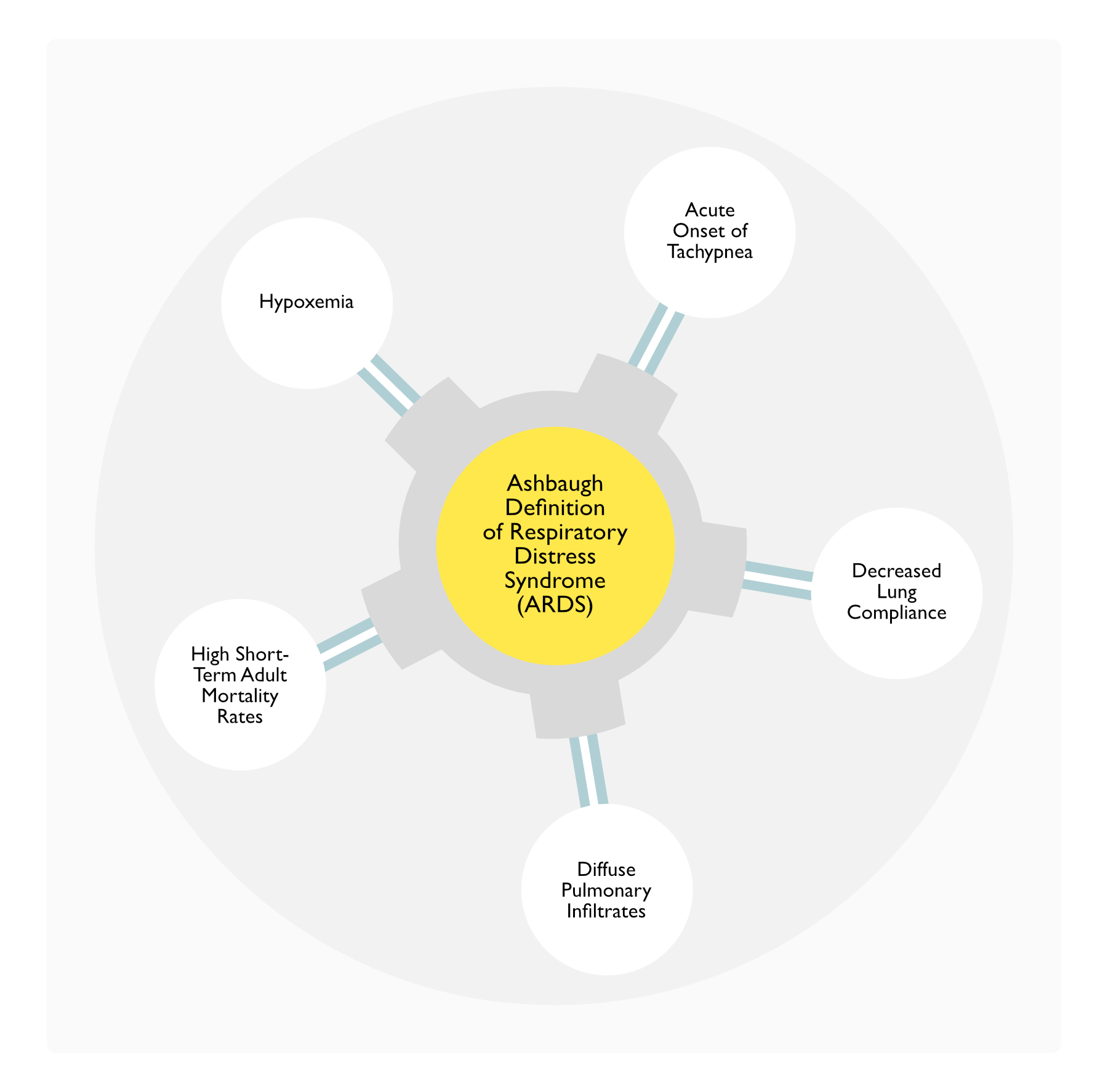
In 1967, Ashbaugh Introduced the Term “Respiratory Distress Syndrome” to Describe a Clinical Syndrome with the Following Clinical Features (Lancet, 1967) [MEDLINE]
LUNG SAFE Global Observational Study of Acute Respiratory Distress Syndrome (ARDS) in 50 Countries (JAMA, 2016) [MEDLINE]
Epidemiology
Approximately 10.4% of ICU Admissions Met ARDS Criteria
Approximately 23.4% of Mechanically Ventilated Patients Met ARDS Criteria
Clinical
Clinical Recognition of ARDS Ranged from 51.3% in Mild ARDS to 78.5% in Severe ARDS
Therapy
Less Than 66% of the Patients Received Tidal Volume <8 mL/kg
Proning was Used in Only 16.3% of Patients with Severe ARDS
Hospital Mortality Rates
Mild ARDS: 34.9%
Moderate ARDS: 40.3%
Severe ARDS: 46.1%
Conclusions
ARDS Recognition and Management Has Room for Potential Clinical Improvement
Cost
Systematic Review of the Costs of Acute Respiratory Distress Syndrome (ARDS) (Chest, 2021) [MEDLINE]: n = 49,483 (from 22 studies)
Mean Inpatient Costs Ranged from $8,476 (2021 US Dollars) to $547,974 (2021 US Dollars) and were Highest in Publications of Lower Quality and in American Health Systems and were Associated with Trauma Cohorts
Mean Outpatient Costs were Highest in Publications with Higher Readmission Rates, Longer Durations of Follow-Up, and in American Health Systems
Risk Factors
Prediction of Acute Respiratory Distress Syndrome (ARDS) Using Clinical Factors
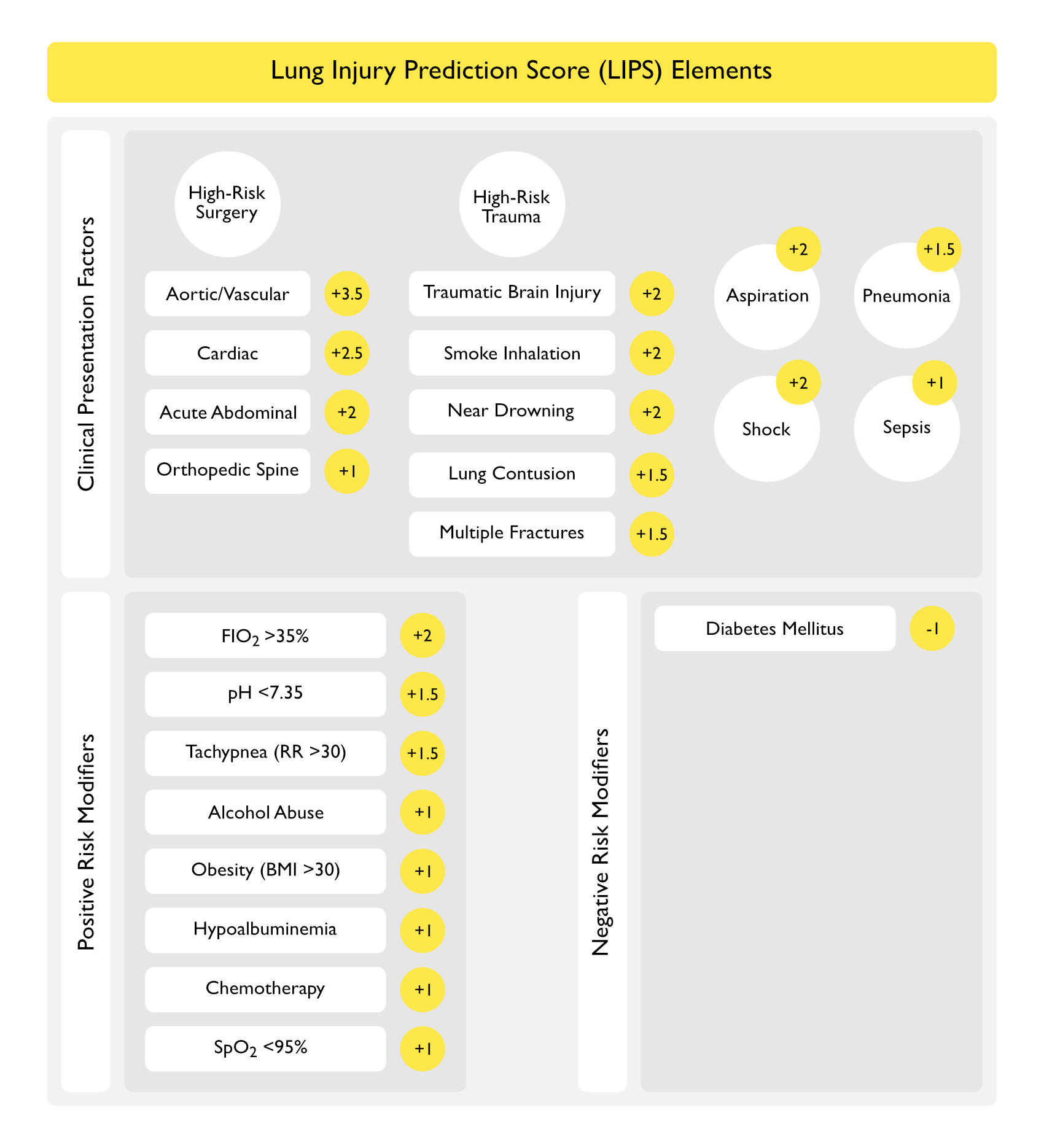
Lung Injury Prediction Score (LIPS) Study (Am J Respir Crit Care Med, 2011) [MEDLINE]: multicenter observational cohort study (n = 5,584 patients at risk)
Acute Lung Injury Occurred at a Median of 2 Days in 6.8% of Patients
Acute Lung Injury Can Be Predicted Early in the Course of Illness Using Clinical Parameters
Aspiration: LIPS points +2 pts
High-Risk Surgery (add 1.5 pts if emergency surgery)
Aortic/Vascular: +3.5 pts
Cardiac: +2.5 pts
