Treatment of Low-Risk Acute Pulmonary Embolism (PE)
General Comments
Home Treatment of Acute Pulmonary Embolism (PE) is More Convenient and Less Expensive than Hospital Treatment and is Preferred by Most Patients (Chest, 2021) [MEDLINE]
Treatment of Acute Pulmonary Embolism (PE) with a Direct Oral Anticoagulant (DOAC) (Such as Apixaban/Rivaroxaban) Does Not Require Initial Heparin Therapy and Facilitates Treatment without Hospital Admission
Clinical Criteria for Outpatient Treatment of Acute Pulmonary Embolism (PE) (or Early Discharge to Home)
Clinical Stability with Good Cardiopulmonary Reserve
No Specific Contraindications, Such as Recent Bleeding, Severe Renal Disease, Severe Liver Disease, or Severe Thrombocytopenia (Defined as Platelet Count <70k)
Patient is Expected to Be Compliant with Treatment
Patient Feels Well Enough to Be Treated as Outpatient
Low Pulmonary Embolism Score
Pulmonary Embolism Severity Index (PESI) Score <85
Simplified Pulmonary Embolism Severity Index (Simplified PESI) Score = 0
Absence of Elevated Cardiac Biomarker (Troponin, etc) Level
Absence of Right Ventricular (RV) Dysfunction
Recommendations (European Society of Cardiology and European Respiratory Society Guidelines for the Diagnosis and Management of Acute Pulmonary Embolism, 2019) (Eur Heart J, 2020) [MEDLINE]
Carefully Selected Patients with Low-Risk Acute Pulmonary Embolism Should Be Considered for Early Discharge and Continuation of Treatment at Home, if Proper Outpatient Care and Anticoagulant Treatment Can Be Provided (Class IIa, Level A)
Recommendations (American Society of Hematology Guidelines for the Management of Venous Thromboembolism, 2020) (Blood Adv, 2020) [MEDLINE]
For Patients with Acute Pulmonary Embolism with a Low Risk for Complications, Offering Home Treatment is Recommended Over Hospital Treatment (Conditional Recommendation, Very Low Certainty in the Evidence
At Best, Clinical Prediction Scores Have a Moderate Ability to Predict Patient Outcomes and, Therefore, Do Not Replace Clinical Judgment
However, They May Help to Select Patients at Low Risk for Complications
Pulmonary Embolism Severity Index (PESI) and Simplified PESI Have Been the Most Widely Validated Scores
This Recommendation Does Not Apply to Patients Who Have Other Conditions Which Might Require Hospitalization, Have Limited or No Home Support, Cannot Afford Medications, or Have a History of Poor Compliance
Patients with Submassive Pulmonary Embolism (Intermediate-High Risk) or Massive Pulmonary Embolism (High-Risk) or at High Risk for Bleeding and Those Requiring Intravenous Analgesics May Benefit from Initial Treatment in the Hospital
Recommendations (Antithrombotic Therapy for VTE Disease: Compendium and Review of CHEST Guidelines 2012-2021) (Chest, 2024) [MEDLINE]
Statement 8.0 (2012): In Patients with Acute Lower Extremity Deep Venous Thrombosis (DVT) and Whose Home Circumstances are Adequate, Initial Treatment at Home is Recommended Over Treatment in the Hospital (Strong Recommendation, Moderate-Certainty Evidence)
Statement 8.2 (2021): In Patients with Low-Risk Pulmonary Embolism (PE), Outpatient Treatment is Recommended Over Hospitalization, Assuming Access to Medications, Ability to Access Outpatient Care, and Home Circumstances are Adequate (Strong Recommendation, Low-Certainty Evidence)
Treatment of Recurrent Venous Thromboembolism (VTE) While Not on Anticoagulation
Recommendations (American Society of Hematology Guidelines for the Management of Venous Thromboembolism, 2020) (Blood Adv, 2020) [MEDLINE]
