Rapid Sequence Intubation Utilizes a Period of Preoxygenation, Followed by the Nearly Simultaneous Administration of a Sedative Induction Agent and a Paralytic Agent to Facilitate Rapid and Effective Endotracheal Intubation (with a Minimal Risk of Aspiration)
Rapid Sequence Intubation is the Most Common Emergency Intubation Technique in a Patient Who is Not Anticipated to Have a Difficult Airway (Ann Emerg Med, 2015) [MEDLINE]
Approximately 85% of First Endotracheal Intubation Attempts in Emergency Departments are Performed Using Rapid Sequence Intubation (Ann Emerg Med, 2015) [MEDLINE]
Rapid Sequence Intubation Decreases Procedure-Related Complications and Increases the Probability of First-Pass Endotracheal Intubation Success (Crit Care Med, 2012) [MEDLINE] (Ann Am Thorac Soc, 2015) [MEDLINE] (Int J Emerg Med, 2017) [MEDLINE]
Rapid Sequence Intubation Has High First-Pass Endotracheal Intubation Success Rates with Video Laryngoscopy (90%) in Patients with Anticipated Difficult Airways (J Emerg Med, 2017) [MEDLINE]:
Only 11% of Non-Cardiac Arrest Patients Had a Predicted Difficult Airway in this Study and None Required a Surgical Airway (J Emerg Med, 2017) [MEDLINE]
Relative Contraindications to Rapid Sequence Intubation
Anticipated Difficult Intubation (Especially if Rescue is Anticipated to Be Difficult or Impossible)
Inability to Tolerate the Apneic Period During Rapid Sequence Intubation (Due to Severe Hypoxemia, Acidosis, etc)
Seven P’s of Rapid Sequence Intubation
Preparation: 10 min before intubation
Preoxygenation: 5 min before intubation
Pre-Intubation Optimization: 3 min before intubation
Paralysis with Induction: induction
Protection: 30 sec after induction
Placement (Intubation): 45 sec after induction
Post-Intubation Management: 60 sec after induction
Physiologic Basis of Rapid Sequence Intubation
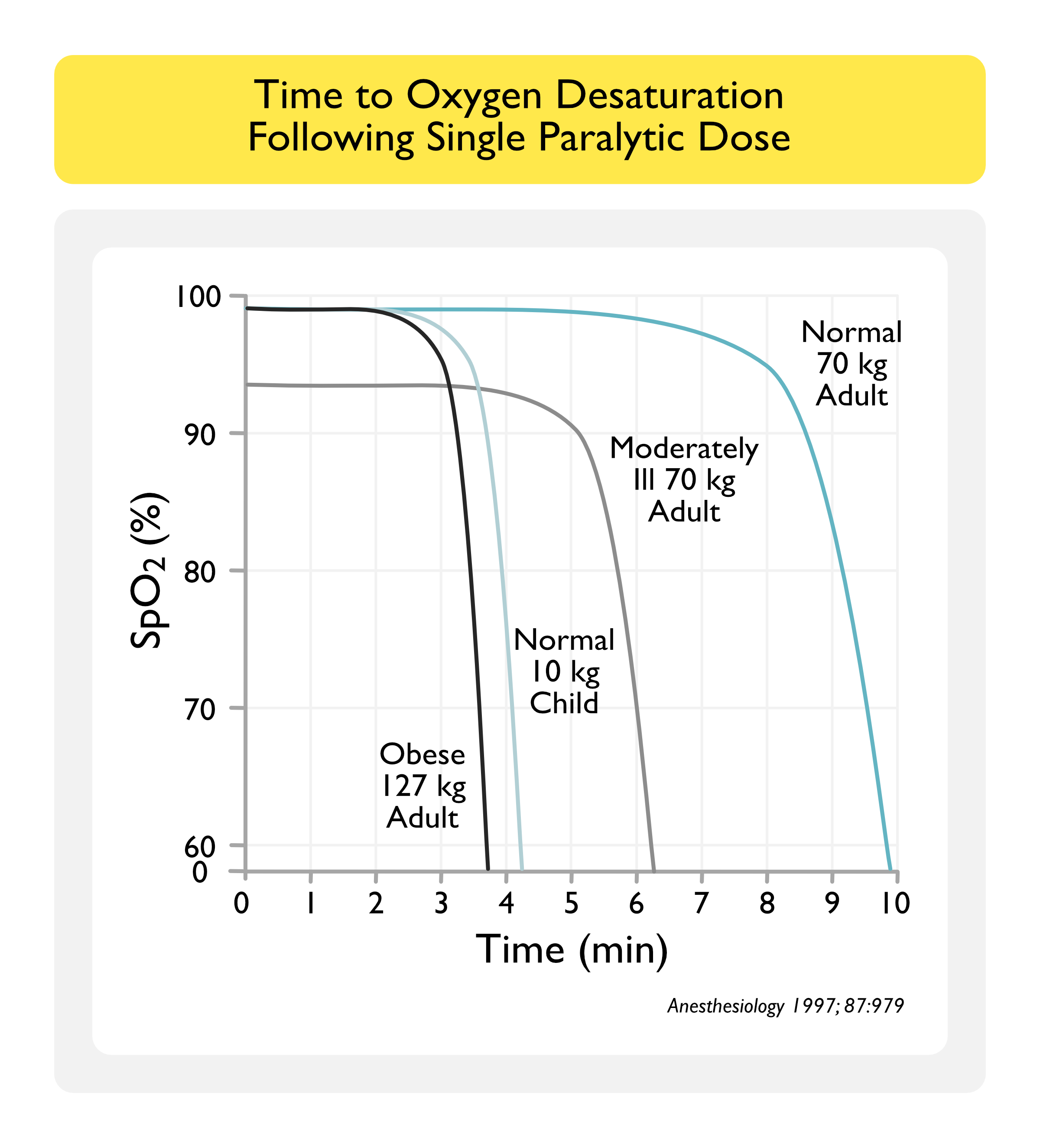
Rapid Sequence Intubation is Based Upon the Observation that, After Preoxygenation, an Average 70 kg Adult Will Maintain SaO2 >90% for 8 min During Apnea (Anesthesiology, 1997) [MEDLINE]
Importantly, Even with Adequate Preoxygenation, this Period of Time is <3 min in Critically Ill, Obese, and Third Trimester Pregnant Patients
This Period of Time is <4 min in Children
Preoxygenation (with the Highest Possible Oxygen Concentration for a Minimum of 3 min) Replaces Nitrogen and Other Gases in the Functional Residual Capacity of the Lung, Creating an Oxygen Reservoir Which is Subsequently Depleted During the Subsequent Rapid Sequence Intubation Apneic Period (Anesth Analg, 2017) [MEDLINE]
Since Rapid Sequence Intubation Utilizes the Monitoring of Oxygen Saturation Using Finger Probe Pulse Oximetry During Apnea, Pulse Oximetry Readings May Lag Behind that of the Central Arterial Circulation in Critically Ill Patients (Can J Anaesth, 1992) [MEDLINE]
Consequently, Pulse Oximetry Must Be Used Judiciously During Rapid Sequence Intubation
Because Obesity is Characterized by Increased Oxygen Consumption and Increased Carbon Dioxide Production, the Time to Desaturation (and the “Safe Apnea Period” During Rapid Sequence Intubation) are Decreased (Anesthesiology, 1997) [MEDLINE]
Body Positioning
Society of Critical Care Medicine Clinical Practice Guidelines for Rapid Sequence Intubation in the Critically Ill Adult Patient (2023) (Crit Care Med, 2023) [MEDLINE]
Use of Head and Torso Inclined (Semi-Fowler) Position is Recommended During Rapid Sequence Intubation (Conditional Recommendation, Very Low Quality of Evidence)
While Rapid Sequence Intubation Has Traditionally Been Performed with the Patient in Neck Flexion and Head Extension (“Sniffing Position”) or Neutral Head and Neck Position (if There is a Concern for Cervical Spine Injury) Together with the Torso Parallel with the Head and Neck
However, Recent Studies Suggest that a Head and Trunk Inclined (Semi-Fowler) Position May Improve First-Pass Success Through Enhanced Preoxygenation (Denitrogenation) Via Increased Functional Residual Capacity (FRC) and Improved Laryngeal View, and Decrease the Risk of Clinically Significant Aspiration of Passively Regurgitated Gastric Contents
Society of Critical Care Medicine Clinical Practice Guidelines for Rapid Sequence Intubation in the Critically Ill Adult Patient (2023) (Crit Care Med, 2023) [MEDLINE]
Nasogastric Tube Decompression is Recommended When the Benefit Outweighs the Risk in Patients Who are Undergoing Rapid Sequence Intubation and are at High Risk of Regurgitation of Gastric Contents
Peri-intubation Vasopressors
Society of Critical Care Medicine Clinical Practice Guidelines for Rapid Sequence Intubation in the Critically Ill Adult Patient (2023) (Crit Care Med, 2023) [MEDLINE]
Peri-Intubation Hypotension is Associated with Increased Intensive Care Unit Mortality (JAMA, 2021) [MEDLINE]
There is Insufficient Evidence to Make a Recommendation Regarding a Difference in the Incidence of Further Hypotension or Post-Intubation Cardiac Arrest Between the Administration of Peri-Intubation Vasopressors or Intravenous Fluids for Hypotensive Critically Ill Patients Undergoing Rapid Sequence Intubation (Insufficient Evidence)
Preoxygenation Technique
Methods to Increase the Reservoir Size During Preoxygenation
Use of Bag-Valve-Mask Ventilation or Noninvasive Positive-Pressure Ventilation, Both of Which Increase the Mean Airway Pressure
Use of 20 Degree Head-Up Patient Positioning, Which Decreases Dependent Atelectasis (Anaesthesia, 2005) [MEDLINE]
Preoxygenation Techniques Based on Patient Type
Patient with Adequate Spontaneous Ventilation and Cooperative
Bag-Valve-Mask Ventilation with Oxygen at 15 L/min
Squeezing the Bag is Not Necessary, But a Tight Mask Seal Must Be Maintained to Ensure a High FIO2
If the Time is Critically Short and the Bag is Squeezed, Eight Vital Capacity Breaths Can Achieve Adequate Preoxygenation in <1 min
Patient with Adequate Spontaneous Ventilation and Uncooperative/Intolerant of Bag-Valve-Mask Ventilation
Non-Rebreather Mask with Flush Rate Oxygen (≥50 L/min): note that standard 15 L/minflow rates are inadequate for preoxygenation due to entrainment of room air (and decrease in the effective FIO2)
High-Flow Nasal Cannula: can also be considered
Patient with Inadequate Spontaneous Ventilation
Bag-Valve-Mask Ventilation with Oxygen at 15 L/min (Synchronized with Patient’s Respiratory Efforts): avoid pressure >20 cm H2O to minimize the degree of gastric insufflation
In its Pure Form, Rapid Sequence Intubation Utilizes Administration of Pharmacologic Sedation (Induction) and Paralysis, Followed by an Apneic Period without Bag-Valve-Mask Ventilation Up to the Point of Endotracheal Tube Placement
Bag-Valve-Mask Ventilation is Avoided, if Possible, to Avoid Gastric Insufflation (Which May Result in Aspiration)
However, In Patients with Right-to-Left Shunt (Usually Intrapulmonary Shunt Resulting from Pneumonia, ARDS, etc), Standard Attempts at Preoxygenation May Be Ineffective
These Patients May Require Positive-Pressure Ventilation with PEEP to Promote Alveolar Recruitment and Facilitate Adequate Preoxygenation
Bag-Valve Mask Ventilation, Noninvasive Positive-Pressure Ventilation, or High-Flow Nasal Cannula Can Be Used to Facilitate Prexoygenation in this Setting
Society of Critical Care Medicine Clinical Practice Guidelines for Rapid Sequence Intubation in the Critically Ill Adult Patient (2023) (Crit Care Med, 2023) [MEDLINE]
Preoxygenation with High-Flow Nasal Cannula is Recommended When Laryngoscopy is Expected to Be Challenging (Conditional Recommendation, Low Quality of Evidence)
Critically Ill Patients are at High Risk of Experiencing Desaturation, Particularly During Prolonged Intubations
Therefore, Preoxygenation is Required to Prolong the Duration of Apnea without Desaturation (“Safe Apnea Time”)
High-Flow Nasal Cannula Does Not Appear to Affect Aspiration Risk (Low Quality Evidence)
Preoxygenation with Noninvasive Positive-Pressure Ventilation is Recommended in Patients with Severe Hypoxemia pO2/FiO2 <150 (Conditional Recommendation, Low Quality of Evidence)
Critically Ill Patients are at High Risk of Experiencing Desaturation, Particularly During Prolonged Intubations
Therefore, Preoxygenation is Required to Prolong the Duration of Apnea without Desaturation (“Safe Apnea Time”)
In Patients with Severe Hypoxemia, Noninvasive Positive-Pressure Ventilation Appears to Have the Strongest Evidence for Decreasing the Incidence of Critical Desaturation During Rapid Sequence Intubation
