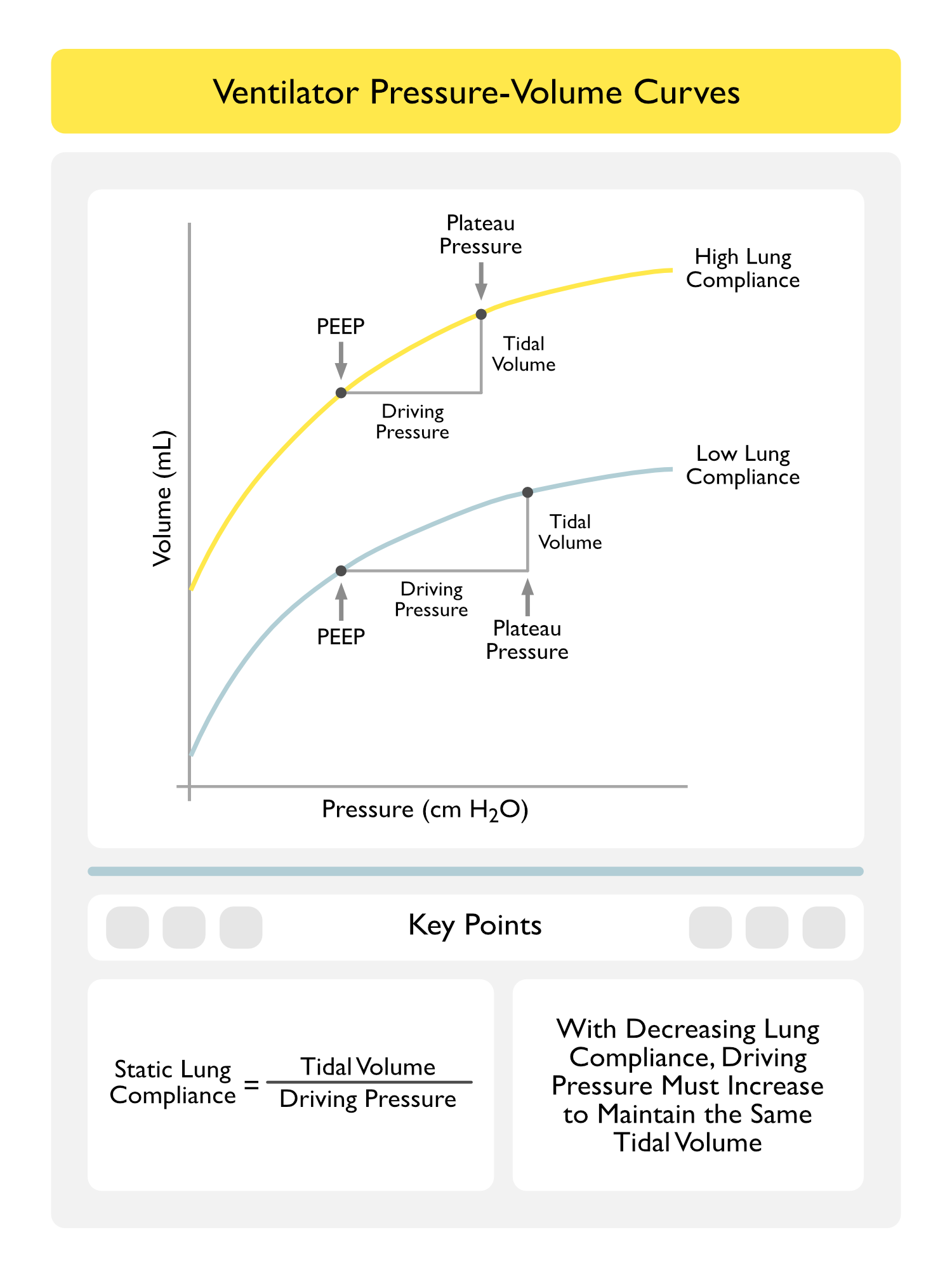
Authors Theorized in Their Study that Optimizing the Tidal Volume/Respiratory System Compliance Ratio (Known as the Driving Pressure = Delta P) Would Provide a Better Predictor of Outcome in ARDS
Driving Pressure (Plateau Pressure – PEEP or Delta P) was the Best Predictor of Survival
Decreases in Tidal Volume or Increases in PEEP Were Beneficial Only if They Resulted in a Decrease in Delta P (In Other Words, PEEP Increments are Protective Only When They are Associated with an Improvement in Respiratory System Compliance, So that the Same Tidal Volume Can Be Delivered with a Lower Delta P)
Further Trials Using Specific Manipulation of Delta P are Required Before Recommending this Strategy as a Standard
Caveat: Delta P Can Only Be Accurately Assessed in Non-Breathing Patients
Recommendations-Tidal Volume Setting in Patients with Acute Respiratory Distress Syndrome (ARDS) (American Thoracic Society/European Society of Intensive Care Medicine/Society of Critical Care Medicine Clinical Practice Guidelines for Mechanical Ventilation in ARDS) (Am J Respir Crit Care Med, 2017) [MEDLINE]
Lung-Protective Ventilation Strategy with Low Tidal Volume Ventilation (4-8 mL/kg PBW) and Low Plateau Pressure (<30 cm H2O) is Recommended (Strong Recommendation, Moderate Confidence)
Predicted Body Weight (PBW)
Male: PBW = 50 + 2.3 (ht in inches – 60)
Female: PBW = 45.5 + 2.3 (ht in inches – 60)
Maintaining the Plateau Pressure (Pplat) <35 cm H2O Decreases the Risk of Barotrauma (Since Plateau Pressure is the Best Clinical Estimate of Mean Alveolar Pressure)
Driving Pressure = Plateau Pressure – PEEP
In Some Cases of ARDS, Low Tidal Volume Ventilation May Require the Use of Permissive Hypercapnia (Which Occurs Due to an Increase in the Relative Amount of Dead Space)
Recommendations-Tidal Volume Setting in Patients with Acute Respiratory Distress Syndrome (ARDS) Associated with Sepsis (2016 Surviving Sepsis Guidelines; Intensive Care Med, 2017) [MEDLINE]
Low Tidal Volume (6 mL/kg PBW) is Recommended Over High Tidal Volume (12 mL/kg PBW) in Sepsis-Associated ARDS (Strong Recommendation, High Quality of Evidence)
Low Tidal Volume (6 mL/kg PBW) is Recommended Over High Tidal Volume (12 mL/kg PBW) in Sepsis-Associated Respiratory Failure without ARDS (Weak Recommendation, Low Quality of Evidence)
Plateau Pressure Upper Limit of 30 cm H2O is Recommended in Sepsis-Associated Severe ARDS (Strong Recommendation, Moderate Quality of Evidence)
Respiratory Rate Max Should Be 35 Breaths/min (Recognizing that Some Patients May Experience Hypercapnia)
Hypercapnia is Generally Well-Tolerated in the Absence of Contraindications (Such as Increased Intracranial Pressure, Sickle Cell Crisis, etc)
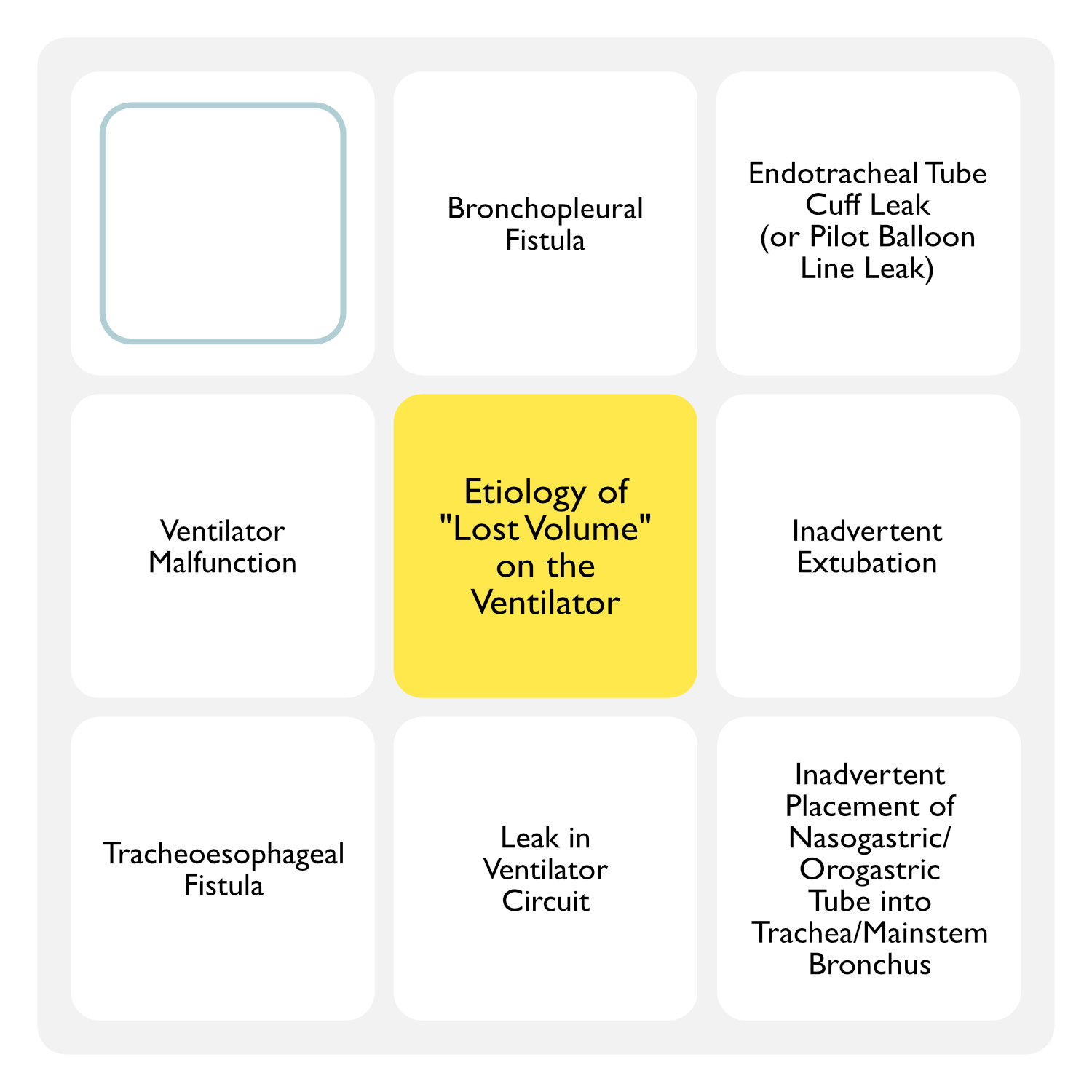
“Lost Volume” on Ventilator
Lost Volume is a Disparity Between the Inspiratory Tidal and Expiratory Tidal Volume (i.e. Expiratory Tidal Volume < Inspiratory Tidal Volume)
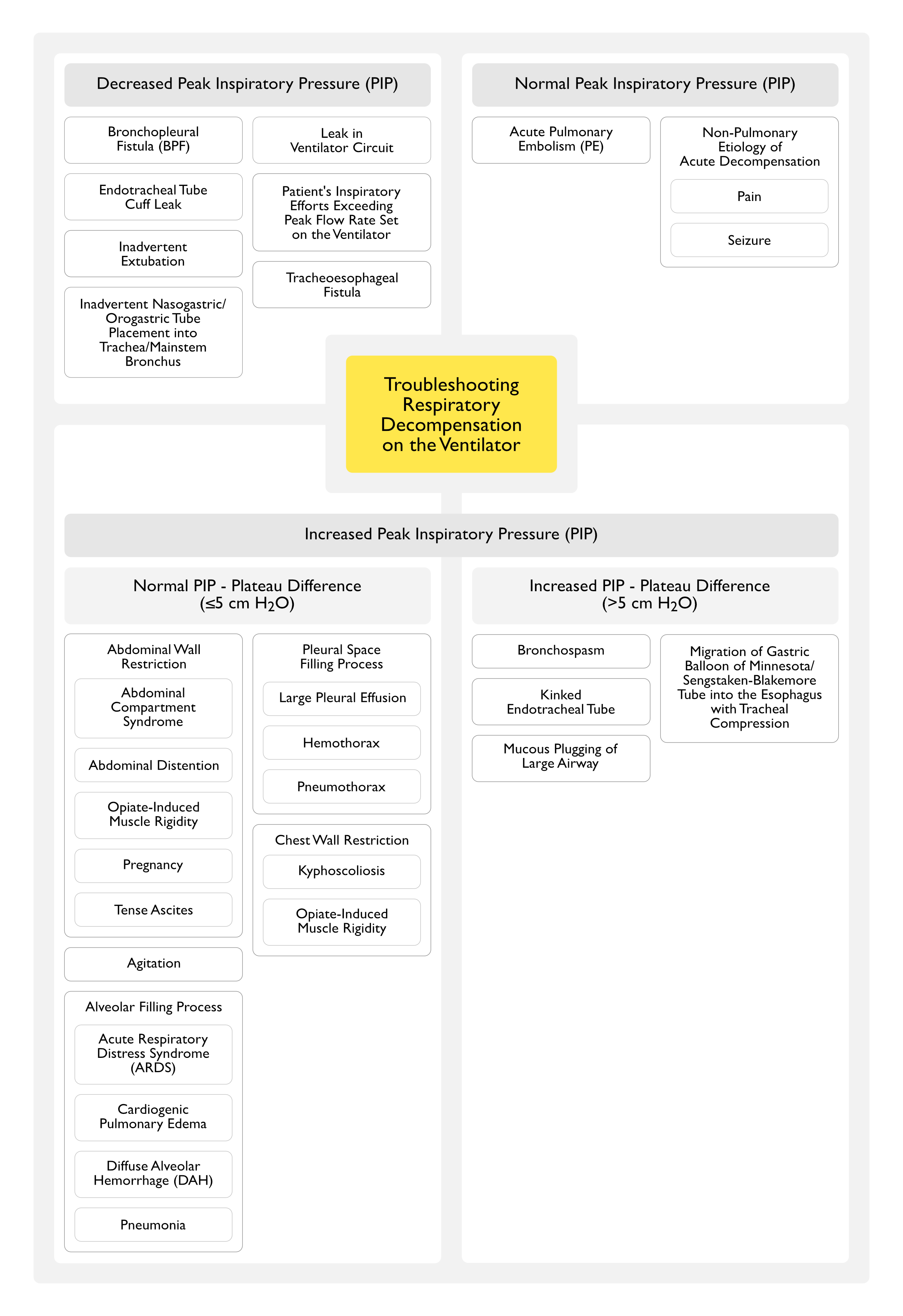
Air Leak Around the Endotracheal Tube Cuff is Frequently Audible or Manifested by Secretions Bubbling Out from the Patient’s Mouth During Exhalation
Inadvertent Extubation
May Occur After Patient Turning or Repositioning
May Be Accompanied by Respiratory Distress or Precipitous Oxygen Desaturation
Inadvertent Nasogastric (NG)/Orogastric (OG) Tube Placement into the Trachea/Mainstem Bronchus (with Suction Applied) (see Nasogastric/Orogastric Tube)
Diagnosis Can Be Made by Chest X-Ray or Bronchoscopy, Demonstrating Nasogastric/Orogastric Tube in the Trachea/Mainstem Bronchus
Leak in Ventilator Circuit
Due to a Loose Connection or Fractured Ventilator Tubing
Ventilator Malfunction
Respiratory Rate (RR)
Respiratory Rate Should Be Adjusted to Maintain Appropriate pCO2 and pH
Respiratory Rate Should Be Set to Allow an Adequate Minute Ventilation, Should the Patient Become Apneic
In ARDS, the Maximum Respiratory Rate Should Be ≤35 Breaths/min
When Increasing the Respiratory Rate in Some Modes of Ventilation, Inspiratory Flow Rate Can Be Increased to Maintain the I/E Ratio: to prevent the development of auto-PEEP
When Increasing the Respiratory Rate, the Patient Should Be Monitored for the Development of Auto-PEEP
High Respiratory Rates in Patients Mechanically-Ventilated for Acute Respiratory Failure Can Produce Dynamic Hyperinflation (with Development of Auto-PEEP), Increase the Dead Space/Tidal Volume Ratio, and Impair Right Ventricular Ejection with a Decrease in the Cardiac Output (Crit Care Med, 2002) [MEDLINE]: n = 14
In a Patient Who Develops Auto-PEEP on a Respiratory Rate Which Achieves a Normal pH, Respiratory Rate Can Be Decreased and “Permissive Hypercapnia” Utilized
Minute Ventilation (VE)
PhysiologicDefinition
VE = VA + VD
Minute Ventilation (VE): expressed in L/min
Alveolar Ventilation (VA): expressed in L/min
Dead Space Ventilation (VD): expressed in L/min
Not on the Ventilator: VD is equivalent to approximately 1/3 of resting tidal volume (or approximately 2.2 ml/kg)
On the Ventilator with Lung Pathology: VD/VT ratio is variable
Clinical Definition
VE = RR x VT
Minute Ventilation (VE): expressed in L/min
Respiratory Rate (RR): expressed in breaths/min
Tidal Volume (VT): expressed in L/breath
Positive End-Expiratory Pressure (PEEP)
Definitions
Extrinsic PEEP: PEEP applied by the clinician
Auto-PEEP (Intrinsic PEEP): PEEP which develops due to intrinsic properties of the lungs and/or airways
Total PEEP = Extrinsic PEEP + Auto-PEEP
Physiology
Use of PEEP in Severe Asthma/COPD Exacerbation with Airway Obstruction
During Severe Asthma/COPD Exacerbation (with Airway Obstruction), the Airways Behave Like a Starling Resistor (Chest, 1989) [MEDLINE]
Ohmic Resistor (i.e. One Which Follows Ohm’s Law)
With an Ohmic Resistor, if Extrinsic PEEP is Decreased, the Peak Airway Pressure (PIP) Would Be Expected to Decrease by a Similar Amount: this is one would expect with normal lungs
Starling Resistor: flow rate in the airways is not dependent on the amount extrinsic PEEP applied
Example Using a “Waterfall” Analogy: the flow rate of a waterfall is not impacted by the level of the pool of water below (of course, until the pool of water rises to the level of the waterfall)
With a Starling Resistor, When Extrinsic PEEP is Decreased, the Peak Airway Pressure (PIP) Does Not Decrease by a Similar Amount: this is due to the fact that flow is determined by upstream events only
Beneficial Effects of Positive End-Expiratory Pressure (PEEP)
PEEP Decreases End-Expiratory Alveolar Derecruitment (Collapse), Rather than Increasing Alveolar Recruitment
End-Expiratory Alveolar Collapse Occurs in Intubated Patients Due to the Fact that the Endotracheal Tube Bypasses the Glottis
Derecruited Lung is Correlated with Intrapulmonary Shunt (Am J Respir Crit Care Med, 2017) [MEDLINE]
Improvement in Oxygenation with Increased PEEP Generally Reflects Lung Recruitment
However, Oxygenation is Also Influenced by Other Factors Which May Be Affected by PEEP (Cardiac Output, etc)
