D-Dimer is the Degradation Product of Cross-Linked Fibrin
D-Dimer is Easy to Obtain
However, D-Dimer May Be Elevated in Conditions Other Than Venous Thromboembolism
“Sensitive” D-Dimer Assays: quantitative or semiquantitative newer generation assays
Rapid Enzyme-Linked Immunosorbent Assay (ELISA)
Immunoturbidimetric Assay
Latex Agglutination Assay
Interpretation
Normal D-Dimer Level: <500 ng/mL (<0.5 μg/mL or <500 μg/L) Fibrinogen Equivalent (FE) Units
Age-Adjusted D-Dimer Thresholds Have Also Been Suggested to Decrease Unnecessary Imaging, But Have Not Widely Adopted in Clinical Practice (Ann Intern Med, 2016) [MEDLINE]
Clinical Efficacy
ANTELOPE Study (Am J Respir Crit Care Med, 2002) [MEDLINE]
The Sensitivity of D-Dimer was Lower in Subsegmental Pulmonary Embolism (53%), as Compared to Large Main, Lobar, and Segmental Pulmonary Embolism (93%)
Systematic Review of D-Dimer in the Diagnosis of Venous Thromboembolism (Ann Intern Med, 2004) [MEDLINE]
For the Diagnosis of Deep Venous Thrombosis (DVT)
Enzyme-linked Immunosorbent Assay (ELISA) D-Dimer Assay Had a 96% Sensitivity (95% CI: 0.91-1.00) and Negative Likelihood Ratio of 12% (95% CI: 0.04-0.33)
Quantitative Rapid Enzyme-linked Immunosorbent Assay (ELISA) D-Dimer Assay Had a 96% Sensitivity (95% CI: 0.90-1.00) and Negative Likelihood Ratio of 9% (95% CI: 0.02-0.41)
For the Diagnosis of Pulmonary Embolism (PE)
Enzyme-linked Immunosorbent Assay (ELISA) D-Dimer Assay Had a 95% Sensitivity (95% CI: 0.85-1.00) and Negative Likelihood Ratio of 13% (95% CI: 0.03-0.58)
Quantitative Rapid Enzyme-linked Immunosorbent Assay (ELISA) D-Dimer Assay Had a 95% Sensitivity (95% CI: 0.83-1.00), and Negative Likelihood Ratio of 13% (95% CI: 0.02-0.84)
Emergency Department Study of the Use of Age-Adjusted D-Dimer Thresholds (Chest, 2014) [MEDLINE]
Use of Age-Adjusted D-Dimer Threshold Decreased Imaging Among Patients >50 y/o with a Revised Geneva Score ≤10
Although the Adoption of an Age-Adjusted D-Dimer Threshold is Probably Safe, the Confidence Intervals Surrounding the Additional 1.5% of Pulmonary Emboli Missed Necessitate Prospective Study Before this Practice Can Be Adopted into Routine Clinical Practice
European ADJUST-PE Study of Age-Adjusted D-Dimer Levels in the Diagnosis of Pulmonary Embolism (JAMA, 2014) [MEDLINE]
Age-Adjusted D-Dimer (Only for Patients ≥50 y/o): defined as 10 x age
Compared with a Fixed D-Dimer Cutoff of 500 μg/L (500 ng/mL), the Combination of a Pre-Test Clinical Probability Assessment and Age-Adjusted D-Dimer Cutoff was Associated with a Larger Number of Patients in Whom Pulmonary Embolism Could Be Considered Ruled Out with a Low Likelihood of Subsequent Clinical Venous Thromboembolism
Retrospective Study of the Use of Age-Adjusted D-Dimer Thresholds in the Emergency Department (Ann Emerg Med, 2016) [MEDLINE]
An Age-Adjusted D-Dimer Limit Has the Potential to Reduce Chest Imaging Among Older Emergency Department Patients and is More Accurate than a Standard Threshold of 500 ng/dL
Systematic Review of D-Dimer in the Diagnosis of Pulmonary Embolism (Cochrane Database Syst Rev, 2016) [MEDLINE]: n = 1585 (total of 4 studies)
Sensitivity: 80-100%
Specificity: 23-63%
High Levels of False-Positive Results were Observed, Especially Among Patients >65 y/o
A Negative D-Dimer is Valuable in Ruling Out Pulmonary Embolism in Patients Who Present to the Ambulatory/Emergency Setting with a Low Pre-Test Probability for Pulmonary Embolism
Evidence from One Study Suggests that D-Dimer May Have Less Utility in Older Patient Populations, But No Empirical Evidence was Available to Support an Increase in the Diagnostic Threshold of Interpretation of D-Dimer Results for those >65 y/o
Systematic Review and Meta-Analysis of Wells Criteria and D-Dimer Testing in the Diagnosis of Pulmonary Embolism (Ann Intern Med, 2016) [MEDLINE]
In Patients with an “Unlikely” Pre-Test Probability of Pulmonary Embolism, Age-Adjusted D-Dimer Testing is Associated with a 5% Increase in the Proportion of Patients with Suspected Pulmonary Embolism in Whom Imaging Can Be Safely Withheld, as Compared to Fixed D-Dimer Testing
Systematic Review and Meta-Analysis of 6 Prospective Studies of Age-Adjusted D-Dimer Thresholds (Ann Intern Med, 2016) [MEDLINE]
Age-Adjusted D-Dimer Testing is Associated with a 5% Absolute Increase in the Proportion of Patients with Suspected Pulmonary Embolism in Whom Imaging Can Be Safely Withheld Compared with Fixed D-Dimer Testing
This Strategy Seems Safe Across Different High-Risk Subgroups, But its Efficiency Varies
If the Pre-D-Dimer Probability of PE is 15% (Intermediate Pre-Test Probability), Only a D-DImer <500 ng/mL Will Result in a Post-Test Probability <3%
Consequently, Given a Pre-Test Probability of 15% (Intermediate Pre-Test Probability) and a CT Pulmonary Artery Angiogram Threshold of 3%, a Strategy to Obtain CT Pulmonary Artery Angiogram for D-Dimer ≥500 ng/ mL is Consistent with the Interval Likelihood Ratios Reported
Study of Age-Adjusted D-Dimer Threshold to YEARS Algorithm in the Diagnosis of Pulmonary Embolism ( J Thromb Haemost, 2017) [MEDLINE]
There was No Added Value of Age-Adjusted D-Dimer Cut-Off to the YEARS Algorithm in Patients with Suspected Pulmonary Embolism
Prospective PEGeD Trial of Probability-Adjusted D-Dimer (NEJM, 2019) [MEDLINE]: n = 2017
Acute Pulmonary Embolism was Considered Ruled Out Without Further Testing in Outpatients with a Low Clinical Pretest Probability and a D-Dimer <1000 ng/mL or with a Moderate Clinical Pretest Probability and a D-Dimer <500 ng/mL
Overall, 7.4% of Patients Had Acute Pulmonary Embolism on Initial Diagnostic Testing
A Combination of a Low Clinical Pretest Probability and D-Dimer <1000 ng/mL Identified a Group of Patients at Low Risk for Pulmonary Embolism During Follow-Up
Recommendations (American Thoracic Society/Society of Thoracic Radiology Clinical Practice Guidelines for the Evaluation of Suspected Pulmonary Embolism in Pregnancy) (Am J Respir Crit Care Med, 2011) [MEDLINE]
In Pregnant Women with Suspected Acute Pulmonary Embolism, D-Dimer Should Not Be Used to Exclude Acute Pulmonary Embolism (Weak Recommendation; Very Low Quality Evidence)
Recommendations (European Society of Cardiology and European Respiratory Society Guidelines for the Diagnosis and Management of Acute Pulmonary Embolism, 2019) (Eur Heart J, 2020) [MEDLINE]
Plasma D-Dimer Measurement (Preferably Using a High Sensitivity Assay, is Recommended in Outpatients/Emergency Department Patients with Low-Intermediate Clinical Probability, or Those that are Acute Pulmonary Embolism-Unlikely, to Decrease the Need for Unnecessary Imaging and Irradiation (Class of Recommendation I; Level of Evidence: A)
As an Alternative to the Fixed D-Dimer Cutoff, a Negative D-Dimer Test Using an Age-Adjusted Cutoff (Age x 10 mg/L, in Patients >50 y/o) Should Be Considered for Excluding Acute Pulmonary Embolism in Patients with Low-Intermediate Clinical Probability, or Those Who are Acute Pulmonary Embolism-Unlikely (Class of Recommendation: IIa, Level of Evidence: B)
As an Alternative to the Fixed or Age-Adjusted D-Dimer Cutoff, D-Dimer Levels Adapted to Clinical Probability Should Be Considered to Exclude Acute Pulmonary Embolism (Class of Recommendation: IIa, Level of Evidence: B)
D-Dimer Measurement is Not Recommended in Patients with High Clinical Probability, as a Normal Result Does Not Safely Exclude Acute Pulmonary Embolism, Even When Using a High Sensitivity Assay (Class of Recommendation: III, Level of Evidence: A)
Recommendations (2026 AHA/ACC/ACCP/ACEP/CHEST/SCAI/SHM/SIR/SVM/SVN Guideline for the Evaluation and Management of Acute Pulmonary Embolism in Adults: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines) (Circulation, 2026) [MEDLINE]
In Patients Presenting with Symptoms Suggestive of Acute Pulmonary Embolism (PE), a Targeted History and Comprehensive Physical Examination is Recommended to Assist in Determining the Clinical Pretest Probability of Acute Pulmonary Embolism (PE) (Class of Recommendation: 1; Level of Evidence: A)
In Adult Patients Undergoing Evaluation for Pulmonary Embolism (PE) and Who Have a Low/Intermediate Clinical Probability of Pulmonary Embolism (PE) (<50%) by Risk Assessment, an Age-Adjusted D-Dimer Value Below the Threshold (Age × 10 μg/L for Fibrinogen Equivalent Units Assays) Effectively Excludes Pulmonary Embolism (PE) and the Need for Imaging (Class of Recommendation: 2a; Level of Evidence: B-R)
In Adult Patients with Suspected Pulmonary Embolism (PE), the YEARS Algorithm Can Be Useful to Identify Which Patients Do Not Need Imaging to Rule Out Pulmonary Embolism (PE) (Class of Recommendation: 2a; Level of Evidence: B-R)
YEARS Algorithm
In Patients Who Have ≥1 of the Following YEARS Criteria, Use a D-Dimer Threshold of 500 μg/L
Acute Pulmonary Embolism (PE) as the Most Likely Diagnosis
Clinical Signs of Deep Venous Thrombosis (DVT)
Hemoptysis
In Patients Who Have for Have No YEARS Criteria, Use a D-Dimer Threshold of 1000 μg/L
In Pregnant Adults, it May Be Reasonable to Use Pregnancy-Adapted YEARS Criteria to Identify Patients Who Do Not Need Imaging for Pulmonary Embolism (PE) (Class of Recommendation: 2b; Level of Evidence: B-R) (NEJM, 2019) [MEDLINE]
