Treatment of Chronic Obstructive Pulmonary Disease (COPD) Exacerbation
Site of Treatment (Global Initiative for Chronic Obstructive Lung Disease/GOLD. Global Strategy for the Diagnosis, Management and Prevention of Chronic Obstructive Pulmonary Disease: 2026 Report) [LINK]
General Comments
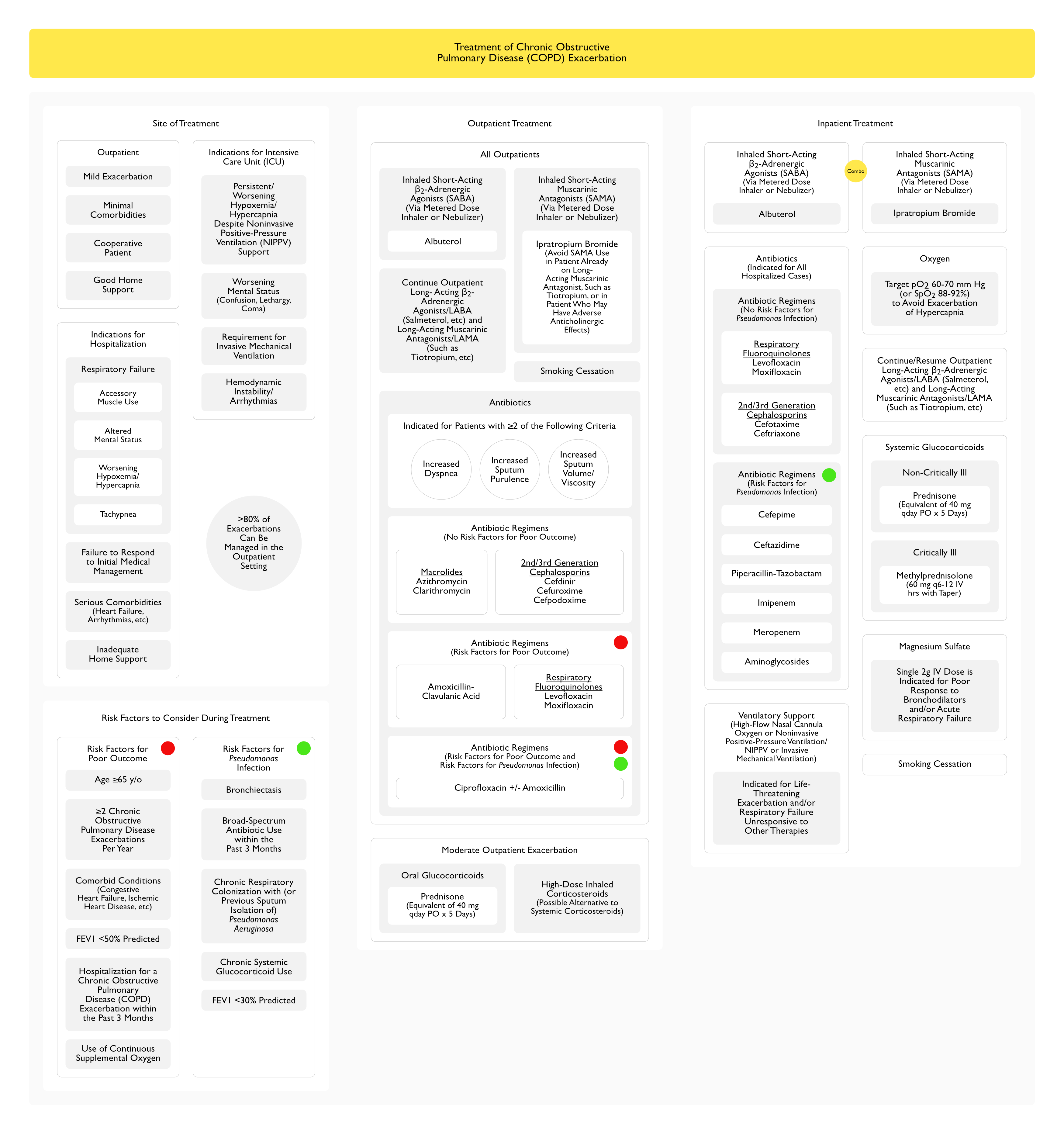
>80% of Chronic Obstructive Pulmonary Disease (COPD) Exacerbations Can Be Managed in the Outpatient Setting
Avoid Short-Acting Muscarinic Antagonists (SAMA) Use in Patient Already on Long-Acting Muscarinic Antagonist (LAMA) (Such as Tiotropium) or in Patient Who May Have Adverse Anticholinergic Effects (Patient with Urinary Retention, etc)
Continue Outpatient Long-Acting β2-Adrenergic Agonists/LABA (Salmeterol, etc) and Long-Acting Muscarinic Antagonists/LAMA (Such as Tiotropium, etc)
Due to Risk of Adverse Anticholinergic Effects
Antibiotics
Indications for Antibiotics in the Outpatient Setting (≥2 Criteria) (Ann Intern Med, 1987) [MEDLINE] (Global Initiative for Chronic Obstructive Lung Disease/GOLD. Global Strategy for the Diagnosis, Management and Prevention of Chronic Obstructive Pulmonary Disease: 2026 Report) [LINK]
Outpatients without Risk Factors for Poor Outcome (See Below): coverage for Streptococcus Pneumoniae, Haemophilus Influenzae, and Moraxella Catarrhalis
Outpatients with Risk Factors for Poor Outcome (See Below): target macrolide-resistant Streptococcus Pneumoniae and enhance eradication of Haemophilus Influenzae
Outpatients with Both Risk Factors for Poor Outcome and Risk of Pseudomonas Infection (See Below): fluoroquinolone resistance is prevalent among Pseudomonas Aeruginosa strains (and amoxicillin has better activity against Streptococcus Pneumoniae)
Combination Therapy with Albuterol and Ipratropium Bromide is Superior to Albuterol Alone in Stable Chronic Obstructive Pulmonary Disease (COPD) (Chest, 1994) [MEDLINE]
However, a Systematic Review Including a Small Number of Trials Which Compared a Combination of a SABA (Albuterol, Fenoterol, Metaproterenol) and a SAMA (Ipratropium Bromide) to a SABA Alone and Did Not Demonstrate a Benefit to the Combination When Assessed at 90 min (Cochrane Database Syst Rev, 2002) [MEDLINE]
Regardless, Combination SABA + SAMA Treatment is Routinely Used in the Setting of Chronic Obstructive Pulmonary Disease (COPD) Exacerbation
It is Unknown Whether a Rapid-Onset Long-Acting β2-Adrenergic Agonist (Formoterol, Indacaterol) Would Be a Reasonable Substitute for Albuterol Nebulizer Treatments in Patients with Chronic Obstructive Pulmonary Disease (COPD) Exacerbation Who are Not Already Using Indacaterol (Pulm Pharmacol Ther, 2013) [MEDLINE]
Combination Therapy with Albuterol and Ipratropium Bromide is Superior to Albuterol Alone in Stable Chronic Obstructive Pulmonary Disease (COPD) (Chest, 1994) [MEDLINE]
However, a Systematic Review Including a Small Number of Trials Which Compared a Combination of a SABA (Albuterol, Fenoterol, Metaproterenol) and a SAMA (Ipratropium Bromide) to a SABA Alone and Did Not Demonstrate a Benefit to the Combination When Assessed at 90 min (Cochrane Database Syst Rev, 2002) [MEDLINE]
Regardless, Combination SABA + SAMA Treatment is Routinely Used in the Setting of Chronic Obstructive Pulmonary Disease (COPD) Exacerbation
Continue (or Resume) Outpatient Long-Acting β2-Adrenergic Agonists/LABA (Salmeterol, etc) and Long-Acting Muscarinic Antagonists/LAMA (Such as Tiotropium, etc)
When Patient is Able to Tolerate These Medications
Titration Supplemental Oxygen to a Target SpO2 88-92% Resulted in Decreased Mortality Rate, as Compared to High-Flow (Non-Titrated) Oxygen in the Prehospital Setting
Retrospective Analysis of Oxygen Therapy in Patients Admitted for COPD Exacerbation (Emerg Med J, 2021) [MEDLINE]: n = 1,027
As Compared to the SpO2 88-92% Target Group, the Adjusted Risk of Death in the SpO2 93-96% and the 97-100% Groups was Higher (Adjusted Odds Ratio 1.98; 95% CI: 1.09-3.60 and 2.97; 95% CI: 1.58-5.58, Respectively)
Clinical Efficacy-High-Flow Nasal Cannula (HFNC)
Secondary Analysis of Multicenter Trial, Studying High-Flow Nasal Cannula (HFNC) vs Conventional Oxygen Therapy in the Setting of Hypercapnic Chronic Obstructive Pulmonary Disease (COPD) Exacerbation (Respir Med, 2023) [MEDLINE]: n = 330 non-acidotic hypercapnic patients
In the High Bicarbonate Subgroup (Bicarbonate 35.0 [33.3-37.9] mmol/L; pCO2 56.8 [52.0-62.8] mm Hg), Patients Supported by High-Flow Nasal Cannula (HFNC) Had a Prolonged Length of Hospital Stay, as Compared to Conventional Oxygen Therapy (Hazard Ratio 1.59 [1.16-2.17], p = 0.004)
However, Patients in the Low Bicarbonate Subgroup (Bicarbonate 28.8 [27.0-30.4] mmol/L, pCo2 48.0 [46.0-50.0] mm Hg) Had a Comparable Length of Hospital Stay Regardless of Type of Oxygen Support
Rate of Noninvasive Positive-Pressure Ventilation (NIPPV) Use in Patients with High Baseline Bicarbonate Group was Significantly Higher than that in Patients with Low Baseline Bicarbonate Group (19.4 % vs. 3.0 %, p < 0.0001)
Patients with High Bicarbonate in High-Flow Nasal Cannula (HFNC) Group Had a Lower Rate of Noninvasive Positive-Pressure Ventilation (NIPPV) Use, as Compared to Conventional Oxygen Therapy Group (15.4 % vs. 23.0 %, p = 0.217)
Nearly All Patients Who Require Emergency Department/Hospital-Based Treatment for a Chronic Obstructive Pulmonary Disease (COPD) Exacerbation Will Require a Course of Systemic Glucocorticoids
Dose/Route of Administration
General Comments
There is No Proven Clinical Benefit of Intravenous Corticosteroids (Methylprednisolone) Over Oral Corticosteroids (Prednisone) in the Setting of Chronic Obstructive Pulmonary Disease (COPD) Exacerbation (Chest, 2007) [MEDLINE] (Cochrane Database Syst Rev, 2014) [MEDLINE] (Eur Respir J, 2017) [MEDLINE]
Oral Corticosteroids are Rapidly Absorbed and Result in Peak Therapeutic Levels within 1 hr with Virtually Complete Bioavailability
Intravenous Corticosteroids are Generally Reserved for Use in the Setting of Respiratory Distress (Where Oral Medications May Be Difficult to Administer), Shock-Associated Decreased Splanchnic Perfusion (Where Oral Absorption May Be Impaired), etc
