Differences Between Cardiopulmonary Bypass and Extracorporeal Membrane Oxygenation (ECMO) (see Cardiopulmonary Bypass)
Cardiopulmonary Bypass is Equipped with Reservoir Into Which Blood from the Heart is Drained: allows a bloodless surgical field for valve and aortic operations
In Contrast, the ECMO Circuit Does Not Contain a Reservoir, So Blood Flow Needs to Be Continuous
Cardiopulmonary Bypass Can Be Utilized in Conjunction with Air Vent Tubing, Cardioplegia Line for Myocardial Preservation, or Cell Salvage Tubing
Requirement for Systemic Heparin Anticoagulation is Less Intense for ECMO Because Blood Flow is Continuous and There is No Blood-Air Interface in the Reservoir
Higher Flow Rates of >4 L/min are Used During ECMO (in Contrast to the Lower Flow Rates of 2 L/min Used During CPB)
However, Continuous Anticoagulation is Necessary to Prevent Thrombus Formation on the Synthetic Thrombogenic Surfaces of Both CPB and ECMO
ECMO Circuits are Designed for Longer-Term Use (May Be Used for Weeks, Depending on the Life of the Membrane Oxygenator), While CPB Use is Designed for Use for a Period of Hours
Indications
General Comments
Venovenous Extracorporeal Membrane Oxygenation (VV-ECMO) (Similar to Extracorporeal CO2 Removal, ECCO2R) Provides Only Respiratory Support: VV-ECMO is dependent on the patient’s intrinsic cardiac output