For Patients Who Develop Deep Venous Thrombosis and/or Acute Pulmonary Embolism Provoked by a Transient Risk Factor and Have a History of Previous Unprovoked Venous Thromboembolism or Venous Thromboembolism Provoked by a Chronic Risk Factor, Use of Indefinite Antithrombotic Therapy is Recommended Over Stopping Anticoagulation After Completing Primary Treatment (Conditional Recommendation, Moderate Certainty in the Evidence)
For Patients Who Develop Deep Venous Thrombosis and/or Acute Pulmonary Embolism Provoked by a Transient Risk Factor and Have a History of a Previous Venous Thromboembolism Also Provoked by a Transient Risk Factor, Stopping Anticoagulation After Completion of Primary Treatment is Recommended Over Indefinite Antithrombotic Therapy (Conditional Recommendation, Moderate Certainty in the Evidence
For Patients with a Recurrent Unprovoked Deep Venous Thrombosis and/or Acute Pulmonary Embolism, Indefinite Antithrombotic Therapy is Recommended Over Stopping Anticoagulation After Completion of Primary Treatment (Strong Recommendation, Moderate Certainty in the Evidence)
Treatment of Recurrent Venous Thromboembolism (VTE) While on Anticoagulation (Chest Antithrombotic Therapy for VTE Disease 2016 Guidelines) (Chest, 2016) [MEDLINE]
Rationale
Risk of Recurrent Venous Thromboembolism Decreases Rapidly After Starting Anticoagulation
Based on This, a Recurrence Soon After Therapy Can Generally Be Managed by Increasing the Intensity of Anticoagulation
When Oral Anticoagulation is Managed Well, the Risk of Recurrence is Approximately 2 Per 100 Patient-Years (Blood, 2017) [MEDLINE]
The Main Reasons for Breakthrough Events are Underlying Disease and Subtherapeutic Drug Levels
Recommendations (Chest Antithrombotic Therapy for VTE Disease 2016 Guidelines) [MEDLINE]
Treatment of Recurrent Venous Thromboembolism on a Non-Low Molecular Weight Heparin (Coumadin or Oral Agent)
Switch to Low Molecular Weight Heparin is Recommended, at Least Temporarily (Grade 2C Recommendation)
Treatment of Recurrent Venous Thromboembolism on a Low Molecular Weight Heparin
Higher Dose of Low Molecular Weight Heparin (by 25-33%) is Recommended (Grade 2C Recommendation)
Recommendations (American Society of Hematology Guidelines for the Management of Venous Thromboembolism, 2020) (Blood Adv, 2020) [MEDLINE]
For Patients with Breakthrough Deep Venous Thrombosis and/ or Acute Pulmonary Embolism During Therapeutic Coumadin Treatment, Use of Low Molecular Weight Heparin is Recommended Over DOAC Therapy (Conditional Recommendation, Very Low Certainty in the Evidence)
Patients Who Present with a New Venous Thromboembolism Event During Therapeutic Coumadin Treatment Should Be Further Investigated to Identify Potential Underlying Etiologies
This Recommendation Does Not Apply to Patients Who Develop Breakthrough Venous Thromboembolism in the Setting of Poor INR Control, in Whom a DOAC May Be a Reasonable Option
Inferior Vena Cava Filter Use in the Management of Venous Thromboembolism Has Increased Over the Last Few Decades (Arch Intern Med, 2010) [MEDLINE] (Am J Med, 2011) [MEDLINE]
Although Most IVC Filters are Currently Designed to Be Retrieved, Many Remain in Patients for Extended Durations or Permanently, Even When the Original Reason for IVC Filter Placement Has Resolved (Chest, 2021) [MEDLINE]
Anticoagulation Failure: objectively documented extension of existing deep venous thrombosis (or new deep venous thrombosis) or pulmonary embolism while therapeutically anticoagulated
Failure of Previous Device to Prevent Pulmonary Embolism (Due to Central Extension of Thrombus Through an Existing Inferior Vena Cava Filter or Recurrent Pulmonary Embolism)
