Mechanisms of Airflow Limitation in COPD (GOLD; Global Strategy for Diagnosis, Management, and Prevention of COPD 2016) [LINK]
Small Airways Disease
Airway Inflammation
Airway Fibrosis
Luminal Plugs Increase Airway Resistance
Decrease of Lung Elastic Recoil
Loss of Alveolar Attachments
Parenchymal Destruction
Dynamic Compression
Background
During Forced Expiration, Airway Diameter is Determined by Multiple Factors
Inherent Size of the Airway
Inherent Size of the Airway Depends on the Level of the Airway in Tracheobronchial Tree, the Airway Smooth Muscle Tone (Which Becomes Relevant During Bronchospasm), and the Amount of Secretions in the Airway
Amount of Radial Traction Exerted by Surrounding Lung Tissue on the Airway Wall
Balance Between the Intrapleural Pressure and the Intra-Airway Pressure
During Forced Expiration, the Intrapleural Pressure is Strongly Positive
“Equal Pressure Point”: point at which the intrapleural pressure = intra-airway pressure
The Level at Which the Equal Pressure Point Occurs Depends on Lung Volume: it is dynamic
At Low Lung Volumes, the Elastic Recoil of the Lung is Lesser, Resulting in an Equal Pressure Point Which is Farther From the Mouth
At High Lung Volumes, the Elastic Recoil of the Lung is Greater, Resulting in Equal Pressure Point Which is Closer to the Mouth
Pursed Lip Breathing Acts to Move the Equal Pressure Point Toward the Mouth
Dynamic Compression Occurs When the Intrapleural Pressure Exceeds the Intra-Airway Pressure During Expiration
Dynamic Compression in Normal Subjects
The Phenomenon of Dynamic Compression Limits Maximum Expiratory Flow in a Lung Volume-Dependent Manner in Normal Subjects
In Normal Subjects, There is a Point at Which the Subject Can No Longer Increase Their Expiratory Flow Rate, Despite Increasing Effort: this point of airflow limitation is due to a critical narrowing of the airways caused by dynamic compression
Dynamic Compression in Chronic Obstructive Pulmonary Disease
Dynamic Compression is Exaggerated in Patients with COPD Due to Multiple Factors
Loss of Elastic Recoil of the Lung
Loss of Radial Traction on Airways Due to Destruction of Lung Tissue
Decreased Small Airway Diameter Due to Bronchospasm and Mucous Hypersecretion
Dynamic Compression in Other Disease States
Effect of Respiratory Muscle Weakness on Dynamic Compression
Weak Expiratory Muscles Does Not Exaggerate Dynamic Compression Because Maximum Expiratory Flow is Independent of Effort (Even in Normal Subjects) and Depends on Lung Volume
Airway Resistance
During a Severe COPD Exacerbation, the Airways Behave Like a Starling Resistor (Chest, 1989) [MEDLINE]
Ohmic Resistor (i.e. One Which Follows Ohm’s Law):
With an Ohmic Resistor, if Extrinsic PEEP is Decreased, the Peak Airway Pressure (PIP) Would Be Expected to Decrease by a Similar Amount: this is one would expect with normal lungs
Starling Resistor: flow rate in the airways is not dependent on the amount extrinsic PEEP applied
Example Using a “Waterfall” Analogy: the flow rate of a waterfall is not impacted by the level of the pool of water below (of course, until the pool of water rises to the level of the waterfall)
With a Starling Resistor, When Extrinsic PEEP is Decreased, the Peak Airway Pressure (PIP) Does Not Decrease by a Similar Amount: this is due to the fact that flow is determined by upstream events only
Chronic Bronchitis: chronic or recurrent secretion of mucus into bronchial tree
Mucus originates from submucosal mucus glands (major source) and goblet cells (minor source)
Mucus gland are enlarged, due to hyperplasia (major source of enlargement) and hypertrophy (minor source of enlargement)
Reid Index: quantifies mucus gland size, defined as ratio of thickness of bronchial mucus glands: thickness of bronchial wall (measured from BM to inner cartilage)
Normal Reid Index: 0.35
Chronic Bronchitis Reid Index: 0.51
Volume Proportion of Mucus Glands: also used to quantify the mucus gland size
Other pathologic changes: goblet cell metaplasia of surface epithelium, chronic inflammation (mononuclear cells, neutrophils), smooth muscle hyperplasia
Emphysema: defined by NHLBI workshop as condition of the lung characterized by abnormal permanent enlargement of airspaces distal to the terminal bronchiole, accompanied by destruction of their walls, and without obvious fibrosis
Destruction : non-uniformity in respiratory airspace enlargement so that the orderly appearance of the acinus and its components is disturbed or lost
Degree of emphysema is the most important correlate of airflow obstruction in cigarette smokers with moderate or severe COPD
Classification of Emphysema