In Patients Presenting with Symptoms/Signs Suggestive of Acute Pulmonary Embolism (PE), Imaging is Recommended for Those Who are Deemed High Probability (>50% Probability of Pulmonary Embolism) by a Validated Clinical Risk Prediction Score or an Elevated D-Dimer Level in Order to Confirm/Exclude Pulmonary Embolism (PE) (Class of Recommendation: 1; Level of Evidence: A)
Allows for Evaluation of Superficial and Deep Venous Systems
Easily Repeated
Non-Invasive
Accuracy
Sensitivity: xxx
Specificity: xxx
Clinical Efficacy-Occlusiveness of Deep Venous Thrombosis
Study of Occlusiveness of Lower Extremity DVT in Patients After Hip Surgery (Thromb Haemost, 1996) [MEDLINE]
Most DVT’s Diagnosed in Asymptomatic Patients After Hip Surgery (59.1%-67.1%, Depending on the Vessel) are Non-Occlusive: for this reason, diagnostic methods based on venous flow measurements would be expected to be less sensitive
Clinical Efficacy-Other
Trial of Clinical Pretest Probability Scoring Combined with Lower Extremity Venous Ultrasound in the Diagnosis of Outpatient DVT (Lancet, 1997) [MEDLINE]
Using Pretest Probability Scoring with Lower Extremity Venous Ultrasound was Safe and Feasible
Prospective Study of Lower Extremity Venous Ultrasound in the Diagnosis of DVT (Ann Intern Med, 2004) [MEDLINE]
It is Safe to Withhold Anticoagulation After Negative Lower Extremity Doppler Studies in Nonpregnant Patients with a First Suspected Episode of Symptomatic Lower Extremity DVT
Systematic Review and Meta-Analysis of Risk Stratification of Patients with Acute PE Based on Presence/Absence of Lower Extremity DVT (Chest, 2016) [MEDLINE]
In Patients Diagnosed with Acute Symptomatic PE, Concomitant DVT was Significantly Associated with an Increased Risk of Death within 30 days of the PE Diagnosis, as Compared to Those without a Concomitant Lower Extremity DVT (6.2% vs 3.8%)
Recommendations (American Thoracic Society/Society of Thoracic Radiology Clinical Practice Guidelines for the Evaluation of Suspected Pulmonary Embolism in Pregnancy) (Am J Respir Crit Care Med, 2011) [MEDLINE]
In Pregnant Women with Suspected Acute Pulmonary Embolism and Symptoms/Signs of Deep Venous Thrombosis, Bilateral Venous Compression Ultrasound of Lower Extremities is Recommended (Weak Recommendation, Very Low Quality Evidence)
If Positive, Anticoagulation Treatment is Recommended (Weak Recommendation, Very Low Quality Evidence)
If Negative, Further Testing is Recommended (Weak Recommendation, Very Low Quality Evidence)
In Pregnant Women with Suspected Acute Pulmonary Embolism and No Symptoms/Signs of Deep Venous Thrombosis, Studies of the Pulmonary Vasculature are Recommended Rather than Venous Compression Ultrasound of the Lower Extremities (Weak Recommendation, Very Low Quality Evidence)
Recommendations (European Society of Cardiology and European Respiratory Society Guidelines for the Diagnosis and Management of Acute Pulmonary Embolism, 2019) (Eur Heart J, 2020) [MEDLINE]
If a Compression Ultrasound Study Demonstrates a Proximal Deep Venous Thrombosis in a Patient with Clinical Suspicion of Acute Pulmonary Embolism, it is Recommended to Accept the Diagnosis of Venous Thromboembolism (and Acute Pulmonary Embolism) (Class I, Level A)
If Compression Ultrasound Study Demonstrates Only Distal Deep Venous Thrombosis, Further Testing Should Be Considered to Confirm Acute Pulmonary Embolism (Class IIa, Level B)
If a Positive Proximal Compression Ultrasound Study is Used to Confirm Acute Pulmonary Embolism, Assessment of Acute Pulmonary Embolism Severity Should Be Considered to Permit Risk-Adjusted Management (Class IIa, Level C)
Recommendations (2026 AHA/ACC/ACCP/ACEP/CHEST/SCAI/SHM/SIR/SVM/SVN Guideline for the Evaluation and Management of Acute Pulmonary Embolism in Adults: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines) (Circulation, 2026) [MEDLINE]
In Patients with Confirmed Acute Pulmonary Embolism (PE), Obtaining Lower Extremity Venous Duplex Ultrasound Examination May Be Reasonable in Patients with Clinical Findings Suggestive of Deep Venous Thrombosis (DVT) or if the Presence of Deep Venous Thrombosis (DVT) Will Change Management or Inform Prognosis (Class of Recommendation: 2b; Level of Evidence: B-NR)
In Patients with Suspected Acute Pulmonary Embolism (PE) and a Negative Computed Tomography (CT) Pulmonary Artery Angiogram or Normal V/Q SPECT, Venous Duplex Ultrasonography is Not Useful for Further Pulmonary Embolism (PE) Diagnostic Evaluation (Class of Recommendation: 3 = No Benefit; Level of Evidence: B-NR)
Recommendations (Chest Antithrombotic Therapy and Prevention of Thrombosis 2012 Guidelines) [MEDLINE]
CT Venogram is an Alternative to Compression Lower Extremity Venous Doppler Ultrasound for the Diagnosis of Lower Extremity Deep Venous Thrombosis When Ultrasound is Impractical (Patients with Lower Extremity Casting, Significant Lower Extremity Edema or Wounds, etc)
Recommendations (European Society of Cardiology and European Respiratory Society Guidelines for the Diagnosis and Management of Acute Pulmonary Embolism, 2019) (Eur Heart J, 2020) [MEDLINE]
Computed Tomography (CT) Venography is Not Recommended as an Adjunct to Computed Tomography (CT) Pulmonary Artery Angiogram for the Diagnosis of Acute Pulmonary Embolism (PE) (Class III, Level B)
Recommendations (2026 AHA/ACC/ACCP/ACEP/CHEST/SCAI/SHM/SIR/SVM/SVN Guideline for the Evaluation and Management of Acute Pulmonary Embolism in Adults: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines) (Circulation, 2026) [MEDLINE]
In Patients with Suspected Acute Pulmonary Embolism (PE), Computed Tomographic Venography of the Inferior Vena Cava (IVC) and Lower Extremity Veins is Not Recommended as a Routine Adjunct to Computed Tomography (CT) Pulmonary Artery Angiogram to Diagnose Venous Thrombosis (Class of Recommendation: 3 = No Benefit; Level of Evidence: B-NR)
Recommendations for Diagnostic Testing Suspected Upper Extremity Deep Venous Thrombosis (Chest Antithrombotic Therapy and Prevention of Thrombosis 2012 Guidelines) [MEDLINE]
If Upper Extremity Compression Venous Doppler Ultrasound is Negative with High Clinical Suspicion, Moderate/High-Sensitivity D-Dimer, Serial Ultrasound, CT Upper Extremity Venogram, or Gadolinium-Enhanced Magnetic Resonance Upper Extremity Magnetic Resonance Imaging (MRI) Venogram is Recommended (Grade 2C Recommendation)
Gadolinium-Enhanced Magnetic Resonance Venogram and Pulmonary Artery Angiogram (MRA) (see Magnetic Resonance Imaging)
Advantages
No Exposure to Iodinated Radiographic Contrast
No Radiation Exposure
Disadvantages
Magnetic Resonance Venogram and Pulmonary Artery Angiogram Have High Rates of Technically Inadequate Studies [MEDLINE]: technically inadequate studies were found in 25% (range: 11-52%) of studies performed in the PIOPED III Study (2010), depending on the center
Due to the large number of technically inadequate studies in PIOPED III, magnetic resonance venography and pulmonary angiogram only identified 57% of patients with pulmonary embolism
Vascular opacification and motion artifact are the principal factors which influence interpretability of MRA [MEDLINE]: some centers appear to obtain better images (for unclear reasons)
Technically Adequate Magnetic Resonance Pulmonary Angiogram
Sensitivity: 78%
Specificity: 99%
Technically Adequate Magnetic Resonance Pulmonary Angiogram + Magnetic Resonance Venogram: combination has significantly higher sensitivity than magnetic resonance pulmonary angiogram alone (however, only 52% of patients had technically inadequate results)
Sensitivity: 92%
Specificity: 96%
Recommendations
Magnetic Resonance Pulmonary Artery Angiogram and Venogram Studies Should Only be Performed in Centers with Local Expertise
Recommendations (European Society of Cardiology and European Respiratory Society Guidelines for the Diagnosis and Management of Acute Pulmonary Embolism, 2019) (Eur Heart J, 2020) [MEDLINE]
Magnetic Resonance Pulmonary Artery Angiogram is Not Recommended to Rule Out Acute Pulmonary Embolism (Class III, Level A)
Recommendations (2026 AHA/ACC/ACCP/ACEP/CHEST/SCAI/SHM/SIR/SVM/SVN Guideline for the Evaluation and Management of Acute Pulmonary Embolism in Adults: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines) (Circulation, 2026) [MEDLINE]
In Patients with Suspected Acute Pulmonary Embolism (PE) Who Cannot Undergo a Computed Tomography (CT) Pulmonary Artery Angiogram, it is Reasonable to Perform a Ventilation/Pertfusion (V/Q) Scan in Preference to Contrast-Enhanced Magnetic Resonance Angiography (MRA) to Improve the Diagnostic Yield (Class of Recommendation: 2a; Level of Evidence: B-R)
Recommendations for Diagnostic Testing Suspected Upper Extremity Deep Venous Thrombosis (Chest Antithrombotic Therapy and Prevention of Thrombosis 2012 Guidelines) [MEDLINE]
If Upper Extremity Compression Venous Doppler Ultrasound is Negative with High Clinical Suspicion, Moderate/High-Sensitivity D-Dimer, Serial Ultrasound, CT Upper Extremity Venogram, or Gadolinium-Enhanced Magnetic Resonance Upper Extremity Magnetic Resonance Imaging (MRI) Venogram is Recommended (Grade 2C Recommendation)