However, Noninvasive Positive-Pressure Ventilation Requires Removal During Laryngoscopy (While High-Flow Nasal Cannula Does Not)
Medication-Assisted Preoxygenation (“Delayed Sequence Intubation”) to Improve Preoxygenation is Recommended in Patients Undergoing Rapid Sequence Intubation Who are Not Able to Tolerate a Face Mask, Noninvasive Positive-Pressure Ventilation, or High-Flow Nasal Cannula Because of Agitation, Delirium, or Combative Behavior (Conditional Recommendation, Very Low Quality of Evidence)
To Achieve This, the Sedative-Hypnotic Agent is Administered to Facilitate Preoxygenation and Once the Clinician is Satisfied that the Patient is Adequately Preoxygenated, then the Neuromuscular Junction Antagonist is Administered, Followed by Intubation
Continuous Passive Oxygenation During Apnea (“Apneic Oxygenation”)
Continuous Passive Oxygenation Can Be Used During the Rapid Sequence Intubation Apneic Period for Patients Who Cannot Tolerate the Apneic Period without Developing Hypoxemia
Continuous Passive Oxygenation Slows Depletion of the Oxygen Reservoir Created During Preoxygenation
Apneic Oxygenation Can Potentially Induce Worsening Hypercapnia in Patients with Chronic Hypoventilation (in this Setting, Predominantly Due to the Worsening of V/Q Mismatch)
The Resulting Hypercapnia Can Be Deleterious in Specific Patient Populations, Such as Those with Increased Intracranial Pressure, Metabolic Acidosis, or Pulmonary Hypertension
Continuous Passive Oxygenation Techniques
High-Flow Nasal Cannula (HFNC)
Standard Nasal Cannula (at a High Flow Rate): at flow rate ≥15 L/min
Clinical Efficacy-Preoxygenation and Continuous Passive Oxygenation During Apnea (“Apneic Oxygenation”)
Study of Nasopharyngeal Apneic Oxygenation Using the Four Breath Technique in Surgical Patients (Anaesthesia, 2006) [MEDLINE]
Apneic Oxygenation (Following Preoxygenation Using the Four Breath Technique) Delayed the Onset of Oxygen Desaturation During Apnea
Study of Apneic Oxygenation in During Simulated Laryngoscopy in Obese Patients (J Clin Anesth, 2010) [MEDLINE]
Nasal Apneic Oxygenation Improved the Frequency/Duration of SpO2 ≥95% and Increased the Minimal SpO2 During Prolonged Laryngoscopy in Obese Patients
Transnasal Humidified Rapid-Insufflation Ventilatory Exchange (THRIVE) Increases Apnea Time During Endotracheal Intubation (Anaesthesia, 2015) [MEDLINE]
High-Nasal Cannula Oxygenation (During Preoxygenation and Continuing as Post-Oxygenation During Intravenous Induction of Anaesthesia and Neuromuscular Blockade Until Airway was Secured) Increases the Apnea Time During Endotracheal Intubation
Proposed Mechanism: combines the benefits of classical apneic oxygenation with continuous positive airway pressure and gaseous exchange through flow-dependent deadspace flushing
French PREOXYFLOW Multicenter Randomized Trial of High-Flow Nasal Cannula in Hypoxemic Patients Undergoing Intubation (Intensive Care Med, 2015) [MEDLINE]: multicenter, randomized opne-labelled, controlled trial in 6 French ICU’s (n = 124)
In Terms of the Lowest Level of Oxygen Desaturation, High-Flow Nasal Cannula (Maintained Throughout the Procedure) was Comparable to High-Flow Face Mask Preoxygenation (Removed at End of General Anesthesia Induction)
No Differences were Observed in Difficult Intubations, Ventilator-Free Days, intubation-Related Events, or Mortality Rate
Trial of High-Flow Nasal Cannula During Endotracheal Intubation in ICU Patients (Crit Care Med, 2015) [MEDLINE]: n = 101
High-Flow Nasal Cannula Oxygen Significantly Improved Preoxygenation and Reduced the Prevalence of Severe Hypoxemia, as Compared to Non-Rebreathing Bag Reservoir Facemask Oxygen
Australian Study of Apneic Oxygenation in Helicopter Emergency Service (Ann Emerg Med, 2015) [MEDLINE]
Apneic Oxygenation Decreased the Incidence of Oxygen Desaturation in Patients Undergoing Rapid Sequence Intubation
Prospective Trial of Delayed Sequence Intubation in Patients with Delirium (Ann Emerg Med, 2015) [MEDLINE]
Dissociative Dose of Ketamine, Allowing Preoxygenation with High-Flow Nonrebreather Mask or Noninvasive Positive-Pressure Ventilation (NIPPV), Followed by Rapid Sequence Intubation was Safe and Effective
Study of Apneic Oxygenation in Adult Patients the Emergency Department (Acad Emerg Med, 2016) [MEDLINE]
Apneic Oxygenation Increased First-Pass Intubation Success without Hypoxemia
Randomized Trial of Apneic Oxygenation During Intubation in Critically Ill Adult Patients in the Medical ICU (Am J Respir Crit Care Med, 2016) [MEDLINE]: n = 150
Apneic Oxygenation Had No Effect on the Lowest Oxygen Saturation in Critically Ill Patients
German Randomized Trial of Flow Nasal Cannula Versus Bag-Valve-Mask for Preoxygenation Before Intubation in Subjects With Hypoxemic Respiratory Failure (Respir Care, 2016) [MEDLINE]: n = 40
No Significant Difference in the Mean Lowest Oxygen Saturation During intubation Between the High-Flow Nasal Cannula Group and the Bag-Valve-Mask-Ventilation Group in Patients with Mild-Moderate Hypoxemic Respiratory Failure
However, On Continuous Monitoring, There was a Significant Decrease in Oxygen Saturation During the Apnea Phase Before Intubation in the Bag-Valve-Mask-Ventilation Group, which was Not Observed in the High-Flow Nasal Cannula Group
French OPTINIV Trial of High-Flow Nasal Cannula Combined with Noninvasive Positive-Pressure Ventilation vs Noninvasive Positive-Pressure Ventilation Alone for Preoxygenation Prior to Intubation (Intensive Care Med, 2016) [MEDLINE]: single-center, blinded, randomized trial
Use of Combined High-Flow Nasal Cannula and Noninvasive Positive-Pressure Ventilation for Preoxygenation Prior to Intubation was More Effective in Decreasing Oxygen Desaturation, as Compared to Noninvasive Positive-Pressure Ventilation Alone
Trial of Apneic Oxygenation During Rapid Sequence Intubation in the Emergency Department (Acad Emerg Med, 2016) [MEDLINE]
Apneic Oxygenation During RSI Increased the First Pass Success (without Hypoxemia) Rate: defined as successful intubation with SaO2 remaining ≥90%
Randomized Trial of Apneic Oxygenation During Intubation in a Medical ICU (Am J Respir Crit Care Med, 2016) [MEDLINE]: n = 150
Apneic Oxygenation with High-Flow Nasal Cannula (15 L/min) During Intubation Did Not Increase the Lowest SaO2, as Compared to Usual Care
Systematic Review and Meta-Analysis of Support Techniques to Prevent Oxygen Desaturation in Critically Ill Patients Requiring Endotracheal Intubation (J Crit Care, 2017) [MEDLINE]
Apneic Oxygenation was Significantly Associated with Higher Minimum Oxygen Saturation During Intubation, as Compared to No Apneic Oxygenation: but there were no significant differences in severe hypoxemia and intubation related-complications
Further Study is Required to Evaluate the Role of Noninvasive Positive-Pressure Ventilation (NIPPV) and High-Flow Nasal Cannula (HFNC)
Systematic Review/Meta-Analysis of Apneic Oxygenation During Emergency Intubation (Am J Emerg Med, 2017) [MEDLINE]
Apneic Oxygenation Significantly Decreased the Incidence of Hypoxemia During Emergency Intubation
Systematic Review/Meta-Analysis of Apneic Oxygenation (J Crit Care, 2017) [MEDLINE]
In Patients Being Intubated for Any Indication Other than Respiratory Failure, Apneic Oxygenation at Any Flow Rate >15 L/min Decreased the Incidence of Desaturation (<90%) and Critical Desaturation (<80%)
Further Trials are Required, Given the Degree of Heterogeneity in Outcomes and Subgroup Analyses
Systematic Review/Meta-Analysis of Apneic Oxygenation (Ann Emerg Med, 2017) [MEDLINE]
Oxygenation Increased Peri-Intubation Oxygen Saturation, Decreased the Rate of Hypoxemia, and Increased First-Pass Success Rate
Randomized ENDAO Trial of Apneic Oxygenation During Rapid Sequence Intubation in the Emergency Department (Acad Emerg Med, 2017) [MEDLINE]: n = 200
Apneic Oxygenation Had No Effect on the Lowest Mean Oxygen Saturation
However, All Patients were Intubated within 120 sec in this Trial, Likely Diluting Out Any Effect that Apneic Oxygenation Might Have Had
Study of Risk Factors for and Prediction of Hypoxemia During Endotracheal Intubation of Critically Ill Adults (Ann Am Thorac Soc, 2018) [MEDLINE]: n = 426
Predictors of Severe Hypoxemia During Endotracheal Intubation of Critically Ill Adult
Hypoxemic Respiratory Failure as Indication for Intubation (Odds Ratio 2.70; 95% CI: 1.58-4.60)
Lower Oxygen Saturation at Induction (Odds Ratio 0.92 Per 1% Increase; 95% CI: 0.89-0.96 Per 1% Increase)
Younger Age (Odds Ratio 0.97 Per 1-Year Increase in Age; 95% CI: 0.95-0.99 Per 1-Year Increase in Age)
