Aspiration Pneumonia is Defined as Pneumonitis/Pneumonia Resulting from the Entry of Oropharyngeal/Gastric Fluids or Material into the Lower Airways and/or Lung
Aspiration Pneumonia Accounted for Approximately 15% of All Community-Acquired Pneumonias (NEJM, 2001) [MEDLINE]
Similar Data for Hospital-Acquired Pneumonias are Not Available
Incidence Rates of Aspiration Pneumonia (as a Percentage of Community-Acquired Pneumonias) are Generally Higher in Populations Admitted from Nursing Homes or Extended Care Facilities (J Am Geriatr Soc, 1986) [MEDLINE]
Study of Aspiration Pneumonia According to the Site of Acquisition (J Am Geriatr Soc, 2006) [MEDLINE]: n = 1,946 adults admitted with pneumonia (from 6 Alberta, Canada hospitals)
Aspiration Pneumonia Accounted for 10% of Community-Acquired Pneumonia Cases
Most Aspiration Pneumonia Cases were Associated with Altered Mental Status Due to Alcohol, Drugs, and/or Liver Disease
Aspiration Pneumonia Accounted for 30% of Continuing Care Facility-Acquired Pneumonia Cases
Approximately 72% of Aspiration Pneumonia Cases were Due to Neurologic Disease Associated with Dysphagia
Multiple Risk Factors May Be Present and Engender Additive/Multiplicative Risk of Aspiration Pneumonia
In a Meta-Analysis in Frail Elderly Patients, Dysphagia Increased the Odds Ratio for Aspiration Pneumonia by a Factor of 9.4 (J Dent Res, 2011) [MEDLINE]
When Cerebrovascular Disease was Added, the Odds Ratio Increased to 12.9
Aspiration May Occur During Initial Placement of the Endotracheal Intubation (Typically Manifested During or Immediately Following Intubation), Due to Emesis with Aspiration at the Time of Intubation (see Invasive Mechanical Ventilation-Adverse Effects and Complications)
In Prospective Observational Studies, the Use of Point-of-Care Gastric Ultrasound Has Been Demonstrated to Predict the Risk of Aspiration During Endotracheal Intubation in the Emergency Department Setting (BMC Emerg Med, 2023) [MEDLINE]
Visible Aspiration was Higher in Participants with a Distended Gastric Status (χ2 = 16.880, p = < 0.001)
Median Gastric Volume in the Patients who Aspirated was 146.37 mL (Ranged: 111.59-201.01 mL)
Using Receiver Operating Characteristic (ROC) Analysis, a Cut-Off of CC Diameter ≥ 2.35 cm (Sensitivity 88%, Specificity 91%) and AP Diameter ≥ 5.15 cm (Sensitivity 88%, Specificity 87%) Predicted Aspiration
Calculated Gastric Ultrasound Cross-Sectional Area Cut-Off ≥9.27 cm2 (Sensitivity 100%, Specificity 87%) and an Ultrasound Gastric Volume ≥111.594 mL (Sensitivity 100%, Specificity 92%) Predicted Aspiration
Aspiration of Oropharyngeal Secretions is Common During the Ongoing Use of Endotracheal Tubes and Tracheostomy Tubes
Aspiration Pneumonia Can Occur as an Early Adverse Effect/Complication (Manifest Within Hours-Weeks After Intubation) Due to Pooling of Pharyngeal Pooling of Oropharyngeal Secretions Above the Endotracheal Tube Cuff with Subsequent Aspiration, as Well as Delayed Triggering of the Swallowing Response (see Invasive Mechanical Ventilation-Adverse Effects and Complications) (Crit Care Med, 1990) [MEDLINE]
Presence of Gag Reflex Does Not Confer Protection Against Aspiration with Endotracheal Intubation or Tracheostomy (Crit Care Med, 1990) [MEDLINE]
Polyurethane Endotracheal Tube Cuffs Decrease the Amount of Leakage Around the Cuff, as Compared to Polyvinyl Chloride Cuff Endotracheal Tubes (Crit Care Med, 2008) [MEDLINE]
Aspiration Can Occur During Extubation
Aspiration Can Occur Following Extubation
In Patients Extubated Following Acute Respiratory Failure, Dysphagia/Aspiration are Observed in 20% of Cases (Chest, 2014) [MEDLINE]
The Frequency of Swallowing Dysfunction Decreases Over Time from Extubation, But Up to 35% of Patients with Swallowing Dysfunction at the Time of Extubation Continue to Manifest Swallowing Dysfunction at the Time of Discharge
No Clinical Factors Reliably Predict if a Patient Will Aspirate
Aspiration of Oropharyngeal Secretions is Common with the Ongoing Use Endotracheal Tubes and Tracheostomy Tubes
Presence of Gag Reflex Does Not Confer Protection Against Aspiration with Endotracheal Intubation or Tracheostomy (Crit Care Med, 1990) [MEDLINE]
Physiology
Due to Pooling of Pharyngeal Pooling of Oropharyngeal Secretions Above the Endotracheal Tube Cuff with Subsequent Aspiration (Crit Care Med, 1990) [MEDLINE] (Br J Anaesth, 2012) [MEDLINE]
Due to Delayed Triggering of the Swallowing Response (Crit Care Med, 1990) [MEDLINE] (Br J Anaesth, 2012) [MEDLINE]
Swallowing Dysfunction (Particularly Disorder of the Pharyngeal Phase) and Aspiration are Common with Tracheostomy (Chest, 1994) [MEDLINE]: increasing age increases the risk of aspiration and aspiration is frequently silent
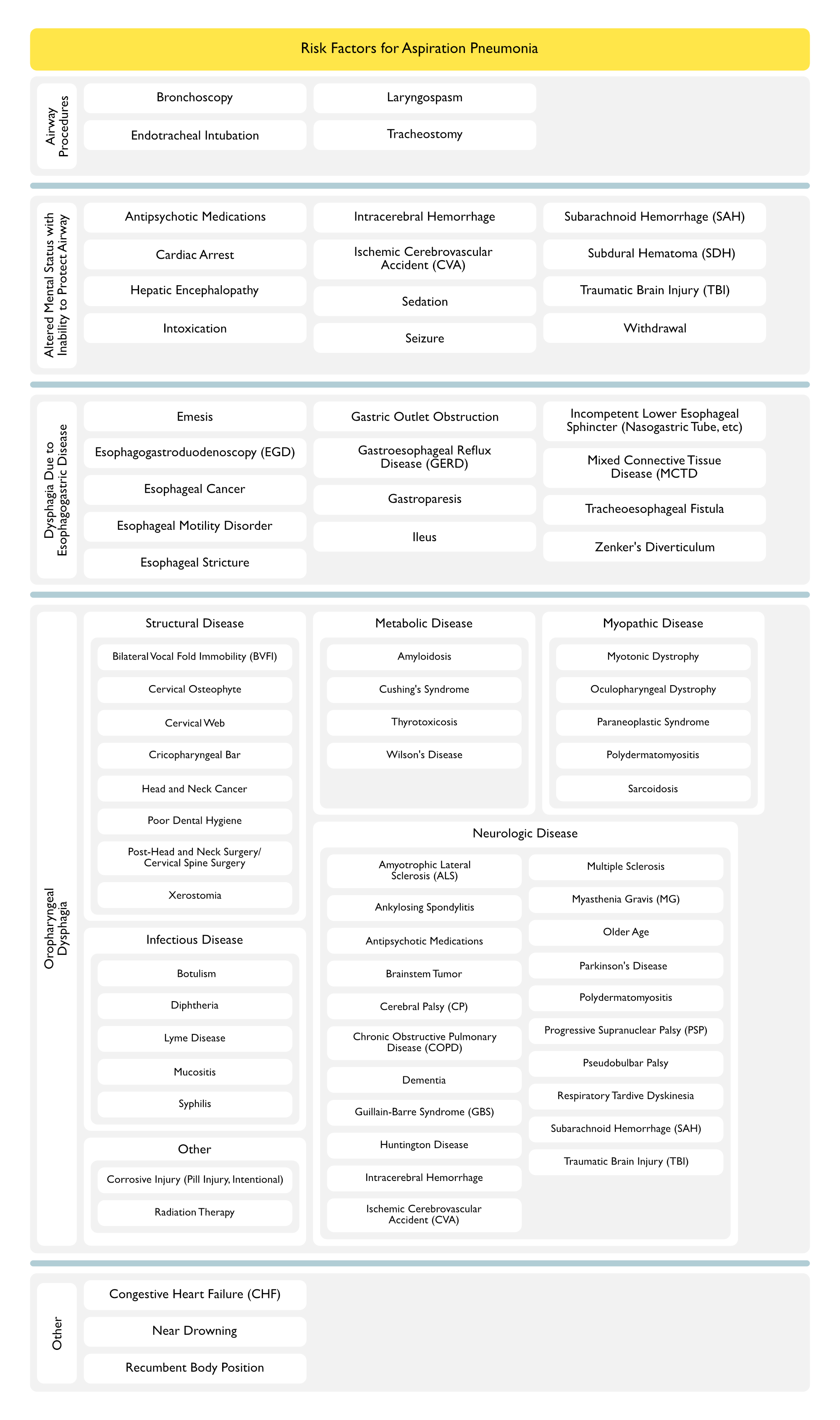
Altered Mental Status with Inability to Protect Airway
Antipsychotic Medications
Epidemiology
In a Large Study Involving 146,552 Hospitalized Patients, Antipsychotic Medications were Found to Increase the risk of Aspiration Pneumonia by 1.5-Fold (J Am Geriatr Soc, 2017) [MEDLINE]
Physiology
May Be Related to Alteration in Mental Status and/or Dysphagia/Swallowing Dysfunction (Expert Rev Clin Pharmacol, 2019) [MEDLINE]
Early-Onset Post-Cardiac Arrest (Aspiration) Pneumonia Developed within 3 Days Post-Cardiac Arrest in 65% of the Patients and the Risk was Found to Be Associated with the Use of Therapeutic Hypothermia (Am J Respir Crit Care Med, 2011) [MEDLINE]
A Target Temperature of 36°C May Be Associated with a Lower Risk of Pneumonia (Chest 2018) [MEDLINE]
Physiology
Multiple Factors May Contribute to Cardiac Arrest-Associated Aspiration Pneumonia
Liver Disease was Present in 11.3% of Aspiration Pneumonia Cases (as Compared to 3.7% of Community-Acquired Pneumonia Cases) (Am J Med, 2013) [MEDLINE]