In Association with Thrombectomy, Embolectomy, or Lytic Therapy
Prophylaxis with No Thromboembolic Disease
Prophylaxis with Thromboembolism in Addition to Anticoagulation
Technique
Filter Positioning
Inferior Vena Cava Filters are Typically Placed Infrarenally, Since Suprarenal Filters May Lead to Renal Vein Compromise, if They Become Clotted
Retrievable Inferior Vena Cava Filters
May Remain in Place for Approximately 2 mos
There is No Data to Support One Inferior Vena Cava Filter Brand Over Another
Clinical Efficacy
Prévention du Risque d’Embolie Pulmonaire par Interruption Cave Study Group (PREPIC) Trial (NEJM, 1998) [MEDLINE]
At 2 Years, Inferior Vena Cava Filter Had No Impact on the Rate of Symptomatic Pulmonary Embolism or Mortality Rate
However, Inferior Vena Cava Filter Placement Increased the Rate of Recurrent Deep venous Thrombosis
Randomized, Open-Label PREPIC2 Trial of IVC Filter Added to Anticoagulation in Severe Acute PE Requiring Hospitalization (JAMA, 2015) [MEDLINE]
Retrievable Inferior Vena Cava Filter Has No Clinical Cenefit Over Anticoagulation Alone (in Terms of Decreasing the Risk of Recurrent Pulmonary Embolism at 3/6 Months or 3-Month/6-Month Mortality Rate)
Based on These Data, Inferior Vena Cava Filter is Not Indicated in Anticoagulated Acute Pulmonary Embolism Patients on the Basis of Poor Cardiopulmonary Reserve, Large Clot Burden, or Suspected Risk of Recurrence
Recommendations (European Society of Cardiology and European Respiratory Society Guidelines for the Diagnosis and Management of Acute Pulmonary Embolism, 2019) (Eur Heart J, 2020) [MEDLINE]
Inferior Vena Cava (IVC) Filters Should Be Considered in Patients with Acute Pulmonary Embolism and Absolute Contraindications to Anticoagulation (Class IIa, Level C)
Inferior Vena Cava (IVC) Filters Should Be Considered in Cases of Acute Pulmonary Embolism Recurrence Despite Therapeutic Anticoagulation (Class IIa, Level C)
Routine Use of Inferior Vena Cava (IVC) Filters is Not Recommended (Class III, Level A)
Recommendations for Inferior Vena Cava (IVC) Filter (Consensus Practice from the PERT Consortium, 2019) (Clin Appl Thromb Hemost, 2019) [MEDLINE]
Consider an Inferior Vena Cava (IVC) Filter for Patients with Contraindications to or Failure of Therapeutic Anticoagulation and for Highly Selected Patients with Intermediate or High-Risk Acute Pulmonary Embolism
Consider an Inferior Vena Cava (IVC) Filter in Select Patients When Large, Free-Floating, Proximal DVT is Identified
Recommendations (American Society of Hematology Guidelines for the Management of Venous Thromboembolism, 2020) (Blood Adv, 2020) [MEDLINE]
For Patients with Proximal Deep Venous Thrombosis and Significant Preexisting Cardiopulmonary Disease, as Well as for Patients with Acute Pulmonary Embolism and Hemodynamic Compromise, Anticoagulation Alone is Recommended Over Anticoagulation Plus Inferior Vena Cava (IVC) Filter Placement (Conditional Recommendation, Low Certainty in the Evidence)
These Recommendations Apply to Patients Who are Eligible to Receive Anticoagulation
For Patients with a Contraindication to Anticoagulation, Insertion of a Retrievable Inferior Vena Cava (IVC) Filter May Be Indicated with Retrieval as Soon as the Patient is Able to Receive Anticoagulation
In Patients with Acute Lower Extremity Deep Venous Thrombosis, Inferior Vena Cava (IVC) Filter is Not Recommended in Addition to Anticoagulation (Strong Recommendation, Moderate-Certainty Evidence)