ECMO Had No Mortality Benefit in Treatment of ARDS Associated with Influenza
CESAR Trial of ECMO in the UK (Lancet, 2009) [MEDLINE]
ECMO Decreased Mortality Rate/Severe Disability at 6 Months
However, the Study was Flawed by Not Defining the Usual Care Group and ECMO Patients Were Concentrated in One Center in the Trial
Systematic Review and Meta-Analysis of ECMO in Adult Patients with ARDS (J Crit Care, 2013) [MEDLINE]
ECMO Had an Unclear Hospital Mortality Benefit: further studies were recommended
Cochrane Review of VV-ECMO and VA-ECMO in Critically Ill Adults (Cochrane Database Syst Rev, 2015) [MEDLINE]
ECMO Had No 6-Month (or Prior to 6 Month) All-Cause Mortality Benefit: low-moderate quality of evidence from trials
Study of the Long-Term Survival and Quality of Life Following ECMO (Eur J Cardiothorac Surg, 2017) [MEDLINE]
Survival to Discharge was Higher in the Non-ECMO Group, as Compared to the ECMO Group: however, this difference was not statistically significant after propensity score matching
One Year Survival was 67% in the Non-ECMO Group vs 60% in the ECMO Group
Two Year Survival was 50% in the Non-ECMO Group vs 45% in the ECMO Group
Single-Center Swedish Retrospective Study of Outcomes After ECMO for ARDS Associated with Sepsis (Crit Care Med, 2017) [MEDLINE]
