Epidemiology: RA is the connective tissue disease most commonly associated with BO
RA-associated BO was originally thought to be associated with gold/penicillamine use -> however, the persistent incidence of RA-associated BO despite decreased use of these drugs suggests that RA itself is responsible
Peak Group: long-standing RA seropositive females in 40’s-50’s -> these cases may have rapid clinical progression
Chronic Graft vs Host Disease (GVHD) (see Graft vs Host Disease): chronic GVHD occurs in 33% of long-term survivors of allo-BMT -> BO occurs in 10% of chronic GVHD cases
Factors Related to Transplant Type: there is an increased risk of BO with the use of peripheral blood stem cells
Methotrexate (see Methotrexate): causes BO only in combination with chronic GVHD, not alone (methotrexate induces MHC expression, which are targets for T-cell in GVHD)
Use of Graft vs Host Disease Prophylaxis (see Graft vs Host Disease): immunosuppression for GVHD increases viral infection risk
Viral Infection: viral infection occurs in 25-30% of post-SCT BO cases
Respiratory Syncytial Virus/Parainfluenza Virus (see Respiratory Syncytial Virus and Parainfluenza Virus): infection with these viruses within the first 100 days post-BMT/SCT increases risk for BO within the first year after transplantation [MEDLINE]
Physiology: BO likely represents chronic graft vs host disease in the lung
10 Year Incidence: 70% of cases develop BO [MEDLINE]
Risk Related to Type of Immunosuppression: incidence of BO is lower with taccolimus, as compared to cyclosporine A [MEDLINE]
Physiology: related to chronic allograft rejection (associated with HLA locus mismatch)
Cofactors: PCP, CMV, altered mucociliary clearance, altered blood flow due to bronchial artery ligation, immunosuppression, and aspiration due to loss of cough)
Diacetyl-Associated BO Cases Have Been Reported in Workers mManufacturing Butter Flavoring Used in Popcorn Processing Plants
Diacetyl is Also a Component (or is Used in the Manufacturing Process) of Buttered Popcorn/Chips, Candy, Butter, Ice Cream, Baked Goods, and Coffee Flavorings
Epidemiology: reports of hydrogen sulfide-associated BO date back to World War I (1914-1918) and the Iran-Iraq War (1980-1988), during which this agent was used
Clinical: acute chemical pneumonitis (chest tightness, dyspnea, massive hemoptysis) -> fibrous exudates and granulation tissue in bronchi/distal bronchioles -> eventual development of bronchiolitis obliterans
Nitrogen Oxides: used in fertilizer production (probably involved in silo-filler’s disease)
Reports of US Soldiers from Iraq/Afghanistan with BO Who Were in Proximity to a Fire in a Sulfur Mine in 2003 (fire produced high ambient air levels of sulfur dioxide, a known cause of BO), exposure to dust storms, exposure to incinerated solid/human waste, and/or exposure to combat smoke (NEJM, 2011) [MEDLINE]
