Factors Which Promote or Exacerbate Acute Respiratory Distress Syndrome (ARDS)
High Tidal Volume (VT)
Plateau Pressure >30 cm H2O
High Respiratory Rate: due to high frequency of stretch
High Rate of Stretch: due to rapid lung inflation
Monocyte Activation
Substudy of LIPS-A Trial Examining Monocyte Activation in ARDS (Am J Respir Crit Care Med, 2018) [MEDLINE]
Biomarkers of Intravascular Monocyte Activation in At-Risk patients were Associated with the Development of ARDS
Ventilator-Induced Lung Injury (VILI)
Marini and Gattinoni Have Described the Progression of Ventilator-Induced Lung Injury (VILI) as a “Shrinking of the Baby Lung”, Whereby in Lungs Subjected to Low Tidal Volume Ventilation, Tissue Moves from the Open to the Atelectatic Compartment, a Process Called the “VILI Vortex” (Crit Care, 2022) [MEDLINE]
By Way of Background, the Lung in Acute Respiratory Distress Syndrome (ARDS) is Composed of Two Distinct, Gravitationally-Separated Compartments
Dependent Lung Regions Consisting of Atelectatic and/or Edematous Airspaces
Normally Inflated Lung Tissue in Less Dependent Regions (Comprising the So-Called “Baby Lung”)
This Concept Led to the Hypothesis that Ventilating ARDS Patients Using Low Tidal Volumes (as is the Current Standard Practice) Would Protect the Baby Lung from Volutrauma Caused by Overdistension, While Simultaneously Allowing the Atelectatic Compartment to Rest and Potentially Recover
This Concept Also Assumed that an Appropriate Amount of Positive End-Expiratory Pressure (PEEP) (as is Also the Current Standard Practice), Based on Oxygenation, Could Avoid the Development of Atelectrauma
Some Have Suggested that Time-Controlled Adaptive Ventilation (TCAV) Using Airway Pressure Release Ventilation (APRV) May Enhance Lung Protection by Stabilizing Alveoli and Progressively Reopening Recalcitrant Atelectatic Lung Regions (Crit Care, 2022) [MEDLINE]
The TCAV Method to Set APRV Uses the Following
The Ratchet Approach Combined with an Extended Inspiratory Duration Necessary to Recruit Alveoli
A Brief Expiratory Duration to Brake the Derecruitment of Rapidly Collapsing Alveoli
Pathology
Pathologic Stages of Acute Respiratory Distress Syndrome (ARDS)
Early Exudative Stage (Characterized by Diffuse Alveolar Damage): first 7-10 days
Diffuse Alveolar Damage is a Nonspecific Reaction to Lung Injury by a Number of Insults (see Diffuse Alveolar Damage)
Diffuse Alveolar Damage is Characterized by Interstitial Edema, Acute/Chronic Inflammation, Type II Cell Hyperplasia, and Hyaline Membrane Formation
In Patients with Confirmed ARDS by the Berlin Definition, Approximately 45% Had Diffuse Alveolar Damage on Autopsy (Am J Respir Crit Care Med, 2013) [MEDLINE]
Fibroproliferative Stage: lasts 14-21 days
Resolution of Pulmonary Edema
Type II Alveolar Cell Proliferation
Squamous Metaplasia
Interstitial Infiltration by Myofibroblasts
Early Collagen Deposition
Fibrotic Stage
Destruction of Normal Lung Architecture
Variable Degree of Fibrosis
Cyst Formation
Diagnosis
History and Physical Exam Elements Which Should Be Explored in the Patient
Cardiac Disease (Which May Suggest Cardiogenic Pulmonary Edema)
Standardly Utilized to Assess for Hypoxemia and Hypercapnia
Arterial Blood Gas is Especially Useful in Patients in Whom SpO2 May Not Correlate Well with the Arterial pO2 (i.e. Patients in Whom the Oxygen-Hemoglobin Dissociation Curve May Be Shifted Either Left or Right, Creating an Unexpected Disparity Between the SpO2 and Arterial pO2)
Diagnose Aspiration Pneumonia (see Aspiration Pneumonia): food material in the airways may suggest aspiration as the etiology
Diagnose Lipoid Pneumonia (see Lipoid Pneumonia): lipid-laden macrophages may suggest the diagnosis (although lung biopsy is usually required ton confirm the diagnosis)
Diagnose Uncommon (or Less Easily Diagnosed) Infectious Etiologies
Bacterial Pneumonia May Be Diagnosed by Bronchoscopy Even When it is Not Suspected Clinically
Autopsy Study Demonstrated Presence of Bacterial Pneumonia in 58% of ARDS Cases, While Only 20% of These Cases were Clinically Suspected Antemortem (Chest. 1981) [MEDLINE]
May Be Useful in Cases Where Other Diagnostic Testing Has Been Negative/Inconclusive (and Patient is Clinically Worsening or Not Improving)
Clinical Efficacy
Open Lung Biopsy Can Be Performed Safely in Select Patients with ARDS and Often Reveals an Unsuspected Diagnosis, Leading to an Alteration in Therapy (Chest, 2004) [MEDLINE]: unsuspected diagnoses in the study included infection (n = 8), alveolar hemorrhage (n = 5), and bronchiolitis obliterans organizing pneumonia (n = 5)
Diffuse Alveolar Damage is Present in Most Patients with Unresolving ARDS and its Frequency is the Same Regardless of the Stage of ARDS (Mild, Moderate, Severe) (Intensive Care Med, 2015) [MEDLINE]: authors concluded that steroid therapy is not recommended
Meta-Analysis of Utility of Open Lung Biopsy in ARDS Demonstrated that Biopsy Revleaed a Wide Range of Diagnoses and was Associated with a Change in Therapy in 78% of Cases (Ann Am Thorac Soc, 2015) [MEDLINE]
The Most Common Diagnoses were “Fibrosis/Pneumonitis” (n = 155, 25%; 95% CI: 14-37%) and Infection (n = 113, 20%; 95% CI: 15-27%): viruses were the most common infectious agents (accounted for 50% of infectious cases)
Diffuse Alveolar Damage was Present in Only 16% of Specimens
Procedure-Related Complications Occurred in 29% of Patients: most commonly persistent air leak
