Ventilation Mode Employing the Use of High Respiratory Rates
Techniques
General Comments: all techniques utilize respiratory rates >100 breaths/min
Conventional Mechanical Ventilation with Small Tidal Volumes and Rapid Respiratory Rates
Chest Wall Oscillation
High-Frequency Percussive Ventilation (HFPV): flow-regulated, pressure-limited, and time-cycled ventilator that delivers a series of high-frequency small volumes (at 200-900 cycles/min) in a successive stepwise stacking pattern
High-Frequency Jet Ventilation
High-Frequency Oscillation Ventilation (HFOV): most widely used type of high-frequency ventilation used in adult critical care -> delivers a small tidal volume by oscillating a bias gas flow in the airway
Clinical Efficacy
Randomized, Controlled Multicenter Oscillatory Ventilation For Acute Respiratory Distress Syndrome (ARDS) Trial (MOAT) Trial of High-Frequency Oscillation Ventilation (Am J Respir Crit Care Med, 2002) [MEDLINE]
While the Study was Not Powered to Evaluate Mortality Differences, But an Insignificant Trend Toward Improved Overall 30-Day Mortality Rate in the High-Frequency Oscillation Ventilation Group, as Compared with the Conventional Ventilation Group (37% vs 52% 30-Day Mortality, p=0.098)
There Were No Significant Difference Between Groups in New or Worsening Barotrauma, Endotracheal Tube Obstruction, or Adverse Hemodynamic Effects
Retrospective Chart Review of High-Frequency Oscillation Ventilation for Rescue Therapy in Medical-Surgical ICU Patients (Chest, 2004) [MEDLINE]: n = 156
High-Frequency Oscillation Ventilation Had Beneficial Effects on pO2/FIO2 Ratios and Oxygenation Index
30-Day Mortality Rate was 61.7%
Pneumothorax Rate was 21.8%
Canadian Clinical Trials Group OSCILLATE High-Frequency Oscillation Study in Acute Respiratory Distress Syndrome(ARDS) (NEJM, 2013) [MEDLINE]
In Adults with Moderate-to-Severe Acute Respiratory Distress Syndrome (ARDS), Early Application of High-Frequency Oscillation Ventilation (as Compared with a Ventilation Strategy of Low Tidal Volume and High PEEP) Did Not Decrease and May Increase, the In-Hospital Mortality Rate
Recommendations for Patients with Acute Respiratory Distress Syndrome (ARDS) (American Thoracic Society/European Society of Intensive Care Medicine/Society of Critical Care Medicine Clinical Practice Guidelines for Mechanical Ventilation in ARDS) (Am J Respir Crit Care Med, 2017) [MEDLINE]
High Frequency Ventilation is Not Routinely Recommended in Moderate-Severe Acute Respiratory Distress Syndrome(ARDS) (Strong Recommendation, Moderate-High Confidence)
Recommendations for Patients with Acute Respiratory Distress Syndrome (ARDS) Associated with Sepsis (2016 Surviving Sepsis Guidelines; Intensive Care Med, 2017) [MEDLINE]
Ventilation Mode
No Ventilator Mode is Recommended Over Another
However, High-Frequency Oscillation Ventilation is Not Recommended in Adult Patients with Sepsis-Associated Acute Respiratory Distress Syndrome (ARDS) (Strong Recommendation, Moderate Quality of Evidence) (see High-Frequency Ventilation)
British Thoracic Society 2019 Guidelines for the Management of Acute Respiratory Distress Syndrome (ARDS) (BMJ Open Respir Res, 2019) [MEDLINE]
Use of High-Frequency Oscillation Ventilation is Not Recommended in the Management of Patients with Acute Respiratory Distress Syndrome (ARDS) (Grade Recommendation: Strongly Against)
Pressure Assist Control Ventilation (PCV)
Concept
Pressure-Targeted, Time-Cycled Mode
Patient Can Trigger Additional Breaths Above the Set Respiratory Rate (with Each Breath Consisting of a Full Pressure Breath)
Types of Breaths
Pressure Control Breaths: machine triggered
Pressure Assist Breaths: patient triggered
Work of Breathing
Very Low: most of the patient’s work of breathing in this mode (which is generally minimal) involves triggering ventilator-delivered breaths (if the patient is nor triggering any breaths, their work of breathing is effectively zero)
Settings
Respiratory Rate (RR)
Delta P (Driving Pressure): since driving pressure is manually set, tidal volume that occurs will depend on lung/chest wall compliance
PEEP: typically initially set to +5
FIO2: typically initially set to 100% FIO2
Monitor
Tidal Volume (VT)
Advantages
Assuming No Change in Lung/Chest Wall Compliance, Provides Guaranteed Delivery of the Desired Minute Ventilation (Due to a Set Driving Pressure and Set Respiratory Rate): this is useful if the patient is heavily sedated/paralyzed or apneic for other reasons
Disadvantages
If Lung/Chest Wall Compliance Decreases During the Course of Ventilation (Due to Hemothorax, Pneumothorax, Pulmonary Edema), Tidal Volume Will Decrease: for this reason, tidal volumes need to be monitored closely in this mode (with ventilator alarms set accordingly)
Recommendations for Patients with Acute Respiratory Distress Syndrome Associated with Sepsis (2016 Surviving Sepsis Guidelines; Intensive Care Med, 2017) [MEDLINE]
No Ventilator Mode is Recommended Over Another for Mechanical Ventilation in Patients with Sepsis
Rationale
Peak Inspiratory Pressure is Generally Lower Than with Volume-Cycled Ventilation: this is due to the flow pattern used with pressure control ventilation
However, GIven the Same Tidal Volume, the Plateau Pressure is the same for Pressure Control Ventilation as it is for Volume-Cycled Ventilation
Improved Patient-Ventilatory Synchrony with PCV: although this is controversial
Improved Gas Exchange with PCV
Increased Mean Airway Pressure
Lower End-Inspiratory Flow Rates
PC has High Initial Flow Rate, Allowing Recruitment of Alveoli with Longer Time Constants
Time Constant of Alveolus (Product of the Resistance x Compliance) Determines How Rapidly the Alveolus Will Fill and Empty
Clinical Efficacy
No Mortality Benefit Has Been Demonstrated for Pressure Control Ventilation
Note that Pressure Control Ventilation was Not Used in the ARDSnet Trial
Note that the Differences Between Pressure Control Ventilation and Modern Volume-Cycled Modes are Probably Negligible (as Many Modern Ventilators Can Be Configured Using a Descending Ramp Flow Waveform
Cochrane Database Systematic Review of Pressure-Controlled vs Volume-Controlled Ventilation in Acute Respiratory Distress Syndrome (ARDS) (Cochrane Database Syst Rev, 2015) [MEDLINE]: n = 1089 (from 3 randomized controlled trials, recruited from 43 intensive care units in Australia, Canada, Saudi Arabia, Spain, and the USA)
For In-Hospital Mortality, Relative Risk with Pressure-Controlled Ventilation was 0.83 (95% CI: 0.67-1.02; Three Trials, 1089 Subjects; Moderate-Quality Evidence), as Compared to Volume-Controlled Ventilation
For 28-Day Mortality, One Study Provided No Evidence of Benefit with the Ventilatory Mode (Relative Risk 0.88 (95% CI: 0.73-1.06; 983 Subjects; Moderate-Quality Evidence)
Currently Available Data were Insufficient to Determine if There was Any Difference Between Pressure-Controlled and Volume-Controlled Ventilation in ARDS
PC-IRV Does Not Appear to Significantly Improve V/Q Matching
Potential Adverse Effects
Elevated Mean Airway Pressure and Auto-PEEP Can Adversely Impact Hemodynamics
Administration
Useful for Refractory Hypoxemia, Despite Adequate PEEP
Typically Requires Sedation and Paralysis, as Most Patients Will Tolerate iInversion of I/E Ratio
Clinical Efficacy
No Mortality Benefit
Recommendations for Patients with Acute Respiratory Distress Syndrome Associated with Sepsis (2016 Surviving Sepsis Guidelines; Intensive Care Med, 2017) [MEDLINE]
Trial of APRV vs Pressure Control Ventilation in Trauma Patients with Acute Respiratory Distress Syndrome (ARDS) (Am J Respir Crit Care Med, 2001) [MEDLINE]: n = 30
APRV was Associated with Increased Respiratory System Compliance, Increased Arterial pO2, Increased Cardiac Index, Increased Oxygen Delivery, Decreased Venous Admixture (QVA/QT), and Decreased Oxygen Extraction
Pressure Control Ventilation was Associated with Decreased Respiratory System Compliance, Decreased Arterial pO2, Decreased Cardiac Index, Decreased Oxygen Delivery, Increased Venous Admixture (QVA/QT), Increased Need for Sufentanil/Midazolam/Norepinephrine/Dobutamine
APRV was Associated with a Shorter Duration of Ventilatory Support and ICU Length of Stay
No Difference in Mortality Rates
Large Randomized Controlled Trial of APRV (Acta Anaesthesiol Scand, 2004) [MEDLINE]: RCT (n = 58) comparing APRV with SIMV with PS (study was terminated early for futility)
No 28-Day or 1-Year Mortality Benefit
No Difference in Ventilator-Free Days at 28 Days
However, Proning was Used in Both Arms and its Effects May Have Overshadowed the Potential Effects of APRV in this Study
Randomized Trial of APRV in Adult Trauma Patients with Respiratory Failure (J Trauma, 2010) [MEDLINE]: n= 63
For Adult Trauma Patients Requiring Mechanical Ventilation >72 hrs, APRV Had a Similar Safety Profile as Low Tidal Volume Ventilation
Trends for APRV Patients to Have Increased Ventilator Days, ICU Length of Stay, and Ventilator-Associated Pneumonia May Be Explained by Initial Higher Acute Physiology and Chronic Health Evaluation II Scores
Retrospective Review of APRV in Trauma Patients (J Trauma Acute Care Surg, 2012) [MEDLINE]
After Controlling for Confounding Factors, APRV Mode Increased the Number of Ventilator Days in Trauma Patients
Animal Study of APRV in Traumatized Pigs with Combined Brain and Lung Trauma (J Trauma Acute Care Surg, 2015) [MEDLINE]
Microdialysis Data Suggested a Trend Toward Increased Cerebral Ischemia Associated with APRV Over Time
Trial of APRV vs Standard Low Tidal Volume Ventilation in Acute Respiratory Distress Syndrome (ARDS) (Intensive Care Med, 2017) [MEDLINE]: n = 148
Early Application of APRV in Acute Respiratory Distress Syndrome (ARDS) Improved Oxygenation, Improved Respiratory System Compliance, Decreased Pplat, Decreased Duration of Mechanical Ventilation, and Decreased the ICU Length of Stay