Prednisone 40 mg qday PO (or Equivalent) x 5 Days (see Prednisone)
Oral Prednisone is Generally Indicated for Patients with Non-Critically-Ill Hospitalized Patients with Chronic Obstructive Pulmonary Disease (COPD) Exacerbation
Methylprednisolone (Solumedrol) 60 mg q6-12 hrs IV (see Methylprednisolone)
Intravenous Methylprednisolone is Generally Indicated for Patients with Critically-Ill Patients with Chronic Obstructive Pulmonary Disease (COPD) Exacerbation
When Using High Initial Doses, Taper at the First Opportunity to Minimize Adverse Effects (Hypoglycemia, etc)
Clinical Efficacy-Corticosteroid Dose
Observational Study of Corticosteroid Dose and Outcome in the Setting of Chronic Obstructive Pulmonary Disease (COPD)) Exacerbation (JAMA, 2010) [MEDLINE]: n = 79,985
Study Excluded Patients Who Required Intensive Care
Median Glucocorticoid Dose Administered in the First 2 Days was Prednisone 60 mg Equivalent for Those on Oral Therapy and Prednisone 600 mg Equivalent for Intravenous Therapy
The Risk of Treatment Failure was No Greater with the Lower Corticosteroid Dose (Odds Ratio 0.93; 95% CI: 0.84-1.02)
Since This was an Observational Study (and Did Not Include Objective Measures of Airflow Limitation), it is Possible that Less Ill Patients were More Likely to Receive Oral Corticosteroid Treatment
Observational Cohort Study of Corticosteroid Dose and Outcome of Patients with Chronic Obstructive Pulmonary Disease (COPD)) Exacerbation in the Intensive Care Unit (ICU) Setting (Am J Respir Crit Care Med, 2014) [MEDLINE]: n = 17,000
Lower Methylprednisolone Dose of ≤240 mg/day vs Higher Methylprednisolone Dose (>240 mg/day), was not Associated with a Mortality Benefit, But was Associated with Slightly Shorter Hospital Stay (-0.44 days; 95% CI -0.67 to -0.21) and Intensive Care Unit (ICU) Stay (-0.31 days; 95% CI -0.46 to -0.16)
Length of Mechanical Ventilation and Need for Insulin Therapy were Lower in the Lower Dose Group
Duration
The Optimal Duration of Systemic Glucocorticoid Therapy is Not Well Established (and Depends on the Severity of the Exacerbation and the Response to Therapy) (Pulm Pharmacol Ther, 2016) [MEDLINE] (Eur Respir J, 2017) [MEDLINE] (Ann Emerg Med, 2018) [MEDLINE] (Cochrane Database Syst Rev, 2018) [MEDLINE] (Global Initiative for Chronic Obstructive Lung Disease/GOLD. Global Strategy for the Diagnosis, Management and Prevention of Chronic Obstructive Pulmonary Disease: 2026 Report) [LINK]
A Range of 5-14 Days is Reasonable, Consistent with the GOLD Guidelines (Eur Respir J, 2017) [MEDLINE] (Global Initiative for Chronic Obstructive Lung Disease/GOLD. Global Strategy for the Diagnosis, Management and Prevention of Chronic Obstructive Pulmonary Disease: 2026 Report) [LINK]
Clinical Efficacy-Duration of Corticosteroid Treatment
Systemic Corticosteroids in COPD Exacerbations (SCCOPE) Trial (NEJM, 1999) [MEDLINE]
Study Compared 2 and 8 wk Regimens and Found No Additional Benefit to the Longer Course
Patients in the 8 wk Group Experienced More Glucocorticoid-Related Adverse Effects
Reduction in the Use of Corticosteroids in Exacerbated COPD (REDUCE) Trial (JAMA, 2013) [MEDLINE]
Comparing Prednisone 40 mg qday for 5 or 14 Days, There was No Difference in Time to Next Exacerbation, Likelihood of an Exacerbation in the Subsequent 180 Days, or Recovery of Lung Function
Mean Cumulative Prednisone Dose was Significantly Higher in the 14 Day Group, But Treatment-Related Adverse Effects (Hyperglycemia, Hypertension, etc) were Not Different Between the Groups
Systematic Review of Corticosteroid Treatment in the Setting of COPD Exacrbation (Cochrane Database Syst Rev, 2018) [MEDLINE]
A 5 Day Course of Oral Glucocorticoids is Probably Comparable to a ≥14 Day Course, But Further Research is Required
REDUCE Trial (Above) was Included in the Analysis
CORTICO-COP Randomized Study of Eosinophil-Guided vs Standard Therapy in COPD Exacerbation (Lancet Respir Med, 2019) [MEDLINE]
Eosinophil-Guided Therapy was Noninferior to Standard Treatment in Days Alive and Out of Hospital within 14 Days of Treatment (Absolute Difference -0.4 Days; 95% CI: -1.3 to 0.5)
There was a 60% Decrease in Cumulative Prednisolone Dose and Les Hyperglycemia in the Intervention Group
Discontinuation vs Taper
At the End of the Treatment Course, Glucocorticoid Therapy May Be Discontinued Rather than Tapered if the Patient Has Recovered
Patients with a History of Worsened (or Recurrent Symptoms) After Glucocorticoid Discontinuation May Benefit from a 5-7 Day Taper if a Short Initial Duration was Chosen (i.e. 5 Days)
Tapering Solely Because of Concerns About Adrenal Suppression is Not Necessary if the Duration of Therapy is <3 wks (a Duration Too Brief to Cause Adrenal Atrophy
Efficacy
Systemic Glucocorticoids, When Added to Bronchodilator Therapies, Improve Symptoms, Improve Lung Function, and Decrease the Length of Hospital Stay (Global Initiative for Chronic Obstructive Lung Disease/GOLD. Global Strategy for the Diagnosis, Management and Prevention of Chronic Obstructive Pulmonary Disease: 2026 Report) [LINK]
Systematic Review and Meta-Analysis of XXX (Cochrane Database Syst Rev, 2014) [MEDLINE]: n = 917 (9 studies)
Systemic Glucocorticoids Decrease the Risk of Treatment Failure by >50%, as Compared to Placebo (Odds Ratio 0.48; 95% CI: 0.35-0.67)
In 2 Studies (n = 415), Systemic Glucocorticoids were Demonstrated to Decrease the Risk of Relapse at 1 Month (Hazard Ratio 0.78; 95% CI: 0.63-0.97)
For Every 9 Treated Patients, 1 Treatment Failure was Avoided
Patients in the Glucocorticoid Group Demonstrated Improvement in Forced Expiratory Volume in 1 Second (FEV1) Up to 72 hrs After Initiation, Though Not After that Time Point
Glucocorticoid Treatment Decrease the Length of Hospital Stay (Mean Difference -1.22 Days; 95% CI: -2.26 to -0.18)
Mortality Up to 30 Days was Not Decreased by Systemic Glucocorticoids
Risk of Hyperglycemia was Significantly Increased with Glucocorticoids, as Compared to Placebo (Odds ratio 2.79; 95% CI: 1.86-4.19).