Decreased End-Expiratory Alveolar Derecruitment Can Mitigate Ventilator-Induced Lung Injury (VILI) (Am J Respir Crit Care Med, 2017) [MEDLINE]
In ARDS, a Combination of Physiologic Variables (pO2/FIO2 Ratio <150 at a PEEP 5 cm H2O, a Decrease in Dead Space, and an Increase in Respiratory System Compliance with an Increase in PEEP to 15 cm H2O) Predicted a Higher Percentage of Potentially Recruitable Lung (NEJM, 2006) [MEDLINE]
Quantification of the Amount of Recruitable Lung Can Be Achieved Using Chest Computed Tomography (CT), Helium Dilution/Nitrogen Washout Techniques, Electrical Impedance Tomography, or Construction of Airway Pressure-Volume Curves at Tidal Ventilation with Different Levels of PEEP (Am J Respir Crit Care Med, 2017) [MEDLINE]
Estimates of Recruitability from Helium Dilution and Pressure–Volume Curves are Strongly Correlated with Each Other, But Both are Poorly Correlated with Estimates of Recruitability Obtained from Chest CT Scanning
This Discrepancy May Be Accounted for by the Fact that CT Measures the Opening of Previously Collapsed Lung Units, While the Helium Dilution and Pressure–Volume Curve Techniques Measure the Volume of Gas Entering Newly Recruited Lung Units Together with Previously Opened Lung Units
PEEP Decreases Intrapulmonary Shunting
PEEP is Transmitted to the Most Compliant Lung Regions and Therefore, is Most Useful for Diffuse Lung Processes (Multilobar Pneumonia, ARDS, Cardiogenic Pulmonary Edema, etc) and is Less Useful for Localized Lung Processes
In Patients with Focal Lung Disease (Pneumonia, etc), PEEP Compresses Alveolar Capillaries in the Uninvolved Regions of the Lung (Causing Dead Space with High V/Q Ratio in That Region), Diverting Blood Flow to the Injured Lung Region (Causing Low V/Q Ratio in That Region) (J Appl Physiol Respir Environ Exerc Physiol, 1982) [MEDLINE]
PEEP Improves Lung Compliance (Am J Respir Crit Care Med, 2017) [MEDLINE]
PEEP Increases the Number of Aerated Alveoli Participating in Tidal Ventilation, Decreasing Tidal Lung Stress and Strain (i.e. Improving Lung Compliance)
PEEP Decreases the Passage of Posterior Pharyngeal Secretions Around the Endotracheal Tube Cuff into the Lungs (Crit Care Med, 2008) [MEDLINE]
PEEP Promotes More Homogeneous Ventilation
PEEP Distributes Ventilation and Blood Flow Differently in the Supine vs Prone Position (Anesthesiology, 2010) [MEDLINE]
PEEP Might Be Less Effective and Worsen V/Q Mismatch During Prone Ventilation
PEEP Decreases Dynamic Airway Compression (Intensive Care Med, 1993) [MEDLINE]
At Lower Levels, PEEP Improves Cardiac Output (NEJM, 1975) [MEDLINE]
Adverse Effects of Positive End-Expiratory Pressure (PEEP)
At Higher Levels, PEEP Decreases Cardiac Output and May Result in Hypotension (Chest, 2005) [MEDLINE]
Mechanism: at higher levels, PEEP increases Intrathoracic pressure (and increasing right atrial pressure), decreasing to the right side of the heart, culminating in a decrease in cardiac output
Decreased Mixed Venous pO2
Decreased Arterial pO2
However, PEEP of 10-20 cm H2O Has Been Demonstrated to Be Well-Tolerated in Most ARDS Patients (Crit Care, 2004) [MEDLINE]
PEEP May Undesirably Cause Alveolar Overdistention
While PEEP is Generally Thought to Have Beneficial Effects When Used in ARDS, PEEP May Result in Predominant Alveolar Recruitment, Predominant Alveolar Overdistention, or a Combination of Both Recruitment and Overdistention
Consequently, PEEP Could Theoretically Increase Contribute to Ventilator-Induced Lung Injury with Overdistention Propagating Lung Inflammation and Injury (Similar to the Effects of Excessive Tidal Volume)
Lung Recruitability is a Critical Determinant Which Will Determine the Effect of PEEP on the Injured Lung and the Amount of Lung Which Can Be Recruited Varies Widely in Patients with ARDS (NEJM, 2006) [MEDLINE]
In Patients with High Lung Recruitability, Much of the Increase in End-Expiratory Lung Volume (EELV) with PEEP Results from Opening of Collapsed Lung Units, Decreasing Cyclic Lung Collapse/Reopening anf Decreasing Dynamic Strain in Aerated Lung Units (Due to an Increase in Aerated Lung Volume Available for Tidal Volume Distribution)
In Patients with Low Lung Recruitability, PEEP Results in Additional Distention of Already Aerated Lung Tissue, Possibly Causing Overdistention Injury
Personalized PEEP Titration, Based on Recruitability, Oxygenation Response After Increases in PEEP (a Marker Lung Recruitment) Predicted a Lower Mortality Rate in ARDS (Am J Respir Crit Care Med, 2014) [MEDLINE]
PEEP May Increase Pulmonary Vascular Resistance (PVR) by Narrowing or Occluding Alveolar Septal Vessels, Which are Surrounded by Alveolar Pressure (Even When Using Low Tidal Volumes) (Crit Care Med, 2010) [MEDLINE]
Consequently, Increased PVR Increases the Right Ventricular Afterload, Further Decreasing Cardiac Output
PEEP Can Worsen Alveolar Dead Space by Increasing the Volume of Lung in Which Alveolar Pressure Exceeds Pulmonary Capillary Pressure (NEJM, 1975) [MEDLINE]
PEEP Increases Peak Inspiratory Pressure (PIP)
The Addition of PEEP Will Generally Increase the PIP by an Equivalent Amount, Except in the Presence of Auto-PEEP
In Fact, the Failure of the PIP to Increase with Application of Extrinsic PEEP is Evidence for the Presence of Auto-PEEP
PEEP Can Increase the Plateau Pressure (Pplat)
PEEP Exacerbates Right-to-Left Shunting Through a Patent Foramen Ovale (PFO) (see Patent Foramen Ovale) (Ann Intern Med, 1993) [MEDLINE]
Mechanism: PEEP may decrease cerebral venous outflow
In Patients with Stroke, PEEP Did Not Increase the Intracranial Pressure (Stroke, 2001) [MEDLINE]
In Severe Traumatic Brain Injury, PEEP Did Not Decrease Cerebral Perfusion (J Trauma, 2002) [MEDLINE]
In Animal Studies and Patients with SAH, PEEP Did Not Directly Increase the Intracranial Pressure, But Did So Only by Inducing Hypotension (Crit Care Med, 2005) [MEDLINE]
Techniques/Strategies to Set the Optimum Amount of PEEP
FIO2/PEEP Table Strategy
The ARDSNet Trial Standardized FIO2/PEEP Table is the One Most Commonly Used [ARDSNet] (NEJM, 2000) [MEDLINE]
The ALVEOLI Trial Compared Low PEEP and High PEEP and Found that Oxygenation Improved in the Higher PEEP Group, Suggesting that There was Greater Recruitment with Higher PEEP (NEJM, 2004) [MEDLINE]
Oxygenation Responses Vary Widely Between Patients with ARDS
While PEEP is Generally Set at a Minimum of 5 cm H2O and Titrated up, the Optimal Level of PEEP in a Patient with ARDS May Depend on the Tidal Volume Being Used (Crit Care, 2018) [MEDLINE]
In a Comparative Study of 4 Bedside Methods to Optimize PEEP (FIO2/PEEP Table, Open Lung Strategy Limited by Plateau Pressure, Stress Index, and a Higher FIO2/PEEP Table), the ARDSNet PEEP/FIO2 Table was the Only Strategy Which Consistently Provided Higher PEEP Levels in Patients with Severe ARDS and Greater Recruitability, and Provided Lower PEEP Levels in Patients with Mild ARDS and Less Recruitability (Crit Care Med, 2014) [MEDLINE]
