Key Determinants of Successful Cardiopulmonary Resuscitation (CPR)
Quality Chest Compressions (100-120/min with 2-2.4” Depth and Full Chest Recoil Between Compressions
Early Defibrillation
American Heart Association Guidelines Recommend Maintaining a Chest Compression Fraction of ≥60% (Meaning on Average, Chest Compressions Should Be Withheld<40% of the Intra-Arrest Time ( J Emerg Med, 2018) [MEDLINE]
There May Be Additional Benefit with Maintaining a Chest Compression Fraction of ≥80% (Circulation, 2009) [MEDLINE] (Resuscitation, 2011) [MEDLINE]
Multiple Interventions May Interrupt Chest Compressions: some of which have unclear benefit
Administration of Resuscitation Medications
Endotracheal Intubation: supraglottic airway insertion can be quicker than endotracheal intubation, don’t interfere with chest compressions, and have a loer complication than endotracheal intubation
Vascular Access Attempts: intraosseous access can be quicker than intravenous access and doesn’t interfere with chest compressions
In Cardiopulmonary Arrest, Systemic and Pulmonary Vascular Perfusion is Very Low Despite Optimal Cardiopulmonary Resuscitation (CPR)
Therefore, Ventilation/Perfusion Relationships Can Be Maintained with Low Minute Ventilation
Hyperventilation Should Be Avoided During CPR, as Increased Intrathoracic Pressure and Gastric Distention Can Impede Effective Chest Compressions (Circulation, 2015) [MEDLINE]
Airway Management Techniques During Cardiopulmonary Resuscitation
Laryngeal Mask Airway (LMA) or Other Similar Supraglottic Airway Device (see Airway Management)
Clinical Efficacy of Endotracheal Intubation in Out-of-Hospital Cardiac Arrest
Randomized Trial of Bag-Mask Ventilation vs Endotracheal Intubation During Cardiopulmonary Resuscitation in Out-of-Hospital Cardiac Arrest (JAMA 2018) [MEDLINE]: n= 2043
Bag-Mask Ventilation and Endotracheal Intubation were Equivalent in Terms of 28-Day Neurologic Outcome for Out-of-Hospital Cardiac Arrest
AIRWAYS-2 Randomized Trial of Supraglottic Airway Device vs Tracheal Intubation in Out-of-Hospital Cardiac Arrest ( JAMA, 2018) [MEDLINE]: n = 9296
Supraglottic Airway Device and Endotracheal Intubation Were Equivalent in Terms of 30-Day Outcome in Out-of-Hospital Cardiac Arrest
Trial of Laryngeal Tube Insertion vs Endotracheal Intubation in Out-of-Hospital Cardiac Arrest (JAMA, 2018) [MEDLINE]: n= 3000
Laryngeal Tube Insertion was Superior to Endotracheal Intubation in Terms of 72 hr Mortality Rate in Out-of-Hospital Cardiac Arrest
Recommendations (American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care, 2015) (Circulation, 2015) [MEDLINE]
Use the Maximal Feasible Inspired Oxygen Concentration During CPR (Class IIb, LOE C-EO)
Method of Oxygenation/Ventilation
Inadequate Evidence to Demonstrate a Difference in Survival or Favorable Neurologic Outcome with the Use of Bag-Mask Ventilation, as Compared to Endotracheal Intubation During CPR
Either a Bag-Mask Device or an Advanced Airway May Be Used for Oxygenation/Ventilation During CPR in Both the In-Hospital and Out-of-Hospital Settings (Class IIb, LOE C-LD)
For Healthcare Providers Trained in Their Use, Either an Supraglottic Airway Device or an Endotracheal Tube May Be Used as the Initial Advanced Airway During CPR (Class IIb, LOE C-LD)
Confirmation of Endotracheal Tube Placement
Continuous Waveform Capnography is Recommended in Addition to Clinical Assessment as the Most Reliable Method of Confirming and Monitoring Correct Endotracheal Tube Placement (Class I, LOE C-LD)
If Continuous Waveform Capnometry is Not Available, a Nonwaveform CO2 Detector, Esophageal Detector Device, or Ultrasound Used by an Experienced Operator is a Reasonable Alternative (Class IIa, LOE C-LD)
Ventilation After Advanced Airway Placement
After Placement of Advanced Airway, it is Reasonable to Deliver 1 Breath Every 6 sec (10 Breaths/min) While Continuous Chest Compressions are Being Performed (Class IIb, LOE C-LD)
May Be Complicated by Gastric Rupture in Some Cases (Am J Emerg Med, 1993) [MEDLINE]
Back Blows
Chest Thrusts
Clinical Efficacy
Efficacy of a Single Maneuver is 50% at Best, with the Highest Efficacy Observed When Using Multiple Maneuvers (Crit Care Med, 1979) [MEDLINE]
Recommendations for Responsive Patient (2010 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care) (Circulation, 2010) [MEDLINE] (2015 American Heart Association Guidelines Update for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care) (Circulation, 2015) [MEDLINE]
In a Patient with Severe Airway Obstruction by a Foreign Body, Multiple Rapid-Sequence Abdominal Thrusts Followed by Chest Thrusts is Recommended
If the Abdomen Cannot Be Encircled or the Patient is in the Late Stages of Pregnancy, Chest Thrusts are the Initial Recommended Maneuver
Recommendations for Unresponsive Patient (2010 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care) (Circulation, 2010) [MEDLINE]
Blind Finger Sweep is Not Recommended, Unless Solid Material Becomes Visible in the Upper Airway During the Course of CPR
Cardiopulmonary Resuscitation (CPR): since chest compressions may produce higher airway pressures than abdominal thrusts in unresponsive patients (Resuscitation, 2000) [MEDLINE]
Head-Tilt Chin-Lift is Frequently the First Maneuver to Utilized in a Patient without a Concern About Possible Cervical Cord Spinal Injury
Technique
Use 2 Hands to Apply Downward Pressure to the Forehead and Use Tips of Index and Middle Fingers to Extend Neck by Lifting Jaw Forward at the Mentum: this maneuver moves the tongue anteriorly out of the posterior pharynx (JACEP, 1976) [MEDLINE]
Jaw-Thrust Maneuver
Background
Jaw Thrust Maneuver Can Be Utilized in a Patient Even if There is a Concern About Possible Cervical Spinal Cord Injury
However, Since Airway Maneuvers are Usually Associated with at Least Some Movement of the Cervical Spine, Caution Must Be Exercised in Any Patient in Whom There is a Concern About Potential Cervical Spinal Cord Injury (Spine; Phila Pa 1976) [MEDLINE] (Anesth Analg, 2000) [MEDLINE]
Technique
With Hands on Parieto-Occipital Skull, Thrusting Jaw Forward (Importantly, without Extending the Neck) Moves the Tongue Anteriorly Out of the Posterior Pharynx (ORL J Otorhinolaryngol Relat Spec, 2005) [MEDLINE]
Airway Adjuncts
General Comments
After Establishment of Upper Airway Patency by the Above Upper Airway Maneuvers, Airway Adjuncts Serve to Maintain Patency
Oropharyngeal Airway
Design
Oropharyngeal Airway is a Tube-Like Plastic Device Which Prevents the Tongue and Oropharyngeal Soft Tissues from Obstructing the Upper Airway
Clinical Use
Oropharyngeal Airway Should Only Be Used in a Patient Under Deep Sedation (Due to the Risk of Vomiting and/or Aspiration)
Sizing
When Held Next to the Patients Face with the Flat End in Line with the Patient’s Mouth, the Tip of a Properly-Sized Oropharyngeal Airway Should Just Reach the Angle of the Mandible
Insertion
Insert the Oropharyngeal Airway Upside Down to Avoid Pushing the Tongue Posteriorly into the Oropharynx
Then Carefully Rotate the Oropharyngeal Airway 180 Degrees While Advancing It into the Posterior Pharynx
Adverse Effects/Complications
Capture of Lips/Tongue Between the Oropharyngeal Airway and Teeth (Causing Injury)
Oropharyngeal Mucosal Injury (May Occur During Rotation): may cause bleeding in a patient with coagulopathy
Inadvertent Displacement of the Tongue into the Posterior Pharynx (Worsening Upper Airway Obstruction)
Use of Incorrectly Size Oropharyngeal Airway
