

Definitions

Respiratory Failure (see Respiratory Failure)
- Definition
- Respiratory Failure is Defined as the Occurrence of One or Both of the Following
- Decreased pO2, as Predicted for the Patient’s Age (Hypoxemia)
- Increased pCO2 (Hypercapnia) in the Setting of a Normal Serum Bicarbonate
- A Normal Serum Bicarbonate is Specified Here Since a Primary Metabolic Alkalosis (with Increased Serum Bicarbonate) Would Be Expected to Result in a Normal Compensatory Increase in pCO2: this normal compensatory mechanism functions to maintain a normal serum pH and would not be considered “respiratory failure”
- Respiratory Failure is Defined as the Occurrence of One or Both of the Following
Hypoxemia (see Hypoxemia)
- Definition
- Hypoxemia is Defined a Decrease in Hemoglobin Oxygen Saturation (as Assessed by Pulse Oximetry: SaO2 or SpO2) or Decrease in Arterial pO2 (as Assessed by Arterial Blood Gas)
- Note that a Patient May Be Hypoxemic, But Not Be Hypoxic
- Example
- A Young Hypoxemic Patient Can Significantly Increase Their Cardiac Output to Maintain Tissue Oxygen Delivery
- Example
Hypoxia (see Hypoxemia)
- Definition
- Hypoxia is Defined as a State of Impaired Tissue Oxygenation
- Note that a Patient May Be Hypoxic, But Not Be Hypoxemic
- Example
- In Cyanide Intoxication, SaO2 Can Be Normal, But Tissues May Be Hypoxic (see Cyanide)
- Example
Anoxia
- Definition
- Anoxia is Defined as Complete Tissue Deprivation of Oxygen Supply
Hypercapnia (see Hypercapnia)
- Definition
- Hypercapnia is Defined as Increase in Arterial pCO2 (i.e. Increased Arterial Blood Partial Pressure of Carbon Dioxide) to >40 mm Hg
Acidemia
- Definition
- Acidemia is Defined as Decrease in Arterial pH < 7.40 (Due to Either Metabolic or Respiratory Acidosis)
- Note that a Patient Can Be Acidemic without having a Respiratory Acidosis
- Example
- Metabolic Acidosis Can Produce Acidemia without the Presence of a Respiratory Acidosis
- Example
Alkalemia
- Definition
- Alkalemia is Defined an Increase in Arterial pH to >7.40 (Due to Either Metabolic or Respiratory Alkalosis)
Acidosis
- Definition
- Acidosis is Defined as the Presence of an Acid-Producing Acid-Base Disturbance (with or without Concomitant Acidemia)