Conclusion
FIO2/PEEP Tables are Easy and Reasonable to Use, But They Do Not Necessarily Guarantee an Optimal PEEP Setting in an Individual Patient
Open Lung Strategy Used in the EXPRESS Trial with High PEEP Until Plateau Pressure Reached 28-30 cm H2O (Not Exceeding This Level to Avoid Overdistention) (JAMA, 2008) [MEDLINE]
However, This Technique Did Not Demonstrate a Mortality Benefit
Higher PEEP Group Had Higher Ventilator-Free Days and Higher Organ Failure–Free Days
Randomized Trial of Open Lung Approach in ARDS (Crit Care Med, 2016) [MEDLINE]
Open Lung Approach Improved Oxygenation and Driving Pressure, without Detrimental Effects on Mortality, Ventilator-Free Days, or Barotrauma
Conclusion
This Strategy Does Not Always Result in the Optimal PEEP for an Individual Patient
Strategy to Optimize Lung Compliance (NEJM, 1975) [MEDLINE]
Conclusion
Unclear Benefit of This Strategy
Driving Pressure-Targeted Strategy
In Meta-Analysis, Low Driving Pressure (Plateau Pressure – PEEP Difference) <13-15 cm H2O was Associated with Decreased Mortality Rate in ARDS (NEJM, 2015) [MEDLINE]
Conclusion
While Promising, This Strategy Needs Prospective Trials to Determine if it Indeed Improves the ARDS Mortality Rate
Strategy to Maintain PEEP to Keep Tidal Ventilation Above the Lower Inflection Point on the Static Pressure-Volume Curve of the Lung (Am J Respir Crit Care Med, 1999) [MEDLINE]
Note: this is the Static Curve, Not the Dynamic Curve Obtained During Mechanical Ventilation
This May reduce the Potential for Sheer Forces Exacerbating Lung Injury in ARDS
However, this Technique is Cumbersome (Requiring Deep Sedation and/or Neuromuscular Blockade) and Trials Do Not Indicate that it Has a Mortality Benefit
Strategy Using the Stress Index to Determine the Optimal Amount of PEEP
Stress Index is a Software-Derived Value Obtained During a Constant Flow Breath (to Determine the Pressure-Time Curve) in a Sedated Patient (i.e. with No Patient Effort) (Anesthesiology, 2013) [MEDLINE] (Respir Care, 2018) [MEDLINE]
Optimal Stress Index is a Straight Diagonal (i.e. 1.0) Reflecting Unchanging Compliance Throughout the Breath
If Recruitment/Derecruitment is Occurring During the Breath, the Stress Index Curve is Concave Bowing Upward (Low Compliance Early, Followed by High Compliance Later in the Breath) -> Stress Index <1
If Overdistention is Occurring During the Breath, the Stress Index Curve is Concave Bowing Downward (High Compliance Early, Followed by Low Compliance Later in the Breath) -> Stress Index >1
Strategy Using Transpulmonary Pressure
This Technique is Based on Fact that Airway Pressures are Not a Reliable Indicator of Lung Stress
Conditions Which Increase Chest Wall Elastance (Edema, Kyphoscoliosis, Abdominal Compartment Syndrome) or Shift the Pressure–Volume Curve of the Respiratory System or the Chest Wall to the Right (Obesity) Will Increase the Airway Pressure
Difficult to Measure in Clinical Practice (Requires Esophageal Manometry)
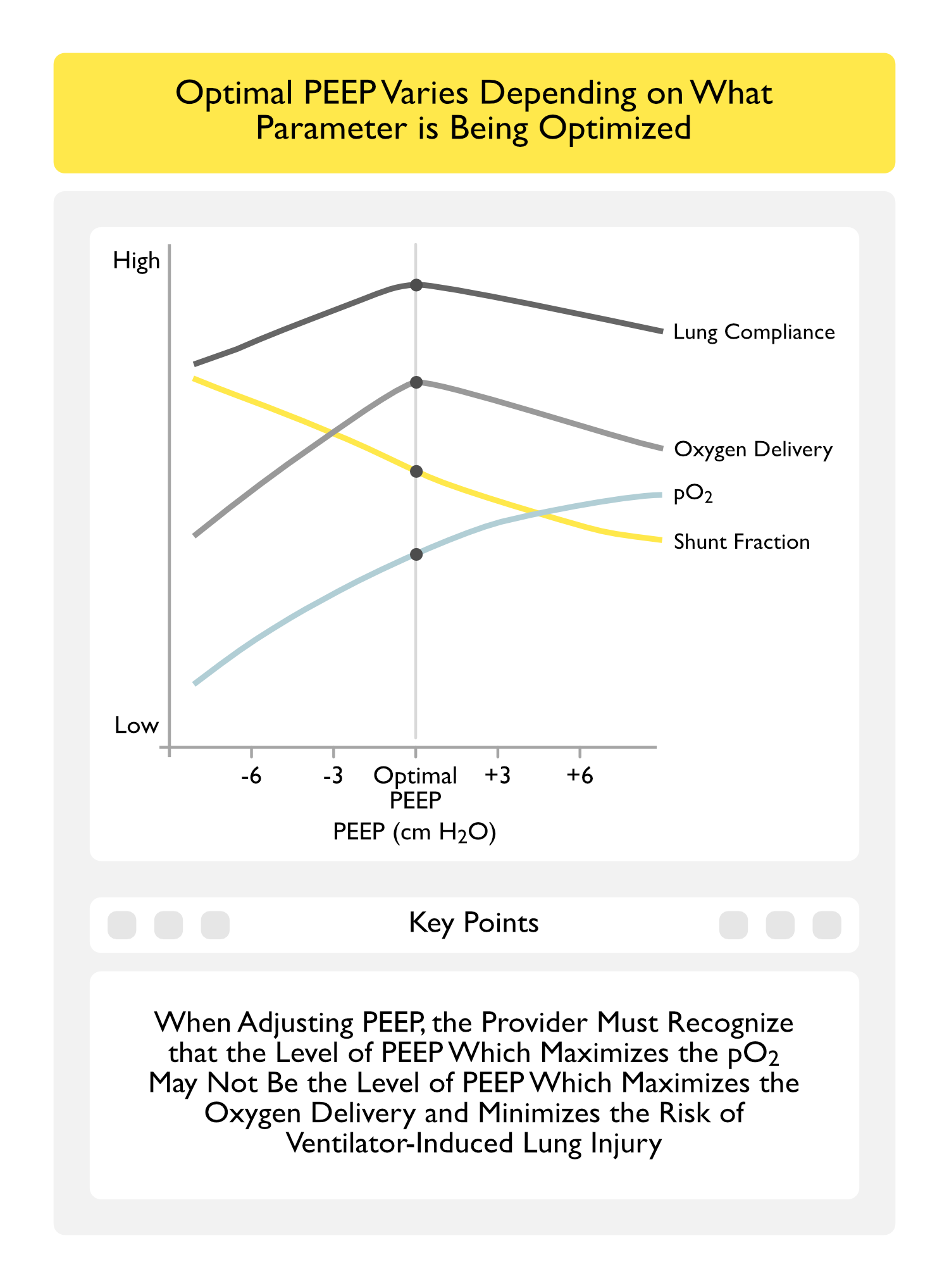
Strategy Using Oxygen Delivery to Determine the Optimal Amount of PEEP
The Level of PEEP Which Optimizes Oxygen Delivery May Not Correlate with the Level of PEEP Which Maximizes Arterial Oxygenation (Br J Anaesth, 2016) [MEDLINE]
Clinical Efficacy-Positive End-Expiratory Pressure (PEEP) in Patients without Acute Respiratory Distress Syndrome (ARDS)
Randomized IMPROVE Trial Examining Intraoperative Low Tidal Volume Ventilation in Patients Undergoing Major Abdominal Surgery (NEJM, 2013) [MEDLINE]
Intraoperative Low Tidal Volume Ventilation (6-8 mL/kg PBW, PEEP 6-8 cm H2O, Recruitment Maneuvers q30 min) was Associated with Decreased Adverse Pulmonary/Extrapulmonary Events, Decreased Need for Mechanical Ventilation and Decreased Hospital Length of Stay in Intermediate and High-Risk Patients Undergoing Major Abdominal Surgery
Lung Protective Strategy Did Not Decrease the Development of ARDS or Impact the Mortality Rate
Randomized PROVHILO Trial of PEEP During Abdominal Surgery (Lancet, 2014) [MEDLINE]
High PEEP (12 cm H20) and Recruitment Strategy During Abdominal Surgery Did Not Decrease Postoperative Pulmonary Complications, as Compared to Low PEEP Strategy (2 cm H2O)
High PEEP Group Required More Vasopressors to Treat Intraoperative Hypotension
Randomized Trial of PEEP in Patients Undergoing Elective Cardiac Surgery and Ventilated for Hypoxemia (JAMA, 2017) [MEDLINE]: n = 320
Alveolar Recruitment with PEEP Decreased Pulmonary Complications, ICU Length of Stay, and Decreased Mortality Rate without Increasing the Risk of Barotrauma
Spanish Randomized iPROVE Trial of Multiple Ventilation Strategiesin Patients Undergoing Abdominal Surgery (Lancet Respir Med, 2018) [MEDLINE]: n = 1,012
Strategies: individualized intraoperative ventilation with individualized PEEP after a lung recruitment maneuver plus individualized postoperative CPAP, individualized intraoperative ventilation plus postoperative CPAP, and standard intraoperative ventilation plus postoperative CPAP, or standard intraoperative ventilation plus standard postoperative oxygen therapy
Ventilation Strategy Did Not Impact the Postoperative Complication Rate
Conclusions
Overall
Optimal Level of PEEP in Mechanically-Ventilated Patients without ARDS is Unknown
Severe Airway Obstruction (Asthma/COPD Exacerbation, etc)
Use of Extrinsic PEEP in Patients with Auto-PEEP Should Not Exceed 50-80% of the Amount of Auto-PEEP
PEEP Does Not Appear to Have a Clinical Benefit Above that of Positive-Pressure Ventilation Alone in Patients with Cardiogenic Pulmonary Edema (Chest, 1998) [MEDLINE]
In Patients with ALI/ARDS Who Receive Low Tidal Volume Ventilation (6 ml/kg PBW) and Plateau Pressure Limit of 30 cm H2O, Lower or Higher PEEP Levels Had No Impact on Mortality Rate, ICU Length of Stay, Weaning from the Ventilator, Ventilator-Free Days, or Organ Failure-Free Days
Expiratory Pressure (EXPRESS) Study (JAMA, 2008) [MEDLINE]: French multicenter RCT (n = 767)
Setting PEEP Aimed at Increasing Alveolar Recruitment While Limiting Hyperinflation Had No Impact on Mortality Rate
However, it Improved Lung Function, Increased Ventilator-Free Days, and Decreased Non-Pulmonary Organ Failure-Free Days
Lung Open Ventilation (LOV) Study (JAMA, 2008) [MEDLINE]
Open Lung Ventilation Had No Impact on Mortality Rate
However, There was Decreased Need for Salvage Therapies and Lower Incidence of Refractory Hypoxemia
Systematic Review and Meta-Analysis of PEEP Levels in ARDS (JAMA, 2010) [MEDLINE]
Higher PEEP was Not Associated with Improved Hospital Survival, as Compared to Lower PEEP
However, in the Subset of ARDS Patients with pO2/FiO2 Ratio <200 mm Hg, PEEP Improved Survival
Trial Examining Predictors of Ventilator-Induced Lung Injury in ARDS (Anesthesiology, 2013) [MEDLINE]
