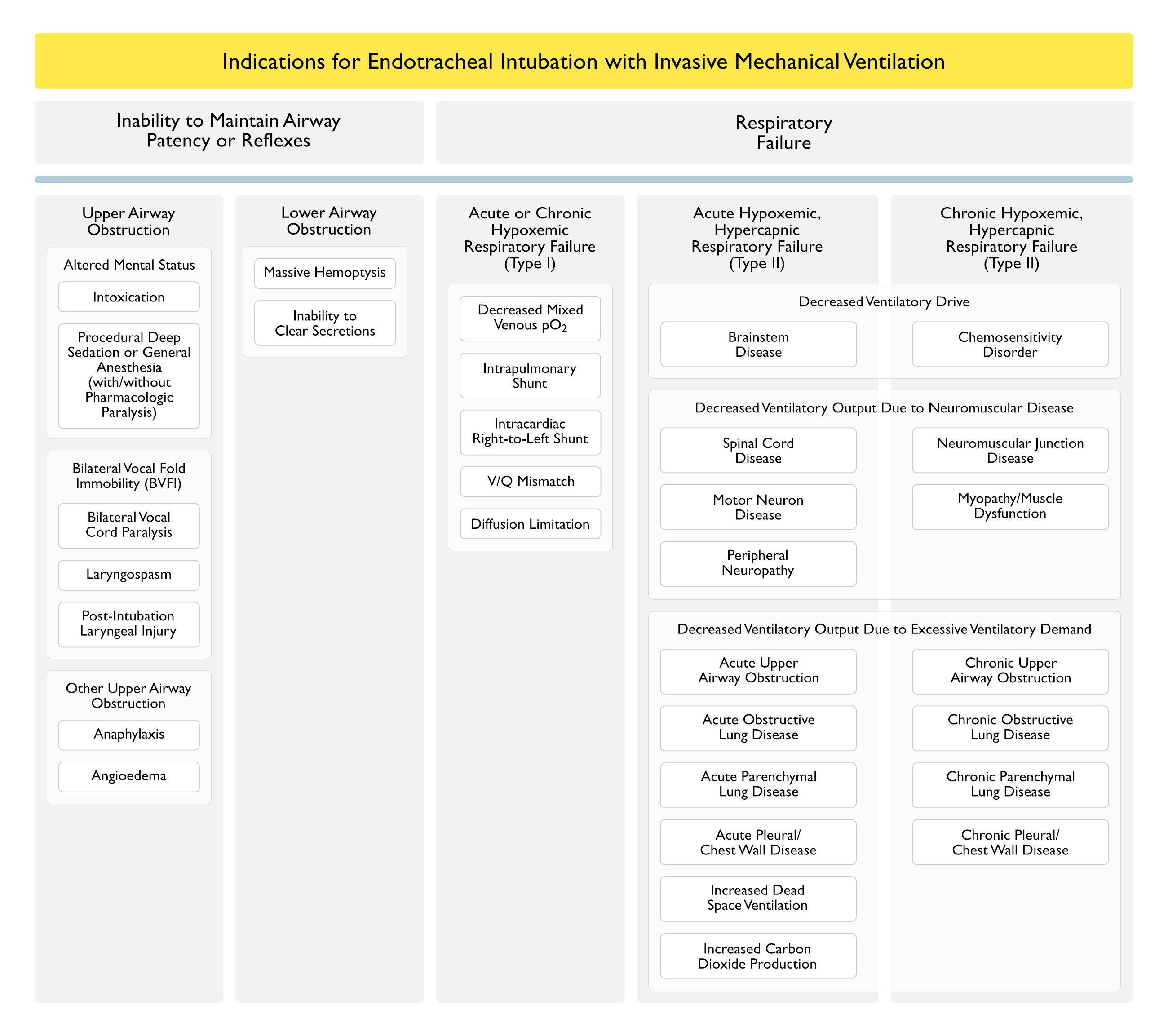
Decreased Ventilatory Output Due to Neuromuscular Disease
Decreased Ventilatory Output Due to Excessive Ventilatory Demand
Physiology
Physiologic/Clinical Benefits of Positive-Pressure Mechanical Ventilation
Positive-Pressure Mechanical Ventilation Decreases the Work of Breathing
Increased Work of Breathing (with the Development of Respiratory Muscle Fatigue) is a Common Feature of Various Types of Respiratory Failure
Depending on the Mode/Settings Utilized, Mechanical Ventilation Can Assume Part or All of the Work of Breathing, Allowing the Respiratory Muscles Time to Recover from Fatigue (Am J Med, 1982) [MEDLINE] (Intensive Care Med, 1998) [MEDLINE]
Improvement in V/Q Mismatch on Positive-Pressure Mechanical Ventilation is a Summation of the Following Two Competing Mechanisms
Positive-Pressure Mechanical Ventilation Worsens Physiologic (Alveolar) Dead Space (by Distending Alveoli Which May Be Poorly Perfused, Resulting in High V/Q Areas of the Lung)
Dead Space = Anatomic Dead Space + Physiologic (Alveolar) Dead Space
Note that Positive-Pressure Mechanical Ventilation Does Not Alter the Anatomic Dead Space
Positive-Pressure Mechanical Ventilation (Especially with the Application of PEEP) Decreases Atelectasis, Resulting in Decreased Physiologic Shunt
Shunt = areas of the lung which are underventilated, relative to perfusion (i.e. areas with low V/Q ratios)
Positive-Pressure Mechanical Ventilation Improves Left Ventricular Failure (see Congestive Heart Failure)
Positive-Pressure Mechanical Ventilation Decreases Venous Return to the Right Side of the Heart (Preload) and Decreases Left Ventricular Afterload (NEJM, 1991) [MEDLINE]
Hemodynamic Effects of Positive-Pressure Mechanical Ventilation are Due to Transmission of the Airway Pressure to the Adjacent Thoracic Structures
Transmission is Greatest When There is Low Chest Wall Compliance (Due to Fibrothorax, etc) or High Chest Wall Compliance (Due to COPD, etc)
Transmission is Least When There is High Chest Wall Compliance (Due to Sternotomy, etc) or Low Lung Compliance (Due to ARDS, Pulmonary Edema, etc)
Heterogeneity of Ventilation While on Positive-Pressure Mechanical Ventilation
Distribution of Ventilation (While on Positive-Pressure Mechanical Ventilation) is Heterogenous Due to Regional Differences in Alveolar Compliance, Airway Resistance, and Dependency (Upper Lung Zone vs Lower Lung Zone)