Higher Body Mass Index (Odds Ratio 1.03 Per 1 kg/m2; 95% CI: 1.00-1.06 Per 1 kg/m2)
Race (Odds Ratio 4.58 for White vs Black; 95% CI, 1.97-10.67; Odds Ratio 4.47 for Other vs Black; 95% CI: 1.19-16.84)
Operator with <100 Prior Intubations (Odds Ratio 2.83; 95% CI: 1.37-5.85)
Comprehensive Systematic Review of Randomized Trials for Endotracheal Intubation in Critically Ill Patients (Crit Care, 2018) [MEDLINE]: n = 22 trials
Analyzed 1 Trial Using Pre-Procedure Checklist, 6 Trials of Preoxygenation or Apneic Oxygenation, 3 Trials of Sedatives, 1 Trial of Neuromuscular Blocking Agents, 1 Trial of Patient Positioning, 9 Trials of Video Laryngoscopy, and 1 Trial of Post-Intubation Lung Recruitment
Preoxygenation with Noninvasive Positive-Pressure Ventilation and/or High-Flow Nasal Cannula Before Endotracheal Intubation was Beneficial
Post-Intubation Lung Recruitment Maneuvers May Increase Post-Intubation Oxygenation
No Effect was Found for Use of a Pre-Intubation Checklist, Apneic Oxygenation (on Oxygenation and Hemodynamics), Video Laryngoscopy (on Number and Length of Intubation Attempts), Sedatives and Neuromuscular Blockers (on Hemodynamics)
Video Laryngoscopy was Associated with Severe Adverse Effects in Multiple Trials
Ramped Position Increased the Number of Intubation Attempts
Thiopental Had Negative Hemodynamic Effects
Multicenter, Randomized PreVent Trial of Bag-Valve-Mask Ventilation During Endotracheal Intubation in Critically Ill Patients (NEJM, 2019) [MEDLINE]: n = 401 (7 intensive care units in the US)
Bag-Valve-Mask Ventilation During Endotracheal Intubation Resulted in Improved Oxygenation, as Compared to Apnea Between Induction and Laryngoscopy
Operator-Reported Aspiration Occurred During 2.5% of Intubations in the Bag-Valve-Mask Ventilation Group and During 4.0% of Intubations in the No-Ventilation Group (P = 0.41)
Incidence of New Opacity on Chest X-Ray in the 48 hrs After Endotracheal Intubation was 16.4% in the Bag-Valve-Mask Ventilation Group and 14.8% in the No Ventilation Group (P = 0.73)
Randomized PROTRACH Trial of Nasal High-Flow Preoxygenation for Endotracheal Intubation in the Critically Ill Patient (Intensive Care Med, 2019) [MEDLINE]: n = 192 randomized, n = 184 in intent-to-treat analysis
Compared with Standard Bag-Valve-Mask Oxygenation, Preoxygenation with High-Flow Nasal Cannula Did Not improve the Lowest Oxygen Saturation During Intubation in the Non-Severely Hypoxemic Patients, But Led to a Decrease in Intubation-Related Adverse Events
Cricoid Pressure (Sellick’s Maneuver)
Definition
Cricoid Pressure Applied During Bag-Valve-Mask Ventilation Decrease Gastric Insufflation
Cricoid Pressure Applied During Rapid Sequence Intubation (and Maintained Until the Endotracheal Tube Cuff is Inflated) Theoretically Decreases Emesis with Aspiration
Cautions
Cricoid Pressure is Frequently Applied Improperly and Inconsistently
Cricoid Pressure May Impair Lower Esophageal Sphincter Function
Cricoid Pressure May Result in Esophageal Injury
Cricoid Pressure May Result in Undesirable Movement of the Cervical Spine in Patients with Cervical Spinal Cord Injury
Cricoid Pressure May Contribute to Airway Obstruction, Even When Using a Video Laryngoscope (Ann Emerg Med, 2006) [MEDLINE] (Ann Emerg Med, 2013) [MEDLINE]
Clinical Efficacy
Review of Cricoid Pressure to Prevent Aspiration During Endotracheal Intubation (Emerg Med J, 2005) [MEDLINE]
There is Little Evidence that Cricoid Pressure Decreases the Incidence of Aspiration During Rapid Sequence Intubation
Cadaver Study of Airway Maneuvers During Laryngoscopy (Ann Emerg Med, 2006) [MEDLINE]
Bimanual Laryngoscopy Improved the Laryngoscopic View, as Compared to Cricoid Pressure, BURP, and No Manipulation
Cricoid Pressure and BURP Frequently Worsen the Laryngoscopic View
Anatomic MRI Study of the Effects of Cricoid Pressure During Endotracheal Intubation (Anesth Analg, 2009) [MEDLINE]
Cricoid Pressure Results in Compression of the Postcricoid Hypopharynx (Hypopharynx and Cricoid Ring Move Together as an Anatomic Unit)
The Location and Movement of the Esophagus is Irrelevant to the Efficiency of Cricoid Pressure in Regard to Prevention of Gastric Regurgitation into the Pharynx
Compression of the Esophagus Occurs with Midline and Lateral Displacement of the Cricoid Cartilage Relative to the Underlying Vertebral Body
Intubation Bundles Can Decrease the Incidence of Post-Intubation Adverse Effects/Complications in the Intensive Care Unit (Intensive Care Med, 2010) [MEDLINE]: n = 244
Bundle Components
Capnography
Cricoid Pressure
Intravenous Fluid Loading
Preoxygenation with Noninvasive Positive-Pressure Ventilation
Preparation and Early Administration of Sedation
Presence of Two Operators
Protective Ventilation
Rapid Sequence Induction
Vasopressor Use (If Required)
Observational Study of Identification of the Cricothyroid Membrane in Female Subjects Using Palpation (Anesth Analg, 2012) [MEDLINE]
Misidentification of the Cricothyroid Membrane in Female Patients is Common and its Localization is Less Precise in Those Who are Obese
Cochrane Database Systematic Review of Cricoid Pressure During Rapid Sequence Endotracheal Intubation (Cochrane Database Syst Rev, 2015) [MEDLINE]
No Randomized Trials are Available to Evaluate the Efficacy of Cricoid Pressure During Rapid Sequence Endotracheal Intubation
Non-Randomized Trials Suggest that Cricoid Pressure is Not Required to Safely Perform Rapid Sequence Endotracheal Intubation
Randomized IRIS Trial of Cricoid Pressure in Operating Room Rapid Sequence Intubation (JAMA Surg, 2019) [MEDLINE]: n = 3472
Cricoid Pressure Had No Clinical Benefit in Preventing Aspiration, as Compared to Sham Cricoid Procedure
Secondary End Points (Pneumonia, Length of Stay, Mortality) Were Similar Between the Two Groups
Intubation Time was Longer in the Cricoid Pressure Group
Recommendations
While Cricoid Pressure May Decrease Gastric Insufflation During Bag-Valve-Mask Ventilation, it is No Longer Recommended for Use During Rapid Sequence Endotracheal Intubation
Backward-Upward-Rightward (BURP) Maneuver
Definition
Backward-Upward-Rightward Movement of Larynx by Manipulating the Thyroid Cartilage
Clinical Efficacy
Cadaver Study of Airway Maneuvers During Laryngoscopy (Ann Emerg Med, 2006) [MEDLINE]
Bimanual Laryngoscopy Improved the Laryngoscopic View, as Compared to Cricoid Pressure, BURP, and No Manipulation
Cricoid Pressure and BURP Frequently Worsen the Laryngoscopic View
Mandibular Advancement
May Improve the Laryngoscopic View
Clinical Efficacy
Mandibular Advancement May Improve the Laryngoscopic View During Intubation Performed by Inexperienced Operators (Anesthesiology, 2004) [MEDLINE]
Gum Elastic Bougie
Clinical Efficacy
BEAM Randomized Trial of Gum Elastic Bougie vs Endotracheal Tube and Stylet in Difficult Emergency Intubation in the Emergency Department (JAMA, 2018) [MEDLINE]: n = 757
Among All Patients, Gum Elastic Bougie Increased First-Pass Success Rate in Emergency Intubation (98%), as Compared to Endotracheal Tube and Stylet (87%) (Absolute Between-Group Difference, 11%; 95% CI: 7%-14%])
Among the 380 Patients with at Least 1 Difficult Airway Characteristic, Gum Elastic Bougie Increased First-Pass Success Rate in Emergency Intubation (96%), as Compared to Endotracheal Tube and Stylet (82%) (Absolute Between-Group Difference, 14%; 95% CI: 8%-20%])
Median Duration of the First Intubation Attempt (38 sec vs 36 sec) and the Incidence of Hypoxemia (13% vs 14%) Did Not Differ Significantly Between the Gum Elastic Bougie vs Endotracheal Tube and Stylet Groups
Induction Medications for Rapid Sequence Intubation (RSI)
Adrenal Suppression (see Adrenal Insufficiency): this side effect has created ongoing concern about the use of etomidate for induction for endotracheal intubation in critically ill patients
In the KETASED Multicenter, Randomized Trial of Etomidate vs Ketamine for Intubation of Acutely Ill Patients, Ketamine was a Safe Alternative to Etomidate for Endotracheal Intubation (Although the Percentage of Patients with Adrenal Insufficiency was Significantly Higher in the Etomidate Group) (Lancet, 2009) [MEDLINE]
In a Propensity Score Analysis of Etomidate in Patients with Septic Shock Treated with Hydrocortisone, Etomidate Did Not Impact Life-Threatening Complications Following Intubation, But When Associated with Hydrocortisone, it Also Did Not Worsen Outcome (Crit Care, 2012) [MEDLINE]