Approximately 64% of ECMO Patients Survived to Discharge
High Mortality Rate Within the First Few Months After Discharge
Systematic Review and Meta-Analysis of Mortality and Complications with the Use of Venovenous ECMO in ARDS (Ann Intensive Care, 2017) [MEDLINE]
Mortality Rate at Hospital Discharge was 37.7%
Factors Associated with Increased Hospital Mortality
Age
Year of Study
Mechanical Ventilation and Prone Positioning Days Prior to ECMO
Systematic Review of Venovenous ECMO for ARDS (J Crit Care, 2017) [MEDLINE]: n = 27 studies
Mortality Benefit of ECMO is Unclear
French EOLIA Trial of VV-ECMO in Severe ARDS (NEJM, 2018) [MEDLINE]
Clinical Triggers for Randomization
pO2/FiO2 Ratio <50 mm Hg for >3 hrs
pO2/FiO2 Ratio <80 mm Hg for >6 hrs
Arterial Blood pH <7.25 with pCO2 ≥60 mm Hg for >6 hrs
VV-ECMO Did Not Improve the 60-Day Mortality in Severe ARDS, as Compared to Conventional Ventilator Management (with VV-ECMO as Rescue Therapy) (Relative Risk 0.76; 95% Confidence Interval 0.55 to 1.04; P = 0.09)
Crossover to ECMO Occurred a Mean (± SD) of 6.5 ± 9.7 Days After Randomization in 28% of Patients in the Control Group, with 57% of These Patients Dying