Proximal Acinar (Centrilobular): most common/primary feature is enlargement of respiratory bronchioles
Typical COPD (Upper Lung Zones: Sup/Post UL and Sup Seg-LL): due to tobacco abuse
Simple Coal Worker’s Pneumoconiosis (Upper Lung Zones: Sup/Post UL and Sup Seg-LL): due to occupational coal dust exposure
Panacinar (Panlobular)
Widespread (Most Severe in Lower Zones)——————————————————————————-Alpha1-Antitrypsin Deficiency (Homo PiZ, Homo PiS, and PiSZ)
Lower Zones——————————————————————————————————————–Centrilobular Emphysema and COPD, IVDA
Lower Zones (In Anterior Margins)—————————————————————————————–Variant of Aging (in 7th-9th Decades)
Unilateral Swyer-James Syndrome—————————————————————————————–(Associated with Bronchiolar Obstruction)
Distal Acinar (Paraseptal): least common form/only rarely associated with clinical airflow obstruction
Upper Zones (In Anterior and Posterior Margins)————————————————————————Spontaneous Pneumothorax
Small Airways Disease
Small Airways Disesase defined by Macklem [Ann Int Med, 1971] as patient with clinical features of chronic obstructive airways disease without evidence of emphysema or chronic bronchitis
Pathology: non-specific pattern of peribronchiolar inflammation with varying concentric peribronciolar fibrosis/thickening of walls of terminal and respiratory bronchioles
There is a correlation between small airway wall thickness and the degree of emphysema
Pulmonary Hypertension
pulmonary HTN due to COPD (Chronic Bronchitis > Emphysema)/ Cystic Fibrosis/ Bronchiectasis
Anatomic lung blood vessel distortion/ pulmonary vascular destruction/ hypercapnia and hypoxia-induced vasoconstriction/ increased blood viscosity due to polycythemia
PA pressure usually increases with exercise
PA pressure usually decreases (but not to normal) with oxygen therapy
Flattening results in compromised inspiratory force generation
Horizontal orientation of diaphragm (and loss of zone of apposition between chest wall and diaphragm) -> results in diaphragmatic force vector on rib cage becoming more inward, rather than cephalad
Hoover Sign: paradoxic inward inspiratory movement of lower lateral rib cage
Recruitment of Accessory Muscles: increases oxygen consumption
Development of Auto-PEEP: due to airway obstruction (with increased airway resistance)
Results in inspiratory pressure load that diaphragm must overcome with each inspiration
Association between systemic immune-inflammation index and chronic obstructive pulmonary disease: A population-based study. BMC Pulm Med. Published online August 10, 2023. doi:10.1186/s12890-023-02583-5 [MEDLINE]
Background: The Systemic Immune-Inflammation Index (SII) is a quantitative measurement of the systemic immune-inflammatory response in the human body. The SII has been shown to have prognostic value in various clinical settings, including critical illness, sepsis, and cancer. Its role in chronic obstructive pulmonary disease (COPD) remains unclear and requires further investigation
Methods: We analyzed demographic data from 16,636 participants in the National Health and Nutrition Examination Survey. Logistic regression analysis was performed to assess the correlation between COPD, lung function, chronic respiratory symptoms and SII. We used Cox proportional hazards (PH) model to analyze the relationship between SII and mortality in COPD patients and healthy individuals. We used propensity score matching (PSM) method to match the COPD population with similar baseline levels with the normal population to further analyze the correlation between SII and COPD
Results: We recruited 16,636 participants, ages 40 and above, for the study. A multivariable logistic regression analysis revealed that a higher SII level was independently associated with an elevated likelihood of COPD (Odds Ratio (OR) = 1.449; 95% Confidence Interval (CI): 1.252-1.676, P < 0.0001) after controlling for all other factors. Results of subgroup analysis showed a significant positive correlation between SII and COPD in different age groups, gender, Body Mass Index, smoking status, and those with a history of hypertension. The SII index had positive correlation with COPD after PSM (OR = 1.673; 95%CI: 1.443-1.938). After full adjustment, an increase in the SII is associated with a higher all-cause mortality rate. The hazard ratio (HR) with a 95% CI in the general population, COPD patients, and healthy individuals are 1.161 (1.088, 1.239), 1.282 (1.060, 1.550), and 1.129 (1.055, 1.207), respectively
Conclusions: Higher SII levels are linked to higher prevalence of COPD. COPD patients with a higher SII levels have a higher risk of all-cause mortality. Additional large-scale, long-term studies are necessary to confirm these results.