Too Large Oropharyngeal Airway: may push the epiglottis into the airway, worsening upper airway obstruction
Too Small Oropharyngeal Airway: may be ineffective and/or become lost in the oropharynx
Vomiting (with/without Aspiration): may occur in a patient who is not adequately sedated prior to oropharyngeal device insertion
Nasopharyngeal Airway (Nasal Trumpet)
Design
Nasopharyngeal Airway is a Soft Rubber or Plastic Tube Which is Passed Through the Nose into the Posterior Pharynx
Clinical Use
Nasopharyngeal Airway May Be Used in a Patient with Clenched Jaw or Inability to Tolerate an Oropharyngeal Airway (Due to Inadequate Sedation)
Sizing
Nasopharyngeal Airway Comes Sizing is Based on the Internal Diameter: with the larger internal diameter = longer length
Small Adult: 6-7 cm
Medium Adult: 7-8 cm
Large Adult: 8-9 cm
Size Should Be Selected Based on Length of the Nasopharyngeal Airway (Emerg Med J, 2005) [MEDLINE]
When Holding the Nasopharyngeal Airway Next to Patient’s Mandible with the Flared End at the Patient’s Mouth, the Distal Tip of a Properly-Sized Nasopharyngeal Airway Should Just Reach the Angle of the Patient’s Mandible
Insertion
Lubricate the Nasopharyngeal Airway (with Water-Soluble Lubricant or Lidocaine Jelly) and Insert Along the Floor of the Nares into the Posterior Pharynx (Following a Downward Angle of Approximately 15 Degrees): note that the contact time for lidocaine jelly is insufficient to provide anesthesia during the insertion, but it may provide anesthesia after the nasopharyngeal airway is already in place
Adverse Effects/Complications
Inadvertent Intracranial Nasopharyngeal Airway Incursion: has been rarely described in patients with basilar skull fractures
Nasopharyngeal Mucosal Injury: may cause epistaxis in up to 30% of cases (Anaesthesia, 1993) [MEDLINE]
Epistaxis May Be Severe in a Patient with Coagulopathy
Use of Excessively Long Nasopharyngeal Airway (Which May Extend into the Esophagus and Cause Gastric Distention During Subsequent Bag-Valve-Mask Ventilation)
Pre-Intubation Assessment
American Society of Anesthesiologists (ASA) Physical Status Classification
ASA 1: Normal Healthy Patient
Example: varicose veins in otherwise healthy patient
ASA 2: Mild Systemic Disease That Does Not Impair Normal Activity
ASA 4: Severe Systemic Disease That is a Constant Threat to Life
Example: CHF, major organ insufficiency, etc
ASA 5: Moribund Patient Who is Not Expected to Survive for 24 hrs With or Without Surgery
Example: intracranial hemorrhage in coma, etc
ASA 6: Declared Brain Dead with Plan for Organ Donation
Assessment for Physiologic Factors Which May Increase the Risk of Intubation
Physiologic Risk Factors Which Increase the Risk of Cardiovascular Compromise During or After Airway Management, Regardless of Anatomic Difficulty with Endotracheal Intubation (West J Emerg Med, 2015) [MEDLINE]
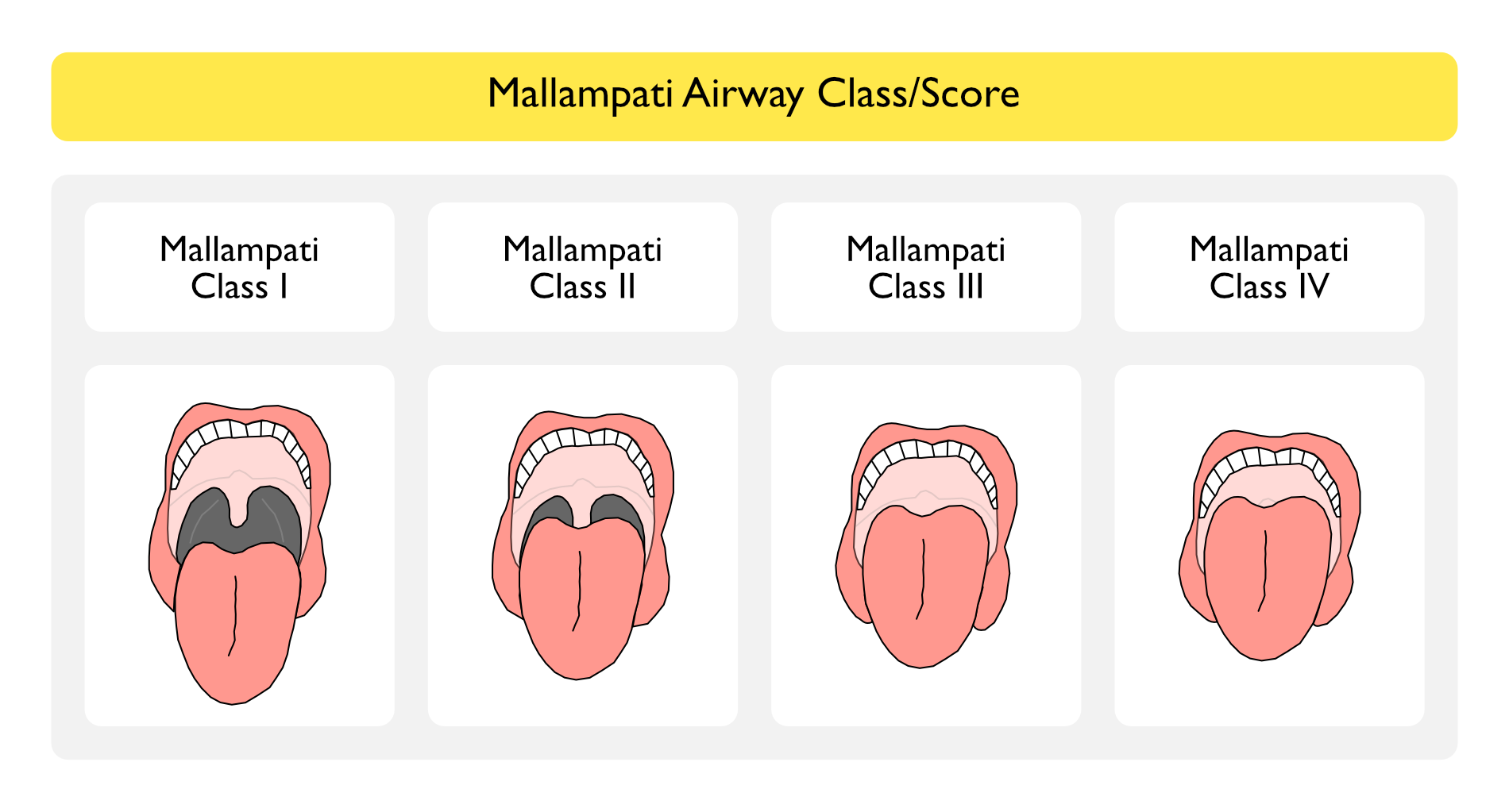
Technique: assessed in upright patient with mouth wide open and tongue out -> allows assessment of oral size and anatomy of tongue and oropharynx
Class I: hard palate, soft palate, entire uvula, fauces, and pillars visible
Class II: hard palate, soft palate, part of uvula, and fauces visible
Class III: hard palate, soft palate, and base of uvula visible -> predicts difficult mask ventilation and difficult intubation
Class IV: only hard palate visible -> predicts difficult mask ventilation and difficult intubation
Clinical Efficacy
In Non-Cardiac Arrest Emergency Department Intubations, Only 32% of Patients were Able to Follow Simple Commands (Allowing Mallampati Assessment) and Not Cervical Spine Immobilized (Allowing Neck Mobility and Thyromental Measurement) (Ann Emerg Med, 2004) [MEDLINE]
In Emergency Department Intubations, Mallampati Could Be Performed in Only 26% of Patients, Due to Lack of Patient Cooperation and Clinical Instability (J Emerg Med, 2010) [MEDLINE]
In Terms of Predicting Difficulty to Intubate, Modified Mallampati Score (≥3) had a Positive Likelihood Ratio 4.1 (95% CI: 3.0-5.6) and Specificity 0.87 (95% CI: 0.81-0.91) (JAMA, 2019) [MEDLINE]
Extended Mallampati Score (EMS)
Technique
Mallampati Performed with the Craniocervical Junction Extended (Rather than Neutral)
Clinical Efficacy
Prospective Study of the Extended Mallampati Score in Patients with BMI ≥40 (Anesth Analg, 2008) [MEDLINE]: n = 346
On Average, Craniocervical Extension Decreased the Modified Mallampati Class (P < 0.0001)
Compared to the Modified Mallampati, the Extended Mallampati Score Improved Specificity and Predictive Value While Maintaining Sensitivity
Compared to the Modified Mallampati and Other Tests, an Extended Mallampati Score Class of 3-4 and a Diagnosis of Diabetes Mellitus were the Only Statistically Significant Predictors of Difficult Laryngoscopy in the Morbidly Obese Patient (see Diabetes Mellitus)
There was No Difference in the Incidence of Difficult Laryngoscopy or Intubation in the Morbidly Obese Patient, as Compared to Patients with a BMI <40
STOP-Bang Score
Study of STOP-Bang Scoring in Preoperative Patients (British Journal of Anaesthesia, 2012) [MEDLINE]: n= 746
Bang
BMI
Age
Neck Circumference
Gender
For STOP-Bang Score of 5, the Odds Ratio (OR) for Moderate/Severe and Severe OSA was 4.8 and 10.4, Respectively
For STOP-Bang Score of 6, the Odds Ratio for Moderate/Severe and Severe OSA was 6.3 and 11.6, Respectively
For STOP-Bang Score of 7 and 8, the Odds Ratio for Moderate/Severe and Severe OSA was 6.9 and 14.9, Respectively
The Predicted Probabilities for Moderate/Severe OSA Increased from 0.36 to 0.60 as the STOP-Bang Score Increased from 3 to 7 and 8
STOP-Bang Score of 5-8 Identified Patients with High Probability of Moderate/Severe OSA
Upper Lip Bite Test
Technique
Easy to Perform Assessment of Patient’s Ability of Lower Incisors to Extend and Reach the Upper Lip
Clinical Efficacy
Systematic Review of Upper Lip Bite Test to Predict Difficult Intubation (JAMA, 2019) [MEDLINE]: n= 33, 559 Patients (62 High-Quality Studies)
Approximately 10% (95% CI: 8.2%-12%) of Patients were Difficult to Intubate in the Systematic Review
In Terms of Predicting Difficulty to Intubate, Grade of Class 3 on the Upper Lip Bite Test Had a Positive Likelihood Ratio of 14 (95% CI: 8.9-22) and Specificity 0.96 (95% CI: 0.93-0.97)
In Terms of Predicting Difficulty to Intubate, Shorter Hyomental Distance Had a Range of <3-5.5 cm, Positive Likelihood Ratio 6.4 (95% CI: 4.1-10), and Specificity 0.97 (95% CI: 0.94-0.98)
In Terms of Predicting Difficulty to Intubate, Retrognathia (Mandible Measuring <9 cm from the Angle of the Jaw to the Tip of the Chin or Subjectively Short) Had a Positive Likelihood Ratio 6.0 (95% CI, 3.1-11) and Specificity 0.98 (95% CI: 0.90-1.0)
In Terms of Predicting Difficulty to Intubate, Combination of Physical Findings Based on the Wilson Score Had a Positive Likelihood Ratio 9.1 (95% CI: 5.1-16) and Specificity 0.95 [95% CI: 0.90-0.98)
In Terms of Predicting Difficulty to Intubate, Modified Mallampati Score (≥3) had a Positive Likelihood Ratio 4.1 (95% CI: 3.0-5.6) and Specificity 0.87 (95% CI: 0.81-0.91)
An Abnormal Upper Lip Bite Test Raises the Probability of Difficult Intubation from 10% to >60% for the Average Risk Patient
Naguib Airway Assessment Method
Commonly Utilized in Operative Settings
Uses Measurements in an Equation to Predict Difficult Intubation
Positive = Difficult Laryngoscopy
Negative = Easy Laryngoscopy
Clinical Efficacy
Study of Diagnostic Validity of Multivariate Airway Scoring Systems to Predict Difficult Laryngoscopy (J Intl Med Res, 2016) [MEDLINE]