Rationale: stress index describes the shape of the airway pressure-time curve profile and may indicate tidal recruitment or tidal overdistension (convex downward pressure curve indicates initial low compliance with better compliance later in the breath due to recruitment, while convex upward curve indicates overdistention -> optimal curve is straight diagonal initial pressure waveform)
Plateau Pressure Partitioned to the Respiratory System (Pplat,Rs) >25 cm H20 and Stress Index Partitioned to the Respiratory System (SI,Rs) >1.05 were Most Associated with Injurious Ventilation
Study of Contribution of Driving Pressure to Mortality in ARDS (NEJM, 2015) [MEDLINE]: study used data from 9 prior randomized trials
Rationale: lower tidal volume, lower plateau pressure, and higher PEEP are all believed to decrease mechanical stresses on the lung in ARDS (which can induce ventilator-associated lung injury)
However, There is an Uncertainty When Optimizing One Component Adversely Affects Another (Example: Increasing PEEP May Undesirably Increase the Plateau Pressure), Which this Study Attempted to Address
Authors Theorized in Their Study that Optimizing the Tidal Volume/Respiratory System Compliance Ratio (Known as the Driving Pressure = Delta P) Would Provide a Better Predictor of Outcome in ARDS
Driving Pressure (Plateau Pressure – PEEP or Delta P) was the Best Predictor of Survival
Decreases in Tidal Volume or Increases in PEEP Were Beneficial Only if They Resulted in a Decrease in Delta P (In Other Words, PEEP Increments are Protective Only When They are Associated with an Improvement in Respiratory System Compliance, So that the Same Tidal Volume Can Be Delivered with a Lower Delta P)
Further Trials Using Specific Manipulation of Delta P are Required Before Recommending this Strategy as a Standard
Caveat: Delta P Can Only Be Accurately Assessed in Non-Breathing Patients
Randomized Trial of Open Lung Approach in ARDS (Crit Care Med, 2016) [MEDLINE]: n = 200
Open Lung Approach Improved Oxygenation and Driving Pressure, without Detrimental Effects on Mortality, Ventilator-Free Days, or Barotrauma
Study of Driving Pressure and Lung Stress in ARDS (Crit Care, 2016) [MEDLINE]
The Applied Tidal Volume (mL/kg of Ideal Body Weight) was Not Related to Lung Gas Volume (r2 = 0.0005; p = 0.772)
At Both PEEP Levels, the higher Airway Driving Pressure Group Had a Significantly Higher Lung Stress, Respiratory System and Lung Elastance, as Compared to the Lower Airway Driving Pressure Group
Airway Driving Pressure was Significantly Related to Lung Stress (at PEEP +5, r2 = 0.581; p < 0.0001/at PEEP +15, r2 = 0.353; p < 0.0001)
For a Lung Stress of 24 and 26 cmH2O, the Optimal Cutoff Values for the Airway Driving Pressure were 15.0 cm H2O (ROC AUC 0.85, 95 % CI: 0.782-0.922) and 16.7 (ROC AUC 0.84, 95 % CI: 0.742-0.936)
Systematic Review and Meta-Analysis of Driving Pressure and Mortality Rate in ARDS (Crit Care Med, 2018) [MEDLINE]: n = 6,062 (7 studies)
Median (Interquartile Range) Driving Pressure Between Higher and Lower Driving Pressure Groups was 15 cm H2O (14-16 cm H2O)
Higher Driving pressure was Associated with a Significantly Higher Mortality Rate (Pooled Risk Ratio 1.44; 95% CI: 1.11-1.88; I = 85%)
Sensitivity Analysis Restricted to the Three Studies with Similar Driving Pressure Cutoffs (13-15 cm H2O) Demonstrated Similar Results (Pooled Risk Ratio, 1.28; 95% CI: 1.14-1.43; I = 0%)
Optimal PEEP (as Determined by Stress Index on the Ventilator) Depended on Tidal Volume
Phase 2 Randomized EPVent-2 Trial Evaluating Esophageal Pressure-Guided Positive End-Expiratory Pressure (PEEP) Titration Strategy in ARDS (JAMA, 2019) [MEDLINE]: n = 200 (14 hospitals in North America)
In Moderate-Severe ARDS (with Standard Low Tidal Volume Ventilation), Esophageal Pressure-Guided PEEP Titration Strategy Did Not Improve Mortality Rate or Ventilator-Free Days, as Compared to a Standard Empirical FIO2/PEEP Strategy
General Recommendations for Patients with Acute Respiratory Distress Syndrome (ARDS)
PEEP of 0 cm H2O is Generally is Accepted to Be Harmful in ARDS
PEEP of 8-15 cm H2O is Appropriate in Most Patients with ARDS: although higher PEEP levels might be used in patients for whom a greater potential for recruitment can be demonstrated
Although Further Trials are Required Before This Strategy Can Be Recommended, Increasing PEEP May Only Be Beneficial if it Results in a Decrease in the Delta P (Plateau Pressure – PEEP)
Recommendations for Patients with Acute Respiratory Distress Syndrome (ARDS) (American Thoracic Society/European Society of Intensive Care Medicine/Society of Critical Care Medicine Clinical Practice Guidelines for Mechanical Ventilation in ARDS) (Am J Respir Crit Care Med, 2017) [MEDLINE]
Higher PEEP (Rather Than Lower PEEP) is Recommended in Adults with Moderate-Severe ARDS (Conditional Recommendation, Moderate Confidence)
Recommendations for Patients with Acute Respiratory Distress Syndrome (ARDS) Associated with Sepsis (2016 Surviving Sepsis Guidelines; Intensive Care Med, 2017) [MEDLINE]
Higher PEEP is Recommended Over Lower PEEP in Adults with Sepsis-Associated Moderate-Severe ARDS (Weak Recommendation, Moderate Quality of Evidence)
The Optimal Method for Selecting PEEP is Unclear
Potential Methods Include Titrating PEEP Upward on a Tidal Volume of 6 mL/kg Until the Plateau Pressure is 28 cm H20, Titrating PEEP to Optimize Thoracoabdominal Compliance with the Lowest Driving Pressure, Titrating PEEP Based on Decreasing the FIO2 to Maintain Adequate Oxygenation, etc
Flow Rate and Pattern
Physiology
Peak Flow Rate Should Be Set at a Level Sufficient to Overcome the Pulmonary and Ventilator Impedance
Insufficient Flow Rates Result in Increased Work of Breathing, Dyspnea, Spuriously Low Peak Inspiratory Pressure, and/or Scalloping of the Inspiratory Pressure Curve (NEJM, 1994) [MEDLINE]
Flow Waveform
Square (Constant Flow) Waveform
Decelerating (Ramp) Flow Waveform: may distribute ventilation more evenly than other patterns of flow, especially in the setting of airway obstruction (Intensive Care Med, 1985) [MEDLINE]
This Waveform Decreases the Peak Airway Pressure, Physiologic Dead Space, and pCO2, While Leaving Oxygenation Unchanged (Chest, 2002) [MEDLINE]
Sinusoidal Waveform
Application
Set Peak Flow Rates Typically Range from 60 L/min to 100 L/min
High Peak Flow Rates are Commonly Used in Patients with Obstructive Lung Disease: these allow shorter inspiratory times with longer expiratory times (i.e. lower I/E ratio), decreasing the risk of dynamic hyperinflation (Intensive Care Med, 1996) [MEDLINE]
Normal I/E Ratio: 1:2
Typical I/E Ratio Employed During Mechanical Ventilation of Patient with Obstructive Lung Disease: 1:3 to 1:5
of High Inspiratory Flow Rate During Assist Control Ventilation is Associated with an Increase in the Respiratory Rate (During Both Wakefulness and Sleep and in Health and Disease States) (Curr Opin Crit Care, 2003)* [MEDLINE]: such changes occur before changes in the arterial blood gas, consistent with either Hering-Breuer reflex activity or effects of flow-sensitive receptors