In Retrospective Trauma Study Using Propofol as an Induction Agent for Rapid Sequence Intubation, Propofol Did Not Result in Hypotension (Mean Dose: 127 ± 5 mg), as Compared to Etomidate (Mean Dose: 21 ± 6 mg) (Eur J Trauma Emerg Surg, 2015) [MEDLINE]
In a Systematic Review and Meta-Analysis of Mostly Retrospective/Observational Studies of Single-Dose Etomidate for Endotracheal Intubation in Patients with Sepsis, Etomidate Did Not Increase the Mortality Rate (Chest, 2015) [MEDLINE]
In a Cochrane Database Systematic Review of Single-Dose Etomidate for Induction for Endotracheal Intubation, There was No Conclusive Evidence that Etomidate Increased the Mortality Rate or Healthcare Resource Utilization in Critically Ill Patients (But Did Increase the Risk of Adrenal Dysfunction and Multiorgan System Dysfunction by a Small Amount) (Cochrane Database Syst Rev, 2015) [MEDLINE]
In a Comparison of Etomidate and Ketamine for Induction During Rapid Sequence Intubation of Adult Trauma Patients, Patient-Centered Outcomes were Comparable for Either Agent (Ann Emerg Med, 2017) [MEDLINE]
In the KEEP PACE Randomized Trial of Ketamine/Propofol vs Decreased-Dose Etomidate for Induction Prior to Endotracheal Intubation of Critically Ill Patients, Ketamine/Propofol Admixture (0.5 mg/kg of Ketamine and Propofol Each) was Comparable to Decreased Dose Etomidate (0.15 mg/kg) in Terms of Maintaining Mean Arterial Blood Pressure, Use of Vasopressors, and Difficulty of Intubation (J Trauma Acute Care Surg, 2019) [MEDLINE]
In a Meta-Analysis of Etomidate for Induction Prior to Endotracheal Intubation (n = 2,704. 11 Trials), Etomidate Increased the Mortality Rate 23% vs 20% (Risk Ratio 1.16; 95% CI: 1.01-1.33; P = 0.03; I2 = 0%; Number Needed to Harm = 31) (J Crit Care, 2023) [MEDLINE]
Tonic-Clonic Movements (Seizure-Like): may occur in some cases (due to enhanced muscle tone)
Transient Erythema/Morbilliform Rash: has been reported
Clinical Efficacy
In the KETASED Multicenter, Randomized Trial of Etomidate vs Ketamine for Intubation of Acutely Ill Patients, Ketamine was a Safe Alternative to Etomidate for Endotracheal Intubation (Although the Percentage of Patients with Adrenal Insufficiency was Significantly Higher in the Etomidate Group) (Lancet, 2009) [MEDLINE]
In Small Case Series, Ketamine and Propofol (“Ketofol”) Can Be Used as Induction Agents for Intubation of Hemodynamically-Unstable Critically Ill Patients (Am J Case Rep, 2015) [MEDLINE]
In a Comparison of Etomidate and Ketamine for Induction During Rapid Sequence Intubation of Adult Trauma Patients, Patient-Centered Outcomes were Comparable for Either Agent (Ann Emerg Med, 2017) [MEDLINE]
In the KEEP PACE Randomized Trial of Ketamine/Propofol vs Decreased-Dose Etomidate for Induction Prior to Endotracheal Intubation of Critically Ill Patients, Ketamine/Propofol Admixture (0.5 mg/kg of Ketamine and Propofol Each) was Comparable to Decreased Dose Etomidate (0.15 mg/kg) in Terms of Maintaining Mean Arterial Blood Pressure, Use of Vasopressors, and Difficulty of Intubation ( J Trauma Acute Care Surg, 2019) [MEDLINE]
Other Pharmacologic Effects: effect on glutamate receptors, effect on cannabinoid receptors, and sodium channel blocking effects
Onset: 9-51 sec (usual: 30 sec)
Duration (with Bolus Dose): 3-10 min
Half-Life (with Infusion): 30-60 min (longer half-life is observed with prolonged infusion, however, the duration of the clinical effect is typically minutes, as propofol is rapidly distributed into peripheral tissues)
Study of the Safety of Propofol as an Induction Agent (Using 0.5-1.0 mg/kg as the Initial Dose, Average Dose of Propofol: 99 mg, SD ± 7.39) for Urgent Endotracheal Intubation in the ICU Demonstrated Hypotension in Only 4% of Cases (Concomitant Vasopressors were Used in 59% of Cases) (J Intensive Care Med, 2015) [MEDLINE]
In Retrospective Trauma Study Using Propofol as an Induction Agent for Rapid Sequence Intubation, Propofol Did Not Result in Hypotension (Mean Dose: 127 ± 5 mg), as Compared to Etomidate (Mean Dose: 21 ± 6 mg) (Eur J Trauma Emerg Surg, 2015) [MEDLINE]
In Small Case Series, Ketamine and Propofol (“Ketofol”) Can Be Used as Induction Agents for Intubation of Hemodynamically-Unstable Critically Ill Patients (Am J Case Rep, 2015) [MEDLINE]
In the KEEP PACE Randomized Trial of Ketamine/Propofol vs Decreased-Dose Etomidate for Induction Prior to Endotracheal Intubation of Critically Ill Patients, Ketamine/Propofol Admixture (0.5 mg/kg of Ketamine and Propofol Each) was Comparable to Decreased Dose Etomidate (0.15 mg/kg) in Terms of Maintaining Mean Arterial Blood Pressure, Use of Vasopressors, and Difficulty of Intubation ( J Trauma Acute Care Surg, 2019) [MEDLINE]
Society of Critical Care Medicine Clinical Practice Guidelines for Rapid Sequence Intubation in the Critically Ill Adult Patient (2023) (Crit Care Med, 2023) [MEDLINE]
In Critically Ill Adults with Hemodynamic Instability and Depressed Level of Consciousness Who are Undergoing Endotracheal Intubation, Administration of a Sedative-Hypnotic Induction Agent is Recommended When a Neuromuscular Junction Antagonist is Used for Intubation
There is No Difference Between Etomidate and Other Induction Agents Administered for Rapid Sequence Intubation with Respect to Mortality or the Incidence of Hypotension or Vasopressor Use in the Peri-Intubation Period and Through Hospital Discharge (Conditional Recommendation, Moderate Quality of Evidence)
Administration of Corticosteroids is Not Recommended Following Rapid Sequence Intubation with Etomidate for the Purpose of Counteracting Etomidate-Induced Adrenal Suppression (Conditional Recommendation, Low Quality of Evidence)
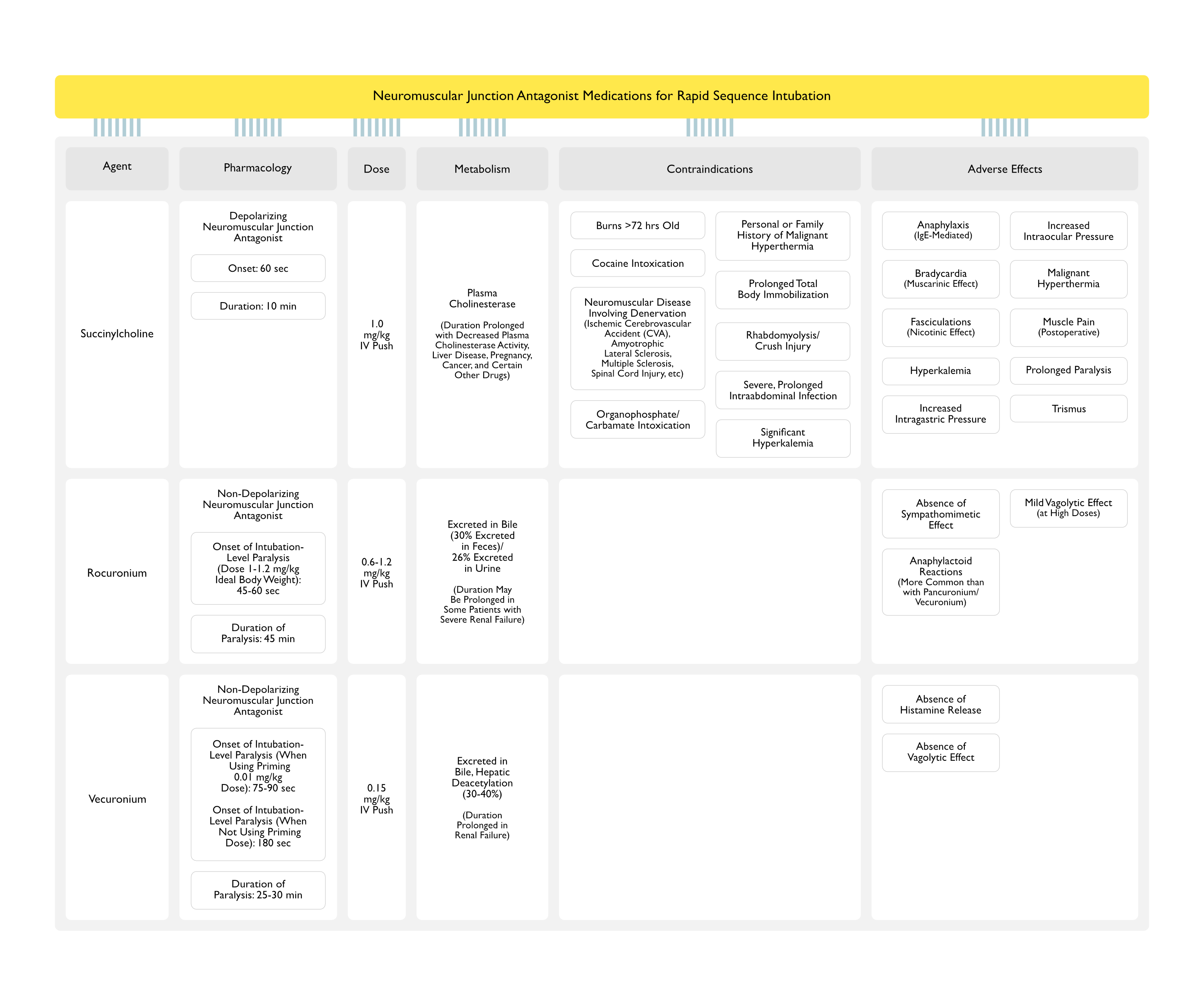
Neuromuscular Junction Antagonist Medications for Rapid Sequence Intubation (RSI)
Onset of Intubation-Level Paralysis (with Dose 1-1.2 mg/kg Ideal Body Weight): 45-60 sec
However, in the Emergency Setting, Clinicians Frequently Estimate Patient Body Weight Incorrectly (Emerg Med Australas, 2005) [MEDLINE] (Spartan Med Res J, 2017) [MEDLINE]
Onset of Intubation-Level Paralysis (When Using a 0.01 mg/kg Priming Dose): 75-90 sec
Priming Dose Accelerates the Onset of Paralysis from the Intubation Dose Which Follows
Onset of Intubation-Level Paralysis (When Not Using a 0.01 mg/kg Priming Dose): 180 sec
Note that Not Using a Priming Dose Results in a Long Time to Achieve Adequate Intubation Conditions (Potentially Requiring Bag-Valve-Mask Ventilation to Maintain Oxygenation)
Duration of Paralysis: 25-30 min
Clinical Efficacy-Use of Neuromuscular Junction Antagonists for Rapid Sequence Intubation (RSI)
In Multicenter, Prospective, Observational Study, Neuromuscular Blocker Administration for Emergent Endotracheal Intubation in the Intensive Care Unit was Associated with Decreased Hypoxemia and Decreased Procedure-Related Complications (Crit Care Med, 2012) [MEDLINE]
In Single Center Observational Study, Neuromuscular Junction Antagonist Administration for Emergent Endotracheal Intubation in the Intensive Care Unit was Associated with Increased First-Pass Success Rates (Even with the Use of a Video Laryngoscope), But Did Not Impact Procedure-Related Complication Rates (Ann Am Thorac Soc, 2015) [MEDLINE]
Clinical Efficacy-Comparison of Neuromuscular Junction Antagonists for Rapid Sequence Intubation (RSI)
While Data are Contradictory Regarding the Efficacy of Succinylcholine vs Rocuronium, in Clinical Use, There is Little Difference Between These Two Agents (Except for the Significantly Longer Duration of Paralysis with Rocuronium)
Meta-Analysis of Succinylcholine vs Rocuronium for Rapid Sequence Intubation (Acad Emerg Med, 2002) [MEDLINE]: n = 40 studies
Succinylcholine Created Excellent Intubation Conditions More Reliably than Rocuronium
If a Second-Line Agent was Required, Rocuronium Used with Propofol Created Intubation Conditions Equivalent to Those with Succinylcholine
Meta-Analysis of Vecuronium vs Rocuronium for Rapid Sequence Intubation (Clin Exp Pharmacol Physiol, 2006) [MEDLINE]” n = 21 studies
The Result of the Meta-Analysis of Differences was -57.9 sec (95% CI: -71.4 to -44.3 sec), Favoring Rocuronium Over Vvecuronium
Comparative Study of Succinylcholine vs Rocuronium for Rapid Sequence Intubation (Acad Emerg Med, 2011) [MEDLINE]: n = 327 intubations
Succinylcholine and Rocuronium were Equivalent with Regard to First-Attempt Intubation Success in the Emergency Department When Dosed According to the Ranges Used in the Study
Systematic Review of Succinylcholine vs Rocuronium for Rapid Sequence Intubation (Cochrane Database Syst Rev, 2015) [MEDLINE]: n = 4,151 (50 trials)