Acute Abdomen: +2 pts
Orthopedic Spine: +1 pt
High-Risk Trauma
Traumatic Brain Injury: +2 pts
Smoke Inhalation: +2 pts
Near Drowning: +2 pts
Lung Contusion: +1.5 pts
Multiple Fractures: +1.5 pts
Pneumonia: +1.5 pts
Shock: +2 pts
Sepsis: +1 pt
Negative Risk Modifiers (Decrease the Risk of Acute Lung Injury)
Diabetes Mellitus: -1 pt (only if sepsis)
Note: Diabetes Mellitus is the Only Risk factor Which Decreases the Risk of Developing ARDS
Positive Risk Modifiers (Increase the Risk of Acute Lung Injury)
FIO2 >35%: +2 pts
pH <7.35: +1.5 pts
Tachypnea with RR >30: +1.5 pts
Alcohol Abuse: +1 pts
Obesity with BMI >30: +1 pt
Hypoalbuminemia: +1 pt
Chemotherapy: +1 pt
SpO2 <95%: +1 pt
Scoring
Over 4 points (Optimal Cutoff Point in the Study Based on the Area Under the Curve Analysis): 69% sensitivity and 78% specificity for the prediction of development of ARDS
Prediction of Acute Respiratory Distress Syndrome (ARDS) Using Clinical Factors Present in the Emergency Department
Emergency Department Lung Injury Prediction Score Study (EDLIPS)/LIPS-1 Study (Int J Emerg Med, 2012) [MEDLINE]
Incidence of Acute Lung Injury was 7%
EDLIPS (Obtained Early in ED Course) Discriminated Patients Who Developed Acute Lung Injury Better than APACHE II Scoring and Similar to Original LIPS Score
Protective Factors
Older Age
Clinical Efficacy
Prospective Multicenter Observational Cohort Study of Hospitalized Patients at Risk of Developing Acute Respiratory Distress Syndrome (ARDS) (from 3/09-8/09) (J Intensive Care Med, 2019) [MEDLINE]: n = 5,584 (22 hospitals)
Approximately 6.8% of the Patients Developed ARDS
After Adjusting for Severity of Illness and the Risk of ARDS Development Attributable to Other Factors, Older Adult Patients Had a Lower Incidence of ARDS, as Compared to Younger Patients (Odds Ratio: 0.28, 95% Confidence Interval: 0.18-0.42)
