Auscultation Over Bilateral Lung Fields and Auscultation Over the Epigastric Area: note that auscultation over the lung field alone is inadequate to confirm endotracheal tube placement (epigastric auscultation is additionally required to confirm a lack of breath sounds in that location)
Clinical Efficacy
Auscultation Alone Mistakenly Identifies Location of the Endotracheal Tube in 16% of Cases (Anesth Analg, 1986) [MEDLINE]
Observation of Chest Wall Movement is an Unreliable Means of Confirming Endotracheal Tube Placement, as Chest Wall Movement May Occur in Esophageal Intubation (Anaesth Intensive Care, 1980) [MEDLINE]
Single-View (Antero-Posterior) CXR Cannot Reliably Confirm Endotracheal Intubation: although it is usually obtained to determine the location of the distal tip of the endotracheal tube
Condensation in Endotracheal Tube (“Fogging”)
Clinical Efficacy
Observation of Condensation (Fogging) in the Endotracheal Tube is an Unreliable Means of Confirming Endotracheal Tube Placement, as Condensation Occurs in the Endotracheal Tube in 83% of Esophageal Intubations (Ann Emerg Med, 1998) [MEDLINE]
Endotracheal Introducer (Eschmann Introducer or Gum Elastic Bougie)
Technique
Bougie is Inserted and Advanced, Feeling the “Clicks” of the Tracheal Rings
Sensitivity of Ring Clicks in the Detection of Endotracheal Intubation: 95%
End-Tidal Carbon Dioxide Detection
General Comments
End-Tidal Carbon Dioxide Detection is Most Accurate Means of Confirming Endotracheal Tube Placement in the Non-Cardiac Arrest Patient: end-tidal carbon dioxide detection is a standard of care practice to confirm appropriate endotracheal intubation
In the Setting of Cardiac Arrest (without a Detectable Pulse), Gas Exchange in the Lungs is Markedly Decreased and Carbon Dioxide May Not Be Detectable Despite Appropriate Endotracheal Tube Positioning in the Trachea (Crit Care Med, 1985) [MEDLINE]
However, the Detection of Carbon Dioxide Which Persists for 6 Breaths in the Cardiac Arrest Patient Indicates Appropriate Endotracheal Tube Positioning in the Trachea
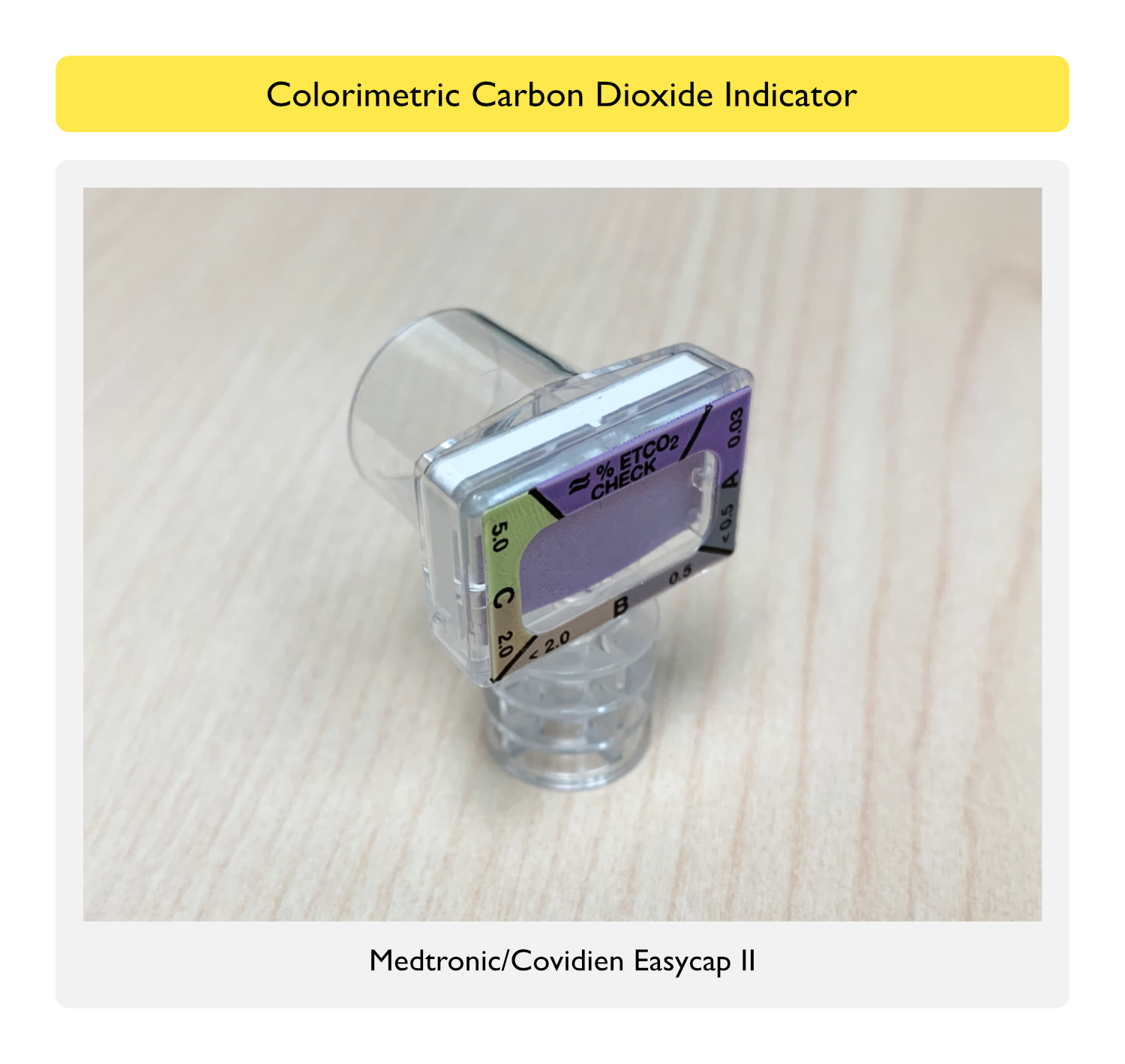
Colorimetric Carbon Dioxide Indicator
Principle/Technique: colorimetric carbon dioxide indicators use sulfonephthalein-impregnated pH-sensitive (litmus) filter paper as an indicator which tidally changes (breath by breath) from purple to yellow in the presence of exhaled carbon dioxide
Easy CAP II (Medtronic)
A Range Corresponds to ETCO2 <0.5%: dark tan-purple
B Range Corresponds to ETCO2 0.5-2%: dark tan-light tan
C Range Corresponds to ETCO2 2-5%: light tan-yellow
False-Positive Results: yellow color change without successful endotracheal intubation
Difficult Intubation with Prolonged Bag Ventilation: air previously pushed into the stomach during bag ventilation may cause yellow color change during the first few breaths
However, if Color Remains Yellow After >4-5 breaths, this Indicates Endotracheal Intubation (Anesth Analg, 1989) [MEDLINE]
Epinephrine (see Epinephrine): acidic medication which can cause (non-tidal) yellow color change
Lidocaine (see Lidocaine): acidic medication which can cause (non-tidal) yellow color change
Regurgitation of Gastric Contents During Intubation: gastric acid can cause (non-tidal) yellow color change
False-Negative Results: lack of yellow color change even with successful endotracheal intubation
Acute Pulmonary Embolism (PE) (see Acute Pulmonary Embolism): due to decreased pulmonary blood flow and decreased delivery of carbon dioxide to the lungs
Airway Obstruction: indicator may not turn yellow, due to poor carbon dioxide exchange across the obstructed airway (Emerg Med J, 2003) [MEDLINE]
Cardiac Arrest (see Cardiac Arrest: due to decreased pulmonary blood flow and decreased delivery of carbon dioxide to the lungs
If Chest Compressions are Adequate (with Adequate Blood Flow to the Lungs), Indicator Will Likely Turn Yellow
Indicator Has Only 69% Sensitivity for Endotracheal Intubation When Used During Cardiopulmonary Resuscitation (Ann Emerg Med, 1992) [MEDLINE]
Endotracheal Tube Cuff Leak
When Using Colorimetric Carbon Dioxide Indicator: cuff leak (with endotracheal tube still properly positioned in the trachea) will typically produce a weak yellow color change (due to loss of carbon dioxide around the endotracheal tube)
When Using Waveform Capnography: cuff leak (with endotracheal tube still properly positioned in the trachea) results in decreased amplitude of the plateau (due to loss of carbon dioxide around the endotracheal tube)
Clinical Efficacy
Sensitivity of End-Tidal Carbon Dioxide Detection Approaches 100% in Non-Cardiac Arrest Patients
Sensitivity of End-Tidal Carbon Dioxide Detection is Variable in Cardiac Arrest Patients: ranges from 62-100% in various studies (depending on the modality used and the duration of cardiac arrest)
In Non-Cardiac Arrest, Infrared Capnometry and Infrared Capnography Have a 100% Sensitivity/100% Specificity in Detecting Endotracheal Intubation (Intensive Care Med. 2002) [MEDLINE]
In Cardiac Arrest, Infrared Capnometry Has a 88% Sensitivity/100% Specificity in Detecting Endotracheal Intubation (Intensive Care Med. 2002) [MEDLINE]
Principle/Technique: end-tidal carbon dioxide monitor attached to the end of the endotracheal tube uses infrared absorption to detect carbon dioxide
Displays Either Waveform Capnography or Digital Readout
Clinical Efficacy
Sensitivity of End-Tidal Carbon Dioxide Detection Approaches 100% in Non-Cardiac Arrest Patients
Sensitivity of End-Tidal Carbon Dioxide Detection is Variable in Cardiac Arrest Patients: ranges from 62-100% in various studies (depending on the modality used and the duration of cardiac arrest)
In Non-Cardiac Arrest, Infrared Capnometry and Infrared Capnography Have a 100% Sensitivity/100% Specificity in Detecting Endotracheal Intubation (Intensive Care Med. 2002) [MEDLINE]
In Cardiac Arrest, Infrared Capnometry Has a 88% Sensitivity/100% Specificity in Detecting Endotracheal Intubation (Intensive Care Med. 2002) [MEDLINE]
Esophageal Detector Device
Technique
Uses Suction Applied with Syringes (or Bulb Suction Device) to Distinguish the Trachea from Esophagus
Trachea is Rigid and Allows Free Flow of Air into the Device
Esophagus is Collapsible and Does Not Allow Free Flow of Air When Suction is Applied
Transtracheal Ultrasound
Technique
Advantages
Technique Can Be Performed Quickly and Offers Real-Time Information