VV-ECMO Group Had Higher Rate Bleeding Events and Severe Thrombocytopenia, But Lower Rate of Ischemic Cerebrovascular Accidents
Criteria to Start Venovenous Extracorporeal Membrane Oxygenation (VV-ECMO)
French REVA (Reseau Europeen De Recherche En Ventilation Artificielle) Criteria (2009)
pO2/FiO2 Ratio <50 Despite High PEEP (10-20 cm H2O) and High FiO2 (>80%)
Plateau Pressure At Least 35 cm H2O Despite Decrease in Tidal Volume to 4 mL/kg
NEJM, 2011 Review of ECMO in ARDS Criteria [MEDLINE]
Severe Hypoxemia: pO2/FiO2 Ratio <80 Despite High PEEP (15–20 cm of H2O) for at Least 6 hrs in Patient with Potentially Reversible Respiratory Failure
Uncompensated Hypercapnia with Acidemia (pH <7.15) Despite the Optimized Ventilator Management
Excessively High Plateau Pressure (>35–45 cm of H2O, According to the Patient’s Body Size) Despite Optimized Ventilator Management
Extracorporeal Life Support Organization (ELSO) Criteria (Extracorporeal Life Support Organization (ELSO) Guidelines for Adult Respiratory Failure v1.3, 2013) [LINK]
pO2/FiO2 Ratio <150: ECMO should be considered
pO2/FiO2 Ratio <80: ECMO should be utilized
pCO2 >80 m Hg or Plateau Pressure >30 cm H2O: ECMO should be utilized
Contraindications
Absolute
Contraindication to Anticoagulation: although in patients with severe bleeding, anticoagulation can be held for limited periods of time