Lower Extremity Impedance Plethysmography (IPG)
Indications
Sensitive for Above the Knee Deep Venous Thrombosis
Lower Extremity Radiofibrinogen Study
Indications
Sensitive for Calf/Lower Thigh Deep Venous Thrombosis
Arterial Blood Gas Patterns in the Setting of Acute Pulmonary Embolism (PE)
Hypocapnia with Respiratory Alkalosis
Physiology
Due to Hyperventilation Associated with Pulmonary Hypertension
Hypoxemia with Elevated A-a Gradient
Epidemiology
Hypoxemia (pO2 <80 mm Hg) Occurs in Approximately 74% of Acute Pulmonary Embolism Cases (Chest, 1991) [MEDLINE]
Alveolar-Arterial (A-a) Gradient >20 mm Hg Occurs in Approximately 86% of Acute Pulmonary Embolism Cases (Chest, 1991) [MEDLINE]
Physiology
Due to V/Q Mismatch/Intrapulmonary Shunt/Decreased Cardiac Output with Low SvO2
Clinical
Presence of SaO2 <95% at Time of Acute Pulmonary Embolism Diagnosis Confers an Increased Risk of In-Hospital Complications (Such as Respiratory Failure, Cardiogenic Shock, and Death)
General Comments Rehgarding V/Q Scan in the Setting of Acute Pulmonary Embolism
Overall Diagnostic Accuracy of V/Q is Poor (Ranges from 15-86%) in 72% of All Patients, Insufficient to Diagnose Acute Pulmonary Embolism or Exclude the Diagnosis of Acute Pulmonary Embolism
Normal Scan
Normal V/S SCan Virtually Excludes the Diagnosis of Acute Pulmonary Embolism
Low Probability Scan
Low Clinical Probability + Low Probability V/Q Svcan = 4% Probability of Acute Pulmonary Embolism
Note: if clinical probability is high, low probability V/Q has 40% probability of Acute Pulmonary Embolism
Intermediate Probability Scan = Ranges from 15-66% Probability of Acute Pulmonary Embolism (Depending on the Clinical Probability)
High Probability Scan
High Clinical Probability + High Probability V/Q Scan = 95% Probability of Acute Pulmonary Embolism (These Patients Can Be Treated with Heparin, Thrombolytics without Pulmonary Angiogram)
Note: if clinical probability is low, high prob V/Q has 56% probability of Acute Pulmonary Embolism
Recommendations (European Society of Cardiology and European Respiratory Society Guidelines for the Diagnosis and Management of Acute Pulmonary Embolism, 2019) (Eur Heart J, 2020) [MEDLINE]
If the Perfusion Lung Scan is Normal, Acute Pulmonary Embolism Can Be Excluded without Further Testing (Class I, Level A)
If the V/Q Scan is High Probability for Acute Pulmonary Embolism, it Should Be Considered to Accept that the Diagnosis of Acute Pulmonary Embolism (without Further Testing) (Class IIa, Level B)
A Non-Diagnostic V/Q Scan Should Be Considered as Exclusion of Acute Pulmonary Embolism when Combined with a Negative Lower Extremity Proximal Compression Ultrasound Study in Patients with Low Clinical Probability or Who are Acute Pulmonary Embolism-Unlikely (Class IIa, Level B)
Recommendations (2026 AHA/ACC/ACCP/ACEP/CHEST/SCAI/SHM/SIR/SVM/SVN Guideline for the Evaluation and Management of Acute Pulmonary Embolism in Adults: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines) (Circulation, 2026) [MEDLINE]
Diagnosis
In Patients Presenting with Symptoms/Signs Suggestive of Acute Pulmonary Embolism (PE), Imaging is Recommended for Those Who are Deemed High Probability (>50% Probability of Pulmonary Embolism) by a Validated Clinical Risk Prediction Score or an Elevated D-Dimer Level in Order to Confirm/Exclude Pulmonary Embolism (PE) (Class of Recommendation: 1; Level of Evidence: A)
In Patients Undergoing Imaging Evaluation for Suspected Acute Pulmonary Embolism (PE), a Positive Computed Tomography (CT) Pulmonary Artery Angiogram or High Probability Ventilation/Perfusion (V/Q) Scan is Sufficient to Diagnose Pulmonary Embolism (PE) (Class of Recommendation: 1; Level of Evidence: A)
In Patients Undergoing Imaging Evaluation, a Computed Tomography (CT) Pulmonary Artery Angiogram is Recommended in Preference to a V/Q Scan to Confirm the Diagnosis of Acute Pulmonary Embolism (PE) (Class of Recommendation: 1; Level of Evidence: B-R)
In Pregnant Patients Presenting with Symptoms, YEARS Criteria Suggestive of Acute Pulmonary Embolism (PE), and a Normal Chest X-Ray, Imaging Evaluation with Low-Radiation Dose Computed Tomography (CT) Pulmonary Artery Angiogram is Reasonable Over Low-Dose Perfusion Scintigraphy (Class of Recommendation: 2a; Level of Evidence: B-NR)
In Patients Undergoing Evaluation for Pulmonary Embolism (PE), V/Q Single-Photon Emission Computed Tomography (SPECT) is Reasonable in Preference to a Planar V/Q Scan as a Diagnostic Study (Class of Recommendation: 2a; Level of Evidence: B-R)
In Patients with Suspected Acute Pulmonary Embolism (PE) Who Cannot Undergo a Computed Tomography (CT) Pulmonary Artery Angiogram, it is Reasonable to Perform a V/Q Scan in Preference to Contrast-Enhanced Magnetic Resonance Angiography (MRA) to Improve the Diagnostic Yield (Class of Recommendation: 2a; Level of Evidence: B-R)
Ventilation-Perfusion Single-Photon Emission Computed Tomography (SPECT) Study
Recommendations (European Society of Cardiology and European Respiratory Society Guidelines for the Diagnosis and Management of Acute Pulmonary Embolism, 2019) (Eur Heart J, 2020) [MEDLINE]
V/Q Single-Photon Emission Computed Tomography (SPECT) Study May Be Considered for the Diagnosis of Acute Pulmonary Embolism (Class IIb, Level B)
Recommendations (2026 AHA/ACC/ACCP/ACEP/CHEST/SCAI/SHM/SIR/SVM/SVN Guideline for the Evaluation and Management of Acute Pulmonary Embolism in Adults: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines) (Circulation, 2026) [MEDLINE]
Diagnosis
In Patients Presenting with Symptoms/Signs Suggestive of Acute Pulmonary Embolism (PE), Imaging is Recommended for Those Who are Deemed High Probability (>50% Probability of Pulmonary Embolism) by a Validated Clinical Risk Prediction Score or an Elevated D-Dimer Level in Order to Confirm/Exclude Pulmonary Embolism (PE) (Class of Recommendation: 1; Level of Evidence: A)
In Patients Undergoing Evaluation for Pulmonary Embolism (PE), V/Q Single-Photon Emission Computed Tomography (SPECT) is Reasonable in Preference to a Planar V/Q Scan as a Diagnostic Study (Class of Recommendation: 2a; Level of Evidence: B-R)
Sensitivity is 86% in Large (Main/Lobar/Segmental) Vessels
Sensitivity is 75% in All Vessels
Specificity
Specificity is 91% in Large (Main/Lobar/Segmental) Vessels
Specificity is 89% in All Vessels
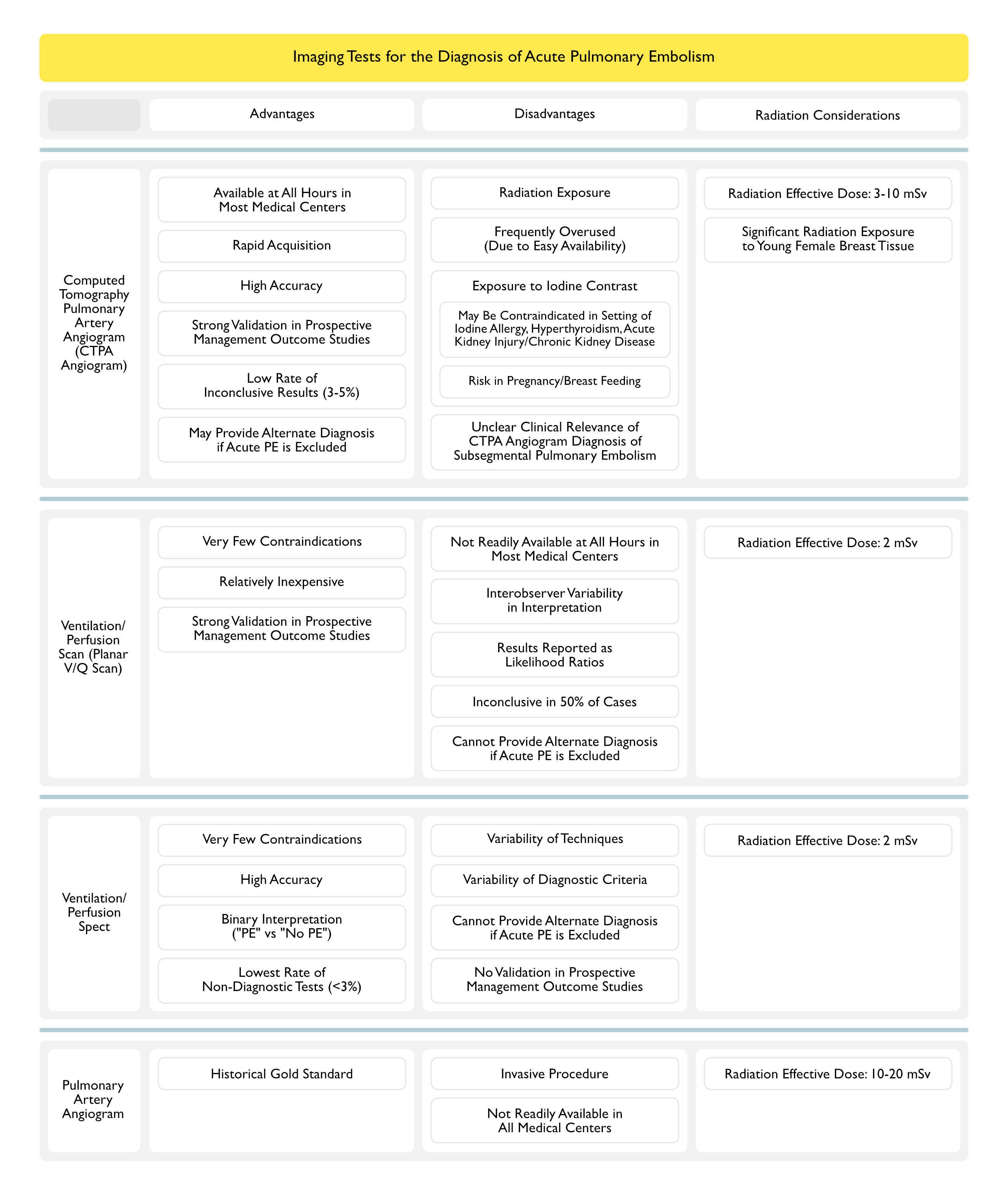
CT Pulmonary Angiogram Has Traditionally Been Considered Most Accurate for Large/Main/Lobar/Segmental Pulmonary Emboli and Less Accurate for Smaller/Peripheral Subsegmental Pulmonary Emboli
However, There is Improved Detection of Pulmonary Embolism by Multi-Detector CT Pulmonary Angiogram (9.4%) vs Single-Detector CT Pulmonary Angiogram (4.7%)
Low Risk of Pulmonary Embolism (PE) Following a Negative CT Pulmonary Angiogram
There is a <2% Risk of Pulmonary Embolism in 3-month Follow-Up in Patients with Negative CT Pulmonary Artery Angiogram + Low-Intermediate Clinical Probability + Negative Lower Extremity Dopplers
This Risk Increases to 5% if the Clinical Probability is High
Clinical Efficacy
Study of the Prognostic Role of Right Ventricular Enlargement on Multidetector-Row Chest CT in Acute Pulmonary Embolism (Circulation, 2004) [MEDLINE]: n = 63
Sensitivity and Specificity of RV Dimension/LV Dimension Ratio >0.9 for Predicting Adverse Events were 37.5% and 92.3% on the Axial View and 83.3% and 48.7% on the Reconstructed 4-Chamber View, Respectively
RV Dimension/LV Dimension Ratio >0.9 on the 4-Chamber View was an Independent Predictor for Adverse Events (Odds Ratio 4.02; 95% CI: 1.06 to 15.19; P = 0.041) when Adjusted for Age, Obesity, Cancer, and Recent Surgery
Grading of CT Signs of Right Ventricular Dysfunction in Acute Pulmonary Embolism (PE) (AJR Am J Roentgenol, 2010) [MEDLINE]
Volumetric Determination of the Right Ventricular Volume/Left Ventricular Volume Ratio
Most Reproducible/Least User-Dependent of the CT Measurements (as Compared to Septal Bowing or Inferior Vena Cava Reflux)
Ratio >1.2 is Suggestive of Right Ventricular (RV) Strain
Right Ventricular (RV) Dysfunction (by Echocardiogram or CT PA Angiogram): 2 pts
Heart Rate (HR) ≥100 BPM: 1 pt
Scoring: range 0-7
Stage I (0-2 points)
3.6% risk for in-hospital PE-related complications
4.2% risk for 30-day PE-related complications
1.7% 30-day PE-related mortality
Stage II (3-4 points)
9.7% risk for in-hospital PE-related complications
10.8% risk for 30-day PE-related complications
5.0% 30-day PE-related mortality
Stage III (>4 points)
28.0% risk for in-hospital PE-related complications
29.2% risk for 30-day PE-related complications
15.5% 30-day PE-related mortality
Systematic Review and Meta-Analysis of Predictive Value of CT Pulmonary Artery Angiogram in Acute Pulmonary Embolism (Am J Med, 2015) [MEDLINE]: n = 13,162 (49 studies)
An Abnormally Increased RV/LV Diameter Ratio Measured on Transverse Sections was Associated with an Approximately 2.5-Fold Risk for All-Cause Mortality (Pooled Odds Ratio 2.5; 95% CI: 1.8-3.5) and Adverse Outcome (Odds Ratio 2.3; 95% CI: 1.6-3.4) and a 5-Fold Risk for Pulmonary Embolism-Related Mortality (Odds Ratio 5.0; 95% CI: 2.7-9.2)
