Pulmonary Embolism Response Teams (PERT) Have Been Put into Practice in Many Centers to Facilitate the More Eficient Management of Patients with Acute Pulmonary Embolism (Particularly with Regard to Rapid Identification and Deployment of Systemic Thrombolytics, Catheter-Directed Thrombolysis, and Surgical Embolectomy)
Recommendations (European Society of Cardiology and European Respiratory Society Guidelines for the Diagnosis and Management of Acute Pulmonary Embolism, 2019) (Eur Heart J, 2020) [MEDLINE]
Set-Up of a Multidisciplinary Team and Program for the Management of High-Risk (and in Selected Cases, Intermediate-Risk Acute Pulmonary Embolism) Should Be Considered, Depending on the Resources and Expertise Available in Each Hospital (Class IIa, Level C)
Recommendations (Consensus Practice from the PERT Consortium, 2019) (Clin Appl Thromb Hemost, 2019) [MEDLINE]
Utilize a Multidisciplinary Pulmonary Embolism Response Team (PERT) in Patients with Intermediate or High-Risk Acute Pulmonary Embolism, as Well as for Acute Pulmonary Embolism Patients in Whom There is Uncertainty Regarding Treatment
General Goals of Anticoagulation in Venous Thromboembolism
Prevention of Early Complications of Venous Thromboembolism
General Comments
The Benefits of Anticoagulation are the Greatest During the Initial Period of Anticoagulation
Anticoagulation Decreases Risk of Deep Venous Thrombosis Recurrence and the Decreases the Mortality Rate (Lancet, 1960) [MEDLINE]
In Patients Admitted for Acute Pulmonary Embolism Through the Emergency Department, Early Anticoagulation was Associated with Decreased Mortality Rate (Chest, 2010) [MEDLINE]: n = 400 emergency department patients with acute pulmonary embolism (treated with unfractionated heparin from 2002-2005)
Overall, the In-Hospital Mortality Rate was 3.0% and 30-Day Mortality Rate was 7.7% in the Study
Patients Who Received Heparin in the Emergency Department Had Decreased In-Hospital Mortality Rate (1.4% vs 6.7%; P = 0.009) and Decreased 30-Day Mortality Rate (4.4% vs 15.3%; P < 0.001), as Compared to Patients Who Received Heparin After Admission
Patients Who Achieved a Therapeutic PTT within 24 hrs Had Decreased In-Hospital Mortality Rate (1.5% vs 5.6%; P = 0.093) and Decreased 30-Day Mortality Rate (5.6% vs 14.8%; P = .037), as Compared to Patients Who Achieved a Therapeutic PTT After 24 hrs
In Multiple Logistic Regression Models, Receiving Heparin in the Emergency Department Remained Predictive of Decreased Mortality Rate, and Intensive Care Unit Admission Remained Predictive of Increased Mortality Rate
Large Prospective Cohort Study of the Effects of Anticoagulation on Major Cardiovascular Events in Patients with Venous Thromboembolism (Chest, 2022) [MEDLINE]: n = 3,790
Treatment of Venous Thromboembolism for >3 Months was Associated with a Decreased Risk of Major Cardiovascular Events (Non-Fatal Acute Coronary Syndrome, Non-Fatal Stroke, and All-Cause Mortality)
Treatment of Venous Thromboembolism with Direct Oral Anticoagulant (DOAC) vs Coumadin was Associated with Decreased Risk of Major Cardiovascular Events
Prevention of Late Complications of Venous Thromboembolism
Prevention of Recurrent Deep Venous Thrombosis (DVT)
Anticoagulation Decreased Risk of DVT Recurrence and Mortality Rate (Lancet, 1960) [MEDLINE]
Anticoagulation Decreased the Risk of Recurrent Venous Thromboembolism to 3.4% and Risk of Fatal Venous Thromboembolism to 0.4% (Ann Intern Med, 2010) [MEDLINE]
Systematic Review and Meta-Analysis of Anticoagulation Regimens for Venous Thromboembolism (JAMA, 2014) [MEDLINE]: n = 45 trials (44,989 patients)
No Statistically Significant Differences (in Terms of Safety/Efficacy) Between Anticoagulation Regimens (Low Molecular Weight Heparin/Coumadin, Unfractionated Heparin/Coumadin, Fondaparinux/Coumadin, Low Molecular Weight Heparin with Dabigatran/Edoxaban, Apixaban, Rivaroxaban, or Low Molecular Weight Heparin Alone)
Combination of Unfractionated Heparin/Coumadin Appeared to Have the Highest Risk of Venous Thromboembolism Recurrence (Hazard Ratio 1.42)
Apixaban/Rivaroxaban Regimens were Associated with the Lowest Risk of Hemorrhage
Recommendations (European Society of Cardiology and European Respiratory Society Guidelines for the Diagnosis and Management of Acute Pulmonary Embolism, 2019) (Eur Heart J, 2020) [MEDLINE]
Intermediate/Low-Risk Pulmonary Embolism
In Patient without Hemodynamic Instability and with Intermediate/High Clinical Probability of Acute Pulmonary Embolism, Initiation of Anticoagulation is Recommended without Delay While Diagnostic Work-Up is in Progress (Class I, Level C)
If Anticoagulation is Initiated Parenterally, Low Molecular Weight Heparin or Fondaparinux is Recommended Over Unfractionated Heparin for Most Patients (Class I, Level A)
When Oral Anticoagulation is Started in a Patient with Acute Pulmonary Embolism Who is Eligible for a Direct Oral Anticoagulant (Apixaban, Dabigatran, Edoxaban, Rivaroxaban), a Direct Oral Anticoagulant is Recommended in Preference to Coumadin (Class I, Level A)
When Patients are Treated with Coumadin, Overlapping with Parenteral Anticoagulation is Recommended Until an INR of 2.5 (Range 2-3) is Reached (Class I, Level A)
Direct Oral Anticoagulant are Not Recommended in Patients with Severe Renal Impairment, During Pregnancy and Lactation, and in Patients with Antiphospholipid Antibody Syndrome (Class III, Level C)
Routine Use of Primary Systemic Thrombolysis is Not Recommended in Patients with Low-Intermediate Risk Acute Pulmonary Embolism (Class III, Level B)
Recommendations (Consensus Practice from the PERT Consortium, 2019) (Clin Appl Thromb Hemost, 2019) [MEDLINE]
Anticoagulation
Anticoagulation Should Be Initiated as Soon as Acute Pulmonary Embolism is Diagnosed (Unless Contraindicated)
Anticoagulation Should Be Initiated Even Prior to the Confirmed Diagnosis When the Clinical Suspicion of Acute Pulmonary Embolism is High and the Bleeding Risk is Low
Utilize Evidence-Based Institution-Specific Anticoagulation Guidelines to Assist in Anticoagulant Choice, Dosing, Administration, and Appropriate Laboratory Monitoring Strategies to Achieve Therapeutic Anticoagulation as Quickly as Possible
Risk Stratification for Anticoagulation-Associated Hemorrhage (Chest Antithrombotic Therapy for VTE Disease 2016 Guidelines) (Chest, 2016) [MEDLINE]
Risk Factors for Anticoagulation-Associated Hemorrhage
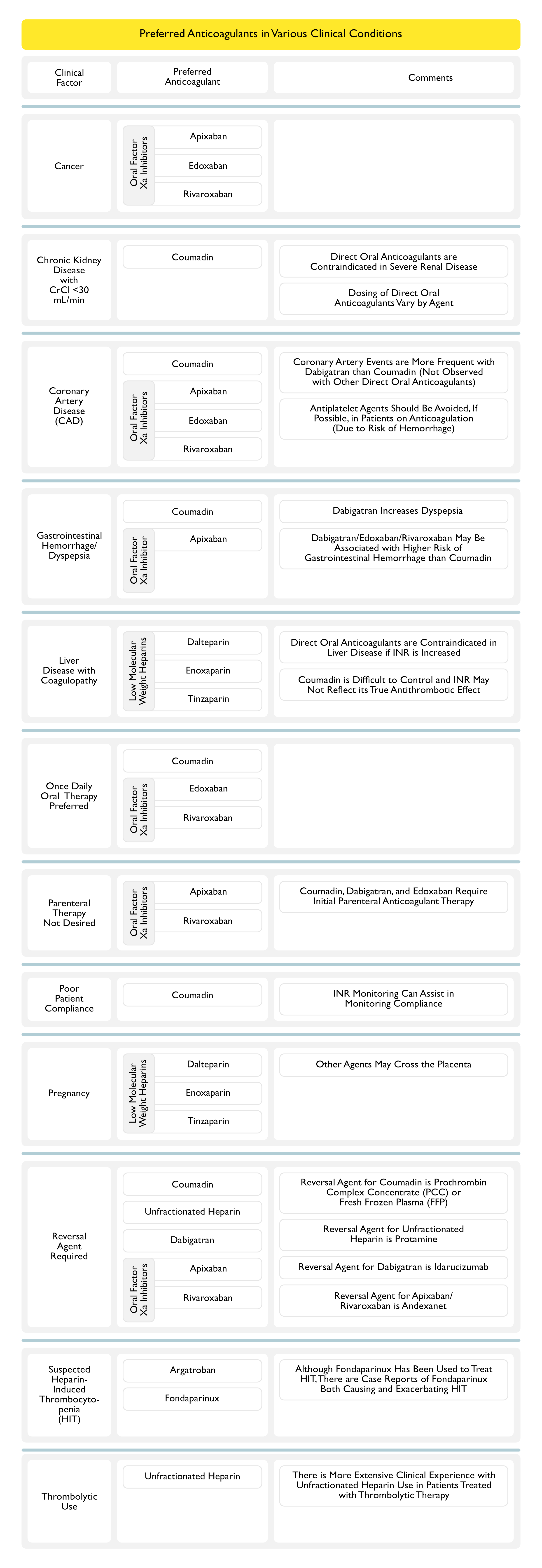
Clinical Features Which May Influence the Choice of Specific Initial/Long-Term Anticoagulants (Chest Antithrombotic Therapy for VTE Disease 2016 Guidelines) (Chest, 2016) [MEDLINE] (Chest Antithrombotic Therapy for VTE Disease 2021 Guidelines) (Chest, 2021) [MEDLINE]
Direct Oral Anticoagulants and Low Molecular Weight Heparins are Contraindicated with Severe Renal Insufficiency
Dosing of Direct Oral Anticoagulants are Variable, Dependent on the Agent
Systematic Review/Meta-Analysis Comparing Rates of Hemorrhage of Novel Oral Anticoagulants vs Coumadin When Used in the Setting of Renal Insufficiency (Chest, 2016) [MEDLINE]
CrCl 50-80 mL/min: direct oral anticoagulants had a significantly decreased risk of major bleeding, as compared to coumadin
CrCl <50 mL/min: direct oral anticoagulants had a non-significantly decreased risk of major bleeding, as compared to coumadin
Apixaban Had the Lowest Rate of Major Bleeding in this Subgroup
There is a More Extensive Clinical Experience with Unfractionated Heparin Use in Patients Treated with Thrombolytic Therapy
Cost/Coverage Issues
Preferred Agents
Variable
Clinical Data
Cost-Effectiveness of Rivaroxaban Compared to Enoxaparin/Coumadin in Treatment of Venous Thrombembolism (J Med Econ, 2014) [MEDLINE]
Rivaroxaban Cost $2,448 Per-Patient Less and was Associated with 0.0058 More QALY’s, as Compared with Enoxaparin + Coumadin
Cost-Effectiveness of Novel Oral Anticoagulants, Compared to Coumadin, in Non-Valvular Atrial Fibrillation and Venous Thromboembolism (J Med Econ, 2015) [MEDLINE]
Medical Costs are Reduced When Direct Oral Anticoagulants are Used Instead of Coumadin for the Treatment of Non-Valvular Atrial Fibrillation/Venous Thromboembolism, with Apixaban Being Associated with the Greatest Reduction in Medical Costs
UK Study of Cost-Effectiveness of Rivaroxaban Compared to Enoxaparin/Coumadin in Treatment of Venous Thrombembolism (Thromb J, 2015) [MEDLINE]
Rivaroxaban was a Cost-Effective Choice for Acute Treatment of Venous Thromboembolism and Secondary Prevention of Venous Thromboembolism, as Compared with Low Molecular Weight Heparin/Coumadin Treatment, Regardless of the Treatment Duration
Initial Treatment of Venous Thromboembolism (VTE) (Deep Venous Thrombosis or Acute Pulmonary Embolism)
Requirements for Initial Parenteral Anticoagulation with Specific Long-Term Anticoagulants
Parenteral Anticoagulation is Indicated Prior to Coumadin (see Coumadin)
Conversion from Parenteral Anticoagulation to Coumadin