- Clinical Scenarios in Which an Acidosis is Present, But in Which the pH is Not Acidemic
- Presence of a Metabolic Acidosis May Not Necessarily Result in an Acidemic pH (pH <7.4), Since Respiratory Compensation (Hyperventilation) Occurs, Resulting in an Increase in the Serum pH
- Presence of a (Chronic) Respiratory Acidosis May Not Necessarily Result in an Acidemic pH (pH <7.4), Since Metabolic Compensation (Renal Bicarbonate Retention) Generally Occurs Over a Period of Days, Resulting in an Increase in the Serum pH
Alkalosis
- Definition
- Alkalosis is Defined as the Presence of an Alkali-Producing Acid-Base Disturbance (with or without Concomitant Alkalemia)
- Clinical Scenarios in Which an Alkalosis is Present, But in Which the pH is Not Alkalemic
- Presence of a Metabolic Alkalosis May Not Necessarily Result in an Alkelemic pH (pH >7.4), Since Respiratory Compensation (Hypoventilation) Occurs Rapidly, Resulting in a Decrease in the Serum pH
- Presence of a (Chronic) Respiratory Alkalosis May Not Necessarily Result in an Alkalemic pH (pH >7.4), Since Metabolic Compensation (Renal Bicarbonate Wasting) Generally Occurs Over a Period of Days, Resulting in a Decrease in the Serum pH
Respiratory Acidosis (see Respiratory Acidosis)
- Definition
- Respiratory Acidosis is Defined as a Disorder Which Results in Increase in Arterial pCO2 with an Associated Decrease in Arterial pH
- Note that a Patient Can Have a Respiratory Acidosis without Being Significantly Acidemic
- Example
- Via Normal Compensatory Mechanisms, Chronic Respiratory Acidosis Induces Metabolic (Predominantly Renal) Compensation (with a Increase in Serum Bicarbonate Over Time), Culminating in Minimal Acidemia
- Example
Terms
- PaO2: arterial pO2 (arterial oxygen tension)
- Usually Referred to Simply as pO2
- PAO2: alveolar PO2 (alveolar oxygen tension)
- SpO2: pulse oximetry, as determined by peripheral pulse oximeter (see Pulse Oximetry)
- SaO2: pulse oximetry, as determined by arterial blood gas co-oximeter (see Arterial Blood Gas)

Etiology of Hypercapnia
Background
Determinants of Arterial pCO2
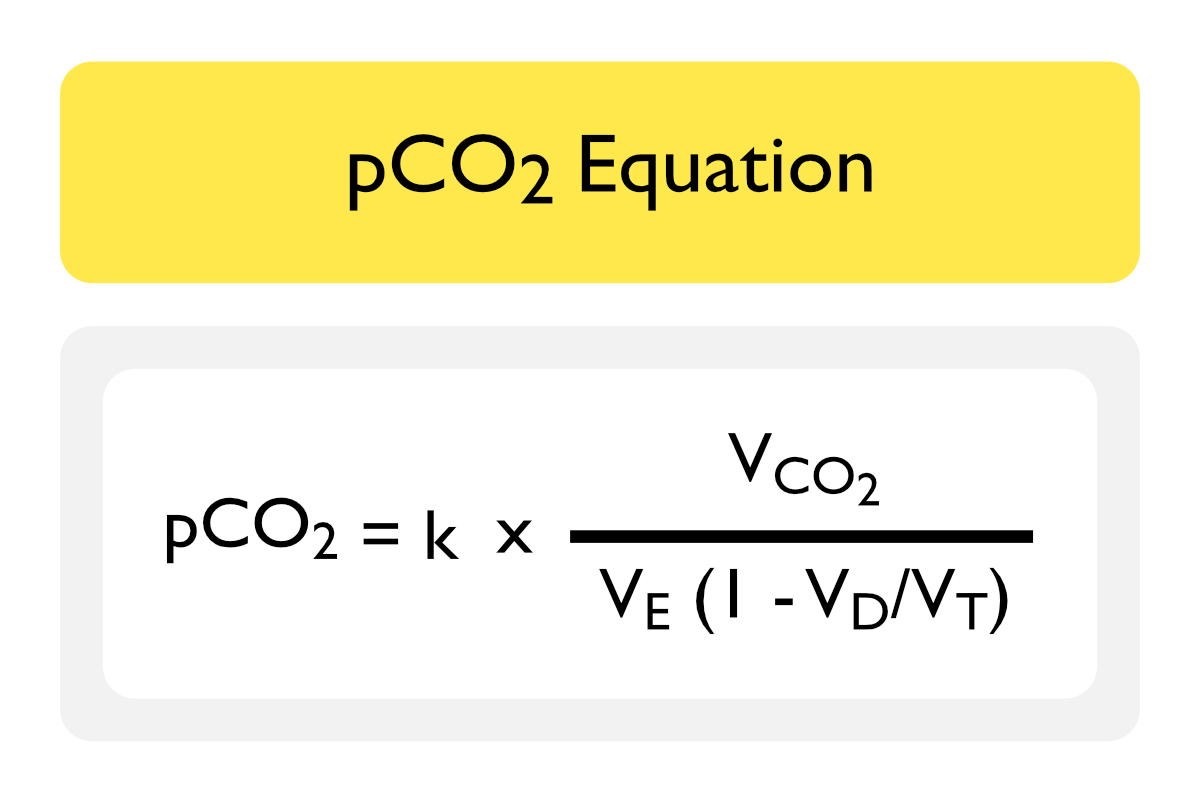
Terms and Assumptions
- pCO2: arterial partial pressure of carbon dioxide
- k: constant