Prospective Randomized Intermountain Trial of Low Tidal vs Traditional APRV and Volume Control Ventilation Protocols (Crit Care Med, 2018) [MEDLINE]: n = 246 planned (study stopped early because of low enrollment and inability to consistently achieve tidal volumes <6.5 mL/kg in the low tidal volume-airway pressure release ventilation arm)
APRV Often Resulted in Release Volumes >12 mL/kg Despite a Protocol Targeting Low Tidal Volume Ventilation
Current APRV Protocols are Unable to Achieve Consistent and Reproducible Delivery of Low Tidal Volume Ventilation Goals
Systematic Review and Meta-Analysis of APRV in Acute Hypoxemic Respiratory Failure (Ann Intensive Care, 2019) [MEDLINE]: n = 330 (5 RCT’s)
Evidence was Low Quality with Moderate Heterogeneity
APRV was Associated with a Higher Number of Ventilator-Free Days at Day 28
APRV was Associated with a Lower Hospital Mortality Rate
APRV was Not Associated with Any Negative Hemodynamic Impact or Increased Risk of Barotrauma
Recommendations for Patients with Acute Respiratory Distress Syndrome Associated with Sepsis (2016 Surviving Sepsis Guidelines; Intensive Care Med, 2017) [MEDLINE]
No Ventilator Mode is Recommended Over Another
Body Position -> Proning
History
1974: proning was first proposed (Am Rev Respir Dis, 1974) [MEDLINE]
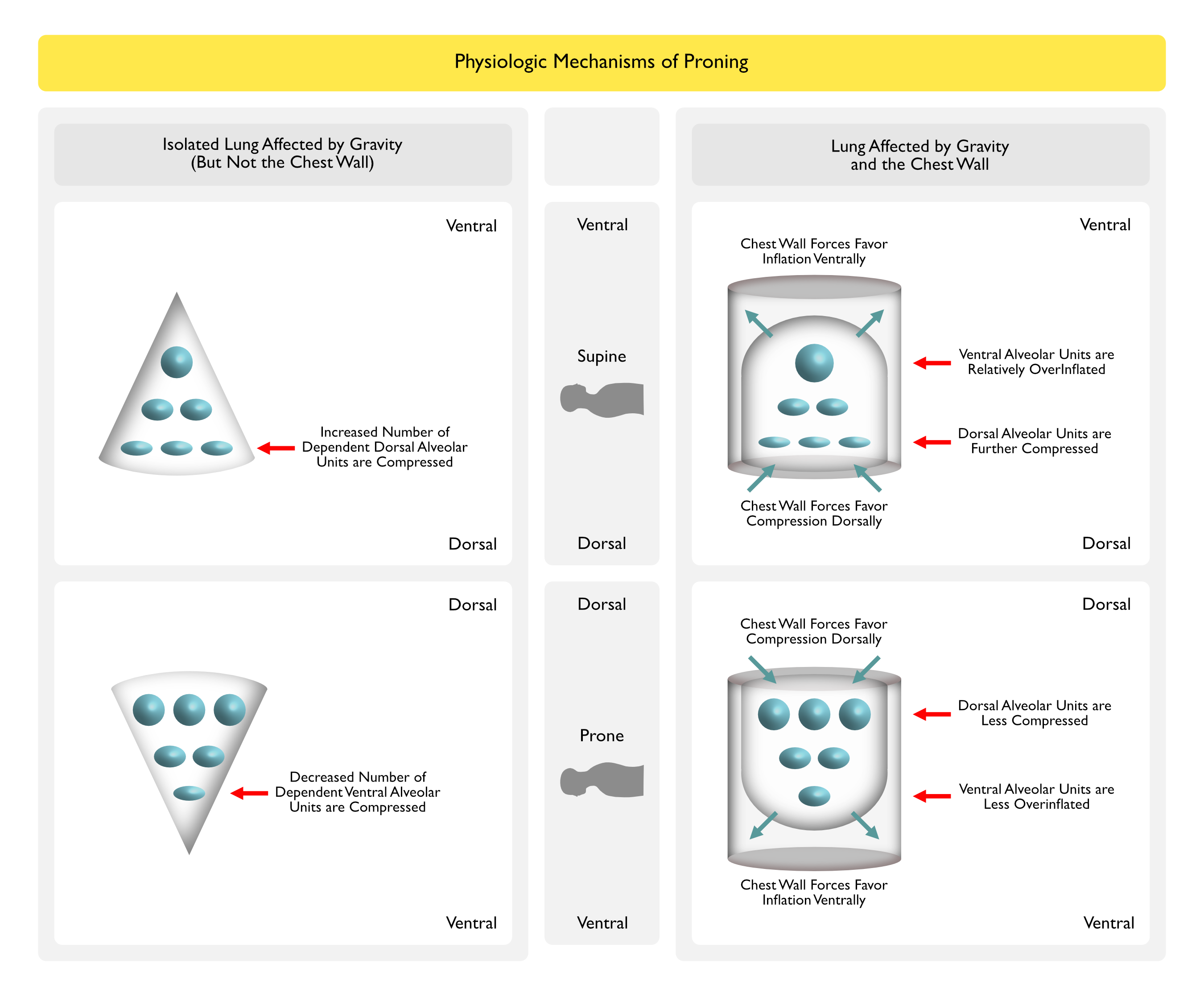
Physiologic Mechanisms
Recruitment of Previously Underventilated Areas (with Minimal Changes in Perfusion), Resulting in Improved V/Q Matching: main mechanism
Decreased Cardiac Compression of Lung Tissue: less lung lies inferior to the heart with patient in the prone position
Decreased Shunt Fraction: due to decreased dependent pleural pressure and decreased pleural pressure gradient
Suggests that Greater Proportion of the Dependent Lung Volume is Above the Closing Volume in the Prone Position
Increased Mobilization of Secretions Toward the Mouth
Recruitment and Stabilization of Dorsal Lung Units
Redistribution of Trans-Lung Forces
Reduction of Supine Gradient of Trans-Lung Pressure
Unknown Aspects of Proning
When to Start Proning
How Long to Continue Proning
Optimal Daily Duration of Proning
Effect on Ventilator-Induced Lung Injury
Technique
Rotoprone Bed
Vollman Proning Device
Practical Application
If Not Using Rotoprone Bed: recommended to execute proning in 2 steps (side first, then prone) to avoid hemodynamic deterioration, dislodgement of lines, etc
Onset of Effect: most of improvement occurs quickly (usually within min)
Timing: can be performed successfully at any time during the course of disease
Duration of Proning: although not entirely clear, periods pf proning >12 hrs are probably necessary to achieve benefit
Repeat Attempts at Proning: proning may improve oxygenation after an initial failure of prior proning
Effect on Gas Exchange: significant improvement in pO2 occurs in 66-75% of patients
Duration of Effect: improvement in oxygenation can persist in some patients when returned to the supine position
Degree of Improvement: not related to the degree of gas exchange impairment
Monitoring of Gas Exchange Efficiency During Proning
pCO2 Better Tracks Gas Exchange Efficiency (Than pO2) and is Probably a Better Reflection of Proning-Induced Recruitment (Crit Care Med, 2003) [MEDLINE]
ALI/ARDS Patients Who Respond to Prone Positioning with Reduction of Their pCO2 Have Improved 28-Day Survival
Proning May Have Lowered the Incidence of Ventilator-Associated Pneumonia
Systematic Review and Meta-Analysis (CMAJ, 2008) [MEDLINE]
Proning Improves Oxygenation and Decreases Risk of Pneumonia
No Mortality Benefit or Impact on Duration of Mechanical Ventilation
Systematic Review and Meta-Analysis (Intensive Care Med, 2010) [MEDLINE]
Proning Improves Mortality Only in Subset of Patients with pO2/FIO2 <100
Proning Increases Risks of Pressure Ulcers, Endotracheal Tube Obstruction, and Chest Tube Dislodgement
French PROSEVA Proning Trial in Severe Acute Respiratory Distress Syndrome (ARDS) (NEJM, 2013) [MEDLINE]: multi-center, randomized, prospective, controlled trial (n = 237 in prone group, n = 229 in supine group) in severe acute respiratory distress syndrome (ARDS) (defined as pO2/FIO2 ratio <150 with FIO2 ≥60% + PEEP ≥5 cm H20 + VT close to 6 ml/kg PBW)
Proning Decreased 28-Day Mortality Rate (16%), as Compared to Supine Group (32.8%)
Proning Decreased 90-Day Mortality Rate (23.6%), as Compared to Supine Group (41%)
No Difference in Complication Rates Between the Groups (Except for Incidence of Cardiac Arrests was Higher in Supine Group)
Systematic Review of Proning in ARDS in Adults (Cochrane Database Syst Rev, 2015) [MEDLINE]
Proning Had No Benefit or Harm
However, the Subgroups with Early Implementation of Proning, Prolonged Proning, and Severe Hypoxemia at Study Entry Demonstrated Mortality Benefit with Proning
Complication of Tracheal Obstruction was Increased with Proning
Small Study of the Effect of Proning on Respiratory Effort in Acute Respiratory Distress Syndrome (Am J Respir Crit Care Med, 2021) [MEDLINE]: n = 12
Proning Improved Oxygenation, Decreased Dynamic Lung Stress, and Decreased Spontaneous Inspiratory Effort (Despite Matched Levels of Sedation)
Improved Oxygenation in Prone Position May Have Decreased Respiratory Drive
Proning is Known to Increase End-Expiratory Lung Volume (and the Force Generated by Diaphragmatic Contraction is Linearly Decreased as Lung Volume is Increased)
Study of the Ability of Chest CT Findings to Predict Proning Response in Moderate-Severe Acute Respiratory Distress Syndrome (ARDS) (BMC Pulm Med, 2022) [MEDLINE]: n = 96
A Greater Difference in the Extent of Consolidation Along the Dependent-Independent Axis (i.e. Median Dorsal-Ventral Difference) on Chest CT Scan was Associated with Subsequent Prone Positioning Oxygenation Response, But Not with the 60-Day Mortality Rate
High Total Ground Glass Opacity Scores (≥15) were Associated with an Increased 60-Day Mortality Rate (Odds Ratio 4.07; 95% Confidence Interval: 1.39-11.89; p = 0.010)
Clinical Efficacy-Timing of Initiation of Proning
Chinese Prospective Observational Study of Timing of Initiation of Proning in Acute Respiratory Distress Syndrome (ARDS) (Crit Care, 2023) [MEDLINE]: n = 57
Oxygenation Significantly Improved After Proning in Early Acute Respiratory Distress Syndrome (ARDS) (157 [121-191] vs. 190 [164-245] mm Hg, p < 0.001), Whereas There was No Significant Change in Persistent Acute Respiratory Distress Syndrome (ARDS) Patients (168 [136-232] vs.177 [155-232] mm Hg, p = 0.10)
Compared to Supine position, Proning Decreased V/Q Mismatch in Early Acute Respiratory Distress Syndrome (ARDS) (28.7 [24.6-35.4] vs 22.8 [20.0-26.8] %, p < 0.001), But Increased V/Q Mismatch in Persistent Acute Respiratory Distress Syndrome (ARDS) (23.8 [19.8-28.6] vs 30.3 [24.5-33.3] %, p = 0.006)
In Early Acute Respiratory Distress Syndrome (ARDS), Proning Significantly Decreased Shunt in the Dorsal Region and Dead Space in the Ventral Region
In Persistent Acute Respiratory Distress Syndrome (ARDS), Proning Increased Global Shunt
A Significant Correlation was Found Between Duration of Acute Respiratory Distress Syndrome (ARDS) Onset to Proning and the Change in V/Q Distribution (r = 0.54, p < 0.001)
Clinical Efficacy-Implementation of Proning
Qualitative Study of the Implementation of Proning in the Intensive Care Unit During the COVID-19 Pandemic (Ann Am Thorac Soc, 2022) [MEDLINE]
ICU Clinicians Reported that During the COVID-19 Pandemic, Proning is Viewed as Standard Early Therapy for COVID-Associated ARDS, Rather than as a Salvage Therapy for Refractory Hypoxemia
With Experience with Proning, Clinicians Gained Increased Comfort with Proning and Now View Proning as a Low-Risk High-Benefit Intervention
Within the ICU, Adequate Trained Staffing, Increased Team Agreement Around Proning, and the Availability of Specific Equipment (to Limit Pressure Injuries, etc Facilitated Greater Proning Use
Hospital Level Supports Included Proning Teams, Centralized Educational Resources Specific to the Management of COVID-19 (Including Proning Recommendations), and an Electronic Medical Record Proning Order
Important Proning Implementation Processes Included Informal Dissemination of Best Practices Through On-the-Job Education and Team Interactions During Routine Bedside Care
Clinical Efficacy-Patient Directed Proning
Non-Blinded Pragmatic Randomized Controlled Trial of Patient-Directed Proning in Non-Intubated Acute Respiratory Distress Syndrome (ARDS) Due to COVID-19 (Ann Am Thorac Soc, 2021) [MEDLINE]: n = 30
Adherence to Patient-Directed Proning was Very Low
Unexpectedly, Patient-Directed Proning Did Not Improve Oxygenation
There was No Change in pO2/FIO2 Ratio at 72 hrs (Prone -80.1; 95% CI: -138.8 to -21.4 vs Usual Care -18.2; 95% CI: -63.0 to 26.5, p = 0.077)
International Expert Guidelines on the Use of Proning in COVID-19-Associated Acute Hypoxemic Respiratory Failure (J Crit Care, 2023) [MEDLINE]
Awake Proning is Recommended in Patients with COVID-19 Receiving High-Flow Oxygen or Noninvasive Positive-Pressure Ventilation
Due to Lack of Evidence from Randomized Controlled Trials, There were No Recommendations on the Use of Awake Proning in COVID-19 Patients Supported with Conventional Oxygen Therapy
Clinical Efficacy-Proning During Venovenous Extracorporeal Membrane Oxygenation (VV-ECMO)
PRONECMO Trial of Proning During Venovenous Extracorporeal Membrane Oxygenation (VV-ECMO) (JAMA, 2023) [MEDLINE] : n = 170
Within 60 Days of Enrollment, 44% of Patients Had Successful Venovenous Extracorporeal Membrane Oxygenation (VV-ECMO) Weaning in the Prone Venovenous Extracorporeal Membrane Oxygenation (VV-ECMO) Group, as Compared to 44% in the Supine Venovenous Extracorporeal Membrane Oxygenation (VV-ECMO) Group (Risk Difference 0.1% [95% CI: -14.9% to 15.2%]; Subdistribution Hazard Ratio, 1.11 [95% CI: 0.71-1.75]; P = 0.64)