Coumadin Should Be Started Concurrently with Parenteral Anticoagulation, Rather Than Waiting (Grade 2C Recommendation) (Chest Antithrombotic Therapy and Prevention of Thrombosis 2012 Guidelines) [MEDLINE]: start coumadin 5 mg qday (with a lower dose used in elderly or those with a high risk of bleeding, malnutrition, debility, congestive heart failure, or liver disease)
Coumadin Should Be Overlapped with Parenteral Anticoagulation for at Least 4-5 Days
Parenteral Anticoagulation Can Be Discontinued When INR Remains >2 for at Least 2 Consecutive Days
Parenteral Anticoagulation is Indicated Prior to Dabigatran (Pradaxa) (see Dabigatran)
Conversion from Unfractionated Heparin Drip/Argatroban Drip to Dabigatran: start dabigatran as soon as heparin drip is stopped
Conversion from Low Molecular Weight Heparin (Enoxaparin, Dalteparin, Tinzaparin) or Fondaparinux to Dabigatran: start dabigatran approximately 2 hrs prior to next scheduled dose of subcutaneous anticoagulant
Parenteral Anticoagulation is Indicated Prior to Edoxaban (Savaysa, Lixiana) (see Edoxaban)
Conversion from Unfractionated Heparin/Argatroban Drip to Edoxaban (Savaysa, Lixiana): discontinue heparin/argatroban drip and initiate edoxaban 4 hrs later
Conversion from Low Molecular Weight Heparin (Enoxaparin, Dalteparin, Tinzaparin) to Edoxaban: discontinue low molecular weight heparin and initiate edoxaban at the time of the next scheduled administration of low molecular weight heparin
Parenteral Anticoagulation is Not Indicated Prior to Apixaban (Eliquis)/Rivaroxaban (Xarelto) (see Apixaban and Rivaroxaban): monotherapy with these agents is considered safe and effective when administered as monotherapy (without heparin pre-treatment) to outpatients
EINSTEIN Trial Demonstrated that in Acute Symptomatic Deep Venous Thrombosis, Rivaroxaban “Monotherapy” was Non-Inferior to Enoxaparin (SQ) Followed by Coumadin (NEJM, 2010) [MEDLINE]
AMPLIFY Trial Demonstrated that in Acute Symptomatic Venous Thromboembolism, Apixaban “Monotherapy” was Non-Inferior to Enoxaparin (SQ) Followed by Coumadin and was Associated with Significantly Lower Risk of Bleeding (NEJM, 2013) [MEDLINE]
Parenteral Anticoagulant Dosing in Morbid Obesity (see Obesity)
Dosing Weight = Ideal Body Weight + 0.3 (Actual Body Weight – Ideal Body Weight)
Dosing weight = Ideal Body Weight + 0.4 (Actual Body Weight – Ideal Body Weight)
Long-Term Treatment of Venous Thromboembolism (VTE) (Deep Venous Thrombosis or Acute Pulmonary Embolism) without Cancer
Agents
First-Line Agents (Oral Anticoagulants)
General Comments
Risk of Bleeding with DOAC’s (and Particularly Intracranial Bleeding) is Less with DOAC’s than with Coumadin Therapy (Chest, 2021) [MEDLINE]
On the Basis of Patients with Atrial Fibrillation, Gastrointestinal Bleeding May Be Higher with Dabigatran, Edoxaban, and Rivaroxaban than with Coumadin Therapy, Although This Has Not Been Seen in Patients with Venous Thromboembolism (Chest, 2021) [MEDLINE]
However, on the Basis of Indirect Comparisons and Studies Reporting on DOAC’s for the Treatment of Cancer-Associated Thrombosis, the Risk of Bleeding May Be Lower with Apixaban than with Other DOAC’s (Chest, 2021) [MEDLINE]
Specific Reversal Agents for DOAC’s Have Been Approved (Yet Even Before the Availability of These, the Risk that a Major Bleed Will Be Fatal Appears to Be No Higher for DOAC’s than for Coumadin Therapy) (Chest, 2021) [MEDLINE]
Direct Comparison Between DOAC’s is Very Limited, But Suggests that Apixaban May Carry a Lower Risk of Bleeding than Other DOAC’s (Chest, 2021) [MEDLINE]
Recommendations (American Society of Hematology Guidelines for the Management of Venous Thromboembolism, 2020) (Blood Adv, 2020) [MEDLINE]
For Patients with Venous Thromboembolism, Use of Direct Oral Anticoagulants (DOAC’s) is Recommended Over Coumadin (Conditional Recommendation, Moderate Certainty in the Evidence)
This Recommendation May Not Apply to Patients with the Following
For Patients with Venous Thromboembolism, There is No Recommendation of One DOAC Over Another (Conditional Recommendation, Very Low Certainty in the Evidence)
Factors Which May Influence the Selection of a Specific DOAC
Cancer
Concomitant Medications (Need for a Concomitant Drug Metabolized Through the CYP3A4 Enzyme or P-Glycoprotein)
Once vs Twice Daily Dosing
Out-of-Pocket Cost
Renal Function
Requirement for Lead-In Parenteral Anticoagulation
For Patients with Deep Venous Thrombosis and/or Acute Pulmonary Embolism with Stable Cardiovascular Disease Who Initiate Anticoagulation and were Previously Taking Aspirin for Cardiovascular Risk Modification, Suspending Aspirin is Recommended Over Continuing it for the Duration of Anticoagulation Therapy (Conditional Recommendation, Very Low Certainty in the Evidence)
A Critical Review of the Indication for Aspirin Therapy is Needed at the Time Anticoagulant Therapy is Initiated, Considering the Increased Risk of Bleeding vs the Potential Benefit in Terms of Cardiovascular Prevention
This Recommendation Does Not Apply to Patients with a Recent Acute Coronary Event or Coronary Intervention
In Patients with Venous Thromboembolism (Lower Extremity Deep Venous Thrombosis or Acute Pulmonary Embolism), Apixaban/Dabigatran/Edoxaban/Rivaroxaban are Recommended Over Coumadin as the Treatment-Phase (First 3 Months) Anticoagulant Therapy (Strong Recommendation, Moderate-Certainty Evidence)
Long-Term Treatment of Venous Thromboembolism (VTE) (Deep Venous Thrombosis or Acute Pulmonary Embolism) with Cancer
Agents
First-Line Agents (Oral Xa Inhibitors)
General Comments
Risk of Bleeding with DOAC’s (and Particularly Intracranial Bleeding) is Less with DOAC’s than with Coumadin Therapy (Chest, 2021) [MEDLINE]
On the Basis of Patients with Atrial Fibrillation, Gastrointestinal Bleeding May Be Higher with Dabigatran, Edoxaban, and Rivaroxaban than with Coumadin Therapy, Although This Has Not Been Seen in Patients with Venous Thromboembolism (Chest, 2021) [MEDLINE]
However, on the Basis of Indirect Comparisons and Studies Reporting on DOAC’s for the Treatment of Cancer-Associated Thrombosis, the Risk of Bleeding May Be Lower with Apixaban than with Other DOAC’s (Chest, 2021) [MEDLINE]
Specific Reversal Agents for DOAC’s Have Been Approved (Yet Even Before the Availability of These, the Risk that a Major Bleed Will Be Fatal Appears to Be No Higher for DOAC’s than for Coumadin Therapy) (Chest, 2021) [MEDLINE]
In Patients with Venous Thromboembolism and Cancer (Cancer-Associated Thrombosis, There is a Higher Risk for Recurrence as Well as a Higher Risk for Major Bleeding than in Patients with Venous Thromboembolism without Cancer (Chest, 2021) [MEDLINE]
Systematic Review and Meta-Analysis of Treatment of Venous Thromboembolism in Patients with Cancer (Lancet Oncol, 2008) [MEDLINE]
Long-Term Full-Dose Low Molecular Weight Heparin is More Effective than Coumadin in the Secondary Prophylaxis of Venous Thromboembolism in Patients with Cancer of Any Stage, Performance Status, or Prognosis
Optimum Treatment Duration is Unclear, But Because the Prothrombotic Tendency Will Persist in Patients with Advanced Cancer, Indefinite Treatment is Generally Recommended
Unblinded, Comparative Effectiveness, Noninferiority Randomized CANVAS Trial of Direct Oral Anticoagulants vs Low Molecular Weight Heparin in Patients with Diagnosis of New Venous Thromboembolism and Cancer (JAMA, 2023) [MEDLINE]: n = 638 (from 67 oncology practices in the US)
Rates of Recurrent Venous Thromboembolism were 6.1% in the Direct Oral Anticoagulant Group and 8.8% in the Low Molecular Weight Heparin Group (Difference -2.7%; 1-sided 95% CI: -100% to 0.7%) Consistent with the Prespecified Noninferiority Criterion
Of the 6 Prespecified Secondary Outcomes, None were Statistically Significant
Major Bleeding Occurred in 5.2% of Participants in the Direct Oral Anticoagulant Group and 5.6% in the Low Molecular Weight Heparin Group (Difference -0.4%; 1-sided 95% CI: -100% to 2.5%) and Did Not Meet the Noninferiority Criterion
Severe Adverse Events Occurred in 33.8% of Participants in the Direct Oral Anticoagulant Group and 35.1% in the Low Molecular Weight Heparin Group
The Most Common Serious Adverse Events were Anemia and Death
Recommendations (American Society of Hematology Guidelines for the Management of Venous Thromboembolism, 2020) (Blood Adv, 2020) [MEDLINE]
For Patients with Venous Thromboembolism, Use of Direct Oral Anticoagulants (DOAC’s) is Recommended Over Coumadin (Conditional Recommendation, Moderate Certainty in the Evidence)
This Recommendation May Not Apply to Patients with the Following
For Patients with Venous Thromboembolism, There is No Recommendation of One DOAC Over Another (Conditional Recommendation, Very Low Certainty in the Evidence)
Factors Which May Influence the Selection of a Specific DOAC
Cancer
Concomitant Medications (Need for a Concomitant Drug Metabolized Through the CYP3A4 Enzyme or P-Glycoprotein)
Once vs Twice Daily Dosing
Out-of-Pocket Cost
Renal Function
Requirement for Lead-In Parenteral Anticoagulation