Decreased Inspiratory Time with Decreased Mean Airway Pressure (Which May Result in Worsened Oxygenation)
Fraction of Inspired Oxygen (FIO2)
Clinical Efficacy
Randomized Trial of Conservative Oxygen Strategy in Mechanically-Ventilated Patients (Am J Respir Crit Care Med, 2016) [MEDLINE]
Conservative Oxygen Strategy (SpO 88-92%) Did Not Impact the ICU or 90-Day Mortality Rate or Risk of Organ Dysfunction, as Compared to Liberal Oxygen Strategy (SpO2 ≥96%)
Italian Oxygen-ICU Trial of Conventional Oxygen Strategy (pO2 Up to 150 mm Hg or SaO2 97-100%) vs Conservative Oxygen Strategy (pO2 70-100 or SaO2 94-98%) in a General ICU Population (Stay of ≥72 hrs) (JAMA, 2016) [MEDLINE]: trial had unplanned, early termination
Conservative Oxygen Strategy Decreased Mortality Rate, as Compared to the Conventional Oxygen Strategy
French HYPERS2S Trial of Hyperoxia and Hypertonic Saline in Septic Shock (Lancet Respir Med, 2017) [MEDLINE]
Trial Stopped Prematurely for Safety Reasons
Setting FiO2 to 100% to Induce Arterial Hyperoxia Might Increase the Mortality Rate in Septic Shock
Hypertonic (3%) Saline Resuscitation Did Not Decrease the Mortality Rate in Septic Shock
Improving Oxygen Therapy in Acute-illness (IOTA) Systematic Review and Meta-Analysis of Conservative vs Liberal Oxygen Strategy in Critically Ill Patients (Lancet, 2018) [MEDLINE]: n = 25 trials (in patients with sepsis, critical illness, stroke, trauma, myocardial infarction, cardiac arrest, and emergency surgery)
In Acutely Ill Adults, Liberal Oxygen Therapy Strategy (Median SaO2 96%, Range 94-99%) Increases the 30-Day (and Longest Follow-Up) Mortality Rate, as Compared to a Conservative Oxygen Therapy Strategy (Relative Risk at 30 Days was 1.21, 95% CI 1.03-1.43)
Supplemental Oxygen Might Become Unfavorable with SaO2 >94-96%
Post Hoc Analysis of HYPERS2S Trial Data (Ann Intensive Care, 2018) [MEDLINE]
Hyperoxia May Be Associated with a Increased Mortality Rate in Patients with Septic Shock Using the Sepsis-3 Criteria (with Serum Lactate > 2 mmol/L), But Not in Patients with Hypotension Alone
In Patients with Serum Lactate ≤2 mmol/L, Hyperoxia Had No Effect on the Mortality Rate, Nor on Other Outcomes
Observational Study of Hyperoxia in the Emergency Department in Patients with Acute Respiratory Failure (Crit Care, 2018) [MEDLINE]: n = 688
Emergency Department Exposure to Hyperoxia is Common and Associated with Increased Mortality in Mechanically Ventilated Patients Achieving Normoxia After Admission
This Suggests that Hyperoxia in the Immediate Post-Intubation Period Could Be Particularly Injurious and Targeting Normoxia from Initiation of Mechanical Ventilation May Improve Outcome
Oxygen Should Be Prescribed to Achieve a Target Saturation of 94–98% for Most Acutely Ill Patients or 88–92% or Patient-Specific Target Range for Those at Risk of Hypercapnic Respiratory Failure
Best Practice is to Prescribe a Target Range for All Hospitalized Patients at the Time of Hospital Admission So that Appropriate Oxygen Therapy Can Be Started in the Event of Unexpected Clinical Deterioration with Hypoxemia and Also to Ensure that the Oximetry Section of the Early Warning Score Can Be Scored Appropriately
Recommendations (British Medical Journal-Oxygen Therapy for Acutely Ill Medical Patients: Clinical Practice Guideline, 2018) (BMJ, 2018) [MEDLINE]
Supplemental Oxygen Therapy Should Be Titrated to SpO2 ≤96% (Strong Recommendation)
SpO2 >96% is Likely Associated with a Small, But Important, Increased Risk of Death without Plausible Clinical Benefit
Recruitment Maneuvers
Rationale
Ventilatory Strategy that Transiently Increases the Transpulmonary Pressure to Reopen the Recruitable Lung Units in Acute Respiratory Distress Syndrome (ARDS) (see Acute Respiratory Distress Syndrome)
There is a Large-Scale Loss of Aerated Lung and Once the End-Inspiratory Pressure Surpasses the Regional Critical Opening Pressure of the Lung Units, Those Lung Units are Likely to Reopen
Study of Lung Recruitment Using CT Scanning with Breath Holding at Various Airway Pressures in Acute Respiratory Distress Syndrome (ARDS) (NEJM, 2006) [MEDLINE]
The Percentage of Recruitable Lung was Extremely Variable in ARDS: on average, 24% of lung could not be recruited
The Percentage of Recruitable Lung was Associated with the Response to PEEP
Cochrane Database Review of Recruitment Maneuvers in Patients with Acute Respiratory Distress Syndrome (ARDS) (Cochrane Database Syst Rev, 2009) [MEDLINE]
No Clinical Benefit of Recruitment Maneuvers in Either Mortality or Length of Mechanical Ventilation
Randomized Trial of Recruitment in Moderate-Severe Acute Respiratory Distress Syndrome (ARDS) (JAMA, 2017) [MEDLINE]: n = 1010
In Moderate-Severe ARDS, Lung Recruitment and Titrated PEEP Strategy Increased 28-Day All-Cause Mortality, as Compared to Low PEEP Strategy
Lung Recruitment and Titrated PEEP Strategy Decreased the Number of Ventilator-Free Days, Increased the Risk of Pneumothorax Requiring Chest Tube Drainage), and Increased the Risk of Barotrauma, as Compared to Low PEEP Strategy
Lung Recruitment and Titrated PEEP Strategy Had No Impact on ICU Length of Stay, Hospital Length of Stay, or In-Hospital Mortality Rate, as Compared to Low PEEP Strategy
Recommendations for Patients with Acute Respiratory Distress Syndrome (ARDS) (American Thoracic Society/European Society of Intensive Care Medicine/Society of Critical Care Medicine Clinical Practice Guidelines for Mechanical Ventilation in ARDS) (Am J Respir Crit Care Med, 2017) [MEDLINE]
Recruitment Maneuvers are Recommended in Adults with ARDS (Conditional Recommendation, Low-Moderate Confidence)
Recruitment Maneuvers Should Be Used with Caution in Patients with Pre-Existing Hypovolemia/Shock Due to Concern About Causing Hemodynamic Compromise
Recommendations for Patients with Acute Respiratory Distress Syndrome (ARDS) Associated with Sepsis (2016 Surviving Sepsis Guidelines; Intensive Care Med, 2017) [MEDLINE]
Recruitment Maneuvers are Recommended in Sepsis-Associated ARDS (Weak Recommendation, Moderate Quality of Evidence)
Selected Patients with Severe Hypoxemia May Benefit from Recruitment Maneuvers in Conjunction with Higher Levels of PEEP
Humidification of the Ventilator Circuit
Rationale for Humidification
The Upper Airway Provides 75% of the Heat and Moisture Supplied to the Alveoli
When the Upper Airway is Bypassed with an Endotracheal Tube, the Humidifier Needs to Supply the Missing Heat/Moisture
Types of Humidification
Active Humidification Via a Heated Humidifier: actively increase the heat and water vapor content of inspired gas
Passive Humidification Via a Heat and Moisture Exchanger: operate passively by storing heat and moisture from a patient’s exhaled gas (and subsequently releasing it into the inhaled gas)
Clinical Efficacy
Review and Clinical Practice Guideline for the Use of Humidification with Mechanical Ventilation (Respir Care, 2012) [MEDLINE]