Because it is Uncertain if There is Benefit to Placement of an Inferior Vena Cava (IVC) Filter in Anticoagulated Patients with High-Risk Acute Pulmonary Embolism (with Hypotension), the Recommendation Against Insertion of an Inferior Vena Cava (IVC) Filter in Patients with Acute Pulmonary Embolism Who are Anticoagulated May Not Apply to this Select Subgroup of Patients
In Patients with Acute Lower Extremity Proximal Deep Venous Thrombosis and a Contraindication to Anticoagulation, Inferior Vena Cava (IVC) Filter is Recommended (Strong Recommendation, Moderate-Certainty Evidence)
In These Patients, the Inferior Vena Cava (IVC) Filter Should Be Promptly Removed When Anticoagulation Has Been Instituted
Criteria for Outpatient Therapy (Patient Must Have All of These to Be Considered for Outpatient Therapy)
Hemodynamically Stable
Low Risk of Hemorrhage
No Renal Insufficiency
Feasible Administration/Monitoring of Anticoagulation at Home (Adequate Mental Capacity to Manage Medications and Monitoring, Adequate Living Conditions, Caregiver Support, Telephone Access, etc)
Contraindications to Outpatient Therapy (Can Fam Physician, 2005) [MEDLINE]
Massive Deep Venous Thrombosis (Iliofemoral Deep Venous Thrombosis, Phlegmasia Cerulea Dolens, etc)
Concurrent Symptomatic Pulmonary Embolism
High Risk of Hemorrhage on Anticoagulation
Comorbid Conditions or Other Factors Which Require Inpatient Care
Recommendations (American Society of Hematology Guidelines for the Management of Venous Thromboembolism, 2020) (Blood Adv, 2020) [MEDLINE]
For Patients with Uncomplicated Deep Venous Thrombosis, Offering Home Treatment is Recommended Over Hospital Treatment (Conditional Recommendation Based, Low Certainty in Evidence)
Recommendation Does Not Apply to Patients Who Have Other Conditions Which Might Require Hospitalization, Have Limited or No Home Support, Cannot Afford Medications, or Have a History of Poor Compliance
Patients with Limb-threatening Deep Venous Thrombosis or a High Risk for Bleeding and Those Requiring Intravenous Analgesics May Benefit from Initial Treatment in the Hospital
Ambulation
Ambulation is Indicated as Soon as Possible (Despite the Theoretical Risk for Embolization)
Usually a Gradual Increase in Ambulation is Advisable
Ambulation Has Not Been Demonstrated to Increase the Risk of Fatal Pulmonary Embolism (XXXXXXXXX)
Graduated Compression Stockings
Rationale
May Provide Symptomatic Relief and Facilitate Ambulation
Theoretical Goal of Therapy is the Prevention of Post-Phlebitic Syndrome (Although Data are Conflicting as to Their Efficacy in this Regard)
Contraindications
Allergy to the Stocking Material
Inability to Apply Stockings
Severe Arterial Insufficiency
Skin Ulceration
Recommendations (American Society of Hematology Guidelines for the Management of Venous Thromboembolism, 2020) (Blood Adv, 2020) [MEDLINE]
For Patients with Deep Venous Thrombosis, with or without an Increased Risk for Postthrombotic Syndrome, the Routine Use of Compression Stockings is Not Recommended (Conditional Recommendations, Very Low Certainty in the Evidence)
Although the Majority of Patients May Not Benefit from the Use of Stockings to Reduce the Risk of Postthrombotic Syndrome, Stockings May Help to Reduce Edema and pain associated with Acute Deep Venous Thrombosis in Selected Patients
In Patients with Acute Lower Extremity Deep Venous Thrombosis, Use of Routine Compression Stockings to Prevent Post-Thrombotic Syndrome is Not Recommended (Weak Recommendation, Low-Certainty Evidence)
No Evidence Exists that the Use of Graduated Compression Stockings Following Deep Venous Thrombosis Reduces the Risk for Recurrent Deep Venous Thrombosis