Any Condition or Organ Dysfunction that Would Limit the Likelihood of Overall Benefit from ECMO, Such as Severe, Irreversible Brain Injury or Untreatable Metastatic Cancer
High FiO2 Requirement >80% for >7 Days
High-Pressure Ventilation (Plateau Pressure >30 cm of H2O) for >7 Days
Limited Vascular Access
Physiology
Blood Flow Rate During VV-ECMO
Determinants of VV-ECMO Blood Flow Rate
Resistance to Flow in the Drainage Cannula
Maximal Flow for Commonly Used Venous Cannulas (at 100 cm H2O Suction): approximately 4-5 L/min
Suction Produced by the Pump or Siphon
Geometry of the Cannulated Vessel (Usually the Inferior Vena Cava or Right Atrium)
Oxygenation During VV-ECMO
Determinants of Oxygen Supply from the VV-ECMO Membrane
VV-ECMO Blood Flow Rate
Hemoglobin
Difference Between the Outlet Minus Inlet Oxygen Content
Because the Outlet Blood is Typically 100% Saturated and PO2 is >500 mm Hg, the Dissolved Oxygen Can Be as Much as 10% of the Oxygen Content
Major Determinants of Oxygenation During VV-ECMO
VV-ECMO Blood Flow Rate
Small Study of the Determinants of Oxygenation and CO2 Removal During VV-ECMO (Int Care Med, 2013) [MEDLINE]
Arterial Oxygenation was Determined by VV-ECMO Blood Flow Rate and ECMO FIO2
ECMO Blood Flow was the Main Determinant of Arterial Oxygenation