Humidification is Recommended for Every Patient on Invasive Mechanical Ventilation (Grade 1A Recommendation)
Active Humidification is Recommended When Using Noninvasive Positive-Pressure Ventilation (NIPPV), as it May Improve Adherence and Comfort (Grade 2B Recommendation)
Passive Humidification is Not Recommended for Noninvasive Positive-Pressure Ventilation (NIPPV) (Grade 2C Recommendation)
Invasive Mechanical Ventilation
When Providing Humidification to Patients with Low Tidal Volumes (i.e. Those on Lung-Protective Ventilation Strategies), Heat and Moisture Exchangers are Not Recommended Because They May Contribute to Additional Dead Space, Which Can Increase the Ventilation Requirement and pCO2
Heat and Moisture Exchanger Should Not Be Used for the Prevention of Ventilator-Associated Pneumonia (VAP) (Grade 2B Recommendation)
Recommendations for Patients with Acute Respiratory Distress Syndrome (ARDS) Associated with Sepsis (2016 Surviving Sepsis Guidelines; Intensive Care Med, 2017) [MEDLINE]
Continuous or Intermittent Sedation Should Be Minimized (with Specific Sedation Endpoints) in Sepsis-Associated Mechanically-Ventilated Respiratory Failure (Best Practice Statement)
Pressures on the Ventilator
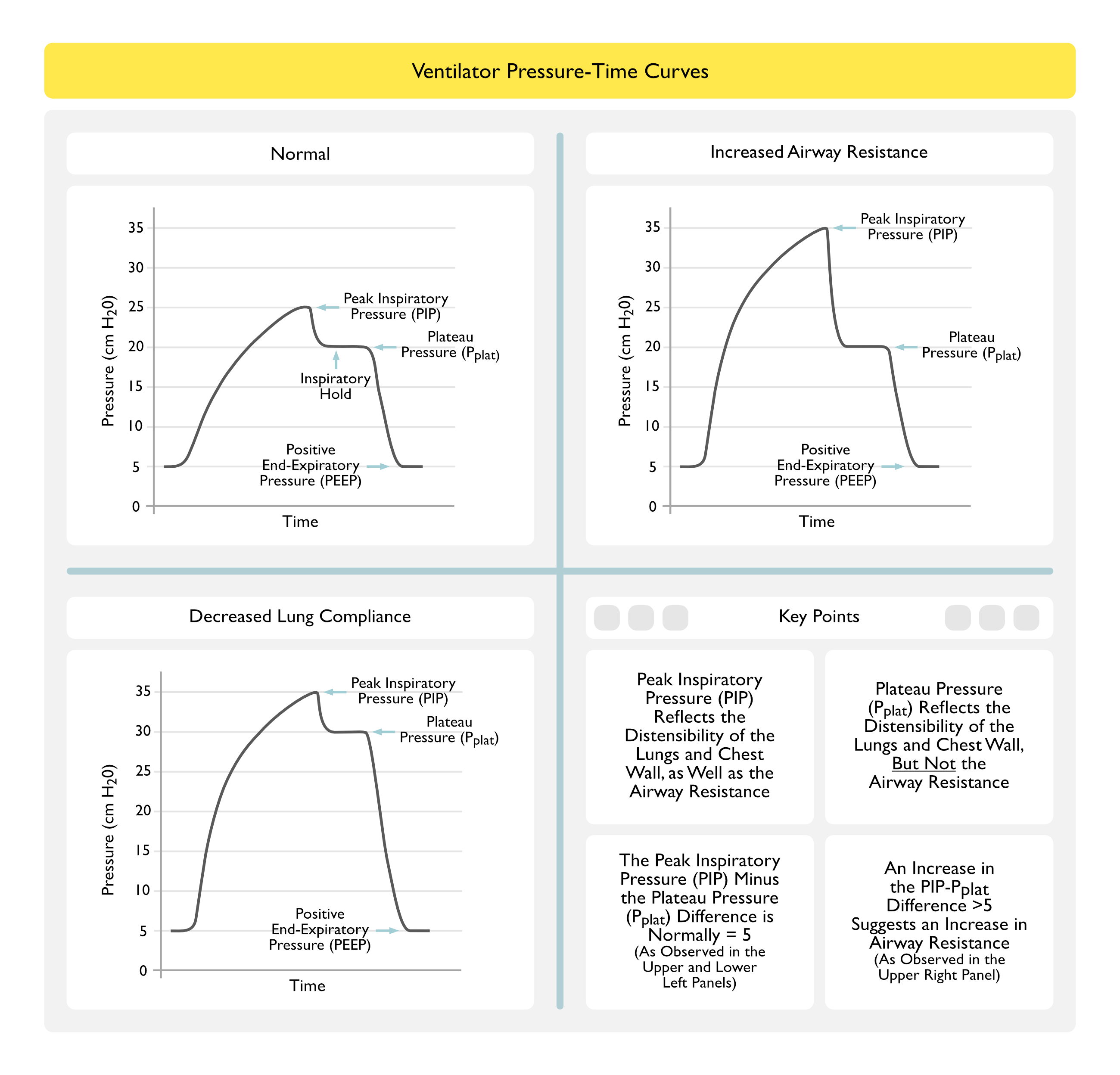
Peak Inspiratory Pressure (PIP)
Peak Inspiratory Pressure is is the Maximal Airway Pressure (as Measure at the Ventilator) Achieved During Gas Delivery
During Volume-Cycled Ventilation: where tidal volume is manually set
Peak Airway Pressure is Dependent on the Following
Airway Resistance
Inspiratory Flow Rate/Pattern
Static Lung Compliance
Tidal Volume
Peak Airway Pressure is the Arithmetic Sum of the Following Pressures
Flow-Related Pressure
Pressure Related to Elastic System Recoil
End-Expiratory Pressure (PEEP + Auto-PEEP)
During Pressure-Cycled Ventilation
Delta P is Manually Set and PIP is Not Used
Plateau Pressure
Plateau Pressure (Pplat) is End-Inspiratory Pressure at a Point of Zero Inspiratory Airflow
Technique: measure during an inspiratory hold maneuver (0.5-1 sec)
Physiology
Pressure is the Pressure Which is Applied by the Mechanical Ventilator to the Small Airways and Alveoli During Positive-Pressure Mechanical Ventilation
Etiology of Increased Plateau Pressure
High PEEP
High Inspiratory Flow Rate
High Tidal Volume
Clinical
Plateau Pressure is the Airway Pressure Which is Best Correlated with the Risk of Barotrauma
Mean Alveolar Pressure
Mean Alveolar Pressure is Pressure Averaged Over the Entire Ventilatory Cycle
Mean Alveolar Pressure Cannot Be Measured Clinically, But it Best Estimated by the Plateau Pressure
Mean Alveolar Pressure is the Most Important Determinant of Oxygenation
Mean Alveolar Pressure Correlates with the Risk of Ventilator-Associated Barotrauma
Mean Airway Pressure
Mean Airway Pressure is Airway Pressure Averaged Over the Entire Ventilatory Cycle
Mean Airway Pressure Usually Underestimates the Mean Alveolar Pressure, But it Correlates with Oxygenation
End-Expiratory Pressure
End-Expiratory Pressure is Airway Pressure at the End of Expiration
If the End-Expiratory Airway Pressure is Positive, This is Termed Positive End-Expiratory Airway Pressure (PEEP)
Extrinsic PEEP: PEEP applied by the clinician
Auto-PEEP (Intrinsic PEEP): PEEP which develops due to intrinsic properties of the lungs and/or airways
Total PEEP = Extrinsic PEEP + Auto-PEEP
Driving Pressure
Driving Pressure = Plateau Pressure – PEEP
Clinical Data
Study of Contribution of Driving Pressure to Mortality in ARDS (NEJM, 2015) [MEDLINE]: study used data from 9 prior randomized trials
Rationale: lower tidal volume, lower plateau pressure, and higher PEEP are all believed to decrease mechanical stresses on the lung in ARDS (which can induce ventilator-associated lung injury)
However, There is an Uncertainty When Optimizing One Component Adversely Affects Another (Example: Increasing PEEP May Undesirably Increase the Plateau Pressure), Which this Study Attempted to Address
Authors Theorized in Their Study that Optimizing the Tidal Volume/Respiratory System Compliance Ratio (Known as the Driving Pressure = Delta P) Would Provide a Better Predictor of Outcome in ARDS
Driving Pressure (Plateau Pressure – PEEP or Delta P) was the Best Predictor of Survival
Decreases in Tidal Volume or Increases in PEEP Were Beneficial Only if They Resulted in a Decrease in Delta P (In Other Words, PEEP Increments are Protective Only When They are Associated with an Improvement in Respiratory System Compliance, So that the Same Tidal Volume Can Be Delivered with a Lower Delta P)
Further Trials Using Specific Manipulation of Delta P are Required Before Recommending this Strategy as a Standard
Caveat: Delta P Can Only Be Accurately Assessed in Non-Breathing Patients
Recommendations
Maintain the Driving Pressure ≤13-15 cm H2O (NEJM, 2015) [MEDLINE]
Troubleshooting Ventilator Waveforms
Sawtooth Pattern Observed in the Expiratory Waveform in the Intubated Patient
Secretions in Endotracheal Tube
Water in Ventilator Tubing
Epidemiology
Frequency of This Event Has Decreased with the Use of Heated Wire Ventilator Circuits
Fentanyl (see Fentanyl): may produce increased chest wall/abdominal wall rigidity in some cases (especially with high doses used during cardiothoracic surgery)
Fentanyl (see Fentanyl): may produce increased chest wall/abdominal wall rigidity in some cases (especially with high doses used during cardiothoracic surgery)
Migration of Gastric Balloon of Minnesota/Sengstaken-Blakemore Tube (Used for Tamponade of Esophageal Varices) into the Esophagus (see Sengstaken-Blakemore Tube and Minnesota Tube)
Physiology: migration of the gastric balloon into the esophagus, resulting in acute tracheal compression
Compliance on the Ventilator
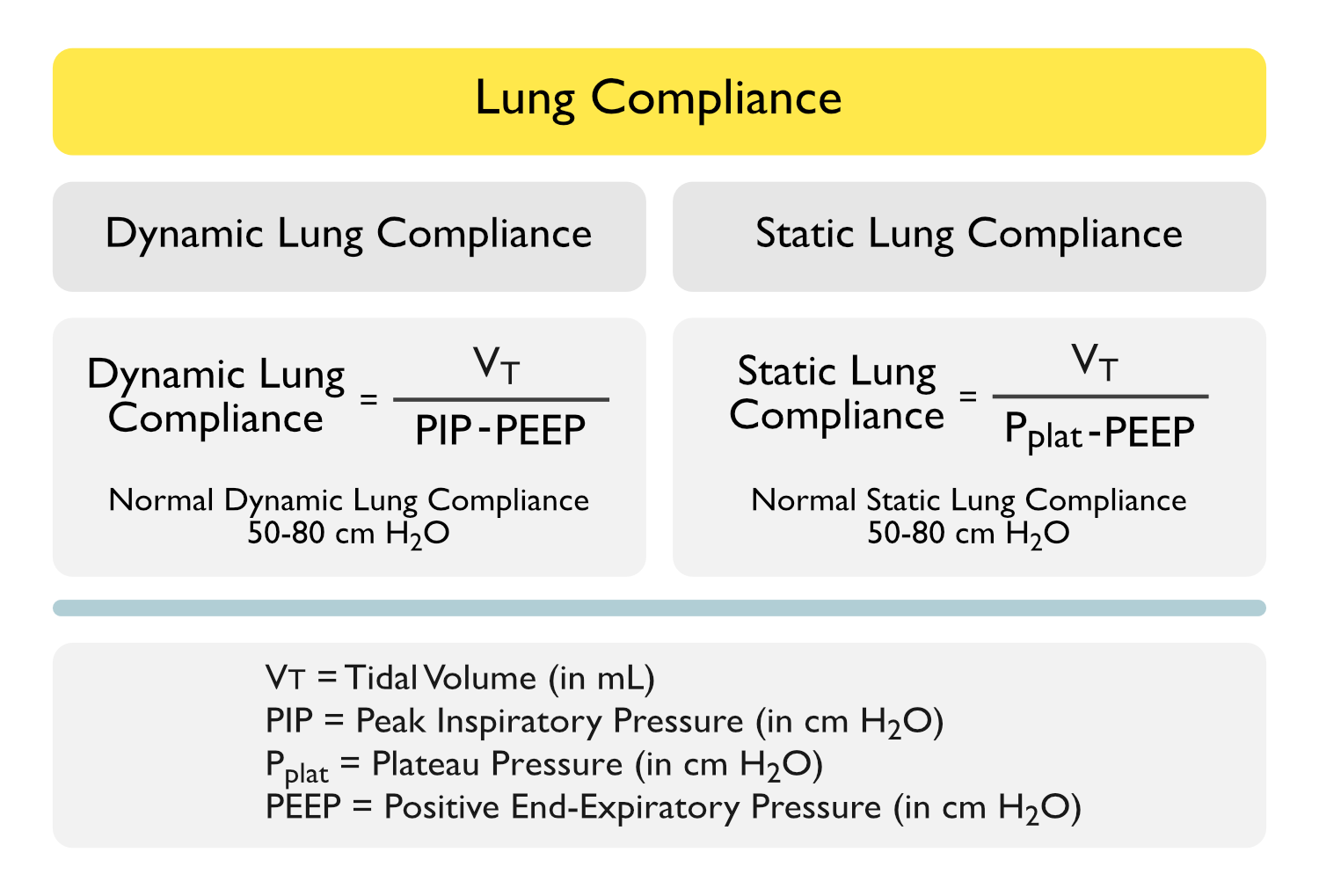
Static Lung Compliance
Static Compliance Reflects the Distensibility of the Lungs and Chest Wall (But Not Airway Resistance, Since it is Measured at Point of No Airflow)
Use the Exhaled Tidal Volume Shown on the Ventilator for the VT in this Equation, Not the Preset Tidal Volume (Since Ventilator Tubing Will Expand During Positive Pressure Ventilation: Expands About 3 cc for Every 1 cm H2O Increase in the Inflation Pressure
Compliance is Most Accurate when Performed During Passive Ventilation (Since the Patient’s Respiratory Muscle Efforts Will Decrease the Chest Wall Compliance) (Normal = 50-80 mL/cm H2O)
Dynamic Lung Compliance
Dynamic Compliance Reflects the Distensibility of the Lungs and Chest Wall and Airway Resistance (Since it is Measured at a Point of Maximal Inspiratory Airflow)
Equation
Dynamic Compliance = VT/(PIP-Total PEEP)
Use the Exhaled Tidal Volume Shown on the Ventilator for the VT in this Equation, Not the Preset Tidal Volume (Since Ventilator Tubing Will Expand During Positive Pressure Ventilation: Expands About 3 cc for Every 1 cm H2O Increase in the Inflation Pressure)
Compliance is Most Accurate when Performed During Passive Ventilation (Since the Patient’s Respiratory Muscle Efforts Will Decrease the Chest Wall Compliance) (Normal = 50-80 mL/cm H2O)