Presence of Free-Floating Thrombus in Deep Venous Thrombosis
Free-Floating Thrombus Occurs in 10% of All Deep Venous Thromboses (J Vasc Surg, 1990) [MEDLINE]
Only 13% are Associated with Clinically-Significant Pulmonary Emboli by V/Q Scan (Usually the Pulmonary Embolism Occurred Before the Diagnosis of the Free-Floating Thrombus)
Most Free-Floating Thrombi Followed Noninvasively by Duplex Scanning Do Not Embolize, But Rather Become Attached to the Vein Wall or Resolve
Assuming Adequate Anticoagulation with Unfractionated Heparin/Low Molecular Weight Heparin (Nadroparin Calcium), Studies Suggest that Presence of DVT with Free-Floating Thrombus Does Not Increase the Risk of Acute Pulmonary Embolism (Arch Intern Med, 1997) [MEDLINE]
However, Similar Studies Have Not Been Done Using Direct Oral Anticoagulants
This is Critical Since Direct Oral Anticoagulants May Have Slower Onsets of Action Than Heparins
Apixaban Has a Peak Onset of Action of 3-4 hrs (see Apixaban)
Rivaroxaban Does Not reach Peak Plasma Levels Until 2-4 hrs Later (see Rivaroxaban)
Catheter-Directed Thrombolysis of Acute Lower Extremity Deep Venous Thrombosis (see Deep Venous Thrombosis)
Clinical Efficacy
Retrospective Analysis of Catheter-Directed Thrombolysis for Lower Extremity DVT (JAMA Int Med, 2014) [MEDLINE]
Catheter-Directed Thrombolysis of Lower Extremity DVT is Associated with 2x-Increased Risk of Transfusion, 3x-Increased Risk of Intracranial Hemorrhage, 1.5x-Increased Risk of Acute PE, and 2x-Increased Risk of IVC Filter Insertion: long-term outcomes were not reported
Indications (Patients Most Likely to Benefit from Catheter-Directed Thrombolysis of Lower Extremity DVT) (Chest Antithrombotic Therapy for VTE Disease 2016 Guidelines) [MEDLINE]
Failure of Anticoagulation
Good Functional Status
Iliofemoral DVT/Phlegmasia Cerulea Dolens
Life Expectancy of At Least 1 Year
Low Risk of Hemorrhage
Symptoms for <14 Days
Recommendations (American Society of Hematology Guidelines for the Management of Venous Thromboembolism, 2020) (Blood Adv, 2020) [MEDLINE]
In Most Patients with Proximal Deep Venous Thrombosis, Anticoagulation Therapy Alone is Recommended Over Thrombolytic Therapy in Addition to Anticoagulation (Conditional Recommendation, Low Certainty in the Evidence)
Thrombolysis is Reasonable to Consider for Patients with Limb-Threatening Deep Venous Thrombosis (Phlegmasia Cerulea Dolens) and for Selected Younger Patients at Low Risk for Bleeding with Symptomatic Deep Venous Thrombosis Involving the Iliac and Common Femoral Veins (Higher Risk for More Severe Postthrombotic Syndrome)
Patients in These Categories Who Value Rapid Resolution of Symptoms, are Averse to the Possibility of Postthrombotic Syndrome, and Accept the Added Risk of Major Bleeding May Prefer Thrombolysis
Use of Thrombolysis Should Be Rare for Patients with Deep Venous Thrombosis Limited to Veins Below the Common Femoral Vein
For Patients with Extensive Deep Venous Thrombosis in Whom Thrombolysis is Considered Appropriate, Use of Catheter-Directed Thrombolysis is Recommended Over Systemic Thrombolysis (Conditional Recommendation, Very Low Certainty in the Evidence)
In Patients with Acute Lower Extremity Deep Venous Thrombosis, Anticoagulation Alone is Recommended Over Interventional (Thrombolytic, Mechanical, or Pharmacomechanical) Therapy (Weak Recommendation, Moderate-Certainty Evidence)
Treatment of Isolated Distal (Calf) Deep Venous Thrombosis (Chest, 2021) (Chest Antithrombotic Therapy for VTE Disease 2021 Guidelines) [MEDLINE]