Hypoxemia (with elevated A-a gradient in most cases, although 1991 study suggests that gradient may normalize in severe COPD with increasing hypercapnia due to shifted oxyHb dissociation curve and V/Q mismatching)
Hypercapnia does not usually occur until FEV1 is <1.3 L
Exacerbations are most commonly associated with Moraxella Catarrhalis/H Flu/Pneumococci
By protected brush, sputum C/S is positive for organisms in 25% of stable COPD patients (and in 52% of acute COPD exacerbation cases: in these, 24% of this group had >104 organisms per ml)
FEV1 Correlates Poorly with Health-Related Quality of Life
Normal FVC
Decreased FEV1/FVC Ratio
Bronchodilator Responsiveness (Defined as Increase in FEV1 and/or FVC ≥12% of Control and ≥200 mL)
Bronchodilator Responsiveness is Observed in <50% of COPD Patients
Total Lung Capacity (TLC)
Disparity Between TLC Measured by Body Plethysmography (Higher) and Helium Dilution (Lower) Suggests a Non-Communicating Gas Space (Bulla)
The Rare Bulla Which Communicates with the Airways (as Demonstrated by a Lesser Disparity of the TLC Between Body Plethysmography and Helium Dilution) Will Contribute More to Dead Space Ventilation, Resulting in Worsening Dyspnea
Functional Residual Capacity (FRC)
Residual Volume (RV)
Increased RV/TLC Ratio (Indicative of Gas Trapping): may be found
DLCO: decreased
Recommendations (GOLD; Global Strategy for Diagnosis, Management, and Prevention of COPD, 2016 [LINK]
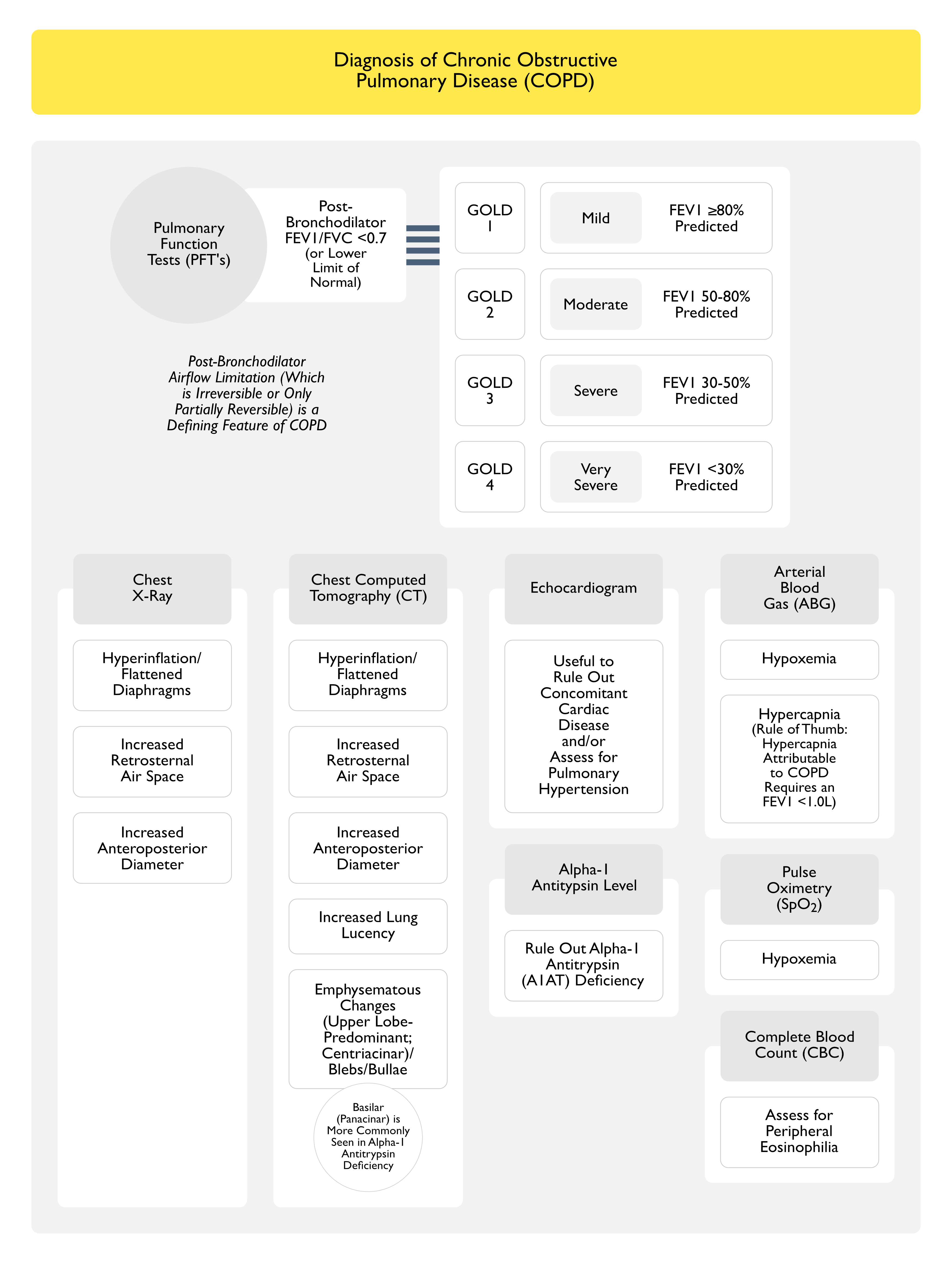
Post-Bronchodilator FEV1/FVC Ratio <70% Should Be Used as a Diagnostic Criterion for COPD
This Criterion Will Result in More Frequent Diagnosis of COPD in the Elderly and Less Frequent Diagnosis in Adults <45 y/o (As Compared to Using Lower Limit of Normal Cutoffs for FEV1 of FVC): especially with milder disease
Lower Limit of Normal Cutoff Values are Highly Dependent on Valid Reference Equations Using Post-Bronchodilator FEV1 Values: however, neither longitudinal studies validating the use of the lower limit of normal nor studies using reference equations in populations where smoking is not the major cause of COPD are available
Grading of Severity of Airflow Obstruction (In Patient with FEV1/FVC Ratio <70%)
GOLD 1 (Mild): FEV1 ≥80% Predicted