In a Study Examining Aspiration Risk Factors on the Risk of Community-Onset Pneumonia, Dementia Had an Odds Ratio of 5.2, Poor Performance Status Had an Odds Ratio of 3.31, and the Use of Sleeping Pills Had an Odds Ratio of 2.08 (Clin Interv Aging, 2017) [MEDLINE]
Patients with ≥2 Risk Factors Had an Increased Incidence of Recurrent Pneumonia and Increased 30-Day and 6-Month Mortality Rates with Rates Increasing in Association with the Number of Risk Factors
Nasogastric/Orogastric Tubes Impair the Function of the Lower Esophageal Sphincter, Increasing the Risk of Gastroesophageal Reflux
Enteral feeding Can Result in High-Volume Aspiration (Especially When Associated with Gastric Dysmotility, Poor Cough Reflex, and Altered Mental Status
However, In 3 Studies of Enteral Feeding Following Stroke (Total of >5000 Patients), Early Enteral Tube Feeding Improved Survival, as Compared to No Feeding, and in the First 2-3 weeks Following Stroke, Nasogastric Tube Feeding was Associated with Improved Survival and Functional Outcomes, as Compared to Percutaneous Enteral Tube Feeding (Health Technol Assess, 2006) [MEDLINE]
Enteral Feedings Tubes are Not Currently Recommended for Patients with Dementia (J Am Geriatr Soc, 2014) [MEDLINE]
Oropharyngeal Dysphagia (Due to Disease of the Pharynx/Upper Esophagus or Upper Esophageal Sphincter Dysfunction) (see Dysphagia)
General Comments
In Aspiration Pneumonia Cases Which Occur in Patients in Continuing Care Facilities, Neurologic Disease with Associated Dysphagia was a Risk Factor in 72% of Cases (J Am Geriatr Soc, 2006) [MEDLINE]
In a Group of Older Patients (>70 y/o) Admitted for Pneumonia, Oropharyngeal Dysphagia was Present in 55% of Cases (Age Ageing, 2010) [MEDLINE]
In a Case-Control Study of Elderly Patients, Oropharyngeal Dysphagia Increased the Risk of Community-Acquired Pneumonia (Odds Ratio: 11.9) and ws Present in 92% of the Patients with Pneumonia (Eur Respir J, 2013) [MEDLINE]
By Videofluoroscopic Evaluation, Only 16.7% of the Patients with Pneumonia were Able to Swallow Safely, as Compared to 80% of the Control Patients
In a Large Study Involving 146,552 Hospitalized Patients, Antipsychotic Medications were Found to Increase the risk of Aspiration Pneumonia by 1.5-Fold (J Am Geriatr Soc, 2017) [MEDLINE]
Physiology
May Be Related to Alteration in Mental Status and/or Dysphagia/Swallowing Dysfunction (Expert Rev Clin Pharmacol, 2019) [MEDLINE]
In a Study Examining Aspiration Risk Factors on the Risk of Community-Onset Pneumonia, Dementia Had an Odds Ratio of 5.2, Poor Performance Status Had an Odds Ratio of 3.31 and the Use of Sleeping Pills Had an Odds Ratio of 2.08 (Clin Interv Aging, 2017) [MEDLINE]
Patients with ≥2 Risk Factors Had an Increased Incidence of Recurrent Pneumonia and Increased 30-Day and 6-Month Mortality Rates with Rates Increasing in Association with the Number of Risk Factors
Stroke was Present in 26.9% of Aspiration Pneumonia Cases (as Compared to 9.5% of Community-Acquired Pneumonia Cases) (Am J Med, 2013) [MEDLINE]
The Frequency of CVA-Associated Pneumonia is Related to the Severity of Neurologic Injury and its Associated Immune Impairment (Cerebrovasc Dis, 2013 [MEDLINE]
Higher Rates of CVA-Associated Pneumonia Occur in Patients Requiring Intensive Care, as Compared to Patients Admitted to a General Stroke Unit
Older Age is Associated with Higher Prevalence of Comorbidities Which Predispose to Aspiration Pneumonia (Stroke, Degenerative Neurologic Disease, Institutionalization in Long-Term Care, etc) (Am J Med, 1998) [MEDLINE] (J Crit Care, 2015) [MEDLINE] (J Hosp Med, 2019) [MEDLINE]
Aspiration Results in a Larger Bacterial Inoculum from the Oropharynx and Prevalence of More Pathogenic Bacteria (Am J Respir Crit Care Med, 2003) [MEDLINE]
Congestive Heart Failure was Present in 28% of Aspiration Pneumonia Cases (as Compared to 17.1% of Community-Acquired Pneumonia Cases) (Am J Med, 2013) [MEDLINE]
Excess Gastric Acid Volume and Increased Intraabdominal Pressure
Recumbent Body Position
Physiology
Recumbency Increases the Risk of Reflux of Gastric Contents into the Oropharynx, Resulting in Aspiration
Physiology
Spectrum of Aspiration
Aspiration of Small Amounts of Oropharyngeal Secretions is Normal in Healthy Persons During Sleep (Chest, 1997) [MEDLINE]
In Addition, Microaspiration is Predominant Pathogenetic Mechanism of Most Pneumonias
Large-Volume Aspiration (Macroaspiration) of Colonized Oropharyngeal or Upper Gastrointestinal Contents Defines True Aspiration Pneumonia
Aspiration Syndromes May Involve the Airways or Pulmonary Parenchyma, Resulting in a Variety of Distinct Clinical Presentations (J Crit Care, 2015) [MEDLINE]
Aspirated Fluids or Material May Consist of Any of the Following
Aspiration Pneumonia vs Aspiration (Chemical) Pneumonitis
Aspiration Pneumonia is a Pulmonary Parenchymal Infection Caused by Specific Microorganisms
Chemical Pneumonitis is a Pulmonary Inflammatory Response to Irritative Gastric Contents
Bacterial Colonization of Human Oropharynx and Upper Airway
Bacteria Colonize the Oral Cavity (Including the Gingiva, Dental Plaque, and Tongue) (J Clin Microbiol, 2005) [MEDLINE] (J Bacteriol, 2010) [MEDLINE]
Pathogenic Bacteria (Gram-Negative Bacteria Which are Not Found in the Normal Host), May Emerge in the Elderly, Nursing Home Residents, Hospitalized Patients, and in Patients with Nasogastric Tubes (Isr Med Assoc J, 2003) [MEDLINE] (Chest, 2004) [MEDLINE] (J Gerontol A Biol Sci Med Sci, 2018) [MEDLINE]
Microbiology
In the 1970’s, Anaerobes (with or without Aerobes) were the Predominant Microbial Pathogens Associated with Aspiration Pneumonia (Am J Med, 1974) [MEDLINE] (Ann Intern Med, 1974) [MEDLINE] (Arch Intern Med, 1975) [MEDLINE] (Infect Dis Clin North Am, 2013) [MEDLINE]