Within 90 Days, no Significant Difference was Observed in Venovenous Extracorporeal Membrane Oxygenation (VV-ECMO) Duration (28 vs 32 Days; Difference -4.9 [95% CI: -11.2 to 1.5] Days; P = 0.13), Intensive Care Unit Length of Stay, or 90-Day Mortality (51% vs 48%; Risk Difference 2.4% [95% CI: -13.9% to 18.6%]; P = 0.62)
No Serious Adverse Events were Reported During Proning
Recommendations for Patients with Acute Respiratory Distress Syndrome (ARDS) Associated with Sepsis (2012 Surviving Sepsis Guidelines; Crit Care Med, 2013) [MEDLINE]
Proning is Recommended in Patients with pO2/FiO2 Ratio ≤100 in Sepsis-Associated ARDS (Grade 2B Recommendation)
Recommendations for Patients with Acute Respiratory Distress Syndrome (ARDS) (American Thoracic Society/European Society of Intensive Care Medicine/Society of Critical Care Medicine Clinical Practice Guidelines for Mechanical Ventilation in ARDS) (Am J Respir Crit Care Med, 2017) [MEDLINE]
Proning (for >12 hrs Per Day) is Recommended in Adult Patients with Severe ARDS (Strong Recommendation, Moderate-High Confidence)
Recommendations for Patients with Acute Respiratory Distress Syndrome (ARDS) Associated with Sepsis (2016 Surviving Sepsis Guidelines; Intensive Care Med, 2017) [MEDLINE]
Prone Position is Recommended Over Supine Position in Sepsis-Associated ARDS and pO2/FIO2 Ratio <150 (Strong Recommendation, Moderate Quality of Evidence)
British Thoracic Society 2019 Guidelines for the Management of Acute Respiratory Distress Syndrome (ARDS) (BMJ Open Respir Res, 2019) [MEDLINE]
The Routine Use of Prone Positioning is Not Recommended for All Patients with Acute Respiratory Distress Syndrome (ARDS)
The Use of Prone Positioning is Recommended for ≥12 hrs Per Day in Patients with Moderate/Severe Acute Respiratory Distress Syndrome (ARDS) (P/F Ratio <20 kPa) (Grade Recommendation: Strongly in Favor)
American Heart Association (AHA/American Stroke Association (ASA) Recommendations for Patients with Acute Respiratory Distress Syndrome (ARDS) in the Setting of Aneurysmal Subarachnoid Hemorrhage (SAH) (Stroke, 2023) [MEDLINE]
In Patients with Aneurysmal Subarachnoid Hemorrhage (SAH) Who Develop Severe Acute Respiratory Distress Syndrome (ARDS) and Life-Threatening Hypoxemia, Rescue Maneuvers Such as Proning and Alveolar Recruitment Maneuvers with Intracranial Pressure Monitoring May Be Reasonable to Improve Oxygenation (Class of Recommendation: 2b, Level of Evidence: B-NR)
Recommendations (European Society of Intensive Care Medicine/ESCIM Taskforce on Acute Respiratory Distress Syndrome/ARDS Guidelines, 2023) (Intensive Care Med, 2023)[MEDLINE]
Prone Position is Recommended Over Supine Position for Patients with Moderate‐Severe Acute Respiratory Distress Syndrome (ARDS) (Defined as pO2/FIO2 <150 mm Hg and PEEP ≥5 cm H2O, Despite Optimization of Ventilation Settings) to Reduce the Mortality Rate (Strong Recommendation, High Level of Evidence in Favor)
Recommendation Also Applies to Acute Respiratory Distress Syndrome (ARDS) from COVID‐19 (Strong Recommendation; Moderate Level of Evidence in Favor for Indirectness)
Starting Prone Position is Recommended in Patients with Acute Respiratory Distress Syndrome (ARDS) Receiving Invasive mechanical Ventilation Early After Intubation, After a Period of Stabilization During Which Low Tidal Volume is Applied and PEEP Adjusted and at the End of Which the pO2/FIO2 Remains <150 mm Hg; and Proning Should Be Applied for Prolonged Sessions (≥16 Consecutive hrs) to Reduce the Mortality Rate (Strong Recommendation; High Level of Evidence in Favor)
Recommendation Also Applies to Acute Respiratory Distress Syndrome (ARDS) from COVID‐19 (Strong Recommendation; Moderate Level of Evidence in Favor for Indirectness)
Awake Prone Positioning is Recommended Over Supine position for Non‐Intubated Patients with COVID‐19‐Related Acute Hypoxemic Respiratory Failure to Reduce the Intubation Rate (Weak Recommendation; Low Level of Evidence in Favor)
No Recommendation Regarding Awake Prone Positioning for Non‐Intubated Patients with COVID‐19‐Related Acute Hypoxemic Respiratory Failure to Reduce the Mortality Rate (No Recommendation; Moderate Level of Evidence of No Effect)
No Recommendation Regarding Awake Prone Positioning for Patients with Acute Hypoxemic Respiratory Failure Not Due to COVID‐19 (No Recommendation; No Evidence)
Body Position -> Head of Bed at ≥30°
Rationale
Head of Bed at ≥30° Decreases the Frequency and Severity of Gastric Aspiration in Mechanically Ventilated Patients (Ann Intern Med, 1992) [MEDLINE]
The Longer the Patient is in Supine Position, the More Likely They are to Aspirate
Clinical Efficacy
Single-Center Study of Obese vs Non-Obese Patients with Acute Respiratory Distress Syndrome (ARDS) (Chest, 2023) [MEDLINE]: n = 40
Twenty Patients were Bbese (BMI 38.4 (34.5-42.3) kg/m2) and Twenty were Non-Obese (BMI 26.6 (25.2-28.5) kg/m2
In the Obese Patients, Lung and Chest Wall Elastance, Driving Pressure, Inspiratory Transpulmonary Pressure, pCO2 and Ventilatory Ratio were Lower in the Supine than Semi-Recumbent Positions (P<0.001)
Airways Resistance was Greater in the Supine Position (P = 0.006)
In the Non-Obese Patients, Only Chest Wall Elastance was lLower in Supine vs Semi-Recumbent Position (P < 0.001)
Conclusion
In Mechanically Ventilated Obese Patients with Acute Respiratory Distress Syndrome (ARDS), Supine Position Provided Lower Lung and Chest Wall Elastance, and Better Carbon Dioxide Clearance, than the Semi-Recumbent Position
Recommendations for Patients with Acute Respiratory Distress Syndrome (ARDS) Associated with Sepsis (2016 Surviving Sepsis Guidelines; Intensive Care Med, 2017) [MEDLINE]
Elevation of the Head of the Bed to 30-45 Degrees is Recommended to Limit the Aspiration Risk and to Prevent the Development of Ventilator-Associated Pneumonia (VAP) During Mechanical Ventilation in Sepsis-Associated Respiratory Failure (Strong Recommendation, Low Quality of Evidence)
Body Position -> Continuous Lateral Rotational/Kinetic Bed Therapy
History
1967: first implemented
Rationale
Continuous Lateral Rotational/Kinetic Bed Therapy Was Developed in Effort to Decrease Complications of Prolonged Immobilization (Pneumonia, Venous Stasis, Skin Breakdown) and Mobilize Secretions
Administration
Utilize Rotational Arc >80° (40° in Either Direction): arcs of less than this amount have unknown benefit
Beds are Not Available for Purchase: can only be rented at $175-$275/day
Clinical Efficacy
Study of Continuous Oscillation Therapy in Acute Respiratory Distress Syndrome (ARDS) (J Crit Care, 1995) [MEDLINE]
In Selected Critically Ill Patients, Oscillating Therapy May Improve Survival and Improve Airway Clearance
However, the Frequency and Degree of Turning Required to Prevent Complications is Unclear
Study of Rotational Therapy in ARDS (Intensive Care Med, 1998) [MEDLINE]
Continuous Axial Rotation Might Acutely Decrease V/Q Mismatch in Mild-Moderate Acute Lung Injury, But it is Not Effective in Progressive-Late Acute Respiratory Distress Syndrome (ARDS)
Further Studies re Required
Review and Meta-Analysis of Rotational Bed Therapy in Acute Respiratory Distress Syndrome (ARDS) (Am J Crit Care, 2007) [MEDLINE]: n = 15 nonrandomized, uncontrolled, or retrospective studies (1987-2004)
As Compared to Nurse Turning q2hrs, Meta-Analysis Suggested that Rotational Bed Therapy Decreased the Incidence of Pneumonia, But Had No Effect on Duration of Mechanical Ventilation, ICU Length of Stay, or Hospital Mortality Rate
Case Series of Rotational Percussion Bed Therapy in Acute Respiratory Distress Syndrome (ARDS) Patients Supported on EMCO Therapy (ASAIO J, 2016) [MEDLINE]
Use of Chest Physiotherapy, Frequent Body Repositioning, and Bronchoscopy May Be Helpful in the Management of Pulmonary Secretions in ARDS Patients Supported with ECMO
Improved Carbon Dioxide Elimination: occurs only at high NO concentrations and only with baseline pCO2 >50 mm Hg
Due to Improved Perfusion, Resulting in Decreased Alveolar Dead Space
Pulmonary Artery Vasodilation: modestly decreased pulmonary artery pressure occurs in the majority of patients
Selective Pulmonary Artery Vasodilation of Better Ventilated Lung Regions, Resulting in Improved V/Q Matching
Anti-Inflammatory/Anti-Platelet Effects: both theoretical
Administration
Half-Life: several milliseconds
FDA Approval: only for treatment of term/near-term (34 wk) neonates with hypoxic respiratory failure and pulmonary hypertension
Dosing and Response: 60-80% respond to <10 ppm with >20% increase in pO2 (lower response rate in sepsis-related acute respiratory distress syndrome, due to higher background inducible NO levels)
Likely Occurs Predominantly in Patients with Methemoglobin Reductase Deficiency
Generation of O2 Radicals
However, Clinically Significant Toxicity Has Not Been Reported in Trials
Clinical Efficacy
Systematic Review and Meta-Analysis (BMJ, 2007) [MEDLINE]
Inhaled Nitric Oxide Results in Limited Improvement in Oxygenation in Patients with Acute Respiratory Distress Syndrome (ARDS), But Confers No Mortality Benefit (and May Cause Harm)
Cochrane Database Systematic Review of iNO in Acute Respiratory Distress Syndrome (ARDS) (Cochrane Database Syst Rev, 2016) [MEDLINE]
Evidence is Insufficient to Support iNO in Any Category of Critically Ill Patients with Acute Hypoxemic Respiratory Failure
Inhaled Nitric Oxide Results in a Transient Improvement in Oxygenation, But Does Not Decrease the Mortality Rate and May Be Harmful, as it Seems to Increase Renal Impairment
US Database Study of Inhaled Nitric Oxide Use in the Treatment of Acute Respiratory Distress Syndrome (ARDS) (Chest, 2022) [MEDLINE]: n = 11,200 (303 hospitals from Premier Healthcare Database)
56.8% of Patients Received Inhaled Nitric Oxide First, 42.1% of Patients Received Inhaled Epoprostenol First, and 1% of Patients Received Both Therapies on the Same Day