CO2 Elimination Depended on the Sweep Gas Flow Rate Through the Oxygenator
ECMO Blood Flow/Cardiac Output Ratio >60% was Associated with Adequate Blood Oxygenation
Packed Red Blood Cell Transfusion Increased O2 Delivery, Allowing Lower ECMO Flows to Reach an Adequate SaO2
VV-ECMO FIO2
Small Study of the Determinants of Oxygenation and CO2 Removal During VV-ECMO (Int Care Med, 2013) [MEDLINE]
Arterial Oxygenation was Determined by VV-ECMO Blood Flow Rate and ECMO FIO2
ECMO Blood Flow was the Main Determinant of Arterial Oxygenation
CO2 Elimination Depended on the Sweep Gas Flow Rate Through the Oxygenator
ECMO Blood Flow/Cardiac Output Ratio >60% was Associated with Adequate Blood Oxygenation
Packed Red Blood Cell Transfusion Increased O2 Delivery, Allowing Lower ECMO Flows to Reach an Adequate SaO2
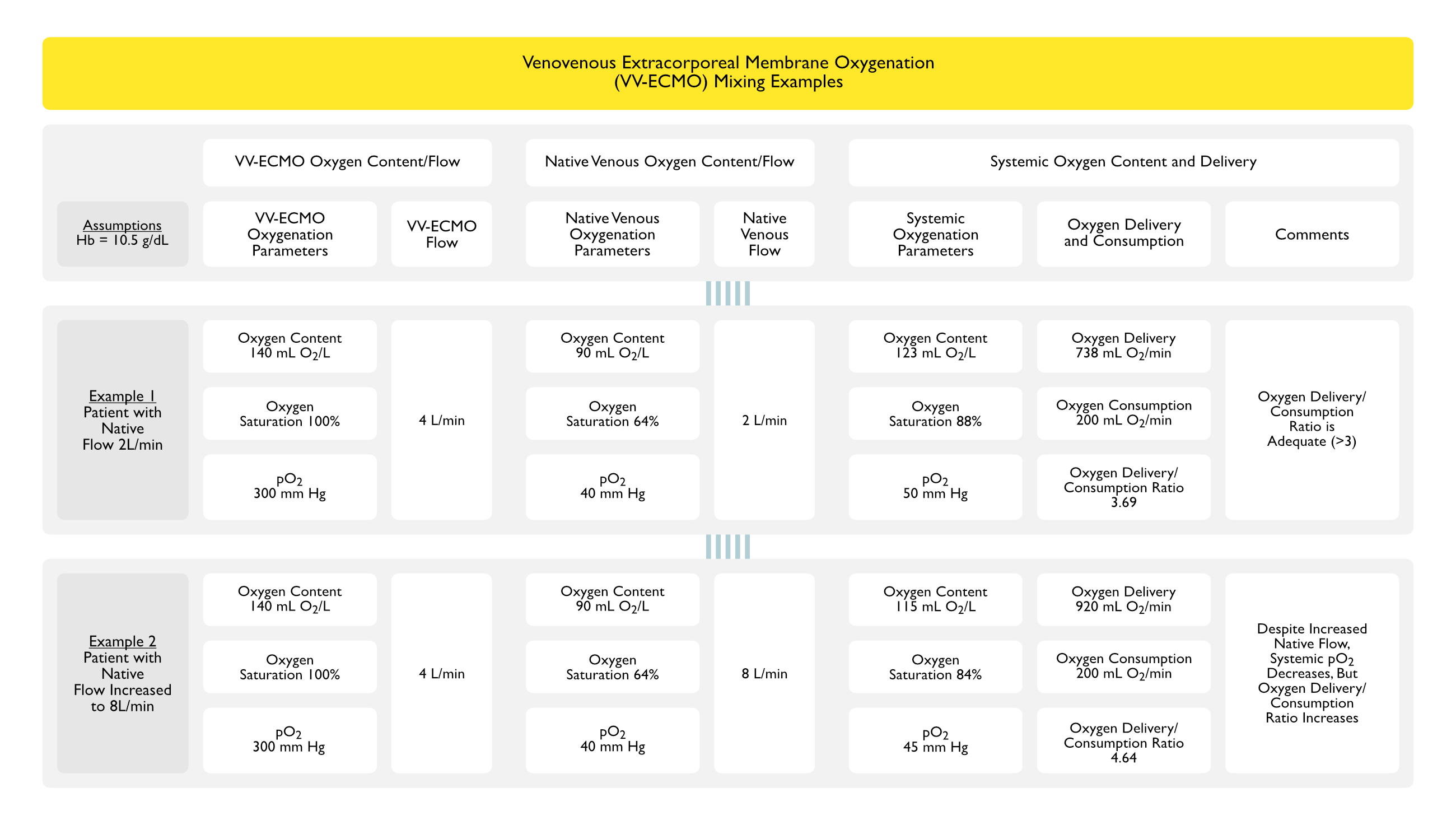
Mixture Between Venovenous Extracorporeal Membrane Oxygenation (VV-ECMO) Oxygenated Blood Flow and the Patient’s Native Venous Blood Flow
Background
In Severe ARDS with VV-ECMO, the Lungs Contribute Little or Nothing to Gas Exchange and the Oxygen Saturation and Carbon Dioxide Levels of the Blood in the Right Ventricle is the Summation of Mixing of Oxygenated ECMO Blood with Deoxygenated Native Venous Blood