All Three Scoring Systems (Naguib, LEMON, and MACOCHA) Demonstrated Inconclusive Zones Which Limit Their Clinical Utility in Predicting Difficult Intubations
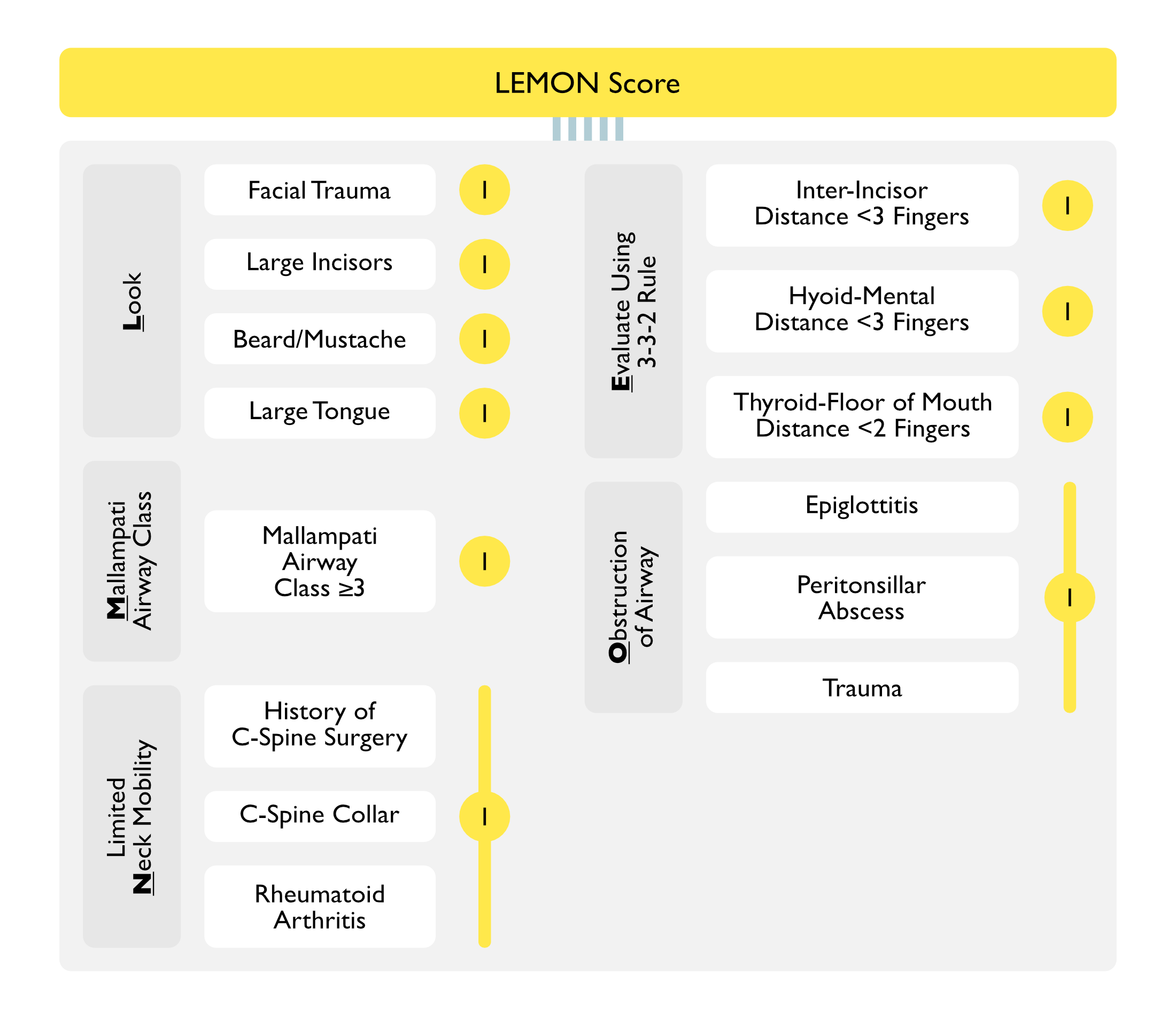
LEMON Airway Assessment Score
Scoring System
Look
Facial Trauma: 1 pt
Large Incisors: 1 pt
Beard/Mustache: 1 pt
Large Tongue: 1 pt
Dentition: assess for dentures, prominent maxillary incisors, broken/loose teeth, and crowns
Scars
Evaluate Using the 3-3-2 Rule
Inter-Incisor Distance <3 Fingers: 1 pt
Hyoid-Mental Distance <3 Fingers: 1 pt
Distance Between the Hyoid Bone (Just Above the Thyroid Cartilage) and Point of Chin (Mentum)
Distance from Thyroid Prominence to the Point of Chin (Mentum) with Next Extended
Thyromental Distance is Considered Important Because During Direct Laryngoscopy, the Tongue is Displaced by the Laryngoscope into the Thyromental Space
A Short Thyromental Distance Indicates Less Space for the Tongue to Be Displaced by the Laryngoscope Blade
Mallampati Airway Class/Score ≥3: 1 pt
Obstruction of Airway (Epiglottitis, Peritonsillar Abscess, Trauma, etc): 1 pt
Limited Neck Mobility (Through Flexion and Extension): 1 pt
Neck Extension May Be Limited with History of C-Spine Surgery
Presence of C-Collar Indicates No C-Spine Mobility
Neck Extension May Be limited Due to Rheumatoid Arthritis (RA) (see Rheumatoid Arthritis): neck extension during intubation in some patients with RA may result in atlanto-axial subluxation, resulting in spinal cord injury
Scoring
Maximum: 10 pts
Clinical Efficacy
Study of LEMON Score for Prediction of Difficult Airway in the Emergency Department (Emerg Med J, 2005) [MEDLINE]
LEMON Score was Able to Successfully Stratify the Risk of Intubation Difficulty in the Emergency Department
Patients with Large Incisors, a Decreased Inter-Incisor Distance, and a Decreased Thyroid to Floor of Mouth Distance were More Likely to Have a Poor Laryngoscopic View (grades 2, 3, or 4)
Study of LEMON and LEON Scores in the Emergency Department ( J Emerg Med, 2009)
The Thyroid-to-Hyoid Distance <2 Fingers was the Only Independent Variable Which Predicted Difficult Intubation
Mallampati Score was Not a Useful Tool in Predicting the Difficulty intubation in the Emergency Department, Such that “LEMON” Can Be Modified to “LEON”
Prospective Validation of the LEMON Score in the Emergency Department (Am J Emerg Med, 2015) [MEDLINE]
Type of Laryngoscope: 84% direct larynogoscope, 16% video laryngoscope
Difficult Intubation: 5.4% with direct larynogoscope, 7.4% with video laryngoscope
Sensitivity: 85.7% with direct laryngoscope, 94.9% with video laryngoscope
Specificity: 47.6% with direct laryngoscope, 40.3% with video laryngoscope
Negative Predictive Value: 98.2% with direct laryngoscope, 9% with video laryngoscope
Study of Diagnostic Validity of Multivariate Airway Scoring Systems to Predict Difficult Laryngoscopy (J Intl Med Res, 2016) [MEDLINE]
All Three Scoring Systems (Naguib, LEMON, and MACOCHA) Demonstrated Inconclusive Zones Which Limit Their Clinical Utility in Predicting Difficult Intubations
Study of the Modified LEMON Score in Patients Undergoing Intubation for Emergency Surgery for Trauma (J Emerg Surg, 2018) [MEDLINE]
Modified LEMON Score (the LEON Score, Omitting the Mallampati Score Component) was Correlated with Difficult Intubation in Adult Trauma Patients Undergoing Emergency Surgery
Systematic Review of Airway Assessment Methods to Predict Difficult Intubation (JAMA, 2019) [MEDLINE]: n= 33, 559 Patients (62 High-Quality Studies)
Approximately 10% (95% CI: 8.2%-12%) of Patients were Difficult to Intubate in the Systematic Review
In Terms of Predicting Difficulty to Intubate, Grade of Class 3 on the Upper Lip Bite Test Had a Positive Likelihood Ratio of 14 (95% CI: 8.9-22) and Specificity 0.96 (95% CI: 0.93-0.97)
In Terms of Predicting Difficulty to Intubate, Shorter Hyomental Distance Had a Range of <3-5.5 cm, Positive Likelihood Ratio 6.4 (95% CI: 4.1-10), and Specificity 0.97 (95% CI: 0.94-0.98)
In Terms of Predicting Difficulty to Intubate, Retrognathia (Mandible Measuring <9 cm from the Angle of the Jaw to the Tip of the Chin or Subjectively Short) Had a Positive Likelihood Ratio 6.0 (95% CI, 3.1-11) and Specificity 0.98 (95% CI: 0.90-1.0)
In Terms of Predicting Difficulty to Intubate, Combination of Physical Findings Based on the Wilson Score Had a Positive Likelihood Ratio 9.1 (95% CI: 5.1-16) and Specificity 0.95 [95% CI: 0.90-0.98)
In Terms of Predicting Difficulty to Intubate, Modified Mallampati Score (≥3) had a Positive Likelihood Ratio 4.1 (95% CI: 3.0-5.6) and Specificity 0.87 (95% CI: 0.81-0.91)
An Abnormal Upper Lip Bite Test Raises the Probability of Difficult Intubation from 10% to >60% for the Average Risk Patient
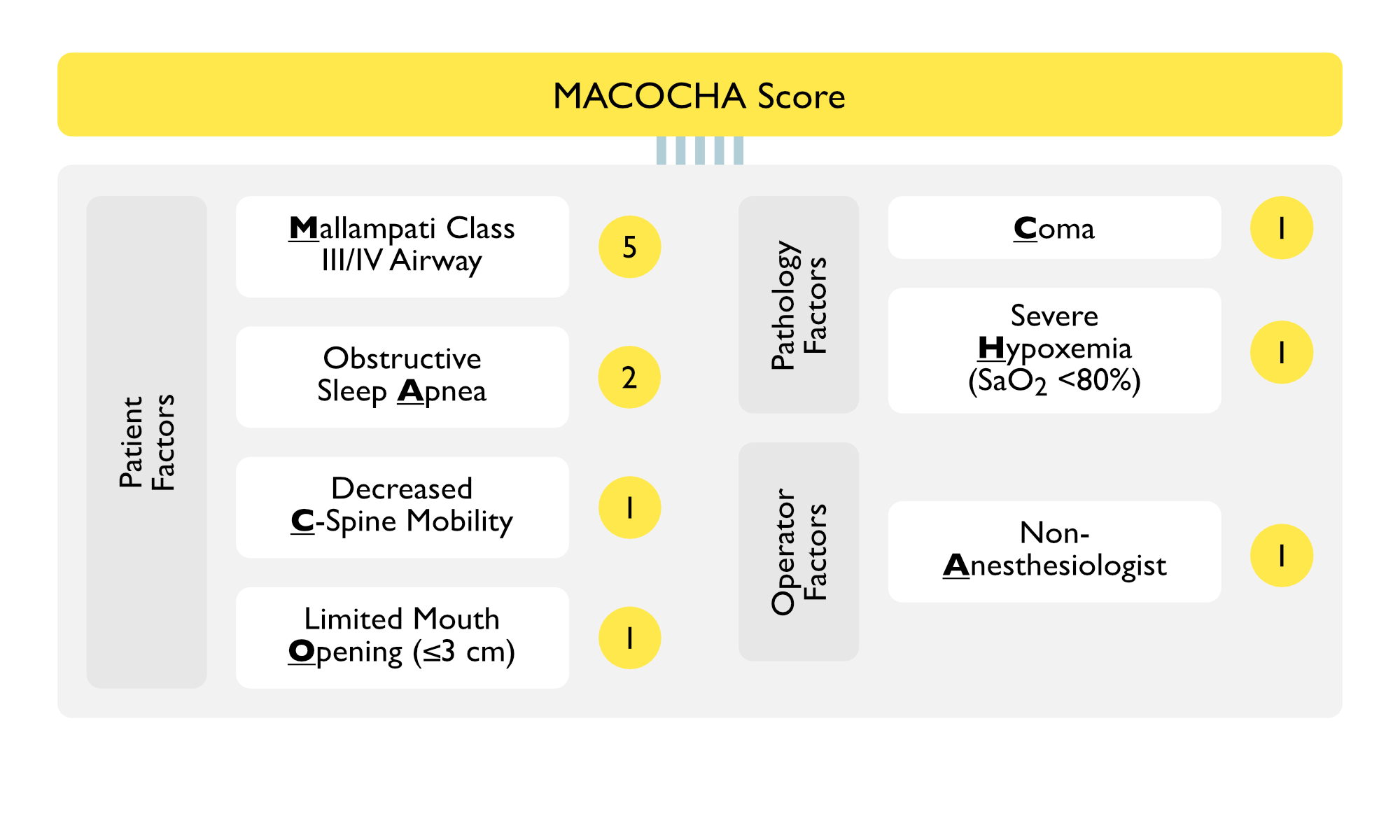
MACHOCHA Airway Assessment Score
Scoring System (Am J Respir Crit Care Med, 2013) [MEDLINE]
MACOCHA Score Can Be Used to Predict Intubation Failure in Non-Anesthesiologist Trainees (J Crit Care, 2015) [MEDLINE]
Study of Diagnostic Validity of Multivariate Airway Scoring Systems to Predict Difficult Laryngoscopy (J Intl Med Res, 2016) [MEDLINE]
All Three Scoring Systems (Naguib, LEMON, and MACOCHA) Demonstrated Inconclusive Zones Which Limit Their Clinical Utility in Predicting Difficult Intubations
Systematic Review of Airway Assessment Methods to Predict Difficult Intubation (JAMA, 2019) [MEDLINE]: n= 33, 559 Patients (62 High-Quality Studies)
Approximately 10% (95% CI: 8.2%-12%) of Patients were Difficult to Intubate in the Systematic Review
In Terms of Predicting Difficulty to Intubate, Grade of Class 3 on the Upper Lip Bite Test Had a Positive Likelihood Ratio of 14 (95% CI: 8.9-22) and Specificity 0.96 (95% CI: 0.93-0.97)
In Terms of Predicting Difficulty to Intubate, Shorter Hyomental Distance Had a Range of <3-5.5 cm, Positive Likelihood Ratio 6.4 (95% CI: 4.1-10), and Specificity 0.97 (95% CI: 0.94-0.98)
In Terms of Predicting Difficulty to Intubate, Retrognathia (Mandible Measuring <9 cm from the Angle of the Jaw to the Tip of the Chin or Subjectively Short) Had a Positive Likelihood Ratio 6.0 (95% CI, 3.1-11) and Specificity 0.98 (95% CI: 0.90-1.0)
In Terms of Predicting Difficulty to Intubate, Combination of Physical Findings Based on the Wilson Score Had a Positive Likelihood Ratio 9.1 (95% CI: 5.1-16) and Specificity 0.95 [95% CI: 0.90-0.98)
In Terms of Predicting Difficulty to Intubate, Modified Mallampati Score (≥3) had a Positive Likelihood Ratio 4.1 (95% CI: 3.0-5.6) and Specificity 0.87 (95% CI: 0.81-0.91)
An Abnormal Upper Lip Bite Test Raises the Probability of Difficult Intubation from 10% to >60% for the Average Risk Patient
Specific Preoperative Airway Assessment of Patients with Known/Suspected Obstructive Sleep Apnea (OSA) (see Obstructive Sleep Apnea)
Recommendations (American Society of Anesthesiologists Practice Guidelines for the Perioperative Management of Patients with Obstructive Sleep Apnea 2014) (Anesthesiology, 2014) [MEDLINE]
Specific Preoperative Airway Assessment of Patients with a Potential Difficult Airway
Recommendations (2022 American Society of Anesthesiologists Practice Guidelines for Management of the Difficult Airway) (Anesthesiology, 2022) [MEDLINE]
Recommendations for Airway Evaluation
Before Initiation of Anesthetic Care/Airway Management, Airway Risk Assessment Should Be Performed by the Person(s) Responsible for Airway Management (Whenever Feasible) to Identify Patient, Medical, Surgical, Environmental, and Anesthetic Factors (Risk of Aspiration, etc) Which May Indicate the Potential for a Difficult Airway