34.3% of Hospitals Exclusively Used Inhaled Nitric Oxide and 38.9% of Hospitals Exclusively Used Inhaled Epoprostenol
No Differences were Found in the Likelihood of Successful Extubation Between Patients Admitted to Inhaled Nitric Oxide-Only Hospitals vs Those Admitted to Inhaled Epoprostenol-Only Hospitals (Subdistribution Hazard Ratio 0.97; 95% CI, 0.80-1.18)
Also, No Differences were Found in Total Hospital Costs or Death
Phase II, SIngle-Blinded, Multicenter Randomized Trial of High-Dose Inhaled Nitric Oxide in Acute Respiratory Distress Syndrome (on Mechanical Ventilation) Associated with COVID-19 (Am J Respir Crit Care Med, 2023) [MEDLINE]: n = 193
At 48 hrs, Mean Change in pO2/FiO2 Ratio was 28.3 mm Hg in the iNOS Group and 21.4 mm Hg in the Control Group (Mean Difference 39.1 mm Hg; 95% Credible Interval: 18.1-60.3)
Mean Time to Reach a PaO2/FiO2.300 mm Hg in the iNOS Group was 8.7 Days, as Compared to 8.4 Days for the Control Group (Mean Difference 0.44; 95% Credible Interval: 23.63-4.53)
At 28 Days, the Proportion of Participants Attaining a PaO2/FiO2.300 mm Hg was 27.7% in the iNOS Group and 17.2% in the Control Group (Risk Ratio 2.03; 95% Credible Interval: 1.11-3.86)
Duration of Ventilation and Mortality at 28 and 90 Days Did Not Differ
No Serious Adverse Events were Reported
British Thoracic Society 2019 Guidelines for the Management of Acute Respiratory Distress Syndrome (ARDS) (BMJ Open Respir Res, 2019) [MEDLINE]
Use of Inhaled Nitric Oxide is Not Recommended in Patients with Acute Respiratory Distress Syndrome (ARDS) (Grade Recommendation: Weakly Against)
Inhaled Pulmonary Vasodilator Which Selectively Dilates Pulmonary Arteries Which Perfuse Well-Ventilated Lung Zones, Resulting in Improved V/Q Matching and Improved Oxygenation
Pulmonary Vasodilation Also Decreases Pulmonary Artery Pressures
Clinical Efficacy
Systematic Review and Meta-Analysis of Inhaled Prostaglandins in Acute Respiratory Distress Syndrome (ARDS) (Chest, 2015) [MEDLINE]
Inhaled Prostaglandins Improve Oxygenation and Decrease Pulmonary Artery Pressures and May Be Associated with Harm
Data are Limited Both in Terms of Methodologic Quality and Demonstration of Clinical Benefit
Use of Inhaled Prostaglandins in ARDS Needs Further Study
US Database Study of Inhaled Nitric Oxide Use in the Treatment of Acute Respiratory Distress Syndrome (ARDS) (Chest, 2022) [MEDLINE]: n = 11,200 (303 hospitals from Premier Healthcare Database)
56.8% of Patients Received Inhaled Nitric Oxide First, 42.1% of Patients Received Inhaled Epoprostenol First, and 1% of Patients Received Both Therapies on the Same Day
34.3% of Hospitals Exclusively Used Inhaled Nitric Oxide and 38.9% of Hospitals Exclusively Used Inhaled Epoprostenol
No Differences were Found in the Likelihood of Successful Extubation Between Patients Admitted to Inhaled Nitric Oxide-Only Hospitals vs Those Admitted to Inhaled Epoprostenol-Only Hospitals (Subdistribution Hazard Ratio 0.97; 95% CI, 0.80-1.18)
Also, No Differences were Found in Total Hospital Costs or Death
Any Condition or Organ Dysfunction that Would Limit the Likelihood of Overall Benefit from ECMO, Such as Severe, Irreversible Brain Injury or Untreatable Metastatic Cancer
High FiO2 Requirement >80% for >7 Days
High-Pressure Ventilation (Plateau Pressure >30 cm of H2O) for >7 Days
Limited Vascular Access
Technique
Requires Local Expertise and Invasive Vascular Access
Venovenous Access is Most Commonly Used (Although Venoarterial Access Can Be Alternatively Used)
ECMO Had No Mortality Benefit in Treatment of Acute Respiratory Distress Syndrome (ARDS) Associated with Influenza
CESAR Trial of ECMO in the UK (Lancet, 2009) [MEDLINE]
ECMO Decreased Mortality Rate/Severe Disability at 6 mo
However, the Study was Flawed by Not Defining the Usual Care Group and ECMO Patients Were Concentrated in One Center in the Trial
Systematic Review and Meta-Analysis of ECMO in Adult Patients with Acute Respiratory Distress Syndrome (ARDS) (J Crit Care, 2013) [MEDLINE]
ECMO Had an Unclear Hospital Mortality Benefit: further studies were recommended
Cochrane Review of VV-ECMO and VA-ECMO in Critically Ill Adults (Cochrane Database Syst Rev, 2015) [MEDLINE]
ECMO Had No 6-Month (or Prior to 6 Month) All-Cause Mortality Benefit: low-moderate quality of evidence from trials
Study of the Long-Term Survival and Quality of Life Following ECMO (Eur J Cardiothorac Surg, 2017) [MEDLINE]
Survival to Discharge was Higher in the Non-ECMO Group, as Compared to the ECMO Group: however, this difference was not statistically significant after propensity score matching
One Year Survival was 67% in the Non-ECMO Group vs 60% in the ECMO Group
Two Year Survival was 50% in the Non-ECMO Group vs 45% in the ECMO Group
Single-Center Swedish Retrospective Study of Outcomes After ECMO for Acute Respiratory Distress Syndrome (ARDS) Associated with Sepsis (Crit Care Med, 2017) [MEDLINE]
Approximately 64% of ECMO Patients Survived to Discharge
High Mortality Rate Within the First Few Months After Discharge
Systematic Review and Meta-Analysis of Mortality and Complications with the Use of Venovenous ECMO in Acute Respiratory Distress Syndrome (ARDS) (Ann Intensive Care, 2017) [MEDLINE]
Mortality Rate at Hospital Discharge was 37.7%
Factors Associated with Increased Hospital Mortality
Age
Year of Study
Mechanical Ventilation and Prone Positioning Days Prior to ECMO
Systematic Review of Venovenous ECMO for Acute Respiratory Distress Syndrome (ARDS) (J Crit Care, 2017) [MEDLINE]: n = 27 studies
Mortality Benefit of ECMO is Unclear
French EOLIA Trial of VV-ECMO in Acute Respiratory Distress Syndrome (ARDS) (NEJM, 2018) [MEDLINE]
In Very Severe Acute Respiratory Distress Syndrome (ARDS), VV-ECMO Did Not Decrease the 60-Day Mortality Rate, as Compared to a Conventional Mechanical Ventilation Strategy Which Included VV-ECMO as a Rescue Therapy
Secondary Analysis of the SUPERNOVA Trial of ECCO2R and Low Tidal Ventilation (4 mL/kg) in Acute Respiratory Distress Syndrome (Thorax, 2019) [MEDLINE]: n = 95 (with moderate acute respiratory distress syndrome (ARDS)
Tidal Volume of 4 mL/kg was Reached by 55% and 64% of Patients with the Lower Extraction vs 90% and 92% of Patients with Higher Extraction Devices at 8 and 24 hrs from Daseline, Respectively (p<0.001)
The Percentage of Patients Experiencing Episodes of ECCO2R-Related Hemolysis and Bleeding was Higher with Lower than with Higher Extraction Devices (21% vs 6%, p=0.045% and 27% vs 6%, p=0.010, Respectively)
Systematic Review and Meta-Analysis of ECMO in Adults with Acute Respiratory Distress Syndrome (ARDS) (Lancet Respir Med, 2019) [MEDLINE]: n = 773 (2 randomized controlled trials and 3 observational studies with matching techniques)
Compared with Conventional Mechanical Ventilation, the Use of Venovenous ECMO in Adults with Severe Acute Respiratory Distress Syndrome was Associated with a Decreased 60-Day Mortality Rate (73 [34%] of 214 vs 101 [47%] of 215; RR 0.73 [95% CI 0.58-0.92]; p=0.008; I2 0%; Moderate Grade Evidence)
However, Venovenous ECMO was Also Associated with a Moderate Risk of Major Hemorrhage (Occurred in 19% of Cases)
Randomized, Multicenter pRotective vEntilation with veno-venouS lung assisT (REST) Trial of ECCO2R and Low Tidal Ventilation in Acute Hypoxemic Respiratory Failure (JAMA, 2021) [MEDLINE]: n = 412
Study was Terminated Early (Due to Futility)
Extracorporeal Carbon Dioxide Removal (ECCO2R) to Facilitate Lower Tidal Volume Ventilation Did Not Impact the 90-Day Mortality Rate, as Compared to Conventional Low Tidal Volume Ventilation
Emulated Target Trial Analysis of ECMO in COVID-Associated Acute Respiratory Distress Syndrome (ARDS) (Am J Respir Crit Care Med, 2022) [MEDLINE]: n = 1,235
ECMO Strategy Had a Higher Survival Probability at Day 7 from the Onset of Eligibility Criteria (87% vs 83%, Risk Difference: 4%; 95% CI: 0-9%) Which Decreased During Follow-Up (Survival at Day 90: 63% vs 65%, Risk Difference: -2%; 95% CI: -10 to 5%)
However, ECMO was Associated with Higher Survival When Performed in High-Volume ECMO Centers or in Regions Where a Specific ECMO Network Organization was Set Up to Handle High Demand, and When Initiated within the First 4 Days of Mechanical Ventilation and in Profoundly Hypoxemic Patients
Retrospective Observational Study of Early VV-ECMO in Acute Respiratory Distress Syndrome (ARDS) (Respir Res, 2023) [MEDLINE]: n = 158 (median age: 58 y/o)
Mean Duration of Invasive Mechanical Ventilation Prior to VV-ECMO was Significantly Shorter in Survivors Than in Non-Survivors [Survivors Median = 1; Interquartile Range: 1-3; Non-Survivors Median = 4; Interquartile Range: 1-5.75; p = 0.0001)
Logistic Regression Demonstrated an Association Between the Duration of Ventilation Prior to VV-ECMO and Patient Mortality
Odds Ratio for 28-Day All-Cause Mortality and In-Hospital Mortality was Significantly Decreased in Patients Who Received VV-ECMO within the First 5 Days of Invasive Mechanical Ventilation
Pooled Analysis of VV-ECMO in Acute Respiratory Distress Syndrome (ARDS) (Am J Respir Crit Care Med, 2023) [MEDLINE]
VV-ECMO Probably Decreased the Mortality Rate at the Latest Follow-Up (Relative Risk 0.76; 95% CI: 0.60–0.95; Moderate Certainty)
VV-ECMO Probably Increased Ventilator-Free Days (Mean Difference 8 Days More; 95% CI: 2–15; Moderate Certainty)
VV-ECMO Probably Increases Vasopressor-Free Days (Mean Difference 8 Days More; 95% CI: 3–13; Moderate Certainty)
VV-ECMO Probably Increased Renal Replacement Therapy–Free Days (Mean Difference 7 Days More; 95% CI: 2–13; Moderate Certainty)
Safety Outcomes
VV-ECMO Probably Increased the Risk of Hemorrhage (Relative Risk 1.64; 95% CI: 1.17–2.31; Moderate Certainty)
VV-ECMO Had Little to No Effect on the Risk of Pneumothorax (RR, 1.13; 95% CI: 0.61–2.12; Low Certainty)
VV-ECMO Had an Uncertain Effect on the Risk of Stroke (Relative Risk 0.38; 95% CI: 0.10–1.39; Very Low Certainty)*