GOLD 2 (Moderate): FEV1 50-80% Predicted
GOLD 3 (Severe): FEV1 30-50% Predicted
GOLD 4 (Very Severe): FEV1 <30% Predicted
Application of the ERS/ATS spirometry standards and race-neutral equations in the COPDGene study. Am J Respir Crit Care Med. Published online April 12, 2024. doi:10.1164/rccm.202311-2145OC [MEDLINE]
Rationale: The European Respiratory Society (ERS) and the American Thoracic Society (ATS) recommend using z-scores, and the ATS has recommended using Global Lung Initiative (GLI)- “Global” race-neutral reference equations for spirometry interpretation. However, these recommendations have been variably implemented and the impact has not been widely assessed, both in clinical and research settings
Objectives: We evaluated the ERS/ATS airflow obstruction severity classification
Methods: In the COPDGene Study (n = 10,108), airflow obstruction has been defined as a forced expiratory volume in one second to forced vital capacity (FEV1/FVC) ratio <0.70, with spirometry severity graded from class 1 to 4 based on race-specific percent predicted (pp) FEV1 cut-points as recommended by the Global Initiative for Chronic Obstructive Lung Disease (GOLD). We compared the GOLD approach, using NHANES III race-specific equations, to the application of GLI-Global equations using the ERS/ATS definition of airflow obstruction as FEV1/FVC ratio < lower limit of normal (LLN) and z-FEV1 cut-points of -1.645, -2.5, and -4 (“zGLI Global”). We tested the four-tier severity scheme for association with COPD outcomes
Measurements and main results: The lowest agreement between ERS/ATS with zGLI Global and the GOLD classification was observed in individuals with milder disease (56.9% and 42.5% in GOLD 1 and 2) and race was a major determinant of redistribution. After adjustment for relevant covariates, zGLI Global distinguished all-cause mortality risk between normal spirometry and the first grade of COPD (Hazard Ratio 1.23, 95% CI 1.04-1.44, p=0.014), and showed a linear increase in exacerbation rates with increasing disease severity, in comparison to GOLD
Conclusions: The zGLI Global severity classification outperformed GOLD in the discrimination of survival, exacerbations, and imaging characteristics.