Presence of Bilateral Pulmonary Infiltrates is Required for the Diagnosis of ARDS
Dependent Atelectasis May Be Present
Chest CT Findings Correlate with Prone Positioning Oxygenation Response
In a Study of Moderate-Severe ARDS (n = 96), a Greater Difference in the Extent of Consolidation Along the Dependent-Independent Axis (i.e. Median Dorsal-Ventral Difference) on Chest CT Scan was Associated with Subsequent Prone Positioning Oxygenation Response, But Not with the 60-Day Mortality Rate (BMC Pulm Med, 2022) [MEDLINE]
High Total Ground Glass Opacity Scores (≥15) were Associated an Increased 60-Day Mortality Rate (Odds Ratio 4.07; 95% Confidence Interval: 1.39-11.89; p = 0.010)
May Be Useful to Evaluate for Pleural Effusion, B-Lines (Which are Believed to Represent Thickened Interlobular Septae), etc
Clinical Efficacy
Study of Interobserver Variability in the Radiographic Diagnosis of Acute Respiratory Distress Syndrome (ARDS) (Chest, 1999) [MEDLINE]
The Radiographic Criterion used in the Current AECC Definition for ALI/ARDS Showed High Interobserver Variability when Applied by Expert iInvestigators in the Fields of Mechanical Ventilation and ARDS
Study of Comparative Accuracy of Chest X-Ray vs Chest CT in the Diagnosis of Acute Respiratory Distress Syndrome (ARDS) (J Crit Care, 2013) [MEDLINE]
Chest X-Ray (as Compared to Chest CT)
Sensitivity: 73%
Specificity: 70%
Positive Predictive Value: 88%
Negative Predictive Value: 47%
Female Sex was Associated with Higher Sensitivity and Lower Specificity
Retrospective, Observational Study of Chest CT in Diagnosing Acute Respiratory Distress Syndrome (ARDS) (Respir Care, 2016) [MEDLINE]
In Patients with ARDS, the Most Common Pathologic Findings of the Lung Parenchyma were Consolidation (94.1% of Cases) and Ground-Glass Infiltrates (85.3% of Cases)
Other CT Scan Findings
Pleural Effusions (80.4%)
Mediastinal Lymphadenopathy (66.7%)
Signs of Right Ventricular Strain and Pulmonary Hypertension (53.9%)
Pericardial Effusion (37.3%)
Subcutaneous Emphysema (12.3%)
Pneumothorax (11.8%)
Pneumomediastinum (7.4%)
Pulmonary Embolism (2.5%)
Results of Chest CT Scans Led to Changes in Management in 26.5% of ARDS Cases
Study of Chest X-Ray Diagnosis of Acute Respiratory Distress Syndrome (ARDS) (Crit Care Med, 2018) [MEDLINE]: n = 463
Radiographic Criteria for Acute Respiratory Distress Syndrome Have Been Criticized for Poor Reliability
Only 56% of Observers Correctly Identified ARDS on Chest X-Ray Studies
An Educational Intervention Did Not Improve the Rate of Successful Identification (58%)
Overall Agreement Between Raters was 0.296 for the Educational intervention Group and 0.272 for the Control Group (p < 0.001)
Often Useful to Rule Out Cardiac Etiology of Cardiogenic Pulmonary Edema: however, it is probably not useful in isolation
Prospective Study of BNP in Sepsis (Crit Care Med, 2006) [MEDLINE]
In patients with Severe Sepsis/Septic Shock, BNP and N-Terminal Pro-BNP Values are Highly Elevated and (Despite Significant Hemodynamic Differences) Comparable with Those Found in Acute Heart Failure Patients
Prospective Cohort Study of Diagnostic Value of BNP in Critically Ill Patients with Pulmonary Edema (Crit Care, 2008) [MEDLINE]: n= 54
BNP Level Drawn within 48 hrs of ICU Admission Do Not Reliably Distinguish ARDS from Cardiogenic Pulmonary Edema, Do Not Correlate with Invasive Hemodynamics, and Daily Measurements Do Not Track Predictably with Volume Status
BNP<100 pg/mL Identified ARDS with Sensitivity of 27%/Specificity of 95%
May Be Useful in Select Cases to Rule Out Cardiac Etiology (of Cardiogenic Pulmonary Edema)
Clinical Efficacy
Study of Pulmonary Capillary Wedge Pressure in Acute Respiratory Distress Syndrome (Intensive Care Med, 2002) [MEDLINE]
Median PCWP was 16.6 mm Hg in ARDS Patients
Patients Who Met Standard Criteria for ARDS Were More Likely to Have a High PCWP
PCWP >18 mm Hg was a Strong Predictor of Mortality in ARDS Patients (After Correction of Baseline Differences)
Study of Swan-Ganz Catheter to Guide Treatment of Acute Respiratory Distress Syndrome (N Engl J Med, 2006) [MEDLINE]
Swan-Ganz Catheter-Guided Therapy Did Not Improve Mortality Rate or Organ Function, But was Associated with More Complications than Central Venous Catheter-Guided Therapy
Study of Swan-Ganz Catheter in Shock and ARDS (JAMA, 2003) [MEDLINE]
Early Use of Swan-Ganz Catheter Did Not Improve Morbidity or Mortality in Patients with Shock and/or ARDS
Recommendations (2016 Surviving Sepsis Guidelines; Intensive Care Med, 2017) [MEDLINE]
Swan-Ganz Catheter is Not Routinely Recommended in the Management of Sepsis-Associated ARDS (Strong Recommendation, High Quality of Evidence)
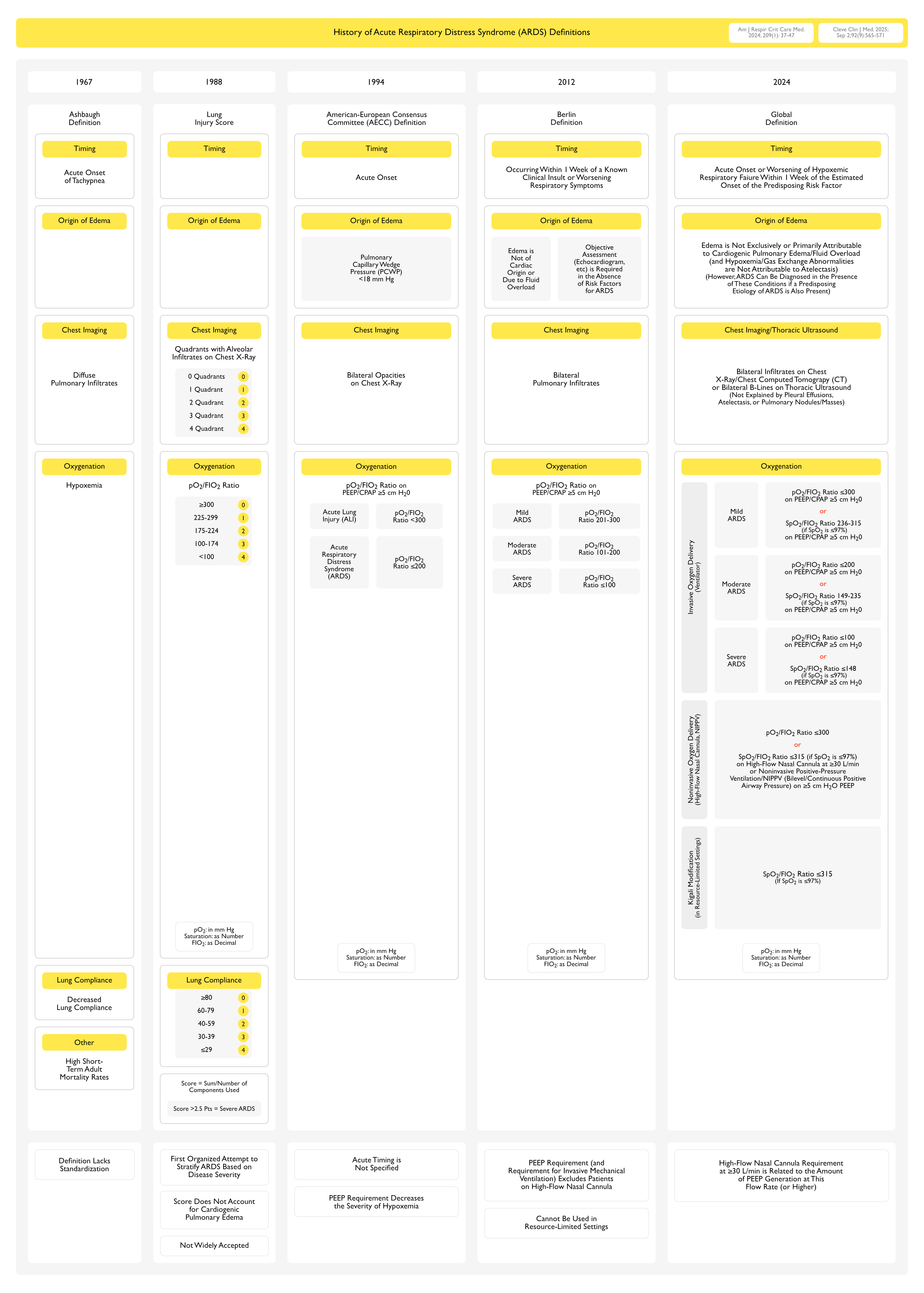
Clinical: Global Definition of Acute Respiratory Distress Syndrome (ARDS) (Am J Respir Crit Care Med, 2024) [MEDLINE] (Cleve Clin J Med, 2025) [MEDLINE]
Criteria Which Apply to All Acute Respiratory Distress Syndrome (ARDS) Categories
Risk Factors and Origin of Edema
Precipitated by an Acute Predisposing Risk Factor (Such as Pneumonia, Non-Pulmonary Infection, Trauma, Transfusion, Aspiration, or Shock)
Pulmonary Edema is Not Exclusively or Primarily Attributable to Cardiogenic Pulmonary Edema/Fluid Overload and Hypoxemia/Gas Exchange Abnormalities are Not Primarily Attributable to Atelectasis
However, Acute Respiratory Distress Syndrome (ARDS) Can Be Diagnosed in the Presence of These Conditions if a Predisposing Risk Factor for Acute Respiratory Distress Syndrome (ARDS) is Also Present