In Patients with Venous Thromboembolism (Lower Extremity Deep Venous Thrombosis or Acute Pulmonary Embolism) in the Setting of Cancer (Cancer-Associated Thrombosis), Oral Xa Inhibitors (Apixaban, Edoxaban, Rivaroxaban) are Recommended Over Low Molecular Weight Heparin for the Initiation and Treatment Phases of Anticoagulant Therapy (Strong Recommendation, Moderate-Certainty Evidence)
Edoxaban and Rivaroxaban Appear to Be Associated with a Higher Risk of Gastrointestinal Major Bleeding than Low Molecular Weight Heparins in Patients with Cancer-Associated Thrombosis and a Luminal Gastrointestinal Malignancy, While Apixaban Does Not
Consequently, Apixaban or Low Molecular Weight Heparins May Be the Preferred Options in Patients with Luminal Gastrointestinal Malignancies
Duration of Anticoagulation
General Comments
Subgroups of Patients with Venous Thromboembolism (Chest, 2021) [MEDLINE]
Venous Thromboembolism Provoked by Surgery (a Major Transient Risk Factor): 3% recurrence rate at 5 yrs
Venous Thromboembolism Provoked by a Nonsurgical Transient Risk Factor (Estrogen Therapy, Pregnancy, Leg Injury, Flight of >8 hrs): 15% recurrence rate at 5 yrs
Unprovoked (Idiopathic) Venous Thromboembolism (Not Meeting Criteria for Provocation by a Transient Risk Factor or by Cancer): 30% recurrence rate at 5 yrs
Recommendations (American Society of Hematology Guidelines for the Management of Venous Thromboembolism, 2020) (Blood Adv, 2020) [MEDLINE]
For Primary Treatment of Patients with Venous Thromboembolism (Whether Provoked by a Transient Risk Factor or by a Chronic Risk Factor or Unprovoked, Use of a Shorter Course of Anticoagulation for Primary Treatment (3-6 mos) is Recommended Over a Longer Course of Anticoagulation for Primary Treatment (6-12 mos) (Conditional Recommendations, Moderate Certainty in the Evidence
These Recommendations are Intended to Address the Duration of Primary Anticoagulant Treatment for All Patients with Deep Venous Thrombosis and/or Acute Pulmonary Embolism, Defined as the Minimal Length of Time for Treatment of the Initial Venous Thromboembolism
Most Patients with Deep Venous Thrombosis and/or Acute Pulmonary Embolism Provoked by Temporary Risk Factors Will Discontinue Anticoagulant Therapy After Completion of the Primary Treatment
In Contrast, Many Patients with Deep Venous Thrombosis and/or Acute Pulmonary Embolism Provoked by Chronic Risk Factors, as Well as Patients with Unprovoked Deep Venous Thrombosis and/or Acute Pulmonary Embolism, May Continue Anticoagulant Therapy Indefinitely for Secondary Prevention After Completion of the Primary Treatment
However, if Patient and Clinician Decides to Stop Anticoagulation, Use of a Longer Course of Primary Anticoagulant Therapy (6-12 mos) is Not Recommended
For Selected Patients with a Chronic Risk Factor for Which Some Improvement is Expected Over Time (Due to Improved Mobility with Rehabilitation, etc), a Longer Course of Anticoagulation for the Primary Treatment Phase (6-12 mos) Could Be Justified
For Patients with Unprovoked Deep Venous Thrombosis and/or Acute Pulmonary Embolism, Routine Use of Prognostic Scores, D-Dimer Testing, or Ultrasound to Detect Residual Vein Thrombosis are Not Recommended to Guide the Duration of Anticoagulation (Conditional Recommendations, Very Low Certainty in the Evidence)
Indefinite Anticoagulation is Probably Appropriate for the Majority of Patients with Unprovoked Venous Thromboembolism
However, in Certain Circumstances, Such as When Patients are Undecided or the Balance Between Risks and Benefits is Uncertain, Clinicians and Patients May Use Prognostic Scores, D-Dimer Testing, or Ultrasound Assessment for Residual Thrombosis from an Initial Deep Venous Thrombosis to Aid in Reaching a Final Decision
After Completion of Primary Treatment of Deep Venous Thrombosis and/or Acute Pulmonary Embolism Provoked by a Chronic Risk Factor, Indefinite Antithrombotic Therapy is Recommended Over Stopping Anticoagulation (Conditional Recommendation, Moderate Certainty in the Evidence)
Patients with Deep Venous Thrombosis and/or Acute Pulmonary Embolism Provoked by a Transient Risk Factor Typically Do Not Require Antithrombotic Therapy after Completion of Primary Treatment
This Recommendation Refers to Patients with Deep Venous Thrombosis and/or Acute Pulmonary Embolism Provoked by a Chronic Persistent Risk Factor
However, This Recommendation Does Not Apply to Patients Who Have a High Risk for Bleeding Complications
After Completion of Primary Treatment for Patients with Unprovoked Deep Venous Thrombosis and/or Acute Pulmonary Embolism, Indefinite Antithrombotic Therapy is Recommended Over Stopping Anticoagulation (Conditional Recommendation, Moderate Certainty in the Evidence)
This Recommendation Does Not Apply to Patients Who Have a High Risk for Bleeding Complications
For Patients with Deep Venous Thrombosis and/or Acute Pulmonary Embolism Who Have Completed Primary Treatment and Will Continue to Receive Secondary Prevention, the Use of Anticoagulation is Recommended Over Aspirin (Conditional Recommendation, Moderate Certainty in the Evidence)
For Patients with Deep Venous Thrombosis and/or Acute Pulmonary Embolism Who Have Completed Primary Treatment and Will Continue Coumadin as Secondary Prevention, the Use of International Normalized Ratio (INR) Range of 2-3 is Recommended Over a Lower INR Range (1.5-1.9) (Strong Recommendation, Moderate Certainty in the Evidence)
For Patients with Deep Venous Thrombosis and/or Acute Pulmonary Embolism Who Have Completed Primary Treatment and Will Continue with a DOAC for Secondary Prevention, Use of Either a Standard-Dose DOAC or a Lower-Dose DOAC is Recommended (Conditional Recommendation, Moderate Certainty in the Evidence)
Lower-Dose DOAC Regimens Which May Be Considered for Patients Who Have Completed Primary Treatment and Will Continue with a DOAC Include the Following
In Patients with Acute Venous Thromboembolism Who Do Not Have a Contraindication, a 3 Month Treatment Phase of Anticoagulation is Recommended (Strong Recommendation, Moderate-Certainty Evidence)
Upon Completion of the 3 Month Treatment Phase of Therapy, All Patients Should Be Assessed for Extended-Phase Therapy
In Patients with Venous Thromboembolism Diagnosed in the Setting of a Major Transient Risk Factor, Extended-Phase Anticoagulation is Not Recommended (Strong Recommendation, Moderate-Certainty Evidence)
Confinement to Bed in Hospital (Only “Bathroom Privileges”) for ≥3 Days with an Acute Illness
Surgery with General Anesthesia for >30 min
In Patients with Venous Thromboembolism Diagnosed in the Setting of a Minor Transient Risk Factor, Extended-Phase Anticoagulation is Not Recommended (Weak Recommendation, Moderate-Certainty Evidence)
Minor Transient Risk Factors
Admission to Hospital for <3 Days with an Acute Illness
Confinement to Bed Out of Hospital for ≥3 Days with an Acute Illness
Leg Injury Associated with Reduced Mobility for ≥3 Days
In Patients with Venous Thromboembolism Diagnosed in the Absence of Transient Provocation (Unprovoked Venous Thromboembolism or Provoked by Persistent Risk Factor), Extended-Phase Anticoagulation with a DOAC is Recommended (Strong Recommendation, Moderate-Certainty Evidence)
In Patients with Venous Thromboembolism Diagnosed in the Absence of Transient Risk Factor (Unprovoked Venous Thromboembolism or Provoked by a Persistent Risk Factor) Who Cannot Receive a DOAC, Extended-Phase Anticoagulation with Coumadin is Recommended (Weak Recommendation, Moderate-Certainty Evidence)
The Recommendation to Offer Extended-Phase Anticoagulation Would Not Automatically Imply that All Patients with Unprovoked Venous Thromboembolism Receive Extended Therapy
Patient Preference and Predicted Risk of Recurrent Venous Thromboembolism or Bleeding Should Also Influence the Decision to Proceed with, or Continue, Extended-Phase Anticoagulation Therapy
Patients Who Receive Extended-Phase Anticoagulation Should Have This Decision Reevaluated at Least Annually, and at Times of Significant Change in Health Status
Extended-Phase anticoagulation Does Not Have a Predefined Stop Date
However, Studies of Extended-Phase anticoagulation Monitored Patients for Durations of About 2-4 yrs
Although Most Patients in These Studies Did Not Stop Anticoagulation Therapy at the End of Follow-Up, the Risk-to-Benefit Balance of Continuing Extended Anticoagulation Therapy Beyond THis Time is Uncertain
In Patients Offered Extended-Phase Anticoagulation, Use of Reduced-Dose Apixaban (2.5 mg BID) or Rivaroxaban (10 mg qday) is Recommended Over Full-Dose Apixaban or Rivaroxaban (Weak Recommendation, Very Low-Certainty Evidence)
In Patients Offered Extended-Phase Anticoagulation, Reduced-Dose DOAC (Apixaban 2.5 mg BID or Rivaroxaban 10 mg qday) is Recommended Over Aspirin or No Therapy (Strong Recommendation, Low-Certainty Evidence) and Rivaroxaban is Recommended Over Aspirin (Weak Recommendation, Moderate-Certainty Evidence)
Rivaroxaban is the Only DOAC to Be Directly Compared to Aspirin for Secondary Prevention of Venous Thromboembolism