When Available in the Patient’s Medical Record, Evaluate Demographic Information, Clinical Conditions, Diagnostic Test Findings, Patient/Family Interviews, and Questionnaire Responses
Assess Multiple Demographic and Clinical Characteristics to Determine a Patient’s Potential for a Difficult Airway or Aspiration
Before Initiation of Anesthetic Care/Airway Management, Conduct an Airway Physical Examination to Identify Physical Characteristics Which May Indicate the Potential for a Difficult Airway
Physical Examination May Include Assessment of Facial Features, Anatomical Measurements, and Landmarks
Additional Evaluation to Characterize the Likelihood or Nature of the Anticipated Airway Difficulty May Include Bedside Endoscopy, Virtual Laryngoscopy/Bronchoscopy, or Three-Dimensional Printing
Assess Multiple Airway Features to Determine a Patient’s Potential for Difficult Airway or Aspiration
Recommendations for Preparation for Difficult Airway Management
Ensure that Airway Management Equipment is Available in the Room
Ensure that a Portable Storage Unit Which Contains Specialized Equipment for Difficult Airway Management is Immediately Available
If a Difficult Airway is Known or Suspected
Ensure that a Skilled Individual is Present or Immediately Available to Assist with Airway Management (When Feasible)
Inform the Patient (or Responsible Person) of the Special Risks and Procedures Pertaining to Management of the Difficult Airway
Properly Position the Patient, Administer Supplemental Oxygen Before Initiating Management of the Difficult Airway, and Continue to Deliver Supplemental Oxygen (Whenever Feasible) throughout the Process of Difficult Airway Management (including Extubation)
At a Minimum, Ensure that Monitoring According to the ASA Standards for Basic Anesthesia Monitoring is Performed Before/During/After Airway Management of All Patients
Recommendations for Anticipated Difficult Airway Management
Have a Preformulated Strategy for Management of the Anticipated Difficult Airway
Strategy Will Depend on the Anticipated Surgery, Condition of the Patient, Patient Cooperation/Consent, Patient Age, and Skills/Preferences of the Anesthesiologist
Develop a Strategy for the Following
Awake Intubation
Patient Who Can Be Adequately Ventilate, But is Difficult to Intubate
Patient Who Cannot Be Ventilated or Intubated
Patient Expected to Demonstrate Difficulty with Emergency Invasive Airway Rescue
When Appropriate, Perform Awake Intubation if the Patient is Suspected to Be a Difficult Intubation and ≥1 of the Following Apply
Patient Expected to Be Difficult to Ventilate (with Face Mask or Supraglottic Airway)
Increased Risk of Aspiration
Patient Expected to Be Intolerant of a Brief Apneic Episode
Patient Expected to Demonstrate Difficulty with Emergency Invasive Airway Rescue
The Uncooperative or Pediatric Patient May Restrict the Options for Difficult Airway Management (Particularly Options Which Involve Awake Intubation)
Airway Management in the Uncooperative or Pediatric Patient May Require an Approach (Such as Intubation Attempts After Induction of General Anesthesia) Which Might Not Be Regarded as a Primary Approach in a Cooperative Patient
Proceed with Airway Management After Induction of General Anesthesia When the Benefits are Judged to Outweigh the Risks
For Either Awake or Anesthetized Intubation, Airway Maneuvers May Be Attempted to Facilitate Intubation
Before Attempting Intubation of the Anticipated Difficult Airway, Determine the Benefit of a Noninvasive vs Invasive Approach to Airway Management
If Noninvasive Approach is Selected, Identify a Preferred Sequence of Noninvasive Airway Management Devices
If Difficulty is Encountered with a Technique, Combination Techniques May Be Used
Be Aware of the Passage of Time, the Number of Attempts, and Oxygen Saturation
Provide and Test Mask Ventilation After Each Attempt (When Feasible)
Limit the Number of Attempts at Endotracheal Intubation or Supraglottic Airway Placement to Avoid Potential Injury and Complications
If Elective Invasive Approach is Selected, Identify a Preferred Intervention
Ensure that an Invasive Airway is Performed by an Individual Trained in Invasive Airway Techniques (Whenever Possible)
If the Selected Approach Fails or is Not Feasible, Identify an Alternative Invasive Intervention
Initiate VV-ECMO When/if Appropriate and Available
Recommendations for Unanticipated and Emergency Difficult Airway Management
Call for Help
Optimize Oxygenation
When Appropriate, Refer to an Algorithm and/or Cognitive Aid
When Encountering an Unanticipated Difficult Airway
Determine the Benefit of Waking and/or Restoring Spontaneous Breathing
Determine the Benefit of a Noninvasive vs Invasive Approach to Airway Management
If a Noninvasive Approach is Selected, Identify a Preferred Sequence of Noninvasive Airway Management Devices to Use
If Difficulty is Encountered with Individual Techniques, Combination techniques May Be Performed
Be Aware of the Passage of Time, the Number of Attempts, and Oxygen Saturation
Provide and Test Mask Ventilation After Each Attempt (When Feasible)
Limit the Number of Attempts at Endotracheal Intubation or Supraglottic Airway Placement to Avoid Potential Injury and Complications
If an Invasive approach to the Airway is Necessary (Due to “Cannot Intubate, Cannot Ventilate” Scenario), Identify a Preferred Intervention
Ensure that an Invasive Airway is Performed by an Individual Trained in Invasive Airway Techniques (Whenever Possible)
Ensure that an Invasive Airway is Performed as Rapidly as Possible
If the Selected Invasive Approach Fails or is Not Feasible, Identify an Alternative Invasive Intervention
Initiate VV-ECMO When/if Appropriate and Available
Bag-Valve-Mask (BVM) Ventilation
General Comments
Proper Bag-Valve-Mask Ventilation Allows for Adequate Oxygenation and Ventilation, Giving the Provider Time to Prepare for a Well-Controlled Endotracheal Intubation (see Endotracheal Intubation)
Requirements for Effective Bag-Valve-Mask Ventilation
Proper Mask Seal
Upper Airway Patency
Ability to Provide the Proper Respiratory Rate, Tidal Volume, and Cadence to Achieve Ventilation
Types of Ventilation Bags
Self-Inflating Ventilation Bag (Ambu Bag)
Technique
Bag Has a Recoil Mechanism, Allowing Self-Inflation: does not require an oxygen flow to reinflate
Ambu Bag Has a One-Way Valve to Prevent Rebreathing: however, with a tight mask seal, some spontaneously breathing patients may be able to generate adequate inspiratory pressure to overcome the one-way valve
Oxygen Flows to the Patient When the Bag is Squeezed
Range of Oxygen Delivery: 95-100% FIO2 (with reservoir)
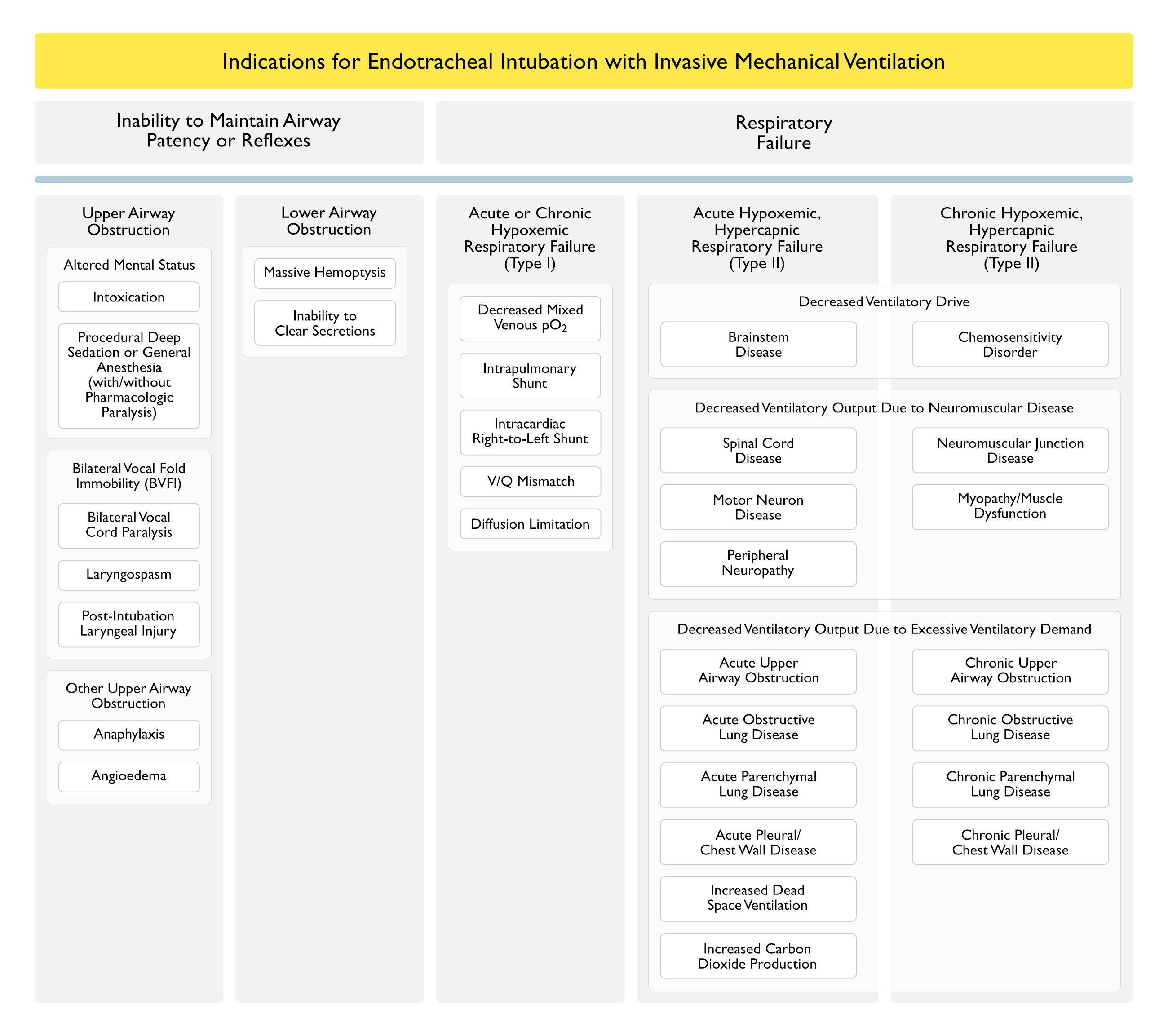
Considerations
Allows Assisted Ventilation in Combination with Supplemental Oxygen: assisted ventilation is useful for patient who may be hypoxemic in combination with hypercapnic (i.e. in type II hypoxemic, hypercapnic respiratory failure)
Should Not Use to Provide Blow By
Requires a Reservoir to Achieve Higher FIO2
Flow-Inflating Ventilation Bag (Anesthesia Bag)
Technique
Flow-Inflating Bag Provides a Constant Flow of Oxygen (When Connected to an Oxygen Source): bag requires a constant oxygen flow to remain inflated
Range of Oxygen Delivery: up to 100% FIO2
Considerations
Allows Assisted Ventilation in Combination with Supplemental Oxygen: assisted ventilation is useful for patient who may be hypoxemic in combination with hypercapnic (i.e. in type II hypoxemic, hypercapnic respiratory failure)
May Use to Provide Blow By