Retrospective Study Examining the Effect of Preadmission Oral Corticosteroid on the Risk of Development of Acute Respiratory Distress Syndrome in Intensive Care Unit Patients with Sepsis (Crit Care Med, 2017) [MEDLINE]: n = 1080
Preadmission Oral Corticosteroid Use Decreases the Risk of Early Acute Respiratory Distress Syndrome (Within 96 hrs of ICU Admission) in ICU Patients with Sepsis (35%), as Compared to Patients Who Had Not Received Preadmission Corticosteroids (42%)
Higher Corticosteroid Doses (Prednisone 30 qday) were Associated with Lower Risk of ARDS (Odds Ratio 0.53) than were Lower Corticosteroid Doses (Prednisone 5 mg qday)
Preadmission Oral Corticosteroid Use Did Not Impact the In-Hospital Mortality Rate, ICU Length of Stay, or Ventilator-Free Days
South Korean Nationwide Cohort Study (2015-2020) of Sodium-Glucose Cotransporter-2 Inhibitors in Adult Patients with Type 2 Diabetes Mellitus (BMC Med, 2023) [MEDLINE]
Primary Outcome was Respiratory Events Composite Endpoint
Secondary Outcomes were the Individual Components of the Primary Outcome and In-Hospital Death
Cox Models were Used to Estimate Hazard Ratios 95% Confidence Intervals
Incidence Rates for Overall Respiratory Events were 4.54 and 7.54 Per 1000 Person-Years Among Sodium-Glucose Cotransporter-2 (SGLT2) Inhibitors and Dipeptidyl Peptidase-4 (DPP-4) Inhibitors Users, Respectively, Corresponding to a Rate Difference of 3 Less Events Per 1000 Person-Years (95% CI – 3.44 to – 2.55)
Hazard Ratios (95% CIs)
0.60 (0.55 to 0.64) for the Composite Respiratory Endpoint (Acute Pulmonary Edema, Acute Respiratory Distress Syndrome, Pneumonia, and Respiratory Failure
0.35 (0.23 to 0.55) for Acute Pulmonary Edema
0.44 (0.18 to 1.05) for Acute Respiratory Syndrome (ARDS)
0.61 (0.56 to 0.66) for Pneumonia
0.49 (0.31 to 0.76) for Respiratory Failure
0.46 (0.41 to 0.51) for In-Hospital Death
Similar Trends were Found Across Individual Sodium-Glucose Cotransporter-2 (SGLT2) Inhibitors, Subgroup Analyses of Age, Sex, History of Comorbidities, and a Range of Sensitivity Analyses