Ventilator Breath Types
Volume Control
Ventilator-Initiated Breaths with a Set Inspiratory Flow Rate
Inspiration is Terminated When the Set Tidal Volume is Reached
Airway Pressure is Determined by the Patient’s Airway Resistance, Lung Compliance, and Chest Wall Compliance
Examples of Ventilator Modes Which Use Volume Control Breaths
Volume Assist Control
Volume Synchronized Mandatory Ventilation (SIMV)
Volume Assist
Patient-Initiated Breaths with a Set Inspiratory Flow Rate
Inspiration is Terminated When a Set Tidal Volume is Reached
Airway Pressure is Determined by the Patient’s Airway Resistance, Lung Compliance, and Chest Wall Compliance
Examples of Ventilator Modes Which Use Volume Assist Breaths
Volume Assist Control
Volume Synchronized Mandatory Ventilation (SIMV)
Pressure Control
Ventilator-Initiated Breaths with a Set Pressure Limit
Inspiration is Terminated When the Set Inspiratory Time Has Elapsed
Tidal Volume is Variable and Dependent on the Patient’s Airway Resistance, Lung Compliance, Chest Wall Compliance, and Tubing Resistance: therefore, a specific minute ventilation is not guaranteed
Examples of Ventilator Modes Which Use Pressure Control Breaths
Ventilator-Initiated Breaths with a Set Pressure Limit
Inspiration is Terminated When the Set Inspiratory Time Has Elapsed
Tidal Volume is Variable and Dependent on the Patient’s Airway Resistance, Lung Compliance, Chest Wall Compliance, and Tubing Resistance: therefore, a specific minute ventilation is not guaranteed
Examples of Ventilator Modes Which Use Pressure Assist Breaths
Ventilator Provides a Driving Pressure for Each Breath, Which Determines the Maximal Flow Rate
Inspiration is Terminated Once the Inspiratory Flow is Decreased to a Predetermined Percentage of its Maximum Value
Examples of Ventilator Modes Which Use Pressure Support Breaths
Pressure Support (PS)
References
Technique
Types of Mechanical Ventilation
Pressure-Cycled vs Volume-Cycled Ventilation
Randomized, prospective trial of pressure-limited versus volume-controlled ventilation in severe respiratory failure. Crit Care Med. 1994;22(1):22 [MEDLINE]
Effects of short-term pressure-controlled ventilation on gas exchange, airway pressures, and gas distribution in patients with acute lung injury/ARDS: comparison with volume-controlled ventilation. Chest. 2002;122(4):1382 [MEDLINE]
Different modes of assisted ventilation in patients with acute respiratory failure. Eur Respir J. 2002;20(4):925 [MEDLINE]
Variables Involved in Positive-Pressure Ventilation
Optimization of respiratory muscle relaxation during mechanical ventilation. Anesthesiology. 1988;69(1):29 [MEDLINE]
Ventilator Settings
Trigger
Inspiratory work of breathing on flow-by and demand-flow continuous positive airway pressure. Crit Care Med. 1989;17(11):1108 [MEDLINE]
Influence of pressure- and flow-triggered synchronous intermittent mandatory ventilation on inspiratory muscle work. Crit Care Med. 1994;22(12):1933 [MEDLINE]
Patient-ventilator interaction during synchronized intermittent mandatory ventilation. Effects of flow triggering. Am J Respir Crit Care Med. 1995;151(1):1 [MEDLINE]
Effects of flow triggering on breathing effort during partial ventilatory support. Am J Respir Crit Care Med. 1998;157(1):135 [MEDLINE]
Flow triggering, pressure triggering, and autotriggering during mechanical ventilation. Crit Care Med. 2000;28(2):579 [MEDLINE]
Tidal Volume (VT)
Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. N Engl J Med. 2000;342(18):1301 [MEDLINE]
Intraoperative ventilation: incidence and risk factors for receiving large tidal volumes during general anesthesia. BMC Anesthesiol. 2011;11:22 [MEDLINE]
Association between use of lung-protective ventilation with lower tidal volumes and clinical outcomes among patients without acute respiratory distress syndrome: a meta-analysis. JAMA. 2012;308(16):1651 [MEDLINE]
A trial of intraoperative low-tidal-volume ventilation in abdominal surgery. N Engl J Med. 2013;369(5):428 [MEDLINE]
Intraoperative low-tidal-volume ventilation. N Engl J Med. 2013;369(19):1861 [MEDLINE]
Intraoperative ventilatory strategies to prevent postoperative pulmonary complications: a meta-analysis. Curr Opin Anaesthesiol. 2013 Apr;26(2):126-33 [MEDLINE]
Association between tidal volume size, duration of ventilation,and sedation needs in patients without acute respiratory distress syndrome: an individual patient data meta-analysis. Intensive Care Med. 2014;40(7):950-957 [MEDLINE]
Lung-Protective Ventilation With Low Tidal Volumes and the Occurrence of Pulmonary Complications in Patients Without Acute Respiratory Distress Syndrome: A Systematic Review and Individual Patient Data Analysis. Crit Care Med. 2015 Oct;43(10):2155-63 [MEDLINE]
A Meta-analysis of Intraoperative Ventilation Strategies to Prevent Pulmonary Complications: Is Low Tidal Volume Alone Sufficient to Protect Healthy Lungs? Ann Surg. 2016 May;263(5):881-7. doi: 10.1097/SLA.0000000000001443 [MEDLINE]
PReVENT Trial. Effect of a Low vs Intermediate Tidal Volume Strategy on Ventilator-Free Days in Intensive Care Unit Patients Without ARDS: A Randomized Clinical Trial. JAMA. 2018 Oct 24. doi: 10.1001/jama.2018.14280 [MEDLINE]
Respiratory Rate
Increasing respiratory rate to improve CO2 clearance during mechanical ventilation is not a panacea in acute respiratory failure. Crit Care Med. 2002;30(7):1407 [MEDLINE]
Positive End-Expiratory Pressure (PEEP)
Occult positive end-expiratory pressure in mechanically ventilated patients with airflow obstruction: The auto-PEEP effect. Am Rev Respir Dis 1982; 126:166-170 [MEDLINE]
Effect of positive end-expiratory pressure and body position in unilateral lung injury. J Appl Physiol Respir Environ Exerc Physiol. 1982;52(1):147 [MEDLINE]
Physiologic PEEP. Respir Care. 1988; 33:620
Determination of auto-PEEP during spontaneous and controlled ventilation by monitoring changes in end-expiratory thoracic gas volume. Chest 1989; 96:613-616 [MEDLINE]
Should PEEP be used in airflow obstruction? Am Rev Respir Dis 1989; 140:1-3 [MEDLINE]
PEEP, auto-PEEP, and waterfalls. Chest. 1989 Sep;96(3):449-51 [MEDLINE]
Auto-PEEP during CPR: an “occult” cause of electromechanical dissociation? Chest 1991;99:492–493 [MEDLINE]
Physiologic effects of positive end-expiratory pressure in chronic obstructive pulmonary disease during acute ventilatory failure and controlled mechanical ventilation. Am Rev Respir Dis. 1993;147:5–13 [MEDLINE]
Positive end-expiratory pressure increases the right to-left shunt in mechanically ventilated patients with patent foramen ovale. Ann Intern Med 1993; 119:887-894 [MEDLINE]
Interaction between intrinsic positive end-expiratory pressure and externally applied positive end-expiratory pressure during controlled mechanical ventilation. Crit Care Med 1993; 21:348-356 [MEDLINE]
The effects of applied vs auto-PEEP on local lung unit pressure and volume in a four-unit lung model. Chest. 1995 Oct;108(4):1073-9 [MEDLINE]