- VCO2: carbon dioxide production (normal = 90-130 L/min/m2)
- Measured Using a Metabolic Cart (Which is Capable of Measuring Expired Carbon Dioxide)
- VE: minute ventilation (respiratory rate x tidal volume)
- VD/VT Ratio: dead space/tidal volume ratio
Specific Etiologies of Hypercapnia
- Respiratory Compensation for Metabolic Alkalosis (see Metabolic Alkalosis)
- Mechanism
- Elevated pH Results in Hypoventilation with a Compensatory Increase in pCO2
- However, the Degree of Hypoventilation is Limited by the Hypoxic Respiratory Drive to Breathe
- The Predicted Compensatory Increase in pCO2 in Response to a Primary Metabolic Alkalosis Obeys the Acid-Base Rules (see Acid-Base Physiology)
- Expect an Increase of 7 in pCO2 for Each Increase of 10 in the HCO3
- Expected pCO2 = (bicarb x 0.7) + 21 + 1.5
- Clinical Pearls
- ALL Cases of Subacute or Chronic Hypercapnia are Accompanied by Elevated Serum Bicarbonate (on Serum Chemistry or Arterial Blood Gas)
- Presence of Elevated Serum Carbon Dioxide Should Raise the Suspicion for Presence of Either a Primary Metabolic Alkalosis OR a Primary Respiratory Acidosis with Compensatory Metabolic Alkalosis
- One Would Order an Arterial Blood Gas to Differentiate These Conditions
- Elevated pH Results in Hypoventilation with a Compensatory Increase in pCO2
- Mechanism
- Increased Carbon Dioxide Production (VCO2)
- Occurs with Overfeeding (Generally with Tube Feedings or Total Parenteral Nutrition)
- Increased Carbon Dioxide Production Only Results in Hypercapnia When Alveolar Ventilation (VE) is Inadequate (ie: in the Presence of Significant Lung Disease, Such as Chronic Obstructive Pulmonary Disease, Acute Respiratory Distress Syndrome, etc)
- Acute Hypoventilation with Acutely Decreased Minute Ventilation (VE) (see Respiratory Failure)
- Chronic Hypoventilation with Chronically Decreased Minute Ventilation (VE) (see Respiratory Failure)
- Increased Dead Space Ventilation with Increased VD/VT Ratio
- Hypercapnia Only Occurs When the VD/VT Ratio Exceeds 50%
Physiology
Simplified Alveolar Gas Equation (see also Hypoxemia)
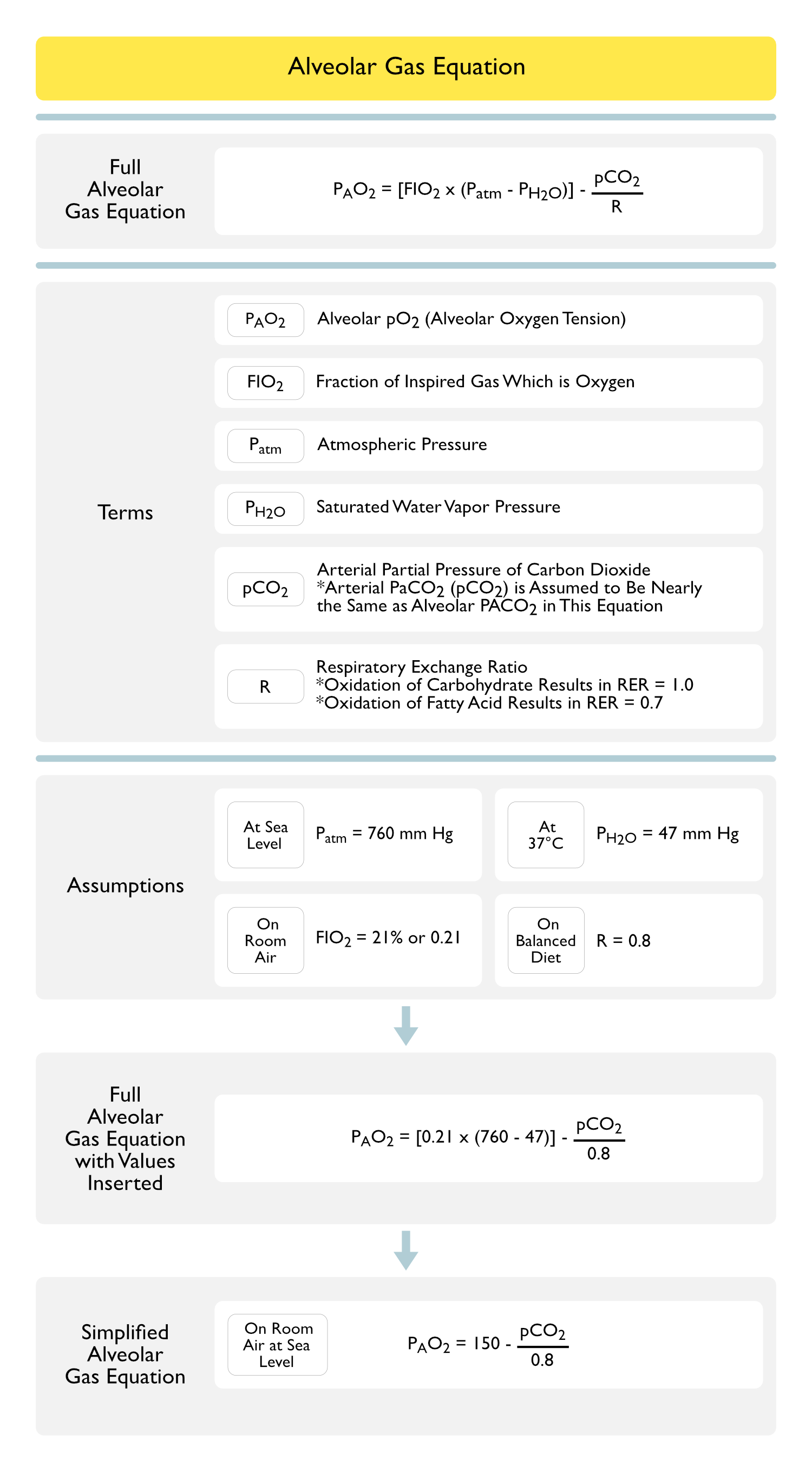
Terms and Assumptions
- PAO2: alveolar partial pressure of oxygen (PO2 or alveolar oxygen tension)
- Respiratory Exchange Ratio: 0.8