Thrombus Load (Odds Ratio 1.6; 95% CI: 0.7-3.9; P = 0.2896) and Central Location (Odds Ratio 1.7; 95% CI: 0.7-4.2; P = o.2609) were Not Predictive for All-Cause Mortality, Although Both were Associated with Adverse Clinical Outcome
Across All Endpoints, the RV/LV Diameter Ratio on Transverse CT Sections Had the Strongest Predictive Value and Most Robust Evidence Base for Adverse Clinical Outcomes in Patients with Acute Pulmonary Embolism
Retrospective Review of CT Pulmonary Artery Angiograms in Tertiary Care Hospital (AJR Am J Roentgenol, 2015) [MEDLINE]: n = 937 CT pulmonary artery angiogram studies
Acute Pulmonary Embolism (PE) was Diagnosed in 18.6% of CT Pulmonary Artery Angiograms
There was Discordance Between the Chest Radiologist and the Original Radiologist in 25.9% of Cases
Discordance Occurred More Commonly When the Original Reported PE was Solitary (46.2% of Solitary PE’s were Considered Negative on Retrospective Review) and Located in a Segmental/Subsegmental Pulmonary Artery (26.8% of Segmental and 59.4% of Subsegmental PE’s were Considered Negative on Retrospective Review)
Temple University Study of Instruction in Identifying Right Heart Strain on CT PA Angiogram (ATS Sch, 2022) [MEDLINE]: n = 93
Study Used RV/LV Ratio ≥1.0
Retrospective Study of Artificial Intelligence (AI) in Detecting Pulmonary Embolism on CT PA Angiogram (Am J Roentgenol, 2022) [MEDLINE]
As Compared to Clinical Reports, AI Exhibited Significantly Lower Specificity (92.7% vs 99.8%, p = .045) and Positive Predictive Value (86.8% vs 97.3%, p = 0.03), But No Significant Difference in Sensitivity (82.5% vs 90.0%, p = 0.37) or Negative Predictive Value (99.8% vs 99.9%, p = 0.36)
For AI, Neither Sensitivity Nor Specificity Varied Significantly in Association with Age, Sex, Examination Location, or Cancer-Related Clinical Scenario (All p > 0.05)
Explanations of False Positives by AI Included Metastatic Lymph Nodes and Pulmonary Venous Filling Defect
Explanations of False Negatives by AI Included Surgically Altered Anatomy and Small-Caliber Subsegmental Vessel
Recommendations (European Society of Cardiology and European Respiratory Society Guidelines for the Diagnosis and Management of Acute Pulmonary Embolism, 2019) (Eur Heart J, 2020) [MEDLINE]
In Suspected High-Risk Acute Pulmonary Embolism (Presence of Hemodynamic Instability), Bedside Echocardiogram or Emergency CT Pulmonary Artery Angiogram (Depending on Availability and Clinical Circumstances) is Recommended for Diagnosis (Class I, Level C)
If the CT Pulmonary Artery Angiogram is Normal in a Patient with Low-Intermediate Clinical Probability, or Who is Acute Pulmonary Embolism-Unlikely, it is Recommended to Reject the Diagnosis of Acute Pulmonary Embolism (without Further Testing) (Class I, Level A)
If the CT Pulmonary Artery Angiogram Demonstrates a Segmental or More Proximal Filling Defect in a Patient with Intermediate-High Clinical Probability, it is Recommended to Accept the Diagnosis of Acute Pulmonary Embolism (without Further Testing) (Class I, Level B)
If the CT Pulmonary Artery Angiogram is Normal in a Patient with High Clinical Probability or Who is Acute Pulmonary Embolism-Likely , It Should Be Considered to Reject the Diagnosis of Acute Pulmonary Embolism (without Further Testing) (Class IIa, Level B)
Further Imaging Tests to Confirm Acute Pulmonary Embolism May Be Considered in Cases of Isolated Subsegmental Filling Defects (Class IIb, Level C)
CT Venography is Not Recommended as an Adjunct to CT Pulmonary Artery Angiogram (Class III, Level B)
Recommendations (2026 AHA/ACC/ACCP/ACEP/CHEST/SCAI/SHM/SIR/SVM/SVN Guideline for the Evaluation and Management of Acute Pulmonary Embolism in Adults: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines) (Circulation, 2026) [MEDLINE]
In Patients Presenting with Symptoms Suggestive of Acute Pulmonary Embolism (PE), a Targeted History and Comprehensive Physical Examination is Recommended to Assist in Determining the Clinical Pretest Probability of Acute Pulmonary Embolism (PE) (Class of Recommendation: 1; Level of Evidence: A)
In Adult Patients Undergoing Evaluation for Pulmonary Embolism (PE) and Who Have a Low/Intermediate Clinical Probability of Pulmonary Embolism (PE) (<50%) by Risk Assessment, an Age-Adjusted D-Dimer Value Below the Threshold (Age × 10 μg/L for Fibrinogen Equivalent Units Assays) Effectively Excludes Pulmonary Embolism (PE) and the Need for Imaging (Class of Recommendation: 2a; Level of Evidence: B-R)
In Adult Patients with Suspected Pulmonary Embolism (PE), the YEARS Algorithm Can Be Useful to Identify Which Patients Do Not Need Imaging to Rule Out Pulmonary Embolism (PE) (Class of Recommendation: 2a; Level of Evidence: B-R)
YEARS Algorithm
In Patients Who Have ≥1 of the Following YEARS Criteria, Use a D-Dimer Threshold of 500 μg/L
Acute Pulmonary Embolism (PE) as the Most Likely Diagnosis
Clinical Signs of Deep Venous Thrombosis (DVT)
Hemoptysis
In Patients Who Have for Have No YEARS Criteria, Use a D-Dimer Threshold of 1000 μg/L
In Pregnant Adults, it May Be Reasonable to Use Pregnancy-Adapted YEARS Criteria to Identify Patients Who Do Not Need Imaging for Pulmonary Embolism (PE) (Class of Recommendation: 2b; Level of Evidence: B-R)
In Patients Presenting with Symptoms/Signs Suggestive of Acute Pulmonary Embolism (PE), Imaging is Recommended for Those Who are Deemed High Probability (>50% Probability of Pulmonary Embolism) by a Validated Clinical Risk Prediction Score or an Elevated D-Dimer Level in Order to Confirm/Exclude Pulmonary Embolism (PE) (Class of Recommendation: 1; Level of Evidence: A)
In Patients Undergoing Imaging Evaluation for Suspected Acute Pulmonary Embolism (PE), a Positive Computed Tomography (CT) Pulmonary Artery Angiogram or High Probability Ventilation/Perfusion (V/Q) Scan is Sufficient to Diagnose Pulmonary Embolism (PE) (Class of Recommendation: 1; Level of Evidence: A)
In Patients Undergoing Imaging Evaluation, a Computed Tomography (CT) Pulmonary Artery Angiogram is Recommended in Preference to a V/Q Scan to Confirm the Diagnosis of Acute Pulmonary Embolism (PE) (Class of Recommendation: 1; Level of Evidence: B-R)
In Pregnant Patients Presenting with Symptoms, YEARS Criteria Suggestive of Acute Pulmonary Embolism (PE), and a Normal Chest X-Ray, Imaging Evaluation with Low-Radiation Dose Computed Tomography (CT) Pulmonary Artery Angiogram is Reasonable Over Low-Dose Perfusion Scintigraphy (Class of Recommendation: 2a; Level of Evidence: B-NR)
In Patients Presenting with an Acute Pulmonary Embolism (PE) Who Undergo Computed Tomography (CT) Pulmonary Artery Angiogram, Reporting the Numerical Right Ventricle (RV)/Left Ventricle (LV) Ratio (Measured by Internal Diameter Assessed on Axial or Reformatted 4D-Chamber View) is Recommended Over Subjective Quantification for Risk Stratification (Class of Recommendation: 1; Level of Evidence: B-R)
Abnormal Values
RV/LV Ratio >0.9
In Patients with Acute Pulmonary Embolism (PE), Reporting of the Following Chronic Features on Computed Tomography (CT) Pulmonary Artery Angiogram May Be Useful to Identify Patients at Risk for Chronic Clinical Sequelae of Pulmonary Embolism (PE), Including Post-Pulmonary Embolism Chronic Thromboembolic Pulmonary Disease (CTEPD) (Class of Recommendation: 2b; Level of Evidence: B-NR)
Intravascular Webs
Intraventricular Septal Flattening
Bronchial Artery Dilation
Pulmonary Artery Retraction or Dilation
RV Hypertrophy
Right Ventricular Imaging (Echocardiogram or Computed Tomography Pulmonary Artery Angiogram) for Risk Stratification
In Patients with Acute Pulmonary Embolism (PE) and an Elevated Clinical Severity Score But without Evidence of Shock (i.e. AHA/ACC Pulmonary Embolism Categories C-D), Right Ventricular Imaging is Recommended for Short-Term Risk Stratification (Class of Recommendation: 1; Level of Evidence: A)
In Patients with Acute Pulmonary Embolism (PE) and an Elevated Clinical Severity Score But without Evidence of Persistent Hypotension or Shock (i.e. AHA/ACC Pulmonary Embolism Categories C-D), Use of Echocardiography Over Computed Tomography (CT) Pulmonary Artery Angiogram is Preferred for Short-Term Risk Stratification (Class of Recommendation: 2a; Level of Evidence: B-NR)
Assessment of Thrombus Burden for Risk Stratification
In Patients with Acute Pulmonary Embolism (PE) in AHA/ACC Pulmonary Embolism Categories A-C, Quantification of Angiographic Thrombus Burden for Short-Term Risk Stratification is Not Recommended (Class of Recommendation: 3 = No Benefit; Level of Evidence: B-NR)
Serum Troponin May Be Elevated in Acute Pulmonary Embolism: due to acute right heart overload
Not Useful for the Diagnosis of Acute Pulmonary Embolism, But Offers Prognostic Information
Elevated Serum Troponin is Associated with Increased Incidence of Prolonged Hypotension and Increased 30-Day Mortality
Troponin I: elevated in 30% of moderate-large PE
Troponin T: elevated in 50% of moderate-large PE
Clinical Efficacy
Grading of Pulmonary Embolism Using Right Ventricular Dysfunction and Troponin Levels (Chest, 2013) [MEDLINE]
Right Ventricular Dysfunction and Elevated Troponin Level: these criteria have an incremental prognostic value for risk stratification in hemodynamically-stable patients with acute pulmonary embolism