Adverse Events
Even Short Courses of Systemic Glucocorticoids are Associated with an Increased Risk of Harm (Fracture, Hyperglycemia, Pneumonia, Sepsis, Venous Thromboembolism, etc)
Antibiotics
General Recommendation
Antibiotics are Generally Recommended for All Hospitalized Patients with a Chronic Obstructive Pulmonary Disease (COPD) Exacerbation (Global Initiative for Chronic Obstructive Lung Disease/GOLD. Global Strategy for the Diagnosis, Management and Prevention of Chronic Obstructive Pulmonary Disease: 2026 Report) [LINK]
Broader Empiric Antibiotic Regimens Should Be Used in the Following Two Risk Groups
Imipenem (see Imipenem): if unable to use a first-line agent
Meropenem (see Meropenem): if unable to use a first-line agent
Aminoglycoside (see Aminoglycoside): not a first-line agent
Use of Procalcitonin/C-Reactive Protein (CRP) to Guide the Use of Antibiotic Therapy
Procalcitonin/C-Reactive Protein (CRP) are Not Generally Helpful Over Clinical Judgement Alone in Deciding on Antibiotic Use in the Setting of Chronic Obstructive Pulmonary Disease (COPD) Exacerbation (Chest, 2007) [MEDLINE] (Cochrane Database Syst Rev, 2017) [MEDLINE] (Eur Respir Rev, 2017) [MEDLINE] (Intensive Care Med, 2018) [MEDLINE] (Eur Respir J, 2019) [MEDLINE] (NEJM, 2019) [MEDLINE]
Clinical Guidelines for Short-Course Antibiotics in Common Infections (Annals of Internal Medicine, 2021) [MEDLINE]
Antibiotic Treatment Duration Should Be Limited to 5 Days When Managing Patients with Chronic Obstructive Pulmonary Disease (COPD) Exacerbation and Acute Uncomplicated Bronchitis in Patients Who Have Clinical Signs of a Bacterial Infection (Presence of Increased Sputum Purulence, Increased Dyspnea, and/or Increased Sputum Volume)
Bronchodilator Properties thought to arise from inhibition of calcium influx into airway smooth muscle cells
Single Magnesium Sulfate 2g IV Dose over 20 min is Indicated for Poor Response to Bronchodilators or Acute Respiratory Failure
Clinical Efficacy
Cochrane Database Systematic Review of Magnesium Sulfate in the Treatment of COPD Exacerbation (Cochrane Database Syst Rev, 2022) [MEDLINE]
The best evidence for benefit in COPD exacerbations comes from a systematic review (3 studies, 170 participants) that found a decrease in hospitalizations with intravenous magnesium compared with placebo (odds ratio [OR] 0.45, 95% CI 0.23-0.88)
Ventilatory Support
Types
High-Flow Nasal Cannula (HFNC) Oxygen (see Oxygen)
life-threatening exacerbations, respiratory failure, or do not improve with supportive therapy with pharmacotherapy and oxygen
Prediction of Hypercapnic Respiratory Failure
Clinical Efficacy
XXXX
A Diagnostic Nomogram for Predicting Hypercapnic Respiratory Failure in Patients with Acute Exacerbation of Chronic Obstructive Pulmonary Disease. Int J Chron Obstruct Pulmon Dis. 2024 May 18:19:1079-1091. doi: 10.2147/COPD.S454558. eCollection 2024 [MEDLINE]
Purpose: To develop and validate a nomogram for assessing the risk of developing hypercapnic respiratory failure (HRF) in patients with acute exacerbation of chronic obstructive pulmonary disease (AECOPD)
Patients and methods: From January 2019 to August 2023, a total of 334 AECOPD patients were enrolled in this research. We employed the Least Absolute Shrinkage and Selection Operator (LASSO) regression and multivariate logistic regression to determine independent predictors and develop a nomogram. This nomogram was appraised by the area under the receiver operating characteristic curve (AUC), calibration curve, Hosmer-Lemeshow goodness-of-fit test (HL test), decision curve analysis (DCA), and clinical impact curve (CIC). The enhanced bootstrap method was used for internal validation
Results: Sex, prognostic nutritional index (PNI), hematocrit (HCT), and activities of daily living (ADL) were independent predictors of HRF in AECOPD patients. The developed nomogram based on the above predictors showed good performance. The AUCs for the training, internal, and external validation cohorts were 0.841, 0.884, and 0.852, respectively. The calibration curves and HL test showed excellent concordance. The DCA and CIC showed excellent clinical usefulness. Finally, a dynamic nomogram was developed (https://a18895635453.shinyapps.io/dynnomapp/)
Conclusion: This nomogram based on sex, PNI, HCT, and ADL demonstrated high accuracy and clinical value in predicting HRF. It is a less expensive and more accessible approach to assess the risk of developing HRF in AECOPD patients, which is more suitable for primary hospitals, especially in developing countries with high COPD-related morbidity and mortality.
Mucolytics for acute exacerbations of chronic obstructive pulmonary disease: a meta-analysis. Eur Respir Rev. 2023 Jan 25;32(167):220141. doi: 10.1183/16000617.0141-2022. Print 2023 Mar 31 [MEDLINE]
This meta-analysis explored the safety and effectiveness of mucolytics as an add-on treatment for chronic obstructive pulmonary disease (COPD) exacerbations
Based on a pre-registered protocol and following Cochrane methods, we systematically searched for relevant randomised or quasi-randomised controlled trials (RCTs)
We used the Risk of Bias v2 tool for appraising the studies and performed random-effect meta-analyses when appropriate
We assessed certainty of evidence using GRADE
This meta-analysis included 24 RCTs involving 2192 patients with COPD exacerbations, entailing at least some concerns of methodological bias. We demonstrated with moderate certainty that mucolytics increase the rate of treatment success (relative risk 1.37, 95% CI 1.08-1.73, n=383), while they also exert benefits on overall symptom scores (standardised mean difference 0.86, 95% CI 0.63-1.09, n=316), presence of cough at follow-up (relative risk 1.93, 95% CI 1.15-3.23) and ease of expectoration (relative risk 2.94, 95% CI 1.68-5.12)
Furthermore, low or very low certainty evidence suggests mucolytics may also reduce future risk of exacerbations and improve health-related quality of life, but do not impact on breathlessness, length of hospital stay, indication for higher level of care or serious adverse events. Overall, mucolytics could be considered for COPD exacerbation management
These findings should be validated in further, rigorous RCTs.
History : first used to treat COPD excerbation in the early 1990’s
Mechanisms
CPAP decreases auto-PEEP during COPD exacerbation -> decreases inspiratory load and work of breathing
Pressure support decreases work of breathing in COPD
Combined CPAP + pressure support (NIPPV) decreases transdiaphragmatic pressure more than each alone
Clinical Efficacy in COPD Exacerbation
NIPPV decreases pCO2, heart rate, respiratory rate, and dyspnea within the first hour of treatment
NIPPV decreases encephalopathy scores
The presence of hypercapneic encephalopathy or coma in COPD exacerbation is not a contraindication to NIPPV
NIPPV decreases intubation rate from 75% -> 25% of cases
NIPPV decreases mortality rate from 30% -> 10% of cases
Mortality rate may not be decreased in the subset of patients with pH <7.30 (at least in patients treated on general medical wards, outside of the ICU): this study suggested that patients with moore severe COPD exacerbation might have better outcomes if treated in the ICU, suggesting the importance of appropriate monitoring of NIPPV [MEDLINE]
Decreased mortality rate may not be observed with the USE of NIPPV in milder COPD exacerbations [MEDLINE]
Decreases mortality rate in the setting COPD exacerbation with concomitant pneumonia [MEDLINE]
NIPPV decreases complication rates and hospital length of stay
Clinical Efficacy of Noninvasive Positive-Pressure Ventilation (NIPPV)
NIPPV Decreased pCO2, Heart Rate, Respiratory Rate, and Dyspnea within the First Hour of Treatment
NIPPV Decreased Encephalopathy Scores
The Presence of Hypercapnic Encephalopathy or Coma in Chronic Obstructive Pulmonary Disease (COPD) Exacerbation is Not a Contraindication to NIPPV
NIPPV Decreased Complication Rates and Hospital Length of Stay
NIPPV Decreased Intubation Rate from 75% -> 25%
NIPPV Decreased Mortality Rate from 30% -> 10%
Decreased Mortality Rate May Not Be Observed with the Use of NIPPV in Milder COPD Exacerbations (Eur Resir J, 1996) [MEDLINE]
NIPPV decreased mortality rate in the setting COPD exacerbation with concomitant pneumonia (Am J Respir Crit Care MED, 1999) [MEDLINE]
Mortality rate may not be decreased in the subset of patients with pH <7.30 (at least in patients treated on general medical wards, outside of the ICU): this study suggested that patients with moore severe COPD exacerbation might have better outcomes if treated in the ICU, suggesting the importance of appropriate monitoring of NIPPV (Lancet, 2000) [MEDLINE]
Systematic Review and Meta-Analysis of Trials Using NIPPV for Prevention or Treatment of Acute Respiratory Failure or as a Tool to Facilitate Early Extubation (Crit Care Med, 2015) [MEDLINE]: n = 78 trials
Overall (in All Populations), NIPPV Decreased the Mortality Rate (at Longest F/U) with Relative Risk 0.73 (95% CI: 0.66–0.81) (p<0.001): number needed to treat = 19
Clinical Efficacy of Combination of Heliox + Noninvasive Positive-Pressure Ventilation (NIPPV)
HELIOX + NIPPV Decreased Airway Resistance and More Rapidly Improved Gas Exchange in COPD Exacerbation (Am J Respir Crit Care MED, 2000) [MEDLINE]
HELIOX + NIPPV Had No Benefit (in Terms of Intubation Rate, Mortality Rate, or Hospital Length of Stay) over NIPPV Alone in Randomized, Prospective Trial in COPD Exacerbation (Crit Care Med, 2003) [MEDLINE]
Clinical Efficacy
UK Randomized Trial of Home Noninvasive Ventilation Following Chronic Obstructive Pulmonary Disease (COPD) Exacerbation (JAMA, 2017)[MEDLINE]: n = 166
Exclusion Criteria: obesity (BMI >35), obstructive sleep apnea syndrome, or other cause of respiratory failure
In COPD Patients with Persistent Hypercapnia Following an Acute COPD Exacerbation, Adding Home Noninvasive Ventilation to Home Oxygen Therapy Prolonged the Time to Hospital Readmission or Death within 12 Months
The 12-Month Risk of Readmission or Death was 63.4% in the Home Oxygen Plus Home Noninvasive Ventilation Group vs 80.4% in the Home Oxygen Alone Group (Absolute Risk Reduction of 17.0%; 95% CI, 0.1%-34.0%)
Recommendations (ERS/ATS Clinical Practice Guidelines for Noninvasive Ventilation for Respiratory Failure, 2017) (Eur Respir J, 2017) [MEDLINE]
Background
Bilevel NIPPV May Theoretically Be Considered in Acute COPD Exacerbation in the Following Clinical Settings
Prevention of Acute Respiratory Acidosis in the Presence of COPD Exacerbation with Chronically Compensated Hypercapnia (with Normal pH)
Prevention of Endotracheal Intubation/Invasive Mechanical Ventilation in the Setting of COPD Exacerbation with Respiratory Failure and Mild-Moderate Acidemia