Several Other DOACs, as Well as Coumadin, are Also Acceptable for Secondary Prevention (Extended-Phase Therapy) After Venous Thromboembolism
In Patients with an Unprovoked Proximal Deep Venous Thrombosis or Acute Pulmonary Embolism Who are Stopping Anticoagulation and Do Not Have a Contraindication to Aspirin, Aspirin is Recommended Over No Aspirin to Prevent Recurrent Venous Thromboembolism (Weak Recommendation, Low-Certainty Evidence)
Because Aspirin Has Been Shown to Be Much Less Effective at Preventing Recurrent Venous Thromboembolism than Anticoagulants, and Because Some Anticoagulants Confer a Similar Risk of Bleeding to Aspirin, We Do Not Consider Aspirin a Reasonable Alternative to Anticoagulation in Patients Who Want Extended Therapy
However, if a Patient Has Decided to Stop Anticoagulation, Prevention of Recurrent Venous Thromboembolism is One of the Benefits of Aspirin Which Needs to Be Balanced Against Aspirin’s Risk of Bleeding and Inconvenience
Use of Aspirin Should Also Be Reevaluated
Treatment of Acute Pulmonary Embolism with Hypotension (i.e. High-Risk or “Massive” Acute Pulmonary Embolism)
Therapeutic Choices
Systemic Thrombolytic Therapy
Systemic Thrombolytic Therapy Accelerates Resolution of Pulmonary Embolism (with More Rapid Lowering of Pulmonary Artery Pressure, Improved Hypoxemia, and Resolution of Perfusion Scan Defects)
However, Systemic Thrombolytic Therapy Also Increases the Risk of Hemorrhage
Catheter-Based (Mechanical-Only) Techniques for Thrombus Removal Involve Fragmentation of the Thrombus Using Various Types of Catheters (Some of Which are Designed for this Purpose)
Thrombus Fragmentation Results in Distal Displacement of the Thrombus with/without Suctioning and Removal of Some of the Thrombus Through the Catheter
Catheter-Directed Thrombolysis Uses Approximately 33% of the Dose of Thrombolytic That Systemic Thrombolysis Uses (Lowering the Risk of Hemorrhage in Brain, Gastrointestinal Trac, etc)
Catheter-Directed Thrombolysis Achieves Higher Local Concentrations of Thrombolytics at the Site of the Pulmonary Embolism and Also Facilitates Thrombus Fragmentation and Permeability Via the Catheter
Systematic Review of Venoarterial Extracorporeal Membrane Oxygenation in Massive Acute Pulmonary Embolism (Crit Care Med, 2021) [MEDLINE]
Venoarterial Extracorporeal Membrane Oxygenation Has an Emerging Role in the Management of Massive Acute Pulmonary Embolism-Related Cardiac Arrest with 61% Survival
Systemic Thrombolysis Preceding Venoarterial Extracorporeal Membrane Oxygenation Did Not Confer a Statistically Significant Increase in the Risk of Death, Yet Age >65 y/o and Cannulation During Cardiopulmonary Resuscitation were Associated with a 3-Fold and 6-Fold Risks of Death, Respectively
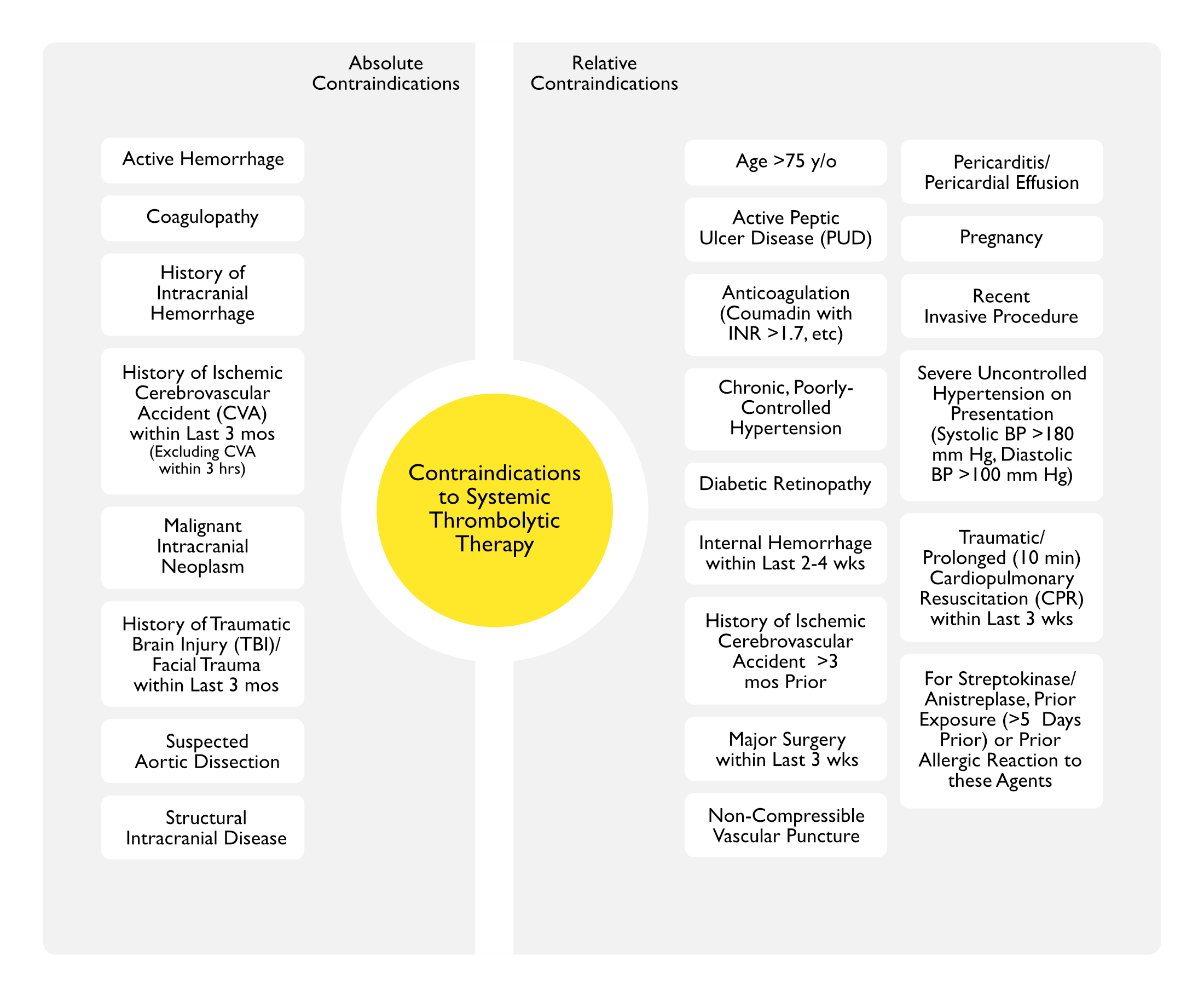
Absolute Contraindications to Systemic Thrombolytic Therapy (Chest Antithrombotic Therapy and Prevention of Thrombosis 2012 Guidelines) [MEDLINE]
History of Ischemic Cerebrovascular Accident (CVA) within Last 3 mos (Excluding Cerebrovascular Accident within the Last 3-4.5 hrs) (see Ischemic Cerebrovascular Accident)
Malignant Intracranial Neoplasm
History of Traumatic Brain Injury (TBI)/Facial Trauma within Last 3 mos (see Traumatic Brain Injury)
Severe Uncontrolled Hypertension on Presentation (Systolic BP >180 mm Hg, Diastolic BP >100 mm Hg)
Traumatic/Prolonged (>10 min) Cardiopulmonary Resuscitation (CPR) within Last 3 wks (see Cardiopulmonary Resuscitation)
For Streptokinase/Anistreplase, Prior Exposure (>5 Days Prior) or Prior Allergic Reaction to these Agents
Clinical Efficacy of Systemic Thrombolysis in Acute Pulmonary Embolism
Meta-Analysis of Thrombolysis in Acute PE (JAMA, 2014) [MEDLINE]: meta-analysis (16 trials, n = 2115)
Thrombolysis Decreased the Mortality Rate (2.17%), as Compared to Anticoagulation Alone (3.89%)
No Mortality Benefit was Observed in Patients >65 y/o, a Population in Whom the Risk of Hemorrhage was the Greatest
Thrombolysis Decreased the Risk of Recurrent PE (1.17%) as Compared to Anticoagulation Alone (3.04%)
Thrombolysis Increased the Risk of Major Hemorrhage (9.2%), as Compared to Anticoagulation Alone (3.4%)
No Significant Difference in Major Hemorrhage in Patients ≤65 y/o
Thrombolysis Increased the Risk of Intracranial Hemorrhage (1.5%), as Compared to Anticoagulation Alone (0.2%)
PEITHO Randomized Controlled Trial of Tenecteplase Thrombolysis (30-50 mg) in Normotensive Intermediate-Risk Pulmonary Embolism (Right Ventricular Dysfunction on Echocardiogram or CT PA Angiogram, Elevated Serum Troponin) (NEJM, 2014) [MEDLINE]: n = 1006 (mean age: 66.15 y/o; SD: 15.29)
Intention-to-Treat Analysis
Tenecteplase Thrombolysis Decreased Hemodynamic Decompensation/Death (2.6%), as Compared to Placebo Group (Anticoagulation Alone) (5.6%) (Odds Ratio 0.44; 95% CI: 0.23–0.87; P = 0.02)
Tenecteplase Thrombolysis (1.2%) Had No Impact on 7-Day Mortality Rate, as Compared to Placebo Group (Anticoagulation Alone) (1.8%) (P = 0.42)
Tenecteplase Thrombolysis (2.4%) Had No Impact on 30-Day Mortality Rate, as Compared to Placebo Group (Anticoagulation Alone) (3.2%) (P = 0.42)
Extracranial Bleeding Occurred in 6.3% in the Tenecteplase Group vs 1.2% in the Placebo Group (P < 0.001)
Stroke Occurred in 2.4% in the Tenecteplase Group (Hemorrhagic in 10 Patients vs 0.2% in the Placebo Group (Hemorrhagic in 1 That One Patient) (P = 0.003)
Mean Time Between Randomization and Death/Hemodynamic Compensation was 1.79 ± 1.6 Days in the Heparin Only (Placebo) Arm
Therefore, in Patients with Intermediate Risk Acute Pulmonary Embolism, Anticoagulation with Unfractionated Heparin/Low Molecular Weight Heparin for 2-3 Days Seems Reasonable Before Switching to Oral Anticoagulation (Eur Heart J, 2020) [MEDLINE]
Clinical Efficacy of Catheter-Directed Therapy in Acute Pulmonary Embolism
Catheter-Based Thrombus Removal Without Thrombolytic Therapy (Suction Thrombectomy)
Percutaneous Mechanical Thrombectomy with the FlowTriever System was Safe and Effective in Patients with Acute Intermediate-Risk Pulmonary Embolism, with Significant Improvement in RV/LV Ratio and Minimal Major Bleeding
Indigo
EXTRACT PE Trial (JACC Cardiovasc Interv, 2021) [MEDLINE]
In this Prospective, Multicenter Study, the Indigo Aspiration System was Associated with a Significant Reduction in the RV/LV Ratio and a Low Major Adverse Event Rate in Submassive Pulmonary Embolism
Intraprocedural Thrombolytic Drugs were Avoided in 98.3% of Patients
Catheter-Directed Thrombolysis
EKOSonic
ULTIMA Randomized Trial of Ultrasound-Assisted Catheter-Directed Thrombolysis in Acute Pulmonary Embolism (Circulation, 2014) [MEDLINE]:
In Intermediate Risk Patients, Catheter-Directed Thrombolysis was Superior to Anticoagulation Alone in Reversing Right Ventricular Dilatation at 24 hrs (With No Increase in Risk of Bleeding Complications)
SEATTLE II Trial (JACC Cardiovasc Interv, 2015) [MEDLINE]
Ultrasound-Facilitated, Catheter-Directed, Low-Dose Fibrinolysis Decreased RV Dilation, Reduced Pulmonary Hypertension, Decreased Anatomic Thrombus Burden, and Minimized Intracranial Hemorrhage in Patients with Acute Massive and Submassive Pulmonary Embolism
Treatment with Using a Ultrasound Catheter-Directed Thrombolysis with Shorter Delivery Duration and Lower-Dose tPA was Associated with Improved Right Ventricular Function and Reduced Clot Burden, as Compared with baseline
Major Bleeding Rate was Low, But One Intracranial Hemorrhage Event Did Occur
Systematic Review and Meta-Analysis Comparing Catheter-Directed Thrombolysis, Systemic Thrombolysis, and Anticoagulation in the Treatment of Intermediate Risk or High Risk Pulmonary Embolism (CMAJ, 2023) [MEDLINE]: n = 20,006 (44 studies)
Compared with Systemic Thrombolysis, Catheter-Directed Thrombolysis was Associated with Decreased Mortality Rate (Odds Ratio 0.43; 95% CI: 0.32-0.57), Intracerebral Hemorrhage (Odds Ratio 0.44; 95% CI 0.29-0.64), Major Bleeding (Odds Ratio 0.61; 95% CI 0.53-0.70), and Blood Transfusion (Odds Ratio 0.46; 95% CI 0.28-0.77)
No Difference in Minor Bleeding was Observed Between the 2 Therapeutic Options (Odds Ratio 1.11; 95% CI 0.66-1.87)
Compared with Anticoagulation, Catheter-Directed Thrombolysis was Associated with Decreased Mortality Rate (Odds Ratio 0.36; 95% CI 0.25-0.52), with No Increased Risk of Intracerebral Hemorrhage (Odds Ratio 1.33; 95% CI 0.63-2.79) or Major Bleeding (Odds Ratio 1.24; 95% CI 0.88-1.75)
Conclusions
With Moderate Certainty of Evidence, the Mortality Rate and Major Bleeding Complications were Lower with Catheter-Directed Thrombolysis than with Systemic Thrombolysis
With Moderate Certainty of Evidence, as Compared to Anticoagulation, Catheter-Directed Thrombolysis was Associated with a Probable Lower Mortality Rate and a Similar Risk of Intracerebral Hemorrhage
These Findings are Largely Based on Observational Data
Recommendations (European Society of Cardiology and European Respiratory Society Guidelines for the Diagnosis and Management of Acute Pulmonary Embolism, 2019) (Eur Heart J, 2020) [MEDLINE]