Timing
Acute Onset or Worsening of Hypoxemic Respiratory Failure within 1 Week of the Estimated Onset of the Predisposing Risk Factor (or New or Worsening Respiratory Symptoms)
This Recognizes that the Onset May Be More Indolent for Some Insults (Such as COVID-19, etc)
Chest Imaging
Bilateral Opacities on Chest Radiography and Computed Tomography or Bilateral B Lines and/or Consolidations on Thoracic Ultrasound (Not Fully Explained by Pleural Effusions, Atelectasis, or Nodules/Masses)
Criteria Which Apply to Specific Acute Respiratory Distress Syndrome (ARDS) Categories
Patients Who Meet All Other Criteria of the Berlin Definition, Except for the Requirement of Mechanical Ventilation Have Been Found to Have a Similar Mortality Rate, and the Degree of Hypoxemia Itself Relates More to the Overall Clinical Trajectory of the Patient (Respir Care, 2015) [MEDLINE] (Am J Respir Crit Care Med, 2017) [MEDLINE] (Lancet Respir Med, 2021 [MEDLINE]
The 60-Day Acute Respiratory Distress Syndrome (ARDS) Mortality Outcomes are Similar Between Patients Meeting Diagnostic Criteria for Acute Respiratory Distress Syndrome (ARDS) Who Were Initially Not Intubated vs Those Patients Who Were Initially Intubated Early (Crit Care Med, 2016) [MEDLINE]
General Comments
Estimated FIO2 = Ambient FIO2 (0.21) + 0.03 x O2 Flow Rate (in L/min)
Blood Gas and Oximetry Measurements Should Be Made When the Patient is at Rest and ≥30 min After Changes in Position, FIO2, and/or Flow Rate
For Pulse Oximetry
Ensure an Adequate Waveform and Oximeter Placement
SpO2/FIO2 Ratio is Not Valid for SpO2 >97%
Pulse Oximetry is Not Recommended for Diagnosis of Acute Respiratory Distress Syndrome (ARDS) if a Hemoglobin Abnormality (Methemoglobinemia, Carboxyhemoglobinemia, etc) is Suspected
pO2/FIO2 Ratio ≤300 on High-Flow Nasal Cannula with a Minimum Flow Rate of ≥30 L/min or Noninvasive Positive-Pressure Ventilation (NIPPV) (on Either Bilevel Positive Airway Pressure or Continuous Positive Airway Pressure) with a Minimum of 5 cm H2O of End-Expiratory Pressure
The Criterion of High-Flow Nasal Cannula 30 L/min is Based on Studies Which Demonstrate that This Level of Support Generates Low Levels of PEEP (Aust Crit Care, 2007) [MEDLINE]
Alternate: Oxygen Saturation as Measured by Pulse Oximetry SpO2/FIO2 ≤315 (if Oxygen Saturation as Measured by Pulse Oximetry is ≤97%) on High-Flow Nasal Cannula with a Minimum Flow Rate of ≥30 L/min or Noninvasive Positive-Pressure Ventilation (NIPPV) (on Either Bilevel Positive Airway Pressure or Continuous Positive Airway Pressure) with a Minimum of 5 cm H2O of Positive End-Expiratory Pressure
Blood Gas and Oximetry Measurements Should Be Made When the Patient is at Rest and ≥30 min After Changes in Position, FIO2, and/or Flow Rate
For Pulse Oximetry
Ensure an Adequate Waveform and Oximeter Placement
SpO2/FIO2 Ratio is Not Valid for SpO2 >97%
Pulse Oximetry is Not Recommended for Diagnosis of Acute Respiratory Distress Syndrome (ARDS) if a Hemoglobin Abnormality (Methemoglobinemia, Carboxyhemoglobinemia, etc) is Suspected
Categories (on PEEP ≥5 cm H2O): patients may move from one category to another during the ourse of disease
Mild: pO2/FIO2 Ratio >200 and ≤300
Alternate (Requires SpO2 ≤97%): SpO2/FIO2 Ratio >235 and ≤315
Moderate: pO2/FIO2 Ratio >100 and ≤200
Alternate (Requires SpO2 ≤97%): SpO2/FIO2 Ratio >148 and ≤235
Severe: pO2/FIO2 Ratio ≤100
Alternate (Requires SpO2 ≤97%): SpO2/FIO2 Ratio ≤148
Kigali Modification for the Diagnosis of Acute Respiratory Distress Syndrome (ARDS) in Resource-Limited Settings
General Comments (Am J Respir Crit Care Med, 2016) [MEDLINE]
Since Many Resource-Constrained Hospitals in the World Do Not Have Invasive Mechanical Ventilation to Administer Positive End-Expiratory Pressure (PEEP), an Arterial Blood Gas (ABG) Analyzer to Measure pO2, and Chest Radiography to Detect Pulmonary Infiltrates, These Limitations May Lead to the Underestimation of the True Incidence of Acute Respiratory Distress Syndrome (ARDS) in Resourced-Constrained Settings and, Therefore, Present an Obstacle to Treatment
The Kigali Modification Addresses These Constraints
Hypoxemia is Defined as SpO2/FIO2 Ratio ≤315 (Only Applicable if the SpO2 is ≤ 97% and There is an Absence of Any Hemoglobin Disorder)
No PEEP Requirement
Pulmonary Opacities Can Be Diagnosed Using Thoracic Ultrasound (Instead of Chest X-Ray) (see Thoracic Ultrasound)
Using the Kigali Modification in a Prospective Study in Rwanda, 4% of Hospitalized Patients were Found to Have Acute Respiratory Distress Syndrome (ARDS), with a Hospital Mortality Rate of 50% (Am J Respir Crit Care Med, 2016) [MEDLINE]
None of These Patients Would Have Been Diagnosed with Acute Respiratory Distress Syndrome (ARDS) Using the Berlin Criteria
Blood Gas and Oximetry Measurements Should Be Made When the Patient is at Rest and ≥30 min After Changes in Position, FIO2, and/or Flow Rate
For Pulse Oximetry (SpO2)
Ensure an Adequate Waveform and Oximeter Placement
SpO2/FIO2 Ratio is Not Valid for SpO2 >97%
Pulse Oximetry is Not Recommended for Diagnosis of Acute Respiratory Distress Syndrome (ARDS) if a Hemoglobin Abnormality (Methemoglobinemia, Carboxyhemoglobinemia, etc) is Suspected
SpO2/FIO2 Ratio ≤315 (Only Applicable if SpO2 is ≤97%)
Neither Positive End-Expiratory Pressure Nor a Minimum Oxygen Flow Rate is Required for Diagnosis in Resource-Limited Settings
