Prevalence and Prognostic Significance of COPD in Adults Younger than 50 Years of Age. NEJM Evid. 2025 Aug;4(8):EVIDoa2400424. doi: 10.1056/EVIDoa2400424 [MEDLINE]
Background: Identification of chronic obstructive pulmonary disease (COPD) diagnosed before 50 years of age (“young COPD”) will help enable the study of preventive and therapeutic interventions for classically diagnosed COPD in later life. However, there remains uncertainty about the definition of young COPD and its prognostic significance
Methods: We assessed the prevalence of young COPD, defined here as spirometric airflow obstruction plus symptoms of cough, phlegm, and dyspnea or 10 or more pack-years of smoking, among 18-to-49-year-old participants from four pooled, prospective U.S. cohorts. We evaluated the association of young COPD with premature mortality and respiratory and cardiovascular events over follow-up, using multivariable-adjusted proportional hazards models
Results: Among 10,680 participants (median age, 40 years; 56.8% women; 41.7% Black; 51.1% unexposed to smoking), the prevalence of people meeting our case definition of young COPD was 4.5%. Compared with nonobstructed participants, the adjusted hazard ratio (an adjusted hazard ratio greater than unity indicates more incident cases) for participants with young COPD for death before 75 years of age was 1.43 (95% confidence interval [CI], 1.19 to 1.73; P<0.001); for incident hospitalization or death due to chronic lower respiratory disease, the adjusted hazard ratio was 2.56 (95% CI, 2.05 to 3.20); for coronary heart disease, the adjusted hazard ratio was 1.12 (95% CI, 0.85 to 1.47); and for heart failure, the adjusted hazard ratio was 1.72 (95%CI, 1.26 to 2.35). The hazards of the clinical outcomes in participants with simple obstruction (spirometric obstruction without symptoms and <10 pack-years; prevalence, 2.4%) were similar to those of nonobstructed participants
Conclusions
Young COPD was present in 4.5% of adults under 50 years of age in the cohorts examined
The diagnosis was associated with premature mortality as well as respiratory and heart-failure events
Cost
COPD-Related Health Care Utilization (2009 Data)
8 Million Office Visits
1.5 Million Emergency Department Visits
715,000 Hospitalizations
Costs Due to COPD
Approximately $49.9 billion: $29.5 billion in direct health-care expenditures, $8.0 billion in indirect morbidity costs, and $12.4 billion in indirect mortality costs
COPD Exacerbations Account for Most of the Morbidity, Mortality, and Costs Associated with COPD
COPD Exacerbations Cause Frequent Hospital Admissions/Relapses/Readmissions, Contribute to Death During Hospitalization or Shortly Thereafter, Significantly Decrease Quality of Life, Expend Financial Resources, and Accelerate a Progressive Decline in Pulmonary Function
Undiagnosis/Overdiagnosis
xxxxx
Undiagnosed and ‘overdiagnosed’ COPD using postbronchodilator spirometry in primary healthcare settings: a systematic review and meta-analysis. BMJ Open Respir Res. 2023 Apr;10(1):e001478. doi: 10.1136/bmjresp-2022-001478 [MEDLINE]
Background: Despite chronic obstructive pulmonary disease (COPD) being a major global cause of mortality and hospitalisation, it is often undiagnosed or inaccurately diagnosed in clinical settings
Objective: To systematically synthesise all peer-reviewed papers from primary healthcare settings that have reported data on: (1) undiagnosed COPD, that is, patients with respiratory symptoms and postbronchodilator airflow obstruction consistent with COPD, without a formal clinician’s diagnosis of COPD either documented in health records or reported by patients and (2) ‘overdiagnosed COPD’, that is, clinician’s diagnosis without postbronchodilator airflow obstruction
Methods: Studies investigating these diagnostic metrics in patients from primary healthcare clinics (according to predefined inclusion/exclusion criteria) were sourced from Medline and Embase and assessed for bias (Johanna Briggs Institute tools for prevalence studies and case series). Meta-analyses of studies of adequate sample size used random effect modelling stratified by risk factor categories
Results: Of 26 eligible articles, 21 cross-sectional studies investigated 3959 cases of spirometry-defined COPD (with or without symptoms), and 5 peer-reviewed COPD case series investigated 7381 patients. The prevalence of spirometry-confirmed COPD without a diagnosis documented in their health records was 14%-26% in studies of symptomatic smokers (N=3). 1 in 4 patients taking inhaled therapies (25% (95% CI 22% to 28%), N=2) and 1 in 6 smokers irrespective of symptoms (16% (95% CI 14% to 18%), N=6) fulfilled diagnostic spirometry criteria but did not report receiving a COPD-related diagnosis. In an adequately powered series of COPD cases documented in primary healthcare records (N=4), only between 50% and 75% of subjects had any airflow obstruction on postbronchodilator spirometry performed by study researchers, therefore, COPD was clinically ‘overdiagnosed’ in 25%-50% of subjects
Discussion: Although data were heterogeneous and of modest quality, undiagnosed COPD was common in primary healthcare, especially for symptomatic smokers and patients treated with inhaled therapies. In contrast, frequent COPD ‘overdiagnosis’ may represent treatment of asthma/reversible component or another medical diagnosis.