Rationale
Approximately 15% of Untreated Distal Deep Venous Thromboses Will Ultimately Extend Proximally into the Popliteal Vein and May Cause Acute Pulmonary Embolism (Chest, 2016) [MEDLINE]
Patients at High Risk for Bleeding are More Likely to Benefit from Serial Imaging
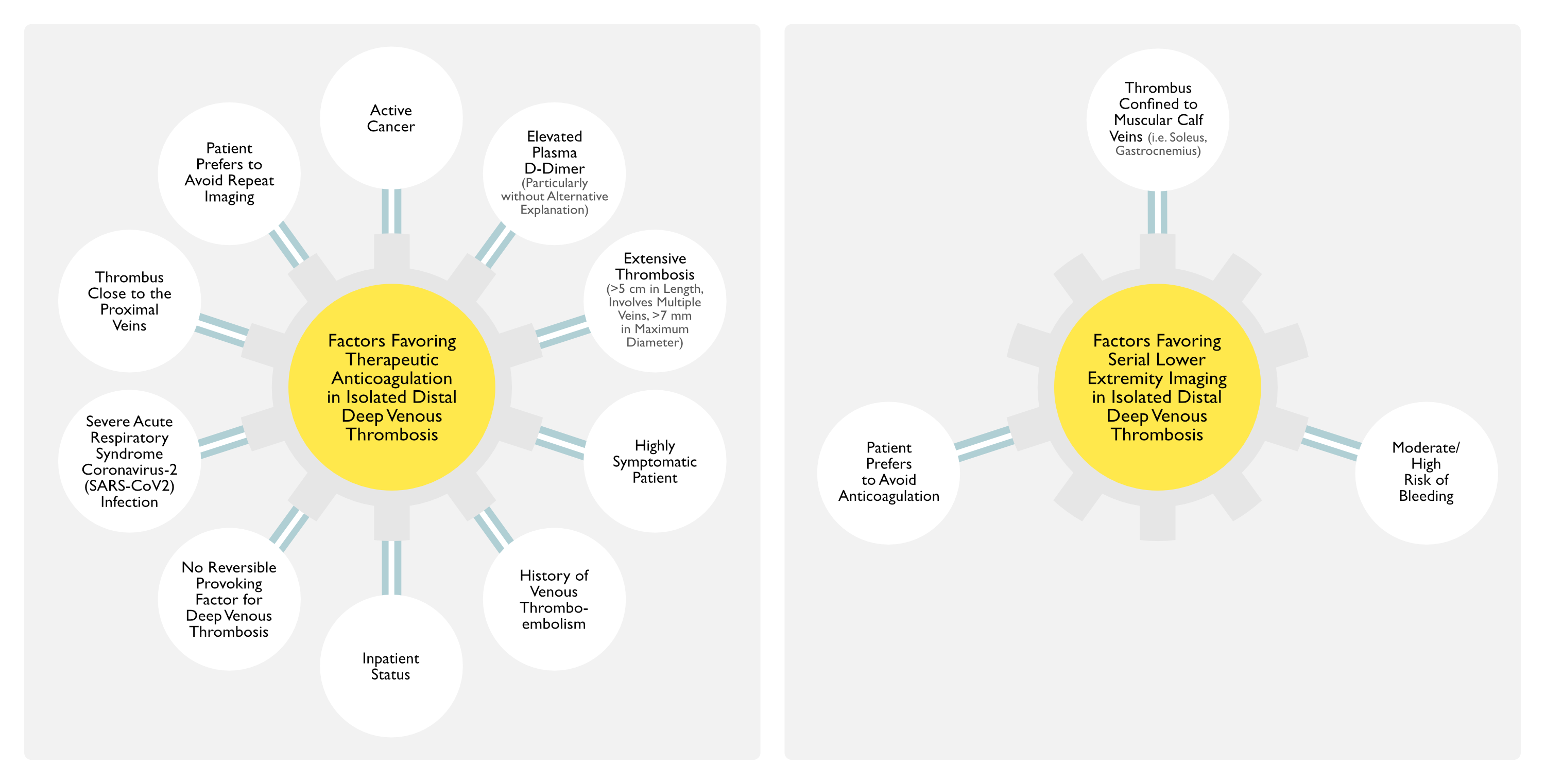
General Factors Which Favor Anticoagulation
Active Cancer
Elevated Plasma D-Dimer (Particularly When Markedly So without an Alternative Explanation) (see Elevated Plasma D-Dimer)
Extensive Thrombosis (Involving Multiple Veins >5 cm in Length, >7 mm in Maximum Diameter)
Highly Symptomatic Patient
History of Venous Thromboembolism
Inpatient Status
No Reversible Provoking Factor for Deep Venous Thrombosis
General Factors Which Favor Serial Lower Extremity Imaging
Thrombus Confined to Muscular Calf Veins (i.e. Soleus, Gastrocnemius)
Moderate/High Risk of Bleeding
Patient Prefers to Avoid Anticoagulation
Isolated Distal Deep Venous Thrombosis without Severe Symptoms or Risk Factors for Extension (See Below)
Serial Lower Extremity Dopplers x 2 wks are Recommended (Weak Recommendation, Moderate-Certainty Evidence)
Serial Lower Extremity Dopplers Should Be Performed Once Weekly or with Worsening Symptoms
During Surveillance
If Thrombus Does Not Extend within the Distal Veins, Anticoagulation is Not Recommended (Strong Recommendation, Moderate-Certainty Evidence)
If Thrombus Extends within the Distal Veins, Anticoagulation is Suggested (Weak Recommendation, Very Low-Certainty Evidence)
If Thrombus Extends into the Proximal Veins, Anticoagulation is Recommended (Strong Recommendation, Moderate-Certainty Evidence)
Isolated Distal Distal Deep Venous Thrombosis with Severe Symptoms or Risk Factors for Extension (See Below)
Anticoagulation is Recommended (Weak Recommendation, Low-Certainty Evidence)
Risk Factors for Extension of Distal Deep Venous Thrombosis
Active Cancer
Elevated Plasma D-Dimer (Particularly When Markedly So without an Alternative Explanation) (see Elevated Plasma D-Dimer)
Extensive Thrombosis (Involving Multiple Veins >5 cm in Length, >7 mm in Maximum Diameter)
History of Venous Thromboembolism
Inpatient Status
No Reversible Provoking Factor for Distal Deep Venous Thrombosis
Thrombosis Close to Proximal Veins
Note: Thrombosis Confined to the Muscular Veins of the Calf (Soleus, Gastrocnemius) has a Lower Risk of Extension than Thrombosis that Involves the Axial (True Deep: Peroneal, Tibial) Veins
Treatment of Lower Extremity Superficial Venous Thrombosis (SVT)
In Patients with Lower Extremity Superficial Venous Thrombosis (SVT) at Increased Risk of Clot Progression to Deep Venous Thrombosis or Acute Pulmonary Embolism (Per the Factors Below), Anticoagulation for 45 Days is Recommended Over No Anticoagulation (Weak Recommendation, Moderate-Certainty Evidence)
Factors Which Favor the Use of Anticoagulation in Patients with Superficial Venous Thrombosis
Active Cancer
Extensive Superficial Venous Thrombosis
History of Venous Thromboembolism or Superficial Venous Thrombosis
Involvement Above the Knee (Particularly if Close to the Saphenofemoral Junction)
Involvement of the Greater Saphenous Vein
Recent Surgery
Severe Symptoms
In Patients with Superficial Venous Thrombosis Who are Treated with Anticoagulation, Fondaparinux (2.5 mg Daily) is Recommended Over Other Anticoagulant Regimens Such as Prophylactic or Therapeutic Dose Low Molecular Weigh Heparins (Weak Recommendation, Low-Certainty Evidence)