- Arterial PaCO2 (pCO2) is Assumed to Be Nearly the Same as Alveolar PACO2 in This Equation
- FIO2 is Assumed to Be Room Air (21% FIO2)
- Altitude is Assumed to Be Sea Level
Inverse Relationship Between Arterial pCO2 and pO2
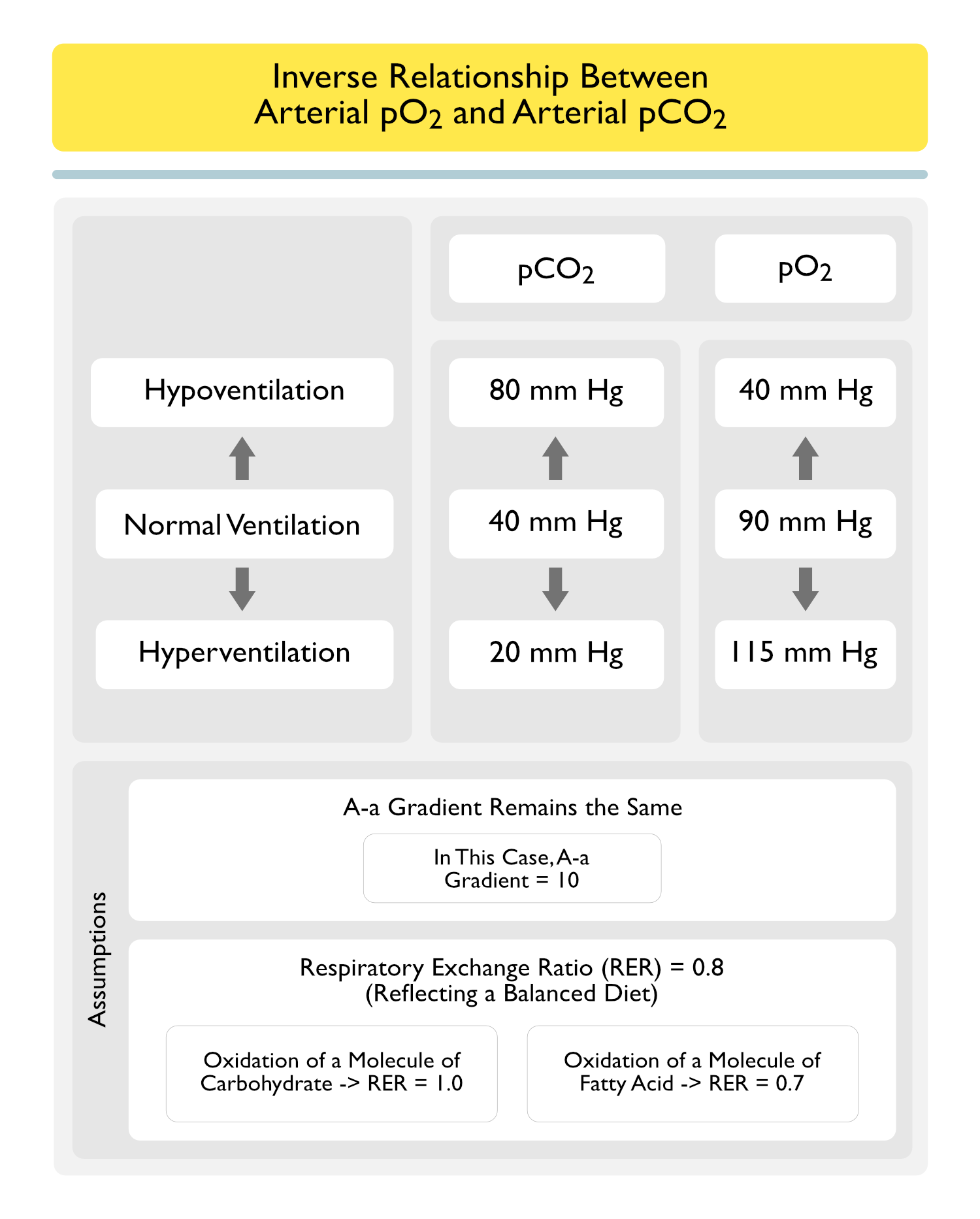
Terms and Assumptions
- A-a Gradient Remains the Same (in this Case, A-a Gradient = 10)
- Respiratory Exchange Ratio: 0.8
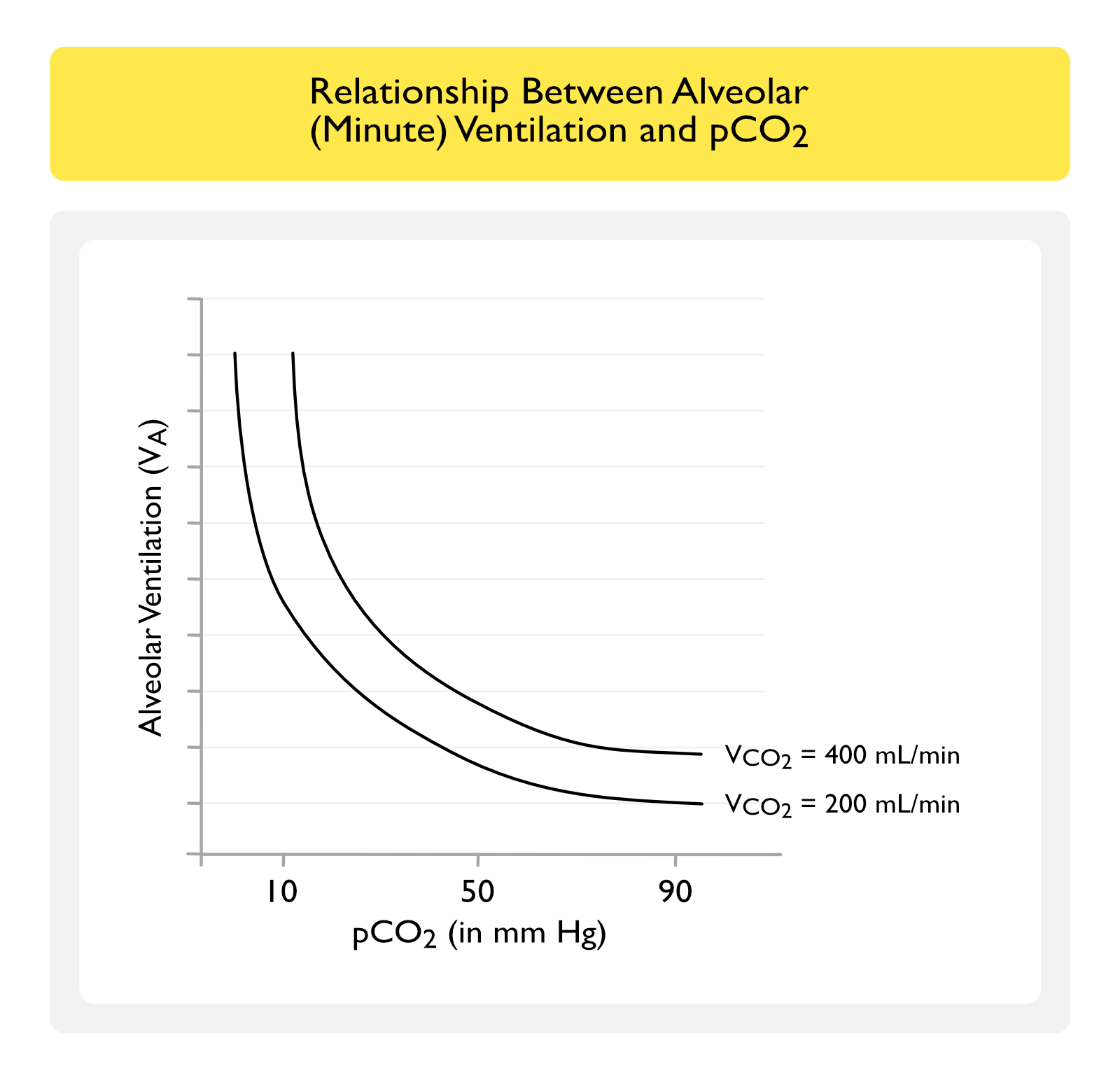
Increased Carbon Dioxide (CO2) Production Normally Results in a Compensatory Increase in Alveolar Ventilation
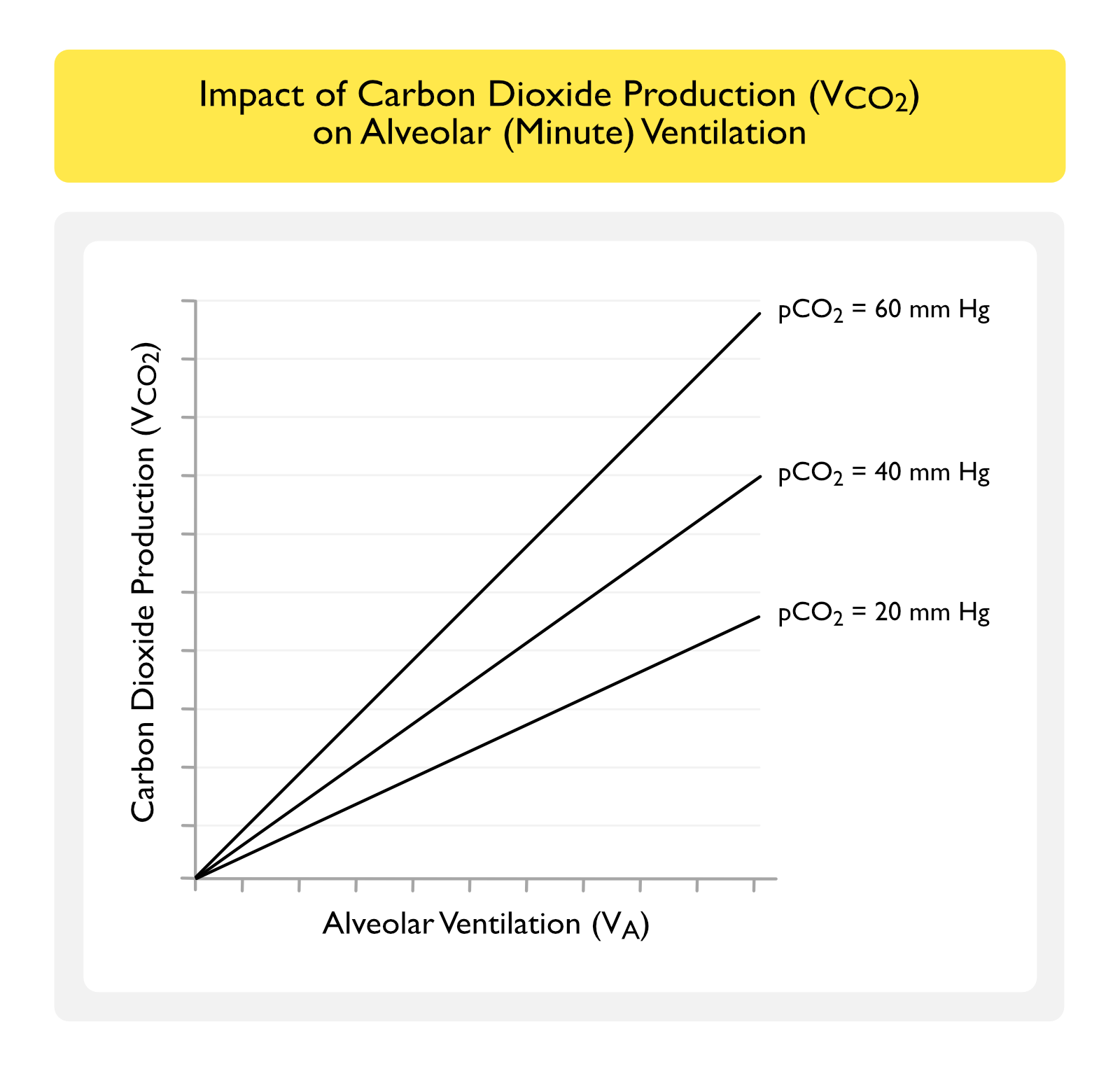
At a Constant Alveolar (Minute) Ventilation, Increased Carbon Dioxide (CO2) Production Should Theoretically Increase the pCO2
- In a Normal Patient
- Increased Carbon Dioxide (CO2) Production Results in an Increase in Alveolar (Minute) Ventilation, Decreasing the pCO2 Back to a Normal Level (i.e. Approximately 40 mm Hg)
- In a Patient with Moderate-Severe Lung Disease
- Patient May Be Unable to Increase Their Alveolar (Minute) Ventilation to Compensate for the Increased Carbon Dioxide (CO2) Production
- Therefor, pCO2 May Increase, Possibly Resulting in Respiratory Failure
Alveolar Ventilation is Inversely (But Not Linearly) Related to pCO2 (at Varying Levels of CO2 Production)
Clinical Examples
- In a Patient with Acute/Chronic Hypocapnia: assuming a constant CO2 production (VCO2), a significant increase in minute ventilation (VE) must be present to maintain the low pCO2
- Example: DKA patient with pH 7.40 and pCO2 30 must maintain a significanty increased VE to maintain the pCO2 at that level -> despite a normal pH, rapid respiratory failure can occur if, for any reason, patient cannot maintain that high VE
- In a Patient with Acute/Chronic Hypercapnia: assuming a constant CO2 production (VCO2), a relatively small decrease in VE can produce a significant increase in pCO2
- Example: chronically hypercapnic COPD with pCO2 60 can experience a significant increase in pCO2 with even a small decrease in VE (due to minimal sedation, etc)
Minute Ventilation (VE) is Inversely (But Not Linearly) Related to pCO2 (at Varying VD/VT Ratios)
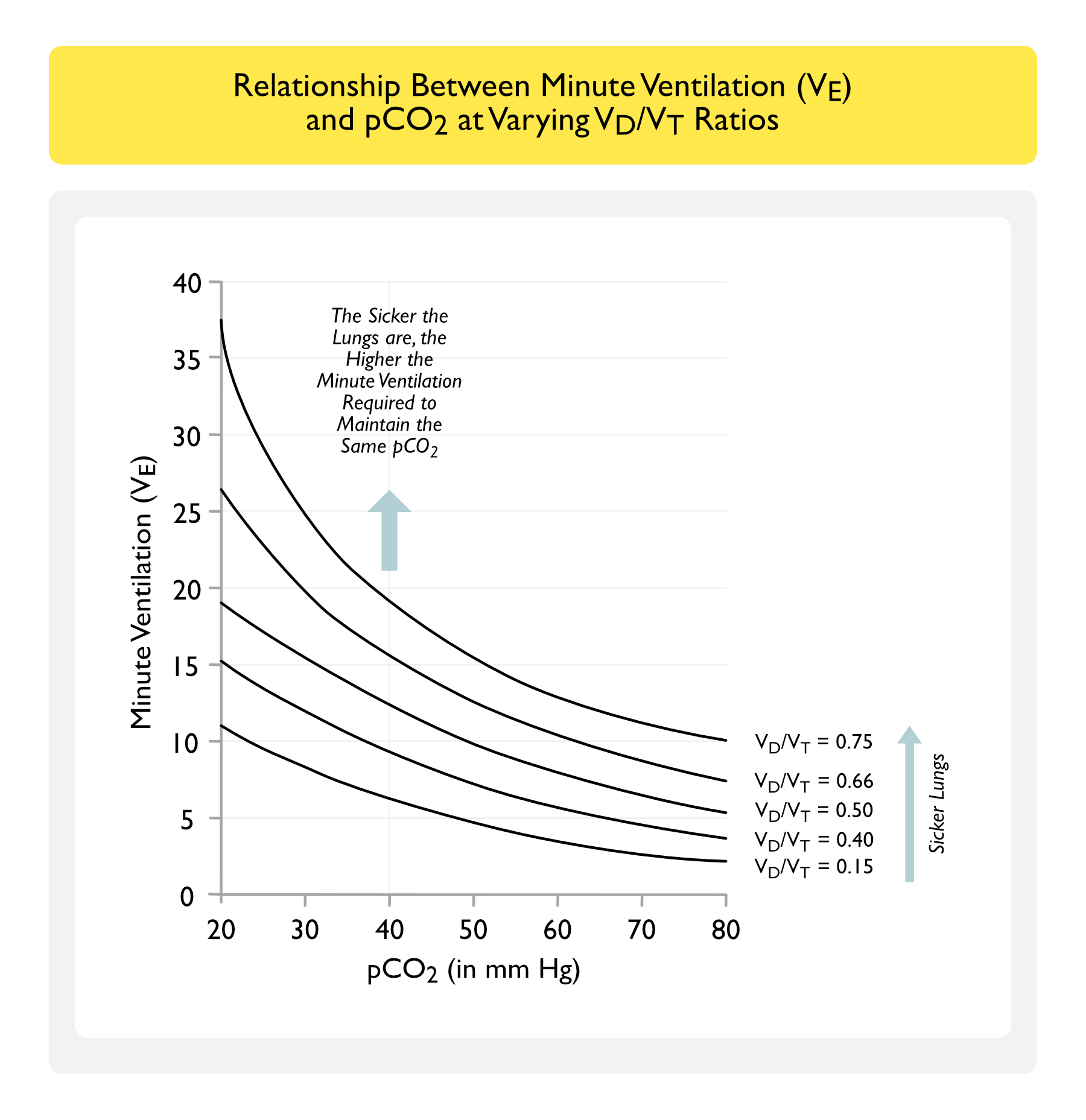
Terms and Assumptions