Association with Cardiovascular Disease
xxx
Association between chronic obstructive pulmonary disease and cardiovascular disease in adults aged 40 years and above: Data from NHANES 2013-2018. BMC Pulm Med. Published online August 31, 2023. doi:10.1186/s12890-023-02606-1 [MEDLINE]
Background: Chronic obstructive pulmonary disease (COPD) and cardiovascular disease (CVD) are two major age-related diseases prevalent in the elderly. However, it is unclear whether there is a higher prevalence of one or more CVDs in COPD patients compared to those without COPD, and the magnitude of this increased prevalence
Methods: This population-based cross-sectional study was conducted using data from the National Health and Nutrition Examination Survey (NHANES) 2013-2018 among American adults aged 40 years and above. Multivariable logistic regression models (including unadjusted model, minimally adjusted model, and fully adjusted model) were conducted to investigate the association between COPD and the prevalence of one or more CVDs, including coronary heart disease, heart failure, angina pectoris, heart attack, diabetes, and stroke
Results: This study included 11,425 participants, consisting of 661 participants with COPD and 10,764 participants without COPD. COPD patients had a significantly higher prevalence of CVD than those without COPD (59.6% vs. 28.4%). After adjusting for covariates, COPD was significantly associated with the prevalence of one CVD (OR = 2.2, 95% CI = 1.6-3.0, p < 0.001), two or more CVDs (OR = 3.3, 95% CI = 2.2-5.0, p < 0.001), and three or more CVDs (OR = 4.3, 95% CI = 2.9-6.5, p < 0.001)
Conclusions: Patients with COPD have a higher prevalence of one or more CVDs compared with those without COPD. Our findings highlight the importance of CVD prevention and management in patients with COPD.
Preserved Ratio Impaired Spirometry (PRISm)
xxx
Lung Function Decline and Airflow Limitation Risk in Preserved Ratio Impaired Spirometry Subtypes by Smoking Status. Chest. 2025 May 10:S0012-3692(25)00570-7. doi: 10.1016/j.chest.2025.05.006 [MEDLINE]
Background: Preserved ratio impaired spirometry (PRISm) is regarded as a COPD precursor, but whether this varies by smoking status remains unclear
Research question: Are annual lung function decline and the risk of developing airflow limitation different among PRISm subtypes by smoking status?
Study design and methods: A total of 2,850 participants from a 15-year population-based prospective cohort were included in this analysis. Participants were categorized into 3 groups: patients with normal spirometry who do not smoke (normal control), patients with PRISm who do not smoke (NS-PRISm), and patients with PRISm who have ever smoked (ES-PRISm). We compared annual lung function decline and the risk of developing airflow limitation among the 3 groups
Results: Participants in the normal control group exhibited the fastest decline in annual lung function, followed by the ES-PRISm group, with the NS-PRISm group showing the slowest decline. Participants in the ES-PRISm group had significantly faster annual lung function decline than the NS-PRISm group. Participants in the ES-PRISm group had a significantly increased risk of developing airflow limitation than the NS-PRISm group (95 of 256 [37.1%] vs 69 of 470 [14.7%]; adjusted hazard ratio [HR], 1.90; 95% CI, 1.31-2.77; P = .001) and normal control group (95 of 256 [37.1%] vs 193 of 2,124 [9.1%]; adjusted HR, 2.69; 95% CI, 1.96-3.69; P < .001). Besides, participants in the NS-PRISm group also exhibited a higher risk of developing airflow limitation than those in the normal control group (69 of 470 [14.7%] vs 193 of 2,124 [9.1%]; adjusted HR, 1.41; 95% CI, 1.07-1.87; P = .016). When the ES-PRISm group was further divided into patients with PRISm who actively smoke and patients with PRISm who formerly smoked, both of these PRISm subtypes showed a faster annual lung function decline and a similarly higher risk of airflow limitation than the NS-PRISm group
Interpretation: These findings suggest that both NS-PRISm and ES-PRISm may be potential precursors to COPD and indicate that PRISm should not be restricted to evaluating patients who actively smoke and formerly smoked alone.