Critiques of the Prior Berlin Definition (Some of Which Apply to the Global Defintion, as Well) (Crit Care, 2022) [MEDLINE]
Berlin Definition Requires the Use of Invasive Mechanical Ventilation to Administer Positive End-Expiratory Pressure (PEEP), an Arterial Blood Gas Analyzer to Measure pO2, and Chest Radiography to Detect Pulmonary Infiltrates
Since Many Resource-Constrained Hospitals in the World Do Not Have These Capabilities, These Limitations May Lead to the Underestimation of the True Incidence of Acute Respiratory Distress Syndrome (ARDS) in Resourced-Constrained Settings and, Therefore, Present an Obstacle to Treatment
In Addition, Patients Who Meet All Other Criteria of the Berlin Definition, Except for the Requirement of Mechanical Ventilation Have Been Found to Have a Similar Mortality Rate, and the Degree of Hypoxemia Itself Relates More to the Overall Clinical Trajectory of the Patient (Respir Care, 2015) [MEDLINE] (Am J Respir Crit Care Med, 2017) [MEDLINE] (Lancet Respir Med, 2021 [MEDLINE]
The 60-Day Acute Respiratory Distress Syndrome (ARDS) Mortality Outcomes are Similar Between Patients Meeting Diagnostic Criteria for Acute Respiratory Distress Syndrome (ARDS) Who Were Initially Not Intubated vs Those Patients Who Were Initially Intubated Early (Crit Care Med, 2016) [MEDLINE]
Berlin Definition Timing Criteria are Problematic
The Use of a 7 Day Latency from a Known Clinical Insult is Arbitrary and is Not Evidence-Based
For Example, the Onset of Respiratory Failure in Severe Acute Respiratory Syndrome Coronavirus-2 (SARS-CoV2, COVID 2019) is Typically 8-12 Days After the First Symptoms (Crit Care, 2020) [MEDLINE]
Berlin Definition Chest Imaging Criteria are Problematic
Study of Chest X-Ray Diagnosis of Acute Respiratory Distress Syndrome (Crit Care Med, 2018) [MEDLINE]: n = 463
Radiographic Criteria for Acute Respiratory Distress Syndrome (ARDS) Have Been Criticized for Poor Reliability
Only 56% of Observers Correctly Identified Acute Respiratory Distress Syndrome (ARDS) on Chest X-Ray Studies
An Educational Intervention Did Not Improve the Rate of Successful Identification (58%)
Overall Agreement Between Raters was 0.296 for the Educational intervention Group and 0.272 for the Control Group (p < 0.001)
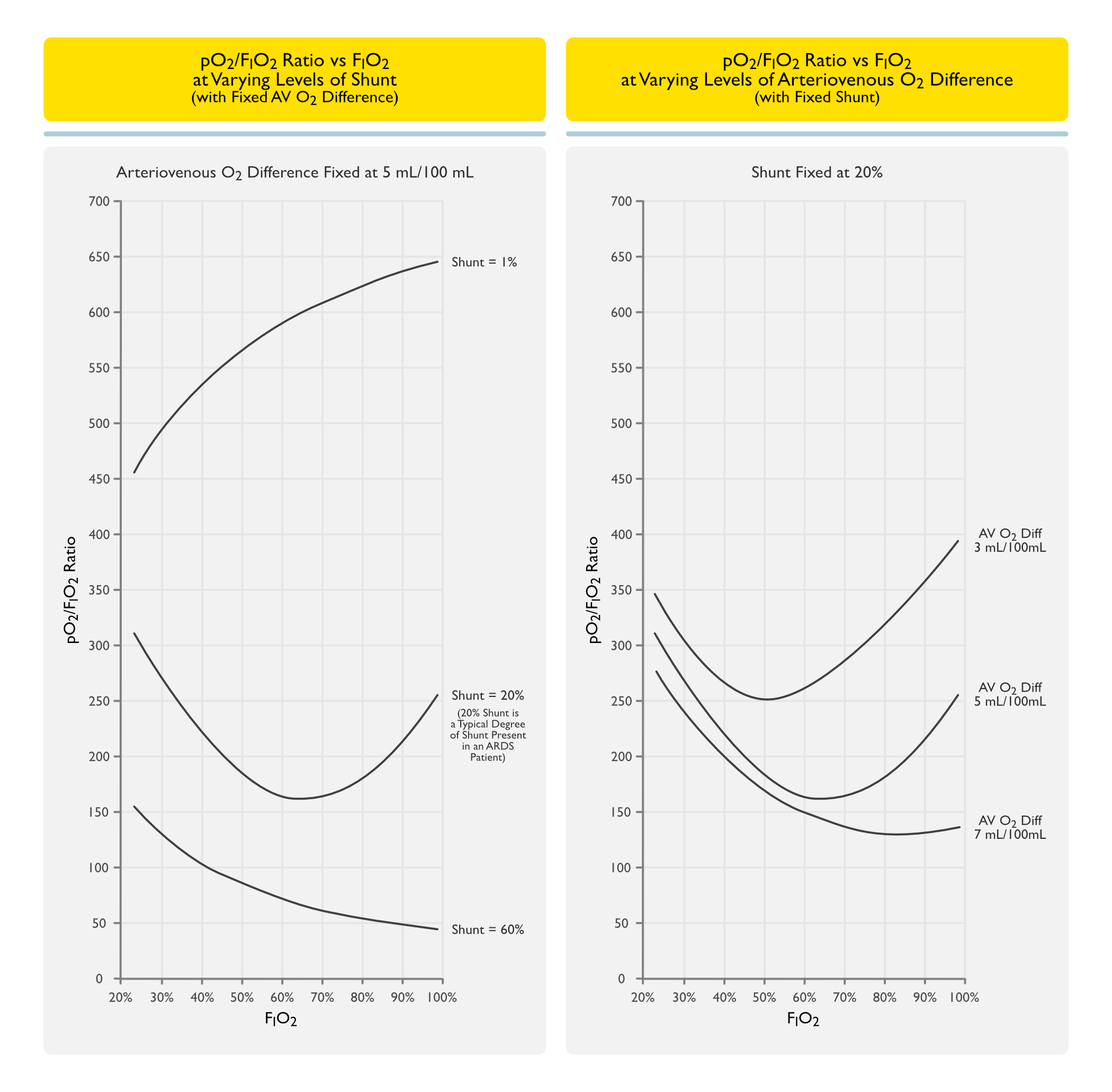
Berlin Definition Oxygenation Criteria are Problematic
pO2 has a Curvilinear Relationship with FIO2 (Am Rev Respir Dis, 1977) [MEDLINE] (Clin Chest Med, 1982) [MEDLINE]
pO2/FIO2 Ratio Varies with the Degree of Ventilation/Perfusion Mismatch and Intrapulmonary Shunt
In Patients with Acute Respiratory Distress Syndrome (ARDS) and a Fixed Degree of Intrapulmonary Shunt, Changes in FIO2 Cause the pO2/FIO2 Ratio to Fluctuate Unpredictably by >100 mm Hg (Crit Care Med, 1997) [MEDLINE]
In Acute Respiratory Distress Syndrome (ARDS) Clinical Trials in Which Ventilator Settings were Standardized, >50% of Patients Screened Demonstrated Adequate Improvement in the P/F Ratio within 30 min of Putting the Patient on the Ventilator that the Patient No Longer Met the Criteria for Acute Respiratory Distress Syndrome (ARDS) (Intensive Care Med, 2004) [MEDLINE]
Clinical: Practical Daily Assessment of Respiratory Failure
While Low-Grade Diffuse Alveolar Hemorrhage May Occur in Some Cases of ARDS, the Presence of Significant Hemoptysis Requires that Diffuse Alveolar Hemorrhage is Ruled Out as a Primary Disorder
Diagnosis
Bronchoscopy (see Bronchoscopy): routinely used to evaluate hemoptysis in the setting of ARDS
Presence of Fever (or Hypothermia) is Associated with Delayed Liberation from Mechanical Ventilation
Analysis of Prospective Cohort Study Evaluating the Impact of Fever on Ventilator Weaning in Patients with Acute Respiratory Distress Syndrome (Ann Am Thorac Soc, 2013) [MEDLINE]: n = 450 (from 13 ICU’s at 4 hospitals in Baltimore, Maryland)
Only 12% of Patients were Normothermic During the First 3 Days After Onset of Acute Respiratory Distress Syndrome
Fever was Associated with Delayed Liberation from Mechanical Ventilation
During the First Week Post-Acute Respiratory Distress Syndrome, Each Additional Day of Fever Resulted in a 33% Reduction in the Likelihood of Successful Ventilator Liberation (95% Confidence Interval for Adjusted Hazard Ratio, 0.57-0.78; P<0.001
Hypothermia was Associated with Delayed Liberation from Mechanical Ventilation and Increased Mortality Rate
Hypothermia was Independently Associated with Decreased Ventilator-Free Days (Hypothermia During Each of the First 3 Days: Reduction of 5.58 Days, 95% CI: -9.04 to -2.13; P = 0.002)
Hypothermia was Independently Associated with Increased Mortality (Hypothermia During Each of the First 3 Days: Relative Risk, 1.68; 95% CI: 1.06-2.66; P = 0.03)
Delirium is a Common Complication in Critical Illness (Both as a Component of the Primary Disease Process and as a Result of Treatments Such as Sedation, etc)
BRAIN-ICU Study (NEJM, 2013) [MEDLINE]: in a study of patients with respiratory failure or shock in the medical or surgical intensive care unit (n = 821), 74% of cases had delirium
Generalized Weakness is a Common Complication of Critical Illness with Prolonged Immobilization
Study of Vasoactive Medications in Mechanically-Ventilated Patients (Chest, 2018) [MEDLINE]: in mechanically-ventilated patients, the use of vasoactive medications was associated with an increased risk of ICU-acquired weakness
Sleep Disturbance
Epidemiology
May Occur as a Complication in a Critically Ill Patient