Possible Explanations for Higher Rates of Anaerobes Reported in Older Studies of Aspiration Pneumonia
More Meticulous Culture Techniques Used in Older Studies
Differences in the Oropharyngeal Microflora Between Healthy Community Dwelling and Hospitalized Adults
Lesser Use of Antibiotics with Anaerobic Activity
Presentation of Patients Later in the Disease Course
However, Recent Studies Indicate that in Aspiration Pneumonia, There Has Been a Shift Toward Bacteria Usually Associated with Community-Acquired Pneumonia (CAP) and Hospital-Acquired Pneumonia (HAP)
Study of Aspiration Pneumonia Cases Who Required ICU Care (Intensive Care Med, 1993) [MEDLINE]
Main Isolates in Patients with Community-Acquired Aspiration Pneumonia
Enterobacteriaceae
Haemophilus Influenzae
Staphylococcus Aureus
Streptococcus Pneumoniae
Main Isolates in Patients with Hospital-Acquired Aspiration Pneumonia
Prospective Study of Microbiology in Aspiration Pneumonia and Ventilator-Associated Pneumonia (Chest, 1999) [MEDLINE]
In Aspiration Pneumonia Associated with Gastrointestinal Disorders, Enteric Gram-Negative Organisms were Predominant
In Community-Acquired Aspiration Events, Streptococcus Pneumoniae and Haemophilus Influenzae were Predominant
Only One Anaerobic Organism Non-Pathogenic) was Isolated in Their Patients
Prospective Study of Aspiration Pneumonia in Elderly Patients from a Long-Term Care Facility Who were Admitted to Intensive Care Unit (Am J Respir Crit Care Med, 2003) [MEDLINE]: n = 95
General Information
Overall, Only 54 Patients (of the n = 95) Had an Identified Microbial Etiology
Polymicrobial Infection was Present in 22% of the 54 Patients in Whom a Microbial Etiology was Determined
Gram-Negative (Aerobic) Bacilli (Haemophilus Influenzae, E. Coli, Klebsiella Pneumoniae, Serratia, Proteus Mirabilis, Enterobacter Cloacae, Pseudomonas Aeruginosa) were Present in 49% of Cases
Gram-Negative Bacilli were the Most Common Isolates
Anaerobic Bacteria (Prevotella, Fusobacterium, Bacteroides, Peptostreptococcus) were Present in Only 16% of Cases
Staphylococcus Aureus was Present in 12% of Cases
Streptococcus Species were Present in 9% of Cases
Streptococcus Pneumoniae was Present in 7% of Cases
Japanese Study of Patients with Lung Abscess (Respiration, 2010) [MEDLINE]: n = 212
Streptococcus was Present in 60% of Cases
Streptococcus was the Most Common Pathogen
Anaerobes were Present in 26% of Cases
Anaerobes were the Second Most Common Pathogens
Study of Aspiration Pneumonia Documenting a Shift to Bacteria Usually Associated with Community-Acquired Pneumonia and Hospital-Acquired Pneumonia (Infect Dis Clin North Am, 2013) [MEDLINE]
Anaerobes are Now Recovered Less Frequently
In Hospital-Acquired Aspiration Pneumonia, Anaerobes are Even Less Common, with Streptococcus, Staphylococcus Aureus, and Gram-Negative Bacilli Predominating (Intensive Care Med, 1993) [MEDLINE] (Chest, 1999) [MEDLINE] (NEJM, 2001) [MEDLINE] (Am J Respir Crit Care Med, 2003) [MEDLINE] (Arch Intern Med, 2007) [MEDLINE] (Infection, 2008) [MEDLINE] (Thorax, 2010) [MEDLINE]
Diagnosis
Assessment of Swallowing Function
Bedside Swallowing Evaluation
Relatively Insensitive for Evidence of Aspiration in Patients with Tracheostomy, Since up to 77% of Aspiration was Silent (Chest, 1994) [MEDLINE] (Chest, 1996) [MEDLINE]
Gag Reflex
Does Not Predict Adequacy of Swallowing Function (as the Gag Reflex Uses Different Muscles than Swallowing and Many Patients without Gag Can Swallow Normally)
Alveolar Infiltrate: often located in dependent lung region (particularly in the superior segment of the right lower low)
Bibasilar Fibrosis: may be seen in cases of chronic aspiration
Clinical Presentations
General Comments
Aspiration of Tube Feedings/Blood
Aspiration of Tube Feedings/Blood Generally Does Not Cause Either a Bacterial Pneumonia or Chemical Pneumonitis, Since the Aspirate is Higher pH and Uncontaminated by Bacteria (NEJM, 2019) [MEDLINE]
Unwitnessed Aspiration
In These Cases, it is Generally Difficult to Distinguish Between Chemical Pneumonitis, Aspiration Pneumonia, and/or Aspiration of Bland Material
In a Study of Older Patients (>65 y/o) with Foreign Body Aspiration, the Event was Clinically Recognized in Only 29% of Cases, Leading to a DIagnostic Delay of 1-3 mos (Clin Interv Aging, 2014) [MEDLINE]
Food Material (Bone Fragments, Plants, etc) Accounted for >80% of the Episodes
Chest Radiographic Findings were Localized to the Right Lung in 65% of the Cases
Flexible Bronchoscopy Removed the Foreign Body Successfully in All Cases (Predominantly in the Right Lower Lobe Bronchus)
Typically Associated with Chronic Aspiration (Microaspiration)
Physiology
Smaller Volumes of Acid Aspiration (Perhaps Over a Long Period of Time) Likely Result in Less Severe Aspiration/Chemical Pneumonitis, Recurrent Aspiration/Chemical Pneumonitis, and/or Pulmonary Fibrosis (Chest, 1976) [MEDLINE] (Chest, 1988) [MEDLINE]
Approximately 13-26% of Patients with Observed Aspiration Develop Pulmonary Superinfection During Their Clinical Course (Am Rev Respir Dis, 1976) [MEDLINE]
Chest X-Ray is Less Sensitive than Chest CT for the Detection of Pulmonary Infiltrates in Pneumonia (Including Aspiration Pneumonia)
In a Study of 208 Patients with Pneumonia (Aspiration Pneumonia Accounted for 6o% of the Cases), the Chest X-Ray was Negative in 28% of Cases (with Pneumonia Detected by Chest CT Scan) (J Infect Chemother 2015) [MEDLINE]
Infiltrates are Most Commonly Posterior and Dependent in Location (Accounting for the Fact that Most Patients Aspiration in the Recumbent Position) and May Appear as Bronchopneumonia (Diffuse Pattern)
In a Study of 53 Patients with Fluoroscopically Documented Dysphagia and Pneumonia, More Patients Had Bronchopneumonia than Lobar Pneumonia (68% vs 15%) (Geriatr Gerontol Int, 2013) [MEDLINE]