Technique is Independent of Pulmonary Blood Flow and Does Not Require Lung Ventilation
Clinical Efficacy
Systematic Review/Meta-Analysis of Transtracheal Ultrasound for Confirmation of Endotracheal Tube Placement (Can J Anaesth, 2015) [MEDLINE]: n = 11 studies
Transtracheal Ultrasound is a Useful Tool to Confirm Endotracheal Tube Placement with Acceptable Sensitivity/Specificity: it can be used as a preliminary test in emergency situations before final confirmation by capnography
Sensitivity: 98%
Specificity: 98%
Systematic Review/Meta-Analysis of Transtracheal Ultrasound for Confirmation of Endotracheal Tube Placement (Resuscitation, 2015) [MEDLINE]
Transtracheal Ultrasound is a Useful Tool to Confirm Endotracheal Tube Placement
Sensitivity: 93%
Specificity: 97%
Combination of Tracheal (to Determine Endotracheal Tube Position) and Pleural Ultrasound (to Detect Lung Sliding) is Superior to Auscultation in Determining Endotracheal Tube Location (Anesthesiology, 2016) [MEDLINE]: small, randomized trial
Recommendation (2022 American Society of Anesthesiologists Practice Guidelines for Management of the Difficult Airway) (Anesthesiology, 2022) [MEDLINE]
Recommendations for Confirmation of Tracheal Intubation
Confirm Endotracheal Intubation Using Capnography or End-Tidal Carbon Dioxide Monitoring
When Uncertain About the Location of the Endotracheal Tube, Determine Whether to Either Remove it and Attempt Ventilation or Use Additional Techniques to Confirm Endotracheal Rube Positioning
Exclusion of Mainstem Bronchial Endotracheal Tube Placement
CXR May Be Used to Confirm Endotracheal Tube Placement
Depth of Endotracheal Tube Insertion
Technique
Depth of Endotracheal Tube Insertion May Be Used to Confirm Endotracheal Tube Placement
Measurement at Teeth/Gums is Preferred, Since These are Fixed Landmarks
Clinical Efficacy
Endotracheal Tube is Usually Inserted to a Depth of 20-21 cm in Females and 22-23 cm in Males (BMJ, 2010) [MEDLINE]
Transtracheal Ultrasound
Clinical Efficacy
Transtracheal Ultrasound May Be Used to Confirm Ventilation Via Detection of Lung Sliding (Acta Anaesthesiol Scand, 2011) [MEDLINE]: lung sliding observed in only one lung indicates mainstem bronchial intubation
Combination of Tracheal (to Determine Endotracheal Tube Position) and Pleural Ultrasound (to Detect Lung Sliding) is Superior to Auscultation in Determining Endotracheal Tube Location (Anesthesiology, 2016) [MEDLINE]: small, randomized trial
Exchange of Endotracheal Tube
Reasons for Exchange of Endotracheal Tube
Endotracheal Tube Cuff Leak
Discrepancy Between Endotracheal Tube Size and Tracheal Diameter (Especially in a Patient with Tracheomalacia)
Pilot Balloon Line or Cuff Leak: some cases of severed pilot balloon lines can be remedied with a pilot balloon line repair kit (assuming the leak is at/near the pilot balloon itself, allowing the pilot balloon line to be cut and repaired)
Mucous Plugging Due to Inadequate Saline Lavage and Suctioning of the Endotracheal Tube
Example: in postoperative patients with tracheal resection, suctioning is frequently discouraged to avoid disruption of the anastomosis -> these patients can rapidly develop concretions within the endotracheal tube within a matter of days, leading to life-threatening endotracheal tube obstruction with inability to ventilate
Gradual Development of Endotracheal Tube Obstruction is Manifested by an Increasing Peak Airway Pressure-Plateau Pressure Difference
Risks of Endotracheal Tube Exchange
Airway Trauma: since intubation itself contributes to at least some degree of laryngeal and tracheal mucosal injury (even in the best of circumstances), reintubations can be expected to increase the risk of this trauma to some extent
Gum Elastic Bougie (Plastic Stylet): a plastic intubating stylet is the most commonly used method to change a dysfunctional endotracheal tube in a patient whose airway is not anticipated to be difficult
While Endotracheal Tube Change Can Be Performed Blindly (without Concomitant Airway Visualization) in Many Cases, Use of a Direct Laryngoscope/Video Laryngoscope is Highly Recommended in Case the Operator is Unable to Pass the New Endotracheal Tube Through the Vocal Cords
Endotracheal Tube Changer: a plastic hollow-bore tube changer (with adapters to allow either supplemental oxygen therapy or bag ventilation) is preferred in a patient whose airway is anticipated to be difficult
While Endotracheal Tube Change Can Be Performed Blindly (without Concomitant Airway Visualization) in Many Cases, Use of a Direct Laryngoscope/Video Laryngoscope is Highly Recommended in Case the Operator is Unable to Pass the New Endotracheal Tube Through the Vocal Cords
Removal of the Endotracheal Tube with Reintubation by Any of the Methods Described Above: this method can be used by experienced operators in a patient whose airway is not anticipated ot be difficult
Endotracheal Tube (ETT) Movement with Head Positioning
ETT Tip Movement Follows Direction of Chin Movement
Neck Flexion (Chin Downward): ETT tip moves downward
Neck Extension (Chin Upward): ETT tip moves upward
Inability to Intubate
General Comments
Supraglottic Airways Can Be Placed into the Pharynx and Utilized to Provide Oxygenation, Ventilation, and Anesthetic Gas Administration without the Need for Endotracheal Intubation
Use for Respiratory Failure in the Prehospital Setting
Use in Operating Room with/without General Anesthesia
Use of General Airway Management
Use for Emergency Airway Management When Endotracheal Intubation is Unsuccessful
Use as a Conduit for Endotracheal Intubation
Use in the Hospital Setting s Part of the Emergency Airway Algorithm
Use for Emergency Airway Management When Endotracheal Intubation is Unsuccessful
Use as a Conduit for Endotracheal Intubation
Types of Supraglottic Airways
Laryngeal Mask Airway (LMA)
Other Supraglottic Devices
Combitube
Laryngeal Tube
Pharyngeal Tube
Laryngeal Mask Airway (LMA)
Rationale
Laryngeal Mask Airway Rests in the Hypopharynx (Facing the Glottis) Forming a Seal Over the Laryngeal Inlet to Allow Mask Ventilation
Laryngeal Mask Airway is Generally Less Stimulating than Endotracheal Intubation
Laryngeal Mask Airway Does Not Fully Protect Against Aspiration
Laryngeal Mask Airway Does Not Prevent Laryngospasm
Indications
Temporary Ventilation During a Surgical Procedure
During Emergency Airway Management When an Endotracheal Tube is Not Initially Desired or Cannot Be Successfully Placed by Laryngoscopy (Can J Anaesth, 2005) [MEDLINE]