SUPERNOVA Trial of ECCO2R and Low Tidal Ventilation: trial underway
Clinical Efficacy-Use of Venovenous Extracorporeal Membrane Oxygenation (VV-ECMO) in Obese Patients
ECMObesity Trial of Venovenous Extracorporeal Membrane Oxygenation (VV-ECMO) in Obese Patients with Acute Respiratory Distress Syndrome (ARDS) (Am J Respir Crit Care Med, 2023) [MEDLINE]: n = 790 (320 with obesity)
Of the Obese Patients, 24.1% Died in the Intensive Care Unit (ICU), as Compared to 35.3% patients without Obesity (p < 0.001)
In Adjusted Models, Obesity was Associated with Lower Intensive Care Unit (ICU) Mortality (Odds Ratio 0.63; 95% CI: 0.43-0.93; p = 0.018)
Examined as a Continuous Variable, Higher Body Mass Index (BMI) was Associated with Decreased Intensive Care Unit (ICU) Mortality in Multivariable Regression (Odds Ratio 0.97; 95% CI 0.95-1.00; p = 0.023)
Propensity Score Matching 199 Patients with Obesity to 199 Patients without Obesity, Patients with Obesity Had a Lower Probability of Intensive Care Unit (ICU) Death than Those without Obesity (22.6% vs 35.2%; p = 0.007)
Clinical Efficacy-Mechanical Ventilation Settings During Venovenous Extracorporeal Membrane Oxygenation (VV-ECMO)
Based Only on Expert Opinion, Protective Mechanical Ventilation Strategies Should Be Used During VV-ECMO (Minerva Anestesiol, 2015) [MEDLINE]
Extracorporeal Life Support Organization (ELSO) Suggests Using Mechanical Ventilation “at Low Settings to Allow Lung Rest”
ELSO Also Suggests that “For Patients with Respiratory Failure, a Common Mistake is to Try to Recruit Lung Volume During the Acute Inflammatory Stage Early in ECMO”
French Consensus Conference on Extracorporeal Life Support for Patients with ARDS Recommends “Adjust Mechanical Ventilation to Minimize Plateau Pressure While Administering a Minimum PEEP” without Citing Specific Values
Prospective, Randomized Trial of Ultraprotective Ventilation in Acute Respiratory Distress Syndrome (ARDS) Patients on Venovenous Extracorporeal Membrane Oxygenation (VV-ECMO) (Crit Care, 2022) [MEDLINE]: n = 39
Despite a Decrease in Mechanical Power with Ultraprotective Ventilation (VT 1-2 mL/kg PBW, RR 5-10 Breaths/min, Positive Expiratory Transpulmonary Pressure, and Proning x 16 hrs), This Strategy for 48 hrs Did Not Reduce Biotrauma (as Assessed by Alveolar Concentrations of Interleukin-1β, Interleukin-6/Interleukin-8/Surfactant Protein D and Blood Concentrations of Serum Advanced Glycation End Products/Angiopoietin), as Compared to Control
Prospective Study of Different PEEP Settings on Mechanical Power During Ultraprotective Ventilation in ARDS Patients Treated with Venovenous Extracorporeal Membrane Oxygenation (VV-ECMO) (Crit Care, 2023) [MEDLINE]
PEEP Titration Protocols
PEEP Titration Per PEEP of 10 cmH2O, Representing the Lowest Recommendation by the Extracorporeal Life Support Organization (PEEPELSO)
PEEP Titration Per the Highest Static Compliance of the Respiratory System (PEEPCstat,RS)
PEEP Titration Per the Target End-Expiratory Transpulmonary Pressure of 0 cm H2O (PEEPPtpexp)
PEEPELSO was Lower, as Compared to PEEPCstat,RS and PEEPPtpexp (10.0 ± 0.0 vs. 16.2 ± 4.7 cmH2O and 17.3 ± 4.0 cmH2O, p < 0.001 Each, Respectively)
PEEPELSO Decreased Mechanical Power, as Compared to PEEPCstat,RS and PEEPPtpexp (5.3 ± 1.3 vs. 6.8 ± 2.0 and 6.9 ± 2.3 J/min, p < 0.001 Each, Respectively)
PEEPELSO Resulted in Less Lung Stress, as Compared to PEEPCstat,RS (p = 0.011) and PEEPPtpexp (p < 0.001) and Increased Cardiac Output and Oxygen Delivery (p < 0.001 Each)
Clinical Efficacy-Proning During Venovenous Extracorporeal Membrane Oxygenation (VV-ECMO)
PRONECMO Trial of Proning During Venovenous Extracorporeal Membrane Oxygenation (VV-ECMO) (JAMA, 2023) [MEDLINE] : n = 170
Within 60 Days of Enrollment, 44% of Patients Had Successful Venovenous Extracorporeal Membrane Oxygenation (VV-ECMO) Weaning in the Prone Venovenous Extracorporeal Membrane Oxygenation (VV-ECMO) Group, as Compared to 44% in the Supine Venovenous Extracorporeal Membrane Oxygenation (VV-ECMO) Group (Risk Difference 0.1% [95% CI: -14.9% to 15.2%]; Subdistribution Hazard Ratio, 1.11 [95% CI: 0.71-1.75]; P = 0.64)
Within 90 Days, no Significant Difference was Observed in Venovenous Extracorporeal Membrane Oxygenation (VV-ECMO) Duration (28 vs 32 Days; Difference -4.9 [95% CI: -11.2 to 1.5] Days; P = 0.13), Intensive Care Unit Length of Stay, or 90-Day Mortality (51% vs 48%; Risk Difference 2.4% [95% CI: -13.9% to 18.6%]; P = 0.62)
No Serious Adverse Events were Reported During Proning
Recommendations for Patients with Acute Respiratory Distress Syndrome (ARDS) Associated with Sepsis (2016 Surviving Sepsis Guidelines; Intensive Care Med, 2017) [MEDLINE]
VV-EMCO May Be Considered in Centers with Local Expertise
British Thoracic Society 2019 Guidelines for the Management of Acute Respiratory Distress Syndrome (ARDS) (BMJ Open Respir Res, 2019) [MEDLINE]
The Routine Use of Venovenous Extracorporeal Membrane Oxygenation (VV-ECMO) is Not Recommended for All Patients with Acute Respiratory Distress Syndrome (ARDS) (Grade Recommendation: Weakly Against)
The Use of Venovenous Extracorporeal Membrane Oxygenation (VV-ECMO) with Lung Protective Mechanical Ventilation is Recommended in Selected Patients with Severe Acute Respiratory Distress Syndrome (ARDS) (Grade Recommendation: Weakly in Favor)
Use of ECCO2R in Established Acute Respiratory Distress Syndrome (ARDS) Should Be the Subject of a Suitably Powered Multicenter Randomized Controlled Trial with Long-Term Follow-Up and Economic Analysis (Grade Recommendation: Research Recommendation)
American Thoracic Society (ATS) 2023 Clinical Practice Guideline for Acute Respiratory Distress Syndrome (ARDS) (Am J Respir Crit Care Med, 2023) [MEDLINE]
Use of VV-ECMO is Suggested in Selected Patients with Severe Acute Respiratory Distress Syndrome (ARDS) (Conditional Recommendation, Low Certainty of Evidence)
Due to the Resource-Intensive Nature of VV-ECMO, Less Invasive Acute Respiratory Distress Syndrome (ARDS) Therapies, Such as Lung Protective Ventilation, Higher PEEP, Neuromuscular Blockade, and Proning Should Be Used Before Consideration of VV-ECMO
Recommendations (European Society of Intensive Care Medicine/ESCIM Taskforce on Acute Respiratory Distress Syndrome/ARDS Guidelines, 2023) (Intensive Care Med, 2023)[MEDLINE]
Patients with Severe Acute Respiratory Distress Syndrome (ARDS) Not Due to COVID‐ 19 as Defined by the EOLIA Trial Eligibility Criteria, Should Be Treated with VV-ECMO in an ECMO Center Which Meets Defined Organizational Standards, Adhering to a Management Strategy Similar to that Used in the EOLIA Trial (Strong Recommendation, Moderate Level of Evidence in Favor)
Recommendation Also Applies to Patients with Severe Acute Respiratory Distress Syndrome (ARDS) Due to COVID‐19 (Strong Recommendation; Low Level of Evidence in Favor for Indirectness)
The Use of ECCO2R for the Treatment of Acute Respiratory Distress Syndrome (ARDS) Not Due to COVID‐19 is Not Recommended to Prevent Mortality Outside of Randomized Controlled Trials (Strong Recommendation, High Level of Evidence of No Effect)
Recommendation Also Applies to Patients with Severe Acute Respiratory Distress Syndrome (ARDS) Due to COVID‐19 (Strong Recommendation; Moderate Level of Evidence of No Effect for Indirectness)
Allogeneic Mesenchymal Stromal Cells
Clinical Efficacy
START (Phase a Safety) Trial of Allogeneic Mesenchymal Stromal Cells in Acute Respiratory Distress Syndrome (ARDS) (Lancet Respir Med, 2019) [MEDLINE]
One Dose of Intravenous Mesenchymal Stromal Cells was Safe in Patients with Moderate-Severe ARDS
Trial of Early Mobilization with Physical/Occupational Therapy in Critically Ill Patients (Lancet, 2009) [MEDLINE]
Early Mobilization (with Interruption of Sedation and Physical/Occupational Therapy) in the Earliest Days of Critical Illness was Safe and Well-Tolerated
Early Mobilization (with Interruption of Sedation and Physical/Occupational Therapy) in the Earliest Days of Critical Illness Improved Functional Outcomes at Hospital Discharge, Decreased Duration of Delirium, and Increased Ventilator-Free Days, as Compared to Standard Care
Multi-Center German/Austrian/US Trial of Early Mobilization in Surgical ICU Patients (Lancet, 2016) [MEDLINE]: n = 200
Early Mobilization Increased Mobilization, Decreased ICU Length of Stay, and Improved Functional Mobility at Hospital Discharge
Early Mobilization Group Had Higher Incidence of Adverse Events (2.8% vs 0.8%), as Compared to Control Group: however, no serious adverse events were observed
Early Mobilization Group Had Higher In-Hospital Mortality Rate (16% vs 8%), as Compared to Control Group
Early Mobilization Group Had Higher 3-Month Mortality Rate (22% vs 17%), as Compared to Control Group
Trial of Standardized Rehabilitation (Daily Physical Therapy) in Acute Respiratory Failure (Requiring Mechanical Ventilation) in the ICU (JAMA, 2016) [MEDLINE]: single-center randomized trial (n = 300)
Standardized Rehabilitation Therapy Did Not Decrease Hospital Length of Stay, ICU Length of Stay, or Ventilator Days in Patients with Acute Respiratory Failure
Systematic Review of Early Mobilization in the ICU (Intensive Care Med, 2017) [MEDLINE]
Active Mobilisation and Rehabilitation in the ICU has No Impact on Short and Long-Term Mortality, But May Improve Mobility Status, Muscle Strength and Days Alive and Out of Hospital at 180 Days
Trial of Chest Physiotherapy with Earlu Mobilization in Critically Ill ICU Patients (Clin Respir J, 2018) [MEDLINE]: n = 439
Intensive Chest Physiotherapy Decreased the Extubation Failure Rate in Mechanically Ventilated Patients
Chest Physiotherapy Improved the Rapid Shallow Breathing Index (RSBI) Score
Single-Center Randomized Trial of In-Bed Cycling and Electrical Stimulation of the Quadriceps in Critically Ill ICU Patients (JAMA, 2018) [MEDLINE]
No Clinical Efficacy in Terms of Global Muscle Strength