Bova Score Grading of Intermediate-Risk Pulmonary Embolism Patients (Eur Respir J, 2014) [MEDLINE]
SBP 90-100 mm Hg: 2 pts
Elevated Troponin: 2 pts
RV Dysfunction (by Echocardiogram or CT): 2 pts
HR ≥100 BPM: 1 pt
Scoring: range 0-7
Stage I (0-2 points)
3.6% risk for in-hospital PE-related complications
4.2% risk for 30-day PE-related complications
1.7% 30-day PE-related mortality
Stage II (3-4 points)
9.7% risk for in-hospital PE-related complications
10.8% risk for 30-day PE-related complications
5.0% 30-day PE-related mortality
Stage III (>4 points)
28.0% risk for in-hospital PE-related complications
29.2% risk for 30-day PE-related complications
15.5% 30-day PE-related mortality
Systematic Review and Meta-Analysis of Biomarkers to Risk Stratify Patients with Acute Pulmonary Embolism (Lung, 2015) [MEDLINE]
Biomarkers Included Serum Troponin, Serum Brain Natriuretic Peptide (BNP) and N-Terminal proBNP (NT-proBNP), or Heart-Type Fatty Acid-Binding Protein (H-FABP)
All Three Biomarkers were Significantly Associated with Increased Risk for Short-Term All-Cause Mortality, Pulmonary Embolism-Related Mortality, and Serious Adverse Events
All-Cause Mortality: Troponin [Odds Ratio 4.80; 95% CI: 3.25-7.08, I(2) = 54%], BNP or NT-proBNP (Odds Ratio 7.98; 95% CI: 4.34-14.67, I(2) = 0%)
Pulmonary Embolism-Related Mortality: Troponin (Odds Ratio 3.80; 95% CI: 2.74-5.27, I(2) = 0%), BNP or NT-proBNP (OR 7.57; 95% CI: 2.89-19.81, I (2) = 0%) and H-FABP (OR 25.97; 95% CI: 6.63-101.66, I(2) = 40%)
H-FABP Had the Lowest Negative Likelihood Ratio of 0.17 for Mortality
High-Sensitivity Cardiac Troponin T (hs-cTnT) Had a Negative Likelihood Ratio of 0.21
Combination of Troponin-T >0.07 µg/L + NT-proBNP >600 ng/L is Associated with 33% 40-Day Mortality Rate (as Compared to 0% Mortality with NT-proBNP level <600 ng/L)
Recommendations (2026 AHA/ACC/ACCP/ACEP/CHEST/SCAI/SHM/SIR/SVM/SVN Guideline for the Evaluation and Management of Acute Pulmonary Embolism in Adults: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines) (Circulation, 2026) [MEDLINE]
Biomarkers for Risk Stratification
In Patients with Acute Pulmonary Embolism (PE) and an Elevated Clinical Severity Score without Features of Hypotension or Shock (i.e. AHA/ACC PE Category C), Measurement of at Least One Cardiac Biomarker (Such as Serum Troponin or Brain Natriuretic peptide) is Recommended to Assist with Risk Stratification for Short-Term Complications and/or Mortality (Class of Recommendation: 1; Level of Evidence: B-NR)
In Patients with Acute Pulmonary Embolism (PE) (i.e. AHA/ACC Pulmonary Embolism Categories C to E) Who are Undergoing Evaluation at an Acute Care Facility, Measurement of Lactate (Either Venous or Arterial) is Recommended to Assist with Risk Stratification for Short-Term Complications and/or Mortality (Class of Recommendation: 1; Level of Evidence: B-NR)
Serum Brain Natriuretic Peptide May Be Elevated in Acute Pulmonary Embolism
Magnitude of Increase in Brain Natriuretic Peptide Correlates with the Risk of Subsequent Complications and Prolonged Hospitalization
BNP >90 pg/ml (within 4 hrs of Presentation): associated with adverse outcomes (death, cardioplumonary resuscitation, mechanical ventilation, pressor therapy, thrombolysis, and embolectomy)
BNP <50 pg/ml (within 4 hrs of Presentation): benign clinical course in 95% of cases
Sensitivity: 60%
Specificity: 62%
Clinical Data
Grading of Factors Associated with 30-Day Frequency of Adverse Events in Prep Study (Am J Respir Crit Care Med, 2010) [MEDLINE]
Altered Mental Status: OR 6.8 (95% CI: 2.0-23.3)
Shock on Admission: OR 2.8 (95% CI: 1.1-7.5)
Cancer: OR 2.9 (95% CI: 1.2-6.9)
Elevated BNP: OR 1.3 for an increase of 250 ng/L (95% CI: 1.1-1.6)
Echocardiographic Right Ventricular Volume/Left Ventricular Volume Ratio: OR 1.2 for an increase of 0.1 (95% CI: 1.1-1.4)
Systematic Review and Meta-Analysis of Biomarkers to Risk Stratify Patients with Acute Pulmonary Embolism (Lung, 2015) [MEDLINE]
Biomarkers Included Serum Troponin, Serum Brain Natriuretic Peptide (BNP) and N-Terminal proBNP (NT-proBNP), or Heart-Type Fatty Acid-Binding Protein (H-FABP)
All Three Biomarkers were Significantly Associated with Increased Risk for Short-Term All-Cause Mortality, Pulmonary Embolism-Related Mortality, and Serious Adverse Events
All-Cause Mortality: Troponin [Odds Ratio 4.80; 95% CI: 3.25-7.08, I(2) = 54%], BNP or NT-proBNP (Odds Ratio 7.98; 95% CI: 4.34-14.67, I(2) = 0%)
Pulmonary Embolism-Related Mortality: Troponin (Odds Ratio 3.80; 95% CI: 2.74-5.27, I(2) = 0%), BNP or NT-proBNP (OR 7.57; 95% CI: 2.89-19.81, I (2) = 0%) and H-FABP (OR 25.97; 95% CI: 6.63-101.66, I(2) = 40%)
H-FABP Had the Lowest Negative Likelihood Ratio of 0.17 for Mortality
High-Sensitivity Cardiac Troponin T (hs-cTnT) Had a Negative Likelihood Ratio of 0.21
Combination of Troponin-T >0.07 µg/L + NT-proBNP >600 ng/L is Associated with 33% 40-Day Mortality Rate (as Compared to 0% Mortality with NT-proBNP level <600 ng/L)
Recommendations (2026 AHA/ACC/ACCP/ACEP/CHEST/SCAI/SHM/SIR/SVM/SVN Guideline for the Evaluation and Management of Acute Pulmonary Embolism in Adults: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines) (Circulation, 2026) [MEDLINE]
Biomarkers for Risk Stratification
In Patients with Acute Pulmonary Embolism (PE) and an Elevated Clinical Severity Score without Features of Hypotension or Shock (i.e. AHA/ACC PE Category C), Measurement of at Least One Cardiac Biomarker (Such as Serum Troponin or Brain Natriuretic peptide) is Recommended to Assist with Risk Stratification for Short-Term Complications and/or Mortality (Class of Recommendation: 1; Level of Evidence: B-NR)
In Patients with Acute Pulmonary Embolism (PE) (i.e. AHA/ACC Pulmonary Embolism Categories C to E) Who are Undergoing Evaluation at an Acute Care Facility, Measurement of Lactate (Either Venous or Arterial) is Recommended to Assist with Risk Stratification for Short-Term Complications and/or Mortality (Class of Recommendation: 1; Level of Evidence: B-NR)
Serum Lactate May Be Used to Risk Stratify Patients in Acute Pulmonary Embolism (PE)
Clinical Efficacy
Prospective Study of Plasma Lactate in Acute Symptomatic Pulmonary Embolism (with Normotension) (Thorax, 2015) [MEDLINE]: n = 496 (between 2012-2014)
Pulmonary Embolism-Related Complications Occurred in 4.0% of Patients (95% CI: 2.5-6.2%)
Patients with Pulmonary Embolism-Related Complications Had Higher Baseline Lactate Levels (Median 2.66 mmol/L; Interquartile Range 1.56-5.96 mmol/L) than Patients without Complications (Median 1.20 mmol/L; Interquartile Range 1.20-2.00 mmol/L) (p<0.001)
Patients with Elevated Plasma Lactate Had an Increased Rate of Pulmonary Embolism-Related Complications (Adjusted Odds Ratio 5.3; 95% CI: 1.9-14.4; p = 0.001), as Compared to Those with Low Plasma Lactate
Combination of Elevated Plasma Lactate with Markers of Right Ventricular Dysfunction (by Echocardiogram) and Myocardial Injury (by Cardiac Troponin) was a Particularly Useful Prognostic Indicator (Positive Predictive Value 17.9%; 95% CI 6.1-36.9%)
Study of Serum Venous Lactate in the Prediction of In-Hospital Adverse Outcomes in Normotensive Acute Pulmonary Embolism (Eur J Intern Med, 2021) [MEDLINE]
An Optimized Venous Lactate Cutoff Value of 3.3 mmol/L Predicted Both In-Hospital Adverse Outcome (Odds Ratio 11.0; 95% CI 4.6-26.3) and All-Cause Mortality (Odds Ratio 3.8; 95%CI 1.3-11.3)
The Established Cutoff Value for Arterial Lactate (2.0 mmol/L) and the Upper Limit of Normal for Venous Lactate (2.3 mmol/l) Had Lower Prognostic Value for Adverse Outcomes (Odds Ratio 3.6; 95% CI 1.5-8.7 and Odds Ratio 5.7; 95% CI 2.4-13.6, Respectively) and Did Not Predict Mortality
If Added to the 2019 European Society of Cardiology Algorithm, Venous Lactate <2.3 mmol/L was Associated with a High Negative Predictive Value (0.99 [95% CI 0.97-1.00]) for Adverse Outcomes in Intermediate-Low Risk Patients, Whereas Lactate Levels ≥3.3 mmol/L Predicted Adverse Outcomes in the Intermediate-High Risk Group (Odds Ratio 5.2; 95% CI 1.8-15.0)
Recommendations (2026 AHA/ACC/ACCP/ACEP/CHEST/SCAI/SHM/SIR/SVM/SVN Guideline for the Evaluation and Management of Acute Pulmonary Embolism in Adults: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines) (Circulation, 2026) [MEDLINE]
Hemodynamic Assessment for Risk Stratification
In Patients with Acute Pulmonary Embolism (PE) in AHA/ACC Pulmonary Embolism Category D2, Evaluating for the Presence of Normotensive Shock Can Be Useful to Identify Patients at Increased Risk for Clinical Deterioration and In-Hospital Death (Class of Recommendation: 2a; Level of Evidence: B-NR)
Normotensive Shock is Defined as Isolated Hypoperfusion without Hypotension Identified by Any of the Following
Serum Lactate >2 mmol/L
Urine Output <720 mL/24 hrs
Creatinine Increase ≥0.3 mg/mL in 24 hrs
Cardiac Index ≤2.2 L/min/m2 from Peripheral Arterial and Mixed Venous Oxygenation Saturation Values
In Patients with Acute Pulmonary Embolism (PE) in AHA/ACC Pulmonary Embolism Category C3, a MAP <80 mm Hg May Be Useful to Identify Patients Who May Require Escalation of Therapy (Class of Recommendation: 2a; Level of Evidence: B-NR)