Reports of Sulfur Mustard-Associated BO Date Back to World War I (1914-1918) and the Iran-Iraq War (1980-1988), During Which this Agent was Used
Clinical: acute chemical pneumonitis (chest tightness, dyspnea, massive hemoptysis) -> fibrous exudates and granulation tissue in bronchi/distal bronchioles -> eventual development of bronchiolitis obliterans
Neuroendocrine Cell Hyperplasia/Multiple Carcinoid Tumorlets (see Carcinoid)
Idiopathic Bronchiolitis Obliterans
May Occur
Physiology
Injury to and Inflammation of Small Airway Epithelial Cells and Subepithelial Structures, Leading to Excessive Fibroproliferation (and Ineffective Epithelial Regeneration)
Decreased Number of Club Cells (formerly called Clara Cells): these cells are known to promote regeneration of bronchiolar epitheliam
Polymorphisms in Innate Immune System Genes: associated with transplant-associated BO
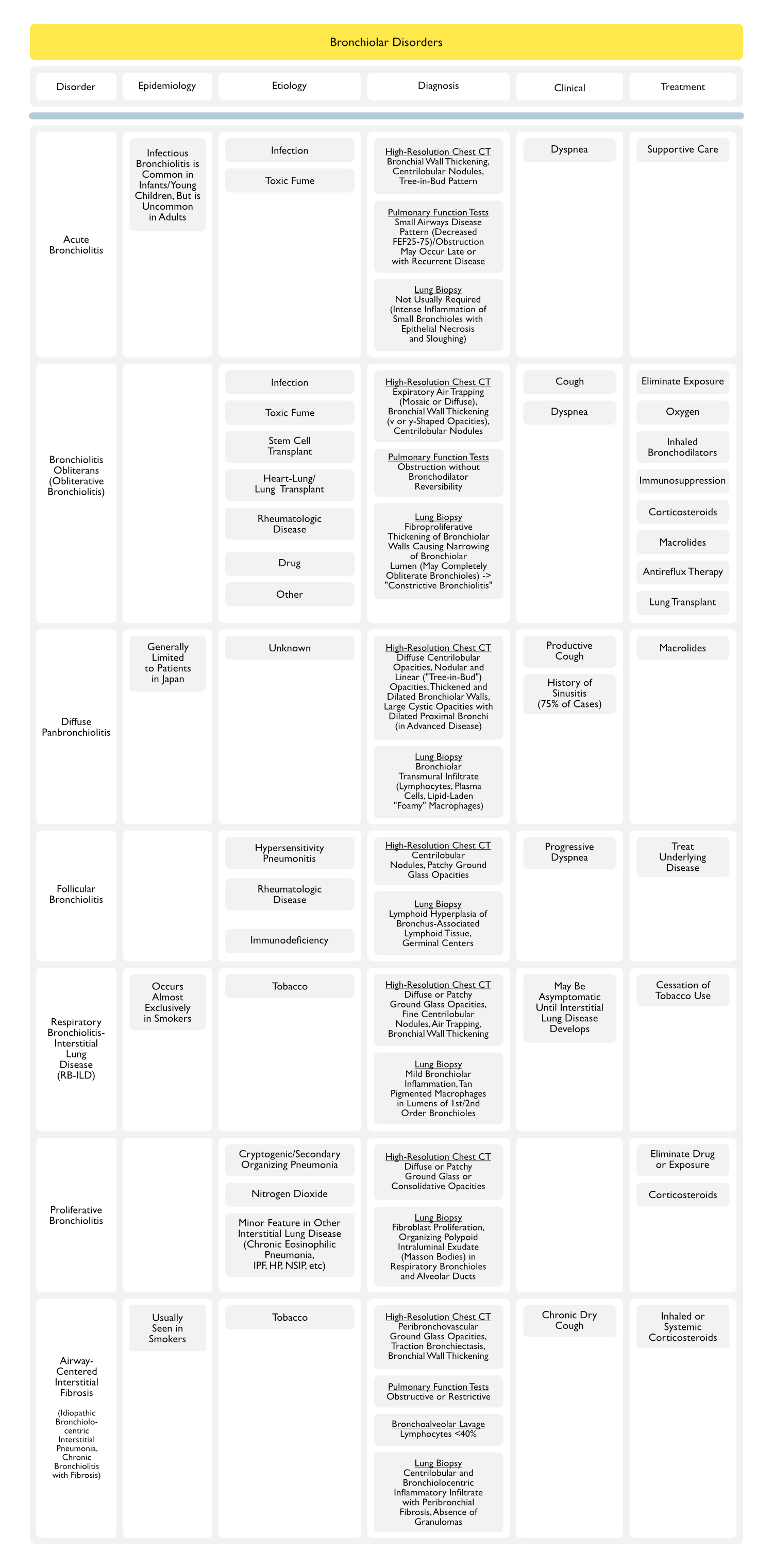
Spirometry: obstruction without bronchodilator reversibility (although less commonly, cases have been described with either mixed obstruction-restriction or rarely, restriction)
FEV1: decreased
FVC: normal-slightly decreased
FEV1/FVC: decreased
Lung Volumes: air trapping
TLC: normal
RV: increased
RV/TLC: increased (consistent with gas trapping)
DLCO: initially normal, decreases with disease progression
Activated T-Cells: in heart-lung and lung transplant cases (primed lymphocyte, cell-mediated lympholysis tests correlate with risk of BO in these patients)
Bronchoalveolar Lavage in Lung Transplants
CD4-Predominance Against Class 2 MHC: correlates with rejection
CD8-Predominance Against Class 1 MHC: correlates with BO
“Constrictive Bronchiolitis” Pattern: fibroproliferative thickening of bronchiolar walls causing narrowing of bronchiolar lumen (may completely obliterate bronchioles)
Clinical Presentations
General Comments
Bronchiolitis Obliterans Syndrome (BOS): term used to describe the clinical entity of bone marrow/stem cell transplant or lung transplant-associated bronchiolitis obliterans (small airways obstruction with airflow limitation, etc) in the absence of histologic confirmation
Latency: BO may occur months-years after transplant
Mean Latency: 16-20 mo after transplant (but may occur as early as 3 mo post-lung transplant)
Diagnosis
CXR: usually normal
HRCT: peripheral bronchiectasis, patchy consolidation, decreased peripheral vascular markings, mosaic attentuation (due to air trapping), and bronchial dilation
FOB with TBB: used to exclude infection, anastomotic complications, and acute rejection and to diagnose BO (TBB has 15-80% sensitivity for diagnosis of BO)
PFT’s: FEV1 and FEF25-75are used to clinically stage BO
Obliterative bronchiolitis. N Engl J Med. 2014 May 8;370(19):1820-8. doi: 10.1056/NEJMra1204664 [MEDLINE]
Toxin-Associated Bronchiolitis Obliterans
Bronchiolitis obliterans from exposure to incinerator fly ash. J Occup Environ Med. 1995 Jul;37(7):850-5 [MEDLINE]