- Graph Assumes a Constant Carbon Dioxide Production (VCO2) of 200 ml/min
- VCO2 = VA x (PaCO2/PB)
- VE = VA x 1.21/(1-VD/VT)
Key Points
- VD/VT Ratio Determines How Efficiently the Lungs Excrete Carbon Dioxide (CO2) Per Breath (i.e How “Sick” the Lungs Are)
- Low VD/VT Ratio = More Efficient Carbon Dioxide (CO2) Excretion Per Breath
- High VD/VT Ratio = Less Efficient Carbon Dioxide (CO2) Excretion Per Breath
- At a Low VD/VT Ratio (Healthy Lungs), a Relatively Low Minute Ventilation (VE) is Required to Maintain pCO2 Constant at 40 mm Hg
- At a High VD/VT Ratio (“Sick Lungs”), a High Minute Ventilation (VE) is Required to Maintain pCO2 Constant at 40 mm Hg
- If This Level of Increased Minute Ventilation Cannot Be Maintained, the Patient Will Develop Hypercapnic Respiratory Failure
Impact on Shunt Fraction on Arterial pO2 and pCO2
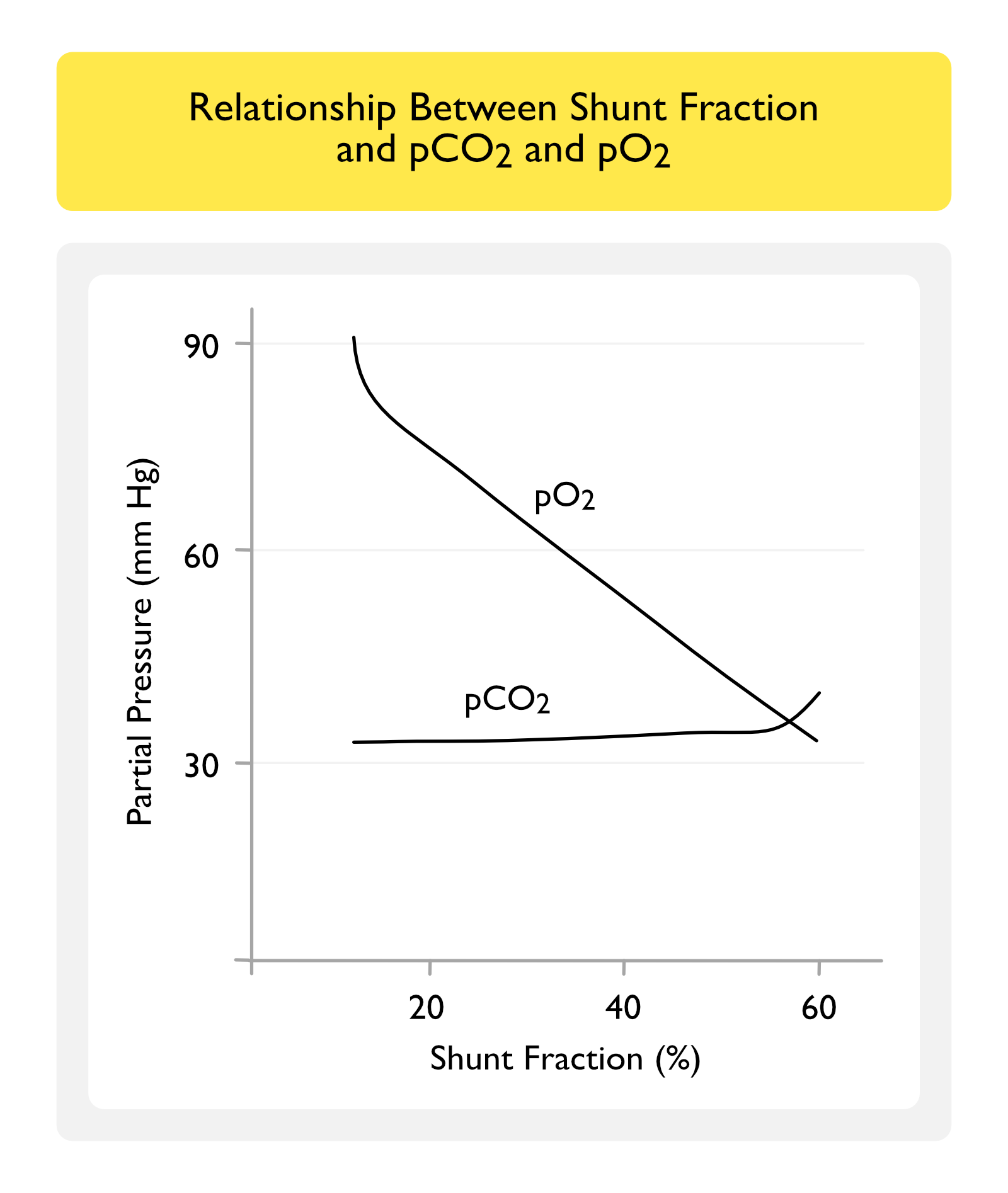
Key Points
- pO2 Decreases Linearly and Inversely with Increasing Shunt Fraction
- The Higher the Degree of Shunt, the Lower the pO2
- In Contrast, pCO2 Remains Relatively Constant Over a Wide Range of Shunt Fractions
- pCO2 Only Increases After the Shunt Fraction Exceeds 50%
- For This Reason, Shunt Does Not Typically Result in Hypercapnia
- pCO2 Only Increases After the Shunt Fraction Exceeds 50%
Diagnosis
Arterial Blood Gas (ABG) (see Arterial Blood Gas)
- Required for the Diagnosis of Hypercapnia/Respiratory Acidosis (see Respiratory Acidosis)
Clinical Evaluation of Hypercapnia (see also Respiratory Failure)
Normal/Unchanged Alveolar-Arterial (A-a) Gradient
Obstructive Pulmonary Function Tests (PFT’s)
- Chronic Obstructive Pulmonary Disease (COPD) (see Chronic Obstructive Pulmonary Disease)
- Hypercapnia in COPD is Multifactorial (Due to Hypoventilation, V/Q Mismatch, etc)
Restrictive Pulmonary Function Tests (PFT’s) + Normal Maximal Inspiratory Pressure (MIP)
- Obesity Hypoventilation Syndrome (OHS) (see Obesity Hypoventilation Syndrome)
- Obstructive Sleep Apnea (OSA) (see Obstructive Sleep Apnea)
- Primary Idiopathic Alveolar Hypoventilation Syndrome (Ondine’s Curse) (see Primary Idiopathic Alveolar Hypoventilation Syndrome)
- Brainstem Disease
- Pharmacologic Central Respiratory Depressants
- Opiates (see Opiates)
- Barbiturates (see Barbiturates)