92% of Patients in This Study Had Posterior Infiltrates
A Decreased Performance Status was Significantly Associated with a Diffuse Distribution of Infiltrates
In a Study of 65 Intubated Patients with Risk Factors for Aspiration and a New Pulmonary Infiltrate, Using Quantitative Bronchoalveolar Lavage Cultures, Serum Procalcitonin Measurement on Days 1 and 3 Did Not Distinguish the 32 Patients with Culture-Positive Aspiration Pneumonia from the 33 with Culture-Negative Pneumonitis (Crit Care Med, 2011) [MEDLINE]
In Mechanically Ventilated Patients, Airway Secretion α-Amylase Levels (from Salivary and Pancreatic Sources) are Elevated (Reflecting the Number of Risk Factors for Aspiration), But Have an Unclear Role in the Diagnosis of Ventilator-Associated Aspiration Pneumonia (Crit Care Med, 2013) [MEDLINE] (Crit Care Med, 2018) [MEDLINE]
Clinical
General Comments
Time of Onset
Onset of Parenchymal Aspiration Pneumonia is Typically within Hours-Few Days After the Aspiration Event
However, Anaerobic Aspiration May Be Subacute Due to Less Virulent Bacteria
Severity of Illness
In a Study of Patients >80 y/o with Pneumonia, Aspiration Pneumonia Had a Higher Mortality Rate, Higher Serum Sodium Level, and Worse Renal Function, as Compared to Patients with Non-Aspiration Pneumonia (Rev Esp Quimioter, 2015) [MEDLINE]
In 1946, Mendelson Described Gastric Acid Aspiration with Aspiration/Chemical Pneumonitis (and Acute Respiratory Distress Syndrome within 2 hrs) in a Series of Young Obstetric Patients Undergoing Ether Anesthesia (Am J Obstet Gynecol, 1946) [MEDLINE]
All Patients Recovered within 24-36 hrs with Radiogrpahic Resolution within 4-7 Days without the Use of Antibiotics
Aspiration/Chemical Pneumonitis May Occur During Laryngoscopic Intubation for General Anesthesia, During Extubation, etc
Chemical Pneumonitis is Uncommon with Modern Anesthesia Technique (as Low as 1 Case Per 3,216 Procedures) (Anesthesiology, 1993) [MEDLINE]
Higher Risk Occurs During Emergency Surgery
Lower Risk Occurs During Elective Surgery
While the Use of Acid-Suppressing Medication (Proton-Pump Inhibitors, Histamine H2 Blockers, etc) is Associated with an Increased Risk of Community-Acquired Pneumonia/Hospital-Acquired Pneumonia (Both of Which are Related to Gastric Overgrowth by Gram-Negative Rod Bacteria), the Neutralization of Gastric pH by These Agents Decreases the Risk of Chemical Pneumonitis (PLoS One, 2015) [MEDLINE] (Anaesth Intensive Care, 2015) [MEDLINE]
Physiology
Macroaspiration of Gastric Contents May Result in Chemical Pneumonitis, But Only with Large-Volume, Low pH (Usually <2.5) Aspiration (NEJM, 2019) [MEDLINE]
In Animal Models of Aspiration, Chemical Pneumonitis Develops Only After Exposure to at Least 120 ml of Low pH (pH = 1) Gastric Contents (NEJM, 2019) [MEDLINE]
In Other Animal Studies, a Large Volume (Around 70 mL in an Adult Human) Inoculum with pH of ≤2.5 was required Cause Chemical Pneumonitis (Surgery, 1972) [MEDLINE]
Smaller Volumes of Acid Aspiration (Perhaps Over a Long Period of Time) Likely Result in Less Severe Aspiration/Chemical Pneumonitis, Recurrent Aspiration/Chemical Pneumonitis, and/or Pulmonary Fibrosis (Chest, 1976) [MEDLINE] (Chest, 1988) [MEDLINE]
Aspiration Gastric Acid, Resulting in an Inflammatory Reaction in the Lower Airways (Independent of Bacterial Infection of the Airways and/or Lungs)
Involves Pro-Inflammatory Tumor Necrosis Factor-α and Interleukin-8 (Crit Care Med, 2011) [MEDLINE]
Neutrophil Recruitment (Crit Care Med, 2011) [MEDLINE]
Pulmonary Surfactant Dysfunction
Reflex Airway Closure
Hyaline Membrane Formation
Alveolar Hemorrhage
Noncardiogenic Pulmonary Edema
Aspiration of Bile Acids May Also Elicit an Inflammatory Response (Chest, 2009) [MEDLINE]
Rapid (within 2 hrs) Developent of Pulmonary Infiltrates (Typically in Dependent Portions of the Lung or in Superior or Posterior Segments of the Lower Lobes, if Aspiration Occurred in the Recumbent Position)
Diffuse Pulmonary Infiltrates (in Patients with the Development of Acute Respiratory Distress Syndrome) (see Acute Respiratory Distress Syndrome)
In Up to 64% of Patients with Aspiration During General Anesthesia, Radiographic Abnormalities Do Not Develop (Crit Care Med, 2011) [MEDLINE]
Bronchoscopy (see Bronchoscopy): not usually necessary
Clinical
General Comments
In Up to 64% of Patients with Aspiration During General Anesthesia, Clinical Manifestations Do Not Occur (Crit Care Med, 2011) [MEDLINE]
Approximately 13-26% of Patients with Observed Aspiration Develop Pulmonary Superinfection During Their Clinical Course (Am Rev Respir Dis, 1976) [MEDLINE]
Acute Respiratory Distress Syndrome Occurs in Approximately 16.5% of Cases (Am J Respir Crit Care Med, 2011) [MEDLINE]
Frequency of Acute Respiratory Distress Syndrome is Higher in Patients with Concomitant Shock, Trauma, or Pancreatitis (Am J Respir Crit Care Med, 2011) [MEDLINE]
Prevention
Perioperative Measures To Decrease the Risk of Aspiration
No Food for at Least 8 hrs and No Clear Liquids for at Least 2 hrs Prior to Elective Surgery Involving General Anesthesia
Avoid Medications Which Promote Aspiration and Interfere with Swallowing (Sedatives, Antipsychotic Agents, Antihistamines, etc) (J Am Geriatr Soc, 2017) [MEDLINE]
Measures to Decrease Risk of Aspiration in Patient with Chronic Dysphagia
Dietary/Feeding Modifications
Speech Therapy-Guided Modification of Patient’s Diet is Recommended
Examples
Mechanical Soft Diet with Thickened Liquids (Rather than Pureed Food and Thin Liquids)
“Nutritional Rehabilitation” (Swallowing Exercises and Early Mobilization, etc) May Assist Patients with Dysphagia and Prevent Aspiration Pneumonia (J Gen Fam Med, 2017) [MEDLINE]