As an Alternative to Endotracheal Intubation/Invasive Mechanical Ventilation in the Setting of COPD Exacerbation with Respiratory Failure and Severe Acidemia
As the Only Method of Ventilatory Support in the Setting of COPD Exacerbation with Respiratory Failure in Patients Who are Not Candidates for or Decline Invasive Mechanical Ventilation
Bilevel NIPPV is Not Recommended as a Preventative Treatment in COPD Exacerbation with Hypercapnia without Acidemia (i.e. Chronic Hypercapnia with Metabolic Compensation) (Conditional Recommendation, Low Certainty of Evidence)
Bilevel NIPPV is Recommended for COPD Exacerbation and Acute/Acute on Chronic Hypoxemic, Hypercapnic Respiratory Failure and Acidemia (pH ≤7.35) (Strong Recommendation, High Certainty of Evidence)
Bilevel NIPPV Should Be Considered with pH ≤7.35, pCO2 >45 mmHg, and Respiratory Rate >20–24 Despite Standard Medical Therapy
There is No Lower Limit of pH Below Which a Trial of NIPPV is Contraindicated
However, the Lower the pH, the Greater the Risk of Failure, Suggesting that the Patient Be Closely Monitored with Rapid Access to Endotracheal Intubation/Invasive Mechanical Ventilation (Should the Need Arise)
A Trial of Bilevel NIPPV is Recommended in COPD Exacerbation and Acute/Acute on Chronic Respiratory Failure Who May Require Endotracheal Intubation/Invasive Mechanical Ventilation, Unless the Patient is Immediately Deteriorating (Strong Recommendation, Moderate Certainty of Evidence)
Respiratory failure unresponsive to NIPPV (or if patient is not a candidate for NIPPV) Clinical Efficacy-Heliox with Invasive Ventilation
Small Prospective Trial of Heliox in Mechanically Ventilated COPD Patients (Crit Care Med, 2000) [MEDLINE]: n = 23
In Mechanically-Ventilated COPD Patients with Auto-PEEP (5+/-2.7 cm H2O vs 9+/-2.5 cm H2O), Heliox Decreased Trapped Lung Volume, Auto-PEEP, Peak Inspiratory Pressure (25+/-6 cm H2O vs 30+/-5 cm H2O), and Mean Airway Pressure, as Compared to Usual Care
In Mechanically-Ventilated COPD Patients with Auto-PEEP, Heliox Did Not Impact Hemodynamics or Arterial Blood Gases
Treatments with No Demonstrated Clinical Benefit in Acute Chronic Obstructive Pulmonary Disease (COPD) Exacerbation
Trial of Extracorporeal Carbon Dioxide Removal (as Add-On Therapy to Noninvasive Positive-Pressure Ventilation) in the Treatment of Chronic Obstructive Pulmonary Disease (COPD) Exacerbation with Hypercapnic Respiratory Failure (Ann Intensive Care, 2022) [MEDLINE]: n = 18
As Compared to Noninvasive Positive-Pressure Ventilation (NIPPV) Alone, Noninvasive Ventilation and ECCO2R Resulted in Increased ICU and Hospital Length of Stay with No Difference in 90-Day Mortality or Functional Outcomes
Systematic Review of Magnesium Sulfate in Acute Chronic Obstructive Pulmonary Disease (COPD) Exacerbation (Ann Thorac Med, 2014) [MEDLINE]: trials were cited as poor -> further study is required
Intravenous Magnesium Sulfate: did not have an immediate bronchodilatory effect, but potentiates the bronchodilatory effect of inhaled beta-2 agonists
Nebulized Magnesium Sulfate: no benefit (in terms of FEV1 or need for hospital admission), as compared to salbutamol alone
Combined Intravenous and Nebulized Magnesium Sulfate: no benefit in terms of hospital admission/intubation/death, as compared to nebulized ipratropium bromide (but the nebulized ipratropium bromide group had a better bronchodilator effect and improvement in arterial blood gas parameters)
Australian New Zealand Clinical Trials Registry Study of Nebulized Magnesium Sulfate Added to Salbutamol in Acute Chronic Obstructive Pulmonary Disease (COPD) Exacerbation (Thorax, 2013) [MEDLINE]: no benefit (in terms of FEV1 or need for hospital admission), as compared to salbutamol alone
Systematic Review of Magnesium Sulfate in Acute Chronic Obstructive Pulmonary Disease (COPD) Exacerbation (Ann Thorac Med, 2014) [MEDLINE]: trials were cited as poor -> further study is required
Intravenous Magnesium Sulfate: did not have an immediate bronchodilatory effect, but potentiates the bronchodilatory effect of inhaled β2 agonists
Nebulized Magnesium Sulfate: no benefit (in terms of FEV1 or need for hospital admission), as compared to salbutamol alone
Combined Intravenous and Nebulized Magnesium Sulfate: no benefit in terms of hospital admission/intubation/death, as compared to nebulized ipratropium bromide (but the nebulized ipratropium bromide group had a better bronchodilator effect and improvement in arterial blood gas parameters)
Combined Intravenous and Nebulized Magnesium Sulfate (see Magnesium Sulfate)
Systematic Review of Magnesium Sulfate in Acute Chronic Obstructive Pulmonary Disease (COPD) Exacerbation (Ann Thorac Med, 2014) [MEDLINE]: trials were cited as poor -> further study is required
Intravenous Magnesium Sulfate: did not have an immediate bronchodilatory effect, but potentiates the bronchodilatory effect of inhaled beta-2 agonists
Nebulized Magnesium Sulfate: no benefit (in terms of FEV1 or need for hospital admission), as compared to salbutamol alone
Combined Intravenous and Nebulized Magnesium Sulfate: no benefit in terms of hospital admission/intubation/death, as compared to nebulized ipratropium bromide (but the nebulized ipratropium bromide group had a better bronchodilator effect and improvement in arterial blood gas parameters)
Prognosis
Mortality Rate is Related to the GOLD Spirometric Class (GOLD; Global Strategy for Diagnosis, Management, and Prevention of COPD, 2016) [LINK]
Longitudinal changes in maximal forced inspiratory flow and clinical outcomes in COPD patients. Chest. Published online August 14, 2024. doi:10.1016/j.chest.2024.07.162 [MEDLINE]
Background: COPD primarily impairs expiratory flow due to progressive airflow obstruction and reduced lung elasticity. Increasing evidence underlines the importance of inspiratory flow as a biomarker for selecting inhaler devices and providing ancillary aerodynamic information
Research question: Does the longitudinal changes in maximum forced inspiratory flow (FIFmax) influence acute exacerbations and lung function decline in patients with COPD?
Study design and methods: This longitudinal study evaluated FIFmax in patients with COPD over a 7-year period from 2004 to 2020. Eligible patients were categorized into 2 groups based on FIFmax trajectory: the increased FIFmax group and the decreased FIFmax group. The study assessed the annual rate of acute exacerbations and the annual decline rate of FEV1. Subgroup analyses were conducted based on treatment status, with a focus on inhaled therapy and inhaler device usage
Results: Among the eligible 956 patients with COPD, 56.5% belonged to the increased FIFmax group. After propensity score matching, the increased FIFmax group experienced lower rates of severe exacerbations (0.16 per year vs 0.25 per year, P = .017) and a slower decline in FEV1 (0 [interquartile range, -51 to 71] mL/y vs -43 [interquartile range, -119 to 6] mL/y; P < .001) compared with the decreased FIFmax group. These associations were particularly prominent in patients using specific inhaler therapies such as dry powder inhalers
Interpretation
This study showed that the longitudinal changes in FIFmax are associated with clinical outcomes in patients with COPD
Patients with increased FIFmax experienced a lower rate of severe exacerbations and a slower decline in lung function
These findings suggest the potential benefits of optimizing inspiratory flow in COPD management, although further studies are needed to confirm these observations due to potential confounding factors
Predictors of Mortality in Chronic Obstructive Pulmonary Disease
BODE Index
BMI: low BMI
Obstruction: degree of airway obstruction by PFT’s
Dyspnea
Medical Research Council (MRC) Dyspnea Scale
Grades 1 and 2 = mild disability, while grades 3-5 = moderate to severe disability
Grade 1) I only get breathless with strenuous exercise
Grade 2) I get short of breath when hurrying on the level or walking up a slight hill
Grade 3) I walk slower than people of the same age on the level because of breathlessness, or I have to stop for breath when walking on my own pace on the level
Grade 4) I stop for breath after walking about 100 yards or after a few minutes on the level
Grade 5) I am too breathless to leave the house or I am breathless when dressing or undressing
Exercise Capacity: poor exercise capacity (as assessed by clinical symptoms or 6-minute walk test)
Prediction of COPD Mortality with 6-Minute Walk Test (see 6-Minute Walk Test)
Cohort Study Examining the Predictive Value of Emphysematous Changes on Chest CT (Ann Int Med, 2014) [MEDLINE]
Presence of Emphysematous Changes on CT Imaging in Patients without Spirometrically-Defined COPD were Linearly Associated with Increased All-Cause Mortality: even after adjusting for confounding variables, such as cardiovascular risk factors and FEV1
The Association was of the Greatest Magnitude Among Smokers
Frailty
xxx
Prevalence and clinical impact of frailty in COPD: a systematic review and meta-analysis. BMC Pulm Med. 2023;23(1):164. doi:10.1186/s12890-023-02454-z [MEDLINE]
Background: Frailty has been increasingly identified as a risk factor of adverse outcomes in chronic obstructive pulmonary disease (COPD). The prevalence and impact of frailty on health outcomes in people with COPD require clarification
Methods: PubMed, Embase, The Cochrane Library and Web of Science (January 1, 2002, to July 1, 2022) were comprehensively searched to identify studies related to frailty and COPD. Comparisons were made between people who did and did not have frailty for pulmonary function, dyspnea severity, 6-minute walking distance, activities of daily life, and mortality
Results: Twenty studies (9 cross-sectional, 10 cohort studies,1 clinical trial) from Europe (9), Asia (6), and North and South America (4), Oceania (1) involving 11, 620 participants were included. The prevalence of frailty was 32.07% (95% confidence interval (CI) 26.64-37.49) with a range of 6.43-71.70% based on the frailty tool used. People with frailty had lower predicted forced expiratory volume in the first second (mean difference – 5.06%; 95%CI -6.70 to -3.42%), shorter 6-minute walking distance (mean difference – 90.23 m; 95%CI -124.70 to -55.76), poorer activities of daily life (standardized mean difference – 0.99; 95%CI -1.35 to -0.62), higher CAT(COPD Assessment Test) score(mean difference 6.2; 95%CI 4.43 to 7.96) and mMRC (modified Medical Research Council) grade (mean difference 0.93; 95%CI 0.85 to 1.02) compared with those who did not (P < 0.001 for all). Meta-analysis showed that frailty was associated with an increased risk of long-term all-cause mortality (HR 1.68; 95% CI 1.37-2.05; I2 = 0%, P < 0.001)
Conclusion: Frailty is prevalent in people with COPD and linked with negative clinical outcomes including pulmonary function, dyspnea severity, exercise capacity, quality of life and mortality.