Respiratory Complications (Including Sloughing of the Bronchial Epithelium, Pneumonia, Atelectasis, and Acute Respiratory Distress Syndrome) are Common During the Acute Phase of Stevens-Johnson Syndrome (SJS) and Toxic Epidermal Necrolysis (TEN)
Approximately 25% of Patients with Pulmonary Involvement Develop Acute Respiratory Failure Requiring Mechanical Ventilation (Crit Care Med, 2014) [MEDLINE]
Acute respiratory distress in adults. Lancet. 1967 Aug 12;2(7511):319-23. doi: 10.1016/s0140-6736(67)90168-7 [MEDLINE]
The American-European Consensus Conference on ARDS. Definitions, mechanisms, relevant outcomes, and clinical trial coordination. Am J Respir Crit Care Med 1994;149:818–824 [MEDLINE]
The acute respiratory distress syndrome. N Engl J Med 1995; 332:27-37
Clinical risk factors for pulmonary barotrauma: a multivariate analysis. Am J Respir Crit Care Med 1995; 152:1235-1240
Pathogenesis and treatment of the adult respiratory distress syndrome. Arch Intern Med 1996; 156:29-38
The relation of pneumothorax and other air leaks to mortality in the acute respiratory distress syndrome. N Engl J Med 1998; 338:341-346
The acute respiratory distress syndrome. N Engl J Med. 2000 May 4;342(18):1334-49 [MEDLINE]
What has computed tomography taught us about the acute respiratory distress syndrome? Am J Respir Crit Care Med. 2001 Nov 1;164(9):1701-11 [MEDLINE]
Pressure-volume curves and compliance in acute lung injury: evidence of recruitment above the lower inflection point. Am J Respir Crit Care Med 1999; 159:1172-1178
Consensus conference on mechanical ventilation. Intensive Care Med 1994; 20:64-79, 150-162
The American-European consensus conference on ARDS. Am J Respir Crit Care Med 1994;149:818-824
Patient-ventilator interactions. Clin Chest Med 1996; 17:423-438.
Patient ventilator interaction. Am J Respir Crit Care Med 2001; 163:1059-1063.