Useful Measures In Patients with Oropharyngeal Dysphagia (Chest, 2014) [MEDLINE]
Patient’s Chin Can Be Positioned Down with the Head Turned to One Side During Feeding
Swallow Small Volumes
Multiple Swallows
Coughing After Each Swallow
Oral Hygiene
Oral Hygiene Has an Inconsistent Clinical Effect on the Risk of Aspiration Pneumonia, Possibly Due to Various Study Design Issues (J Am Geriatr Soc, 2018) [MEDLINE]
Chlorhexidine Oral Care Has Been Demonstrated to Be Associated with Increased Mortality in Ventilated Patients (Possibly Due to Toxic Effects of Aspirated Chlorhexidine) (JAMA Intern Med 2014)
In Non-Ventilated Patients at Risk for Aspiration Pneumonia, a Meta-Analysis Demonstrated that Chlorhexidine Oral Care or Mechanical Oral Cleaning were Effective in Preventing Pneumonia (Odds Ratio: 0.4-0.6) (Infect Control Hosp Epidemiol, 2015)
In a Cluster-Randomized Trial of Nursing Home Patients (n = 834 Patients, Mean Observation Time of >1 Year), There was No Benefit of a Comprehensive Oral Care Program (Manual Tooth and Gum Brushing, Chlorhexidine Oral Washes, and Upright Positioning During Feeding) (Clin Infect Dis, 2015) [MEDLINE]
There was Radiographic Evidence of Pneumonia in 25% of the Patients
In a Randomized Trial (n = 252 Patients), Supplemental Nutrition Plus Daily Oral Cleaning Decreased the Frequency of Pneumonia (7.8%, vs 17.7% with Usual Care; p = 0.06) (Ann Nutr Metab 2017)
In a Case–Control Study (n = 539 Patients) Undergoing Surgery for Esophageal Cancer, Postoperative Pneumonia Developed in 19.1% of the Patients (Medicine-Baltimore, 2017)
Lack of Preoperative Oral Care (Tooth Scaling, Mechanical Cleaning, and Tooth Extraction if Necessary) was an Important Risk Factor
Elimination of Oral Intake
While Difficult, This May Be Required to Decrease the Risk of Aspiration in Patients with Chronic Dysphagia
Nasogastric Tube Feeding
This May Be Required to Decrease the Risk of Aspiration in Patients with Chronic Dysphagia
Feeding Should Be Administered in a Semirecumbent Position (Rather than Supine Position) to Minimize the Risk of Aspiration
Role of Nasogastric Tubes in Preventing Aspiration Pneumonia is Unclear
In a Study (n = 1260 Patients), Patients with a Nasogastric Tube in Place Did Not Have More Aspiration Events During Endoscopic Observation of Swallowing than Patients without a Nasogastric Tube (Arch Phys Med Rehabil, 2008) [MEDLINE]
Post-Pyloric Feeding is Not Superior to Gastric Feeding and the Monitoring of Post-Feeding Gastric Residual Volume May Not Decrease the Risk of Aspiration (Nutr Clin Pract, 2015) [MEDLINE]
For Stroke Patients (Especially Asian Patients), the Use of ACE Inhibitors to Control Blood Pressure Can Decrease the Risk of Aspiration Pneumonia (Possibly by Elevating Substance P Levels, Which Promotes Cough and Improves the Swallowing Reflex) (Am J Respir Crit Care Med, 2004) [MEDLINE] (Adv Ther, 2012) [MEDLINE]
The Antiplatelet Agent, Cilostazol, Has Been Demonstrated to Increase Substance P Levels, Decreasing the Risk of Post-Stroke Aspiration Pneumonia (Cerebrovasc Dis, 2013) [MEDLINE]
Measures to Decrease Risk of Aspiration in the Comatose Patient
Maintain Semirecumbent Body Position
In Comatose Patients, the Risk of Aspiration Pneumonia was Decreased by Maintaining the Patient in Either the Prone or Semirecumbent Body Position (Crit Care Med, 1999) [MEDLINE]
Preemptive Antibiotics in the Setting of Cardiac Arrest/Comatose Patient Requiring Emergent Intubation
General Comments
Preemptive Antibiotics May Be Utilized in Selected Patients with Coma or Post-Cardiac Arrest Encephalopathy to Decrease the Risk of Developing Aspiration Pneumonia
Clinical Efficacy-Cardiac Arrest
French Study of Early Antibiotic Administration in Patients Undergoing Therapeutic Hypothermia After Out-of-Hospital Cardiac Arrest (Targeted Temperature Management) (NEJM, 2019) [MEDLINE]
A 2-Day Amoxicillin-Clavulanate Course in Patients Underoing Therapeutic Hypothermia (32-34 Degrees C) After Cardiac Arrest with an Initial Shockable Rhythm Resulted in a Lower Incidence of Early Ventilator-Associated Pneumonia, as Compared to Placebo
There was No Significant Difference in Ventilator-Free Days or 28-Day Mortality Rate
Clinical Efficacy-Emergency Intubation of Comatose Patient
Cefuroxime Administered Post-Intubation of Patients Comatose Due to Head Injury or Stroke was Found to Be an Effective Prophylactic Strategy to Decrease the Incidence of Ventilator-Associated Pneumonia (Am J Respir Crit Care Med, 1997) [MEDLINE]
In Comatose Patients (Glasgow Coma Score ≤ 8), A Single Dose of Antibiotic Prophylaxis at the Time Intubation Might Decrease the Incidence of Early-Onset Ventilator-Associated Pneumonia, But Not Late-Onset Pneumonia (Chest, 2013) [MEDLINE]
Bronchoscopy May Be Considered in Selected Cases to Clear a Suspected Foreign Body from the Airway and/or to Obtain Bronchoalveolar Lavage (BAL) Samples for Culture
Antibiotics
Need for Antibiotic Treatment of Aspiration Pneumonia
Since it is Difficult to Exclude Bacterial Infection as a Contributing Factor in the Setting of Aspiration, Antibiotics are Commonly Prescribed Despite a Lack of Clear Clinical Benefit
In a Study of Comatose, Mechanically-Ventilated Patients with Aspiration, 46.7% of Patients Had Bacterial Aspiration Pneumonia (Based on Bronchoscopic Brush Samples) (Crit Care Med, 2017) [MEDLINE]
Authors Suggested that Routine Antibiotic Therapy Should Be Initiated Only if Bacterial Infection is Suspected, But May be Discontinued if Bronchoscopic Cultures are Negative
Retrospective Cohort Study of Adult Patients with Acute Aspiration Pneumonitis (Defined by Macroaspiration Event with Witnessed Vomiting/Choking on Food with New Radiographic Pulmonary Infiltrate in Non-Ventilated Patient) (Clin Infect Dis, 2018) [MEDLINE]: n = 200 patients with acute aspiration pneumonitis