High-Risk Acute Pulmonary Embolism (Characterized by Hemodynamic Instability)
In Suspected High-Risk Acute Pulmonary Embolism, Intravenous Anticoagulation with Unfractionated Heparin (Including Weight-Adjusted Bolus) is Recommended without Delay (Class I, Level C)
Systemic Thrombolytic Therapy is Recommended (Class I, Level B)
In Patients in Whom Thrombolysis is Contraindicated or Has Failed, Surgical Pulmonary Embolectomy is Recommended (Class I, Level C)
In Patients in Whom Thrombolysis is Contraindicated or Has Failed, Percutaneous Catheter-Directed Treatment Should Be Considered (Class IIa, Level C)
Norepinephrine and/or Dobutamine Should Be Considered (Class IIa, Level C)
In Patients with Refractory Circulatory Collapse or Cardiac Arrest, Venoarterial Extracorporeal Membrane Oxygenation (VA-ECMO) May Be Considered, in Combination with Surgical Embolectomy or Catheter-Directed Treatment (Class IIb, Level C)
In Patients with Hemodynamic Deterioration on Anticoagulation Treatment, Rescue Thrombolytic Therapy (Class I, Level B) or Alternatively, Surgical Embolectomy or Percutaneous Catheter-Directed Treatment (Class IIa, Level C), are Recommended
Recommendations for Systemic Thrombolysis (Consensus Practice from the PERT Consortium, 2019) (Clin Appl Thromb Hemost, 2019) [MEDLINE]
Consider Full-Dose Systemic Thrombolytics in the Following Groups
High-Risk Acute Pulmonary Embolism without Contraindications to Systemic Thrombolytics
Consider Reduced-Dose Systemic Thrombolytics in the Following Groups
High-Risk Acute Pulmonary Embolism with Relative Contraindications to Thrombolysis
Selected Intermediate to High-Risk Acute Pulmonary Embolism with Evidence of or Risk of Clinical Deterioration Based on Vital Signs, Severity of Right Ventricular Dysfunction, Tissue Perfusion, and/or Gas Exchange, and Presence of Low Bleeding Risk
Consider Systemic Thrombolytics in Patients with Cardiac Arrest and Suspected Acute Pulmonary Embolism
Consider Systemic Thrombolytics in Selected Patients with Intermediate or High-Risk Acute Pulmonary Embolism with Thrombus-in-Transit
Recommendations for Catheter-Directed Therapy (Consensus Practice from the PERT Consortium, 2019) (Clin Appl Thromb Hemost, 2019) [MEDLINE]
Consider Catheter-Directed Thrombolysis in the Following Groups
Intermediate to High-Risk Acute Pulmonary Embolism with Risk for Clinical Deterioration Based on Vital Signs, Severity of Right Ventricular Dysfunction, Tissue Perfusion, and/or Gas Exchange, and without Absolute Contraindication to Thrombolysis
High-Risk Acute Pulmonary Embolism with Relative Contraindications to Systemic Thrombolysis<
Consider Catheter Embolectomy in the Following Groups
Intermediate to High-Risk Acute Pulmonary Embolism with Risk for Clinical Deterioration Based on Vital Signs, Severity of Right Ventricular Dysfunction, Tissue Perfusion, and/or Gas Exchange, with Absolute or Relative Contraindications to Thrombolysis
High-Risk Acute Pulmonary Embolism with Absolute Contraindications to Systemic Thrombolysis
After Failed Systemic Thrombolysis or Catheter-Directed Thrombolysis
Thrombus-in-Transit in the Right Atrium or Right Ventricle (AngioVac System)
Recommendations for Surgical Embolectomy (Consensus Practice from the PERT Consortium, 2019) (Clin Appl Thromb Hemost, 2019) [MEDLINE]
High-Risk Acute Pulmonary Embolism with Contraindications to, or Failure of Systemic Thrombolysis or Catheter-Directed Thrombolysis
Intermediate to High Risk Acute Pulmonary Embolism, with Contraindications to, or Failure of Systemic Thrombolysis or Catheter-Directed Thrombolysis, with Risk for Clinical Deterioration Based on Vital Signs, Severity of Right Ventricular Dysfunction, Tissue Perfusion, and/or Gas Exchange
Right Heart Thrombi, Especially with Large Thromboembolic Burden
Thrombus-in-Transit Across a Patent Foramen Ovale (PFO)
Recommendations for Mechanical Hemodynamic Support (Consensus Practice from the PERT Consortium, 2019) (Clin Appl Thromb Hemost, 2019) [MEDLINE]
Consider Mechanical Mechanical Hemodynamic Support in High-Risk Acute Pulmonary Embolism with Cardiac Arrest, Refractory Shock, and/or Contraindications to or Failure of Systemic Thrombolysis
Recommendations (American Society of Hematology Guidelines for the Management of Venous Thromboembolism, 2020) (Blood Adv, 2020) [MEDLINE]
For Patients with Acute Pulmonary Embolism and Hemodynamic Compromise, Use of Thrombolytic Therapy Followed by Anticoagulation is Recommended Over Anticoagulation Alone (Strong Recommendation, Low Certainty in the Evidence
In this Case, the High Mortality of Patients with Acute Pulmonary Embolism and Hemodynamic Compromise, as Well as the Potential Lifesaving Effect of Thrombolytics, Warranted a Strong Recommendation
For Patients with Acute Pulmonary Embolism with Echocardiography and/or Biomarkers Compatible with Right Ventricular Dysfunction But without Hemodynamic Compromise (Submassive Pulmonary Embolism), Anticoagulation Alone is Recommended Over the Routine Use of Thrombolysis in Addition to Anticoagulation (Conditional Recommendation, Low Certainty in the Evidence
Thrombolysis is Reasonable to Consider for Submassive Pulmonary Embolism and Low Risk for Bleeding in Selected Younger Patients or for Patients at High Risk for Decompensation Due to Concomitant Cardiopulmonary Disease
Patients with Submassive Pulmonary Embolism Should Be Monitored Closely for the Development of Hemodynamic Compromise
For Patients with Acute Pulmonary Embolism in Whom Thrombolysis is Considered Appropriate, Use of Systemic Thrombolysis is Recommended Over Catheter-Directed Thrombolysis (Conditional Recommendation, Very Low Certainty in the Evidence)
This Recommendation Reflects Uncertainty About Catheter-Directed Thrombolysis for Acute Pulmonary Embolism Rooted in the Paucity of Randomized Trial Data and Variability in Procedural Experience Across Centers
In Centers with the Appropriate Infrastructure, Clinical Staff, and Procedural Experience, Catheter-Directed Thrombolysis May Be an Alternative to Systemic Thrombolysis, Especially for Patients with an Intermediate to High Risk for Bleeding, Because the Total Dose and Duration of Administration of Thrombolytic Agents are Lower When Delivered by Catheter
In Patients with Acute Pulmonary Embolism Associated with Hypotension (Systolic Blood Pressure <90 mm Hg) Who Do Not Have a High Bleeding Risk, Systemic Thrombolytic Therapy is Recommended (Weak Recommendation, Low-Certainty Evidence)
Studies of Systemically Administered Thrombolytic Therapy Have Utilized Different Agents at Varying Doses
Due to Lack of Comparative Data Between These Approaches, No Agent/Dosing Strategy is Favored Over Another
In Most Patients with Acute Pulmonary Embolism Which is Not Associated with Hypotension, Systemic Thrombolytic Therapy is Not Recommended (Strong Recommendation, Low-Certainty Evidence
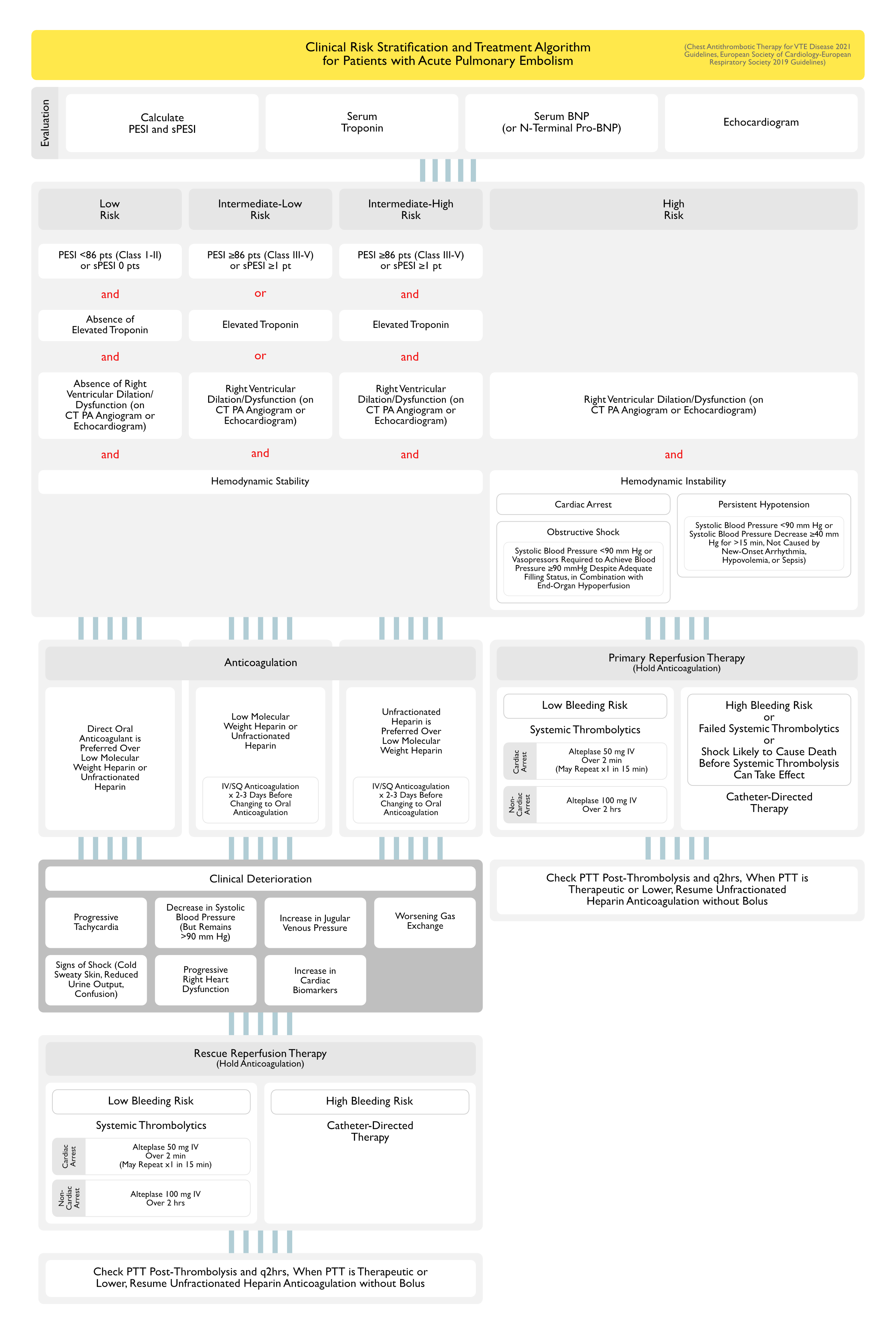
In Selected Patients with Acute Pulmonary Embolism Who Clinically Deteriorate After Starting Anticoagulation But Have Yet to Develop Hypotension and Who Have an Acceptable Bleeding Risk, Systemically Administered Thrombolytic Therapy is Recommended (Weak Recommendation, Low-Certainty Evidence)
Deterioration (Which Has Not Resulted in Hypotension) May Include Any of the Following
Progressive Tachycardia
Decrease in Systolic Blood Pressure (But Remains >90 mm Hg)
Increase in Jugular Venous Pressure
Worsening Gas Exchange
Signs of Shock (Cold Sweaty Skin, Reduced Urine Output, Confusion)
Progressive Right Heart Dysfunction (on Echocardiogram)
Increase in Cardiac Biomarkers
In Patients with Acute Pulmonary Embolism Who are Treated with a Thrombolytic Agent, Systemic Thrombolytic Therapy Using a Peripheral Vein is Recommended Over Catheter-Directed Thrombolysis (Weak Recommendation, Low-Certainty Evidence)
No Randomized Trials or Observational Studies Have Compared Contemporary Catheter-Assisted Thrombus Removal with Systemic Thrombolytic Therapy
In Patients with Acute Pulmonary Embolism Associated with Hypotension Who Also Have High Bleeding Risk, Failed Systemic Thrombolysis, or Shock Which is Likely to Cause Death Before Systemic Thrombolysis Can Take Effect (within Hours), if Appropriate Expertise and Resources are Available, Catheter-Directed Therapy is Suggested (Weak Recommendation, Low-Certainty Evidence)
Treatment of Thrombus in Transit (Clot in Transit)
General Comments
Thrombus in Transit May Be Found in the Inferior Vena Cava, Right Atrium, or Right Ventricle (Circulation, 2019) [MEDLINE]
Thrombus in Transit Accounts for a 5-Fold Increase in Death Resulting from Acute Pulmonary Embolism
Thrombus in Transit is Usually Identified on CT PA Angiogram or Echocardiogram (May Appear as Either Adherent or Free-Floating)
Thrombus in Transit is Present in 4% of Patients with Acute Pulmonary Embolism
Clinical Efficacy
Observational Pooled Analysis of the Treatment of Thrombus in Transit (Vasc Med, 2015) [MEDLINE]: n = 328