Succinylcholine was Superior to Rocuronium for Achieving Excellent Intubating Conditions (Risk Ratio 0.86; 95% CI: 0.81-0.92) and Clinically Acceptable Intubating Conditions (Risk Ratio 0.97; 95% CI: 0.95-0.99)
Observational Study of Succinylcholine vs Rocuronium for Rapid Sequence Intubation (Ann Emerg Medl, 2018) [MEDLINE]: n = 2,275 intubations with succinylcholine and 1,800 intubations with rocuronium
No Difference Between Paralytic Choice with Regard to First-Pass Rapid Sequence Intubation Success or Peri-Intubation Adverse Events
Multicenter, Single-Blind, Noninferiority, Randomized Trial of Succinylcholine vs Rocuronium for Rapid Sequence Intubation (JAMA, 2019) [MEDLINE]: n = 1,248
Among Patients Undergoing Endotracheal Intubation in an Out-of-Hospital Emergency Setting, Rocuronium, as Compared with Succinylcholine, Failed to Demonstrate Noninferiority with Regard to First-Attempt Intubation Success Rate
Society of Critical Care Medicine Clinical Practice Guidelines for Rapid Sequence Intubation in the Critically Ill Adult Patient (2023) (Crit Care Med, 2023) [MEDLINE]
In Critically Ill Adults Undergoing Endotracheal Intubation, Administration of a Neuromuscular Junction Antagonist is Recommended When a Sedative-Hypnotic Induction Agent is Used for Intubation (Strong Recommendation, Low Quality of Evidence)
Administration of Either Rocuronium or Succinylcholine (When There are No Known Contraindications to Succinylcholine) is Recommended for Rapid Sequence Intubation (Conditional Recommendation, Low Quality of Evidence)
Pharmacology: γ-cyclodextrin which binds to vecuronium or rocuronium in a stable 1:1 complex, resulting in encapsulation (chelation) of the drug and consequent decreased availability of free drug to bind to the neuromuscular junction nicotinic acetylcholine receptors
Dose (Intravenous): 16 mg/kg (reverses neuromuscular blockade within approximately 3 min)
Clinical Utility
Sugammadex May Be Considered to Reverse Rocuronium/Vecuronium-Induced Neuromuscular Blockade in a “Can’t Ventilate, Can’t Intubate” Situation
Laryngoscopy Blades
Direct Laryngoscopy Blades
Macintosh Blade
Curved Blade
Tip is Inserted into the Vallecula
Size: 3 or 4 for adults
Miller Blade
Straight Blade
Tip is Inserted on Top of Epiglottis
Size: 3 or 4 for adults
Video Laryngoscope (Glidescope, etc)
Technique
Tip is Inserted into the Vallecula
Clinical Utility
Video Laryngoscopy is Being Increasingly Used (27% of Cases) as the First Emergency Adult Endotracheal Intubation Attempt Method in Emergency Departments: presumably replacing direct laryngoscopy (Ann Emerg Med, 2015) [MEDLINE]
Advantages
Video Laryngoscope Provides a Superior View, as Compared to Direct Laryngoscopy
Video Laryngoscope Results in Less Cervical Spinal Motion, as Compared to Direct Laryngoscopy: beneficial in patients with unsecured cervical spinal cord injury (J Emerg Med, 2013) [MEDLINE]
Disadvantages
Failure of Video Laryngoscopy is Typically Related to Inability to Pass the Endotracheal Tube Despite Visualization of the Glottis
In Contrast, Failure of Direct Laryngoscopy is Typically Related to Inability to Visualize the Glottis
Secretions/Blood in the Airway May Obscure the View of the Video Laryngoscope
Clinical Efficacy
Systematic Review/Meta-Analysis of Video Laryngoscopic vs Direct Laryngoscopic Endotracheal Intubation in the ICU (Intensive Care Med, 2014) [MEDLINE]: 9 trials (n = 2133) comparing direct laryngoscopic vs video laryngoscopic intubation
Compared to Direct Laryngoscopy, Video Laryngoscopy Reduced the Risk of Difficult Orotracheal Intubation [OR 0.29 (95% confidence interval (CI) 0.20-0.44, p < 0.001)], Cormack 3/4 Grade Airways [OR 0.26 (95% CI 0.17-0.41, p < 0.001)], and Esophageal Intubation [0.14 (95% CI 0.02-0.81, p = 0.03)]
Compared to Direct Laryngoscopy, Video Laryngoscopy Increased the First-Attempt Success Rate [OR 2.07 (95% CI 1.35-3.16, p < 0.001)]
No Statistically Significant Difference was Found for Severe Hypoxemia, Severe Cardiovascular Collapse, or Airway Injury
Randomized Trial of Glidescope Video Laryngoscopy (Crit Care Med, 2015) [MEDLINE]
Glidescope Video Laryngoscopy Improved First-Pass Intubation Success Rates for Urgent Endotracheal Intubation Performed by Pulmonary and Critical Care Medicine Fellow, as Compared to Direct Laryngoscopy
Secondary Analysis of Predictors of Difficult Video Laryngoscopy with GlideScope or C-MAC® with D-Blade (Br J Anaesth, 2016) [MEDLINE]
Characteristics Associated with Greater Risk for Difficult Video Laryngoscopy
Head and Neck Position of “Supine Sniffing” vs “Supine Neutral” (Odds Ratio 1.63; 95% CI: 1.1-2.31)
Undergoing Otolaryngologic or Cardiac Surgery vs General Surgery (Odds Ratio 1.89; 95% CI: 1.19, 3.01 and Odds Ratio 6.13; 95% CI: 1.85-20.37], respectively)
Intubation Performed by an attending anaesthestist vs a supervised resident (Odds Ratio 1.83, 95% CI: 1.14-2.92)
Small Mouth (Odds Ratio 1.18; 95% CI: 1.02-1.36)
Single-Center Observational Study of Video Laryngoscopy and Difficult Airway Characteristics in the ICU (Ann Am Thorac Soc, 2017) [MEDLINE]
Presence of Blood in the Airway, Airway Edema, Cervical Immobility, and Obesity are Associated with Higher Odds of First-Attempt Failure with Video Laryngoscopy
Emergency Department Study of Combined Rapid Sequence Intubation and Video Laryngoscopy (J Emerg Med, 2017) [MEDLINE]
Approximately 11% of Patients (n = 50) Had a Predicted Difficult Airway
Rapid Sequence Intubation was Demonstrated to Have High First-Pass Endotracheal Intubation Success Rates (90%) with Video Laryngoscopy in Patients with Anticipated Difficult Airways
None of the Patients with Difficult Airway Required Placement of a Surgical Airway
Randomized Trial of Video Laryngoscopy vs Direct Laryngoscopy on Successful First-Pass Orotracheal Intubation in ICU Patients (JAMA, 2017) [MEDLINE]: n = 371
In ICU Requiring Intubation, Video Laryngoscopy, as Compared to Direct Laryngoscopy, Did Not Improve First-Pass Orotracheal Intubation Rates
In Post-Hoc Analysis, Video Laryngoscopy was Associated with Higher Rates of Severe Life-Threatening Complications, But Not with Mild-Moderate Life-Threatening Complications
The Proportion of First-Attempt Intubations Performed by Non-Experts (Primarily Residents, n = 290) Did Not Differ Between the Groups (84.4% with Video Laryngoscopy vs 83.2% with Direct Laryngoscopy; Absolute Difference 1.2% [95% CI, -6.3% to 8.6%]; P = .76)
The Median Time to Successful intubation was 3 min (range, 2-4 min) for Both Video Laryngoscopy and Direct Laryngoscopy (Absolute Difference, 0 [95% CI, 0 to 0]; P = .95)
Rapid Sequence Intubation Has High First-Pass Endotracheal Intubation Success Rate with Video Laryngoscopy (90%) in Patients with Anticipated Difficult Airways (J Emerg Med, 2017) [MEDLINE]
Only 11% of Non-Cardiac Arrest Patients Had a Predicted Difficult Airway in this Study and None Required a Surgical Airway
Comprehensive Systematic Review of Randomized Trials for Endotracheal Intubation in Critically Ill Patients (Crit Care, 2018) [MEDLINE]: n = 22 trials
Analyzed 1 Trial Using Pre-Procedure Checklist, 6 Trials of Preoxygenation or Apneic Oxygenation, 3 Trials of Sedatives, 1 Trial of Neuromuscular Blocking Agents, 1 Trial of Patient Positioning, 9 Trials of Video Laryngoscopy, and 1 Trial of Post-Intubation Lung Recruitment
Preoxygenation with Noninvasive Positive-Pressure Ventilation and/or High-Flow Nasal Cannula Before Endotracheal Intubation was Beneficial
Post-Intubation Lung Recruitment Maneuvers May Increase Post-Intubation Oxygenation
No Effect was Found for Use of a Pre-Intubation Checklist, Apneic Oxygenation (on Oxygenation and Hemodynamics), Video Laryngoscopy (on Number and Length of Intubation Attempts), Sedatives and Neuromuscular Blockers (on Hemodynamics)
Video Laryngoscopy was Associated with Severe Adverse Effects in Multiple Trials
Ramped Position Increased the Number of Intubation Attempts
Thiopental Had Negative Hemodynamic Effects
Australian/New Zealand Survey Study of Intubation Practices in the Intensive Care Unit (Crit Care Resusc, 2019)[MEDLINE]
Propofol was the Preferred Induction Agent (67% of Respondents) and rocuronium was the Preferred Neuromuscular Blocking Agent (58% of Respondents)
Video Laryngoscopes were Immediately available in 97% of the ICU’s and were Used as the First-Line Device by 43% of Respondents
DEVICE Trial of Video Laryngoscopy in Critically Ill Adults in Emergency Department and Intensive Care Unit Settings (NEJM, 2023) [MEDLINE]: n = 1,417