- Benzodiazepines (see Benzodiazepines)
- Propofol (Diprivan) (see Propofol)
Restrictive Pulmonary Function Tests (PFT’s) + Decreased Maximal Inspiratory Pressure (MIP)
- Chest Wall Disease
- Kyphoscoliosis (see Kyphoscoliosis)
- Motor Neuron Disease
- Amyotrophic Lateral Sclerosis (ALS) (see Amyotrophic Lateral Sclerosis)
- Neuromuscular Junction Disease
- Myasthenia Gravis (see Myasthenia Gravis)
- Myopathy (see Myopathy)
- Duchenne Muscular Dystrophy (see Duchenne Muscular Dystrophy)
- Peripheral Neuropathy (see Peripheral Neuropathy)
- Guillain-Barre Syndrome (see Guillain-Barre Syndrome)
Increased Alveolar-Arterial (A-a) Gradient
Normal VCO2 (Normal Carbon Dioxide Production)
- V/Q Mismatch (V/Q Ratio >1, Dead Space Ventilation)
- Hypercapnia Only Occurs When VD/VT Ratio is >50%
- Chronic Obstructive Pulmonary Disease (COPD) (see Chronic Obstructive Pulmonary Disease)
- Hypercapnia in COPD is Multifactorial (Due to Hypoventilation, V/Q Mismatch, etc)
Increased VCO2 (Increased Carbon Dioxide Production)
- General Comments
- These Conditions Usually Cause Hypercapnia Only in the Setting of Underlying Lung Disease (with Impairment in Carbon Dioxide Excretion)
- Hypermetabolism
- Overfeeding: especially wtih excessive carbohydrate, whch generates more carbon dioxide per calorie than do fats
- Organic Acidosis
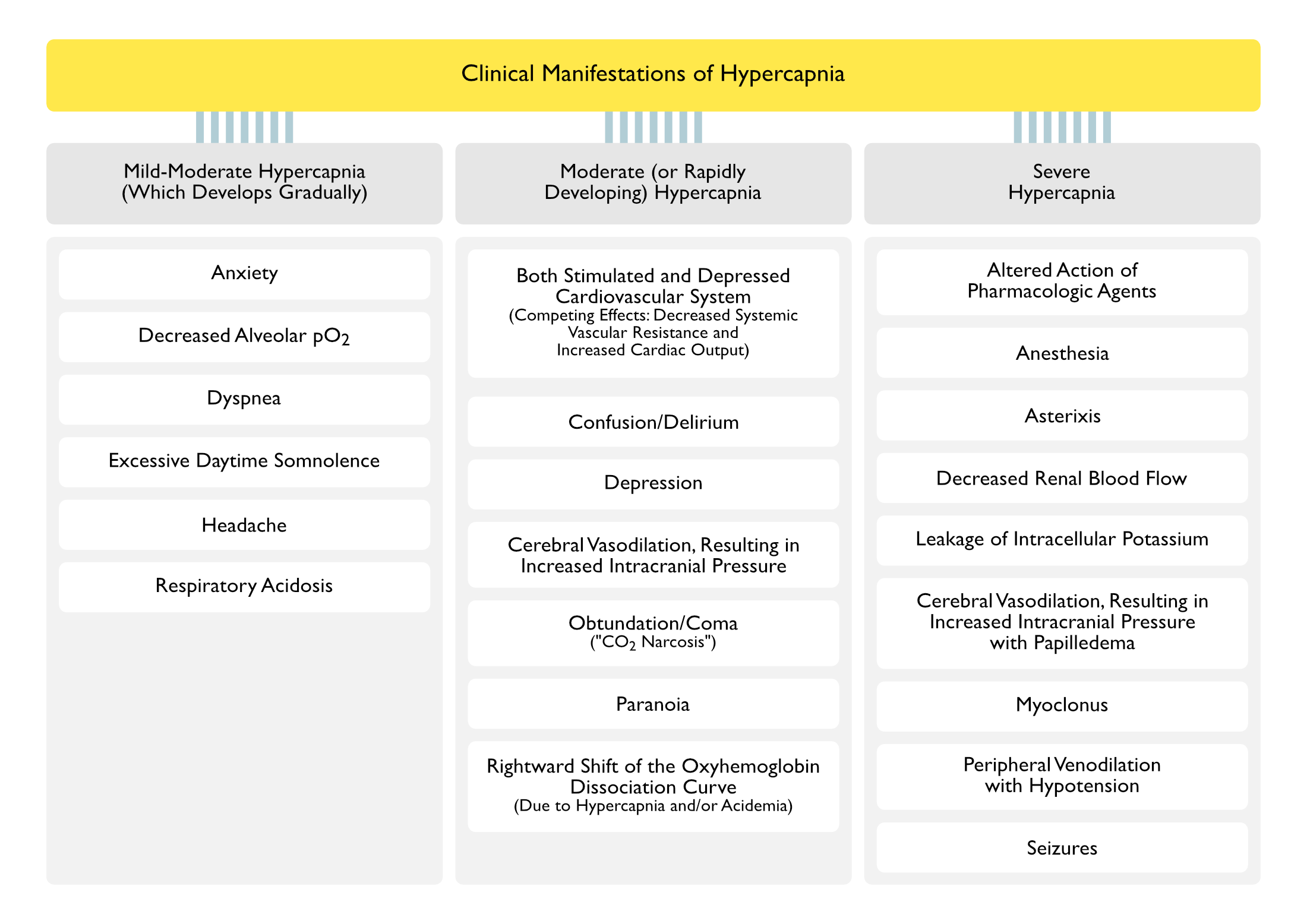
Clinical Manifestations of Hypercapnia/Respiratory Acidosis (see Respiratory Acidosis)
Cardiopulmonary Manifestations
- Acid-Base and Gas Exchange Abnormalities
- Decreased Alveolar pO2 (see Hypoxemia)
- Respiratory Acidosis (see Respiratory Acidosis)
- Arrhythmias
- Decreased Diaphragmatic Contractility
- May Result in Respiratory Failure (see Respiratory Failure)
- Decreased Myocardial Contractility
- May Result in Congestive Heart Failure (CHF) (see Congestive Heart Failure)
- Decreased Renal Blood Flow
- May Occur with pCO2 >150 mm Hg
- Dyspnea (see Dyspnea)
- Mechanisms
- Hypercapnia-Associated Decreased Diaphragmatic Contractility
- May Result in Respiratory Failure (see Respiratory Failure)
- Hypercapnia-Associated Decreased Myocardial Contractility
- May Result in Congestive Heart Failure (CHF) (see Congestive Heart Failure)