Thrombolysis (Odds Ratio 4.8; 95% CI: 1.5–15.4) and Surgical Embolectomy (Odds Ratio 2.6; 95% CI: 0.9–7.6]) were More Often Associated with a Favorable Outcome than Anticoagulation Alone
Study of Treatment of Thrombus in Transit (Am J Med, 2017) [MEDLINE]: n = 255 treated with anticoagulation, n = 70 treated with reperfusion
Comparing Anticoagulation with Reperfusion, There was No Difference in All-Cause Mortality (6.2% vs 14%; P = 0.15) or Pulmonary Embolism-Related Mortality (4.7% vs 7.8%; P = 0.47)
Analysis of Risk Factors for Pulmonary Embolism with Clot in Transit (Thromb Res, 2020) [MEDLINE]: n = 57
Clot in Transit was Present in 8.6% of Patients Who Had an Echocardiogram
Multivariate Analysis Demonstrated Heart Failure (OR 2.8; 95% CI: 1.2-6.5, P = 0.01), a Pre-existing Central Venous Catheter (OR 2.5; 95% CI: 1.1-5.7, P = 0.03), and Hypotension (OR 2.1; 95% CI: 1.1-3.7, P = 0.02) to Be Independently Associated with Clot in Transit
All-Cause Mortality by 7 Days was Higher in Clot in Transit Patients (12.5% vs 5.1%, P = 0.02)
Clot in Transit Patients Who Died were More Likely to Have Presented with Hemodynamic Collapse (57.1% vs 14.0%, P = 0.02), Mental Status Change (100% vs 22.0%, P < 0.001), and to Be Intubated (100% vs 36.0%, P = 0.001)
Review of Considerations in the Setting of Pulmonary Embolism with Clot in Transit (Crit Care Clin, 2020) [MEDLINE]
Clot in Transit is Believed to Be Associated with High Mortality
Case Series of 3 Cases of Catheter-Directed Embolectomy (with Inari FlowTriever) for Right Atrial Clot in Transit (Catheter Cardiovasc Interv, 2021) [MEDLINE]
All of the Patients Had Contraindications to Surgical Thrombo-Embolectomy and Thrombolytic Therapy
Successful Catheter-Based Thrombo-Embolectomy Can Be Perfomed in High-Risk Patients with Right Arial Clot in Transit with or without Acute Pulmonary Embolism
Review of Endovascular Therapies for Clot in Transit (Semin Intervent Radiol, 2022) [MEDLINE]
Review of the Current Endovascular Devices for the Treatment of Right Heart Thrombus and Clot in Transit
Treatment of Asymptomatic Acute Pulmonary Embolism (PE)
Rationale
Asymptomatic Pulmonary Embolism is Diagnosed in About 1% of Outpatients and About 4% of Inpatients Who Have Contrast-Enhanced Chest CT Scans (Chest, 2021) [MEDLINE]
Most Asymptomatic Pulmonary Emboli are Found in Patients with Known Malignancy and are Reported on CT Scans Which Have Been Obtained for Another Indication (Such as Cancer Staging, Surveillance, or Treatment Response Evaluation) (Chest, 2021) [MEDLINE]
About 50% Involve the Lobar or More Central Pulmonary Arteries, While the Remaining 50% Involve More Distal Pulmonary Arteries (Chest, 2021) [MEDLINE]
In Patients Who are Incidentally Found to Have Asymptomatic Pulmonary Embolism, the Standard Initiation and Treatment with Anticoagulation is Recommended, as for Patients with Symptomatic Acute Pulmonary Embolism (Weak Recommendation, Moderate-Certainty Evidence)
Treatment of Acute Subsegmental Pulmonary Embolism (PE)
Rationale/Background
Improvements in Computed Tomography (CT Angiography) Have Led to Increased Diagnosis of Subsegmental Pulmonary Emboli
Subsegmental Pulmonary Emboli Have Increased from Approximately 5% to >10% of All Detected Pulmonary Emboli
Due to Small Size of Subsegmental Pulmonary Emboli, They are More Likely to Be a False-Positive Finding than a Pulmonary Embolism in the Segmental/More Proximal Pulmonary Arteries
Subsgmental Pulmonary Embolism is More Likely to Be a Real Finding if the Following Features are Present
Computed Tomography (CT) Pulmonary Artery Angiogram is of High Quality with Good Opacification of the Distal Pulmonary Arteries
Presence of Multiple Intraluminal Defects
Defects Involve More Proximal (Larger) Subsegmental Arteries
Defects are Seen on >1 Image
Defects are Surrounded by Contrast, Rather than Adherent to Pulmonary Artery Walls
Defects are Seen on >1 Projection
Patient is Symptomatic (as Opposed to Pulmonary Embolism Being an Incidental Finding)
Presence of High Clinical Pretest Probability for Pulmonary Embolism
Elevated Plasma D-Dimer without Another Explanation
Since a True Subsegmental Pulmonary Embolism is Likely to Have Arisen From a Small Deep Venous Thrombosis, the Risk of Progressive or Recurrent Venous Thromboembolism Without Anticoagulation is Expected to Be Lower Than in Patients with a Larger Pulmonary Emboli
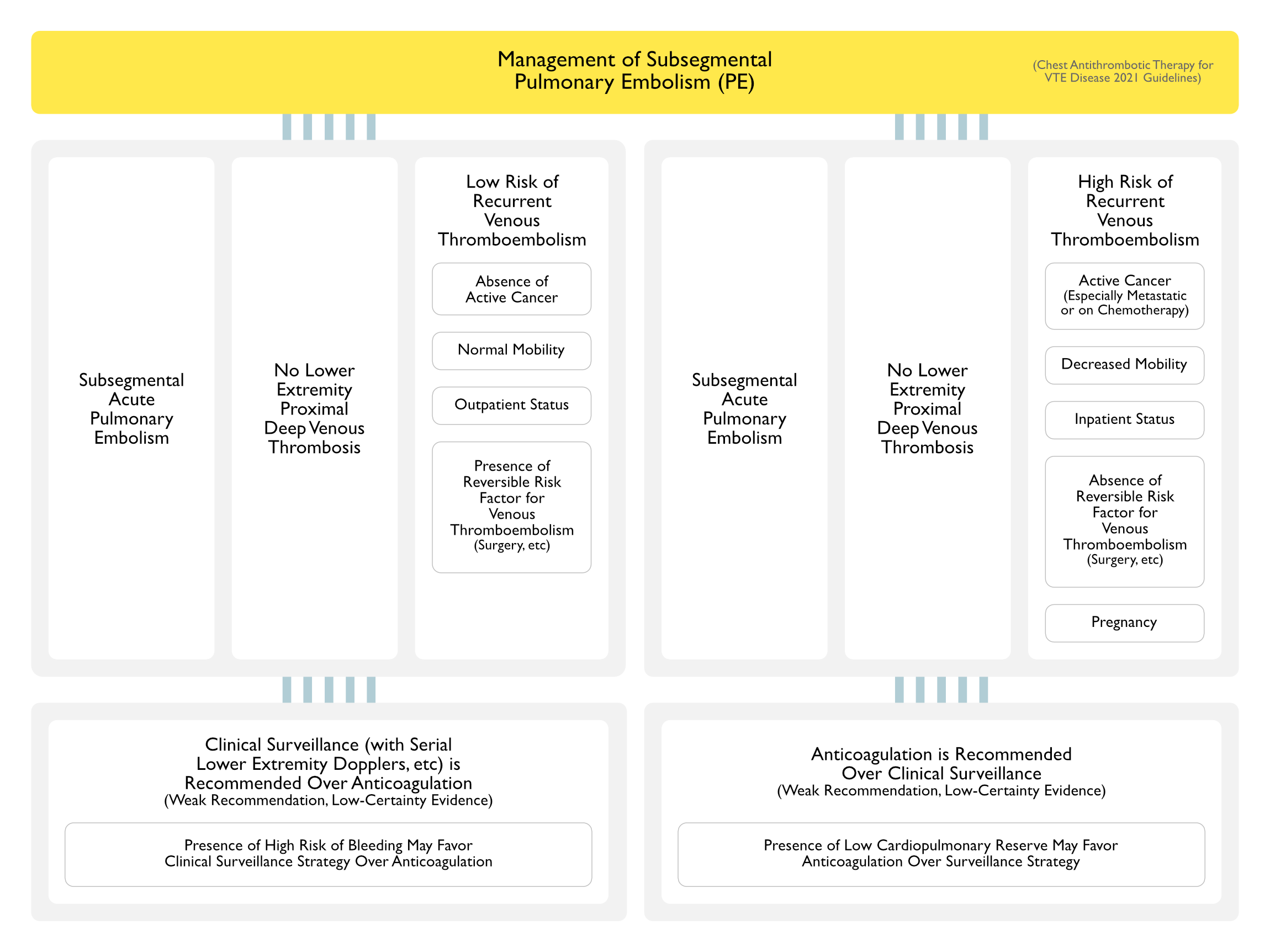
Subsequent Evaluation of Acute Subsegmental Pulmonary Embolism Should Include Lower Extremity Venous Doppler Studies to Classify the Patient According to One of the Following
Subsegmental Acute Pulmonary Embolism + No Lower Extremity Proximal Deep Venous Thrombosis + Low Risk of Recurrent Venous Thromboembolism
Factors Associated with Low Risk of Recurrent Venous Thromboembolism
Absence of Active Cancer
Normal Mobility
Outpatient Status
Presence of Reversible Risk Factor for Venous Thromboembolism (Recent Surgery, etc)
Clinical Surveillance (with Serial Lower Extremity Dopplers, etc) is Recommended Over Anticoagulation (Weak Recommendation, Low-Certainty Evidence)
Presence of High Risk of Bleeding May Favor Clinical Surveillance Strategy Over Anticoagulation
Subsegmental Acute Pulmonary Embolism + No Lower Extremity Proximal Deep Venous Thrombosis + High Risk of Recurrent Venous Thromboembolism
Factors Associated with High Risk of Recurrent Venous Thromboembolism
Active Cancer (Especially if Metastatic or on Chemotherapy)
Decreased Mobility
Hospitalization
Absence of Reversible Risk Factor for Venous Thromboembolism (Recent Surgery, etc)
Anticoagulation is Recommended Over Clinical Surveillance (Weak Recommendation, Low-Certainty Evidence)
Presence of Low Cardiopulmonary Reserve May Favor Anticoagulation Over Surveillance Strategy
References
American College of Chest Physicians Evidence-Based Clinical Practice Guidelines 2012 (9th Edition)
Executive summary: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012 Feb;141(2 Suppl):7S-47S. doi: 10.1378/chest.1412S3 [MEDLINE]
Introduction to the ninth edition: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012 Feb;141(2 Suppl):48S-52S. doi: 10.1378/chest.11-2286 [MEDLINE]
Methodology for the development of antithrombotic therapy and prevention of thrombosis guidelines: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012 Feb;141(2 Suppl):53S-70S. doi: 10.1378/chest.11-2288 [MEDLINE]
Patient values and preferences in decision making for antithrombotic therapy: a systematic review: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012 Feb;141(2 Suppl):e1S-e23S. doi: 10.1378/chest.11-2290 [MEDLINE]
Parenteral anticoagulants: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012 Feb;141(2 Suppl):e24S-e43S. doi: 10.1378/chest.11-2291 [MEDLINE]
Oral anticoagulant therapy: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012 Feb;141(2 Suppl):e44S-e88S. doi: 10.1378/chest.11-2292 [MEDLINE]
Antiplatelet drugs: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012 Feb;141(2 Suppl):e89S-e119S. doi: 10.1378/chest.11-2293 [MEDLINE]
New antithrombotic drugs: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012 Feb;141(2 Suppl):e120S-e151S. doi: 10.1378/chest.11-2294 [MEDLINE] -Evidence-based management of anticoagulant therapy: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012 Feb;141(2 Suppl):e152S-e184S. doi: 10.1378/chest.11-2295 [MEDLINE]
Approach to outcome measurement in the prevention of thrombosis in surgical and medical patients: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012 Feb;141(2 Suppl):e185S-e194S. doi: 10.1378/chest.11-2289 [MEDLINE]
Prevention of VTE in nonsurgical patients: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012 Feb;141(2 Suppl):e195S-e226S. doi: 10.1378/chest.11-2296 [MEDLINE]
Prevention of VTE in nonorthopedic surgical patients: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012 Feb;141(2 Suppl):e227S-e277S. doi: 10.1378/chest.11-2297 [MEDLINE]
Prevention of VTE in orthopedic surgery patients: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012 Feb;141(2 Suppl):e278S-e325S. doi: 10.1378/chest.11-2404 [MEDLINE]
Perioperative management of antithrombotic therapy: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012 Feb;141(2 Suppl):e326S-e350S. doi: 10.1378/chest.11-2298 [MEDLINE]
Diagnosis of DVT: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012 Feb;141(2 Suppl):e351S-e418S. doi: 10.1378/chest.11-2299 [MEDLINE]
Antithrombotic therapy for VTE disease: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012 Feb;141(2 Suppl):e419S-e496S. doi: 10.1378/chest.11-2301 [MEDLINE]
Treatment and prevention of heparin-induced thrombocytopenia: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012 Feb;141(2 Suppl):e495S-e530S. doi: 10.1378/chest.11-2303 [MEDLINE]
Antithrombotic therapy for atrial fibrillation: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012 Feb;141(2 Suppl):e531S-e575S. doi: 10.1378/chest.11-2304 [MEDLINE]