Requires Expertise to Use Effectively (Pediatr Emerg Care, 1997) [MEDLINE]
Technique
General Comments
Position the Mask So that the Top of the Mask is on the Bridge of the Nose and the Bottom of the Mask Covers the Mandibular Alveolar Ridge
Operator Should Not Rest Wrists or the Upper Part of the Mask on the Patients Eyes (to Avoid Inducing a Vagal Response or Causing Corneal Damage
Mask Size
Ensure that Airway Adjunct and Corners of the Mouth are Within the Mask and Allow a Proper Seal
Requires Only a Single Provider to Perform Both Mask Sealing and Bag Ventilation
Place Hand with Thumb Web Resting Against the Mask Connector Tube and Three Fingers Along the Mandible (Using Fingers to Advance the Mandible Forward)
Double-Handed Bag-Valve-Mask Ventilation Technique: generally considered the more effective method (Anesthesiology, 2010) [MEDLINE]
Requires a Second Person to Perform Bag Ventilation
Place Thumb and Index Finger on the Top of Mask and Other Three Fingers Along the Mandible (Using Fingers to Advance the Mandible Forward)
Alternately, the Provider Can Place Their Thenar Eminences on the Top of the Mask and the Other Four Fingers Along the Mandible (Using Fingers to Advance the Mandible Forward): this method may be less fatiguing and provide superior ventilation (Clin Anesth, 2013) [MEDLINE]
Respiratory Rate
Generally, the Respiratory Rate During Bag Ventilation Should Correspond to the Patient’s Expected Acid-Base Status (with Caution to Avoid High Respiratory Rates in the Setting of Hemodynamic Compromise)
During Cardiopulmonary Resuscitation (CPR), Respiratory Rate Should Be <10-12 Breaths/min to Avoid Creating Unnecessary Auto-PEEP Which May Increased Intrathoracic Pressure, Resulting in Decreased Venous Return to the Right Side of the Heart and Decreased Cardiac Output ( Circulation, 2004) [MEDLINE] (Crit Care Med, 2004) [MEDLINE]
During CPR, the Standard Compression:Ventilation Ratio of 30:2 Would Result in a Respiratory Rate of Approximately 8 Breaths/min
Tidal Volume
Generally, a Tidal Volume of 8-10 mL/kg is Adequate
During CPR, Tidal Volume of 5-6 mL/kg is Adequate, Due to Presence of Decreased Cardiac Output (Circulation, 1989) [MEDLINE]
Cricoid Pressure (Sellick’s Maneuver)
Definition
Cricoid Pressure Applied During Bag-Valve-Mask Ventilation Decrease Gastric Insufflation
Cricoid Pressure Applied During Rapid Sequence Intubation Theoretically Decreases Emesis with Aspiration
Maintain Cricoid Pressure Until the Endotracheal Tube Cuff is Inflated
Cautions
Cricoid Pressure is Frequently Applied Improperly and Inconsistently
Cricoid Pressure May Impair Lower Esophageal Sphincter Function
Cricoid Pressure May Result in Esophageal Injury
Cricoid Pressure May Result in Undesirable Movement of the Cervical Spine in Patients with Cervical Spinal Cord Injury
Cricoid Pressure May Contribute to Airway Obstruction, Even When Using a Video Laryngoscope (Ann Emerg Med, 2006) [MEDLINE] (Ann Emerg Med, 2013) [MEDLINE]
Clinical Efficacy
Review of Cricoid Pressure to Prevent Aspiration During Endotracheal Intubation (Emerg Med J, 2005) [MEDLINE]
There is Little Evidence that Cricoid Pressure Decreases the Incidence of Aspiration During Rapid Sequence Intubation
Cochrane Database Systematic Review of Cricoid Pressure During Rapid Sequence Endotracheal Intubation (Cochrane Database Syst Rev, 2015) [MEDLINE]
No Randomized Trials are Available to Evaluate the Efficacy of Cricoid Pressure During Rapid Sequence Endotracheal Intubation
Non-Randomized Trials Suggest that Cricoid Pressure is Not Required to Safely Perform Rapid Sequence Endotracheal Intubation
Recommendations
While Cricoid Pressure May Decrease Gastric Insufflation During Bag-Valve-Mask Ventilation, it is No Longer Recommended for Use During Rapid Sequence Endotracheal Intubation
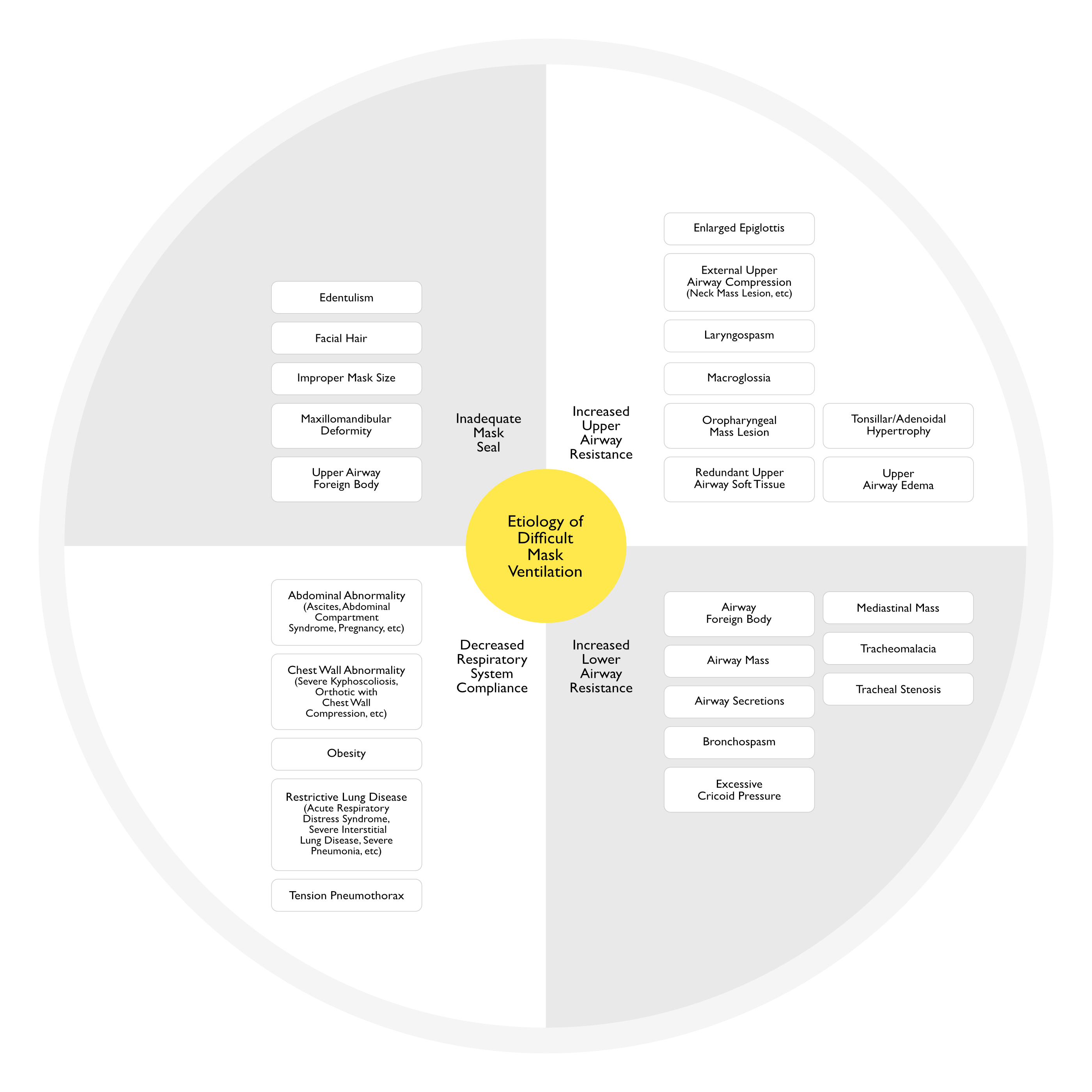
Difficult Mask Ventilation
General Comments
Difficult Mask Ventilation Occurs in Approximately 5% of Adults (Anesthesiology, 2000) [MEDLINE] and (Anesthesiology, 2006) [MEDLINE]
Difficult Mask Ventilation is Associated with Difficult Intubation
Difficult Intubation Occurs in 30% of Patients with Difficult Mask Ventilation, as Compared to Only 8% of Patients without Difficult Mask Ventilation (Anesthesiology, 2000) [MEDLINE]
Difficult Mask Ventilation is Associated with a “Can’t Intubate, Can’t Ventilate” Scenario
Predictors of Difficult Mask Ventilation: the presence of two of these factors had a 72% sensitivity and 73% specificity (Anesthesiology, 2000) [MEDLINE] and (Anesthesiology, 2006) [MEDLINE]
Age >55 y/o: age is associated with increased pharyngeal resistance to airflow (from choanae to epiglottis) in men, but not in women
BMI >26 kg/m2: obesity is associated with decreased posterior airway space behind the base of the tongue, impaired airway patency during sleep, and is a risk factor for OSA
Lack of Teeth
Presence of Beard
History of Snoring
Limited Mandibular Protrusion
Etiology of Difficult Mask Ventilation (Respir Care, 2015) [MEDLINE]
Management of Difficult Bag-Valve-Mask Ventilation the Edentulous Patient
Reinsert False Teeth in the Edentulous Patient to Improve Mask Seal (Anesth Analg, 2007) [MEDLINE]
Changing Location of the Lower Edge of the Mask to Between the Lower Lip and the Alveolar Ridge May Improve Mask Seal in the Edentulous Patient (Anesthesiology, 2010) [MEDLINE]
Preparation for Intubation
Hemodynamic Optimization
Since Sedative Medications and Positive-Pressure Ventilation Can Both Induce Hypotension During and/or Soon After Endotracheal Intubation, Attention Should Be Paid to Intravenous Volume Resuscitation Prior to Intubation
In Most Cases, Preemptive Intravenous Volume Resuscitation and Vasopressors Can Be Utilized Prior to and/or During Endotracheal Intubation to Mitigate or Completely Avoid the Occurrence of Intubation-Associated Hypotension
Body Positioning for Intubation
Body Positions
Sniffing Position: classical position used for intubation
Atlanto-Occipital Extension with Head Elevation of 3-7 cm
Ramped Position
Use of Towels/Blankets to Elevate the Head and Upper Torso, Creating Horizontal Alignment of the External Auditory Meatus with the Sternal Notch
Clinical Efficacy
Comparison of Sniff and Ramped Positions for Laryngoscopic Intubation in Morbidly Obese Patients (Obes Surg, 2004) [MEDLINE]: randomized trial (n = 60)
Sniffing Position was Achieved by Placing a Firm 7 cm Cushion Under the Patient’s Head: this raised the occiput a standard distance from the table
Ramped Position was Achieved by Placing Blankets Under the Upper Body and Head to Horizontally Align the External Auditory Meatus with the Sternal Notch
Ramped Position Significantly Improved the Laryngeal View, as Compared to the Standard Sniffing Position
Study of Head-Elevated Position During Endotracheal Intubation in Decreasing Airway-Related Complications (Anesth Analg, 2016) [MEDLINE]: retrospective study (n = 528)
Back-Up, Head-Elevated Position During Endotracheal Intubation Decreased Airway-Related Complications (Aspiration, Difficult Intubation, Hypoxemia, Esophageal Intubation), as Compared to Supine Positioning
Multicenter, Randomized Trial of Ramped Position vs Sniffing Position During Endotracheal Intubation of Critically Ill Adults (Chest, 2017) [MEDLINE]: average BMI = 27
Ramped Position Did Not Improve Oxygenation During Endotracheal Intubation of Critically Ill Adults, as Compared to the Sniffing Position
Ramped Position May Worsen the Glottic View and Increase the Number of Laryngoscopy Attempts Required for Successful Intubation