Only 30-40% of Acute Pulmonary Emboli Have Positive Echocardiographic Evidence of Acute Pulmonary Embolism
This Percentage is Higher in Cases of Massive Acute Pulmonary Embolism
Features
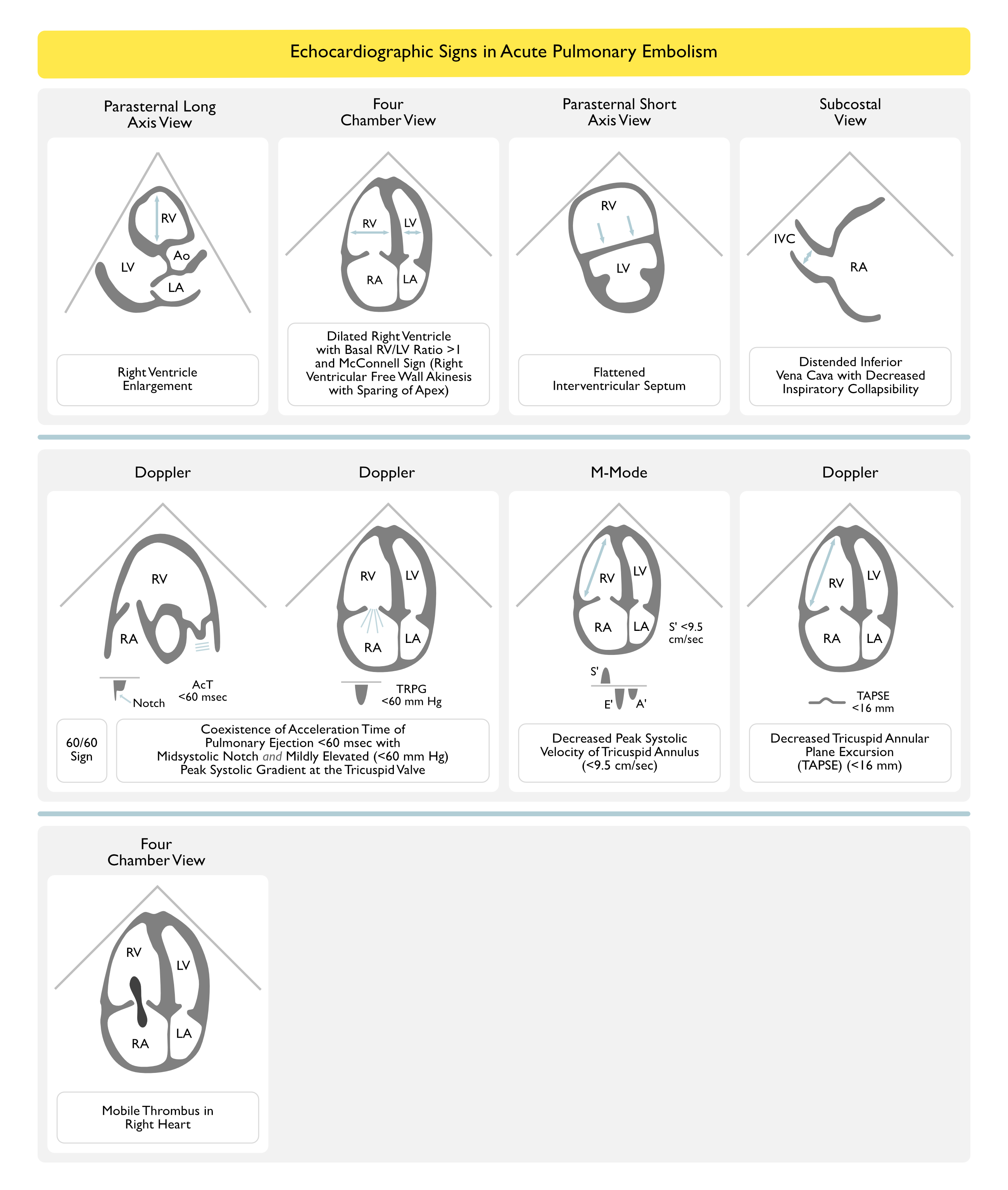
Features of RV Strain/Overload: present in 30-40% of patients with acute PE (higher percentage in patients with massive acute pulmonary embolism)
Decreased Right Ventricular Ejection Fraction
Right Ventricular Enlargement (RVE)
Tricuspid Regurgitation (TR): Doppler of tricuspid regurgitation jet allows estimation of the pulmonary artery pressure
Pulmonic Regurgitation
RV Thrombus: >35% patients with right ventricular thrombus develop acute pulmonary embolism, but only 4% of acute pulmonary embolism patients have an right ventricular thrombus
McConnell’s Sign (77% sensitivity for diagnosis of acute acute pulmonary embolism): regional wall motion abnormalities that spare the right ventricular apex
Normal LV Ejection Fraction: usually seen
Clinical Data
Grading of Factors Associated with 30-Day Frequency of Adverse Events in Prep Study (Am J Respir Crit Care Med, 2010) [MEDLINE]
Altered Mental Status: OR 6.8 (95% CI: 2.0-23.3)
Shock on Admission: OR 2.8 (95% CI: 1.1-7.5)
Cancer: OR 2.9 (95% CI: 1.2-6.9)
Elevated BNP: OR 1.3 for an increase of 250 ng/L (95% CI: 1.1-1.6)
Echocardiographic Right Ventricular Volume/Left Ventricular Volume Ratio: OR 1.2 for an increase of 0.1 (95% CI: 1.1-1.4)
Grading of Pulmonary Embolism Using Right Ventricular Dysfunction and Troponin Levels (Chest, 2013) [MEDLINE]
Right Ventricular Dysfunction and Elevated Troponin Level: these criteria have an incremental prognostic value for risk stratification in hemodynamically-stable patients with acute pulmonary embolism
Bova Score Grading of Intermediate-Risk Pulmonary Embolism Patients (Eur Respir J, 2014) [MEDLINE]
SBP 90-100 mm Hg: 2 pts
Elevated Troponin: 2 pts
RV Dysfunction (by Echocardiogram or CT): 2 pts
HR ≥100 BPM: 1 pt
Scoring: range 0-7
Stage I (0-2 points)
3.6% risk for in-hospital PE-related complications
4.2% risk for 30-day PE-related complications
1.7% 30-day PE-related mortality
Stage II (3-4 points)
9.7% risk for in-hospital PE-related complications
10.8% risk for 30-day PE-related complications
5.0% 30-day PE-related mortality
Stage III (>4 points)
28.0% risk for in-hospital PE-related complications
29.2% risk for 30-day PE-related complications
15.5% 30-day PE-related mortality
Multicenter Prospective Study of TAPSE in Normotensive Acute Pulmonary Embolism (J Thromb Haemost, 2014) [MEDLINE]: n = 782
Patients with a TAPSE of ≤ 1.6 cm at the Time of Pulmonary Embolism Diagnosis were Significantly More Likely to Die from Any Cause (Hazard Ratio 2.3; 95% CI: 1.2-4.7; P = 0.02) and from Pulmonary Embolism (HR 4.4; 95% CI: 1.3-15.3; P = 0.02) During Follow-Up
In Normotensive Acute Pulmonary Embolism Patients, TAPSE Reflects Right Ventricular Function
For These Patients, TAPSE is Independently Predictive of Survival
Recommendations (European Society of Cardiology and European Respiratory Society Guidelines for the Diagnosis and Management of Acute Pulmonary Embolism, 2019) (Eur Heart J, 2020) [MEDLINE]
In Suspected High-Risk Acute Pulmonary Embolism (Presence of Hemodynamic Instability), Bedside Echocardiogram or Emergency CT Pulmonary Artery Angiogram (Depending on Availability and Clinical Circumstances) is Recommended for Diagnosis (Class I, Level C)
Recommendations (2026 AHA/ACC/ACCP/ACEP/CHEST/SCAI/SHM/SIR/SVM/SVN Guideline for the Evaluation and Management of Acute Pulmonary Embolism in Adults: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines) (Circulation, 2026) [MEDLINE]
In Patients with Suspected Acute Pulmonary Embolism (PE), an Echocardiogram is Not Recommended to Confirm/Refute the Diagnosis of Pulmonary Embolism (PE) (Class of Recommendation: 3 = No Benefit; Level of Evidence: B-NR)
In Patients with Acute Pulmonary Embolism (PE) Who Undergo Transthoracic Echocardiography, Right Ventricle (RV) Dysfunction Should Be Assessed and Reported by the Following Parameters to Assist with Risk Stratification (Class of Recommendation: 1; Level of Evidence: B-NR)
RV/LV End-Diastolic Ratio
Abnormal = RV/LV Ratio >0.9
RV End-Diastolic Diameter
Abnormal = End-Diastolic RV Diameter >30 mm (on RV-focused apical 4-chamber view)
Abnormal = RV Basal End-Diastolic Diameter >42 mm (on apical 4-chamber view)
*RV Free Wall Hypokinesis with Sparing of the Apex (McConnell’s Sign)
Tricuspid Systolic Velocity
Paradoxical Septal Motion
Inferior Vena Cava (IVC) Respirophasic Collapse
Right Ventricular Imaging (Echocardiogram or Computed Tomography Pulmonary Artery Angiogram) for Risk Stratification
In Patients with Acute Pulmonary Embolism (PE) and an Elevated Clinical Severity Score But without Evidence of Shock (i.e. AHA/ACC Pulmonary Embolism Categories C-D), Right Ventricular Imaging is Recommended for Short-Term Risk Stratification (Class of Recommendation: 1; Level of Evidence: A)
In Patients with Acute Pulmonary Embolism (PE) and an Elevated Clinical Severity Score But without Evidence of Persistent Hypotension or Shock (i.e. AHA/ACC Pulmonary Embolism Categories C-D), Use of Echocardiography Over Computed Tomography (CT) Pulmonary Artery Angiogram is Preferred for Short-Term Risk Stratification (Class of Recommendation: 2a; Level of Evidence: B-NR)
Assessment of Thrombus Burden for Risk Stratification
In Patients with Acute Pulmonary Embolism (PE) in AHA/ACC Pulmonary Embolism Categories A-C, Quantification of Angiographic Thrombus Burden for Short-Term Risk Stratification is Not Recommended (Class of Recommendation: 3 = No Benefit; Level of Evidence: B-NR)
Right Ventricular Systolic Pressure (RV-SYS): moderately elevated (with normal RV-EDP)
Pulmonary Artery Systolic Pressure (PA-SYS) and Pulmonary Artery Diastolic Pressure (PA-DIA): moderately elevated (severe elevations suggest CTEPH, since vascular remodeling is required to raise pressures this high/acute severe elevations will also produce rapid RV failure)
Prospective Trial of the Diagnostic Accuracy of Multiorgan Point-of Care (POCUS) Ultrasound, as Compared to Computed Tomography Pulmonary Artery Angiogram in the Diagnosis of Acute Pulmonary Embolism in Critically Ill Patients with Suspected Pulmonary Embolism (PLoS One, 2022) [MEDLINE]: n = 88
42% of Patients Had Acute Pulmonary Embolism
Multivariate Analysis Demonstrated a Relative Risk of Acute Pulmonary Embolism of 2.79 (95% CI: 1.61-4.84) for the Presence of Right Ventricular Dysfunction, of 2.54 (95% CI: 0.89-7.20) for D-Dimer Level >1000 ng/mL, and of 1.69 (95% CI: 1.12-2.63) for the Absence of an Alternative dDiagnosis to Acute Pulmonary Embolism on Lung POCUS or Chest X-Ray
The Combination with the Highest Diagnostic Accuracy for Acute Pulmonary Embolism Included the Following Variables
POCUS Transthoracic Echocardiography with Evidence of Right Ventricular Dysfunction
Lung POCUS or Chest X-Ray without an Alternative Diagnosis to Acute Pulmonary Embolism
Plasma D-Dimer Level >1000 ng/mL
Combining These Three Findings Resulted in an Area Under the Curve of 0.85 (95% CI: 0.77-0.94)
50% Sensitivity and 96% Specificity
Clinical Evaluation for Suspected Pulmonary Embolism in Pregnancy (see Pregnancy)
Clinical Efficacy
Markov Decision Model Study of Six International Societal Guidelines for the Evaluation of Suspected Pulmonary Embolism in Pregnancy (Chest, 2022) [MEDLINE]
Base-Case Analysis Demonstrated that the American Thoracic Society/Society of Thoracic Radiology (ATS-STR) Guidelines Yielded the Highest Health Benefits (22.90 QALYs) and was Cost-Effective (ICER of $7,808) Over the Australian Society of Thrombosis and Haemostasis Guidelines and the Society of Obstetric Medicine of Australia and New Zealand (ASTH-SOMANZ) Guidelines
Recommendations (American Thoracic Society/Society of Thoracic Radiology Clinical Practice Guidelines for the Evaluation of Suspected Pulmonary Embolism in Pregnancy) (Am J Respir Crit Care Med, 2011) [MEDLINE]
In Pregnant Women with Suspected Acute Pulmonary Embolism, D-Dimer Should Not Be Used to Exclude Acute Pulmonary Embolism (Weak Recommendation, Very Low Quality Evidence)
In Pregnant Women with Suspected Acute Pulmonary Embolism and Symptoms/Signs of Deep Venous Thrombosis, Bilateral Venous Compression Ultrasound of Lower Extremities is Recommended (Weak Recommendation, Very Low Quality Evidence)
If Positive, Anticoagulation Treatment is Recommended (Weak Recommendation, Very Low Quality Evidence)
If Negative, Further Testing is Recommended (Weak Recommendation, Very Low Quality Evidence)
In Pregnant Women with Suspected Acute Pulmonary Embolism and No Symptoms/Signs of Deep Venous Thrombosis, Studies of the Pulmonary Vasculature are Recommended Rather than Venous Compression Ultrasound of the Lower Extremities (Weak Recommendation, Very Low Quality Evidence)
In Pregnant Women with Suspected Acute Pulmonary Embolism, Chest X-Ray is Recommended as the First Radiation-Associated Procedure in the Imaging Work-Up (Strong Recommendation, Low Quality Evidence)