Clinical Efficacy
Laryngeal Mask Airway Can Be Placed by Emergency Medical Response Personnel in the Field with Subsequent Exchange for an Endotracheal Tube During Transport or in the Emergency Department (Prehosp Emerg Care, 2007) [MEDLINE]
Laryngeal Mask Airway Placement During Out-of-Hospital Cardiac Arrest was Safer than Bag-Valve-Mask Ventilation (Am J Emerg Med, 2015) [MEDLINE]
Laryngeal Mask Airway Placed During Out-of-Hospital Cardiac Arrest Resulted in Improved 72 hr Survival, as Compared to Endotracheal Intubation (JAMA, 2018) [MEDLINE]
In the AIRWAYS-2 Trial, Laryngeal Mask Airway Placed During Out-of-Hospital Cardiac Arrest Did Not Impact the 30-Day Mortality Rate (JAMA, 2018) [MEDLINE]
Contraindications to Use of Laryngeal Mask Airway
Esophageal Varices (see Esophageal Varices): due to risk of hemorrhage or perforation
Gag Reflex (Due to Risk of Emesis/Aspiration)
Gag Reflex Can Be Removed by Using Pharmacologic Paralysis
Gastroesophageal Reflux Disease (GERD) (see Gastroesophageal Reflux Disease): since LMA’s do not offer the same degree of protection against aspiration as endotracheal intubation, they generally should not be used in patients with significant gastroesophageal reflux (except in emergency situations)
However, LMA with a Gastric Decompression Port May Be Preferred in this Population
Mild GERD is Probably Not a Contraindication to LMA Use
Obesity with BMI >35 kg/m2, Limited Access to Airway During Surgery, Surgery Expected to Last >90 min, and/or Use of Lithotomy Position During Surgery
When Used for Airway Management During Surgery, Obesity Increases the Amount of Time Required for LMA Insertion (Cochrane Database Syst Rev, 2013) [MEDLINE]: probably not clinically important (although the failure rate of LMA’s is approximately 3-5%)
When Used for Airway Management During Surgery, Obesity Increases the Risk of Gastric Insufflation
When Used for Airway Management During Surgery, Obesity Increases the Peak Inspiratory Pressure (PIP)
When Used for Airway Management During Surgery, Obesity Increases the Risk of Mask Leak, Although it Does Not Appear to Alter Ventilation (Cochrane Database Syst Rev, 2013) [MEDLINE]
When Used for Airway Management During Surgery in Obese Patients, LMA Significantly Improves Oxygenation During and After Surgery: suggests improved pulmonary performance
Oropharyngeal Trauma with Risk of Perforation
Proximal Esophageal Trauma with Risk of Perforation
Upper Airway Foreign Body (see Airway Foreign Body): since foreign body can be inadvertently moved into the trachea, resulting in tracheal obstruction
Determinants of Proper Laryngeal Mask Airway Sizing
Patient Anatomy
Laryngeal Mask Airway Size: the usual adult LMA sizes are 3/4/5/6 (most LMA’s are available in full sizes, some are available in half sizes too)
Cuff Inflation
General Sizing
Adult Female (Up to 100 kg): usually size 4
Adult Male (Up to 100 kg): usually size 5
Cuff Volume: appropriate cuff volume is usually provided by the manufacturer (note: cuff overinflation should be avoided to prevent worsening mask seal and/or injury the oropharyngeal mucosa)
Size 4 LMA: approximate cuff volume 30 mL (if larger cuff volume is required to maintain an adequate seal, a larger LMA should be placed or the patient should be endotracheally intubated)
Size 5 LMA: approximate cuff volume 40 mL (if larger cuff volume is required to maintain an adequate seal, a larger LMA should be placed or the patient should be endotracheally intubated)
Laryngeal Mask Airway Insertion
Anesthesia
Adequate Anesthesia (General Anesthesia, Intravenous Sedation) is Required Prior to LMA Inseriton to Avoid Gagging, Coughing, Laryngospasm, Breath Holding, and Straining
However, Some Patients Can Tolerate Placement with Topical Anesthesia Alone
Pharmacologic Neuromuscular Blockade Can Be Utilized to Facilitate LMA Placement: decreases the incidence of gagging, laryngospasm, and coughing
Use of Bronchoscopy for Laryngeal Mask Airway Placement
Bronchoscope Can Be Utilized to Verify Correct Placement of the LMA
Features Which Indicate Correct Laryngeal Mask Airway Placement
Ability to Ventilate without Difficulty: as determined by tidal volume, peak airway pressure <20 cm H20, and chest rise
Normal Capnography
No Leak (with Peak Airway Pressure <20 cm H2O)
Other Aspects
With Correct LMA Positioning, Cuff Inflation May Result in Outward Movement of the LMA and Slight Swelling in the Neck
Technique for LMA Fastrach Insertion
Deflate the LMA Cuff Completely and Lubricate Both Sides with Water-Soluble Lubricant
Standing at the Head of the Bed, with LMA in Dominant Hand, Place Mask on the Palate and Advance Along Palate Until Resistance is Felt
In Proper Position, the Handle Will Have a Slight Upward Angle (and Will Not Be Horizontal)
Inflate LMA Fastrach Cuff to Maintain Seal (Pressure <40 cm H2O)
Check for Proper Ventilation with Bag-Valve and Capnography
Technique for Air-Q Insertion
Similar to Placement of the LMA Classic, Except that the Air-Q Does Not Need to Ride Against the Palate During Insertion: cuff is stiff, so that it does not need to touch the pharyngeal structures during insertion
Inflate Air-Q Cuff to Maintain Seal (Pressure <40 cm H2O)
Difficulties Associated with Laryngeal Mask Airway Placement and Function
Epiglottis Entrapment (Tip of Epiglottis Flipped Over by the Laryngeal Mask)
Management
“Up-Down” Technique: withdraw LMA 2-4 cm without deflating the cuff and then reinsert
Patient Maintaining Upper Airway Tone (Which Prevents Proper Seating of the Mask in the Larynx)
Management
Increase Anesthesia/Sedation
Inadequate Laryngeal Mask Seal
Etiology
Folded Over LMA Cuff
Improper LMA Size
Since Larger Size LMA’s Generally Provide a Better Seal with Lower Cuff Inflation Volumes and Pressures, as Compared to Smaller Size LMA’s, Replacing with a Larger LMA May Remedy the Problem
Inadequate Air in the LMA Cuff
High Peak Airway Pressure
Management
Add Air to Cuff (If Necessary)
Replace with Same or Larger LMA
Transition to Endotracheal Intubation: if unable to maintain adequate seal
Poor Patient Anatomy Contributing to Difficult LMA Placement
Management
Rotational Placement of LMA (with Partially-Inflated Cuff) May Facilitate Placement in Difficult Cases
Placement with the Aid of Ultrasound or Bronchoscopy
Intubating Via the Laryngeal Mask Airway
General Comments