Nutritional Support
Clinical Efficacy (General)
OMEGA Trial Examining the Effect of Supplementation with Omega-3 (n-3) Fatty Acids (Docosahexaenoic Acid = DHA, Eicosapentaenoic Acid = EPA), γ-Linolenic Acid, and Antioxidants in Acute Lung Injury (JAMA, 2011) [MEDLINE]
Enteral Omega-3 Fatty Acids, Gamma-Linolenic Acid, and Antioxidants Did Not Improve the Primary Endpoint of Ventilator-Free Days or Other Clinical Outcomes in Patients with Acute Lung Injury and May Be Harmful
EDEN Trial of Enteral Nutrition in Acute Lung Injury (JAMA, 2012) [MEDLINE]
Initial Trophic Feeding (For Up to 6 Days) Did Not Improve Ventilator Days, 60-Day Mortality, or Infectious Complications, as Compared to Full Feeding
Full Feeding Group Had More Gastrointestinal Intolerance (Vomiting, Constipation, and Elevated Gastric Residual Volumes): they received more pro-kinetic agents
Trial of Glutamine and Antioxidants in Critically Ill Patients with Mutiorgan Failure on Mechanical Ventilation (NEJM, 2013) [MEDLINE]
Early Provision of Glutamine or Antioxidants Did Not Improve Clinical Outcomes, and Glutamine was Associated with an Increase in Mortality Among Critically IIl Patients with Multiorgan Failure
Australia/New Zealand TARGET Trial of Energy-Dense Enteral Nutrition in Patients on Mechanical Ventilation (NEJM, 2018) [MEDLINE]
In Patients on Mechanical Ventilation, the Energy-Dense Enteral Nutrition Had No Impact on the 90-Day Mortality Rate, as Compared to Routine Enteral Nutrition
Clinical Efficacy (During Prone Ventilation)
Study of Early Enteral Nutrition in Association with Prone Ventilation (Crit Care Med, 2004) [MEDLINE]
Early Enteral Nutrition is Poorly-Tolerated in Patients Who are Prone-Ventilated
Prokinetic Agents, Transpyloric Feeding, and Semirecumbency Should Be Considered to Enhance Gastric Emptying and to Prevent Vomiting in This Population
Study of Head of Bed Elevation in Enteral Nutrition in Association with Prone Ventilation (Clin Nutr, 2010) [MEDLINE]:
Elevation (25 Degrees) Increased Acceleration of Tube Feedings to Target Rate
Erythromycin Improved Delivery of Enteral Nutrition
Study of Enteral Nutrition in Association with Prone Ventilation (J Parenter Enteral Nutr, 2016) [MEDLINE]
Enteral Nutrition in Association with Prone Ventilation is Feasible, Safe, and Not Associated with an Increased Risk of Gastrointestinal Complications
Recommendations (Society of Critical Care Medicine, SCCM, and American Society for Parenteral and Enteral Nutrition, ASPEN, 2016 Guidelines) [MEDLINE]
High Fat/Low Carbohydrate Tube Feedings are Not Recommended in Patients with Acute Respiratory Failure (Quality of Evidence: Very Low)
Either Trophic or Full Feedings are Acceptable in Acute Respiratory Distress Syndrome (ARDS) with an Expected Duration of Mechanical Ventilation ≥72 hrs (Quality of Evidence: High)
Both Trophic and Full Feeding Strategies Have Similar Outcomes for the First Week of Hospitalization
In Acute Respiratory Failure, Fluid-Restricted, Energy-Dense Enteral Formulations Should Be Considered, Especially in the State of Volume Overload (Quality of Evidence: Expert Consensus)
Supplemental Antioxidant Vitamins (Vitamins E and C) and Trace Minerals (Selenium, Zinc, Copper) May Be Beneficial in Burns, Trauma, Critical Illness Requiring Mechanical Ventilation (Quality of Evidence: Low)
Supplemental Omega-3 (n-3) Fatty Acids (Docosahexaenoic Acid = DHA, Eicosapentaenoic Acid = EPA) Are Not Recommended in Acute Respiratory Distress Syndrome (ARDS)
Weaning
Recommendations for Patients with Acute Respiratory Distress Syndrome (ARDS) Associated with Sepsis (2016 Surviving Sepsis Guidelines; Intensive Care Med, 2017) [MEDLINE]
Spontaneous Breathing Trials (When Specific Criteria are Met) are Recommended in Sepsis-Associated Respiratory Failure (Strong Recommendation, High Quality of Evidence)
Weaning Protocol is Recommended for Appropriate Patients During Mechanical Ventilation in Sepsis-Associated Respiratory Failure (Strong Recommendation)
Therapies with Unclear or No Clinical Benefit in Acute Respiratory Distress Syndrome (ARDS)
Macrolides Have Potential Anti-Inflammatory Effects
Clinical Efficacy
Secondary Analysis of Randomized Controlled Acute Respiratory Distress Syndrome Network Lisofylline and Respiratory Management of Acute Lung Injury (LARMA) Trial Examining Macrolide Use in Acute Respiratory Distress Syndrome (ARDS) (Chest, 2012) [MEDLINE]
Receipt of Macrolide Antibiotics (Erythromycin, Azithromycin) was Associated with Decreased 180-Day Mortality Rate and Shorter Time to Successful Discontinuation of Mechanical Ventilation in Acute Respiratory Distress Syndrome (ARDS), as Compared to Fluoroquinolones and Cephalosporins
Importantly, Patients Receiving Macrolides Were More Likely to Have Pneumonia as Their Acute Respiratory Distress Syndrome (ARDS) Risk Factor, Were Less Likely to Have Non-Pulmonary Sepsis or Be Randomized to Low Tidal Volume Ventilation, and Had Shorter Length of Stay Prior to Trial Enrollment
Cochrane Database Review of Partial Liquid Ventilation in Acute Respiratory Distress Syndrome (ARDS) (Cochrane Database Syst Rev, 2013) [MEDLINE]
Partial Liquid Ventilation Had No Mortality Benefit in Acute Respiratory Distress Syndrome (ARDS) and Some Evidence Suggests an Increased Risk of Adverse Events
An Official American Thoracic Society/European Society of Intensive Care Medicine/Society of Critical Care Medicine Clinical Practice Guideline: Mechanical Ventilation in Adult Patients with Acute Respiratory Distress Syndrome. Am J Respir Crit Care Med. 2017 May 1;195(9):1253-1263. doi: 10.1164/rccm.201703-0548ST [MEDLINE]
Guidelines on the management of acute respiratory distress syndrome. BMJ Open Respir Res. 2019 May 24;6(1):e000420. doi: 10.1136/bmjresp-2019-000420. eCollection 2019 [MEDLINE]
OSCILLATE Trial. High-frequency oscillation in early acute respiratory distress syndrome. N Engl J Med. 2013 Feb 28;368(9):795-805 [MEDLINE]
Pressure Control Ventilation
Pressure-controlled versus volume-controlled ventilation for acute respiratory failure due to acute lung injury (ALI) or acute respiratory distress syndrome (ARDS). Cochrane Database Syst Rev. 2015 Jan 14;1(1):CD008807. doi: 10.1002/14651858.CD008807.pub2 [MEDLINE]
Randomized clinical trial of pressure controlled inverse ratio ventilation and extracorporeal CO2 removal for adult respiratory distress syndrome. Am J Respir Crit Care Med 1994; 149:295-305 [MEDLINE]
Should inverse ratio ventilation be used in adult respiratory distress syndrome? Am J Respir Crit Care Med 1994: 149:1354-1358
Airway pressure release ventilation as a primary ventilatory mode in acute respiratory distress syndrome. Acta Anaesthesiol Scand. 2004 Jul;48(6):722-31 [MEDLINE]
Other approaches to open-lung ventilation: Airway pressure release ventilation. Crit Care Med. 2005 Mar;33(3 Suppl):S228-40 [MEDLINE]
Respiratory controversies in the critical care setting. Does airway pressure release ventilation offer important new advantages in mechanical ventilator support? Respir Care. 2007 Apr;52(4):452-8; discussion 458-60 [MEDLINE]
Airway pressure release ventilation and biphasic positive airway pressure: a systemic review of definitional criteria. Intensive Care Med 2008;34(10):1766-1773 [MEDLINE]
Comparison of APRV and BIPAP in a mechanical model of ARDS (abstract). Respir Care 2010;55(11): 1516
A randomized prospective trial of airway pressure release ventilation and low tidal volume ventilation in adult trauma patients with acute respiratory failure. J Trauma. 2010;69(3):501-510 [MEDLINE]
Airway pressure release ventilation in acute respiratory distress syndrome. Crit Care Clin. 2011 Jul;27(3):501-9. doi: 10.1016/j.ccc.2011.05.003 [MEDLINE]
Airway pressure release ventilation: what do we know? Respir Care. 2012 Feb;57(2):282-92 [MEDLINE]
Airway pressure release ventilation prevents ventilator-induced lung injury in normal lungs. JAMA Surg. 2013 Nov;148(11):1005-12. doi: 10.1001/jamasurg.2013.3746 [MEDLINE]
Early application of airway pressure release ventilation may reduce mortality in high-risk trauma patients: a systematic review of observational trauma ARDS literature. J Trauma Acute Care Surg. 2013 Oct;75(4):635-41 [MEDLINE]
Early airway pressure release ventilation prevents ARDS-a novel preventive approach to lung injury. Shock. 2013 Jan;39(1):28-38. doi: 10.1097/SHK.0b013e31827b47bb [MEDLINE]
Airway pressure release ventilation in morbidly obese surgical patients with acute lung injury and acute respiratory distress syndrome Am Surg. 2013 Mar;79(3):242-6 [MEDLINE]
Airway Pressure Release Ventilation and High-Frequency Oscillatory Ventilation: Potential Strategies to Treat Severe Hypoxemia and Prevent Ventilator-Induced Lung Injury. Respir Care. 2015 Oct;60(10):1509-21. doi: 10.4187/respcare.04255 [MEDLINE]
Airway Pressure Release Ventilation May Result in Occult Atelectrauma in Severe ARDS. Respir Care. 2016 Sep;61(9):1278-80. doi: 10.4187/respcare.05099 [MEDLINE]
Should Airway Pressure Release Ventilation Be the Primary Mode in ARDS? Respir Care. 2016 Jun;61(6):761-73. doi: 10.4187/respcare.04653 [MEDLINE]
Partial Liquid Ventilation
Partial liquid ventilation for preventing death and morbidity in adults with acute lung injury and acute respiratory distress syndrome. Cochrane Database Syst Rev. 2013 Jul 23;7:CD003707 [MEDLINE]
Body Position -> Proning
Conference on the scientific basis of respiratory therapy. Pulmonary physiotherapy in the pediatric age group. Comments of a devil’s advocate. Am Rev Respir Dis 1974; 110: 143-144 [MEDLINE]
Effect of prone position on patients with hydrostatic pulmonary edema compared with patients with acute respiratory distress syndrome and pulmonary fibrosis. Am J Respir Crit Care Med 2000;151:360-368 [MEDLINE]
Effect of prone positioning on the survival of patients with acute respiratory failure. N Engl J Med 2001;345:568-573 [MEDLINE]