Bronchiolitis obliterans syndrome in popcorn production plant workers. Eur Respir J 2004;24:298-302 [MEDLINE]
Bronchiolitis obliterans following exposure to sulfur mustard: chest high resolution computed tomography. Eur J Radiol 2004;52:164-9 [MEDLINE]
Inhaled corticosteroids and long-acting beta 2-agonists in treatment of patients with chronic bronchiolitis following exposure to sulfur mustard. Inhal Toxicol 2007;19:889-94 [MEDLINE]
Therapeutics effect of N-acetyl cysteine on mustard gas exposed patients: evaluating clinical aspect in patients with impaired pulmonary function test. Respir Med 2008;102:443-8 [MEDLINE]
Constrictive bronchiolitis in soldiers returning from Iraq and Afghanistan. N Engl J Med. 2011 Jul 21;365(3):222-30. doi: 10.1056/NEJMoa1101388 [MEDLINE]
Effect of recombinant human IFNγ in the treatment of chronic pulmonary complications due to sulfur mustard intoxication. J Immunotoxicol 2014;11:72-7 [MEDLINE]
The role of N-acetylcysteine in the management of acute and chronic pulmonary complications of sulfur mustard: a literature review. Inhal Toxicol. 2014 Aug;26(9):507-23. doi: 10.3109/08958378.2014.920439 [MEDLINE]
Transplant-Associated Bronchiolitis Obliterans
Early bronchiolitis obliterans following lung transplantation: accuracy of expiratory thin-section CT for diagnosis. Radiology. 2000;216(2):472-477 [MEDLINE]
Bronchiolitis obliterans syndrome in heart-lung transplant recipients: diagnosis with expiratory CT. Radiology 2001;218:533-9 [MEDLINE]
Maintenance azithromycin therapy for bronchiolitis obliterans syndrome: results of a pilot study. Am J Respir Crit Care Med 2003; 168:121-5 [MEDLINE]
Airflow decline after myeloablative allogeneic hematopoietic cell transplantation: the role of community respiratory viruses. J Infect Dis 2006;193:1619-25 [MEDLINE]
Azithromycin is associated with increased survival in lung transplant recipients with bronchiolitis obliterans syndrome. J Heart Lung Transplant 2010;29:531-7 [MEDLINE]
Clinical and immunological evaluation of 12-month azithromycin therapy in chronic lung allograft rejection. Clin Transplant 2011;25:E381-9 [MEDLINE]
A randomised controlled trial of azithromycin to prevent chronic rejection after lung transplantation. Eur Respir J 2011;37:164-72 [MEDLINE]
The Registry of the International Society for Heart and Lung Transplantation: fifteenth pediatric lung and heart-lung transplantation report-2012. J Heart Lung Transplant 2012;31:1087-95 [MEDLINE]
The Registry of the International Society for Heart and Lung Transplantation: 29th adult lung and heart-lung translant report-2012. J Heart Lung Transplant 2012;31:1073-86 [MEDLINE]
Tacrolimus and cyclosporine have differential effects on the risk of development of bronchiolitis obliterans syndrome: results of a prospective, randomized international trial in lung transplantation. J Heart Lung Transplant 2012;31:797-804 [MEDLINE]