AKI Occurs in Approximately 68% of ARDS Patients (After ARDS Onset) (Ann Intensive Care, 2019) [MEDLINE]
Retrospective Study of Risk Factors for the Development of AKI in Patients with ARDS (Ann Intensive Care, 2019) [MEDLINE]: n = 357
Approximately 24.6% of Patients had Stage I AKI, 27% had stage II AKI, and 48.4% had Stage III AKI
Median Time of AKI Onset for Stage I AKI was 2 Days (Interquartile Range: 1.5–5.5), While Stage II and III AKI was 4 Days
Risk Factors
Acidosis (on Day 1 of ARDS): subdistribution hazard ratio per 0.1 units decrease was 1.18 (95% CI: 1.05–1.32)
Age: subdistribution hazard ratio 1.01 (95% CI: 1.00–1.02)
Higher Severity of Illness (SOFA Score): subdistribution hazard ratio 1.16 (95% CI: 1.12–1.21)
History of Diabetes Mellitus (see Diabetes Mellitus): subdistribution hazard ratio 1.42 (95% CI: 1.07–1.89)
Prevention
General Comments
Prevention of Acute Respiratory Distress Syndrome (ARDS) is an Important Clinical Goal, Since the Radiographic Identification of the Findings of Acute Respiratory Distress Syndrome (ARDS) is Generally Unreliable (Crit Care Med, 2018) [MEDLINE]
LIPS-A (Phase 2b) Trial of Aspirin to Prevent Acute Respiratory Distress Syndrome (ARDS) in Patients Presenting to the ED Who are At-Risk for Acute Respiratory Distress Syndrome (ARDS) (JAMA, 2016) [MEDLINE]
Aspirin Administered to At-Risk Patients in the Emergency Department Had No Clinical Benefit in the Prevention of ARDS at 7 Days
Low Tidal Volume Ventilation
IMPROVE Trial of Low Tidal Volume Ventilation in Abdominal Surgery Patients at Risk for Acute Respiratory Distress Syndrome (ARDS) (N Engl J Med, 2013) [MEDLINE]
As Compared with Nonprotective Mechanical vVentilation, the Lung Protective Ventilation in Intermediate/High-Risk Patients Undergoing Major Abdominal Surgery was Associated with Improved Clinical Outcomes and Decreased Health Care Utilization
Meta-Analysis of Low Tidal Volume Ventilation in Patients without Acute Respiratory Distress Syndrome (ARDS) (Intensive Care Med, 2014) [MEDLINE]
Use of Lower Tidal Volumes in Patients without ARDS at the Onset of Mechanical Ventilation Could Be Associated with a Shorter Duration of Ventilation
Use of Lower Tidal Volumes Seems No to Affect Sedation or Analgesia Needs, But This Must Be Confirmed in a Robust, Well-Powered Randomized Controlled Trial
Meta-Analysis of Efficacy of Intraoperative Low Tidal Volume Ventilation in Preventing Postoperative Pulmonary Complications (Ann Surg, 2016) [MEDLINE]: n = 1054 (16 studies)
Intraoperative Low Tidal Volume Ventilation in Conjunction with PEEP and Recruitment Maneuvers Improved Clinical Pulmonary Outcomes (Atelectasis, Lung Infection, Acute Lung Injury) and Decreased Hospital Length of Stay in Otherwise Healthy Patients Undergoing General Surgery
PReVENT Trial Comparing Low (7 mL/kg PBW) vs Intermediate (9 mL/kg PBW) Tidal Volume Ventilation in ICU Patients at Risk for Acute Respiratory Distress Syndrome (ARDS) (JAMA, 2018) [MEDLINE]: n = 961 (6 centers)
Study Design
The Majority of Patients were Randomized within 1 hr of Start of Mechanical Ventilation
Only Patients Who were Not Expected to Be Extubated within 24 hrs of Randomization were Included in the Trial
Low Tidal Volume Group Used Higher Tidal Volume (7 mL/kg PBW) than in Other Similar Studies (Which Generally Used 6 mL/kg PBW), Because Pressure Support was Used More Frequently in this Group
By Day 1, 58% of Patients in the Low Tidal Volume Group were Receiving Pressure Support Ventilation (Which Allowed Large Spontaneous Tidal Volumes if the Patients were on Minimal Ventilatory Support)
On Day 1, 59% of Patient in the Low Tidal Volume Group Received a Tidal Volume >6 mL/kg PBW and 14% of Patients Received a Tidal Volume >9.5 mL/kg PBW
On Days 1 and 2, Respectively, Estimates Suggest that Only 25% and 25% of Patients in the Intermediate Tidal Volume Group Received Tidal Volumes >10 mL/kg PBW
In ICU Patients without ARDS, There was No Difference Between Low Tidal Volume Ventilation Strategy (7 mL/kg PBW) and Intermediate Tidal Volume Ventilation Strategy (9 mL/kg PBW), in Terms of Ventilator-Free Days at Day 28
In ICU Patients without ARDS, There was No Difference Between Low Tidal Volume Ventilation Strategy (7 mL/kg PBW) and Intermediate Tidal Volume Ventilation Strategy (9 mL/kg PBW), in Terms of ICU Length of Stay, Hospital Length of Stay, 90-Day Mortality, Incidence of ARDS, Incidence of Pneumonia, Incidence of Severe Atelectasis, and Incidence of Pneumothorax
Possible Explanations for Lack of Effect of the Low Tidal Volume Ventilation Strategy
The Low Tidal Volume Ventilation Strategy was Associated with Respiratory Acidosis, Which Might Have Influenced the Duration of Ventilation
Driving Pressure in the Intermediate Volume Ventilation Strategy was Still within a Protective Range for Patients without ARDS
Critique
Some Experts Have Suggested that the PReVENT Trial Demonstrates that a Negative Trial May Be the Result of Inadequate Separation Between Interventions
References
Physiology
Ventilator-related causes of lung injury: the mechanical power. Intensive Care Med. 2016;42 (10):1567-1575 [MEDLINE]
Early Intravascular Events Are Associated with Development of Acute Respiratory Distress Syndrome. A Substudy of the LIPS-A Clinical Trial. Am J Respir Crit Care Med. 2018 Jun 15;197(12):1575-1585. doi: 10.1164/rccm.201712-2530OC [MEDLINE]
Unshrinking the baby lung to calm the VILI vortex. Crit Care. 2022 Aug 7;26(1):242. doi: 10.1186/s13054-022-04105-x [MEDLINE]