Successful First-Attempt Intubation Occurred in 85.1% of Patients in the Video Laryngoscope Group and 70.8% of Patients in the Direct Laryngoscope Group (Absolute Risk Difference of 14.3 Percentage Points; 95% CI: 9.9 to 18.7; P < 0.001)
A Total of 21.4% of Patients in the Video Laryngoscope Group and 20.9% of Patients in the Direct Laryngoscope Group Had a Severe Complication During Intubation (Absolute Risk Difference of 0.5 Percentage Points; 95% CI: -3.9 to 4.9)
Safety Outcomes (Including Esophageal Intubation, Injury to the Teeth, and Aspiration) were Similar in the Two Groups
Consensus Guideline Recommendations to Prevent Unrecognized Esophageal Intubation from the Project for Universal Management of Airways and International Airway Societies (Anaesthesia, 2022) [MEDLINE]
Exhaled Carbon Dioxide Monitoring and Pulse Oximetry Should Be Available and Used for All Episodes of Airway Management
Routine Use of Video Laryngoscopy is Recommended Whenever Feasible
At Each Attempt at Laryngoscopy, the Airway Operator Should Verbalize the View Obtained
The Airway Operator and Assistant Should Each Verbalize Whether Sustained Exhaled Carbon Dioxide and Adequate Oxygen Saturation are Present
Inability to Detect Sustained Exhaled Carbon Dioxide Requires Esophageal intubation to Be Actively Excluded
The Default Response to the Failure to Satisfy the Criteria for Sustained Exhaled Carbon Dioxide Should Be to Remove the Tube and Attempt Ventilation Using a Facemask or Supraglottic Airway
If Immediate Tube Removal is Not Undertaken, Actively Exclude Esophageal Intubation
Repeat Laryngoscopy, Flexible Bronchoscopy, Ultrasound and Use of an Esophageal Detector Device are Valid Techniques
Clinical Examination Should Not Be Used to Exclude Esophageal intubation
Endotracheal Tube Removal Should Be Undertaken if Any of the Following are Present
Esophageal Placement Cannot Be Excluded
Sustained Exhaled Carbon Dioxide Cannot Be Restored
Oxygen Saturation Deteriorates at Any Point Before Restoring Sustained Exhaled Carbon Dioxide
Actions Should Be Taken to Standardize and Improve the Distinctiveness of Variables on Monitor Displays
Interprofessional Education Programs Addressing the Technical and Team Aspects of Task Performance Should Be Undertaken to Implement These Guidelines
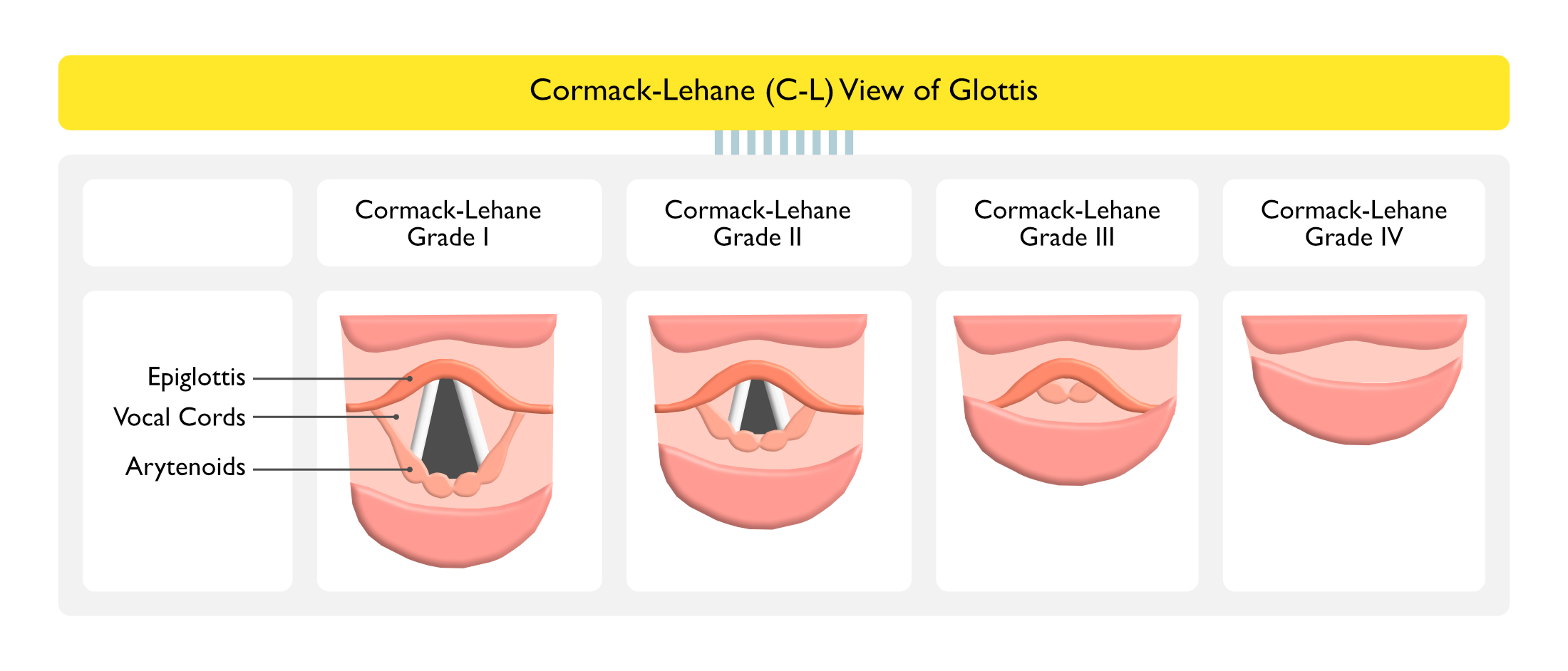
Cormack-Lehane (C-L) View of Glottis
Grade I: full view of glottis
Grade II: partial glottic view
Grade III: minimal glottic view
Grade IV: no view of glottis
Lighted Stylet (Trachlight, etc)
Lighted Stylet Can Be Used for Management of the Difficult Anterior Airway, Where Airway Anatomy is Not Distorted
Device Transilluminates the Glottis Through the Soft Tissues of the Neck
Device Requires Training to Become Proficient with its Use: typically 10-20 intubations are required before proficiency is attained
Hemodynamic Responses with Lighted Stylet are Similar to that with Direct/Video Laryngoscopy
Advantages
Ability to Intubate When the Glottis Cannot Be Visualized Using Direct Laryngoscopy
Decreased Pharyngeal Trauma, as Compared to Direct Laryngoscopy
Produces Less Cervical Spinal Motion than Direct/Video Laryngoscopy: beneficial in patients with cervical spinal cord injury
Disadvantages
Cannot Be Used with Any Airway Anatomic Distortion (Such as Trauma, Tumor, Airway Foreign Body, etc)
Awake Fiberoptic Intubation is Successful in 88-100% of Difficult Airway Patients (Category B3-B Evidence) (American Society of Anesthesiologists Task Force on Management of the Difficult Airway; Anesthesiology, 2013) [MEDLINE]
Extension of Apnea Time During Endotracheal Intubation
Clinical Efficacy
High-Flow Nasal Cannula May Be Used to Facilitate Oxygenation During Fiberoptic Intubation (Chest, 2015) [MEDLINE]
Nasotracheal Intubation
Technique
Disadvantages
Higher Incidence of Maxillary Sinusitis
References
General
Safe intrahospital transport of critically ill ventilator-dependent patients. Chest 1989; 96:631-635 [MEDLINE]
Airway considerations in the management of patients requiring long-term endotracheal intubation. Anesth Analg. 1992;74(2):276 [MEDLINE]
Unplanned extubations in the adult intensive care unit. Am J Respir Crit Care Med 1998; 157:1131-1137 [MEDLINE]
Death and other complications of emergency airway management in critically ill adults. Anesthesiology 1995; 82:367-376 [MEDLINE]
Bedside procedures: solutions to the pitfalls of intrahospital transport. Crit Care Clin 2000; 16:1-6 [MEDLINE]
Difficult airway management in the emergency department. J Emerg Med. 2002 Jan;22(1):31-48 [MEDLINE]
Clinical practice guidelines for sustained neuromuscular blockade in the adult critically ill patient. Crit Care Med. 2002 Jan;30(1):142-56 [MEDLINE]
Towards evidence based emergency medicine: best BETs from the Manchester Royal Infirmary. Colourimetric CO(2) detector compared with capnography for confirming ET tube placement. Emerg Med J 2003: 20: 265-266 [MEDLINE]
The effectiveness of out-of-hospital use of continuous end-tidal carbon dioxide monitoring on the rate of unrecognized misplaced intubation within a regional emergency medical services system. Ann Emerg Med 2005; 45:497-503 [MEDLINE]
Clinical review: management of difficult airways. Crit Care 2006;10:243. doi: 10.1186/cc5112 [MEDLINE]
2010 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Part 8: adult advanced cardiovascular life support. Circulation 2010; 122(18 Suppl 3):S729-S767 [MEDLINE]
Airway management in critically ill patients. Lung 2011; 189:181-192 [MEDLINE]
Emergency airway management: the difficult airway. Emerg Med Clin North Am 2012; 30:401-420 [MEDLINE]
Practice guidelines for management of the difficult airway: an updated report by the American Society of Anesthesiologists Task Force on Management of the Difficult Airway. Anesthesiology. 2013;118:251–270 [MEDLINE]
The effect of body mass index on intubation success rates and complications during emergency airway management. Intern Emerg Med. 2013 Feb;8(1):75-82. Epub 2012 Nov 25 [MEDLINE]
Heated humidified high-flow nasal oxygen in adults: mechanisms of action and clinical implications. Chest. 2015;148(1):253–261 [MEDLINE]
Endotracheal intubation in the ICU. Crit Care. 2015;19:258 [MEDLINE]
Experts’ guidelines of intubation and extubation of the ICU patient of French Society of Anaesthesia and Intensive Care Medicine (SFAR) and French-speaking Intensive Care Society (SRLF) : In collaboration with the pediatric Association of French-speaking Anaesthetists and Intensivists (ADARPEF), French-speaking Group of Intensive Care and Paediatric emergencies (GFRUP) and Intensive Care physiotherapy society (SKR). Ann Intensive Care. 2019 Jan 22;9(1):13. doi: 10.1186/s13613-019-0483-1 [MEDLINE]
Airway Management in Critical Illness: An Update. Chest. 2020 Apr;157(4):877-887. doi: 10.1016/j.chest.2019.10.026 [MEDLINE]
Simulation Training for Critical Care Airway Management: Assessing Translation to Clinical Practice Using a Small Video-Recording Device. Chest 2020 Jul;158(1):272-278. doi: 10.1016/j.chest.2020.01.047 [MEDLINE]
2022 American Society of Anesthesiologists Practice Guidelines for Management of the Difficult Airway. Anesthesiology. 2022 Jan 1;136(1):31-81. doi: 10.1097/ALN.0000000000004002 [MEDLINE]
Intubation Techniques
Rapid Sequence Intubation (RSI)
General
A comparison of blind nasotracheal and succinylcholine-assisted intubation in the poisoned patient. Ann Emerg Med. 1987;16(6):650 [MEDLINE]
Decreased circulation time in the upper limb reduces the lag time of the finger pulse oximeter response. Can J Anaesth. 1992 Jan;39(1):87-9 [MEDLINE]
Rapid-sequence intubation in head trauma. Ann Emerg Med. 1993;22(6):1008 [MEDLINE]
Critical hemoglobin desaturation will occur before return to an unparalyzed state following 1 mg/kg intravenous succinylcholine. Anesthesiology. 1997;87(4):979 [MEDLINE]
Airway management in the emergency department: a one-year study of 610 tracheal intubations. Ann Emerg Med. 1998;31(3):325 [MEDLINE]
Complications of emergency intubation with and without paralysis. Am J Emerg Med. 1999;17(2):141 [MEDLINE]
The failed intubation attempt in the emergency department: analysis of prevalence, rescue techniques, and personnel. J Emerg Med. 2002;23(2):131 [MEDLINE]
A preliminary study of the optimal anesthesia positioning for the morbidly obese patient. Obes Surg. 2003;13(1):4 [MEDLINE]
Airway management by US and Canadian emergency medicine residents: a multicenter analysis of more than 6,000 endotracheal intubation attempts. Ann Emerg Med. 2005;46(4):328 [MEDLINE]