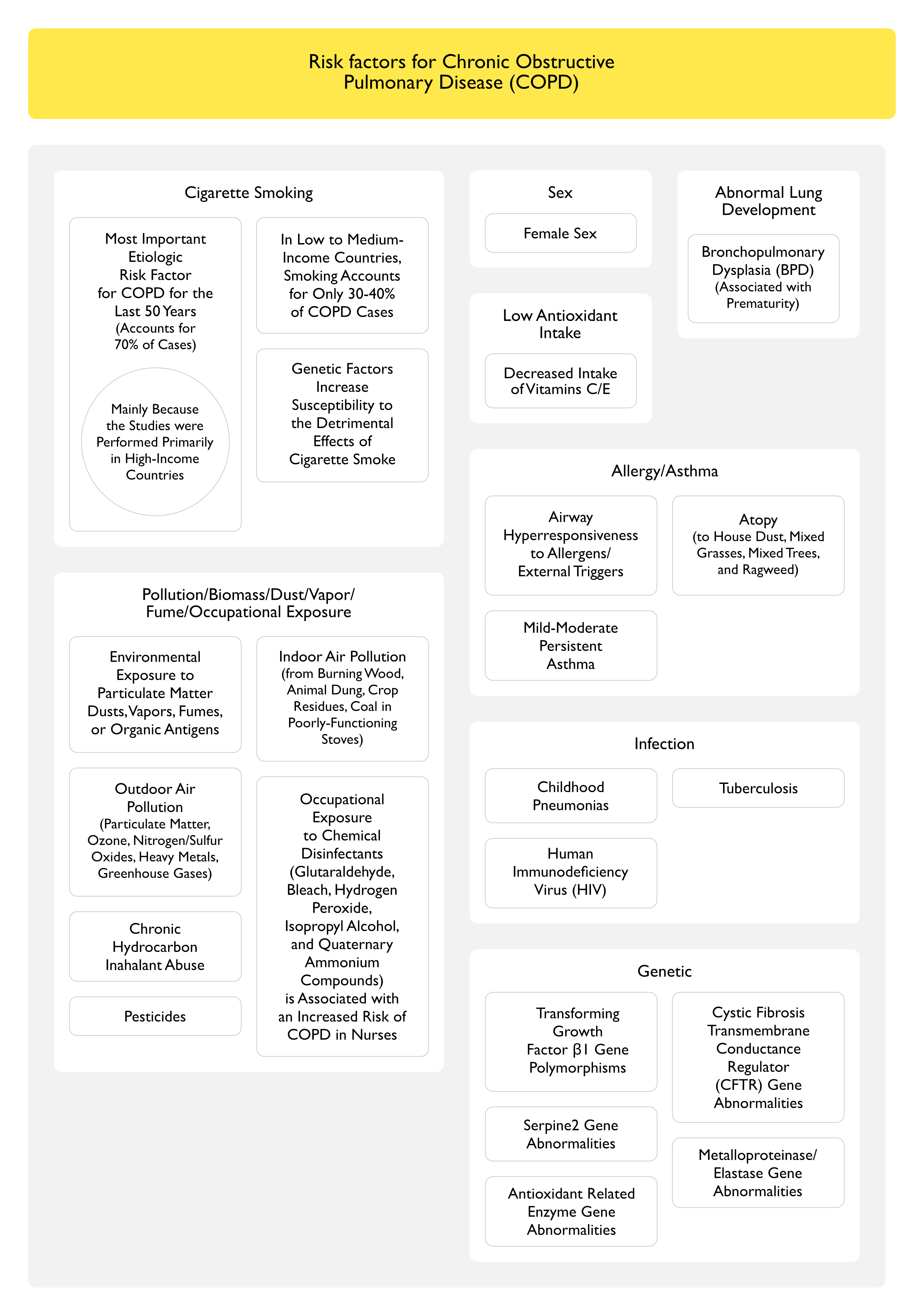
Risk Factors for Chronic Obstructive Pulmonary Disease (COPD)
Female Sex
xxx
Gender, tobacco and chronic obstructive pulmonary disease: analysis of the 2020 National Health Interview Survey. BMJ Open Respir Res. 2025 May 8;12(1):e002462. doi: 10.1136/bmjresp-2024-002462 [MEDLINE]
Rationale: Recent studies describe an increasing prevalence of chronic obstructive pulmonary disease (COPD) and higher COPD exacerbation rates among women compared with men despite lower average cigarette use, which has raised the question of whether women are more susceptible to the effects of tobacco smoke. We examined associations between gender, cigarette smoking and COPD in a national dataset
Methods: We used cross-sectional data for US respondents aged ≥40 years from the 2020 National Health Interview Survey (NHIS). Weighted multivariable logistic regressions assessed the relationship between gender and respondent-reported physician-diagnosed COPD, adjusting for tobacco use and sociodemographic covariates. Additional analyses were performed to determine if the relationship between cigarette smoking and COPD was modified by gender
Results: Women had a higher COPD prevalence (7.8%) than men (6.5%) despite lower cigarette smoke exposure. Women were less likely to have ever smoked, and among respondents who had smoked, women had a lower average pack-year history compared with men. In multivariable regressions, female gender was associated with a higher risk of COPD (adjusted risk ratio 1.47, 95% CI 1.30 to 1.65) and the relative risk was similar for respondents both with and without a history of smoking. Moreover, there was no significant interaction between gender and smoking status or gender and pack-year exposure relating to COPD prevalence
Conclusions: Among adults aged ≥40 years, women had a roughly 50% greater risk of COPD than men. Higher susceptibility to cigarette smoking in women did not explain the difference.