Systemic Inflammation
xx
Association between systemic immune-inflammation index and chronic obstructive pulmonary disease: A population-based study. BMC Pulm Med. Published online August 10, 2023. doi:10.1186/s12890-023-02583-5 [MEDLINE]
Background: The Systemic Immune-Inflammation Index (SII) is a quantitative measurement of the systemic immune-inflammatory response in the human body. The SII has been shown to have prognostic value in various clinical settings, including critical illness, sepsis, and cancer. Its role in chronic obstructive pulmonary disease (COPD) remains unclear and requires further investigation
Methods: We analyzed demographic data from 16,636 participants in the National Health and Nutrition Examination Survey. Logistic regression analysis was performed to assess the correlation between COPD, lung function, chronic respiratory symptoms and SII. We used Cox proportional hazards (PH) model to analyze the relationship between SII and mortality in COPD patients and healthy individuals. We used propensity score matching (PSM) method to match the COPD population with similar baseline levels with the normal population to further analyze the correlation between SII and COPD
Results: We recruited 16,636 participants, ages 40 and above, for the study. A multivariable logistic regression analysis revealed that a higher SII level was independently associated with an elevated likelihood of COPD (Odds Ratio (OR) = 1.449; 95% Confidence Interval (CI): 1.252-1.676, P < 0.0001) after controlling for all other factors. Results of subgroup analysis showed a significant positive correlation between SII and COPD in different age groups, gender, Body Mass Index, smoking status, and those with a history of hypertension. The SII index had positive correlation with COPD after PSM (OR = 1.673; 95%CI: 1.443-1.938). After full adjustment, an increase in the SII is associated with a higher all-cause mortality rate. The hazard ratio (HR) with a 95% CI in the general population, COPD patients, and healthy individuals are 1.161 (1.088, 1.239), 1.282 (1.060, 1.550), and 1.129 (1.055, 1.207), respectively
Conclusions: Higher SII levels are linked to higher prevalence of COPD. COPD patients with a higher SII levels have a higher risk of all-cause mortality. Additional large-scale, long-term studies are necessary to confirm these results.
Mortality After Hospital Admission
Research Letter Studying the Mortality Rate in COPD Following Hospitalization for Pneumonia vs Acute Exacerbation (Eur Respir J, 2022) [MEDLINE]
In patients with chronic obstructive pulmonary disease (COPD), the 30-day risk of death was higher after hospitalization for pneumonia than after hospitalization for a severe COPD exacerbation
Characteristics, treatments, in-hospital and long-term outcomes among inpatients with acute exacerbation of chronic obstructive pulmonary disease in China: sex differences in a large cohort study. BMC Pulm Med. 2024;24(1):125. doi:10.1186/s12890-024-02948-4 [MEDLINE]
Background: Data related to the characteristics, treatments and clinical outcomes of acute exacerbation of chronic obstructive pulmonary disease (AECOPD) patients in China are limited, and sex differences are still a neglected topic
Methods: The patients hospitalized for AECOPD were prospectively enrolled from ten medical centers in China between September 2017 and July 2021. Patients from some centers received follow-up for 3 years. Data regarding the characteristics, treatments and in-hospital and long-term clinical outcomes from male and female AECOPD patients included in the cohort were analyzed and compared
Results: In total, 14,007 patients with AECOPD were included in the study, and 11,020 (78.7%) were males. Compared with males, female patients were older (74.02 ± 10.79 vs. 71.86 ± 10.23 years, P < 0.001), and had more comorbidities (2.22 ± 1.64 vs. 1.73 ± 1.56, P < 0.001), a higher frequency of altered mental status (5.0% vs. 2.9%, P < 0.001), lower diastolic blood pressure (78.04 ± 12.96 vs. 79.04 ± 12.47 mmHg, P < 0.001). In addition, there were also significant sex differences in a range of laboratory and radiographic findings. Females were more likely to receive antibiotics, high levels of respiratory support and ICU admission than males. The in-hospital and 3-year mortality were not significantly different between males and females (1.4% vs. 1.5%, P = 0.711; 35.3% vs. 31.4%, P = 0.058), while female smokers with AECOPD had higher in-hospital mortality than male smokers (3.3% vs. 1.2%, P = 0.002) and male smokers exhibited a trend toward higher 3-year mortality compared to female smokers (40.7% vs. 33.1%, P = 0.146)
Conclusions
In AECOPD inpatients, females and males had similar in-hospital and long-term survival despite some sex differences in clinical characteristics and treatments, but female smokers had significantly worse in-hospital outcomes than male smokers
Increased Risk of Morbidity/Mortality in the Setting of Chronic Obstructive Pulmonary Disease (COPD)
Obesity Is Associated With Increased Morbidity in Moderate to Severe COPD. Chest. 2017 Jan;151(1):68-77. doi: 10.1016/j.chest.2016.08.1432 [MEDLINE]
Background: Obesity is prevalent in the United States; however, the impact of obesity on COPD morbidity is unclear. We hypothesized that obesity is associated with worse outcomes in COPD
Methods: We examined 3,631 participants from the multicenter prospective cohort study Genetic Epidemiology of COPD (COPDGene) who had spirometry-confirmed COPD, a postbronchodilator FEV1 < 80% predicted, and a BMI ≥ 18.5 kg/m2. We conducted logistic and linear regression analyses to determine the association between COPD outcomes and obesity class, adjusting for relevant confounders. The referent for obesity classes included normal/overweight individuals (BMI range, 18.5-29.9 kg/m2)
Results: Overall, 35% of participants were obese, with 21% class I (BMI range, 30-34.9 kg/m2), 9% class II (BMI range, 35-39.9 kg/m2), and 5% class III (BMI ≥ 40 kg/m2). The number of comorbidities increased with increasing obesity class (P < .001). Increasing obesity class was independently associated with worse respiratory-specific and general quality of life (QOL) (St. George’s Respiratory Questionnaire score and Short Form-36 score version 2, respectively), reduced 6-min walk distance (6MWD), increased dyspnea (Modified Medical Research Council score ≥ 2), and greater odds of severe acute exacerbation of COPD (AECOPD). The associations between obesity and worse outcomes were independent of the presence of comorbidities, except in the case of SF-36 and severe exacerbations
Conclusions: Obesity is prevalent among individuals with COPD and associated with worse COPD-related outcomes, ranging from QOL and dyspnea to 6MWD and severe AECOPD. These associations were strengthened when obesity was analyzed as a dose-dependent response. Obesity in patients with COPD may contribute to a worse COPD-related course.
Hospitalization Outcomes of Patients with Asthma, COPD, and Asthma-COPD Overlap Syndrome. Chronic Obstr Pulm Dis. 2025 Jul 30;12(4):260-273. doi: 10.15326/jcopdf.2024.0566 [MEDLINE]
Background and objectives: Chronic obstructive pulmonary disease (COPD) and asthma account for a significant health care burden within the United States. The asthma-COPD overlap (ACO) phenotype has been associated with increased exacerbation frequency and health care utilization compared to either disease alone. However, hospital-based outcomes of these diagnoses have not been described in the literature
Methods: Hospitalization data were extracted from the Healthcare Cost and Utilization Project Nationwide Readmissions Database (HCUP-NRD 2012-2015). Using International Classification of Diseases, Ninth Revision, Clinical Modification codes, we classified patients as having asthma, COPD, or ACO. We used analytic sample weights to compute national estimates, and weighted regression analyses to evaluate hospitalization outcomes
Results: Of 2,522,013 patients reviewed, 1,732,946 (68.7%) had COPD, 668,867 (26.5%) had asthma, and 120,200 (4.8%) had ACO. Patients with ACO were younger than those with COPD (63 versus 69 years old, p< 0.05), with a higher rate of respiratory failure and an increased hospital length of stay. Index admission mortality was higher in patients with COPD (adjusted odds ratios [OR] [95%]: 2.10 [1.84; 2.40]) and asthma (adjusted OR [95%]: 1.59 [1.38; 1.83]) as compared to those with ACO. However, the all-cause readmission rate was higher in the COPD group (15.7%) but not in the asthma group (10.7%) as compared to the ACO group (11.5%)
Conclusion: While ACO was associated with higher rates of baseline comorbidities, increased length of stay, and higher health care cost during index admission, this did not translate into higher in-hospital mortality, complication rates, or risk for asthma-related readmission mortality when compared to asthma or COPD alone, highlighting the complexity of the ACO disease burden
References
General
Role of hypoxia in the pulmonary hypertension of chronic bronchitis and emphysema. Scand J Respir Dis Suppl. 1971;77:61 [MEDLINE]
Prognostic value of pulmonary artery pressure in chronic obstructive pulmonary disease. Thorax 1981;36:752–8 [MEDLINE]
Usefulness of the Medical Research Council (MRC) dyspnoea scale as a measure of disability in patients with chronic obstructive pulmonary disease. Thorax. 1999;54(7):581-586
The body-mass index, airflow obstruction, dyspnea, and exercise capacity index in chronic obstructive pulmonary disease. N Engl J Med. 2004;350(10):1005-1012.