Diagnosis
General
Diagnosis of nosocomial bacterial pneumonia in acute, diffuse lung injury. Chest. 1981;80(3):254 [MEDLINE]
The Randomized Educational Acute Respiratory Distress Syndrome Diagnosis Study: A Trial to Improve the Radiographic Diagnosis of Acute Respiratory Distress Syndrome. Crit Care Med. 2018 May;46(5):743-748. doi: 10.1097/CCM.0000000000003000 [MEDLINE]
Interobserver variability in applying a radiographic definition for ARDS. Chest. 1999 Nov;116(5):1347-53 [MEDLINE]
Accuracy of the chest radiograph to identify bilateral pulmonary infiltrates consistent with the diagnosis of acute respiratory distress syndrome using computed tomography as reference standard. J Crit Care. 2013 Aug;28(4):352-7. doi: 10.1016/j.jcrc.2012.12.002 [MEDLINE]
Imaging of Acute Lung Injury. Radiol Clin North Am. 2016 Nov;54(6):1119-1132. doi: 10.1016/j.rcl.2016.05.006 [MEDLINE]
Congestive heart failure and adult respiratory distress syndrome. New insights using computed tomography. Radiol Clin North Am. 1996;34(1):33 [MEDLINE]
Computed tomography in adult respiratory distress syndrome: what has it taught us? Eur Respir J. 1996;9(5):1055 [MEDLINE]
Accuracy of the chest radiograph to identify bilateral pulmonary infiltrates consistent with the diagnosis of acute respiratory distress syndrome using computed tomography as reference standard. J Crit Care. 2013 Aug;28(4):352-7. doi: 10.1016/j.jcrc.2012.12.002 [MEDLINE]
Value of Computed Tomography of the Chest in Subjects With ARDS: A Retrospective Observational Study. Respir Care. 2016 Mar;61(3):316-23. doi: 10.4187/respcare.04308 [MEDLINE]
Prognostic value of computed tomographic findings in acute respiratory distress syndrome and the response to prone positioning. BMC Pulm Med. 2022;22(1):71. doi:10.1186/s12890-022-01864-9 [MEDLINE]
High values of the pulmonary artery wedge pressure in patients with acute lung injury and acute respiratory distress syndrome. Intensive Care Med. 2002;28(8):1073 [MEDLINE]
Early use of the pulmonary artery catheter and outcomes in patients with shock and acute respiratory distress syndrome: a randomized controlled trial. JAMA. 2003;290(20):2713 [MEDLINE]
Pulmonary-artery versus central venous catheter to guide treatment of acute lung injury. N Engl J Med. 2006;354(21):2213 [MEDLINE]
Comparable increase of B-type natriuretic peptide and amino-terminal pro-B-type natriuretic peptide levels in patients with severe sepsis, septic shock, and acute heart failure. Crit Care Med. 2006;34(8):2140 [MEDLINE]
Diagnostic utility of B-type natriuretic peptide in critically ill patients with pulmonary edema: a prospective cohort study. Crit Care. 2008;12(1):R3 [MEDLINE]
Acute eosinophilic pneumonia with respiratory failure: a new syndrome? Am Rev Respir Dis. 1992;145(3):716 [MEDLINE]
Acute eosinophilic pneumonia. A summary of 15 cases and review of the literature. Medicine (Baltimore). 1996;75(6):334 [MEDLINE]
Diagnosis of nosocomial bacterial pneumonia in acute, diffuse lung injury. Chest. 1981;80(3):254 [MEDLINE]
Idiopathic acute eosinophilic pneumonia: a study of 22 patients. Am J Respir Crit Care Med. 2002;166(9):1235 [MEDLINE]
Lung Biopsy
Open-lung biopsy in patients with acute respiratory distress syndrome. Anesthesiology. 1998;88(4):935 [MEDLINE]
Combined bronchoalveolar lavage and transbronchial lung biopsy: safety and yield in ventilated patients. Eur Respir J. 2003;21(3):489 [MEDLINE]
The role of open-lung biopsy in ARDS. Chest. 2004;125(1):197 [MEDLINE]
Yield and safety of bedside open lung biopsy in mechanically ventilated patients with acute lung injury or acute respiratory distress syndrome. Surgery. 2008 Mar;143(3):426-33 [MEDLINE]
Open lung biopsy in nonresolving ARDS frequently identifies diffuse alveolar damage regardless of the severity stage and may have implications for patient management. Intensive Care Med. 2015 Feb;41(2):222-30 [MEDLINE]
Open Lung Biopsy Among Critically Ill, Mechanically Ventilated Patients. A Metaanalysis. Ann Am Thorac Soc. 2015;12(8):1226 [MEDLINE]
The Role of Open Lung Biopsy in Critically Ill Patients with Hypoxic Respiratory Failure: A Retrospective Cohort Study. Can Respir J. 2016;2016:8715024 [MEDLINE]
Utility of surgical lung biopsy in critically ill patients with diffuse pulmonary infiltrates: a retrospective review. Intern Med J. 2016;46(11):1306 [MEDLINE]
Clinical Manifestations
General
State of the art: ventilation-perfusion relationships. Am Rev Respir Dis. 1977;116(5):919–43 [MEDLINE]
Gas exchange in the adult respiratory distress syndrome. Clin Chest Med. 1982;3(1):57–67 [MEDLINE]
Incidence, site, and outcome of infections in patients with the adult respiratory distress syndrome. Am Rev Respir Dis. 1986;134(1):12 [MEDLINE]
Nosocomial pneumonia in ventilated patients: a cohort study evaluating attributable mortality and hospital stay. Am J Med. 1993;94(3):281 [MEDLINE]
The effect of late-onset ventilator-associated pneumonia in determining patient mortality. Chest. 1995;108(6):1655 [MEDLINE]
Nosocomial pneumonia and mortality among patients in intensive care units. JAMA. 1996;275(11):866 [MEDLINE]
Variability of indices of hypoxemia in adult respiratory distress syndrome. Crit Care Med. 1997;25(1):41–5 [MEDLINE]
“Imitators” of the ARDS: implications for diagnosis and treatment. Chest. 2004;125(4):1530 [MEDLINE]
Comparison of the SpO2/FIO2 ratio and the PaO2/FIO2 ratio in patients with acute lung injury or ARDS. Chest. 2007;132(2):410 [MEDLINE]