Low smoking exposure and development and prognosis of COPD over four decades: A population-based cohort study. Eur Respir J. Published online July 26, 2024. doi:10.1183/13993003.00314-2024 [MEDLINE]
Background: A diagnosis of COPD is mainly considered in individuals with >10 pack-years of smoking. We tested the hypothesis that low smoking exposure, below the critical threshold of 10 pack-years, increases risk of COPD and leads to poor prognosis
Methods: We followed non-obstructed adult smokers from the Copenhagen City Heart Study for COPD, defined as a forced expiratory volume in 1 s (FEV1)/forced vital capacity <0.70 and FEV1 <80% predicted, and for related clinical outcomes. First, we followed individuals for 5 years according to baseline smoking for risk of developing COPD, and thereafter for up to four decades for severe exacerbations and death
Results: In 6098 non-obstructed smokers, 1781 (29%) developed COPD after 5 years of follow-up: 23% of individuals with <10 pack-years of smoking at baseline, 26% of those with 10-19.9 pack-years, 30% of those with 20-39.9 pack-years and 39% of those with ≥40 pack-years. During four decades of follow-up, we recorded 620 exacerbations and 5573 deaths. Compared to individuals without COPD with <10 pack‑years of smoking, multivariable adjusted hazard ratios (HRs) for exacerbations were 1.94 (95% CI 1.36-2.76) in those without COPD and ≥10 pack-years, 2.83 (95% CI 1.72-4.66) in those with COPD and <10 pack-years, 4.34 (95% CI 2.93-6.43) in those with COPD and 10-19.9 pack-years, 4.39 (95% CI 2.98-6.46) in those with COPD and 20-39.9 pack-years and 4.98 (95% CI 3.11-7.97) in those with COPD and ≥40 pack-years. Corresponding HRs for all-cause mortality were 1.20 (95% CI 1.10-1.32), 1.31 (95% CI 1.13-1.53), 1.59 (95% CI 1.40-1.79), 1.81 (95% CI 1.62-2.03) and 1.81 (95% CI 1.55-2.10)
Conclusion: Low smoking exposure below the critical threshold of 10 pack-years increases risk of COPD in middle-aged adults within 5 years, and these individuals have increased risk of severe exacerbation and early death over four decades.