Decrease in PaCO2 with prone position is predictive of improved outcome in acute respiratory distress syndrome. Crit Care Med. 2003 Dec;31(12):2727-33 [MEDLINE]
Effect of systematic prone positioning in hypoxemic acute respiratory failure. JAMA 2004;292:2379-2387 [MEDLINE]
A multicenter trial of prolonged prone ventilation in severe acute respiratory distress syndrome. Am J Respir Crit Care Med 2006; 173: 1233-1239 [MEDLINE]
Effect of mechanical ventilation in the prone position on clinical outcomes in patients with acute hypoxemic respiratory failure: a systematic review and meta-analysis. CMAJ. 2008 Apr 22;178(9):1153-61 [MEDLINE]
The effect of prone positioning in acute respiratory distress syndrome or acute lung injury. Intensive Care Med 2008;34:1002-1011 [MEDLINE]
Prone ventilation reduces mortality in patients with acute respiratory failure and severe hypoxemia: systematic review and meta-analysis. Intensive Care Med. 2010 Apr;36(4):585-99 [MEDLINE]
PROSEVA: Prone positioning in severe acute respiratory distress syndrome. Engl J Med. 2013 Jun 6;368(23):2159-68. doi: 10.1056/NEJMoa1214103. Epub 2013 May 20 [MEDLINE]
In prone ventilation, one good turn deserves another. N Engl J Med 2013;368(23):2227-2228 [MEDLINE]
Effects of interventions on survival in acute respiratory distress syndrome: an umbrella review of 159 published randomized trials and 29 meta-analyses. Intensive Care Med 2014; 40: 769-787 [MEDLINE]
Prone positioning reduces mortality from acute respiratory distress syndrome in the low tidal volume era: a meta- analysis. Intensive Care Med 2014; 40: 332-341 [MEDLINE]
The efficacy and safety of prone positional ventilation in acute respiratory distress syndrome: updated study-level meta-analysis of 11 randomized controlled trials. Crit Care Med 2014; 42: 1252-1262 [MEDLINE]
Prone position for acute respiratory failure in adults. Cochrane Database Syst Rev 2015; 11: CD008095 [MEDLINE]
Efficacy of prone position in acute respiratory distress syndrome patients: A pathophysiology-based review. World J Crit Care Med. 2016 May 4;5(2):121-36. doi: 10.5492/wjccm.v5.i2.121. eCollection 2016 [MEDLINE]
Prone Position Reduces Spontaneous Inspiratory Effort in Patients with Acute Respiratory Distress Syndrome: A Bi-Center Study. Am J Respir Crit Care Med. 2021 Feb 10. doi: 10.1164/rccm.202012-4509LE [MEDLINE]
Patient-Directed Prone Positioning in Awake Patients with COVID-19 Requiring Hospitalization (PAPR). Ann Am Thorac Soc. 2021 Feb 17. doi: 10.1513/AnnalsATS.202011-1466RL [MEDLINE]
Factors Influencing the Implementation of Prone Positioning During the COVID-19 Pandemic: A Qualitative Study. Ann Am Thorac Soc. 2022 Aug 10. doi: 10.1513/AnnalsATS.202204-349OC [MEDLINE]
2023 Guideline for the Management of Patients With Aneurysmal Subarachnoid Hemorrhage: A Guideline From the American Heart Association/American Stroke Association. Stroke. 2023 Jul;54(7):e314-e370. doi: 10.1161/STR.0000000000000436 [MEDLINE]
Effects of early versus delayed application of prone position on ventilation-perfusion mismatch in patients with acute respiratory distress syndrome: a prospective observational study. Crit Care. 2023 Nov 27;27(1):462. doi: 10.1186/s13054-023-04749-3 [MEDLINE]
Prone Positioning During Extracorporeal Membrane Oxygenation in Patients With Severe ARDS: The PRONECMO Randomized Clinical Trial. JAMA. 2023 Dec 1:e2324491. doi: 10.1001/jama.2023.24491 [MEDLINE]
Body Position -> Head of Bed at 30°
Pulmonary aspiration of gastric contents in patients receiving mechanical ventilation: the effect of body position. Ann Intern Med 1992; 116:540-543 [MEDLINE]
Changes in respiratory mechanics with trunk inclination differs between obese and non-obese ARDS patients. Chest. 2023 Oct 11:S0012-3692(23)05564-2. doi: 10.1016/j.chest.2023.09.032 [MEDLINE]
Body Position -> Continuous Lateral Rotational/Kinetic Bed Therapy
Effect of air-supported, continuous, postural oscillation on the risk of early ICU pneumonia in nontraumatic critical illness. Chest. 1993 May;103(5):1543-7 [MEDLINE]
Acute effects of continuous rotational therapy on ventilation-perfusion inequality in lung injury. Intensive Care Med. 1998 Feb;24(2):132-7 [MEDLINE]
Rotational bed therapy to prevent and treat respiratory complications: a review and meta-analysis. Am J Crit Care. 2007 Jan;16(1):50-61; quiz 62 [MEDLINE]
Automated Rotational Percussion Bed and Bronchoscopy Improves Respiratory Mechanics and Oxygenation in ARDS Patients Supported with Extracorporeal Membrane Oxygenation. ASAIO J. 2016 May-Jun;62(3):e27-9. doi: 10.1097/MAT.0000000000000341 [MEDLINE]
Effects of inhaled nitric oxide in patients with acute respiratory distress syndrome: results of a randomized phase II trial. Inhaled Nitric Oxide in ARDS Study Group. Crit Care Med. 1998;26(1):15 [MEDLINE]
Low-dose inhaled nitric oxide in patients with acute lung injury: a randomized controlled trial. JAMA. 2004;291(13):1603 [MEDLINE]
Effect of nitric oxide on oxygenation and mortality in acute lung injury: systematic review and meta-analysis. BMJ. 2007 Apr 14;334(7597):779 [MEDLINE]
Therapies for refractory hypoxemia in acute respiratory distress syndrome. JAMA. 2010;304(22):2521 [MEDLINE]
Inhaled nitric oxide for acute respiratory distress syndrome and acute lung injury in adults and children: a systematic review with meta-analysis and trial sequential analysis. Anesth Analg. 2011;112(6):1411 [MEDLINE]
Inhaled nitric oxide does not reduce mortality in patients with acute respiratory distress syndrome regardless of severity: systematic review and meta-analysis. Crit Care Med. 2014;42(2):404 [MEDLINE]
Inhaled nitric oxide for acute respiratory distress syndrome (ARDS) in children and adults. Cochrane Database Syst Rev. 2016 Jun 27;(6):CD002787. doi: 10.1002/14651858.CD002787.pub3 [MEDLINE]
The effect of inhaled nitric oxide in acute respiratory distress syndrome in children and adults: a Cochrane Systematic Review with trial sequential analysis. Anaesthesia. 2017 Jan;72(1):106-117 [MEDLINE]
Inhaled Nitric Oxide vs Epoprostenol During Acute Respiratory Failure: An Observational Target Trial Emulation. Chest. 2022 Dec;162(6):1287-1296. doi: 10.1016/j.chest.2022.08.001 [MEDLINE]
High-Dose Inhaled Nitric Oxide in Acute Hypoxemic Respiratory Failure Due to COVID-19: A Multicenter Phase II Trial. Am J Respir Crit Care Med. 2023 Dec 15;208(12):1293-1304. doi: 10.1164/rccm.202304-0637OC [MEDLINE]
Inhalational agents for pulmonary hypertension. Lancet. 1993 Oct;342(8877):941-2 [MEDLINE]
Inhaled prostacyclin (PGI2) versus inhaled nitric oxide in adult respiratory distress syndrome. Am J Respir Crit Care Med. 1996;154(6 Pt 1):1671 [MEDLINE]
Direct comparison of inhaled nitric oxide and aerosolized prostacyclin in acute respiratory distress syndrome. Am J Respir Crit Care Med. 1996;153(3):991 [MEDLINE]
Is outcome from ARDS related to the severity of respiratory failure? Eur Respir J. 1997;10(6):1297 [MEDLINE]
Dose-response to inhaled aerosolized prostacyclin for hypoxemia due to ARDS. Chest. 2000 Mar;117(3):819-27 [MEDLINE]
Nebulized prostacyclin (PGI2) in acute respiratory distress syndrome: impact of primary (pulmonary injury) and secondary (extrapulmonary injury) disease on gas exchange response. Crit Care Med. 2001 Jan;29(1):57-62 [MEDLINE]
Aerosolized prostacyclin for acute lung injury (ALI) and acute respiratory distress syndrome (ARDS). Cochrane Database Syst Rev. 2010 [MEDLINE]
The use of inhaled prostaglandins in patients with ARDS: a systematic review and meta-analysis. Chest. 2015;147(6):1510 [MEDLINE]
Inhaled Nitric Oxide vs Epoprostenol During Acute Respiratory Failure: An Observational Target Trial Emulation. Chest. 2022 Dec;162(6):1287-1296. doi: 10.1016/j.chest.2022.08.001 [MEDLINE]
Extracorporeal membrane oxygenation in severe acute respiratory failure. A randomized prospective study. JAMA. 1979 Nov 16;242(20):2193-6 [MEDLINE]
Low-frequency positive-pressure ventilation with extracorporeal CO2 removal in severe acute respiratory failure. JAMA. 1986;256(7):881-886 [MEDLINE]
Randomized clinical trial of pressure-controlled inverse ratio ventilation and extracorporeal CO2 removal for adult respiratory distress syndrome. Am J Respir Crit Care Med. 1994 Feb;149(2 Pt 1):295-305 [MEDLINE]
Clinical predictors of and mortality in acute respiratory distress syndrome: potential role of red cell transfusion. Crit Care Med 33: 1191–1198, 2005 [MEDLINE]
Association of RBC transfusion with mortality in patients with acute lung injury. Chest 132: 1116–1123, 2007 [MEDLINE]
Venoarterial extracorporeal membrane oxygenation for treatment of cardiogenic shock: clinical experiences in 45 adult patients. J Thorac Cardiovasc Surg. 2008;135(2):382–388 [MEDLINE]
Outcomes and long-term quality-of-life of patients supported by extracorporeal membrane oxygenation for refractory cardiogenic shock. Crit Care Med. 2008;36:1404–1411 [MEDLINE]
Review of ECMO (extra corporeal membrane oxygenation) support in critically ill adult patients. Heart Lung Circ 2008;17:S41–S47. doi: 10.1016/j.hlc.2008.08.009. Epub 2008 Oct 29 [MEDLINE]
Extracorporeal Life Support Organization (ELSO). Patient Specific Supplements to the ELSO General Guidelines, 2009. https://square.umin.ac.jp/jrcm/pdf/ecmo/ecmotext12.pdf
Efficacy and economic assessment of conventional ventilatory support versus extracorporeal membrane oxygenation for severe adult respiratory failure (CESAR): a multicentre randomised controlled trial. Lancet. 2009 Oct 17;374(9698):1351-63 [MEDLINE]
Extracorporeal Membrane Oxygenation for 2009 Influenza A (H1N1) Acute Respiratory Distress Syndrome. JAMA. 2009 Nov 4;302(17):1888-95 [MEDLINE]
Extracorporeal Life Support Organization. Patient specific guidelines: a supplement to the ELSO general guidelines. April 2009:15-19 (https://www.elso.med.umich .edu/WordForms/ELSO%20P+%20Specif ic %20Guidelines.pdf)