While Intubation Through an Intubating Laryngeal Mask Airway Can Be Achieved Blindly, May Providers Utilize a Bronchoscope to Intubate by this Technique
Endotracheal Tube is Loaded Onto the Bronchoscope and the Bronchoscope/Tube are Passed Through the LMA Channel
Technique for Intubation Via Laryngeal Mask Airway Fastrach
General Comments
LMA Fastrach Contains a Bar Which Elevates the Epiglottis as the Endotracheal Tube Passes Through the Aperture
LMA Fastrach Has a Ramp in the Intubating Channel Which Directs the Endotracheal Tube Anteriorly and Centrally to Facilitate Movement into the Trachea (and Minimize Damage to Glottis)
LMA Fastrach May Use Either a Standard Endotracheal Tube or a Proprietary Non-Kinking Endotracheal Tube
If Standard Endotracheal Tube is Used, Warm it Beforehand (to Increase Flexibility) and Insert it onto a Bronchoscope, then Insert the Bronchoscope/Endotracheal Tube Asssembly into the LMA with the Curvature Reversed (To Facilitate the Tip Exiting the LMA at a Shallow Angle and Entering the Trachea)
At 15 cm Depth, an Endotracheal Tube Emerges from the LMA and Lifts the Epiglottis Elevating Bar
Proprietary Endotracheal Tube
Vertical Black Line Should Face the Operator (This Aligns the Bevel with the Vocal Cords)
Horizontal Black Line Marks the 15 cm Insertion Depth (at Which the Tube Exits the LMA)
Perform a “Skillet Lift” Using the LMA Fastrach Handle to Align the Cuff with the Glottic Opening
Gently Advance the Endotracheal Tube: if resistance is encountered, glottic alignment is not correct
When Endotracheal Placement is Confirmed, Deflate the LMA Fastrach Cuff to Relieve the Mucosal Pressure
After Intubation, Carefully Remove the LMA Fastrach
LMA Fastrach May Remain in Place for Several Hours Prior to Removal
Technique for Intubation Via the Air-Q
General Comments
Large Adult Size Air-Q Can Accomodate a 8.5 Endotracheal Tube
Air-Q Has a Mild Curvature and is Designed to Utilize a Standard Endotracheal Tube: it does not require a specialized non-kinking endotracheal tube
Lubricate the Endotracheal Tube with Water-Soluble Lubricant
Remove the 15 mm Bag Connector and Insert the Endotracheal Tube into the Lumen
Move Endotracheal Tube Up and Down in the Lumen to Lubricate the Channel
Advance the Endotracheal Tube into the Trachea
May Need to Gently Insert/Withdraw the Air-Q to Facilitate Endotracheal Tube Passage
Inflate the Endotracheal Tube Cuff
When Endotracheal Placement is Confirmed, Deflate the Air-Q Cuff to Relieve the Mucosal Pressure
After Confirmation of Endotracheal Tube Placement, Remove the Air-Q Using the Removal Stylet: this decreases the risk of damage to the pilot balloon
Air-Q May Remain in Place for Several Hours Prior to Removal
Ventilation Technique
Spontaneous Ventilation
Advantages
Better Tolerance of LMA Malpositioning
Decreases Air Leak Around the LMA
Limits the Development of Gastric Insufflation
Positive-Pressure Ventilation
Pressure-Limited Ventilation (Pressure Support, Pressure Control) is Used More Commonly than Volume-Limited Ventilation, Since the LMA Does Not Seal the Pharynx and There is Leak Around the Device (with Resulting Gastric Insufflation and/or Inadequate Ventilation)
LMA’s are Generally Designed for Use with Peak Airway Pressure <20 cm H2O: higher peak airway pressure may result in LMA leak and/or gastric insufflation
LMA ProSeal was Designed for Use with Somewhat Higher Peak Airway Pressures (<25 cm H2O): cuff has a posterior extension which provides a “double seal”
Advantages
Allows Control of Respiratory Rate and Tidal Volume
Ventilation is Assured During Deeper Levels of Sedation
Adverse Effects/Complications
General Comments
Laryngeal Mask Airway-Associated Complications are Low: occur in approximately 0.15% of cases (Anesth Analg, 1996) [MEDLINE]
High Laryngeal Mask Airway Cuff Pressure May Increase the Risk of Airway Complications (Anesthesiology, 2010) [MEDLINE] (Can J Anaesth, 2013) [MEDLINE]
Laryngeal Mask Airway May Function to Some Extent to Seal Off the Trachea from Aspiration of Regurgitated Gastric Contents
However, Vomiting or Increase in Intragastric Pressure Can Overcome this Protection, Resulting in Aspiration (Br J Anaesth, 2002) [MEDLINE]
Laryngeal Mask Airway Decreases Lower Esophageal Sphincter Tone Via a Reflex Mechanism (Br J Anaesth, 1992) [MEDLINE]: this is similar to the reflex which occurs while swallowing a bolus of food
This Results in Increased Acid Reflux into the Esophagus During Lithotomy and Trendelenburg Positioning (Can J Anaesth, 1999) [MEDLINE]
Prevention
Patient Selection
Assess Risk Factors for Aspiration
Assess Lung/Chest Wall Compliance for Factors that Might Increase Peak Airway Pressure
Procedure Selection (Accounting for Expected Patient Positioning Which Might Contribute to Aspiration)
Maintenance of Adequate Depth of Anesthesia During Laryngeal Mask Airway Insertion and During Surgery
Minimization of Peak Airway Pressure During Mechanical Ventilation to Avoid Gastric Insufflation
Ensure Adequate Reversal of Neuromuscular Blockade Prior to Emergence from General Anesthesia
Use of Laryngeal Mask Airway with Gastric Decompression Port (Anaesthesia, 2011) [MEDLINE]
Incision of the Cricothyroid Membrane with Insertion of a Tube to Establish an Artificial Airway
History
Cricothyroidotomy (Initially Referred to as “High Tracheostomy”) was First Performed by Dr. Chevalier Jackson in 1909: cases were often performed due to upper airway obstruction related to diphtheria
Due to Complications of Tracheal Stenosis, He Later Criticize the Use of Cricothyroidotomy
Epidemiology
The Historical Rate of Cricothyroidotomies Has Been Demonstrated to Decrease Over Time, Attributable to Several Factors (Acad Emerg Med, 1998) [MEDLINE]
Adoption of Rapid Sequence Intubation (RSI)
Decreased Concern Related to the Perfomance of Endotracheal Intubation in Trauma Patients Without Initial Evaluation to Rule Out Cervical Spinal Cord Injury
Establishment of Emergency Medicine Residencies with the Presence of 24 hr Supervising Emergency Medicine Faculty
Rates of Cricothyroidotomy Might Be Expected to Continue to Decline with the Increased Use of Video Laryngoscopy and the Advancement of Other Airway Management Techniques
In a Single-Center Retrospective Study, Cricothyroidotomy Comprised 1% of All Emergency Department Intubations (and 10.9% of All Prehospital Intubations) (J Emerg Med. 2003) [MEDLINE]
Indications
General Indications for Cricothyroidotomy
Inability to Intubate Patient
Contraindication to Intubation