Acute respiratory distress syndrome: the Berlin Definition. JAMA. 2012 Jun 20;307(23):2526-33 [MEDLINE]
The acute respiratory distress syndrome: what’s in a name? JAMA 2012;307:2542–2544 [MEDLINE]
Berlin definition of ARDS: an expanded rationale, justification, and supplementary material. Intensive Care Med. 2012 Oct;38(10):1573-82 [MEDLINE]
Comparison of the Berlin definition for acute respiratory distress syndrome with autopsy. Am J Respir Crit Care Med. 2013;187(7):761 [MEDLINE]
Nonlinear Imputation of PaO2/FIO2 From SpO2/FIO2 Among Mechanically Ventilated Patients in the ICU: A Prospective, Observational Study. Crit Care Med. 2017;45(8):1317 [MEDLINE]
Acute respiratory failure in COVID-19: is it “typical” ARDS? Crit Care. 2020;24(1):198 [MEDLINE]
ARDS: hidden perils of an overburdened diagnosis. Crit Care. 2022 Dec 17;26(1):392. doi: 10.1186/s13054-022-04271-y [MEDLINE]
A New Global Definition of Acute Respiratory Distress Syndrome. Am J Respir Crit Care Med. 2024 Jan 1;209(1):37-47. doi: 10.1164/rccm.202303-0558WS [MEDLINE]
Intensive Care Unit (ICU)-Acquired Weakness
Impact of Vasoactive Medications on ICU-Acquired Weakness in Mechanically Ventilated Patients Chest. 2018 Oct;154(4):781-787. doi: 10.1016/j.chest.2018.07.016 [MEDLINE]
Ventilator-Induced Lung Injury (VILI)/Barotrauma
Incidence of pulmonary barotrauma in a medical ICU. Crit Care Med. 1983;11(2):67 [MEDLINE]
Persistent bronchopleural air leak during mechanical ventilation. A review of 39 cases. Chest. 1986;90(3):321 [MEDLINE]
The effects of ventilatory pattern on hyperinflation, airway pressures, and circulation in mechanical ventilation of patients with severe air-flow obstruction. Am Rev Respir Dis. 1987 Oct;136(4):872-9 [MEDLINE]
Closure of a bronchopleural fistula with bronchoscopic instillation of tetracycline. Chest. 1991;99(4):1040 [MEDLINE]
Mean airway pressure: physiologic determinants and clinical importance–Part 2: Clinical implications. Crit Care Med. 1992;20(11):1604 [MEDLINE]
Risk factors for morbidity in mechanically ventilated patients with acute severe asthma. Am Rev Respir Dis. 1992;146(3):60 [MEDLINE]
Pulmonary barotrauma in mechanical ventilation: patterns and risk factors. Chest 1992; 102:568-572
Barotrauma: detection, recognition, and management. Chest 1993; 104:578-584
Continuous venous air embolism in patients receiving positive end-expiratory pressure. Am Rev Respir Dis. 1993;147(4):1034 [MEDLINE]
Mechanisms of ventilator-induced lung injury. Crit Care Med. 1993;21(1):131 [MEDLINE]
Lung structure and function in different stages of severe adult respiratory distress syndrome. JAMA. 1994;271(22):1772 [MEDLINE]
Peak airway pressure: why the fuss? Chest. 1994;105(1):242 [MEDLINE]
Frequency and importance of barotrauma in 100 patients with acute lung injury. Crit Care Med. 1995;23(2):272 [MEDLINE]
Independent lung ventilation with a single ventilator using a variable resistance valve. Chest. 1995;107(1):256 [MEDLINE]
Frequency and importance of barotrauma in 100 patients with acute lung injury. Crit Care Med. 1995;23(2):272 [MEDLINE]
Clinical risk factors for pulmonary barotrauma: a multivariate analysis. Am J Respir Crit Care Med. 1995;152(4 Pt 1):1235 [MEDLINE]
Closure of a bronchopleural fistula using decalcified human spongiosa and a fibrin sealant. Ann Thorac Surg. 1997;64(1):230 [MEDLINE]
The relation of pneumothorax and other air leaks to mortality in the acute respiratory distress syndrome. N Engl J Med. 1998;338(6):341 [MEDLINE]
International consensus conferences in intensive care medicine: Ventilator-associated Lung Injury in ARDS. This official conference report was cosponsored by the American Thoracic Society, The European Society of Intensive Care Medicine, and The Societéde Réanimation de Langue Française, and was approved by the ATS Board of Directors, July 1999. Am J Respir Crit Care Med. 1999;160(6):2118 [MEDLINE]
Nitric oxide and high frequency jet ventilation in a patient with bilateral bronchopleural fistulae and ARDS. Can J Anaesth. 2000;47(1):53 [MEDLINE]
The Macklin effect: a frequent etiology for pneumomediastinum in severe blunt chest trauma. Chest. 2001 Aug;120(2):543-7 [MEDLINE]
Relationship between ventilatory settings and barotrauma in the acute respiratory distress syndrome. Intensive Care Med. 2002;28(4):406 [MEDLINE]
Airway pressures and early barotrauma in patients with acute lung injury and acute respiratory distress syndrome. Am J Respir Crit Care Med. 2002;165(7):978 [MEDLINE]
Management of a bronchopleural fistula using differential lung airway pressure release ventilation. J Cardiothorac Vasc Anesth. 2003;17(6):744 [MEDLINE]
Pneumothorax associated with long-term non-invasive positive pressure ventilation in Duchenne muscular dystrophy. Neuromuscul Disord. 2004 Jun;14(6):353-5 [MEDLINE]
Incidence, risk factors and outcome of barotrauma in mechanically ventilated patients. Intensive Care Med. 2004;30(4):612 [MEDLINE]
Management of advanced ARDS complicated by bilateral pneumothoraces with high-frequency oscillatory ventilation in an adult. Br J Anaesth. 2004;93(3):454 [MEDLINE]
High frequency oscillatory ventilation in the management of a high output bronchopleural fistula: a case report. Can J Anaesth. 2004;51(1):78 [MEDLINE]
Pneumothorax: an important complication of non-invasive ventilation in neuromuscular disease. Neuromuscul Disord. 2004 Jun;14(6):351-2 [MEDLINE]