- Hypercapnia-Associated Acidemia, Resulting in Stimulation of Central and Peripheral Chemoreceptors
- Hypercapnia-Induced Increase in Respiratory Drive (Early), Then Decreased Respiratory Drive (Later)
- Hypercapnia-Associated Decreased Diaphragmatic Contractility
- Mechanisms
- Early Increased Respiratory Drive, Later Decreased Respiratory Drive
- Leakage of Intracellular Potassium
- May Occur with pCO2 >150 mm Hg
- Peripheral Venodilation with Hypotension (see Hypotension)
- May Occur with Severe Hypercapnia
- Rightward Shift of the Oxyhemoglobin Dissociation Curve (Due to Hypercapnia and/or Acidemia)
- Decreased Hemoglobin Affinity for Oxygen in the Lungs (with Decreased Oxygen Loading) and Increased Oxygen Unloading at the Tissues (Bohr Effect)
Neurologic Manifestations
- Altered Mental Status (see Altered Mental Status)
- Confusion (see Confusion)
- May Occur with Moderate (or Rapidly Developing) Hypercapnia
- Delirium (see Delirium)
- May Occur with Moderate (or Rapidly Developing) Hypercapnia
- Obtundation/Coma (“CO2 Narcosis”) (see Obtundation/Coma)
- Acute Hypercapnia Initially Increases the Respiratory Drive (with Associated Hyperventilation) (Anesthesiology, 1960) [MEDLINE] (NEJM, 1984) [MEDLINE]
- Later, Acute Hypercapnia Decreases the Respiratory Drive, Leading to Worsening Hypercapnia with Depressed Mental Status (“CO2 Narcosis”)
- Normal (Normocapnic) Patients Generally Do Not Develop Altered Mental Status Until the pCO2 Exceeds 75-80 mm Hg
- Chronically Hypercapnic Patients Generally Do Not Develop Altered Mental Status Until the pCO2 Exceeds 90-100 mm Hg
- These Later Effects are Mediated Via Increased Brain Glutamine, Increased Brain γ-Aminobutyric Acid (GABA), Decreased Brain Glutamate, and Decreased Brain Aspartate
- Confusion (see Confusion)
- Anesthesia (see Anesthesia)
- May Occur with pCO2 >200 mm Hg
- Anxiety (see Anxiety)
- May Occur with Mild-Moderate Hypercapnia (Which Develops Gradually
- Asterixis (see Asterixis)
- May Occur with Severe Hypercapnia
- Depression (see Depression)
- May Occur with Moderate (or Rapidly Developing) Hypercapnia
- Excessive Daytime Somnolence (see Excessive Daytime Somnolence)
- May Occur with Mild-Moderate Hypercapnia (Which Develops Gradually
- Headache (see Headache)