Paternal prepubertal passive smoke exposure is related to impaired lung function trajectories from childhood to middle age in their offspring. Thorax. 2025 Sep 2:thorax-2024-222482. doi: 10.1136/thorax-2024-222482 [MEDLINE]
Introduction: Paternal prepubertal passive smoke exposure may increase the risk of childhood asthma. However, its association with impaired lung function trajectories at risk of chronic obstructive pulmonary disease in offspring was not investigated. We assessed the association between paternal prepubertal passive smoke exposure and lung function from childhood to middle age in their offspring
Methods: Data were analysed from 890 father-offspring pairs from the Tasmanian Longitudinal Health Study. The offspring were probands in the original cohort who underwent spirometry at six time points from ages 7 to 53 years. Lung function (forced expiratory volume in 1 s (FEV1), forced vital capacity (FVC) and FEV1/FVC) trajectories were previously derived using group-based trajectory modelling. Fathers reported their own passive smoke exposure before age 15 years. Multinomial logistic regressions assessed associations between paternal prepubertal passive smoke exposure and lung function trajectories in offspring. Potential mediations and interactions were assessed for active paternal smoking, offspring passive smoke exposure and respiratory illnesses during childhood, and subsequent active smoking
Results: Paternal prepubertal passive smoke exposure was associated with the below average FEV1 (adjusted multinomial OR (aMOR) 1.56; 95% CI 1.05 to 2.31) and early low-rapid decline FEV1/FVC trajectories (aMOR 2.30; 95% CI 1.07 to 4.94) in offspring. The association with the below average FEV1 trajectory was augmented for offspring exposed to childhood passive smoke (aMOR 2.36; 95% CI 1.34 to 4.13; p-interaction = 0.053). Observed associations partly mediated through smoking and respiratory illnesses in fathers and offspring (each contributing <15%)
Conclusions: Paternal prepubertal passive smoke exposure was associated with impaired lung function trajectories in offspring, which highlights the adverse impact of smoking on multiple generations
Environmental Pollutants
Indoor Air Pollution: biomass cooking and heating in poorly-ventilated structures are important risk factors for COPD
Outdoor Air Pollution: probably a small contributor, in comparison to tobacco smoke
Short-term air pollution exposure and exacerbation events in mild to moderate COPD: a case-crossover study within the CanCOLD cohort. Thorax. 2023 May 5;thorax-2022-219619. doi: 10.1136/thorax-2022-219619 [MEDLINE]
Background: Infections are considered as leading causes of acute exacerbations of chronic obstructive pulmonary disease (COPD). Non-infectious risk factors such as short-term air pollution exposure may play a clinically important role. We sought to estimate the relationship between short-term air pollutant exposure and exacerbations in Canadian adults living with mild to moderate COPD
Methods: In this case-crossover study, exacerbations (‘symptom based’: ≥48 hours of dyspnoea/sputum volume/purulence; ‘event based’: ‘symptom based’ plus requiring antibiotics/corticosteroids or healthcare use) were collected prospectively from 449 participants with spirometry-confirmed COPD within the Canadian Cohort Obstructive Lung Disease. Daily nitrogen dioxide (NO2), fine particulate matter (PM2.5), ground-level ozone (O3), composite of NO2 and O3 (Ox), mean temperature and relative humidity estimates were obtained from national databases. Time-stratified sampling of hazard and control periods on day ‘0’ (day-of-event) and Lags (‘-1’ to ‘-6’) were compared by fitting generalised estimating equation models. All data were dichotomised into ‘warm’ (May-October) and ‘cool’ (November-April) seasons. ORs and 95% CIs were estimated per IQR increase in pollutant concentrations
Results: Increased warm season ambient concentration of NO2 was associated with symptom-based exacerbations on Lag-3 (1.14 (1.01 to 1.29), per IQR), and increased cool season ambient PM2.5 was associated with symptom-based exacerbations on Lag-1 (1.11 (1.03 to 1.20), per IQR). There was a negative association between warm season ambient O3 and symptom-based events on Lag-3 (0.73 (0.52 to 1.00), per IQR)
Conclusions: Short-term ambient NO2 and PM2.5 exposure were associated with increased odds of exacerbations in Canadians with mild to moderate COPD, further heightening the awareness of non-infectious triggers of COPD exacerbations.
HIV Infection Accelerates the Onset of Smoking-Related Emphysema (see Human Immunodeficiency Virus, [[Human Immunodeficiency Virus]])
In a Population-Based Study Using Ontario’s Health Administration Database of Patients Diagnosed with COPD Between 1996-2015, the Rate of COPD was Higher in HIV-Positive Patients, as Compared to HIV-Negative Patients (10.4 vs 9.0 Cases Per 1000 Person-Years; Standardized Incidence ratio 1.16, 95% Confidence Interval 1.10 to 1.21; Adjusted Rate Ratio 1.34, 95% CI 1.27 to 1.41) (CMAJ Open, 2020) [MEDLINE]
In a Sensitivity Analysis, Smoking Explained the Observed Differences in COPD Incidence
Inflammatory Bowel Disease (IBD) (see Inflammatory Bowel Disease): chronic bronchitis is associated with UC
xxx
Positive Family History of COPD (Chest, 2011) [MEDLINE]
xxxxx
Poverty
Clearly a risk factor for COPD, but exact contributors are unclear
Toxins/Chemicals
Chronic Hydrocarbon Inhalant Abuse (see Hydrocarbons


{kind=link}