Longitudinal changes in maximal forced inspiratory flow and clinical outcomes in COPD patients. Chest. Published online August 14, 2024. doi:10.1016/j.chest.2024.07.162 [MEDLINE]
Background: COPD primarily impairs expiratory flow due to progressive airflow obstruction and reduced lung elasticity. Increasing evidence underlines the importance of inspiratory flow as a biomarker for selecting inhaler devices and providing ancillary aerodynamic information
Research question: Does the longitudinal changes in maximum forced inspiratory flow (FIFmax) influence acute exacerbations and lung function decline in patients with COPD?
Study design and methods: This longitudinal study evaluated FIFmax in patients with COPD over a 7-year period from 2004 to 2020. Eligible patients were categorized into 2 groups based on FIFmax trajectory: the increased FIFmax group and the decreased FIFmax group. The study assessed the annual rate of acute exacerbations and the annual decline rate of FEV1. Subgroup analyses were conducted based on treatment status, with a focus on inhaled therapy and inhaler device usage
Results: Among the eligible 956 patients with COPD, 56.5% belonged to the increased FIFmax group. After propensity score matching, the increased FIFmax group experienced lower rates of severe exacerbations (0.16 per year vs 0.25 per year, P = .017) and a slower decline in FEV1 (0 [interquartile range, -51 to 71] mL/y vs -43 [interquartile range, -119 to 6] mL/y; P < .001) compared with the decreased FIFmax group. These associations were particularly prominent in patients using specific inhaler therapies such as dry powder inhalers
Interpretation
This study showed that the longitudinal changes in FIFmax are associated with clinical outcomes in patients with COPD
Patients with increased FIFmax experienced a lower rate of severe exacerbations and a slower decline in lung function
These findings suggest the potential benefits of optimizing inspiratory flow in COPD management, although further studies are needed to confirm these observations due to potential confounding factors
Cohort Study Examining the Predictive Value of Emphysematous Changes on Chest CT (Ann Int Med, 2014) [MEDLINE]
Presence of Emphysematous Changes on CT Imaging in Patients without Spirometrically-Defined COPD were Linearly Associated with Increased All-Cause Mortality
Even after adjusting for confounding variables, such as cardiovascular risk factors and FEV1
The Association was of the Greatest Magnitude Among Smokers
Study of the Impact Centrilobular vs Paraseptal Emphysema on the Longitudinal Changes in Diffusing Capacity and Mortality in Chronic Obstructive Pulmonary Disease (COPD) (Chest, 2023) [MEDLINE]
This pooled analysis included 399 patients with COPD from two prospective Observational COPD Cohorts
Centrilobular Emphysema and Paraseptal Emphysema were visually assessed on CT scan according to the Fleischner Society statement
The diffusing capacity and transfer coefficient of the lung for carbon monoxide (Dlco and KCO) and FEV1 were evaluated at least annually over a 5-year Period
Mortality was recorded over 10 years
Longitudinal changes in FEV1, Dlco, and KCO and mortality were compared between mild or less severe and moderate or more severe Centrilobular Emphysema and between present and absent Paraseptal Emphysema in each Global Initiative for Chronic Obstructive Lung Disease (GOLD) Stage
Results
The Dlco and KCO decline was weakly associated with FEV1 and greater in GOLD stage 3 or above than in GOLD stages 1 and 2\
Furthermore, moderate or more severe CLE, but not present PSE, was associated with steeper declines in Dlco for GOLD stages 1 and 3 or higher and KCO for all GOLD stages independent of age, sex, height, and smoking history
The moderate or more severe CLE, but not present PSE, was associated with additional FEV1 decline and higher 10-year mortality among patients with GOLD stage 3 or higher
Conclusions
A CT scan finding of moderate or more severe CLE, but not PSE, was associated with a subsequent accelerated impairment in diffusing capacity and higher long-term mortality in severe GOLD stage among patients with COPD