Upper Airway Obstruction: note that cricothyroidotomy will only be effective if the airway obstruction is proximal to the site of the cricothyroidotomy
Specific Etiologies Requiring Cricothyroidotomy (Acad Emerg Med, 1998) [MEDLINE]
Facial Fracture: 32% of cases
Emesis in the Airway: 32% of cases
Failure of Intubation (in the Absence of Clinical Issues): 11% of cases
Traumatic Upper Airway Obstruction: 7% of cases
Relative Contraindications
Childhood (<5-12 y/o): since the childhood airway is funnel-shaped with the narrowest aspect at the cricoid ring rather than at the vocal cords (with an increased risk of developing subglottic stenosis) and procedure can damage the relatively soft cricoid cartilage in children
Remote Radiation Therapy (or Other Deformity/Scarring) Which May Alter the Upper Airway Anatomy
Tumor
Intrinsic Airway Tumor
Technique
Cricothyroid Membrane Lies Below the Thyroid Cartilage and Above the Cricoid Cartilage
Laterally on Both Sides of the Cricothyroid Membrane are the Cricothyroideus Muscles
Location of the Cricothyroid Membrane by Palpation Can Be Difficult Even for Experienced Providers with Surgical Airway Experience (Success Rates ≤50%) (Can J Anaesth, 2016) [MEDLINE]
This is Especially True in Obese Patients (Anaesthesia, 2015) [MEDLINE]
Location of the Cricothyroid Membrane by Ultrasound
May Be Useful, But Studies are Lacking
Cook Melker Kit Procedure
Components: 6 mL syringe, 18 gauge needle with overlying catheter, a guide wire, a tissue dilator, cuffed cricothyroidotomy tube, and tracheostomy tape
Time Required: 1-4 min (Anaesthesist, 2003) [MEDLINE]
Steps
Stand at the Patient’s Right Side
Immobilize the Larynx by Holding the Thyroid Cartilage with the Left Hand
With Right Hand, Insert Needle (Pointed at a Downward 45 Degree Angle) into the Cricothyroid Membrane with Syringe Filled with Saline, Aspirating as You Go: watch for air bubbles into the syringe, indicating that you are in the trachea
Remove Syringe and Pass Wire Through the Needle
Remove Needle
Make a 1-2 cm Horizontal Incision Through the Skin and Cricothyroid Membrane: take care to not incise too deep (which may injury the posterior tracheal wall) or with the blade oriented superiorly (which may injure the vocal cords)
Thread the Dilator/Tube Assembly Over the Wire into the Airway
Remove the Dilator and Wire
Secure Airway Tube with Tracheostomy Tape and Attach to Either Bag Ventilation or Mechanical Ventilator
Complications
Early Adverse Effects/Complications
Bleeding: usually occurs and can be controlled with direct pressure/packing
Cricoid Cartilage Fracture
Infection
Passage of Tube into Extratracheal Location
Posterior Tracheal Wall Perforation
Thyroid Cartilage Fracture
Tracheal Ring Fracture
Unintentional Tracheostomy
Late Adverse Effects/Complications
Subglottic Stenosis
Voice Changes
Adverse Effects and Complications of Airway Management, Endotracheal Intubation, and Invasive Mechanical Ventilation
Patient Awareness of Paralysis During Endotracheal Intubation
Study of Awareness of Paralysis in Emergency Department Patients Undergoing Endotracheal Intubation (Chest, 2023) [MEDLINE]: n = 886
Approximately 7.4% of Patients Recalled Awareness of Paralysis During Endotracheal Intubation (95% CI: 5.8-9.4)
Logistic Regression Model Demonstrated that Decreased Level of Consciousness Prior to Intubation was Associated with Lower Odds of Awareness (Adjusted Odds Ratio 0.39; 95% CI: 0.22-0.69)
The Class of Neuromuscular Blocking Agent Used, Sedative Used, Preintubation Shock Index, and Postintubation Sedation were Not Significantly Associated with Recall of Paralysis During Endotracheal Intubation
Impact on Medical Malpractice Claims
Significant Morbidity/Mortality (as Well as Medical Malpractice) is Related to Adverse Events/Complications of Airway Management and Endotracheal Intubation
Inadequate Ventilation, Esophageal Intubation, and Difficult Endotracheal Intubation are the Most Common Mechanisms of Respiratory Adverse Events/Complications Associated with Endotracheal Intubation/Mechanical Ventilation by Anesthesiologists (Anesthesiology, 1991) [MEDLINE]
US Review of Airway Complications in Patients Undergoing General Anesthesia (Anesthesiology, 2009) [MEDLINE]: mortality rate of 1.1 per million
British National Health Service Review of Major Airway Complications in Patients Undergoing General Anesthesia (Br J Anaesth. 2011) [MEDLINE]: 46 events per million (associated mortality of 5.6 per million)
British National Health Service Review of Major Airway Complications Noted that 25% of Reported Airway Events Occurred in the Intensive Care Unit or Emergency Department (and 61% of Those Events Resulted in Permanent Patient Harm or Death) (Br J Anaesth, 2011) [MEDLINE]
Closed Claims Analysis of Difficult Endotracheal Intubation by Anesthesiologists (Comparison of 2000-2012 to 1993-1999 Time Periods) (Anesthesiology, 2019) [MEDLINE]
Patients in 2000-2012 Difficult Intubation Claims were Sicker (78% American Society of Anesthesiologists, ASA, Physical Status III-V) and Had More Emergency Procedures (37%) as Compared to Patients in 1993-1999 Claims (47% ASA Physical Status III-V; P < 0.001 and 22% Emergency; P = 0.025)
More Difficult Endotracheal Intubation Events Occurred in Nonperioperative Locations in 2000-2012 than 1993-1999 (23% vs 10%; P = 0.035)
Outcomes Differed Between Time Periods (P < 0.001), with a Higher Proportion of Death in 2000-2012 claims (73% vs 42% in 1993-1999 Claims; P < 0.001 Adjusted for Multiple Testing)
In 2000-2012 Claims, Preoperative Predictors of Difficult Endotracheal Intubation were Present in 76% of Cases
In the 97 Claims with Sufficient Information for Assessment, Inappropriate Airway Management Occurred in 73% of Cases (κ = 0.44-0.66)
A “Can’t Intubate, Can’t Oxygenate” Emergency Occurred in 80 Claims with Delayed Surgical Airway in 39% of Cases
Multiple Intubation Attempts
Multiple Intubation Attempts is a Risk Factor for Adverse Events/Complications of Airway Management and Endotracheal Intubation
In Emergency Endotracheal Intubations Performed in Critically Ill Patients Suffering Deterioration, As Compared to ≤2 Attempts, Repeated Attempts (≥3) were Significantly Associated with Increased Incidence of Hypoxemia (11.8% vs 70%), Regurgitation of Gastric Contents (1.9% vs 22%), Aspiration of Gastric Contents (0.8% vs 13%), Bradycardia (1.6% vs 21%), and Cardiac Arrest (0.7% vs 11%; P<0.001) (Anesth Analg, 2004) [MEDLINE]