Early and intermediate results of rescue extracorporeal membrane oxygenation in adult cardiogenic shock. Ann Thorac Surg. 2009;88(6):1897–1903 [MEDLINE]
Extracorporeal membrane oxygenation in nonintubated patients as bridge to lung transplantation. Am J Transplant 2010;10:2173–2178 [MEDLINE]
A review of the fundamental principles and evidence base in the use of extracorporeal membrane oxygenation (ECMO) in critically ill adult patients. J Intensive Care Med. 2011;26:13– 26. doi: 10.1177/0885066610384061 [MEDLINE]
Extracorporeal membrane oxygenation for ARDS in adults. N Engl J Med. 2011;365:1905–1914 [MEDLINE]
Extracorporeal membrane oxygenation for respiratory failure in adults. Curr Opin Crit Care Med. 2012;18:99–104 [MEDLINE]
Venovenous extracorporeal membrane oxygenation in adults: Practical aspects of circuits, cannulae, and procedures. J Cardiothorac Vasc Anesth 2012;26:893–909 [MEDLINE]
Venoarterial extracorporeal membrane oxygenation support for refractory cardiovascular dysfunction during severe bacterial septic shock. Crit Care Med. 2013 Jul;41(7):1616-26. doi: 10.1097/CCM.0b013e31828a2370 [MEDLINE]
Extracorporeal membrane oxygenation for severe respiratory failure in adult patients: a systematic review and meta-analysis of current evidence. J Crit Care. 2013 Dec;28(6):998-1005. doi: 10.1016/j.jcrc.2013.07.047. Epub 2013 Aug 16 [MEDLINE]
Extracorporeal Life Support Organization (ELSO) Guidelines for Adult Respiratory Failure v1.3 (2013) [LINK]
Extracorporeal life support devices and strategies for management of acute cardiorespiratory failure in adult patients: a comprehensive review. Crit Care. 2014;18(3):219–229 [MEDLINE]
Mechanical ventilation during extracorporeal membrane oxygenation. Crit Care. 2014 Jan 21;18(1):203. doi: 10.1186/cc13702 [MEDLINE]
Extracorporeal membrane oxygenation for critically ill adults. Cochrane Database Syst Rev. 2015 Jan 22;1:CD010381. doi: 10.1002/14651858.CD010381.pub2 [MEDLINE]
Roller and Centrifugal Pumps: A Retrospective Comparison of Bleeding Complications in Extracorporeal Membrane Oxygenation. ASAIO J. 2015 Sep-Oct;61(5):496-501. doi: 10.1097/MAT.0000000000000243 [MEDLINE]
Extracorporeal membrane oxygenation in adults with cardiogenic shock. Circulation. 2015;131(7): 676–680 [MEDLINE]
Setting mechanical ventilation in ARDS patients during VV-ECMO: where are we? Minerva Anestesiol. 2015 Dec;81(12):1369-76 [MEDLINE]
Contemporary extracorporeal membrane oxygenation therapy in adults: Fundamental principles and systematic review of the evidence. J Thorac Cardiovasc Surg. 2016 Jul;152(1):20-32. doi: 10.1016/j.jtcvs.2016.02.067. Epub 2016 Mar 12 [MEDLINE]
Management of refractory hypoxemia during venovenous extracorporeal membrane oxygenation for ARDS. ASAIO J. 2015 May-Jun;61(3):227-36. doi: 10.1097/MAT.0000000000000207 [MEDLINE]
Complications of Prone Positioning During Extracorporeal Membrane Oxygenation for Respiratory Failure: A Systematic Review. Respir Care. 2016 Feb;61(2):249-54. doi: 10.4187/respcare.03882. Epub 2015 Oct 13 [MEDLINE]
Long-term survival and quality of life after extracorporeal life support: a 10-year report. Eur J Cardiothorac Surg. 2017 May 18. doi: 10.1093/ejcts/ezx100 [MEDLINE]
Long-Term Survival in Adults Treated With Extracorporeal Membrane Oxygenation for Respiratory Failure and Sepsis. Crit Care Med, 2017 Feb;45(2):164-170. doi: 10.1097/CCM.0000000000002078 [MEDLINE]
Systematic review and meta-analysis of complications and mortality of venovenous extracorporeal membrane oxygenation for refractory acute respiratory distress syndrome. Ann Intensive Care. 2017 Dec;7(1):51. doi: 10.1186/s13613-017-0275-4 [MEDLINE]
Extracorporeal membrane oxygenation (ECMO) as a treatment strategy for severe acute respiratory distress syndrome (ARDS) in the low tidal volume era: A systematic review. J Crit Care. 2017 Apr 27;41:64-71. doi: 10.1016/j.jcrc.2017.04.041 [MEDLINE]
Fifty Years of Research in ARDS. Is Extracorporeal Circulation the Future of Acute Respiratory Distress Syndrome Management? Am J Respir Crit Care Med. 2017 May 1;195(9):1161-1170. doi: 10.1164/rccm.201701-0217CP [MEDLINE]
EOLIA Trial. Extracorporeal Membrane Oxygenation for Severe Acute Respiratory Distress Syndrome. N Engl J Med. 2018;378(21):1965 [MEDLINE]
Venovenous extracorporeal membrane oxygenation for acute respiratory distress syndrome: a systematic review and meta-analysis. Lancet Respir Med. 2019 Feb;7(2):163-172. doi: 10.1016/S2213-2600(18)30452-1 [MEDLINE]
ECMO for severe ARDS: systematic review and individual patient data meta-analysis. Intensive Care Med 2020;46:2048–2057 [MEDLINE]
Effect of Lower Tidal Volume Ventilation Facilitated by Extracorporeal Carbon Dioxide Removal vs Standard Care Ventilation on 90-Day Mortality in Patients With Acute Hypoxemic Respiratory Failure: The REST Randomized Clinical Trial. JAMA. 2021 Aug 31. doi: 10.1001/jama.2021.13374 [MEDLINE]
Ultra-lung-protective ventilation and biotrauma in severe ARDS patients on veno-venous extracorporeal membrane oxygenation: a randomized controlled study. Crit Care. 2022 Dec 12;26(1):383. doi: 10.1186/s13054-022-04272-x [MEDLINE]
Mortality in Patients with Obesity and ARDS Receiving ECMO: The Multicenter ECMObesity Study. Am J Respir Crit Care Med. 2023 Aug 28. doi: 10.1164/rccm.202212-2293OC [MEDLINE]
Early vvECMO implantation may be associated with lower mortality in ARDS. Respir Res. 2023 Sep 26;24(1):230. doi: 10.1186/s12931-023-02541-z [MEDLINE]
Effects of different positive end-expiratory pressure titration strategies on mechanical power during ultraprotective ventilation in ARDS patients treated with veno-venous extracorporeal membrane oxygenation: A prospective interventional study. Crit Care. 2023 Sep 8;79:154406. doi: 10.1016/j.jcrc.2023.154406 [MEDLINE]
Prone Positioning During Extracorporeal Membrane Oxygenation in Patients With Severe ARDS: The PRONECMO Randomized Clinical Trial. JAMA. 2023 Dec 1:e2324491. doi: 10.1001/jama.2023.24491 [MEDLINE]
Allogeneic Mesenchymal Stromal Cells
Treatment with allogeneic mesenchymal stromal cells for moderate to severe acute respiratory distress syndrome (START study): a randomised phase 2a safety trial. Lancet Respir Med. 2019 Feb;7(2):154-162. doi: 10.1016/S2213-2600(18)30418-1 [MEDLINE]
The timing of tracheotomy in critically ill patients undergoing mechanical ventilation: a systematic review and meta-analysis of randomized controlled trials. Chest 2011;140(6):1456–1465 [MEDLINE]
Early percutaneous tracheotomy versus prolonged intubation of mechanically ventilated patients after cardiac surgery: a randomized trial. Ann Intern Med 2011;154:373–383 [MEDLINE]
Effect of early vs late tracheostomy placement on survival in patients receiving mechanical ventilation: the TracMan randomized trial. JAMA. 2013;309:2121–2129 [MEDLINE]
Early Mobilization/Rehabilitation
Early physical and occupational therapy in mechanically ventilated, critically ill patients: a randomised controlled trial. Lancet 2009;373:1874–1882 [MEDLINE]
Muscle wasting and early mobilization in acute respiratory distress syndrome. Clin Chest Med. 2014 Dec;35(4):811-26. doi: 10.1016/j.ccm.2014.08.016 [MEDLINE]
Early, goal-directed mobilisation in the surgical intensive care unit: a randomised controlled trial. Lancet. 2016 Oct;388(10052):1377-1388 [MEDLINE]
Standardized Rehabilitation and Hospital Length of Stay Among Patients With Acute Respiratory Failure: A Randomized Clinical Trial. JAMA. 2016 Jun;315(24):2694-702 [MEDLINE]
The effects of active mobilisation and rehabilitation in ICU on mortality and function: a systematic review. Intensive Care Med. 2017 Feb;43(2):171-183. doi: 10.1007/s00134-016-4612-0 [MEDLINE]
Chest Physiotherapy with Early Mobilization may Improve Extubation Outcome in Critically Ill Patients in the Intensive Care Units. Clin Respir J. 2018 Sep 28. doi: 10.1111/crj.12965 [MEDLINE]
Early Mobilization in the Intensive Care Unit to Improve Long-Term Recovery. Crit Care Clin. 2018 Oct;34(4):557-571. doi: 10.1016/j.ccc.2018.06.005 [MEDLINE]
Effect of In-Bed Leg Cycling and Electrical Stimulation of the Quadriceps on Global Muscle Strength in Critically Ill Adults: A Randomized Clinical Trial. JAMA. 2018 Jul 24;320(4):368-378. doi: 10.1001/jama.2018.9592 [MEDLINE]
Early Mobilization of Patients in Intensive Care: Organization, Communication and Safety Factors that Influence Translation into Clinical Practice. Crit Care. 2018 Mar 20;22(1):77. doi: 10.1186/s13054-018-1998-9 [MEDLINE]
Early mobilization of critically ill patients in the intensive care unit: A systematic review and meta-analysis. PLoS One. 2019 Oct 3;14(10):e0223185. doi: 10.1371/journal.pone.0223185. eCollection 2019 [MEDLINE]
Early Active Mobilization during Mechanical Ventilation in the ICU. N Engl J Med. 2022 Nov 10;387(19):1747-1758. doi: 10.1056/NEJMoa2209083 [MEDLINE]
Association of active mobilisation variables with adverse events and mortality in patients requiring mechanical ventilation in the intensive care unit: a systematic review and meta-analysis. Lancet Respir Med. 2024 Mar 18:S2213-2600(24)00011-0. doi: 10.1016/S2213-2600(24)00011-0 [MEDLINE]
Nutritional Support
OMEGA Trial. Enteral omega-3 fatty acid, gamma-linolenic acid, and antioxidant supplementation in acute lung injury. JAMA. 2011;306:1574–1581 [MEDLINE]
A randomized trial of glutamine and antioxidants in critically ill patients. N Engl J Med. 2013;368:1489–1497 [MEDLINE]
Guidelines for the Provision and Assessment of Nutrition Support Therapy in the Adult Critically Ill Patient: Society of Critical Care Medicine (SCCM) and American Society for Parenteral and Enteral Nutrition (A.S.P.E.N.). JPEN J Parenter Enteral Nutr. 2016 Feb;40(2):159-211. doi: 10.1177/0148607115621863 [MEDLINE]
Activated Protein C
Recombinant human activated protein C in the treatment of acute respiratory distress syndrome: a randomized clinical trial. PLoS One. 2014 Mar 14;9(3):e90983. doi: 10.1371/journal.pone.0090983. eCollection 2014 [MEDLINE]