Randomized Clinical Trial Comparing the Sniffing and Neutral Position Using Channelled (KingVision) and Non-Channelled (C-MAC®) Video Laryngoscopes (Anaesthesia, 2018) [MEDLINE]
No Significant Difference in the Ease of Intubation Between the Sniffing and the Neutral Position When Using the KingVision and the C-MAC Video Laryngoscopes
Comprehensive Systematic Review of Randomized Trials for Endotracheal Intubation in Critically Ill Patients (Crit Care, 2018) [MEDLINE]: n = 22 trials
Ramped Position Increased the Number of Intubation Attempts (Although Only 1 Trial was Reviewed)
Systematic Review and Meta-Analysis of Ramped (Inclined) Positioning for Endotracheal Intubation (Emerg Med J, 2022) [MEDLINE]: n = 18,371 intubations (from 5,113 studies)
No Statistically Significant Difference in the Primary Outcome of First-Pass Success Rate (Relative Risk 1.02; 95% CI: 0.98-1.05) or Secondary Outcomes of Esophageal Intubation, Glottic View, Hypotension, Hypoxemia, Mortality or Peri-Intubation Arrest
Likewise, there were No Statistically Significant Differences in Any of the Outcomes in Predefined Subgroup Analyses of Randomized Controlled Trials, Intubations in Acute Settings or Intubations Performed with >45 Degrees of Incline
Overall Quality of Evidence was Very Low/Low for Most Outcomes
Preparation of the Endotracheal Tube (ETT)
Purposes of the Endotracheal Tube
Maintenance of Airway Patency in in Patient Who Cannot Do So Independently
Maintenance of Upper Airway Patency During Positive-Pressure Mechanical Ventilation
While Negative-Pressure Ventilation May Induce Upper Airway Collapse (Requiring an Endotracheal Tube to Maintain Airway Patency with Large Negative Airway Pressures), Maintenance of Airway Patency During Positive-Pressure Ventilation is Also Critically Important
Pulmonary Toilet
Maintenance of the Ability to Therapeutically Clear Airways (i.e. Suctioning of Secretions and Blood)
Choice of Endotracheal Tube
Standard Single-Lumen Endotracheal Tube
Rusch Endotracheal Tube
Rusch Endotracheal Tube is a Reinforced Tube
Commonly Used When Flexibility of the Endotracheal Tube is Desired without Compromise of Tube Patency (Either During Intubation or Following Intubation During a Surgical Procedure)
Commonly Used for Surgical Procedures Involving the Upper Airway, Cervical Spine, etc
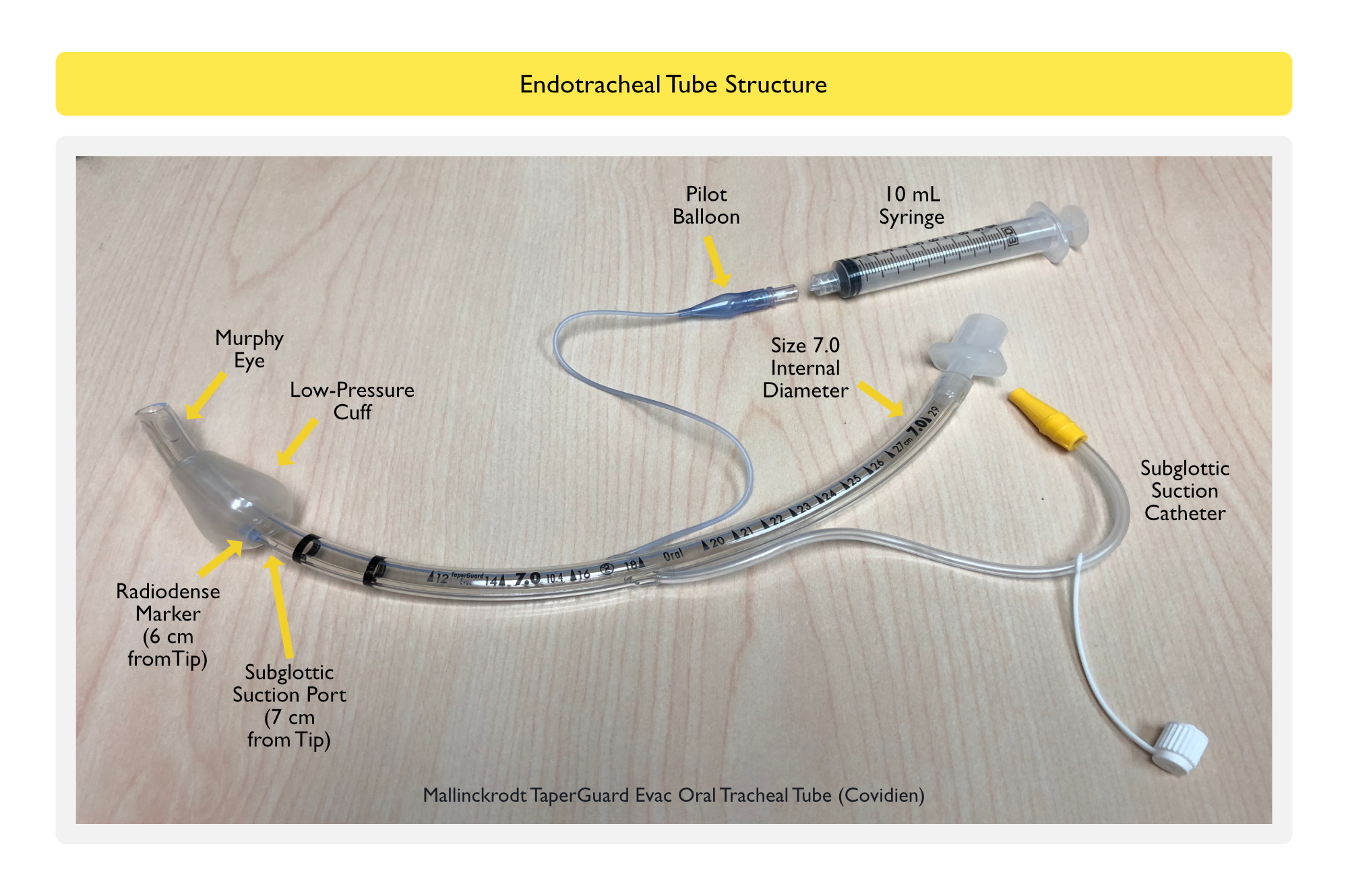
Subglottic Suction Port Endotracheal Tube
Subglottic Suction Port Endotracheal Tubes are Designed to Allow Suctioning of Secretions from Above the Endotracheal Tube Cuff and Theoretically Decrease the Risk of Ventilator-Associated Pneumonia (VAP) (see Hospital-Acquired Pneumonia and Ventilator-Associated Pneumonia)
Dual-Lumen Endotracheal Tube May Be Used for Single-Lung Isolation/Ventilation (During Cardiothoracic Surgery, for the Management of Severe Hemoptysis, etc)
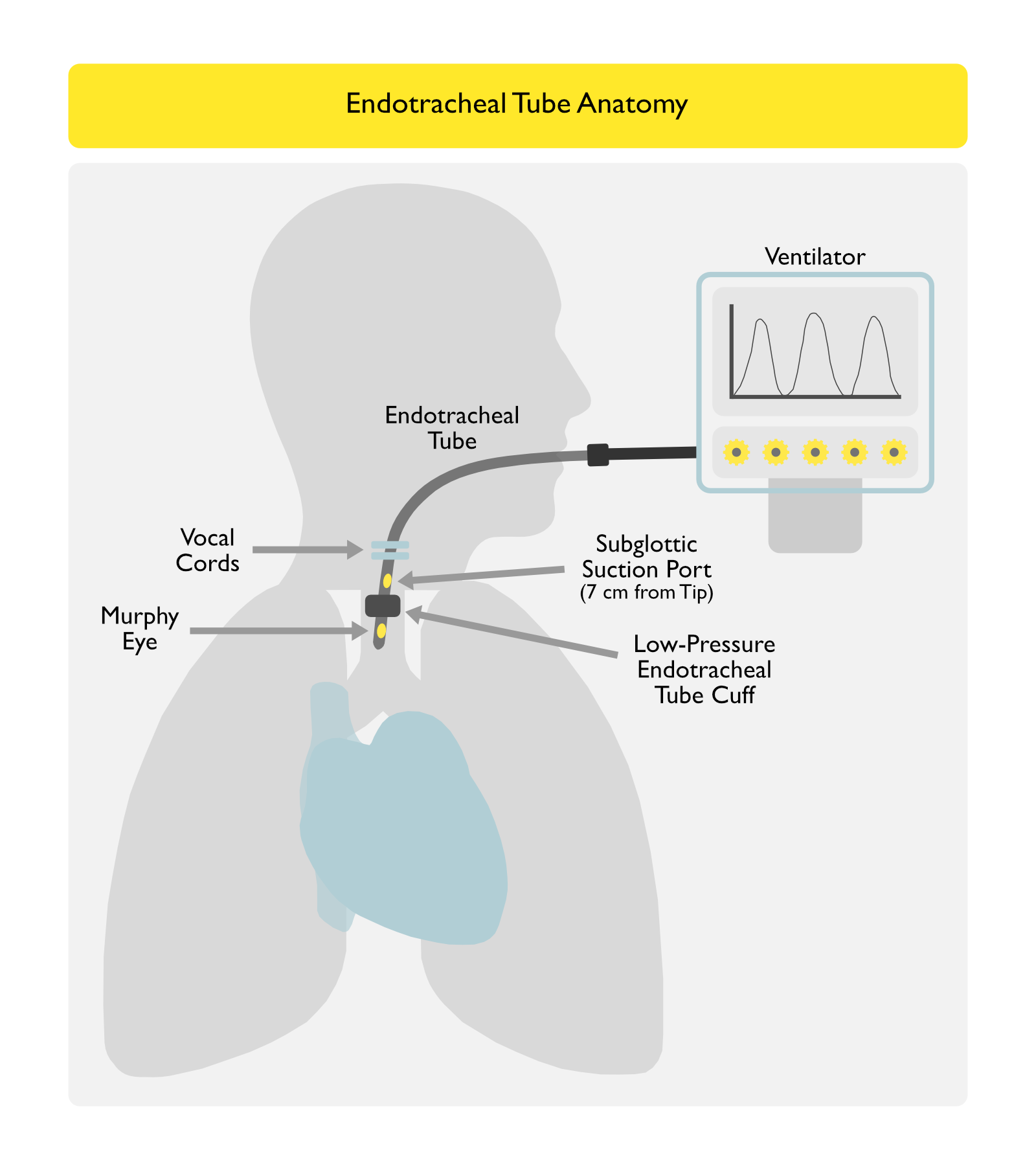
Structure of the Endotracheal Tube
Anatomic Relationships of the Endotracheal Tube
Physical Preparation of the Endotracheal Tube
Push Top Endotracheal Tube Connector Piece Firmly into the Endotracheal Tube: this is important since insertion of this piece deeper into the endotracheal tube after intubation can be difficult in some cases
Determine if Stylet Will Be Utilized (and if it Should Be Loaded in the Endotracheal Tube)
Standard Aluminum Stylet
Gum Elastic Bougie with Bent Tip
Stiff Metal Stylet (Glidescope Stylet, etc)
Check Endotracheal Tube Cuff Balloon for Integrity: keep the 10 mL syringe available for cuff inflation after intubation
Lubricate Endotracheal Tube Cuff: avoid lubricating endotracheal tube above the cuff, as this can make handling of the tube difficult during intubation
Assure that a Colorimetric Carbon Dioxide Detector is Present
Confirmation of Functioning Suction Set-Up
Yankauer Suction Set-Up Should Be Tested for Function: in some cases with large volumes of anticipated orla material, a second suction set-up should be prepared
Preparation of Backup Airway Management Devices and Personnel with Airway Expertise
Prior to Intubation, Other Airway Devices (Including Bronchoscope, Laryngeal Mask Airway, etc) and Personnel Should Be Readily Available, Should Difficulty Be Encountered During Intubation
Pre-Intubation Airway Assessment is Crucial to Predict the Risk of a Difficult Airway Prior to Intubation, Triggering More Robust Advance Preparation
However, Since a Difficult Intubation Can Be Encountered Unexpectedly in Some Cases, Routine Preparation of Other Equipment is Always Advisable
Confirmation of Adequate Intravenous Access and Intravenous Fluids
Ensure that Patient Has at Least Two Functional Intravenous Lines in Place
Adequate Intravenous Access is Critical to Deliver Sedative and Paralytic Medications Which are Standardly Used to Facilitate Endotracheal Intubation
Loss of Functional Intravenous Lines During the Course of Endotracheal Intubation Can Significantly Delay the Performance of Rapid Sequence Intubation, Resulting in Undesired Prolonged Bag-Valve-Mask Ventilation and Gastric Insufflation
Intravenous Fluids and Vasopressors Should Be Available to Manage Post-Intubation Hypotension
Confirmation of Preparation of Sedative and Paralytic Medications for Intubation
In Addition to Below, Additional Sedatives (Propofol Drip, etc) May Be Desired to Manage Sedation After Intubation: this is critical when a short-acting sedative (such as etomidate) is used in conjunction with a long-acting paralytic agent (such as rocuronium, etc)
Team-Oriented Approach with Protocol/Checklist/Cognitive Aids
Prospective Multicenter Study of a Bundle to Decrease Endotracheal Intubation Complications in the ICU (Intensive Care Med, 2010) [MEDLINE]: n = 244 intubations
Bundle Components
Capnography
Cricoid Pressure
Intravenous Fluid Loading
Preoxygenation with Noninvasive Positive Pressure Ventilation
Preparation and Early Administration of Sedation and Vasopressor Use if Needed
Presence of two operators, rapid sequence induction
Protective Ventilation
Intubation Management Protocol Decreased Immediate Severe Life-Threatening Complications (Cardiac Arrest or Death, Severe Cardiovascular Collapse, and Hypoxemia Occurring within 60 min of Endotracheal Intubation of ICU Patients
Single-Center, Prospective Observational Trial of Team Approach, Mandatory Checklist, Use of Crew Resource Management Tactics, and Postevent Debriefing to Improve the Quality of Endotracheal Intubation by Pulmonary/Critical Care Fellows (J Intensive Care Med, 2011) [MEDLINE]: n- 101 intubations
Emergency Endotracheal Intubation Could Be Performed by Pulmonary/Critical Care Fellows with Safety Comparable to Other Providers
Literature Review of Cognitive Aids in the Assistance of Anesthetic Management (Anesth Analg, 2013) [MEDLINE]
Cognitive Aids are Prompts (Posters, Flowcharts, Checklists, or Mnemonics) Designed to Assist Users Complete a Task or Series of Tasks _ Ten Studies Using Simulation Suggested that Technical Performance Improved with the Use of Cognitive Aids in Some Anesthetic Emergencies (Malignant Hyperthermia, Cardiopulmonary Resuscitation, and Airway Management)
Cognitive Aids Would Benefit from More Extensive Simulation-Based Usability Testing Before Use
Study of Implementation of a Difficult Airway Response Team (DART) at the Johns Hopkins Hospital (Anesth Analg, 2015) [MEDLINE]
DART is a Comprehensive Program for Improving Difficult Airway Management
Between July, 2008-June, 2013, DART Managed 360 Adult Difficult Airway Events, Comprising 8% of All Code Blue Activations