In Patients with Superficial Venous Thrombosis Who Refuse or are Unable to Use Parenteral Anticoagulation, Rivaroxaban 10 mg Daily is Recommended as a Reasonable Alternative to Fondaparinux (2.5 mg Daily) (Weak Recommendation, Low-Certainty Evidence)
Recommendations (Chest Antithrombotic Therapy and Prevention of Thrombosis 2012 Guidelines) [MEDLINE]
Anticoagulation is Recommended for Upper Extremity Deep Venous Thrombosis Involving the Axillary or More Proximal Veins
Catheter-Directed Thrombolysis of Upper Extremity Deep Venous Thrombosis Which Involves Axillary or More Proximal Veins
Indications (Patients Most Likely to Benefit from Catheter-Directed Thrombolysis of Upper Extremity DVT) (Chest Antithrombotic Therapy for VTE Disease 2016 Guidelines) [MEDLINE]
Good Functional Status
Life Expectancy of ≥1 Year
Low Risk of Hemorrhage
Severe Symptoms
Symptoms Present for <14 Days
Thrombus Involving Most of the Axillary and Subclavian Vein
Recommendations (Chest Antithrombotic Therapy for VTE Disease 2016 Guidelines) [MEDLINE]
Anticoagulation is Recommended Over Catheter-Directed Thrombolysis in Upper Extremity Deep Venous Thrombosis (Grade 2C Recommendation)
In Patients Who Undergo Catheter-Directed Thrombolysis of Upper Extremity Deep Venous Thrombosis, the Same Intensity/Duration of Anticoagulation is Recommended as in Those Who Do Not Undergo Thrombolysis (Grade 1B Recommendation)
Follow-Up of Acute Pulmonary Embolism
Recommendations for Follow-Up of Acute Pulmonary Embolism (Consensus Practice from the PERT Consortium, 2019) (Clin Appl Thromb Hemost, 2019) [MEDLINE]
Acute Pulmonary Embolism Patients Should Have a Short Interval Follow-Up Visit (2 wks-3 mos) Post-Pulmonary Embolism, or Sooner if Symptoms or Patient Complexity Suggest the Need for This
Expert Follow-Up with the PERT Team is Recommended
The Initial Post-Discharge Visit Should Focus on the Patient’s Clinical Status, Anticoagulation Regimen (Type, Dose, Duration, Compliance, and Tolerance), Consideration for Inferior Vene Cave Filter Removal, Evaluation of Thrombophilia and Age-Appropriate Cancer Screening
Patients with Persistent or Recurrent Symptoms, Particularly After 3 mos, Merit Follow-Up Testing
If Chronic Thromboembolic Pulmonary Hypertension (CTEPH) is Highly Suspected or Confirmed, the Patient Should Be Referred to an Expert CTEPH Center
Randomized Controlled Trial of the Effect on Exercise Training on Residual Dyspnea After Acute Pulmonary Embolism (Chest, 2023) [MEDLINE]: n = 211
At Follow-Up, the Rehabilitation Group Performed Better on the Incremental Shuttle Walk Test, as Compared to the Control Group (Mean Difference 53.0 m; 95% CI: 17.7-88.3; P = 0.0035)
The Rehabilitation Group Reported Better Scores on the Pulmonary Embolism-Quality of Life Questionnaire (Mean Difference -4%; 95% CI: -0.09 to 0.00; P = 0.041) at Follow-Up, But There were No Differences in Generic Quality of Life, Dyspnea Scores, or the Endurance Shuttle Walk Test
No Adverse Events Occurred During the Intervention
Prognosis
Mortality Rate
General Comments
Less than 10% of All Acute Pulmonary Emboli Result in Death
90% of Deaths Due to Acute Pulmonary Embolism Occur within the First 1-2 hrs
Contribution of Acute Pulmonary Embolism to United States Death Rate
High-Risk was Defined as Patients with Acute Pulmonary Embolism Who Were in Shock or Suffered Cardiac Arrest
From 1999-2017, 58,784 Patients were Hospitalized in United States with a Primary Diagnosis of Pulmonary Embolism that was High-Risk
Mortality in All High-Risk Patients Decreased from 72.7% in 1999 to 49.8% in 2017 (p < 0.0001)
Most High-Risk Patients, 60.3% were Treated with Anticoagulants Alone and Did Not Receive an Inferior Vena Cava Filter