Influence of cardiac output on intrapulmonary shunt. J Appl Physiol 1979; 46:315-321
Respiratory system mechanics in ventilated patients: techniques and indications. Mayo Clin Proc 1987; 62:358-368
Physiologic approach to mechanical ventilation Crit Care Med 1990; 18:103-113
Current definitions of acute lung injury and the acute respiratory distress syndrome do not reflect their true severity and outcome. Intensive Care Med. 1999;25(9):930-935 [MEDLINE]
Screening of ARDS patients using standardized ventilator settings: influence on enrollment in a clinical trial. Intensive Care Med. 2004;30(6):1111-1116 [MEDLINE]
Severe Hypoxemic Respiratory Failure, Part 1—Ventilatory Strategies. Chest 2010; 137(5):1203–1216 [MEDLINE]
Severe hypoxemic respiratory failure: part 2-Nonventilatory strategies. Chest. 2010 Jun;137(6):1437-48 [MEDLINE]
Acute respiratory distress syndrome: the Berlin Definition. JAMA. 2012 Jun 20;307(23):2526-33 [MEDLINE]
The acute respiratory distress syndrome: what’s in a name? JAMA 2012;307:2542–2544 [MEDLINE]
Update in acute respiratory distress syndrome and mechanical ventilation. Am J Respir Crit Care Med 2012;188:285–292 [MEDLINE]
The new definition for acute lung injury and acute respiratory distress syndrome: is there room for improvement? Curr Opin Crit Care. 2013 Feb;19(1):16-23 [MEDLINE]
Surviving sepsis campaign: international guidelines for management of severe sepsis and septic shock: 2012. Crit Care Med. 2013 Feb;41(2):580-637. doi: 10.1097/CCM.0b013e31827e83af [MEDLINE]
Incidence of mortality and morbidity related to postoperative lung injury in patients who have undergone abdominal or thoracic surgery: a systematic review and meta-analysis. Lancet Respir Med. 2014 Dec;2(12):1007-15. doi: 10.1016/S2213-2600(14)70228-0. Epub 2014 Nov 13 [MEDLINE]
The association between physiologic dead-space fraction and mortality in subjects with ARDS enrolled in a prospective multi-center clinical trial. Respir Care. 2014;59:1611–1618 [MEDLINE]
Driving pressure and survival in the acute respiratory distress syndrome. N Engl J Med 2015;372:747-755 [MEDLINE]
Driving pressure and respiratory mechanics in ARDS. N Engl J Med 2015;372:776-777 [MEDLINE]
LUNG SAFE Study. Epidemiology, Patterns of Care, and Mortality for Patients With Acute Respiratory Distress Syndrome in Intensive Care Units in 50 Countries. JAMA. 2016 Feb 23;315(8):788-800. doi: 10.1001/jama.2016.0291 [MEDLINE]
Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016. Intensive Care Med. 2017 Jan 18. doi: 10.1007/s00134-017-4683-6 [MEDLINE]
An Update on Management of Adult Patients with Acute Respiratory Distress Syndrome: An Official American Thoracic Society Clinical Practice Guideline. Am J Respir Crit Care Med. 2023 Nov 30. doi: 10.1164/rccm.202311-2011ST [MEDLINE]
Incidence and outcomes of acute lung injury. N Engl J Med. 2005;353(16):1685 [MEDLINE]
LUNG SAFE Study. Epidemiology, Patterns of Care, and Mortality for Patients With Acute Respiratory Distress Syndrome in Intensive Care Units in 50 Countries. JAMA. 2016 Feb 23;315(8):788-800. doi: 10.1001/jama.2016.0291 [MEDLINE]
Preadmission Oral Corticosteroids Are Associated With Reduced Risk of Acute Respiratory Distress Syndrome in Critically Ill Adults With Sepsis. Crit Care Med. 2017 May;45(5):774-780. doi: 10.1097/CCM.0000000000002286 [MEDLINE]
Older Adult Patients Are at Lower Risk of ARDS Compared to Younger Patients at Risk: Secondary Analysis of a Multicenter Cohort Study. J Intensive Care Med. 2019 May 8:885066619848357. doi: 10.1177/0885066619848357 [MEDLINE]
The Cost of ARDS: A Systematic Review. Chest. 2021 Aug 31;S0012-3692(21)03829-0. doi: 10.1016/j.chest.2021.08.057 [MEDLINE]
Association of adverse respiratory events with sodium-glucose cotransporter 2 inhibitors versus dipeptidyl peptidase 4 inhibitors among patients with type 2 diabetes in South Korea: a nationwide cohort study. BMC Med. 2023 Feb 10;21(1):47. doi: 10.1186/s12916-023-02765-2 [MEDLINE]
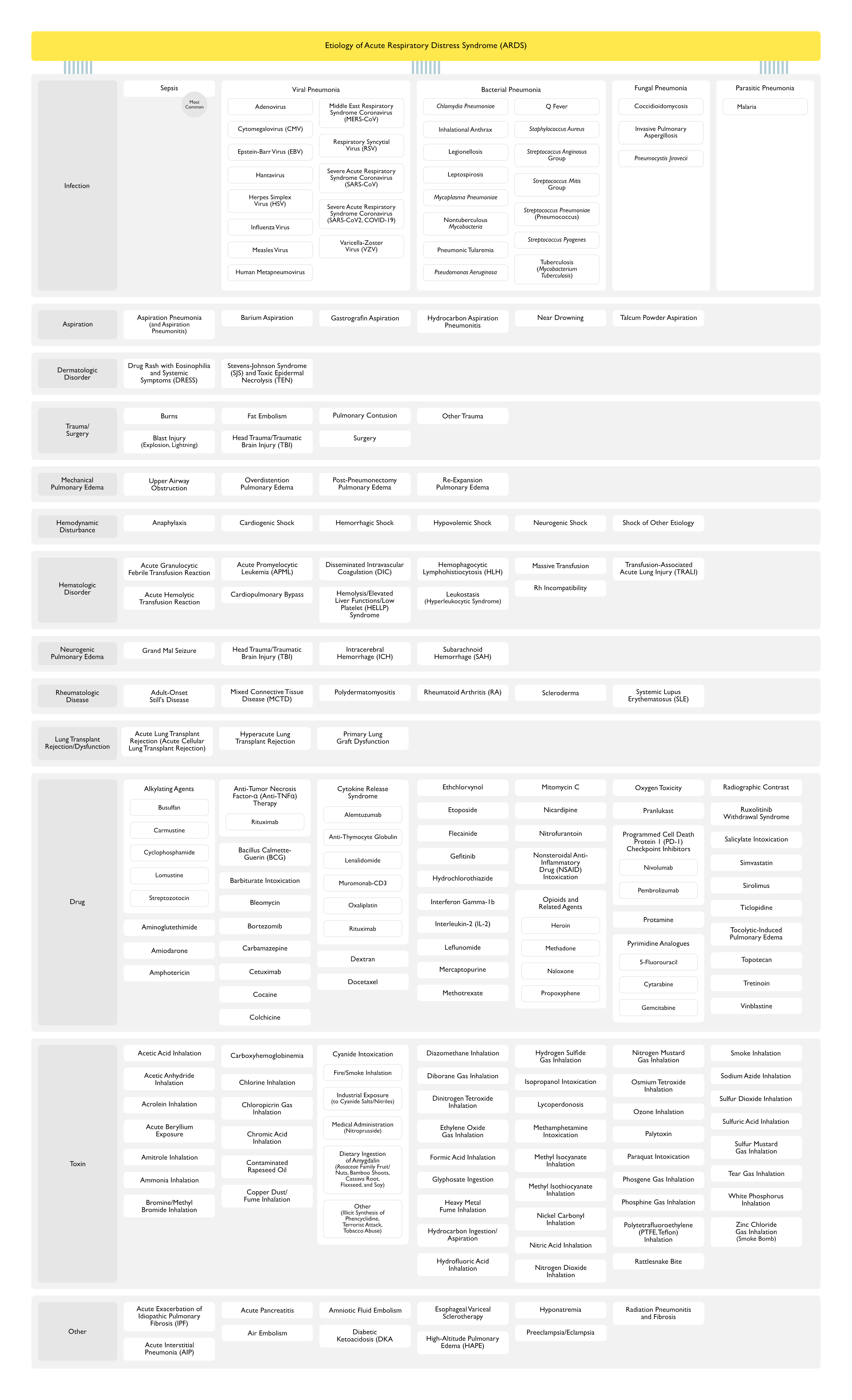
Etiology
Infection
Chronic alcohol abuse is associated with an increased incidence of acute respiratory distress syndrome and severity of multiple organ dysfunction in patients with septic shock. Crit Care Med. 2003;31(3):869 [MEDLINE]
Risk factors for the development of acute lung injury in patients with septic shock: an observational cohort study. Crit Care Med. 2008;36(5):1518 [MEDLINE]
Early risk factors and the role of fluid administration in developing acute respiratory distress syndrome in septic patients. Ann Intensive Care. 2017;7(1):11. Epub 2017 Jan 23 [MEDLINE]
Hyponatremia, cerebral edema, and noncardiogenic pulmonary edema in marathon runners. Ann Intern Med. 2000 May 2;132(9):711-4. doi: 10.7326/0003-4819-132-9-200005020-00005 [MEDLINE]