Predisposing Patient Factors Included BMI >40, History of Head and Neck Tumor, Prior Difficult Intubation, Cervical Spine Injury, Airway Edema, Airway Bleeding, and Previous or Current Tracheostomy
There Were No Airway Management Related Deaths, Sentinel Events, or Malpractice Claims in Adult Patients Managed by DART
Study of the Vortex Tool for Emergency Airway Management in “Can’t Intubate, Can’t Oxygenate” (CICO) Scenarios (Br J Anaesth, 2016) [MEDLINE]
The Vortex is Flexible Enough for the Same Tool to Be Applied to Any Circumstance in which Airway Management Takes Place, Independent of Context, Patient Type, or the Intended Airway Device
Multicenter Randomized Trial of a Checklist for Endotracheal Intubation of Critically Ill Adults (Chest, 2018) [MEDLINE]: n = 262
The Verbal Performance of a Written, Preprocedure Checklist Did Not Increase the Lowest Arterial Oxygen Saturation or Lowest Systolic Blood Pressure During Endotracheal Intubation of Critically Ill Adults, as Compared to Usual Care
Comprehensive Systematic Review of Randomized Trials for Endotracheal Intubation in Critically Ill Patients (Crit Care, 2018) [MEDLINE]
No Effect was Found for Use of a Pre-Intubation Checklist (Although Only 1 Trial was Reviewed)
Review of Difficult Airway Management Team (DART Experience at the Johns Hopkins Hospital (Crit Care Clin, 2018) [MEDLINE]
Article Details the Lessons Learned and Recommendations for Initiating a DART Program
Study of Simulation-Based Airway Management Training of Critical Care Fellows Using a Checklist (Chest 2020) [MEDLINE]
Simulation-Based Airway Management Training of Early Critical Care Fellows (Using a Checklist) Transferred Well to Real-Life Critical Care Airway Management Skills Later in Fellowship
References
General
Safe intrahospital transport of critically ill ventilator-dependent patients. Chest 1989; 96:631-635 [MEDLINE]
Airway considerations in the management of patients requiring long-term endotracheal intubation. Anesth Analg. 1992;74(2):276 [MEDLINE]
Unplanned extubations in the adult intensive care unit. Am J Respir Crit Care Med 1998; 157:1131-1137 [MEDLINE]
Death and other complications of emergency airway management in critically ill adults. Anesthesiology 1995; 82:367-376 [MEDLINE]
Bedside procedures: solutions to the pitfalls of intrahospital transport. Crit Care Clin 2000; 16:1-6 [MEDLINE]
Difficult airway management in the emergency department. J Emerg Med. 2002 Jan;22(1):31-48 [MEDLINE]
Clinical practice guidelines for sustained neuromuscular blockade in the adult critically ill patient. Crit Care Med. 2002 Jan;30(1):142-56 [MEDLINE]
Towards evidence based emergency medicine: best BETs from the Manchester Royal Infirmary. Colourimetric CO(2) detector compared with capnography for confirming ET tube placement. Emerg Med J 2003: 20: 265-266 [MEDLINE]
The effectiveness of out-of-hospital use of continuous end-tidal carbon dioxide monitoring on the rate of unrecognized misplaced intubation within a regional emergency medical services system. Ann Emerg Med 2005; 45:497-503 [MEDLINE]
Clinical review: management of difficult airways. Crit Care 2006;10:243. doi: 10.1186/cc5112 [MEDLINE]
2010 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Part 8: adult advanced cardiovascular life support. Circulation 2010; 122(18 Suppl 3):S729-S767 [MEDLINE]
Airway management in critically ill patients. Lung 2011; 189:181-192 [MEDLINE]
Emergency airway management: the difficult airway. Emerg Med Clin North Am 2012; 30:401-420 [MEDLINE]
Practice guidelines for management of the difficult airway: an updated report by the American Society of Anesthesiologists Task Force on Management of the Difficult Airway. Anesthesiology. 2013;118:251–270 [MEDLINE]
The effect of body mass index on intubation success rates and complications during emergency airway management. Intern Emerg Med. 2013 Feb;8(1):75-82. Epub 2012 Nov 25 [MEDLINE]
Heated humidified high-flow nasal oxygen in adults: mechanisms of action and clinical implications. Chest. 2015;148(1):253–261 [MEDLINE]
Endotracheal intubation in the ICU. Crit Care. 2015;19:258 [MEDLINE]
Experts’ guidelines of intubation and extubation of the ICU patient of French Society of Anaesthesia and Intensive Care Medicine (SFAR) and French-speaking Intensive Care Society (SRLF) : In collaboration with the pediatric Association of French-speaking Anaesthetists and Intensivists (ADARPEF), French-speaking Group of Intensive Care and Paediatric emergencies (GFRUP) and Intensive Care physiotherapy society (SKR). Ann Intensive Care. 2019 Jan 22;9(1):13. doi: 10.1186/s13613-019-0483-1 [MEDLINE]
Airway Management in Critical Illness: An Update. Chest. 2020 Apr;157(4):877-887. doi: 10.1016/j.chest.2019.10.026 [MEDLINE]
Simulation Training for Critical Care Airway Management: Assessing Translation to Clinical Practice Using a Small Video-Recording Device. Chest 2020 Jul;158(1):272-278. doi: 10.1016/j.chest.2020.01.047 [MEDLINE]
2022 American Society of Anesthesiologists Practice Guidelines for Management of the Difficult Airway. Anesthesiology. 2022 Jan 1;136(1):31-81. doi: 10.1097/ALN.0000000000004002 [MEDLINE]
Indications
Part 7: Adult Advanced Cardiovascular Life Support: 2015 American Heart Association Guidelines Update for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation. 2015 Nov 3;132(18 Suppl 2):S444-64. doi: 10.1161/CIR.0000000000000261 [MEDLINE]
Effect of Bag-Mask Ventilation vs Endotracheal Intubation During Cardiopulmonary Resuscitation on Neurological Outcome After Out-of-Hospital Cardiorespiratory Arrest: A Randomized Clinical Trial. JAMA 2018; 319:779 [MEDLINE]
Effect of a Strategy of a Supraglottic Airway Device vs Tracheal Intubation During Out-of-Hospital Cardiac Arrest on Functional Outcome: The AIRWAYS-2 Randomized Clinical Trial. JAMA 2018; 320:779 [MEDLINE]
Effect of a Strategy of Initial Laryngeal Tube Insertion vs Endotracheal Intubation on 72-Hour Survival in Adults With Out-of-Hospital Cardiac Arrest: A Randomized Clinical Trial. JAMA 2018; 320:769 [MEDLINE]
Assessment for Upper Airway Obstruction
A life-saving maneuver to prevent food-choking. JAMA. 1975;234(4):398 [MEDLINE]
Heimlich versus a slap on the back. N Engl J Med. 1979;300(17):990 [MEDLINE]
The choking controversy: critique of evidence on the Heimlich maneuver. Crit Care Med. 1979;7(10):475 [MEDLINE]
Chest compression–an alternative to the Heimlich manoeuver? Resuscitation. 1992;24(1):91 [MEDLINE]
Traumatic rupture of the stomach secondary to Heimlich maneuver. Am J Emerg Med. 1993;11(6):611 [MEDLINE]
Assessment of upper airway anatomy in awake, sedated and anaesthetised patients using magnetic resonance imaging. Anaesth Intensive Care. 1994;22(2):165 [MEDLINE]
Magnetic resonance imaging of the upper airway. Effects of propofol anesthesia and nasal continuous positive airway pressure in humans. Anesthesiology. 1996;84(2):273 [MEDLINE]
Gastric rupture secondary to successful Heimlich manoeuvre. Postgrad Med J. 1998;74(876):609 [MEDLINE]
Airway pressure with chest compressions versus Heimlich manoeuvre in recently dead adults with complete airway obstruction. Resuscitation. 2000;44(2):105 [MEDLINE]
Rupture of the lesser gastric curvature after a Heimlich maneuver. Surg Endosc. 2003;17(9):1495 [MEDLINE]
Part 4: CPR overview: 2010 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation. 2010;122(18 Suppl 3):S676 [MEDLINE]
Part 5: Adult Basic Life Support and Cardiopulmonary Resuscitation Quality: 2015 American Heart Association Guidelines Update for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation. 2015;132(18 Suppl 2):S414 [MEDLINE]