Antimicrobial Prophylaxis Did Not Impact the 30-Day Mortalty Rate or Need for Critical Care
Duration of Antibiotic Therapy in Aspiration Pneumonia
Retrospective Study of Time to Clinical Stability in Community-Acquired Pneumonia vs Community-Acquired Aspiration Pneumonia (Intern Emerg Med, 2014) [MEDLINE]: n = 329 (community-acquired pneumonia cases and 329 community-acquired aspiration pneumonia cases)
In Community-Acquired Pneumonia, the Median Time to Clinical Stability was 4 Days
In Community-Acquired Aspiration Pneumonia, There was a Bimodal Distribution in the Median Time to Clinical Stability with Dual Peaks at Days 2 and 5
Community-Acquired Aspiration Pneumonia Patients Who Required >2 Days to Achieve Clinical Stability Had a Higher Mortality Rate, as Compared to Those with ≤2 Days (Odds Ratio 5.95; 95% CI: 2.85-12.4), and a Longer Hospital Stay (6.6 ± 5.8 vs 3.9 ± 1.2 Days; p < 0.001)
Time to Achieve Clinical Stability May Assist in Identifying Community-Acquired Aspiration Pneumonia Patients Who May Require a Shorter Course of Antimicrobial Therapy
Need for Anaerobic Antibiotic Coverage in the Treatment of Aspiration Pneumonia
Clinical Efficacy
Canadian Multicenter Retrospective Cohort Study of Anaerobic Antibiotic Coverage in the Treatment of Aspiration Pneumonia (Chest 2024) [MEDLINE]: n = 3,999 (18 hospitals in Ontario, Canada)
In-Hospital Mortality Rate was 30.3% in the Non-Anaerobic Therapy Group and 32.1% in the Anaerobic Therapy Group
Clostridium Difficile Colitis Occurred in ≤0.2% of Patients in the Non-Anaerobic Therapy Group and 0.8-1.1% of Patients in the Anaerobic Therapy Group
After Overlap Weighting of Propensity Scores, the Adjusted Risk Difference of Anaerobic Therapy Minus Non-Anaerobic Therapy was 1.6% (95% CI: -1.7% to 4.9%) for In-Hospital Mortality Rate and 1.0% (95% CI: 0.3% to 1.7%) for Clostridium Difficile Colitis
Authors Concluded that Anaerobic Coverage is Likely Unnecessary in Aspiration Pneumonia Because it is Associated with No Additional Mortality Benefit and an Increased Risk of Clostridium Difficile Colitis
Recommendations (American Thoracic Society-ATS and Infectious Diseases Society of America-IDSA Community-Acquired Pneumonia Practice Guidelines, 2019) (Am J Respir Crit Care Med, 2019) [MEDLINE]
Routine Addition of Anaerobic Antibiotic Coverage for Suspected Aspiration Pneumonia is Not Recommended, Unless Lung Abscess or Empyema is Suspected (Conditional Recommendation, Very Low Quality of Evidence)
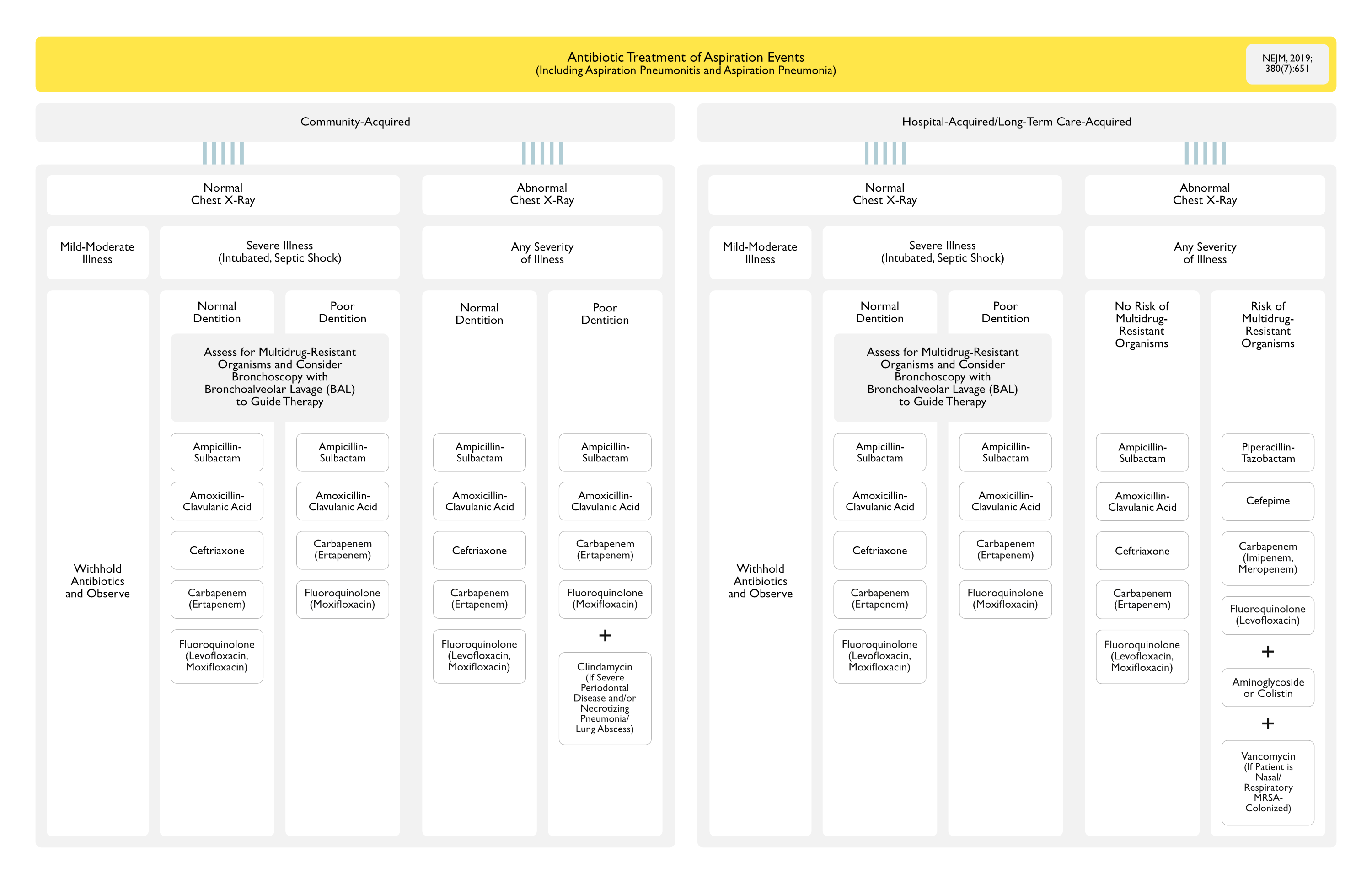
Antibiotic Selection in the Treatment of Aspiration Pneumonia
Antibiotic Selection Depends on the Site of Acquisition (Community, Hospital, or a Long-Term Care Facility) and Risk Factors for Multidrug-Resistant Organisms (MDRO’s)
Risk Factors Include Treatment with Broad-Spectrum Antibiotics in the Past 90 days and Hospitalization for at Least 5 Days
If Antibiotics are Initially Started, Reevaluation of the Need (After 24-48 hrs) for Continued Antibiotic Therapy is Recommended
With Mixed (Aerobic and Anaerobic) Infections, Elimination of Aerobic Organisms Usually Alters the Local Redox Potential, Eliminating the Anaerobes (NEJM, 2019) [MEDLINE]
Corticosteroids Have No Clinical Benefit in the Setting of Aspiration Pneumonia or Aspiration/Chemical Pneumonitis (Am J Med, 1977) [MEDLINE]
Prognosis
Mortality Rate
Patients at Risk for Aspiration Pneumonia Have a 30-Day Mortality Rate of 17.2%, as Compared to Other Patients (7.7%) (Am J Med, 2013) [MEDLINE]
However, After Adjusting for Greater Severity of Illness and Comorbidities, the Difference was Not Significant (Odd Ratio: 1.05; 95% Confidence Interval: 0.63-1.76; p = 0.8)
Patients at Risk for Aspiration Pneumonia were at Greater Risk for Poor Long-Term Outcome and Increased 1-Year Mortality Rate After Multivariate Assessment (Hazard Ratio: 1.73; 95% CI: 1.15-2.58) (Am J Med, 2013) [MEDLINE]
Aspiration Pneumonia is Associated with a Higher Mortality Rate than Other Types of Community-Acquired Pneumonia (29.4% vs 11.6%) (Ann Am Thorac Soc, 2018) [MEDLINE]
In This Study Which Included Data from 4,200 Hospitals, Aspiration was Found to Be Documented in 4-26% of Pneumonia Episodes
Consequently, the Risk-Adjusted Mortality (Used as a Quality Metric) is Lower for Hospitals Reporting a High Frequency of Aspiration than for Hospitals Reporting a Low Frequency of Aspiration
References
General
The aspiration of stomach contents into the lungs during obstetric anesthesia. Am J Obstet Gynecol. 1946;52:191 [MEDLINE]
Aspiration pneumonitis. Mayo Clin Proc. 1970;45(5):347 [MEDLINE]
Aspiration pneumonia: physiologic data following experimental aspiration. Surgery. 1972;72(2):238 [MEDLINE]
Pulmonary aspiration of gastric contents. Am Rev Respir Dis. 1976;114(6):1129 [MEDLINE]
Pulmonary fibrosis associated with tracheobronchial aspiration. A study of the frequency of hiatal hernia and gastroesophageal reflux in interstitial pulmonary fibrosis of obscure etiology. Chest. 1976;69(4):512 [MEDLINE]
Aspiration resulting from gastroesophageal reflux. A cause of chronic bronchopulmonary disease. Chest. 1988;93(4):676 [MEDLINE]
Pulmonary aspiration in mechanically ventilated patients with tracheostomies. Chest. 1994 Feb;105(2):563-6 [MEDLINE]
Identification of patients with acute lung injury. Predictors of mortality. Am J Respir Crit Care Med. 1995;152(6 Pt 1):1818 [MEDLINE]
Pneumonia in residents of long-term care facilities: epidemiology, etiology, management, and prevention. Am J Med. 1998;105(4):319 [MEDLINE]
The role of anaerobes in patients with ventilator-associated pneumonia and aspiration pneumonia: a prospective study. Chest. 1999;115(1):178 [MEDLINE]