In Pregnant Women with Suspected Acute Pulmonary Embolism and a Normal Chest X-Ray, V/Q Scan is Recommended as the Next Imaging Test Rather than CT Pulmonary Artery Angiogram (Strong Recommendation, Low Quality Evidence)
In Pregnant Women with Suspected Acute Pulmonary Embolism and a Non-Diagnostic V/Q Scan, Further Diagnostic Testing is Recommended Over Clinical Management Alone (Weak Recommendation, Low Quality Evidence)
In Patients with a Non-Diagnostic V/Q Scan in Whom a Decision is Made to Further Investigate, CT Pulmonary Artery Angiogram is Recommended Over Digital Subtraction Angiography (Strong Recommendation, Very Low Quality Evidence)
In Pregnant Women with Suspected Acute Pulmonary Embolism and an Abnormal Chest X-Ray, CT Pulmonary Artery Angiogram is Suggested as the Next Imaging Test Rather than V/Q Scan (Weak Recommendation, Very Low Quality Evidence)
References
American College of Chest Physicians Evidence-Based Clinical Practice Guidelines 2012 (9th Edition)
Executive summary: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012 Feb;141(2 Suppl):7S-47S. doi: 10.1378/chest.1412S3 [MEDLINE]
Introduction to the ninth edition: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012 Feb;141(2 Suppl):48S-52S. doi: 10.1378/chest.11-2286 [MEDLINE]
Methodology for the development of antithrombotic therapy and prevention of thrombosis guidelines: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012 Feb;141(2 Suppl):53S-70S. doi: 10.1378/chest.11-2288 [MEDLINE]
Patient values and preferences in decision making for antithrombotic therapy: a systematic review: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012 Feb;141(2 Suppl):e1S-e23S. doi: 10.1378/chest.11-2290 [MEDLINE]
Parenteral anticoagulants: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012 Feb;141(2 Suppl):e24S-e43S. doi: 10.1378/chest.11-2291 [MEDLINE]
Oral anticoagulant therapy: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012 Feb;141(2 Suppl):e44S-e88S. doi: 10.1378/chest.11-2292 [MEDLINE]
Antiplatelet drugs: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012 Feb;141(2 Suppl):e89S-e119S. doi: 10.1378/chest.11-2293 [MEDLINE]
New antithrombotic drugs: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012 Feb;141(2 Suppl):e120S-e151S. doi: 10.1378/chest.11-2294 [MEDLINE] -Evidence-based management of anticoagulant therapy: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012 Feb;141(2 Suppl):e152S-e184S. doi: 10.1378/chest.11-2295 [MEDLINE]
Approach to outcome measurement in the prevention of thrombosis in surgical and medical patients: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012 Feb;141(2 Suppl):e185S-e194S. doi: 10.1378/chest.11-2289 [MEDLINE]
Prevention of VTE in nonsurgical patients: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012 Feb;141(2 Suppl):e195S-e226S. doi: 10.1378/chest.11-2296 [MEDLINE]
Prevention of VTE in nonorthopedic surgical patients: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012 Feb;141(2 Suppl):e227S-e277S. doi: 10.1378/chest.11-2297 [MEDLINE]
Prevention of VTE in orthopedic surgery patients: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012 Feb;141(2 Suppl):e278S-e325S. doi: 10.1378/chest.11-2404 [MEDLINE]
Perioperative management of antithrombotic therapy: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012 Feb;141(2 Suppl):e326S-e350S. doi: 10.1378/chest.11-2298 [MEDLINE]
Diagnosis of DVT: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012 Feb;141(2 Suppl):e351S-e418S. doi: 10.1378/chest.11-2299 [MEDLINE]
Antithrombotic therapy for VTE disease: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012 Feb;141(2 Suppl):e419S-e496S. doi: 10.1378/chest.11-2301 [MEDLINE]
Treatment and prevention of heparin-induced thrombocytopenia: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012 Feb;141(2 Suppl):e495S-e530S. doi: 10.1378/chest.11-2303 [MEDLINE]
Antithrombotic therapy for atrial fibrillation: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012 Feb;141(2 Suppl):e531S-e575S. doi: 10.1378/chest.11-2304 [MEDLINE]
Antithrombotic and thrombolytic therapy for valvular disease: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012 Feb;141(2 Suppl):e576S-e600S. doi: 10.1378/chest.11-2305 [MEDLINE]
Antithrombotic and thrombolytic therapy for ischemic stroke: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012 Feb;141(2 Suppl):e601S-e636S. doi: 10.1378/chest.11-2302 [MEDLINE]
Primary and secondary prevention of cardiovascular disease: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012 Feb;141(2 Suppl):e637S-e668S. doi: 10.1378/chest.11-2306 [MEDLINE]
Antithrombotic therapy in peripheral artery disease: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012 Feb;141(2 Suppl):e669S-e690S. doi: 10.1378/chest.11-2307 [MEDLINE]
VTE, thrombophilia, antithrombotic therapy, and pregnancy: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012 Feb;141(2 Suppl):e691S-e736S. doi: 10.1378/chest.11-2300 [MEDLINE]
Antithrombotic therapy in neonates and children: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012 Feb;141(2 Suppl):e737S-e801S. doi: 10.1378/chest.11-2308 [MEDLINE]
European Society of Cardiology/European Respiratory Society Clinical Practice Guidelines 2014
2014 ESC guidelines on the diagnosis and management of acute pulmonary embolism. Eur Heart J. 2014;35(43):3033-3069, 3069a-3069 k [MEDLINE]
American College of Chest Physicians Evidence-Based Clinical Practice Guidelines 2016
Antithrombotic Therapy for VTE Disease: CHEST Guideline and Expert Panel Report. Chest. 2016 Feb;149(2):315-52. doi: 10.1016/j.chest.2015.11.026. Epub 2016 Jan 7 [MEDLINE]
European Society of Cardiology/European Respiratory Society Clinical Practice Guidelines 2019
2019 ESC Guidelines for the diagnosis and management of acute pulmonary embolism developed in collaboration with the European Respiratory Society (ERS). Eur Heart J. 2020 Jan 21;41(4):543-603. doi: 10.1093/eurheartj/ehz405 [MEDLINE]
PERT Consortium Clinical Practice Guidelines 2019
Diagnosis, Treatment and Follow Up of Acute Pulmonary Embolism: Consensus Practice from the PERT Consortium. Clin Appl Thromb 2019 Jan-Dec;25:1076029619853037. doi: 10.1177/1076029619853037 [MEDLINE]
American Society of Hematology Clinical Practice Guidelines 2020
American Society of Hematology 2020 guidelines for management of venous thromboembolism: treatment of deep vein thrombosis and pulmonary embolism. Blood Adv. 2020 Oct 13;4(19):4693-4738. doi: 10.1182/bloodadvances.2020001830 [MEDLINE]
American College of Chest Physicians Evidence-Based Clinical Practice Guidelines 2021
Antithrombotic Therapy for VTE Disease: Second Update of the CHEST Guideline and Expert Panel Report. Chest. 2021 Dec;160(6):e545-e608. doi: 10.1016/j.chest.2021.07.055 [MEDLINE]
American College of Chest Physicians Evidence-Based Clinical Practice Guidelines 2012-2021
Antithrombotic Therapy for VTE Disease: Compendium and Review of CHEST Guidelines 2012-2021. Chest. 2024 Aug;166(2):388-404. doi: 10.1016/j.chest.2024.03.003 [MEDLINE]
AHA/ACC/ACCP/ACEP/CHEST/SCAI/SHM/SIR/SVM/SVN Evidence-Based Clinical Practice Guidelines 2026
2026 AHA/ACC/ACCP/ACEP/CHEST/SCAI/SHM/SIR/SVM/SVN Guideline for the Evaluation and Management of Acute Pulmonary Embolism in Adults: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2026 Feb 19. doi: 10.1161/CIR.0000000000001415 [MEDLINE]
General
Anticoagulant drugs in the treatment of pulmonary embolism. A controlled trial. Lancet. 1960 Jun 18;1(7138):1309-12 [MEDLINE]
Source of non-lethal pulmonary emboli. Lancet. 1974 Feb 16;1(7851):258-9 [MEDLINE]
A prospective study of venous thromboembolism after major trauma. N Engl J Med 1994; 331:1601–1606 [MEDLINE]
A clinical trial of vena caval filters in the prevention of pulmonary embolism in patients with proximal deep-vein thrombosis. Prévention du Risque d’Embolie Pulmonaire par Interruption Cave Study Group. N Engl J Med. 1998;338(7):409 [MEDLINE]
Vena caval filters: a comprehensive review. Blood. 2000;95(12):3669 [MEDLINE]
Predictors of rehospitalization for symptomatic venous thromboembolism after total hip arthroplasty. N Engl J Med. 2000;343(24):1758 [MEDLINE]
Extended-duration prophylaxis against venous thromboembolism after total hip or knee replacement: a meta-analysis of the randomised trials. Lancet. 2001;358(9275):9 [MEDLINE]
Deep vein thrombosis and its prevention in critically ill adults. Arch Intern Med 2001;161:1268–1279 [MEDLINE]
Pulmonary embolism mortality in the United States, 1979-1998: an analysis using multiple-cause mortality data. Arch Intern Med. 2003;163(14):1711 [MEDLINE]
Derivation and validation of a prognostic model for pulmonary embolism. Am J Respir Crit Care Med 2005; 172:1041-1046 [MEDLINE]
Deep venous thrombosis in medical-surgical critically ill patients: prevalence, incidence, and risk factors. Crit Care Med. 2005 Jul;33(7):1565-71 [MEDLINE]
Effectiveness of managing suspected pulmonary embolism using an algorithm combining clinical probability, D-dimer testing, and computed tomography. JAMA. 2006;295(2):172 [MEDLINE]
Clinical Practice: Acute pulmonary embolism. N Engl J Med 2008;359:2804–2813 [MEDLINE]
Prevention of thalidomide- and lenalidomide-associated thrombosis in myeloma. Leukemia. 2008 Feb;22(2):414-23. doi: 10.1038/sj.leu.2405062 [MEDLINE]