Antithrombotic and thrombolytic therapy for valvular disease: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012 Feb;141(2 Suppl):e576S-e600S. doi: 10.1378/chest.11-2305 [MEDLINE]
Antithrombotic and thrombolytic therapy for ischemic stroke: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012 Feb;141(2 Suppl):e601S-e636S. doi: 10.1378/chest.11-2302 [MEDLINE]
Primary and secondary prevention of cardiovascular disease: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012 Feb;141(2 Suppl):e637S-e668S. doi: 10.1378/chest.11-2306 [MEDLINE]
Antithrombotic therapy in peripheral artery disease: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012 Feb;141(2 Suppl):e669S-e690S. doi: 10.1378/chest.11-2307 [MEDLINE]
VTE, thrombophilia, antithrombotic therapy, and pregnancy: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012 Feb;141(2 Suppl):e691S-e736S. doi: 10.1378/chest.11-2300 [MEDLINE]
Antithrombotic therapy in neonates and children: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012 Feb;141(2 Suppl):e737S-e801S. doi: 10.1378/chest.11-2308 [MEDLINE]
European Society of Cardiology/European Respiratory Society Clinical Practice Guidelines 2014
2014 ESC guidelines on the diagnosis and management of acute pulmonary embolism. Eur Heart J. 2014;35(43):3033-3069, 3069a-3069 k [MEDLINE]
American College of Chest Physicians Evidence-Based Clinical Practice Guidelines 2016
Antithrombotic Therapy for VTE Disease: CHEST Guideline and Expert Panel Report. Chest. 2016 Feb;149(2):315-52. doi: 10.1016/j.chest.2015.11.026. Epub 2016 Jan 7 [MEDLINE]
European Society of Cardiology/European Respiratory Society Clinical Practice Guidelines 2019
2019 ESC Guidelines for the diagnosis and management of acute pulmonary embolism developed in collaboration with the European Respiratory Society (ERS). Eur Heart J. 2020 Jan 21;41(4):543-603. doi: 10.1093/eurheartj/ehz405 [MEDLINE]
PERT Consortium Clinical Practice Guidelines 2019
Diagnosis, Treatment and Follow Up of Acute Pulmonary Embolism: Consensus Practice from the PERT Consortium. Clin Appl Thromb 2019 Jan-Dec;25:1076029619853037. doi: 10.1177/1076029619853037 [MEDLINE]
American Society of Hematology Clinical Practice Guidelines 2020
American Society of Hematology 2020 guidelines for management of venous thromboembolism: treatment of deep vein thrombosis and pulmonary embolism. Blood Adv. 2020 Oct 13;4(19):4693-4738. doi: 10.1182/bloodadvances.2020001830 [MEDLINE]
American College of Chest Physicians Evidence-Based Clinical Practice Guidelines 2021
Antithrombotic Therapy for VTE Disease: Second Update of the CHEST Guideline and Expert Panel Report. Chest. 2021 Dec;160(6):e545-e608. doi: 10.1016/j.chest.2021.07.055 [MEDLINE]
American College of Chest Physicians Evidence-Based Clinical Practice Guidelines 2012-2021
Antithrombotic Therapy for VTE Disease: Compendium and Review of CHEST Guidelines 2012-2021. Chest. 2024 Aug;166(2):388-404. doi: 10.1016/j.chest.2024.03.003 [MEDLINE]
General
Anticoagulant drugs in the treatment of pulmonary embolism. A controlled trial. Lancet. 1960 Jun 18;1(7138):1309-12 [MEDLINE]
Source of non-lethal pulmonary emboli. Lancet. 1974 Feb 16;1(7851):258-9 [MEDLINE]
A prospective study of venous thromboembolism after major trauma. N Engl J Med 1994; 331:1601–1606 [MEDLINE]
A clinical trial of vena caval filters in the prevention of pulmonary embolism in patients with proximal deep-vein thrombosis. Prévention du Risque d’Embolie Pulmonaire par Interruption Cave Study Group. N Engl J Med. 1998;338(7):409 [MEDLINE]
Vena caval filters: a comprehensive review. Blood. 2000;95(12):3669 [MEDLINE]
Predictors of rehospitalization for symptomatic venous thromboembolism after total hip arthroplasty. N Engl J Med. 2000;343(24):1758 [MEDLINE]
Extended-duration prophylaxis against venous thromboembolism after total hip or knee replacement: a meta-analysis of the randomised trials. Lancet. 2001;358(9275):9 [MEDLINE]
Deep vein thrombosis and its prevention in critically ill adults. Arch Intern Med 2001;161:1268–1279 [MEDLINE]
Pulmonary embolism mortality in the United States, 1979-1998: an analysis using multiple-cause mortality data. Arch Intern Med. 2003;163(14):1711 [MEDLINE]
Derivation and validation of a prognostic model for pulmonary embolism. Am J Respir Crit Care Med 2005; 172:1041-1046 [MEDLINE]
Deep venous thrombosis in medical-surgical critically ill patients: prevalence, incidence, and risk factors. Crit Care Med. 2005 Jul;33(7):1565-71 [MEDLINE]
Effectiveness of managing suspected pulmonary embolism using an algorithm combining clinical probability, D-dimer testing, and computed tomography. JAMA. 2006;295(2):172 [MEDLINE]
Clinical Practice: Acute pulmonary embolism. N Engl J Med 2008;359:2804–2813 [MEDLINE]
Prevention of thalidomide- and lenalidomide-associated thrombosis in myeloma. Leukemia. 2008 Feb;22(2):414-23. doi: 10.1038/sj.leu.2405062 [MEDLINE]
Comparative study on risk factors and early outcome of symptomatic distal versus proximal deep vein thrombosis: results from the OPTIMEV study. Thromb Haemost. 2009 Sep;102(3):493-500. doi: 10.1160/TH09-01-0053 [MEDLINE]
RIETE Investigators. Simplification of the pulmonary embolism severity index for prognostication in patients with acute symptomatic pulmonary embolism. Arch Intern Med 2010; 170: 1383–1389 [MEDLINE]
Coagulopathy does not protect against venous thromboembolism in hospitalized patients with chronic liver disease. Chest. 2010;137(5):1145 [MEDLINE]
Gadolinium-enhanced magnetic resonance angiography for pulmonary embolism. A multicenter prospective study (PIOPED III). Ann Intern Med 2010;152:434-443 [MEDLINE]
Reproducibility of CT signs of right ventricular dysfunction in acute pulmonary embolism. AJR Am J Roentgenol 2010; 194:1500-1506 [MEDLINE]
Prognostic factors for pulmonary embolism: the PREP study, a prospective multicenter cohort study. Am J Respir Crit Care Med 2010; 181:168-173 [MEDLINE]
Systematic review: case-fatality rates of recurrent venous thromboembolism and major bleeding events among patients treated for venous thromboembolism. Ann Intern Med. 2010 May 4;152(9):578-89. doi: 10.7326/0003-4819-152-9-201005040-00008 [MEDLINE]
Deep vein thrombosis: a clinical review. J Blood Med. 2011; 2: 59–69 [MEDLINE]
Time trends in pulmonary embolism in the United States: evidence of overdiagnosis. Arch Intern Med. 2011;171(9):831 [MEDLINE]
Influence of preceding length of anticoagulant treatment and initial presentation of venous thromboembolism on risk of recurrence after stopping treatment: analysis of individual participants’ data from seven trials. BMJ. 2011 May 24;342:d3036. doi: 10.1136/bmj.d3036 [MEDLINE]
Obesity and pulmonary embolism: the mounting evidence of risk and the mortality paradox. Thromb Res. 2011;128:518–523 [MEDLINE]
Impact of vena cava filters on in-hospital case fatality rate from pulmonary embolism. Am J Med. 2012 May;125(5):478-84. Epub 2012 Feb 4 [MEDLINE]
Factors in the technical quality of gadolinium enhanced magnetic resonance angiography for pulmonary embolism in PIOPED III. Int J Cardiovasc Imaging. 2012 Feb;28(2):303-12. doi: 10.1007/s10554-011-9820-7. Epub 2011 Feb 24 [MEDLINE]
A meta-analysis of anticoagulation for calf deep venous thrombosis. J Vasc Surg. 2012 Jul;56(1):228-37.e1; discussion 236-7. doi: 10.1016/j.jvs.2011.09.087. Epub 2011 Dec 29 [MEDLINE]
Use of Glucocorticoids and Risk of Venous Thromboembolism: A Nationwide Population-Based Case-Control Study. JAMA Intern Med. 2013 Apr 1:1-1 [MEDLINE]
Acute pulmonary embolism: external validation of an integrated risk stratification model. Chest 2013 Jun 13. doi: 10.1378/chest.12-2938 [MEDLINE]
Identification of intermediate-risk patients with acute symptomatic pulmonary embolism. Eur Respir J. 2014 Sep;44(3):694-703. doi: 10.1183/09031936.00006114. Epub 2014 Apr 2 [MEDLINE]
Vena cava filters in unstable elderly patients with acute pulmonary embolism. Am J Med. 2014 Mar;127(3):222-5 [MEDLINE]
2014 ESC guidelines on the diagnosis and management of acute pulmonary embolism. Eur Heart J. 2014;35(43):3033-3069, 3069a-3069 k [MEDLINE]
Non-steroidal anti-inflammatory drugs and risk of venous thromboembolism: a systematic review and meta-analysis. Rheumatology (Oxford). 2015 Apr;54(4):736-42. doi: 10.1093/rheumatology/keu408. Epub 2014 Sep 24 [MEDLINE]
Diagnostic prediction models for suspected pulmonary embolism: systematic review and independent external validation in primary care. BMJ. 2015;351:h4438 [MEDLINE]
Free-floating thrombus and embolic risk in patients with angiographically confirmed proximal deep venous thrombosis. A prospective study. Arch Intern Med. 1997 Feb 10;157(3):305-8 [MEDLINE]
Low-molecular-weight heparin versus a coumarin for the prevention of recurrent venous thromboembolism in patients with cancer. N Engl J Med. 2003 Jul 10;349(2):146-53 [MEDLINE]
Low-molecular-weight heparin compared with intravenous unfractionated heparin for treatment of pulmonary embolism: a meta-analysis of randomized, controlled trials. Ann Intern Med. 2004 Feb 3;140(3):175-83 [MEDLINE]