- May Occur with Mild-Moderate Hypercapnia (Which Develops Gradually
- Increased Intracranial Pressure (ICP) (see Increased Intracranial Pressure) (Anesthesiology, 1960) [MEDLINE] (NEJM, 1984) [MEDLINE]
- Hypercapnia Causes Cerebral Vasodilation with Increased Cerebral Blood Flow
- The Increased Cerebral Blood Flow May Undesirably Potentiate Neurologic Injury in Traumatic Brain injury (TBI), etc (see Traumatic Brain injury)
- Papilledema May Occur with Severe Hypercapnia (see Papilledema)
- Hypercapnia Causes Cerebral Vasodilation with Increased Cerebral Blood Flow
- Myoclonus (see Myoclonus)
- May Occur with Severe Hypercapnia
- Paranoia (see Paranoia)
- May Occur with Moderate (or Rapidly Developing) Hypercapnia
- Seizures (see Seizures)
- May Occur with Severe Hypercapnia
Manifestations Due to the Acidosis Itself
- Altered Action of Pharmacologic Agents
- Intracellular Acidosis Potentiates the Effect of Neuromuscular Junction Antagonists (Cisatracurium, Rocuronium, etc) (see Neuromuscular Junction Antagonists)
- Cardiovascular Instability/Cardiac Arrest (see Cardiac Arrest)
- Central Nervous System Depression
- Decreased Calcium Binding to Albumin (with Increase Serum Ionized Calcium Levels) (see Hypercalcemia)
- Hyperkalemia Due to Extracellular Shift of Potassium (see Hyperkalemia)
- Hypotension/Pulseless Electrical Activity (PEA) (see Hypotension and Pulseless Electrical Activity)
- Due to Decreased Systemic Vascular Resistance (SVR)
Treatment
Noninvasive Positive-Pressure Ventilation (NIPPV) (see Noninvasive Positive-Pressure Ventilation)
- See Noninvasive Positive-Pressure Ventilation
Invasive Mechanical Ventilation (see Invasive Mechanical Ventilation-General)
- See Invasive Mechanical Ventilation-General
References
General
- Effects of carbon dioxide on the cardiovascular system. Anesthesiology. 1960;21:652 [MEDLINE]
Etiology
- Causes of and compensations for hypoxemia and hypercapnia. Compr Physiol. 2011 Jul;1(3):1541-53. doi: 10.1002/cphy.c091007 [MEDLINE]
- Oxygen-induced hypercapnia in COPD: myths and facts. Crit Care. 2012 Oct 29;16(5):323. doi: 10.1186/cc11475 [MEDLINE]
- Effects of hypercapnia on the lung. J Physiol. 2017 Apr 15;595(8):2431-2437. doi: 10.1113/JP273781 [MEDLINE]