Auto-PEEP and electromechanical dissociation. N Engl J Med 1996;335:674–675 [MEDLINE]
Does positive end-expiratory pressure ventilation improve left ventricular function? A comparative study by transesophageal echocardiography in cardiac and noncardiac patients. Chest. 1998;114(2):556 [MEDLINE]
Pressure-volume curves and compliance in acute lung injury: evidence of recruitment above the lower inflection point. Am J Respir Crit Care Med. 1999 Apr;159(4 Pt 1):1172-8 [MEDLINE]
Use of pulse oximetry to recognize severity of airflow obstruction in obstructive airway disease: correlation with pulsus paradoxus. Chest 1999;115:475–481 [MEDLINE]
Influence of positive end-expiratory pressure on intracranial pressure and cerebral perfusion pressure in patients with acute stroke. Stroke. 2001;32(9):2088 [MEDLINE]
Intrinsic (or auto-) positive end-expiratory pressure during spontaneous or assisted ventilation. Intensive Care Med 2002;28:1552 [MEDLINE]
Positive end-expiratory pressure alters intracranial and cerebral perfusion pressure in severe traumatic brain injury. J Trauma. 2002;53(3):488 [MEDLINE]
The National Heart, Lung, and Blood Institute ARDS Clinical Trials Network. Higher versus lower positive end-expiratory pressures in patients with the acute respiratory distress syndrome. N Engl J Med 2004;351:327-36 [MEDLINE]
Effects of positive end-expiratory pressure on gastric mucosal perfusion in acute respiratory distress syndrome. Crit Care. 2004;8(5):R306 [MEDLINE]
Effects of positive end-expiratory pressure on regional cerebral blood flow, intracranial pressure, and brain tissue oxygenation. Crit Care Med. 2005;33(10):2367 [MEDLINE]
Cardiovascular issues in respiratory care. Chest. 2005;128(5 Suppl 2):592S [MEDLINE]
Review of ventilatory techniques to optimize mechanical ventilation in acute exacerbation of chronic obstructive pulmonary disease. Int J Chron Obstruct Pulmon Dis 2007 Dec;2(4):441–452 [MEDLINE]
Positive-end expiratory pressure reduces incidence of ventilator-associated pneumonia in nonhypoxemic patients. Crit Care Med. 2008;36(8):2225 [MEDLINE]
Positive-end expiratory pressure setting in adult acute lung injury and acute respiratory distress syndrome: a randomized, controlled trial. JAMA 2008;299:646 [MEDLINE]
Effect of positive expiratory pressure and type of tracheal cuff on the incidence of aspiration in mechanically ventilated patients in an intensive care unit. Crit Care Med. 2008;36(2):409 [MEDLINE]
Clinical concise review: Mechanical ventilation of patients with chronic obstructive pulmonary disease. Crit Care Med. 2008 May;36(5):1614-9. doi: 10.1097/CCM.0b013e318170f0f3 [MEDLINE]
Positive end-expiratory pressure redistributes regional blood flow and ventilation differently in supine and prone humans. Anesthesiology. 2010;113(6):1361 [MEDLINE]
Cardiac output estimation using pulmonary mechanics in mechanically ventilated patients. Biomed Eng Online. 2010;9:80 [MEDLINE]
Dynamic hyperinflation and auto-positive end-expiratory pressure: lessons learned over 30 years. Am J Respir Crit Care Med. 2011;184:756–762 [MEDLINE]
Patient-ventilator interactions. Implications for clinical management. Am J Respir Crit Care Med. 2013;188:1058–1068 [MEDLINE]
High versus low positive end-expiratory pressure during general anaesthesia for open abdominal surgery (PROVHILO trial): a multicentre randomised controlled trial. Lancet. 2014 Aug 9;384(9942):495-503. doi: 10.1016/S0140-6736(14)60416-5. Epub 2014 Jun 2 [MEDLINE]
Asynchronies during mechanical ventilation are associated with mortality. Intensive Care Med. 2015;41(4): 633–641; published online Feb 2015 [MEDLINE]
Effect of Intensive vs Moderate Alveolar Recruitment Strategies Added to Lung-Protective Ventilation on Postoperative Pulmonary Complications: A Randomized Clinical Trial. JAMA. 2017;317(14):1422 [MEDLINE]
Best PEEP trials are dependent on tidal volume. Crit Care. 2018;22(1):115 [MEDLINE]
Individualised perioperative open-lung approach versus standard protective ventilation in abdominal surgery (iPROVE): a randomised controlled trial. Lancet Respir Med. 2018;6(3):193 [MEDLINE]
Flow Rate and Pattern
Decelerating inspiratory flow waveform improves lung mechanics and gas exchange in patients on intermittent positive-pressure ventilation. Intensive Care Med. 1985;11(2):68 [MEDLINE]
The inspiratory workload of patient-initiated mechanical ventilation. Am Rev Respir Dis. 1986;134(5):902 [MEDLINE]
Optimization of respiratory muscle relaxation during mechanical ventilation. Anesthesiology. 1988;69(1):29 [MEDLINE]
Mechanical ventilation. N Engl J Med. 1994;330(15):1056 [MEDLINE]
Different modes of assisted ventilation in patients with acute respiratory failure. Eur Respir J. 2002;20(4):925 [MEDLINE]
Effects of inspiratory flow waveforms on lung mechanics, gas exchange, and respiratory metabolism in COPD patients during mechanical ventilation. Chest. 2002;122(6):2096 [MEDLINE]
Fraction of Inspired Oxygen (FIO2)
Conservative versus Liberal Oxygenation Targets for Mechanically Ventilated Patients. A Pilot Multicenter Randomized Controlled Trial. Am J Respir Crit Care Med. 2016 Jan;193(1):43-51 [MEDLINE]
Effect of Conservative vs Conventional Oxygen Therapy on Mortality Among Patients in an Intensive Care Unit: The Oxygen-ICU Randomized Clinical Trial. JAMA. 2016 Oct 18;316(15):1583-1589. doi: 10.1001/jama.2016.11993 [MEDLINE]
Hyperoxia and hypertonic saline in patients with septic shock (HYPERS2S): a two-by-two factorial, multicentre, randomised, clinical trial. Lancet Respir Med. 2017 Mar;5(3):180-190. doi: 10.1016/S2213-2600(17)30046-2 [MEDLINE]
BTS guideline for oxygen use in adults in healthcare and emergency settings. Thorax. 2017;72(Suppl 1):ii1 [MEDLINE]
Mortality and morbidity in acutely ill adults treated with liberal versus conservative oxygen therapy (IOTA): a systematic review and meta-analysis. Lancet. 2018 Apr 28;391(10131):1693-1705. doi: 10.1016/S0140-6736(18)30479-3 [MEDLINE]
Hyperoxia toxicity in septic shock patients according to the Sepsis-3 criteria: a post hoc analysis of the HYPER2S trial. Ann Intensive Care. 2018 Sep 17;8(1):90. doi: 10.1186/s13613-018-0435-1 [MEDLINE]
Emergency department hyperoxia is associated with increased mortality in mechanically ventilated patients: a cohort study. Crit Care. 2018 Jan 18;22(1):9. doi: 10.1186/s13054-017-1926-4 [MEDLINE]
Oxygen therapy for acutely ill medical patients: a clinical practice guideline. BMJ. 2018 Oct 24;363:k4169. doi: 10.1136/bmj.k4169. [MEDLINE]
Recruitment Maneuvers
Recruitment manoeuvres for adults with acute lung injury receiving mechanical ventilation. Cochrane Database Syst Rev. 2009 Apr 15;(2):CD006667 [MEDLINE]
Effect of Lung Recruitment and Titrated Positive End-Expiratory Pressure (PEEP) vs Low PEEP on Mortality in Patients With Acute Respiratory Distress Syndrome: A Randomized Clinical Trial. JAMA. 2017 Oct 10;318(14):1335-1345. doi: 10.1001/jama.2017.14171 [MEDLINE]