In Emergency Department Intubations, ≥3 Intubation Attempts were Associated with a Significantly Increased Rate of Adverse Events (35% vs 9%) (Ann Emerg Med, 2012) [MEDLINE]
Patients Requiring 1 Intubation Attempts Had a 14.2% Adverse Event Rate, Patients Requiring 2 Intubation Attempts Had a 47.2% Adverse Event Rate, and Patients Requiring 3 Intubation Attempts in the Emergency Department Had a 63.6% Adverse Event Rate (Acad Emerg Med, 2013) [MEDLINE]
Japanese Study of Intubation Outcomes in Intubations Performed by Residents in the Emergency Department (Using Data from the Japanese Emergency Airway Network Prospective Cohort Study) (JAMA Netw Open, 2022)[MEDLINE]: n = 11,297 (from 15 institutions, during period of 2012-2019)
Overall, 4,480 Patients (40%) Underwent Intubation by Transitional Year Residents (PGY1-PGY2) and 3,588 (31%) Underwent Intubation by Physicians (PGY3-PGY5)
Overall First Pass Success Rate was 71%
Intubations Performed by a less experienced physician had a significantly lower first-pass Success Rate with an Adjusted Risk Difference of −23% (95% CI, −30% to −16%) for PGY1 Residents, as Compared to ≥PGY6 Physicians
These Associations Remained in Logistic Regression Models (Adjusted Odds Ratio 0.30; 95% CI, 0.22 to 0.41) for PGY1 Residents vs ≥PGY6 Physicians
Overall, 1,802 Patients (16%) Had Intubation-Related Adverse Events
A Lower Number of PGY Years was Also Associated with a Higher Rate of Any Adverse Events (Adjusted Risk Difference 7%; 95% CI: 3% to 11%, for PGY1 Residents vs ≥PGY6 Physicians)
Intubation Bundles
Intubation Bundles Can Decrease the Incidence of Post-Intubation Adverse Effects/Complications in the Intensive Care Unit (Intensive Care Med, 2010) [MEDLINE]: n = 244
Bundle Components
Capnography
Cricoid Pressure
Intravenous Fluid Loading
Preoxygenation with Noninvasive Positive-Pressure Ventilation
Preparation and Early Administration of Sedation
Presence of Two Operators
Protective Ventilation
Rapid Sequence Induction
Vasopressor Use (If Required)
Specific Adverse Effects and Complications of Endotracheal Intubation and Invasive Mechanical Ventilation
Accidental intubation of the oesophagus. Anaesth Intensive Care. 1980;8(2):183 [MEDLINE]
End-tidal CO2 as a guide to successful cardiopulmonary resuscitation: a preliminary report. Crit Care Med. 1985;13(11):910 [MEDLINE]
Esophageal intubation: a review of detection techniques. Anesth Analg. 1986;65(8):886 [MEDLINE]
Unrecognized endobronchial intubation of emergency patients. Ann Emerg Med. 1989;18(8):853 [MEDLINE]
A comparative study of methods of detection of esophageal intubation. Anesth Analg. 1989;69(5):627 [MEDLINE]
Multicenter study of a portable, hand-size, colorimetric end-tidal carbon dioxide detection device. Ann Emerg Med. 1992 May;21(5):518-23 [MEDLINE]
Women are at greater risk than men for malpositioning of the endotracheal tube after emergent intubation. Crit Care Med. 1994;22(7):1127 [MEDLINE]
Proper depth placement of oral endotracheal tubes in adults prior to radiographic confirmation. Acad Emerg Med. 1995;2(1):20 [MEDLINE]
Use of tube condensation as an indicator of endotracheal tube placement. Ann Emerg Med. 1998;31(5):575 [MEDLINE]
Comparison of three different methods to confirm tracheal tube placement in emergency intubation. Intensive Care Med. 2002;28(6):701 [MEDLINE]
Towards evidence based emergency medicine: best BETs from the Manchester Royal Infirmary. Colourimetric CO(2) detector compared with capnography for confirming ET tube placement. Emerg Med J. 2003 May;20(3):265-6 [MEDLINE]
The assessment of three methods to verify tracheal tube placement in the emergency setting. Resuscitation 2003; 56:153-157 [MEDLINE]
An assessment of a tracheal tube introducer as an endotracheal tube placement confirmation device. Am J Emerg Med. 2005;23(6):754 [MEDLINE]
Caution when using colorimetry to confirm endotracheal intubation. Anesth Analg 2007;104:738 [MEDLINE]
Endobronchial intubation detected by insertion depth of endotracheal tube, bilateral auscultation, or observation of chest movements: randomised trial. BMJ. 2010;341:c5943 [MEDLINE]
Ultrasonography in the management of the airway. Acta Anaesthesiol Scand. 2011 Nov;55(10):1155-73. Epub 2011 Sep 7 [MEDLINE]
Tracheal rapid ultrasound exam (T.R.U.E.) for confirming endotracheal tube placement during emergency intubation. Resuscitation. 2011 Oct;82(10):1279-84. Epub 2011 Jun 1 [MEDLINE]
Transtracheal ultrasound for verification of endotracheal tube placement: a systematic review and meta-analysis. Can J Anaesth. 2015 Apr;62(4):413-23. Epub 2014 Dec 24 [MEDLINE]
Ultrasonography for confirmation of endotracheal tube placement: a systematic review and meta-analysis. Resuscitation. 2015;90:97 [MEDLINE]
Auscultation versus Point-of-care Ultrasound to Determine Endotracheal versus Bronchial Intubation: A Diagnostic Accuracy Study. Anesthesiology. 2016 May;124(5):1012-20 [MEDLINE]
Endotracheal Tube Movement with Change in Head Position
Alteration of endotracheal tube position. Flexion and extension of the neck. Crit Care Med. 1976 Jan-Feb;4(1):8-12 [MEDLINE]
Laryngeal Mask Airway (LMA)
Effect of the laryngeal mask airway on lower oesophageal sphincter pressure in patients during general anaesthesia. Br J Anaesth. 1992 Oct;69(4):346-8 [MEDLINE]
Clinical significance of pulmonary aspiration during the perioperative period. Anesthesiology. 1993;78(1):56 [MEDLINE]
The incidence of aspiration associated with the laryngeal mask airway: a meta-analysis of published literature. J Clin Anesth. 1995;7(4):297 [MEDLINE]
Gastric regurgitation during general anaesthesia in different positions with the laryngeal mask airway. Anaesthesia. 1995 Dec;50(12):1053-5 [MEDLINE]
Survey of laryngeal mask airway usage in 11,910 patients: safety and efficacy for conventional and nonconventional usage. Anesth Analg. 1996 Jan;82(1):129-33 [MEDLINE]
Gastroesophageal reflux during spontaneous respiration with the laryngeal mask airway. Can J Anaesth. 1999 Mar;46(3):268-70 [MEDLINE]
ProSeal laryngeal mask protects against aspiration of fluid in the pharynx. Br J Anaesth. 2002 Apr;88(4):584-7 [MEDLINE]
Aspiration and the laryngeal mask airway: three cases and a review of the literature. Br J Anaesth. 2004 Oct;93(4):579-82 [MEDLINE]
The Proseal LMA is a useful rescue device during failed rapid sequence intubation: two additional cases. Can J Anaesth. 2005 Jun;52(6):630-3 [MEDLINE]