Pulmonary hemodynamics in advanced COPD candidates for lung volume reduction surgery or lung transplantation. Chest 2005;127:1531–6 [MEDLINE]
Severe pulmonary hypertension and chronic obstructive pulmonary disease. Am J Respir Crit Care Med 2005;172:189–94 [MEDLINE]
The modified BODE index: validation with mortality in COPD. Eur Respir J. 2008;32(5):1269-1274
Anxiety and depression in COPD: current understanding, unanswered questions, and research needs. Chest. 2008 Oct;134(4 Suppl):43S-56S. doi: 10.1378/chest.08-0342 [MEDLINE]
Global Initiative for Chronic Obstructive Lung Disease: Global Strategy for the Diagnosis, Management and Prevention of Chronic Obstructive Lung Disease Updated 2008. Available at: https://www.goldcopd.org/Guidelineitem.asp?l1=2&l2=1&intId=2003. Accessed December 15, 2009
Prevalence of major comorbidities in subjects with COPD and incidence of myocardial infarction and stroke: a comprehensive analysis using data from primary care. Thorax. 2010;65(11):956–962 [MEDLINE]
Family History Is a Risk Factor for COPD. Chest 2011; 140 (2): 343-350 [MEDLINE]
ECLIPSE Trial. Six-minute-walk test in chronic obstructive pulmonary disease: minimal clinically important difference for death or hospitalization. Am J Respir Crit Care Med 2013;187:382-386 [MEDLINE]
Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012;380:2095-2128 [MEDLINE]
Association between emphysema-like lung on cardiac computed tomography and mortality in persons without airflow obstruction: A cohort study. Ann Intern Med 2014;161:863-873 [MEDLINE]
Chronic productive cough is associated with death in smokers with early COPD. COPD. 2014 Aug;11(4):451-8. doi: 10.3109/15412555.2013.837870. Epub 2013 Oct 15 [MEDLINE]
Relation of chronic obstructive pulmonary disease to atrial and ventricular arrhythmias. Am J Cardiol. 2014 Jul 15;114(2):272-7 [MEDLINE]
Global Initiative for Chronic Obstructive Lung Disease (GOLD); Global Strategy for Diagnosis, Management, and Prevention of COPD, 2016 [LINK]
Epidemiology
Incidence of chronic obstructive pulmonary disease in people with HIV in Ontario, 1996-2015: a retrospective population-based cohort study. CMAJ Open. 2020 Feb 18;8(1):E83-E89. doi: 10.9778/cmajo.20190028 [MEDLINE]
Diagnosis
Stronger associations of centrilobular than paraseptal emphysema with longitudinal changes in diffusing capacity and mortality in COPD. Chest. Published online January 31, 2023. doi:10.1016/j.chest.2023.01.034 [MEDLINE]
Clinical Manifestations
Neurologic Manifestations
Association of rest-activity circadian rhythm with chronic respiratory diseases, a cross-section survey from NHANES 2011-2014. Respir Med. 2023 Feb 6;209:107147. doi: 10.1016/j.rmed.2023.107147 [MEDLINE]
Pulmonary Manifestations
Nocturnal Hypoxemia
Nocturnal oxyhemoglobin desaturation in COPD patients with arterial oxygen tensions above 60 mm Hg. Chest. 1987;92(4):604 [MEDLINE]
A double-blind trial of nocturnal supplemental oxygen for sleep desaturation in patients with chronic obstructive pulmonary disease and a daytime PaO2 above 60 mm Hg. Am Rev Respir Dis. 1992;145(5):1070 [MEDLINE]
Severe pulmonary hypertension in COPD – impact on survival and diagnostic approach. CHEST. Published online January 2, 2022. doi: 10.1016/j.chest.2022.01.031 [MEDLINE]
Chronic obstructive pulmonary disease. N Engl J Med. 2000;343(4):269 [MEDLINE]
Bacteria in exacerbations of chronic obstructive pulmonary disease: phenomenon or epiphenomenon? Proc Am Thorac Soc. 2004;1(2):109-14. doi: 10.1513/pats.2306029 [MEDLINE]
Pulmonary embolism in patients with unexplained exacerbation of chronic obstructive pulmonary disease: prevalence and risk factors. Ann Intern Med. 2006;144(6):390 [MEDLINE]
Infection in the pathogenesis and course of chronic obstructive pulmonary disease. N Engl J Med. 2008;359(22):23 [MEDLINE]
Prevalence of viral infection detected by PCR and RT-PCR in patients with acute exacerbation of COPD: a systematic review. Respirology. 2010 Apr;15(3):536-42 [MEDLINE]
The effect of cold temperature on increased exacerbation of chronic obstructive pulmonary disease: a nationwide study. PLoS One. 2013;8(3):e57066 [MEDLINE]
Associations of ambient air pollution with chronic obstructive pulmonary disease hospitalization and mortality. Am J Respir Crit Care Med. 2013;187(7):721 [MEDLINE]
Heat, heat waves, and hospital admissions among the elderly in the United States, 1992-2006. Environ Health Perspect. 2014;122(11):1187 [MEDLINE]
Short-term Exposure to Ambient Fine Particulate Matter Increases Hospitalizations and Mortality in COPD: A Systematic Review and Meta-analysis. Chest. 2016;149(2):447 [MEDLINE]
Synergistic effects of temperature and humidity on the symptoms of COPD patients. Int J Biometeorol. 2017;61(11):1919 [MEDLINE]
Trends in moderate and severe exacerbations among COPD patients in the UK from 2005 to 2013. Respir Med. 2018;144:1 [MEDLINE]
Pulmonary Embolism Among Patients With Acute Exacerbation Of Chronic Obstructive Pulmonary Disease: Implications For Emergency Medicine. J Emerg Med. 2018;55(3):339 [MEDLINE]
Incidence and Impact of Pulmonary Embolism During Severe COPD Exacerbation. Respir Care. 2019;64(12):1531 [MEDLINE]
Differences in COPD Exacerbation Risk Between Women and Men: Analysis From the UK Clinical Practice Research Datalink Data. Chest. 2019;156(4):674 [MEDLINE]
Analysis of environmental risk factors for chronic obstructive pulmonary disease exacerbation: A case-crossover study (2004-2013). PLoS One. 2019;14(5):e0217143 [MEDLINE]
Prevalence of Pulmonary Embolism Among Patients With COPD Hospitalized With Acutely Worsening Respiratory Symptoms. JAMA. 2021;325(1):59 [MEDLINE]
Effect of a Pulmonary Embolism Diagnostic Strategy on Clinical Outcomes in Patients Hospitalized for COPD Exacerbation: A Randomized Clinical Trial. JAMA. 2021;326(13):1277 [MEDLINE]
Prevalence of pulmonary embolism in patients with acute exacerbations of COPD: A systematic review and meta-analysis. Am J Emerg Med. 2021;50:606 [MEDLINE]
Randomized Clinical Trial of Air Cleaners to Improve Indoor Air Quality and Chronic Obstructive Pulmonary Disease Health: Results of the CLEAN AIR Study. Am J Respir Crit Care Med. 2022;205(4):421 [MEDLINE]
The impact of personal and outdoor temperature exposure during cold and warm seasons on lung function and respiratory symptoms in COPD. ERJ Open Res. 2022;8(1) [MEDLINE]
Short-term air pollution exposure and exacerbation events in mild to moderate COPD: a case-crossover study within the CanCOLD cohort. Thorax. 2023;78(10):974. [MEDLINE]
Prevalence, Risk Factor and Clinical Characteristics of Venous Thrombus Embolism in Patients with Acute Exacerbation of COPD: A Prospective Multicenter Study. Int J Chron Obstruct Pulmon Dis. 2023;18:907 [MEDLINE]
Air pollution and respiratory health in patients with COPD: should we focus on indoor or outdoor sources? Thorax. 2024;79(12):1116 [MEDLINE]
Treatment
General
Salmeterol plus theophylline combination therapy in the treatment of COPD. Chest 2001;119:1661-1670 [MEDLINE]
Short-term vs Conventional Glucocorticoid Therapy in Acute Exacerbations of Chronic Obstructive Pulmonary Disease. The REDUCE Randomized Clinical Trial. JAMA. 2013 Jun 5;309(21):2223-31. doi: 10.1001/jama.2013.5023 [MEDLINE]
Prevention of acute exacerbations of COPD: American College of Chest Physicians and Canadian Thoracic Society Guideline. Chest. 2015 Apr;147(4):894-942. doi: 10.1378/chest.14-1676 [MEDLINE]
Vaccination
Injectable vaccines for preventing pneumococcal infection in patients with chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2010 Nov 10;(11):CD001390. doi: 10.1002/14651858.CD001390.pub3 [MEDLINE]
Out-patient rehabilitation improves activities of daily living, quality of life and exercise tolerance in chronic obstructive pulmonary disease. Eur Respir J. 1997;10(12):2801-2806
Meta-analysis of respiratory rehabilitation in chronic obstructive pulmonary disease. A Cochrane systematic review. Eura Medicophys. 2007;43(4):475-485
Optimizing pulmonary rehabilitation in chronic obstructive pulmonary disease–practical issues: a Canadian Thoracic Society Clinical Practice Guideline. Can Respir J. 2010 Jul-Aug;17(4):159-68 [MEDLINE]
Pulmonary rehabilitation following exacerbations of chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2011 Oct 5;(10):CD005305. doi: 10.1002/14651858.CD005305.pub3 [MEDLINE]
British Thoracic Society guideline on pulmonary rehabilitation in adults. Thorax. 2013 Sep;68 Suppl 2:ii1-30. doi: 10.1136/thoraxjnl-2013-203808 [MEDLINE]
Depressed mood predicts pulmonary rehabilitation completion among women, but not men. Respir Med. 2014 Jul;108(7):1007-13. doi: 10.1016/j.rmed.2014.04.010. Epub 2014 Apr 26 [MEDLINE]
Pulmonary Rehabilitation as a Mechanism to Reduce Hospitalizations for Acute Exacerbations of COPD: A Systematic Review and Meta-Analysis. Chest. 2016 Oct;150(4):837-859. doi: 10.1016/j.chest.2016.05.038. Epub 2016 Aug 3 [MEDLINE]