Mortality in These Patients Decreased from 79.0% in 1999 to 55.7% in 2017 (p<0.0001)
Thrombolytic Therapy was Administered to 16.1% of High-Risk Patients, Open Pulmonary Embolectomy Alone was Used in 4.3%, and Extracorporeal Membrane Oxygenation was Used in 0.4%
Review of Acute Pulmonary Embolism (JAMA, 2022) [MEDLINE]
Incidence of Acute Pulmonary Embolism is Approximately 60-120 Per 100,000 People Per Year
Approximately 60,000-100,000 Patients Die from Acute Pulmonary Embolism Each Year in the United States
Prognostic Value of Deep Venous Thrombosis (DVT) Presenting with Acute Pulmonary Embolism (PE)
Clinical Data
Prospective Cohort Study of Presence of Deep Venous Thrombosis in Patients with First Episode of Acute Symptomatic Pulmonary Embolism (Am J Respir Crit Care Med, 2010) [MEDLINE]: n = 707
Multivariate Cox Proportional Hazards Regression was Performed to Adjust for Significant Covariates
Of the Patients Diagnosed with Acute Pulmonary Embolism, 51.2% Had Concomitant Deep Venous Thrombosis and 10.9% Died During Follow-Up
Patients with Concomitant Deep Venous Thrombosis Had an Increased All-Cause Mortality (Adjusted Hazard Ratio 2.05; 95% CI: 1.24-3.38; P = 0.005) and Pulmonary Embolism-Specific Mortality (Adjusted Hazard Ratio 4.25; 95% CI: 1.61-11.25; P = 0.04), as Compared to Those without Concomitant Deep Venous Thrombosis
In an External Validation Cohort of 4,476 Patients with Acute Pulmonary Embolism Enrolled in the International Multicenter RIETE Registry, Concomitant Deep Venous Thrombosis Remained a Significant Predictor of All-Cause (Adjusted Hazard Ratio 1.66; 95% CI: 1.28-2.15; P < 0.001) and Pulmonary Embolism-Specific Mortality (Adjusted Hazard Ratio 2.01; 95% CI: 1.18-3.44; P = 0.01)
References
Follow-Up of Acute Pulmonary Embolism (PE)
The effects of exercise training in patients with persistent dyspnoea after pulmonary embolism: a randomized controlled trial. Chest. Published online May 4, 2023. doi:10.1016/j.chest.2023.04.042 [MEDLINE]
A clinical trial of vena caval filters in the prevention of pulmonary embolism in patients with proximal deep vein thrombosis: Prévention du Risque d’Embolie Pulmonaire par Interruption Cave Study Group. N Engl J Med. 1998;338(7):409-415 [MEDLINE]
PREPIC Study Group. Eight-year follow-up of patients with permanent vena cava filters in the prevention of pulmonary embolism: the PREPIC (Prevention du Risque d’Embolie Pulmonaire par Interruption Cave) randomized study. Circulation. 2005;112(3):416-422 [MEDLINE]
A population-based study of inferior vena cava filters in patients with acute venous thromboembolism. Arch Intern Med. 2010;170(16): 1456-1462 [MEDLINE]
Increasing use of vena cava filters for prevention of pulmonary embolism. Am J Med. 2011;124(7):655-661 [MEDLINE]
PREPIC2 Trial. Effect of a retrievable inferior vena cava filter plus anticoagulation vs anticoagulation alone on risk of recurrent pulmonary embolism: a randomized clinical trial. JAMA. 2015 Apr 28;313(16):1627-35. doi: 10.1001/jama.2015.3780 [MEDLINE]
Prognosis
Prognostic significance of deep vein thrombosis in patients presenting with acute symptomatic pulmonary embolism. Am J Respir Crit Care Med. 2010 May 1;181(9):983-91. doi: 10.1164/rccm.200908-1204OC [MEDLINE]
19-Year Trends in Mortality of Patients Hospitalized in the United States with High-Risk Pulmonary Embolism. Am J Med. 2021 Feb 22;S0002-9343(21)00108-X. doi: 10.1016/j.amjmed.2021.01.026 [MEDLINE]
Acute Pulmonary Embolism: A Review. JAMA. 2022 Oct 4;328(13):1336-1345. doi: 10.1001/jama.2022.16815 [MEDLINE]