Satisfaction of patients treated surgically for intractable aspiration. Chest. 1999 Nov;116(5):1251-6 [MEDLINE]
Aspiration pneumonia: dental and oral risk factors in an older veteran population. J Am Geriatr Soc. 2001;49(5):557 [MEDLINE]
Aspiration pneumonitis and aspiration pneumonia. N Engl J Med 2001; 344:665-71 [MEDLINE]
Microbiology of severe aspiration pneumonia in institutionalized elderly. Am J Respir Crit Care Med. 2003;167(12):1650. [MEDLINE]
Differences in the features of aspiration pneumonia according to site of acquisition: community or continuing care facility. J Am Geriatr Soc. 2006;54(2):296 [MEDLINE]
Health care-associated pneumonia requiring hospital admission: epidemiology, antibiotic therapy, and clinical outcomes. Arch Intern Med. 2007;167(13):1393 [MEDLINE]
Bile acid aspiration in suspected ventilator-associated pneumonia. Chest. 2009;136(1):118 [MEDLINE]
Nursing home-acquired pneumonia: a 10 year single-centre experience. Thorax. 2010;65(4):354 [MEDLINE]
Prevalence and prognostic implications of dysphagia in elderly patients with pneumonia. Age Ageing. 2010;39(1):39 [MEDLINE]
Early-onset pneumonia after cardiac arrest: characteristics, risk factors and influence on prognosis. Am J Respir Crit Care Med. 2011 Nov;184(9):1048-54 [MEDLINE]
Risk factors for aspiration in community-acquired pneumonia: analysis of a hospitalized UK cohort. Am J Med. 2013;126(11):995 [MEDLINE]
A comparison between time to clinical stability in community-acquired aspiration pneumonia and community-acquired pneumonia. Intern Emerg Med. 2014;9(2):143 [MEDLINE]
Aspiration pneumonia: a review of modern trends. J Crit Care. 2015 Feb;30(1):40-8. doi: 10.1016/j.jcrc.2014.07.011 [MEDLINE]
Periodontal-disease-associated biofilm: A reservoir for pathogens of medical importance. Microb Pathog. 2016;94:27 [MEDLINE]
Antipsychotics and the Risk of Aspiration Pneumonia in Individuals Hospitalized for Nonpsychiatric Conditions: A Cohort Study. J Am Geriatr Soc. 2017;65(12):2580 [MEDLINE]
Aspiration Pneumonia. N Engl J Med. 2019;380(7):651 [MEDLINE]
Dysphagia and risk of aspiration pneumonia: A nonrandomized, pair-matched cohort study. J Dent Sci. 2019;14(3):241 [MEDLINE]
Aspiration Pneumonia in Older Adults. J Hosp Med. 2019;14(7):429 [MEDLINE]
Risk Factors
Swallowing disorders in patients with prolonged orotracheal intubation or tracheostomy tubes. Crit Care Med. 1990;18(12):1328 [MEDLINE]
Risk factors for developing pneumonia within 48 hours of intubation. Am J Respir Crit Care Med 1999;159:1742-6 [MEDLINE]
FOOD: a multicentre randomised trial evaluating feeding policies in patients admitted to hospital with a recent stroke. Health Technol Assess 2006; 10:iii-iv, ix-x, 1-120 [MEDLINE]
Effect of positive expiratory pressure and type of tracheal cuff on the incidence of aspiration in mechanically ventilated patients in an intensive care unit. Crit Care Med. 2008;36(2):409 [MEDLINE]
Meta-analysis of dysphagia and aspiration pneumonia in frail elders. J Dent Res 2011;90:1398-404 [MEDLINE]
Symptoms of dysphagia in patients with COPD. J Bras Pneumol. Mar-Apr 2011;37(2):176-83. doi: 10.1590/s1806-37132011000200007 [MEDLINE]
Stroke-associated pneumonia: major advances and obstacles. Cerebrovasc Dis 2013;35:430-43 [MEDLINE]
Swallowing dysfunction after critical illness. Chest 2014;146:1681-9 [MEDLINE]
American Geriatrics Society Ethics Committee and Clinical Practice and Models of Care Committee. American Geriatrics Society feeding tubes in advanced dementia position statement. J Am Geriatr Soc 2014;62:1590-3 [MEDLINE]
Gastroesophageal reflux disease in COPD: links and risks. Int J Chron Obstruct Pulmon Dis. 2015 Sep 14;10:1935-49. doi: 10.2147/COPD.S77562. eCollection 2015 [MEDLINE]
Antipsychotics and the risk of aspiration pneumonia in individuals hospitalized for nonpsychiatric conditions: a cohort study. J Am Geriatr Soc 2017;65:2580-6 [MEDLINE]
Impact of the number of aspiration risk factors on mortality and recurrence in community-onset pneumonia. Clin Interv Aging 2017;12:2087-94 [MEDLINE]
Ventilator management and respiratory care after cardiac arrest: oxygenation, ventilation, infection, and injury. Chest 2018;153:1466-77 [MEDLINE]
A comprehensive review of swallowing difficulties and dysphagia associated with antipsychotics in adults. Expert Rev Clin Pharmacol. 2019 Mar;12(3):219-234. doi: 10.1080/17512433.2019.1577134 [MEDLINE]
Evaluation of the Swallowing and Voice Functions in Ankylosing Spondylitis Patients. Dysphagia. 2021 Jul 14. doi: 10.1007/s00455-021-10340-1 [MEDLINE]
Physiology
The bacteriology of aspiration pneumonia. Am J Med 1974;56:202-7 [MEDLINE]
Bacteriology of aspiration pneumonia: a prospective study of community-and hospital-acquired cases. Ann Intern Med 1974;81:329-31 [MEDLINE]
Bacteriologic flora of aspiration-induced pulmonary infections. Arch Intern Med 1975; 135:711-4 [MEDLINE]
Quantitative aspiration during sleep in normal subjects. Chest. 1997 May;111(5):1266-72. doi: 10.1378/chest.111.5.1266 [MEDLINE]
The role of anaerobes in patients with ventilator-associated pneumonia and aspiration pneumonia: a prospective study. Chest 1999;115:178-83 [MEDLINE]
Saliva secretion and oral flora in prolonged nasogastric tube-fed elderly patients. Isr Med Assoc J 2003;5:329-32 [MEDLINE]
Microbiology of severe aspiration pneumonia in institutionalized elderly. Am J Respir Crit Care Med 2003;167:1650-4 [MEDLINE]
Colonization of dental plaques: a reservoir of respiratory pathogens for hospital-acquired pneumonia in institutionalized elders. Chest 2004;126:1575-82 [MEDLINE]
Defining the normal bacterial flora of the oral cavity. J Clin Microbiol 2005;43:5721-32 [MEDLINE]
Bile acid aspiration in suspected ventilator-associated pneumonia. Chest 2009;136:118-24 [MEDLINE]