Comparative study on risk factors and early outcome of symptomatic distal versus proximal deep vein thrombosis: results from the OPTIMEV study. Thromb Haemost. 2009 Sep;102(3):493-500. doi: 10.1160/TH09-01-0053 [MEDLINE]
RIETE Investigators. Simplification of the pulmonary embolism severity index for prognostication in patients with acute symptomatic pulmonary embolism. Arch Intern Med 2010; 170: 1383–1389 [MEDLINE]
Coagulopathy does not protect against venous thromboembolism in hospitalized patients with chronic liver disease. Chest. 2010;137(5):1145 [MEDLINE]
Gadolinium-enhanced magnetic resonance angiography for pulmonary embolism. A multicenter prospective study (PIOPED III). Ann Intern Med 2010;152:434-443 [MEDLINE]
Reproducibility of CT signs of right ventricular dysfunction in acute pulmonary embolism. AJR Am J Roentgenol 2010; 194:1500-1506 [MEDLINE]
Prognostic factors for pulmonary embolism: the PREP study, a prospective multicenter cohort study. Am J Respir Crit Care Med 2010; 181:168-173 [MEDLINE]
Systematic review: case-fatality rates of recurrent venous thromboembolism and major bleeding events among patients treated for venous thromboembolism. Ann Intern Med. 2010 May 4;152(9):578-89. doi: 10.7326/0003-4819-152-9-201005040-00008 [MEDLINE]
Deep vein thrombosis: a clinical review. J Blood Med. 2011; 2: 59–69 [MEDLINE]
Time trends in pulmonary embolism in the United States: evidence of overdiagnosis. Arch Intern Med. 2011;171(9):831 [MEDLINE]
Influence of preceding length of anticoagulant treatment and initial presentation of venous thromboembolism on risk of recurrence after stopping treatment: analysis of individual participants’ data from seven trials. BMJ. 2011 May 24;342:d3036. doi: 10.1136/bmj.d3036 [MEDLINE]
Obesity and pulmonary embolism: the mounting evidence of risk and the mortality paradox. Thromb Res. 2011;128:518–523 [MEDLINE]
Impact of vena cava filters on in-hospital case fatality rate from pulmonary embolism. Am J Med. 2012 May;125(5):478-84. Epub 2012 Feb 4 [MEDLINE]
Factors in the technical quality of gadolinium enhanced magnetic resonance angiography for pulmonary embolism in PIOPED III. Int J Cardiovasc Imaging. 2012 Feb;28(2):303-12. doi: 10.1007/s10554-011-9820-7. Epub 2011 Feb 24 [MEDLINE]
A meta-analysis of anticoagulation for calf deep venous thrombosis. J Vasc Surg. 2012 Jul;56(1):228-37.e1; discussion 236-7. doi: 10.1016/j.jvs.2011.09.087. Epub 2011 Dec 29 [MEDLINE]
Use of Glucocorticoids and Risk of Venous Thromboembolism: A Nationwide Population-Based Case-Control Study. JAMA Intern Med. 2013 Apr 1:1-1 [MEDLINE]
Acute pulmonary embolism: external validation of an integrated risk stratification model. Chest 2013 Jun 13. doi: 10.1378/chest.12-2938 [MEDLINE]
Identification of intermediate-risk patients with acute symptomatic pulmonary embolism. Eur Respir J. 2014 Sep;44(3):694-703. doi: 10.1183/09031936.00006114. Epub 2014 Apr 2 [MEDLINE]
Vena cava filters in unstable elderly patients with acute pulmonary embolism. Am J Med. 2014 Mar;127(3):222-5 [MEDLINE]
2014 ESC guidelines on the diagnosis and management of acute pulmonary embolism. Eur Heart J. 2014;35(43):3033-3069, 3069a-3069 k [MEDLINE]
Non-steroidal anti-inflammatory drugs and risk of venous thromboembolism: a systematic review and meta-analysis. Rheumatology (Oxford). 2015 Apr;54(4):736-42. doi: 10.1093/rheumatology/keu408. Epub 2014 Sep 24 [MEDLINE]
Diagnostic prediction models for suspected pulmonary embolism: systematic review and independent external validation in primary care. BMJ. 2015;351:h4438 [MEDLINE]
Diagnosis
General
An official American Thoracic Society/Society of Thoracic Radiology clinical practice guideline: evaluation of suspected pulmonary embolism in pregnancy. Am J Respir Crit Care Med. 2011 Nov 15;184(10):1200-8. doi: 10.1164/rccm.201108-1575ST [MEDLINE]
Short-term clinical outcome of normotensive patients with acute PE and high plasma lactate. Thorax. 2015 Apr;70(4):333-8. doi: 10.1136/thoraxjnl-2014-206300 [MEDLINE]
Comparison of Guidelines for Evaluation of Suspected Pulmonary Embolism in Pregnancy: A Cost-effectiveness Analysis. Chest. 2022 Jun;161(6):1628-1641. doi: 10.1016/j.chest.2021.11.036 [MEDLINE]
The electrocardiographic manifestations of pulmonary embolism. J Emerg Med. 1988;6(4):301 [MEDLINE]
Clinical characteristics of patients with acute pulmonary embolism. Am J Cardiol. 1991;68(17):1723 [MEDLINE]
The ECG in pulmonary embolism. Predictive value of negative T waves in precordial leads–80 case reports. Chest. 1997;111(3):537 [MEDLINE]
Diagnostic value of the electrocardiogram in suspected pulmonary embolism. Am J Cardiol. 2000;86(7):807 [MEDLINE]
Prognostic value of the ECG on admission in patients with acute major pulmonary embolism. Eur Respir J. 2005;25(5):843 [MEDLINE]
Findings From 12-lead Electrocardiography That Predict Circulatory Shock From Pulmonary Embolism: Systematic Review and Meta-analysis. Acad Emerg Med. 2015 Oct;22(10):1127-37. Epub 2015 Sep 22 [MEDLINE]
New Electrocardiographic Changes in Patients Diagnosed with Pulmonary Embolism. J Emerg Med. 2017;52(3):280. Epub 2016 Oct 11 [MEDLINE]
The value of electrocardiography in prognosticating clinical deterioration and mortality in acute pulmonary embolism: A systematic review and meta-analysis. Clin Cardiol. 2017 Oct;40(10):814-824. doi: 10.1002/clc.22742. Epub 2017 Jun 19 [MEDLINE]
Prognostic significance of electrocardiogram at presentation in patients with pulmonary embolism of different severity. Thromb Res. 2018 Jan 31;163:123-127. doi: 10.1016/j.thromres.2018.01.025 [MEDLINE]
Hampton’s Hump. N Engl J Med. 2021 Oct 30. doi: 10.1056/NEJMicm2109756 [MEDLINE]
ANTELOPE Study. Embolus location affects the sensitivity of a rapid quantitative D-dimer assay in the diagnosis of pulmonary embolism. Am J Respir Crit Care Med. 2002;165(3):345 [MEDLINE]
D-dimer for the exclusion of acute venous thrombosis and pulmonary embolism: a systematic review. Ann Intern Med. 2004;140(8):589 [MEDLINE]
Potential of an age adjusted D-dimer cut-off value to improve the exclusion of pulmonary embolism in older patients: a retrospective analysis of three large cohorts. BMJ. 2010;340:c1475 [MEDLINE]
Assessment of the safety and efficiency of using an age-adjusted D-dimer threshold to exclude suspected pulmonary embolism. Chest. 2014;146(6):1444 [MEDLINE]
Age-adjusted D-dimer cutoff levels to rule out pulmonary embolism: the ADJUST-PE study. JAMA. 2014 Mar 19;311(11):1117-24. doi: 10.1001/jama.2014.2135 [MEDLINE]
An Age-Adjusted D-dimer Threshold for Emergency Department Patients With Suspected Pulmonary Embolus: Accuracy and Clinical Implications. Ann Emerg Med. 2016 Feb;67(2):249-57 [MEDLINE]
Age-Adjusted Cutoff D-Dimer Level to Rule Out Acute Pulmonary Embolism: A Validation Cohort Study. Am J Med. 2016 Aug;129(8):872-8 [MEDLINE]
D-dimer test for excluding the diagnosis of pulmonary embolism. Cochrane Database Syst Rev. 2016 Aug 5;(8):CD010864. doi: 10.1002/14651858.CD010864.pub2 [MEDLINE]
Wells Rule and d-Dimer Testing to Rule Out Pulmonary Embolism: A Systematic Review and Individual-Patient Data Meta-analysis. Ann Intern Med. 2016 Aug;165(4):253-61. Epub 2016 May 17 [MEDLINE]
A Test in Context: D-Dimer. J Am Coll Cardiol. 2017 Nov 7;70(19):2411-2420. doi: 10.1016/j.jacc.2017.09.024 [MEDLINE]
D-dimer Interval Likelihood Ratios for Pulmonary Embolism. Acad Emerg Med. 2017 Jul;24(7):832-837. doi: 10.1111/acem.13191. Epub 2017 Jun 14 [MEDLINE]
No added value of the age-adjusted D-dimer cut-off to the YEARS algorithm in patients with suspected pulmonary embolism. J Thromb Haemost. 2017;15(12):2317 [MEDLINE]
PEGeD Trial. Diagnosis of Pulmonary Embolism With d-Dimer Adjusted to Clinical Probability. N Engl J Med. 2019 Nov 28;381(22):2125-2134. doi: 10.1056/NEJMoa1909159 [MEDLINE]
Prognostic Value of Biomarkers in Acute Non-massive Pulmonary Embolism: A Systematic Review and Meta-analysis. Lung. 2015 Oct;193(5):639-51. doi: 10.1007/s00408-015-9752-4 [MEDLINE]
Right ventricular enlargement on chest computed tomography: prognostic role in acute pulmonary embolism. Circulation. 2004 May 25;109(20):2401-4. doi: 10.1161/01.CIR.0000129302.90476.BC [MEDLINE]
Overdiagnosis of Pulmonary Embolism by Pulmonary CT Angiography. AJR Am J Roentgenol. 2015 Aug;205(2):271-7. doi: 10.2214/AJR.14.13938 [MEDLINE]
Predictive Value of Computed Tomography in Acute Pulmonary Embolism: Systematic Review and Meta-analysis. Am J Med. 2015 Jul;128(7):747-59.e2. doi: 10.1016/j.amjmed.2015.01.023 [MEDLINE]
Yield of CT Pulmonary Angiography in the Emergency Department When Providers Override Evidence-based Clinical Decision Support. Radiology. 2016 Sep 30:151985 [MEDLINE]
Detection of Incidental Pulmonary Embolism on Conventional Contrast-Enhanced Chest CT: Comparison of an Artificial Intelligence Algorithm and Clinical Reports. AJR Am J Roentgenol. 2022 Jul 13. doi: 10.2214/AJR.22.27895 [MEDLINE]
Teaching Nonradiologists to Identify Right Heart Strain on Computed Tomography Scans of Acute Pulmonary Embolism. ATS Sch. 2022 Jun 30;3(2):175-179. doi: 10.34197/ats-scholar.2021-0128BR. eCollection 2022 Jun [MEDLINE]