Physical and affective components of dyspnoea are improved by pulmonary rehabilitation in COPD. BMJ Open Respir Res. 2022 Jan;9(1):e001160. doi: 10.1136/bmjresp-2021-001160 [MEDLINE]
Long-term results of continuous oxygen therapy at sea level. Chest. 1975;68(4):486 [MEDLINE]
Continuous or nocturnal oxygen therapy in hypoxemic chronic obstructive lung disease: a clinical trial. Nocturnal Oxygen Therapy Trial Group. Ann Intern Med. 1980;93(3):391 [MEDLINE]
Long term domiciliary oxygen therapy in chronic hypoxic cor pulmonale complicating chronic bronchitis and emphysema. Report of the Medical Research Council Working Party. Lancet. 1981;1(8222):681 [MEDLINE]
Psychologic effects of continuous and nocturnal oxygen therapy in hypoxemic chronic obstructive pulmonary disease. Arch Intern Med. 1983;143(10):1941 [MEDLINE]
Evolution of physiological variables in patients with chronic obstructive pulmonary disease before and during long-term oxygen therapy. Respiration. 1991;58(3-4):126 [MEDLINE]
Psychological status of COPD patients before and after one year of long-term oxygen therapy. Monaldi Arch Chest Dis. 1996;51(1):7 [MEDLINE]
Long-term home care programmes may reduce hospital admissions in COPD with chronic hypercapnia. Eur Respir J. 1996;9(8):1605 [MEDLINE]
Does long-term oxygen therapy affect quality of life in patients with chronic obstructive pulmonary disease and severe hypoxaemia? Eur Respir J. 1996;9(11):2335 [MEDLINE]
Effect of long-term oxygen therapy on survival in patients with chronic obstructive pulmonary disease with moderate hypoxaemia. Thorax. 1997;52(8):674 [MEDLINE]
A randomized trial of nocturnal oxygen therapy in chronic obstructive pulmonary disease patients. Eur Respir J. 1999;14(5):1002 [MEDLINE]
Dose-response effect of oxygen on hyperinflation and exercise endurance in nonhypoxaemic COPD patients. Eur Respir J. 2001;18(1):77 [MEDLINE]
Enhancement of exercise performance in COPD patients by hyperoxia: a call for research. Chest. 2002;122(5):1830 [MEDLINE]
Does long-term oxygen therapy reduce hospitalisation in hypoxaemic chronic obstructive pulmonary disease? Eur Respir J. 2002;20(1):38 [MEDLINE]
Long-term oxygen therapy improves health-related quality of life. Respir Med. 2004;98(4):285 [MEDLINE]
Long-term oxygen therapy stops the natural decline of endurance in COPD patients with reversible hypercapnia. Respiration. 2004;71(4):342 [MEDLINE]
Long-term oxygen treatment in chronic obstructive pulmonary disease: recommendations for future research: an NHLBI workshop report. Am J Respir Crit Care Med. 2006;174(4):373 [MEDLINE]
Short burst oxygen therapy after activities of daily living in the home in chronic obstructive pulmonary disease. Thorax. 2007;62(8):702 [MEDLINE]
Effect of oxygen on health quality of life in patients with chronic obstructive pulmonary disease with transient exertional hypoxemia. Am J Respir Crit Care Med. 2007;176(4):343 [MEDLINE]
Effect of high flow oxygen on mortality in chronic obstructive pulmonary disease patients in prehospital setting: randomised controlled trial. BMJ. 2010;341:c5462 [MEDLINE]
Oxygen therapy for patients with COPD: current evidence and the long-term oxygen treatment trial. Chest. 2010;138(1):179 [MEDLINE]
LOTT Trial. A Randomized Trial of Long-Term Oxygen for COPD with Moderate Desaturation. N Engl J Med. 2016;375(17):1617 [MEDLINE]
Long-Acting β2-Agonists (LABA)
Combined corticosteroid and long-acting beta(2)-agonist in one inhaler versus placebo for chronic obstructive pulmonary disease. Cochrane Database Syst Rev 2013;11:CD003794 [MEDLINE]
Long-acting beta2-agonist in addition to tiotropium versus either tiotropium or long-acting beta2-agonist alone for chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2015 Oct 22;(10):CD008989. doi: 10.1002/14651858.CD008989.pub3 [MEDLINE]
Long-Acting Muscarinic Antagonists (LAMA)
Tiotropium versus placebo for chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2012 Jul 11;7:CD009285. doi: 10.1002/14651858.CD009285.pub2 [MEDLINE]
Long-acting beta2-agonist in addition to tiotropium versus either tiotropium or long-acting beta2-agonist alone for chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2015 Oct 22;(10):CD008989. doi: 10.1002/14651858.CD008989.pub3 [MEDLINE]
Randomised, double blind, placebo controlled study of fluticasone propionate in patients with moderate to severe chronic obstructive pulmonary disease: the ISOLDE trial. BMJ 2000;320:1297-303 [MEDLINE]
Salmeterol and fluticasone propionate and survival in chronic obstructive pulmonary disease. N Engl J Med 2007; 356:775-89 [MEDLINE]
Effect of fluticasone propionate/salmeterol (250/50) on COPD exacerbations and impact on patient outcomes. COPD. 2009;6(5):320-329
Safety and efficacy of combined long-acting beta-agonists and inhaled corticosteroids vs long-acting beta-agonists monotherapy for stable COPD: a systematic review. Chest. 2009;136(4):1029-1038
Pneumonia risk in COPD patients receiving inhaled corticosteroids alone or in combination: TORCH study results. Eur Respir J. 2009; 34(3):641-647 [MEDLINE]
Combined corticosteroid and long-acting beta(2)-agonist in one inhaler versus placebo for chronic obstructive pulmonary disease. Cochrane Database Syst Rev 2013;11:CD003794 [MEDLINE]
Influence of previous use of inhaled corticoids on the development of pleural effusion in community-acquired pneumonia. Am J Respir Crit Care Med. 2013;187(11):1241 [MEDLINE]
WISDOM Investigators. Withdrawal of inhaled glucocorticoids and exacerbations of COPD. N Engl J Med 2014;371:1285-1294 [MEDLINE]
Withdrawal of inhaled corticosteroids can be safe in COPD patients at low risk of exacerbation: a real-life study on the appropriateness of treatment in moderate COPD patients (OPTIMO). Respir Res. 2014 Jul 8;15:77. doi: 10.1186/1465-9921-15-77 [MEDLINE]
ETHOS Trial. Triple Inhaled Therapy at Two Glucocorticoid Doses in Moderate-to-Very-Severe COPD. N Engl J Med 2020; 383:35-48 [MEDLINE]
Association of Inhaled Corticosteroids With All-cause Death Risk in COPD Patients: A Meta-analysis of Sixty Randomized Controlled Trials. Chest. 2022 Jul 31;S0012-3692(22)01345-9. doi: 10.1016/j.chest.2022.07.015 [MEDLINE]
Secretion Clearance
Mucolytic agents for chronic bronchitis or chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2012 Aug 15;8:CD001287 [MEDLINE]
Twice daily N-acetylcysteine 600 mg for exacerbations of chronic obstructive pulmonary disease (PANTHEON): a randomised, double-blind placebo-controlled trial. Lancet Respir Med. 2014 Mar;2(3):187-94 [MEDLINE]
Mucolytic agents versus placebo for chronic bronchitis or chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2019;5:CD001287 [MEDLINE]
Oscillatory positive expiratory pressure therapy in COPD (O-COPD): a randomised controlled trial. Thorax. 2022 Aug 10;thoraxjnl-2022-219077. doi: 10.1136/thorax-2022-219077 [MEDLINE]
Azithromycin for Prevention of Exacerbations of COPD. NEJM 2011; 365(8): 689-698 [MEDLINE]
Predictors of chronic obstructive pulmonary disease exacerbation reduction in response to daily azithromycin therapy. Am J Respir Crit Care Med 2014;189:1503-1508 [MEDLINE]
Reduction of morbidity and mortality by statins, angiotensin-converting enzyme inhibitors, and angiotensin receptor blockers in patients with chronic obstructive pulmonary disease. J Am Coll Cardiol 2006;47:2554-2560 [MEDLINE]
Reduction of morbidity and mortality by statins, angiotensin-converting enzyme inhibitors, and angiotensin receptor blockers in patients with chronic obstructive pulmonary disease. J Am Coll Cardiol 2006;47:2554-2560 [MEDLINE]
STATCOPE Trial. Simvastatin for the prevention of exacerbations in moderate-to-severe COPD. N Engl J Med. 2014 Jun 5;370(23):2201-10. doi: 10.1056/NEJMoa1403086. Epub 2014 May 18 [MEDLINE]
Statin use and exacerbations in individuals with chronic obstructive pulmonary disease. Thorax. 2015 Jan;70(1):33-40 [MEDLINE]
Cardiovascular safety in patients receiving roflumilast for the treatment of COPD. Chest. 2013; 144(3):758–765 [MEDLINE]
Benefits and harms of roflumilast in moderate to severe COPD. Thorax. 2014 Jul;69(7):616-22 [MEDLINE]
Effect of roflumilast on exacerbations in patients with severe chronic obstructive pulmonary disease uncontrolled by combination therapy (REACT): a multicentre randomised controlled trial. Lancet. 2015 Mar 7;385(9971):857-66. doi: 10.1016/S0140-6736(14)62410-7. Epub 2015 Feb 13 [MEDLINE]
Roflumilast: a review of its use in the treatment of COPD. Int J Chron Obstruct Pulmon Dis. 2016 Jan 6;11:81-90. doi: 10.2147/COPD.S89849. eCollection 2016 [MEDLINE]
Opioid therapy for refractory dyspnea in patients with advanced chronic obstructive pulmonary disease: patients’ experiences and outcomes. CMAJ Open. 2013 Jan 24;1(1):E27-36. doi: 10.9778/cmajo.20120031. eCollection 2013 [MEDLINE]