Enoxaparin in the treatment of deep vein thrombosis with or without pulmonary embolism: an individual patient data meta-analysis. Chest. 2005 Oct;128(4):2203-10 [MEDLINE]
Treatment of deep vein thrombosis: what factors determine appropriate treatment? Can Fam Physician. 2005;51:217 [MEDLINE]
Management of venous thromboembolism in patients with advanced cancer: a systematic review and meta-analysis. Lancet Oncol. 2008 Jun;9(6):577-84. doi: 10.1016/S1470-2045(08)70149-9 [MEDLINE]
Clinical Practice: Acute pulmonary embolism. N Engl J Med 2008;359:2804–2813 [MEDLINE]
Fondaparinux and the management of heparin-induced thrombocytopenia: the journey continues. Ann Pharmacother 2009;43:1636–1646 [MEDLINE]
Unfractionated heparin dosing for venous thromboembolism in morbidly obese patients: case report and review of the literature. Pharmacotherapy. 2010 Mar;30(3):324. doi: 10.1592/phco.30.3.324 [MEDLINE]
Early anticoagulation is associated with reduced mortality for acute pulmonary embolism. Chest. 2010 Jun;137(6):1382-90. doi: 10.1378/chest.09-0959 [MEDLINE]
EINSTEIN Trial. Oral rivaroxaban for symptomatic venous thromboembolism. N Engl J Med. 2010;363(26):2499 [MEDLINE]
AMPLIFY Trial. Oral apixaban for the treatment of acute venous thromboembolism. N Engl J Med. 2013;369(9):799 [MEDLINE]
Use of Glucocorticoids and Risk of Venous Thromboembolism: A Nationwide Population-Based Case-Control Study. JAMA Intern Med. 2013 Apr 1:1-1 [MEDLINE]
Cost-effectiveness of rivaroxaban compared with enoxaparin plus a vitamin K antagonist for the treatment of venous thromboembolism. J Med Econ. 2014 Jan;17(1):52-64. doi: 10.3111/13696998.2013.858634. Epub 2013 Nov 14 [MEDLINE]
Fibrinolysis for patients with intermediate risk pulmonary embolism. N Engl J Med 2014;370:1402–1411 [MEDLINE]
Clinical and safety outcomes associated with treatment of acute venous thromboembolism: a systematic review and meta-analysis. JAMA. 2014 Sep 17;312(11):1122-35. doi: 10.1001/jama.2014.10538 [MEDLINE]
Unfractionated heparin dosing for therapeutic anticoagulation in critically ill obese adults. J Crit Care 2015;30:395–399 [MEDLINE]
Comparison of differences in medical costs when new oral anticoagulants are used for the treatment of patients with non-valvular atrial fibrillation and venous thromboembolism vs warfarin or placebo in the US. J Med Econ. 2015 Jun;18(6):399-409. doi: 10.3111/13696998.2015.1007210. Epub 2015 Feb 9 [MEDLINE]
Cost-effectiveness analysis of treatment of venous thromboembolism with rivaroxaban compared with combined low molecular weight heparin/vitamin K antagonist. Thromb J. 2015 Jun 11;13:20. doi: 10.1186/s12959-015-0051-3. eCollection 2015 [MEDLINE]
Major Bleeding and Hemorrhagic Stroke with Direct Oral Anticoagulants in Patients with Renal Failure: Systematic Review and Meta-Analysis of Randomized Trials. Chest. 2016,(): doi:10.1016/j.chest.2015.12.029 [MEDLINE]
How I treat recurrent venous thromboembolism in patients receiving anticoagulant therapy. Blood. 2017 Jun 22;129(25):3285-3293. doi: 10.1182/blood-2017-03-742304 [MEDLINE]
Massive Fatal Pulmonary Embolism While on Therapeutic Heparin Drip. J Investig Med High Impact Case Rep. Jan-Dec 2020;8:2324709620914787. doi: 10.1177/2324709620914787 [MEDLINE]
2019 ESC Guidelines for the diagnosis and management of acute pulmonary embolism developed in collaboration with the European Respiratory Society (ERS). Eur Heart J. 2020 Jan 21;41(4):543-603. doi: 10.1093/eurheartj/ehz405 [MEDLINE]
Anticoagulation for Venous Thromboembolism: Impact on the Risk of Major Adverse Cardiovascular Events. Chest. 2022 Jun 14;S0012-3692(22)01087-X. doi: 10.1016/j.chest.2022.05.038 [MEDLINE]
Direct Oral Anticoagulants vs Low-Molecular-Weight Heparin and Recurrent VTE in Patients With Cancer: A Randomized Clinical Trial. JAMA. 2023 Jun 13;329(22):1924-1933. doi: 10.1001/jama.2023.7843 [MEDLINE]
Embolectomy/Catheter-Directed Therapy
Pulmonary embolectomy: a 20-year experience at one center. Ann Thorac Surg 1991; 51:232-236
Medical compared with surgical treatment for massive pulmonary embolism. Lancet 1994; 343:565-577
ULTIMA Trial. Randomized, controlled trial of ultrasound-assisted catheter-directed thrombolysis for acute intermediate-risk pulmonary embolism. Circulation 2014;129:479-86 [MEDLINE]
Comparative outcomes of catheter-directed thrombolysis plus anticoagulation vs anticoagulation alone to treat lower-extremity proximal deep vein thrombosis. JAMA Intern Med. 2014;174(9):1494-1501 [MEDLINE]
Randomized, controlled trial of ultrasound-assisted catheter-directed thrombolysis for acute intermediate-risk pulmonary embolism. Circulation 2014;129:479–486 [MEDLINE]
Pulmonary Embolism Response to Fragmentation, Embolectomy, and Catheter Thrombolysis (PERFECT): Initial Results From a Prospective Multicenter Registry. Chest. 2015 Sep;148(3):667-673. doi: 10.1378/chest.15-0119 [MEDLINE]
A Prospective, Single-Arm, Multicenter Trial of Ultrasound-Facilitated, Catheter-Directed, Low-Dose Fibrinolysis for Acute Massive and Submassive Pulmonary Embolism: The SEATTLE II Study. JACC Cardiovasc Interv 2015;8:1382-92 [MEDLINE]
A Prospective, Single-Arm, Multicenter Trial of Catheter-Directed Mechanical Thrombectomy for Intermediate-Risk Acute Pulmonary Embolism: The FLARE Study. JACC Cardiovasc Interv. 2019 May 13;12(9):859-869. doi: 10.1016/j.jcin.2018.12.022 [MEDLINE]
Interventional Therapies for Acute Pulmonary Embolism: Current Status and Principles for the Development of Novel Evidence: A Scientific Statement From the American Heart Association. Circulation. 2019 Nov 12;140(20):e774-e801. doi: 10.1161/CIR.0000000000000707 [MEDLINE]
Percutaneous Thrombectomy in Emergency Department Patients with Pulmonary Embolism: The FLARE ED Sub-study. J Emerg Med. 2020 Feb;58(2):175-182. doi: 10.1016/j.jemermed.2019.11.044 [MEDLINE]
Indigo Aspiration System for Treatment of Pulmonary Embolism: Results of the EXTRACT-PE Trial. JACC Cardiovasc Interv. 2021 Feb 8;14(3):319-329. doi: 10.1016/j.jcin.2020.09.053 [MEDLINE]
Catheter-directed thrombolysis compared with systemic thrombolysis and anticoagulation in patients with intermediate- or high-risk pulmonary embolism: systematic review and network meta-analysis. CMAJ. 2023 Jun 19;195(24):E833-E843. doi: 10.1503/cmaj.220960 [MEDLINE]
Thrombolytics
Urokinase pulmonary embolism trial. A national cooperative study. Circulation 1973; 47,48 (suppl 2):1-108
Alteplase versus heparin in acute pulmonary embolism: randomized trial assessing right-ventricular function and pulmonary perfusion. Lancet 1993; 34:507-511
Thrombolytic therapy for pulmonary embolism. Cochrane Database System Rev. 2009;(3): CD004437 [MEDLINE]
Thrombolysis for pulmonary embolism and risk of all-cause mortality, major bleeding, and intracranial hemorrhage: a meta-analysis. JAMA. 2014 Jun 18;311(23):2414-21. doi: 10.1001/jama.2014.5990 [MEDLINE]
PEITHO Trial: Fibrinolysis for patients with intermediate-risk pulmonary embolism. N Engl J Med. 2014 Apr 10;370(15):1402-11. doi: 10.1056/NEJMoa1302097 [MEDLINE]
Systematic review and meta-analysis for thrombolysis treatment in patients with acute submassive pulmonary embolism. Patient Prefer Adherence. 2014;8:275-282 [MEDLINE]
Systemic thrombolytic therapy for acute pulmonary embolism: a systematic review and meta-analysis. Eur Heart J. 2015 Mar 7;36(10):605-14. doi: 10.1093/eurheartj/ehu218 [MEDLINE]
Antithrombotic Therapy for VTE Disease: CHEST Guideline and Expert Panel Report. Chest. 2016 Feb;149(2):315-52. doi: 10.1016/j.chest.2015.11.026. Epub 2016 Jan 7 [MEDLINE]
A Randomized Trial of the Optimum Duration of Acoustic Pulse Thrombolysis Procedure in Acute Intermediate-Risk Pulmonary Embolism: the OPTALYSE PE trial. JACC Cardiovasc Interv. 2018;11:1401–1410. doi: 10.1016/j.jcin.2018.04.008 [MEDLINE]
Venoarterial Extracorporeal Membrane Oxygenation in Massive Pulmonary Embolism-Related Cardiac Arrest: A Systematic Review. Crit Care Med. 2021 May 1;49(5):760-769. doi: 10.1097/CCM.0000000000004828 [MEDLINE]
Thrombus in Transit
Comparative efficacy of different modalities for treatment of right heart thrombi in transit: a pooled analysis. Vasc Med. 2015 Apr;20(2):131-8. doi: 10.1177/1358863X15569009 [MEDLINE]
Treatment of right heart thrombi associated with acute pulmonary embolism. Am J Med. 2017;130:588–595. doi: 10.1016/j.amjmed.2016.11.027 [MEDLINE]
Pulmonary embolism with clot in transit: An analysis of risk factors and outcomes. Thromb Res. 2020 Mar;187:139-147. doi: 10.1016/j.thromres.2020.01.006 [MEDLINE]
Special Considerations in Pulmonary Embolism: Clot-in-Transit and Incidental Pulmonary Embolism. Crit Care Clin. 2020 Jul;36(3):531-546. doi: 10.1016/j.ccc.2020.02.008 [MEDLINE]
Catheter directed embolectomy of right atrial clot in transit-A case series. Catheter Cardiovasc Interv. 2021 Apr 1;97(5):869-873. doi: 10.1002/ccd.29391 [MEDLINE]
Right Heart Clot-in-Transit: Endovascular Therapies. Semin Intervent Radiol. 2022 Dec 20;39(5):515-522. doi: 10.1055/s-0042-1757942. eCollection 2022 Oct [MEDLINE]