More Compliant Lung Zones with Low Airway Resistance Will Be the Most Ventilated (and Most Distended), While Less Compliant Lung Zones with High Airway Resistance Will Be the Least Ventilated (and Least Distended)
References
General
American Association for Respiratory Care Consensus Group. Essentials of Mechanical Ventilators. Respir Care 1992; 37:1000-1008
Classification for mechanical ventilators. Respir Care 1992; 37:1009-1025
Increased initial flow rate reduces inspiratory work of breathing during pressure support ventilation in patients with exacerbation of chronic obstructive pulmonary disease. Intensive Care Med. 1996 Nov;22(11):1147-54 [MEDLINE]
The treatment of acidosis in acute lung injury with tris-hydroxymethyl aminomethane (THAM). Am J Respir Crit Care Med. 2000 Apr;161(4 Pt 1):1149-53 [MEDLINE]
High-frequency oscillatory ventilation for acute respiratory distress syndrome in adults: A randomized, controlled trial. Am J Respir Crit Care Med 2002;166:801-808
Effect of inspiratory time and flow settings during assist-control ventilation. Curr Opin Crit Care. 2003 Feb;9(1):39-44 [MEDLINE]
High-frequency oscillatory ventilation in adults: The Toronto experience. Chest 2004;126:518 [MEDLINE]
Humidification during invasive and noninvasive mechanical ventilation: 2012. Respir Care. 2012 May;57(5):782-8. doi: 10.4187/respcare.01766 [MEDLINE]
An Official American Thoracic Society/American College of Chest Physicians Clinical Practice Guideline: Liberation from Mechanical Ventilation in Critically Ill Adults. Rehabilitation Protocols, Ventilator Liberation Protocols, and Cuff Leak Tests. Am J Respir Crit Care Med. 2017 Jan 1;195(1):120-133. doi: 10.1164/rccm.201610-2075ST [MEDLINE]
Official Executive Summary of an American Thoracic Society/American College of Chest Physicians Clinical Practice Guideline: Liberation from Mechanical Ventilation in Critically Ill Adults. Am J Respir Crit Care Med. 2017 Jan 1;195(1):115-119. doi: 10.1164/rccm.201610-2076ST [MEDLINE]
Physiology
Clinical manifestations of inspiratory muscle fatigue. Am J Med. 1982;73(3):308 [MEDLINE]
Hypercapnia. N Engl J Med. 1989;321(18):1223 [MEDLINE]
Treatment of severe cardiogenic pulmonary edema with continuous positive airway pressure delivered by face mask. N Engl J Med. 1991;325(26):1825 [MEDLINE]
Influence of mechanical ventilation on blood lactate in patients with acute respiratory failure. Intensive Care Med. 1998;24(9):924 [MEDLINE]