Managing dyspnea in patients with advanced chronic obstructive pulmonary disease: a Canadian Thoracic Society clinical practice guideline. Can Respir J. 2011 Mar-Apr;18(2):69-78 [MEDLINE]
Endobronchial Valves/Coils
Bronchoscopic lung volume reduction for end-stage emphysema: report on the first 98 patients. Chest 2006;129:518-526 [MEDLINE]
VENT Study Research Group. A randomized study of endobronchial valves for advanced emphysema. N Engl J Med 2010;363(13):1233-1244 [MEDLINE]
Endobronchial Valves for Emphysema without Interlobar Collateral Ventilation (STELVIO). N Engl J Med 2015; 373:2325-2335December 10, 2015DOI: 10.1056/NEJMoa1507807 [MEDLINE]
Lung Volume Reduction Coil Treatment vs Usual Care in Patients With Severe Emphysema: The REVOLENS Randomized Clinical Trial. JAMA. 2016 Jan;315(2):175-84 [MEDLINE]
Lung Volume Reduction
Weight gain after lung reduction surgery is related to improved lung function and ventilatory efficiency. Am J Respir Crit Care Med 2012;186:1109-1116 [MEDLINE]
Segmental volume reduction using thermal vapour ablation in patients with severe emphysema: 6-month results of the multicentre, parallel-group, open-label, randomised controlled STEP-UP trial. Lancet Respir Med. 2016 Mar;4(3):185-93. doi: 10.1016/S2213-2600(16)00045-X. Epub 2016 Feb 16 [MEDLINE]
Survival in COPD patients treated with bronchoscopic lung volume reduction. Respir Med. 2022 Mar 16;196:106825. doi: 10.1016/j.rmed.2022.106825 [MEDLINE]
Ventilation-Based Treatment
Noninvasive ventilatory support does not facilitate recovery from acute respiratory failure in chronic obstructive pulmonary disease. Eur Respir J. 1996 Jun;9(6):1240-5 [MEDLINE]
Acute respiratory failure in patients with severe community-acquired pneumonia. A prospective randomized evaluation of noninvasive ventilation. Am J Respir Crit Care Med. 1999 Nov;160(5 Pt 1):1585-91 [MEDLINE]
Early use of non-invasive ventilation for acute exacerbations of chronic obstructive pulmonary disease on general respiratory wards: a multicentre randomised controlled trial. Lancet. 2000 Jun 3;355(9219):1931-5 [MEDLINE]
Non-invasive positive pressure ventilation to treat respiratory failure resulting from exacerbations of chronic obstructive pulmonary disease: Cochrane systematic review and meta-analysis. BMJ. 2003 Jan 25;326(7382):185 [MEDLINE]
Which patients with acute exacerbation of chronic obstructive pulmonary disease benefit from noninvasive positive-pressure ventilation? A systematic review of the literature. Ann Intern Med. 2003 Jun 3;138(11):861-70 [MEDLINE]
Non-invasive positive pressure ventilation for the treatment of severe stable chronic obstructive pulmonary disease: a prospective, multicentre, randomised, controlled clinical trial. Lancet Respir Med. 2014 Sep;2(9):698-705. doi: 10.1016/S2213-2600(14)70153-5 [MEDLINE]
Association of Home Noninvasive Positive Pressure Ventilation With Clinical Outcomes in Chronic Obstructive Pulmonary Disease: A Systematic Review and Meta-analysis. JAMA. 2020 Feb 4;323(5):455-465. doi: 10.1001/jama.2019.22343 [MEDLINE]
PEEP, auto-PEEP, and waterfalls. Chest. 1989 Sep;96(3):449-51 [MEDLINE]
In chronic obstructive pulmonary disease, a combination of ipratropium and albuterol is more effective than either agent alone. An 85-day multicenter trial. COMBIVENT Inhalation Aerosol Study Group. Chest. 1994;105(5):1411 [MEDLINE]
Effect of systemic glucocorticoids on exacerbations of chronic obstructive pulmonary disease. Department of Veterans Affairs Cooperative Study Group. N Engl J Med. 1999;340(25):1941 [MEDLINE]
Effects of helium-oxygen on intrinsic positive end-expiratory pressure in intubated and mechanically ventilated patients with severe chronic obstructive pulmonary disease. Crit Care Med. 2000;28(8):2721-2728 [MEDLINE]
Anti-cholinergic bronchodilators versus beta2-sympathomimetic agents for acute exacerbations of chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2002;2003(4):CD003900. doi: 10.1002/14651858.CD003900 [MEDLINE]
Oral or IV prednisolone in the treatment of COPD exacerbations: a randomized, controlled, double-blind study. Chest. 2007;132(6):1741 [MEDLINE]
Effect of high flow oxygen on mortality in chronic obstructive pulmonary disease patients in prehospital setting: randomised controlled trial. BMJ. 2010;341:c5462 [MEDLINE]
Association of corticosteroid dose and route of administration with risk of treatment failure in acute exacerbation of chronic obstructive pulmonary disease. JAMA. 2010;303(23):2359 [MEDLINE]
Dynamic hyperinflation and auto-positive end-expiratory pressure: lessons learned over 30 years. Am J Respir Crit Care Med. 2011;184:756–762 [MEDLINE]
Different durations of corticosteroid therapy for exacerbations of COPD. Cochrane Database Syst Rev 2011;(10) CD00697 [MEDLINE]
Short-term vs conventional glucocorticoid therapy in acute exacerbations of COPD: The REDUCE randomized clinical trial. JAMA 2013; 309: 2233-2231 [MEDLINE]
Use of nebulised magnesium sulphate as an adjuvant in the treatment of acute exacerbations of COPD in adults: a randomised double-blind placebo-controlled trial. Thorax. 2013 Apr;68(4):338-43. doi: 10.1136/thoraxjnl-2012-202225 [MEDLINE]
The effect of indacaterol during an acute exacerbation of COPD. Pulm Pharmacol Ther. 2013;26(6):630 [MEDLINE]
Short-term vs conventional glucocorticoid therapy in acute exacerbations of chronic obstructive pulmonary disease: the REDUCE randomized clinical trial. JAMA. 2013;309(21):2223 [MEDLINE]
Outcomes associated with corticosteroid dosage in critically ill patients with acute exacerbations of chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2014 May;189(9):1052-64 [MEDLINE]
Systemic corticosteroids for acute exacerbations of chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2014 Sep 1;2014(9):CD001288. doi: 10.1002/14651858.CD001288.pub4 [MEDLINE]
Different durations of corticosteroid therapy for exacerbations of chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2014 Dec 10;12:CD006897. doi: 10.1002/14651858.CD006897.pub3 [MEDLINE]
Magnesium for acute exacerbation of chronic obstructive pulmonary disease: A systematic review of randomised trials. Ann Thorac Med. 2014 Apr;9(2):77-80. doi: 10.4103/1817-1737.128844 [MEDLINE]
Effect of Home Noninvasive Ventilation With Oxygen Therapy vs Oxygen Therapy Alone on Hospital Readmission or Death After an Acute COPD Exacerbation: A Randomized Clinical Trial. JAMA. 2017 Jun 6;317(21):2177-2186. doi: 10.1001/jama.2017.4451 [MEDLINE]
Official ERS/ATS clinical practice guidelines: noninvasive ventilation for acute respiratory failure. Eur Respir J. 2017 Aug 31;50(2). pii: 1602426. doi: 10.1183/13993003.02426-2016 [MEDLINE]
Management of COPD exacerbations: a European Respiratory Society/American Thoracic Society guideline. Eur Respir J. 2017;49(3) [MEDLINE]
Does high-flow nasal cannula oxygen improve outcome in acute hypoxemic respiratory failure? A systematic review and meta-analysis. Respir Med. 2017;131:58 [MEDLINE]
High Flow Nasal Cannula, Is There a Role in COPD? Tanaffos. 2017;16(Suppl 1):S12 [MEDLINE]
Different durations of corticosteroid therapy for exacerbations of chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2018;3(3):CD006897 [MEDLINE]
Eosinophil-guided corticosteroid therapy in patients admitted to hospital with COPD exacerbation (CORTICO-COP): a multicentre, randomised, controlled, open-label, non-inferiority trial. Lancet Respir Med. 2019;7(8):699 [MEDLINE]
Appropriate Use of Short-Course Antibiotics in Common Infections: Best Practice Advice From the American College of Physicians. Ann Intern Med. 2021 Apr 6. doi: 10.7326/M20-7355 [MEDLINE]
An Updated Definition and Severity Classification of Chronic Obstructive Pulmonary Disease Exacerbations: The Rome Proposal. Am J Respir Crit Care Med. 2021;204(11):1251 [MEDLINE]
Oxygen therapy and inpatient mortality in COPD exacerbation. Emerg Med J. 2021;38(3):170 [MEDLINE]
Magnesium sulfate for acute exacerbations of chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2022;5(5):CD013506 [MEDLINE]
A randomised controlled trial of non-invasive ventilation compared with extracorporeal carbon dioxide removal for acute hypercapnic exacerbations of chronic obstructive pulmonary disease. Ann Intensive Care. 2022 Apr 21;12(1):36. doi: 10.1186/s13613-022-01006-8 [MEDLINE]
High-velocity nasal insufflation versus noninvasive positive pressure ventilation for moderate acute exacerbation of chronic obstructive pulmonary disease in the emergency department: A randomized clinical trial. Acad Emerg Med. 2025;32(4):403 [MEDLINE]
Prognosis
Mortality after admission with pneumonia is higher than after admission with an exacerbation of COPD. Eur Respir J. 2022 Mar 10;2102899. doi: 10.1183/13993003.02899-2021 [MEDLINE]