Use of manometry for laryngeal mask airway reduces postoperative pharyngolaryngeal adverse events: a prospective, randomized trial. Anesthesiology. 2010 Mar;112(3):652-7 [MEDLINE]
Major complications of airway management in the UK: results of the Fourth National Audit Project of the Royal College of Anaesthetists and the Difficult Airway Society. Part 1: anaesthesia. Br J Anaesth. 2011 May;106(5):617-31 [MEDLINE]
Major complications of airway management in the UK: results of the Fourth National Audit Project of the Royal College of Anaesthetists and the Difficult Airway Society. Part 2: intensive care and emergency departments. Br J Anaesth. 2011;106(5):632 [MEDLINE]
Can we make airway management (even) safer?–lessons from national audit. Anaesthesia. 2011;66 Suppl 2:27 [MEDLINE]
New supraglottic airway with built-in pressure indicator decreases postoperative pharyngolaryngeal symptoms: a randomized controlled trial. Can J Anaesth. 2013 Dec;60(12):1197-203 [MEDLINE]
Feasibility of a laryngeal tube for airway management during cardiac arrest by first responders. Resuscitation. 2013;84(4):446 [MEDLINE]
Supraglottic airway devices versus tracheal intubation for airway management during general anaesthesia in obese patients. Cochrane Database Syst Rev. 2013 [MEDLINE]
Airway management by physician-staffed Helicopter Emergency Medical Services – a prospective, multicentre, observational study of 2,327 patients. Scand J Trauma Resusc Emerg Med. 2015;23:57 [MEDLINE]
Safety and feasibility of the laryngeal tube when used by EMTs during out-of-hospital cardiac arrest. Am J Emerg Med. 2015;33(8):1050 [MEDLINE]
Effect of a Strategy of Initial Laryngeal Tube Insertion vs Endotracheal Intubation on 72-Hour Survival in Adults With Out-of-Hospital Cardiac Arrest: A Randomized Clinical Trial. JAMA. 2018;320(8):769 [MEDLINE]
Effect of a Strategy of a Supraglottic Airway Device vs Tracheal Intubation During Out-of-Hospital Cardiac Arrest on Functional Outcome: The AIRWAYS-2 Randomized Clinical Trial. JAMA. 2018;320(8):779 [MEDLINE]
Cricothyrotomy in the emergency department. Ann Emerg Med. 1982;11(7):361 [MEDLINE]
Cricothyrotomy in the emergency department revisited. J Emerg Med. 1989;7(2):115 [MEDLINE]
Prehospital cricothyrotomy: an investigation of indications, technique, complications, and patient outcome. Ann Emerg Med. 1990;19(3):279 [MEDLINE]
Declining rate of cricothyrotomy in trauma patients with an emergency medicine residency: implications for skills training. Acad Emerg Med. 1998;5(3):247 [MEDLINE]
Comparison of 2 cricothyrotomy techniques: standard method versus rapid 4-step technique. Ann Emerg Med. 1998;32(4):442 [MEDLINE]
Outcomes of emergency surgical airway procedures in a hospital-wide setting. Laryngoscope. 1999;109(11):1766 [MEDLINE]
Comparison of wire-guided cricothyrotomy versus standard surgical cricothyrotomy technique. J Emerg Med. 1999;17(6):957 [MEDLINE]
Cricothyroidotomy: when, why, and why not? Am J Otolaryngol. 2000;21(3):195 [MEDLINE]
Cricothyrotomy: a 5-year experience at one institution. J Emerg Med. 2003;24(2):151 [MEDLINE]
[Emergency cricothyrotomy–puncture or anatomical preparation? Peculiarities of two methods for emergency airway access demonstrated in a cadaver model]. Anaesthesist. 2003;52(4):304 [MEDLINE]
Needle vs surgical cricothyroidotomy: a short cut to effective ventilation. Anaesthesia. 2006;61(10):962[MEDLINE]
A comparison of two emergency cricothyroidotomy kits in human cadavers. Anesth Analg. 2008;106(1):182 [MEDLINE]
Accuracy of surface landmark identification for cannula cricothyroidotomy. Anaesthesia. 2010;65(9):889 [MEDLINE]
Accuracy of identification of the cricothyroid membrane in female subjects using palpation: an observational study. Anesth Analg. 2012 May;114(5):987-92 [MEDLINE]
Accuracy of conventional digital palpation and ultrasound of the cricothyroid membrane in obese women in labour. Anaesthesia. 2015 Nov;70(11):1230-4 [MEDLINE]
Comparing success rates of anesthesia providers versus trauma surgeons in their use of palpation to identify the cricothyroid membrane in female subjects: a prospective observational study. Can J Anaesth. 2016 Jul;63(7):807-817 [MEDLINE]
Adverse Effects/Complications
Ulcerative tracheo-oesophageal fistula during treatment by tracheostomy and intermittent positive pressure ventilation. Thorax. 1972;27(3):338 [MEDLINE]
Tracheal injury following prolonged intubation. Aust N Z J Surg. 1976 Feb;46(1):18-25 [MEDLINE]
Intubation lesions of the larynx. Br J Anaesth. 1978;50(6):587 [MEDLINE]
Postoperative sore throat: influence of tracheal tube lubrication versus cuff design. Can Anaesth Soc J. 1980;27(2):156 [MEDLINE]
Laryngeal injuries secondary to nasogastric tubes. Ann Otol Rhinol Laryngol. 1981;90(5 Pt 1):469 [MEDLINE]
The influence of endotracheal tube cuff design and cuff lubrication on postoperative sore throat. Anesthesiology. 1983;58(4):376 [MEDLINE]
Laryngotracheal injury due to endotracheal intubation: incidence, evolution, and predisposing factors. A prospective long-term study. Crit Care Med. 1983;11(5):362 [MEDLINE]
True vocal cord paralysis following intubation. Laryngoscope. 1985;95(11):1352 [MEDLINE]
Correlation of endotracheal tube size with sore throat and hoarseness following general anesthesia. Anesthesiology. 1987 Sep;67(3):419-21 [MEDLINE]
Laryngeal complications of prolonged intubation. Chest. 1989;96(4):877 [MEDLINE]
Anesthesia-induced dental injury. Int Anesthesiol Clin. 1989;27(2):120 [MEDLINE]
Unsuspected cervical fractures: a common problem in ankylosing spondylitis. Anesthesiology. 1989;70(5):869 [MEDLINE]
Tracheoesophageal fistula formation in intubated patients. Risk factors and treatment with high-frequency jet ventilation. Chest. 1990;98(1):161 [MEDLINE]
Swallowing disorders in patients with prolonged orotracheal intubation or tracheostomy tubes. Crit Care Med. 1990;18(12):1328 [MEDLINE]
Adverse respiratory events infrequently leading to malpractice suits. A closed claims analysis. Anesthesiology. 1991;75(6):932 [MEDLINE]
Surgical considerations in tracheal stenosis. Laryngoscope. 1992 Mar;102(3):237-43 [MEDLINE]
Resolution of laryngeal injury following translaryngeal intubation. Am Rev Respir Dis. 1992;145(2 Pt 1):361 [MEDLINE]
Evaluation of risk factors for laryngeal edema after tracheal extubation in adults and its prevention by dexamethasone. A placebo-controlled, double-blind, multicenter study. Anesthesiology. 1992;77(2):245 [MEDLINE]