A prospective, randomised controlled trial comparing the efficacy of pre-oxygenation in the 20 degrees head-up vs supine position. Anaesthesia. 2005;60(11):1064 [MEDLINE]
Nasopharyngeal oxygen insufflation following pre-oxygenation using the four deep breath technique. Anaesthesia. 2006;61(5):427 [MEDLINE]
Rapid sequence induction and intubation: current controversy. Anesth Analg. 2010 May;110(5):1318-25 [MEDLINE]
Neuromuscular blocking agent administration for emergent tracheal intubation is associated with decreased prevalence of procedure-related complications. Crit Care Med. 2012 Jun;40(6):1808-1 [MEDLINE]
Association between repeated intubation attempts and adverse events in emergency departments: an analysis of a multicenter prospective observational study. Ann Emerg Med. 2012 Dec;60(6):749-754.e2 [MEDLINE]
The importance of first pass success when performing orotracheal intubation in the emergency department. Acad Emerg Med. 2013;20(1):71 [MEDLINE]
Neuromuscular blockade improves first-attempt success for intubation in the intensive care unit. A propensity matched analysis. Ann Am Thorac Soc. 2015;12(5):734 [MEDLINE]
Techniques, success, and adverse events of emergency department adult intubations. Ann Emerg Med. 2015 Apr;65(4):363-370.e1 [MEDLINE]
Difficult Airway Society 2015 guidelines for management of unanticipated difficult intubation in adults. Br J Anaesth. 2015 Dec;115(6):827-48. doi: 10.1093/bja/aev371 [MEDLINE]
The Physiologically Difficult Airway. West J Emerg Med. 2015;16(7):1109 [MEDLINE]
The effectiveness of rapid sequence intubation (RSI) versus non-RSI in emergency department: an analysis of multicenter prospective observational study. Int J Emerg Med. 2017;10(1):1 [MEDLINE]
Management of Patients with Predicted Difficult Airways in an Academic Emergency Department. J Emerg Med. 2017;53(2):163 [MEDLINE]
Society of Critical Care Medicine Clinical Practice Guidelines for Rapid Sequence Intubation in the Critically Ill Adult Patient. Crit Care Med. 2023 Oct 1;51(10):1411-1430. doi: 10.1097/CCM.0000000000006000 [MEDLINE]
Peri-intubation Vasopressors
INTUBE Study. Intubation practices and adverse peri-intubation events in critically ill patients from 29 countries. JAMA 2021; 325:1164–1172 [MEDLINE]
Preoxygenation and Continuous Passive Oxygenation During Apnea (“Apneic Oxygenation”)
Optimizing preoxygenation in adults. Can J Anaesth. 2009 Jun;56(6):449-66 [MEDLINE]
Apneic oxygenation during prolonged laryngoscopy in obese patients: a randomized, controlled trial of nasal oxygen administration. J Clin Anesth. 2010;22(3):164 [MEDLINE]
Preoxygenation with 20ºhead-up tilt provides longer duration of non-hypoxic apnea than conventional preoxygenation in non-obese healthy adults. J Anesth. 2011 Apr;25(2):189-94 [MEDLINE]
Preoxygenation and prevention of desaturation during emergency airway management. Ann Emerg Med. 2012 Mar;59(3):165-75.e1 [MEDLINE]
PREOXYFLOW Trial. High-flow nasal cannula oxygen during endotracheal intubation in hypoxemic patients: a randomized controlled clinical trial. Intensive Care Med. 2015;41(9):1538 [MEDLINE]
Transnasal humidified rapid-insufflation ventilatory exchange (THRIVE): a physiological method of increasing apnoea time in patients with difficult airways. Anaesthesia 2015;70:323-9 [MEDLINE]
Use of high-flow nasal cannula oxygen therapy to prevent desaturation during tracheal intubation of intensive care patients with mild-to-moderate hypoxemia. Crit Care Med. 2015;43:574–583 [MEDLINE]
Apneic oxygenation was associated with decreased desaturation rates during rapid sequence intubation by an Australian helicopter emergency medicine service. Ann Emerg Med. 2015 Apr;65(4):371-6 [MEDLINE]
Delayed sequence intubation: a prospective observational study. Ann Emerg Med. 2015;65(4):349 [MEDLINE]
Randomized Trial of Apneic Oxygenation during Endotracheal Intubation of the Critically Ill. Am J Respir Crit Care Med. 2016;193(3):273 [MEDLINE]
First Pass Success Without Hypoxemia Is Increased With the Use of Apneic Oxygenation During Rapid Sequence Intubation in the Emergency Department. Acad Emerg Med. 2016;23(6):703 [MEDLINE]
High-Flow Nasal Cannula Versus Bag-Valve-Mask for Preoxygenation Before Intubation in Subjects With Hypoxemic Respiratory Failure. Respir Care. 2016;61(9):1160 [MEDLINE]
Pre-oxygenation: Implications in emergency airway management. Am J Emerg Med. 2017;35(8):1177 [MEDLINE]
Respiratory support techniques to avoid desaturation in critically ill patients requiring endotracheal intubation: A systematic review and meta-analysis J Crit Care. 2017 Oct;41:98-106. doi: 10.1016/j.jcrc.2017.05.003 [MEDLINE]
Emergency Department use of Apneic Oxygenation Versus Usual Care During Rapid Sequence Intubation: A Randomized Controlled Trial (The ENDAO Trial). Acad Emerg Med. 2017;24(11):1387 [MEDLINE]
Apneic oxygenation reduces the incidence of hypoxemia during emergency intubation: A systematic review and meta-analysis. Am J Emerg Med. 2017;35(8):1184 [MEDLINE]
Intubation using apnoeic oxygenation to prevent desaturation: A systematic review and meta-analysis. J Crit Care. 2017;41:42 [MEDLINE]
Effectiveness of Apneic Oxygenation During Intubation: A Systematic Review and Meta-Analysis. Ann Emerg Med. 2017;70(4):483 [MEDLINE]
Risk Factors for and Prediction of Hypoxemia during Tracheal Intubation of Critically Ill Adults. Ann Am Thorac Soc. 2018 Nov;15(11):1320-1327. doi: 10.1513/AnnalsATS.201802-118OC [MEDLINE]
Tracheal intubation in critically ill patients: a comprehensive systematic review of randomized trials. Crit Care. 2018 Jan 20;22(1):6. doi: 10.1186/s13054-017-1927-3 [MEDLINE]
PROTRACH Trial. Nasal high-flow preoxygenation for endotracheal intubation in the critically ill patient: a randomized clinical trial. Intensive Care Med. 2019 Apr;45(4):447-458. doi: 10.1007/s00134-019-05529-w [MEDLINE]
PreVent Trial. Bag-Mask Ventilation during Tracheal Intubation of Critically Ill Adults. N Engl J Med. 2019;380(9):811 [MEDLINE]
Cricoid Pressure (Sellick Maneuver)
Best evidence topic report. Cricoid pressure in emergency rapid sequence induction. Emerg Med J. 2005;22(11):815 [MEDLINE]
Laryngeal view during laryngoscopy: a randomized trial comparing cricoid pressure, backward-upward-rightward pressure, and bimanual laryngoscopy. Ann Emerg Med. 2006;47(6):548 [MEDLINE]
Cricoid pressure in emergency department rapid sequence tracheal intubations: a risk-benefit analysis. Ann Emerg Med. 2007;50(6):653 [MEDLINE]
The effect of cricoid pressure on intubation facilitated by the gum elastic bougie. Anaesthesia. 2007;62(5):456 [MEDLINE]
Cricoid pressure results in compression of the postcricoid hypopharynx: the esophageal position is irrelevant. Anesth Analg. 2009 Nov;109(5):1546-52. doi: 10.1213/ane.0b013e3181b05404 [MEDLINE]
Cricoid pressure and laryngeal manipulation in 402 pre-hospital emergency anaesthetics: essential safety measure or a hindrance to rapid safe intubation? Resuscitation. 2010 Jul;81(7):810-6. doi: 10.1016/j.resuscitation.2010.02.023 [MEDLINE]
Accuracy of identification of the cricothyroid membrane in female subjects using palpation: an observational study. Anesth Analg. 2012 May;114(5):987-92. doi: 10.1213/ANE.0b013e31824970ba [MEDLINE]
Videographic analysis of glottic view with increasing cricoid pressure force. Ann Emerg Med. 2013 Apr;61(4):407-13 [MEDLINE]
The effectiveness of cricoid pressure for occluding the esophageal entrance in anesthetized and paralyzed patients: an experimental and observational glidescope study. Anesth Analg. 2014;118(3):580 [MEDLINE]
Effectiveness and risks of cricoid pressure during rapid sequence induction for endotracheal intubation. Cochrane Database Syst Rev. 2015 [MEDLINE]
Effect of Cricoid Pressure Compared With a Sham Procedure in the Rapid Sequence Induction of Anesthesia: The IRIS Randomized Clinical Trial. JAMA Surg. 2019 Jan 1;154(1):9-17. doi: 10.1001/jamasurg.2018.3577 [MEDLINE]
Backward-Upward-Rightward (BURP) Maneuver
Laryngeal view during laryngoscopy: a randomized trial comparing cricoid pressure, backward-upward-rightward pressure, and bimanual laryngoscopy. Ann Emerg Med. 2006;47(6):548 [MEDLINE]
Cricoid pressure and laryngeal manipulation in 402 pre-hospital emergency anaesthetics: essential safety measure or a hindrance to rapid safe intubation? Resuscitation. 2010 Jul;81(7):810-6. doi: 10.1016/j.resuscitation.2010.02.023 [MEDLINE]