Effectiveness of meropenem for the treatment of aspiration pneumonia in elderly patients. Intern Med 2009;48:129-35 [MEDLINE]
The human oral microbiome. J Bacteriol 2010;192:5002-17 [MEDLINE]
How important are anaerobic bacteria in aspiration pneumonia: when should they be treated and what is optimal therapy. Infect Dis Clin North Am 2013;27:149-55 [MEDLINE]
Oropharyngeal dysphagia is a risk factor for community-acquired pneumonia in the elderly. Eur Respir J 2013;41:923-8 [MEDLINE]
Relationships of variations in the tongue microbiota and pneumonia mortality in nursing home residents. J Gerontol A Biol Sci Med Sci 2018;73:1097-102 [MEDLINE]
Diagnosis
Diagnostic use of serum procalcitonin levels in pulmonary aspiration syndromes. Crit Care Med 2011;39: 1251-6 [MEDLINE]
Bronchoalveolar lavage amylase is associated with risk factors for aspiration and predicts bacterial pneumonia. Crit Care Med 2013; 41:765-73 [MEDLINE]
Detection failure rate of chest radiography for the identification of nursing and healthcare-associated pneumonia. J Infect Chemother 2015;21:492-6 [MEDLINE]
Diagnosis and Treatment of Adults with Community-acquired Pneumonia. An Official Clinical Practice Guideline of the American Thoracic Society and Infectious Diseases Society of America. Am J Respir Crit Care Med. 2019 Oct 1;200(7):e45-e67. doi: 10.1164/rccm.201908-1581ST [MEDLINE]
Significance of mini bronchoalveolar lavage fluid amylase level in ventilator-associated pneumonia: a prospective observational study. Crit Care Med 2018;46:71-8 [MEDLINE]
Clinical
Clinical significance of pulmonary aspiration during the perioperative period. Anesthesiology 1993;78:56-62 [MEDLINE]
Aspiration-induced lung injury. Crit Care Med 2011;39:818-26 [MEDLINE]
Early identification of patients at risk of acute lung injury: evaluation of lung injury prediction score in a multicenter cohort study. Am J Respir Crit Care Med 2011; 183:462-70 [MEDLINE]
Computed tomography findings of aspiration pneumonia in 53 patients. Geriatr Gerontol Int 2013;13:580-5 [MEDLINE]
The clinical features of foreign body aspiration into the lower airway in geriatric patients. Clin Interv Aging 2014;9: 1613-8 [MEDLINE]
Clinical features and outcomes of aspiration pneumonia and non-aspiration pneumonia in octogenarians and nonagenarians admitted in a General Internal Medicine unit. Rev Esp Quimioter 2015;28:310-3 [MEDLINE]
Gastroesophageal reflux disease is a risk factor for severity of organizing pneumonia. Respiration. 2015;89(2):119-26 [MEDLINE]
Risk of community-acquired pneumonia with outpatient proton-pump inhibitor therapy: a systematic review and meta-analysis. PLoS One 2015;10(6):e0128004 [MEDLINE]
High-risk residual gastric content in fasted patients undergoing gastrointestinal endoscopy: a prospective cohort study of prevalence and predictors. Anaesth Intensive Care 2015;43:728-33 [MEDLINE]
Prevention
Protective effect of intravenously administered cefuroxime against nosocomial pneumonia in patients with structural coma. Am J Respir Crit Care Med 1997;155:1729-34 [MEDLINE]
Efficacy of single-dose antibiotic against early-onset pneumonia in comatose patients who are ventilated. Chest 2013;143: 1219-25 [MEDLINE]
Prevention of Early Ventilator-Associated Pneumonia after Cardiac Arrest. N Engl J Med. 2019;381(19):1831 [MEDLINE]
Treatment
Effects of corticosteroids in the treatment of patients with gastric aspiration. Am J Med. 1977;63(5):719 [MEDLINE]
Treatment of anaerobic pleuropulmonary infections. Ann Intern Med. 1975 Sep;83(3):375-89 [MEDLINE]
Metronidazole in the treatment of anaerobic infections. Am Rev Respir Dis 1979;120: 337-43 [MEDLINE]
Metronidazole vs clindamycin treatment of anerobic pulmonary infection: failure of metronidazole therapy. Arch Intern Med 1981;141:1424-7 [MEDLINE]
Aspiration pneumonia. Rev Infect Dis 1991;13:Suppl 9:S737-S742. 61. Levison ME, Mangura CT, Lorber B, et al. Clindamycin compared with penicillin for the treatment of anaerobic lung abscess. Ann Intern Med 1983;98:466- 71 [MEDLINE]
Clindamycin vs penicillin for anaerobic lung infections: high rate of penicillin failures associated with penicillin-resistant Bacteroides melaninogenicus. Arch Intern Med 1990;150:2525-9 [MEDLINE]
Is penicillin G an adequate initial treatment for aspiration pneumonia? A prospective evaluation using a protected specimen brush and quantitative cultures. Intensive Care Med. 1993;19(5):279 [MEDLINE]
Reappraisal of clindamycin IV monotherapy for treatment of mild-to-moderate aspiration pneumonia in elderly patients. Chest 2005;127:1276-82 [MEDLINE]
Infectious Diseases Society of America/American Thoracic Society Consensus Guidelines on the Management of Community-Acquired Pneumonia in Adults. Clin Infect Dis. 2007 Mar 1;44 Suppl 2(Suppl 2):S27-72. doi: 10.1086/511159 [MEDLINE]
Moxifloxacin vs ampicillin/ sulbactam in aspiration pneumonia and primary lung abscess. Infection 2008;36: 23-30 [MEDLINE]
Diagnosis and Treatment of Adults with Community-acquired Pneumonia. An Official Clinical Practice Guideline of the American Thoracic Society and Infectious Diseases Society of America. Am J Respir Crit Care Med. 2019 Oct 1;200(7):e45-e67. doi: 10.1164/rccm.201908-1581ST [MEDLINE]
Anaerobic antibiotic coverage in aspiration pneumonia and the associated benefits and harms: A retrospective cohort study. Chest. 2024 Feb 20:S0012-3692(24)00260-5. doi: 10.1016/j.chest.2024.02.025 [MEDLINE]
Prognosis
Risk factors for aspiration in community-acquired pneumonia: analysis of a hospitalized UK cohort. Am J Med. 2013 Nov;126(11):995-1001. doi: 10.1016/j.amjmed.2013.07.012 [MEDLINE]
Variation in the diagnosis of aspiration pneumonia and association with hospital pneumonia outcomes. Ann Am Thorac Soc 2018;15:562-9 [MEDLINE]