Use of a modified endobronchial tube for mechanical ventilation of patients with bronchopleural fistula. Eur J Cardiothorac Surg. 2005;28(1):169 [MEDLINE]
Independent lung ventilation in the management of traumatic bronchopleural fistula. Am Surg. 2006;72(6):530 [MEDLINE]
Occurrence of pneumothorax during noninvasive positive pressure ventilation through a helmet. J Clin Anesth. 2007 Dec;19(8):632-5 [MEDLINE]
Extracorporeal membrane oxygenator as a bridge to successful surgical repair of bronchopleural fistula following bilateral sequential lung transplantation: a case report and review of literature. J Cardiothorac Surg. 2007;2:28 [MEDLINE]
[Evaluation of the incidence of pneumothorax and background of patients with pneumothorax during noninvasive positive pressure ventilation]. Nihon Kokyuki Gakkai Zasshi. 2008 Nov;46(11):870-4 [MEDLINE]
Benefits and complications of noninvasive mechanical ventilation for acute exacerbation of chronic obstructive pulmonary disease. Rev Bras Ter Intensiva. 2008 Jun;20(2):184-9 [MEDLINE]
Independent lung ventilation in the postoperative management of large bronchopleural fistula. J Thorac Cardiovasc Surg. 2010;139(2):e21 [MEDLINE]
Neuromuscular blockers in early acute respiratory distress syndrome. N Engl J Med. 2010;363(12):1107 [MEDLINE]
Pressure and volume limited ventilation for the ventilatory management of patients with acute lung injury: a systematic review and meta-analysis. PLoS One. 2011;6(1):e14623 [MEDLINE]
Intrabronchial valves: a case series describing a minimally invasive approach to bronchopleural fistulas in medical intensive care unit patients. J Bronchology Interv Pulmonol. 2012 Apr;19(2):137-41 [MEDLINE]
Neuromuscular blocking agents in acute respiratory distress syndrome: a systematic review and meta-analysis of randomized controlled trials. Crit Care. 2013 Mar;17(2):R43 [MEDLINE]
Differential lung ventilation and venovenous extracorporeal membrane oxygenation for traumatic bronchopleural fistula. Ann Thorac Surg. 2013;96(5):1859 [MEDLINE]
Pulmonary interstitial emphysema in adults: a clinicopathologic study of 53 lung explants. Am J Surg Pathol. 2014 Mar;38(3):339-45 [MEDLINE]
Pressure-controlled versus volume-controlled ventilation for acute respiratory failure due to acute lung injury (ALI) or acute respiratory distress syndrome (ARDS). Cochrane Database Syst Rev. 2015;1:CD008807 [MEDLINE]
Independent lung ventilation in the management of ARDS and bronchopleural fistula. Heart Lung. 2016;45(3):258 [MEDLINE]
High-Frequency Oscillatory Ventilation (HFOV) as Primary Ventilator Strategy in the Management of Severe Acute Respiratory Distress Syndrome (ARDS) with Pneumothorax in the Setting of Trauma. Am Surg. 2017;83(5):525 [MEDLINE]
Positive pressure ventilation in a patient with a right upper lobar bronchocutaneous fistula: right upper bronchus occlusion using the cuff of a left-sided double lumen endobronchial tube. J Anesth. 2017;31(4):627 [MEDLINE]
Bronchopleural Fistula Resolution with Endobronchial Valve Placement and Liberation from Mechanical Ventilation in Acute Respiratory Distress Syndrome: A Case Series. Case Rep Crit Care. 2017;2017:3092457 [MEDLINE]
Human pulmonary vascular response to 4 h of hypercapnia and hypocapnia measured using Doppler echocardiography. J Appl Physiol 2003, 94:1543-1551 [MEDLINE]
Impact of acute hypercapnia and augmented positive end-expiratory pressure on right ventricle function in severe acute respiratory distress syndrome. Intensive Care Med 2009, 35:1850-1858 [MEDLINE]
Pulmonary vascular and right ventricular dysfunction in adult critical care: current and emerging options for management: a systematic literature review. Crit Care. 2010;14(5):R169 [MEDLINE]
Other
Fever is associated with delayed ventilator liberation in acute lung injury. Ann Am Thorac Soc. 2013 Dec;10(6):608-15. doi: 10.1513/AnnalsATS.201303-052OC [MEDLINE]
Complications
Factors associated with acute kidney injury in acute respiratory distress syndrome. Ann Intensive Care 2019 Jul 1;9(1):74. doi: 10.1186/s13613-019-0552-5 [MEDLINE]
Prevention
Early identification of patients at risk of acute lung injury. Am J Respir Crit Care Med 2011;183:462–470 [MEDLINE]
Lung injury prediction score for the emergency department: first step towards prevention in patients at risk. Int J Emerg Med 2012;5:33–43 [MEDLINE]
IMPROVE Trial. A trial of intraoperative low-tidal-volume ventilation in abdominal surgery. N Engl J Med. 2013 Aug 1;369(5):428-37. doi: 10.1056/NEJMoa1301082 [MEDLINE]
Intraoperative low-tidal-volume ventilation. N Engl J Med. 2013;369(19):1861 [MEDLINE]
Association between tidal volume size, duration of ventilation,and sedation needs in patients without acute respiratory distress syndrome: an individual patient data meta-analysis. Intensive Care Med. 2014;40(7):950-957 [MEDLINE]
LIPS-A Trial. Effect of Aspirin on Development of ARDS in At-Risk Patients Presenting to the Emergency Department: The LIPS-A Randomized Clinical Trial. JAMA. 2016;315(22):2406 [MEDLINE]
A Meta-analysis of Intraoperative Ventilation Strategies to Prevent Pulmonary Complications: Is Low Tidal Volume Alone Sufficient to Protect Healthy Lungs? Ann Surg. 2016 May;263(5):881-7. doi: 10.1097/SLA.0000000000001443 [MEDLINE]
PReVENT Trial. Effect of a Low vs Intermediate Tidal Volume Strategy on Ventilator-Free Days in Intensive Care Unit Patients Without ARDS: A Randomized Clinical Trial. JAMA. 2018 Oct 24. doi: 10.1001/jama.2018.14280 [MEDLINE]