A novel bimanual lip extraction and backward, upward, rightward pressure combination for improved laryngoscopy. Am J Emerg Med. 2017 Jan;35(1):177. doi: 10.1016/j.ajem.2016.10.014 [MEDLINE]
Mandibular Advancement
Mandibular advancement improves the laryngeal view during direct laryngoscopy performed by inexperienced physicians. Anesthesiology. 2004 Mar;100(3):598-601 [MEDLINE]
Gum Elastic Bougie
BEAM Trial. Effect of Use of a Bougie vs Endotracheal Tube and Stylet on First-Attempt Intubation Success Among Patients With Difficult Airways Undergoing Emergency Intubation: A Randomized Clinical Trial. JAMA. 2018 Jun 5;319(21):2179-2189. doi: 10.1001/jama.2018.6496 [MEDLINE]
Induction and Paralytic Medications for Rapid Sequence Intubation
Pharmacological properties of ketamine. Drug Alcohol Rev. 1996 Jun;15(2):145-55 [MEDLINE]
KETASED Trial. Etomidate versus ketamine for rapid sequence intubation in acutely ill patients: a multicentre randomised controlled trial. Lancet. 2009 Jul 25;374(9686):293-300. doi: 10.1016/S0140-6736(09)60949-1 [MEDLINE]
Effects of etomidate on complications related to intubation and on mortality in septic shock patients treated with hydrocortisone: a propensity score analysis. Crit Care. 2012 Nov 21;16(6):R224. doi: 10.1186/cc11871 [MEDLINE]
Systematic assessment of dexmedetomidine as an anesthetic agent: a meta-analysis of randomized controlled trials. Arch Med Sci. 2014 Feb 24;10(1):19-24. doi: 10.5114/aoms.2014.40730 [MEDLINE]
Safety of Propofol as an Induction Agent for Urgent Endotracheal Intubation in the Medical Intensive Care Unit. J Intensive Care Med. 2015 Dec;30(8):499-504. doi: 10.1177/0885066614523100 [MEDLINE]
Use of propofol as an induction agent in the acutely injured patient. Eur J Trauma Emerg Surg. 2015 Aug;41(4):405-11. doi: 10.1007/s00068-014-0479-3 [MEDLINE]
Single-dose etomidate does not increase mortality in patients with sepsis: a systematic review and meta-analysis of randomized controlled trials and observational studies. Chest. 2015 Feb;147(2):335-346. doi: 10.1378/chest.14-1012 [MEDLINE]
Single induction dose of etomidate versus other induction agents for endotracheal intubation in critically ill patients. Cochrane Database Syst Rev. 2015 Jan 8;1:CD010225. doi: 10.1002/14651858.CD010225.pub2 [MEDLINE]
Ketamine and propofol combination (“ketofol”) for endotracheal intubations in critically ill patients: a case series. Am J Case Rep. 2015 Feb 13;16:81-6. doi: 10.12659/AJCR.892424 [MEDLINE]
Comparison of Etomidate and Ketamine for Induction During Rapid Sequence Intubation of Adult Trauma Patients. Ann Emerg Med. 2017 Jan;69(1):24-33.e2. doi: 10.1016/j.annemergmed.2016.08.009 [MEDLINE]
Ketamine/propofol admixture vs etomidate for intubation in the critically ill: KEEP PACE Randomized clinical trial. J Trauma Acute Care Surg. 2019 Oct;87(4):883-891. doi: 10.1097/TA.0000000000002448 [MEDLINE]
Paralytic Agents for Rapid Sequence Intubation
Safety and efficacy of sugammadex for the reversal of rocuronium-induced neuromuscular blockade in cardiac patients undergoing noncardiac surgery. Eur J Anaesthesiol. 2009 Oct;26(10):874-84. doi: 10.1097/EJA.0b013e32832c605b [MEDLINE]
Use of sugammadex in patients with a history of pulmonary disease. J Clin Anesth. 2012 Jun;24(4):289-97. doi: 10.1016/j.jclinane.2011.09.006 [MEDLINE]
Neuromuscular blocking agent administration for emergent tracheal intubation is associated with decreased prevalence of procedure-related complications. Crit Care Med. 2012 Jun;40(6):1808-13. doi: 10.1097/CCM.0b013e31824e0e67 [MEDLINE]
Dialysability of sugammadex and its complex with rocuronium in intensive care patients with severe renal impairment. Br J Anaesth. 2012 Sep;109(3):382-90. doi: 10.1093/bja/aes207 [MEDLINE]
Rapid reversal of neuromuscular blockade by sugammadex after continuous infusion of rocuronium in patients with liver dysfunction undergoing hepatic surgery. Acta Anaesthesiol Taiwan. 2014 Jun;52(2):54-8. doi: 10.1016/j.aat.2014.04.007 [MEDLINE]
Neuromuscular blockade improves first-attempt success for intubation in the intensive care unit. A propensity matched analysis. Ann Am Thorac Soc. 2015 May;12(5):734-41. doi: 10.1513/AnnalsATS.201411-517OC [MEDLINE]
Low-Dose or High-Dose Rocuronium Reversed with Neostigmine or Sugammadex for Cesarean Delivery Anesthesia: A Randomized Controlled Noninferiority Trial of Time to Tracheal Intubation and Extubation. Anesth Analg. 2016 May;122(5):1536-45. doi: 10.1213/ANE.0000000000001197 [MEDLINE]
Sugammadex: A Review of Neuromuscular Blockade Reversal. Drugs. 2016 Jul;76(10):1041-52. doi: 10.1007/s40265-016-0604-1 [MEDLINE]
Efficacy and safety of sugammadex versus neostigmine in reversing neuromuscular blockade in adults. Cochrane Database Syst Rev. 2017 Aug 14;8:CD012763. doi: 10.1002/14651858.CD012763 [MEDLINE]
Safety and efficacy of sugammadex for the reversal of rocuronium-induced neuromuscular blockade in cardiac patients undergoing noncardiac surgery. Eur J Anaesthesiol. 2009 Oct;26(10):874-84. doi: 10.1097/EJA.0b013e32832c605b [MEDLINE]
Use of sugammadex in patients with a history of pulmonary disease. J Clin Anesth. 2012 Jun;24(4):289-97. doi: 10.1016/j.jclinane.2011.09.006 [MEDLINE]
Neuromuscular blocking agent administration for emergent tracheal intubation is associated with decreased prevalence of procedure-related complications. Crit Care Med. 2012 Jun;40(6):1808-13. doi: 10.1097/CCM.0b013e31824e0e67 [MEDLINE]
Dialysability of sugammadex and its complex with rocuronium in intensive care patients with severe renal impairment. Br J Anaesth. 2012 Sep;109(3):382-90. doi: 10.1093/bja/aes207 [MEDLINE]
Rapid reversal of neuromuscular blockade by sugammadex after continuous infusion of rocuronium in patients with liver dysfunction undergoing hepatic surgery. Acta Anaesthesiol Taiwan. 2014 Jun;52(2):54-8. doi: 10.1016/j.aat.2014.04.007 [MEDLINE]
Neuromuscular blockade improves first-attempt success for intubation in the intensive care unit. A propensity matched analysis. Ann Am Thorac Soc. 2015 May;12(5):734-41. doi: 10.1513/AnnalsATS.201411-517OC [MEDLINE]
Low-Dose or High-Dose Rocuronium Reversed with Neostigmine or Sugammadex for Cesarean Delivery Anesthesia: A Randomized Controlled Noninferiority Trial of Time to Tracheal Intubation and Extubation. Anesth Analg. 2016 May;122(5):1536-45. doi: 10.1213/ANE.0000000000001197 [MEDLINE]
Sugammadex: A Review of Neuromuscular Blockade Reversal. Drugs. 2016 Jul;76(10):1041-52. doi: 10.1007/s40265-016-0604-1 [MEDLINE]
Efficacy and safety of sugammadex versus neostigmine in reversing neuromuscular blockade in adults. Cochrane Database Syst Rev. 2017 Aug 14;8:CD012763. doi: 10.1002/14651858.CD012763 [MEDLINE]
Awake Laryngoscopy
Endotracheal intubation in the ICU. Crit Care. 2015;19:258 [MEDLINE]
Awake Laryngoscopy in the Emergency Department. J Emerg Med. 2017;52(3):324 [MEDLINE]
Video Laryngoscopy
Videolaryngoscopy with glidescope reduces cervical spine movement in patients with unsecured cervical spine. J Emerg Med. 2013 Apr;44(4):750-6 [MEDLINE]
Video laryngoscopy versus direct laryngoscopy for orotracheal intubation in the intensive care unit: a systematic review and meta-analysis. Intensive Care Med. 2014 May;40(5):629-39. doi: 10.1007/s00134-014-3236-5 [MEDLINE]
Comparison of video laryngoscopy versus direct laryngoscopy during urgent endotracheal intubation: a randomized controlled trial. Crit Care Med. 2015;43(3):636 [MEDLINE]
Predictors of difficult videolaryngoscopy with GlideScope® or C-MAC® with D-blade: secondary analysis from a large comparative videolaryngoscopy trial. Br J Anaesth. 2016 Jul;117(1):118-23. doi: 10.1093/bja/aew128 [MEDLINE]
Difficult Airway Characteristics Associated with First-Attempt Failure at Intubation Using Video Laryngoscopy in the Intensive Care Unit. Ann Am Thorac Soc. 2017 Mar;14(3):368-375. doi: 10.1513/AnnalsATS.201606-472OC [MEDLINE]
Video Laryngoscopy vs Direct Laryngoscopy on Successful First-Pass Orotracheal Intubation Among ICU Patients: A Randomized Clinical Trial. JAMA. 2017 Feb 7;317(5):483-493. doi: 10.1001/jama.2016.20603 [MEDLINE]
A practice survey of airway management in Australian and New Zealand intensive care units. Crit Care Resusc. 2019 Jun;21(2):139-147 [MEDLINE]
Preventing unrecognised oesophageal intubation: a consensus guideline from the Project for Universal Management of Airways and international airway societies. Anaesthesia. 2022 Dec;77(12):1395-1415. doi: 10.1111/anae.15817 [MEDLINE]
DEVICE Trial. Video versus Direct Laryngoscopy for Tracheal Intubation of Critically Ill Adults. N Engl J Med. 2023 Jun 16. doi: 10.1056/NEJMoa2301601 [MEDLINE]