Airway Maneuvers
Resuscitation–opening the airway. A comparative study of techniques for opening an airway obstructed by the tongue. JACEP. 1976;5(8):588 [MEDLINE]
The effect of airway maneuvers on the unstable C1-C2 segment. A cadaver study. Spine (Phila Pa 1976). 1997;22(11):1215 [MEDLINE]
Cervical spine motion during airway management: a cinefluoroscopic study of the posteriorly destabilized third cervical vertebrae in human cadavers. Anesth Analg. 2000;91(5):1274 [MEDLINE]
Effectiveness of the jaw-thrust maneuver in opening the airway: a flexible fiberoptic endoscopic study. ORL J Otorhinolaryngol Relat Spec. 2005;67(1):39 [MEDLINE]
Airway Adjuncts
The nasopharyngeal airway. Assessment of position by fibreoptic laryngoscopy. Anaesthesia. 1993;48(7):575 [MEDLINE]
The nasopharyngeal airway: dispelling myths and establishing the facts. Emerg Med J. 2005;22(6):394 [MEDLINE]
Preintubation Assessment
Limitations of difficult airway prediction in patients intubated in the emergency department. Ann Emerg Med. 2004 Oct;44(4):307-13 [MEDLINE]
Can an Airway Assessment Score Predict Difficulty at Intubation in the Emergency Department? Emerg Med J 2005 Feb;22(2):99-102. doi: 10.1136/emj.2003.008771 [MEDLINE]
The extended Mallampati score and a diagnosis of diabetes mellitus are predictors of difficult laryngoscopy in the morbidly obese. Anesth Analg. 2008 Dec;107(6):1919-23. doi: 10.1213/ane.0b013e31818a9946 [MEDLINE]
Determination of Difficult Intubation in the ED Am J Emerg Med 2009 Oct;27(8):905-10. doi: 10.1016/j.ajem.2008.07.003 [MEDLINE]
Feasibility of the preoperative Mallampati airway assessment in emergency department patients. J Emerg Med. 2010 Jun;38(5):677-80. doi: 10.1016/j.jemermed.2008.12.019 [MEDLINE]
High STOP-Bang score indicates a high probability of obstructive sleep apnoea. British Journal of Anaesthesia 108 (5): 768–75 (2012) [MEDLINE]
Early identification of patients at risk for difficult intubation in the intensive care unit: development and validation of the MACOCHA score in a multicenter cohort study. Am J Respir Crit Care Med. 2013 Apr 15;187(8):832-9. doi: 10.1164/rccm.201210-1851OC [MEDLINE]
The MACOCHA score is feasible to predict intubation failure of nonanesthesiologist intensive care unit trainees. J Crit Care. 2015 Oct;30(5):876-80. doi: 10.1016/j.jcrc.2015.04.118 [MEDLINE]
Prospective validation of the modified LEMON criteria to predict difficult intubation in the ED. Am J Emerg Med. 2015 Oct;33(10):1492-6. doi: 10.1016/j.ajem.2015.06.038 [MEDLINE]
The diagnostic validity of clinical airway assessments for predicting difficult laryngoscopy using a grey zone approach. J Int Med Res. 2016 Aug;44(4):893-904. doi: 10.1177/0300060516642647 [MEDLINE]
Correlation Between Modified LEMON Score and Intubation Difficulty in Adult Trauma Patients Undergoing Emergency Surgery. World J Emerg Surg 2018 Jul 24;13:33. doi: 10.1186/s13017-018-0195-0. eCollection 2018 [MEDLINE]
Will This Patient Be Difficult to Intubate?: The Rational Clinical Examination Systematic Review. JAMA. 2019 Feb 5;321(5):493-503. doi: 10.1001/jama.2018.21413 [MEDLINE]
Bag-Valve-Mask Ventilation
Simultaneous aortic, jugular bulb, and right atrial pressures during cardiopulmonary resuscitation in humans. Insights into mechanisms. Circulation. 1989;80(2):361 [MEDLINE]
Comparison of self-inflating bags with anesthesia bags for bag-mask ventilation in the pediatric emergency department. Pediatr Emerg Care. 1997;13(5):312 [MEDLINE]
Prediction of difficult mask ventilation. Anesthesiology 2000;92:1229–1236 [MEDLINE]
Hyperventilation-induced hypotension during cardiopulmonary resuscitation. Circulation. 2004;109(16):1960 [MEDLINE]
Death by hyperventilation: a common and life-threatening problem during cardiopulmonary resuscitation. Crit Care Med. 2004;32(9 Suppl):S345 [MEDLINE]
Incidence and predictors of difficult or impossible mask ventilation. Anesthesiology 2006;105:885–891 [MEDLINE]
The effect of leaving dentures in place on bag-mask ventilation at induction of general anesthesia. Anesth Analg. 2007;105(2):370 [MEDLINE]
A two-handed jaw-thrust technique is superior to the one-handed “EC-clamp” technique for mask ventilation in the apneic unconscious person. Anesthesiology. 2010;113(4):873 [MEDLINE]
Face mask ventilation in edentulous patients: a comparison of mandibular groove and lower lip placement. Anesthesiology. 2010;112(5):1190 [MEDLINE]
Efficacy of facemask ventilation techniques in novice providers. Clin Anesth. 2013 May;25(3):193-7 [MEDLINE]
Optimizing Mask Ventilation: Literature Review and Development of a Conceptual Framework. Respir Care. 2015 Dec;60(12):1834-40. doi: 10.4187/respcare.04183 [MEDLINE]
Preparation for Intubation
Body Position
Analysis of the forces and position required for direct laryngoscopic exposure of the anterior vocal folds. Ann Otol Rhinol Laryngol. 1999;108(8):715 [MEDLINE]
Head and neck elevation beyond the sniffing position improves laryngeal view in cases of difficult direct laryngoscopy. J Clin Anesth. 2002;14(5):335 [MEDLINE]
Head-elevated laryngoscopy position: improving laryngeal exposure during laryngoscopy by increasing head elevation. Ann Emerg Med. 2003;41(3):322 [MEDLINE]
Laryngoscopy and morbid obesity: a comparison of the “sniff” and “ramped” positions. Obes Surg. 2004;14(9):1171 [MEDLINE]
Head-Elevated Patient Positioning Decreases Complications of Emergent Tracheal Intubation in the Ward and Intensive Care Unit. Anesth Analg. 2016 Apr;122(4):1101-7 [MEDLINE]
A Multicenter, Randomized Trial of Ramped Position vs Sniffing Position During Endotracheal Intubation of Critically Ill Adults. Chest. 2017 Oct;152(4):712-722. doi: 10.1016/j.chest.2017.03.061 [MEDLINE]
A randomised clinical trial comparing the ‘sniffing’ and neutral position using channelled (KingVision® ) and non-channelled (C-MAC® ) videolaryngoscopes. Anaesthesia. 2018 Jul;73(7):847-855. doi: 10.1111/anae.14289 [MEDLINE]
Effect of inclined positioning on first-pass success during endotracheal intubation: a systematic review and meta-analysis. Emerg Med J. 2022 Apr 7;emermed-2021-211968. doi: 10.1136/emermed-2021-211968 [MEDLINE]
Team-Oriented Approach/Protocol/Check List
An intervention to decrease complications related to endotracheal intubation in the intensive care unit: a prospective, multiple-center study. Intensive Care Med. 2010 Feb;36(2):248-55. doi: 10.1007/s00134-009-1717-8 [MEDLINE]
A program to improve the quality of emergency endotracheal intubation. J Intensive Care Med. 2011 Jan-Feb;26(1):50-6. doi: 10.1177/0885066610384070 [MEDLINE]
The use of cognitive aids during emergencies in anesthesia: a review of the literature. Anesth Analg. 2013 Nov;117(5):1162-71. doi: 10.1213/ANE.0b013e31829c397b [MEDLINE]
Difficult airway response team: a novel quality improvement program for managing hospital-wide airway emergencies. Anesth Analg. 2015 Jul;121(1):127-39. doi: 10.1213/ANE.0000000000000691 [MEDLINE]
The Vortex: a universal ‘high-acuity implementation tool’ for emergency airway management. Br J Anaesth. 2016 Sep;117 Suppl 1:i20-i27. doi: 10.1093/bja/aew175 [MEDLINE]
A Multicenter Randomized Trial of a Checklist for Endotracheal Intubation of Critically Ill Adults. Chest. 2018 Apr;153(4):816-824. doi: 10.1016/j.chest.2017.08.1163 [MEDLINE]
A Decade of Difficult Airway Response Team: Lessons Learned from a Hospital-Wide Difficult Airway Response Team Program. Crit Care Clin. 2018 Apr;34(2):239-251. doi: 10.1016/j.ccc.2017.12.008 [MEDLINE]