Massive airway leaks: an analysis of the role of endotracheal tubes. Crit Care Med. 1993;21(4):518 [MEDLINE]
Mediastinitis and sepsis syndrome following intubation. Anaesthesia. 1994;49(10):883 [MEDLINE]
Risk factors associated with prolonged intubation and laryngeal injury. Otolaryngol Head Neck Surg. 1994;111(4):453 [MEDLINE]
[A survey of perioperative bronchospasm in 105 patients with reactive airway disease]. Masui. 1995;44(3):396 [MEDLINE]
Management of acquired tracheoesophageal fistula. Chest Surg Clin N Am. 1996 Nov;6(4):819-36 [MEDLINE]
Gastroesophageal reflux in patients with subglottic stenosis. Arch Otolaryngol Head Neck Surg. 1998 May;124(5):551-5 [MEDLINE]
Airway injury during anesthesia: a closed claims analysis. Anesthesiology. 1999;91(6):170 [MEDLINE]
Postextubation fiberoptic endoscopic evaluation of swallowing after prolonged endotracheal intubation: a randomized, prospective trial. Crit Care Med. 2001;29(9):1710 [MEDLINE]
Association of airway abnormalities and risk factors in 37 subglottic stenosis patients. Otolaryngol Head Neck Surg. 2006 Sep;135(3):434-7 [MEDLINE]
Review of tracheo-esophageal fistula associated with endotracheal intubation. J Surg Educ. 2007 Jul-Aug;64(4):237-40 [MEDLINE]
Risk factors for adult laryngotracheal stenosis: a review of 74 cases. Ann Otol Rhinol Laryngol. 2007 Mar;116(3):206-10 [MEDLINE]
Short-term effects of endotracheal intubation on voice. J Voice. 2007 Nov;21(6):762-8 [MEDLINE]
Age and comorbidity as risk factors for vocal cord paralysis associated with tracheal intubation. Br J Anaesth. 2007 Apr;98(4):524-30 [MEDLINE]
Effect of positive expiratory pressure and type of tracheal cuff on the incidence of aspiration in mechanically ventilated patients in an intensive care unit. Crit Care Med. 2008;36(2):409 [MEDLINE]
CDC/NHSN surveillance definition of health care-associated infection and criteria for specific types of infections in the acute care setting. Am J Infect Control. 2008;36(5):309 [MEDLINE]
Spiral CT virtual bronchoscopy with multiplanar reformatting in the evaluation of post-intubation tracheal stenosis: comparison between endoscopic, radiological and surgical findings. Eur Arch Otorhinolaryngol. 2009;266(6):863 [MEDLINE]
Epidemiology of anesthesia-related mortality in the United States, 1999-2005. Anesthesiology. 2009 Apr;110(4):759-65 [MEDLINE]
Incidence and impact of dysphagia in patients receiving prolonged endotracheal intubation after cardiac surgery. Can J Surg. 2009;52(2):119 [MEDLINE]
An intervention to decrease complications related to endotracheal intubation in the intensive care unit: a prospective, multiple-center study. Intensive Care Med. 2010;36(2):248 [MEDLINE]
The incidence of dysphagia following endotracheal intubation: a systematic review. Chest. 2010;137(3):665 [MEDLINE]
Postoperative patient complaints: a prospective interview study of 12,276 patients. J Clin Anesth. 2010;22(1):13 [MEDLINE]
Cost analysis of intubation-related tracheal injury using a national database. Otolaryngol Head Neck Surg. 2010 Jul;143(1):31-6. doi: 10.1016/j.otohns.2009.11.004 [MEDLINE]
Endotracheal tube size and sore throat following surgery: a randomized-controlled study. Acta Anaesthesiol Scand. 2010 Feb;54(2):147-53 [MEDLINE]
Post-intubation laryngeal injuries and extubation failure: a fiberoptic endoscopic study. Intensive Care Med. 2010 Jun;36(6):991-8. Epub 2010 Mar 18 [MEDLINE]
Postextubation obstructive pseudomembranes: a case series and review of a rare complication after endotracheal intubation. Lung. 2011 Feb;189(1):81-6. Epub 2010 Nov 17 [MEDLINE]
Laryngeal injury from prolonged intubation: a prospective analysis of contributing factors. Laryngoscope. 2011;121(3):596 [MEDLINE]
Major complications of airway management in the UK: results of the Fourth National Audit Project of the Royal College of Anaesthetists and the Difficult Airway Society. Part 1: anaesthesia. Br J Anaesth. 2011 May;106(5):617-31. doi: 10.1093/bja/aer058 [MEDLINE]
Major complications of airway management in the UK: results of the Fourth National Audit Project of the Royal College of Anaesthetists and the Difficult Airway Society. Part 2: intensive care and emergency departments. Br J Anaesth. 2011 May;106(5):632-42. doi: 10.1093/bja/aer059 [MEDLINE]
Association between repeated intubation attempts and adverse events in emergency departments: an analysis of a multicenter prospective observational study. Ann Emerg Med. 2012 Dec;60(6):749-754.e2 [MEDLINE]
Incidence of and risk factors for severe cardiovascular collapse after endotracheal intubation in the ICU: a multicenter observational study. Crit Care. 2015 Jun 18;19:257. doi: 10.1186/s13054-015-0975-9 [MEDLINE]
Postintubation hypotension in intensive care unit patients: A multicenter cohort study J Crit Care. 2015 Oct;30(5):1055-60. doi: 10.1016/j.jcrc.2015.06.007 [MEDLINE]
Push-dose pressors for immediate blood pressure control. Clin Exp Emerg Med. 2015 Jun 30;2(2):131-132. eCollection 2015 Jun [MEDLINE]
Surgical Management of Benign Acquired Tracheoesophageal Fistulas: A Ten-Year Experience. Ann Thorac Surg. 2016;102(4):1081 [MEDLINE]
Incidence and risk factors of postoperative sore throat after endotracheal intubation in Korean patients. J Int Med Res. 2017;45(2):744 [MEDLINE]
Effect of Endotracheal Tube Cuff Shape on Postoperative Sore Throat After Endotracheal Intubation. Anesth Analg. 2017;125(4):1240 [MEDLINE]
The Effect of Zinc Lozenge on Postoperative Sore Throat: A Prospective Randomized, Double-Blinded, Placebo-Controlled Study. Anesth Analg. 2018;126(1):78 [MEDLINE]
Cardiac Arrest and Mortality Related to Intubation Procedure in Critically Ill Adult Patients: A Multicenter Cohort Study. Crit Care Med. 2018 Apr;46(4):532-539. doi: 10.1097/CCM.0000000000002925 [MEDLINE]
Management of Difficult Tracheal Intubation: A Closed Claims Analysis. Anesthesiology. 2019 Oct;131(4):818-829. doi: 10.1097/ALN.0000000000002815 [MEDLINE]
INTUBE Study. Intubation practices and adverse peri-intubation events in critically ill patients from 29 countries. JAMA 2021; 325:1164–1172 [MEDLINE]
Association of Number of Physician Postgraduate Years With Patient Intubation Outcomes in the Emergency Department. JAMA Netw Open. 2022 Apr 1;5(4):e226622. doi: 10.1001/jamanetworkopen.2022.6622 [MEDLINE]
Recall of Awareness During Paralysis Among ED Patients Undergoing Tracheal Intubation. Chest. 2023 Feb;163(2):313-323. doi: 10.1016/j.chest.2022.08.2232 [MEDLINE]