Due to the Lack of Meaningful Lung Function, The Blood in the Right Ventricle Will Have the Same Oxygen Saturation and Carbon Dioxide Levels of the Blood on the Arterial Side of the Circulation
Mixing Point
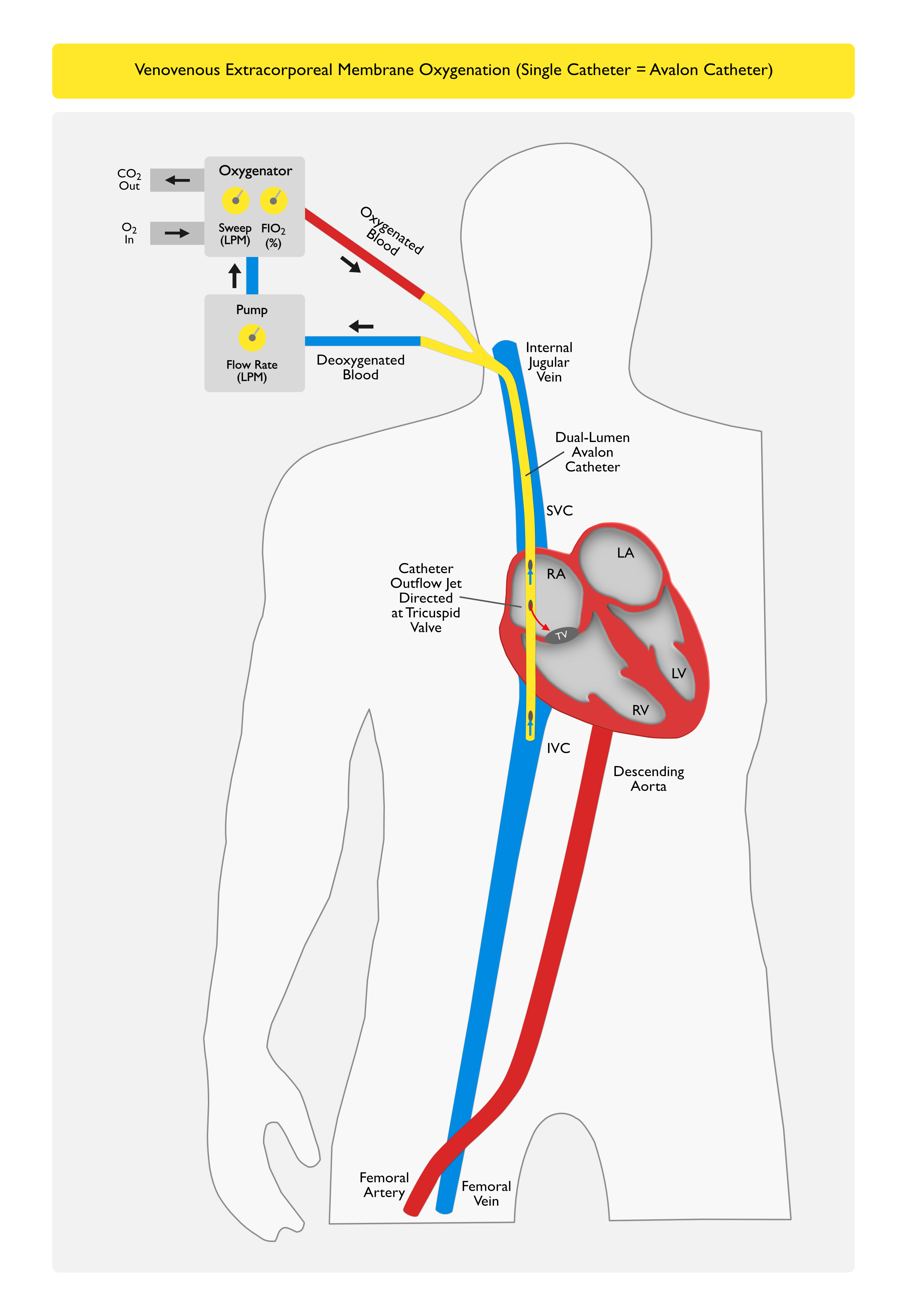
Single (Avalon Catheter, Crescent Catheter) Catheter Setup (Inserted Via the Right Internal Jugular Vein): mixing point occurs in the right atrium
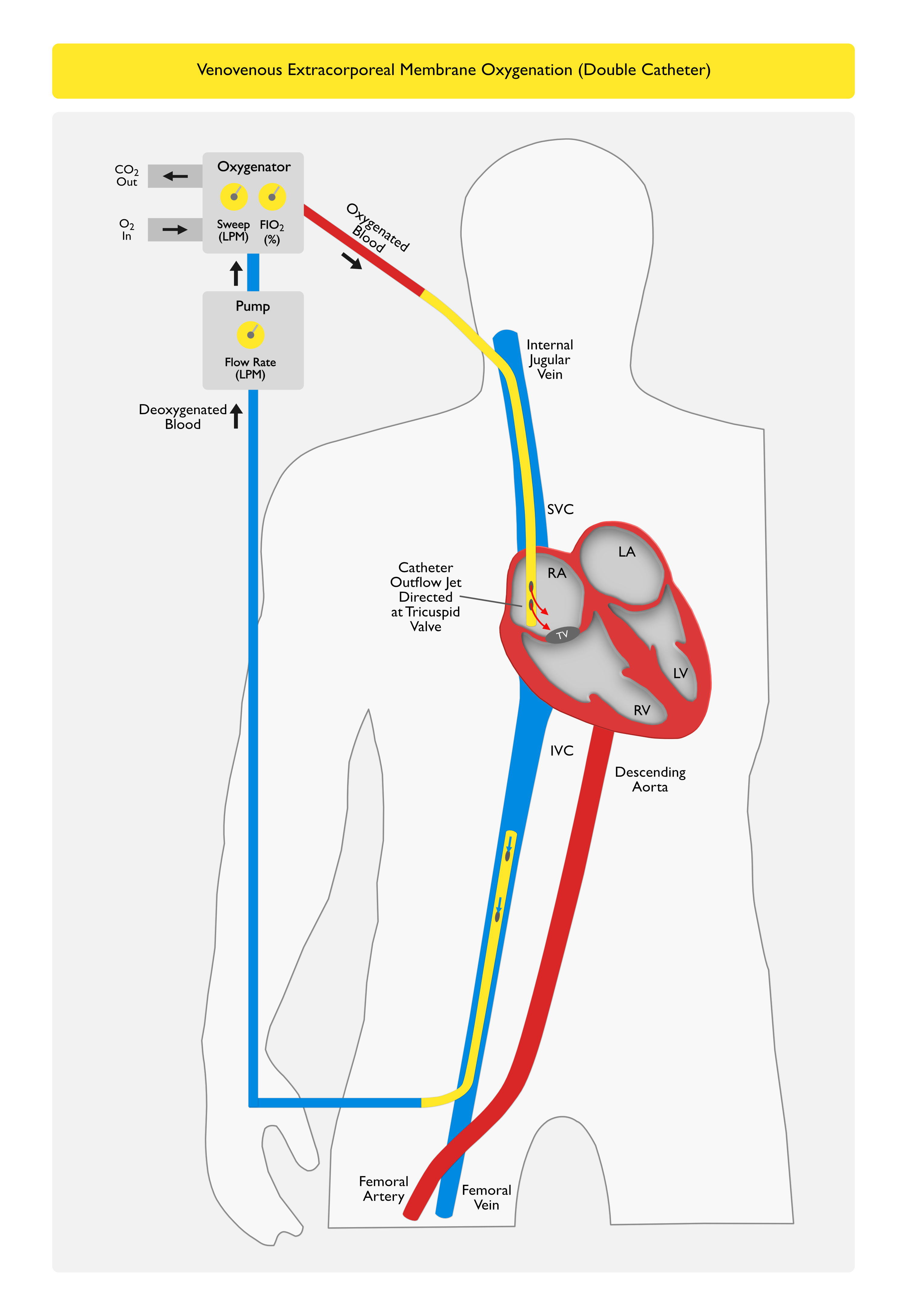
Double Catheter Setup
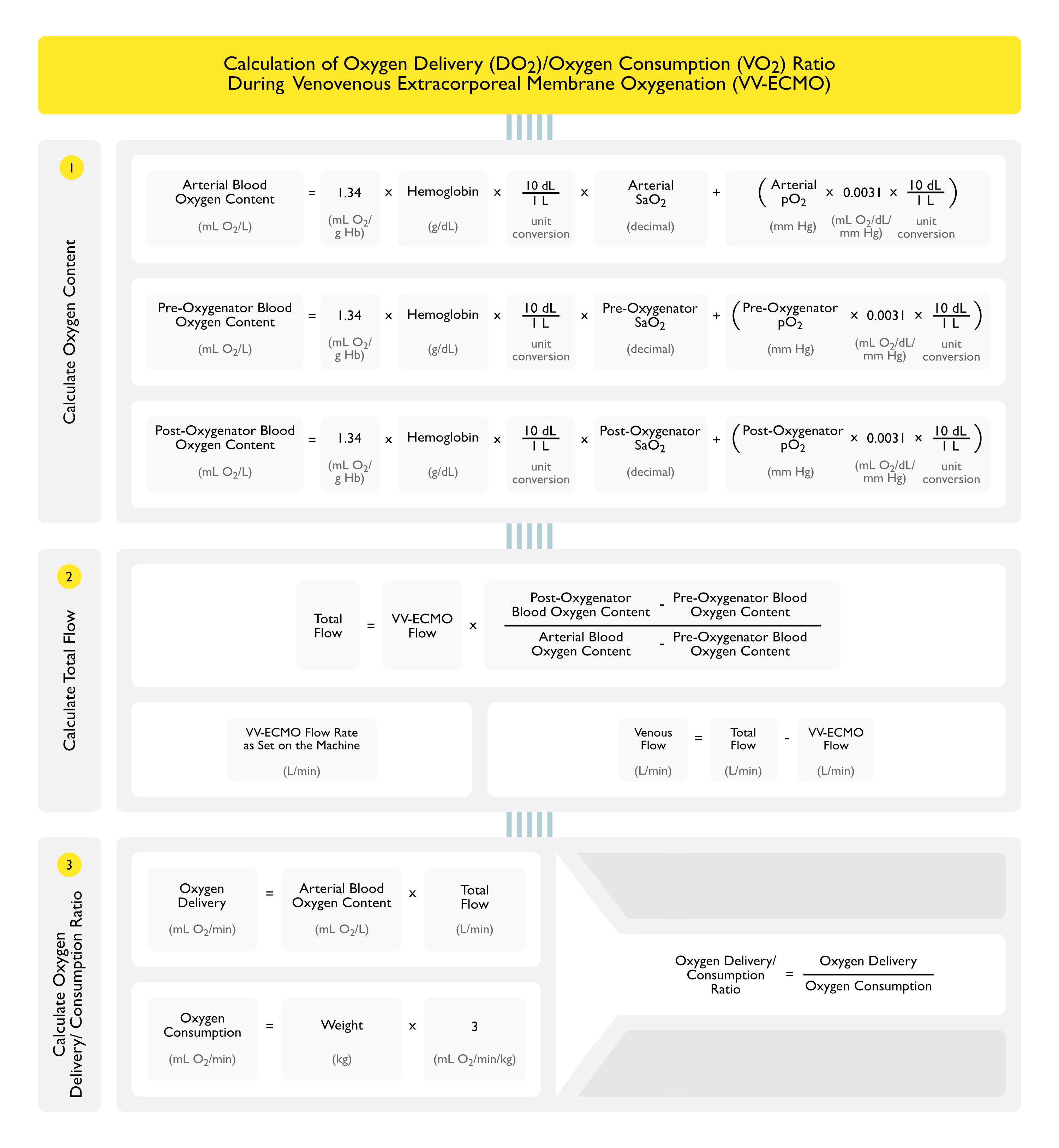
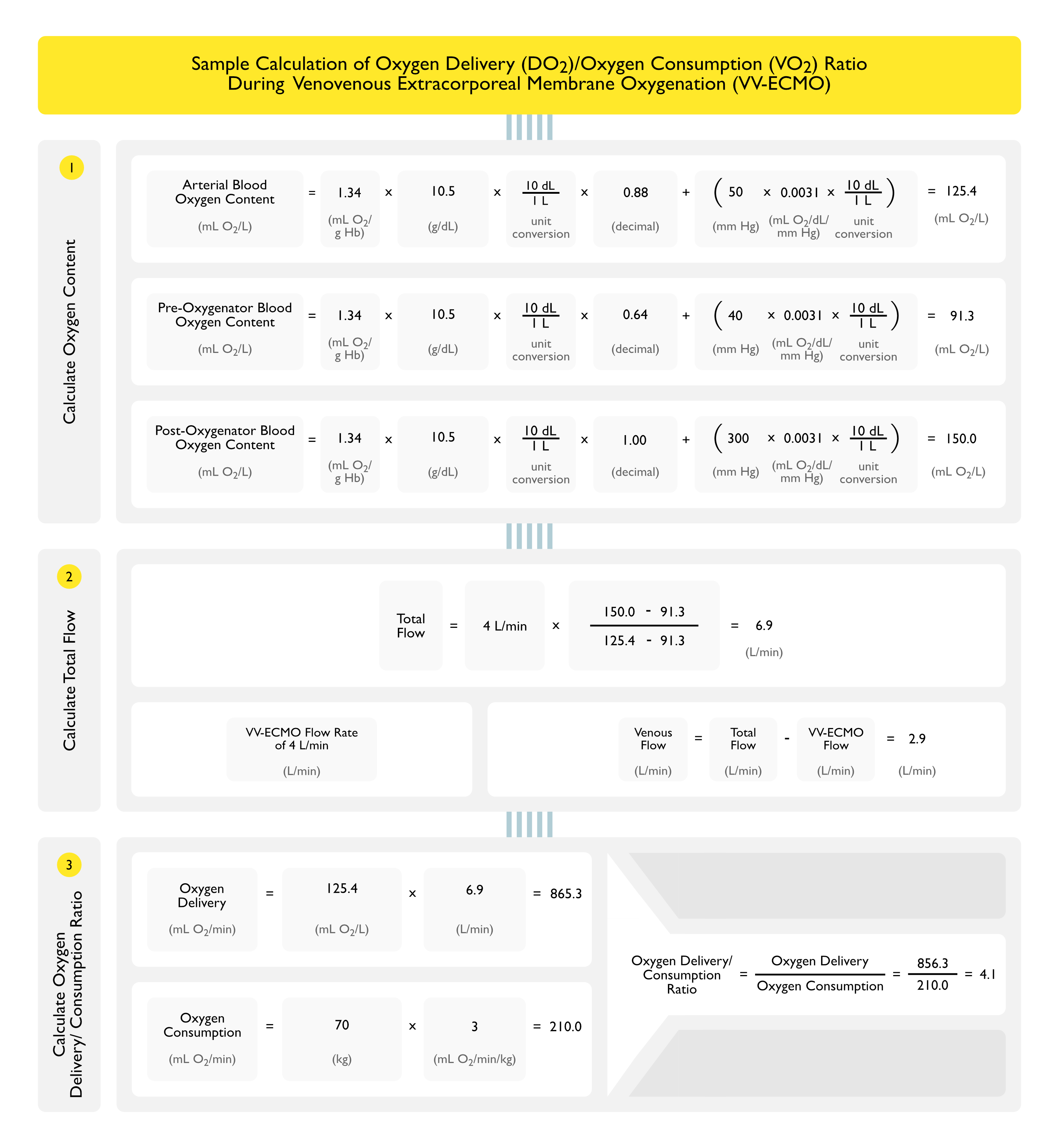
Calculation of the Oxygen Delivery/Oxygen Consumption Ratio
General Comments
Calculation of the Oxygen Delivery/Oxygen Consumption Ratio is a Standard Means to Determine if Oxygen Delivery is Adequate in Patient on VV-ECMO
This Calculation is Critical Since the Arterial pO2 May Be Significantly Lower than the pO2 of a Patient in ARDS Who is Not on VV-ECMO
These Low pO2 Values May Alarm Staff Who are Used to Meeting Specific pO2 Goals in Patients in ARDS
In a Patient on VV-ECMO, the Oxygen Delivery/Oxygen Consumption Ratio Goal is More Clinically Relevant (than the Arterial pO2) in Maintaining Tissue Oxygenation
Step 1: Calculation of Oxygen Content of Arterial Blood, Pre-Oxygenator (Venous) Blood, and Post-Oxygenator Blood
Arterial Oxygen Content = 13.4 x Hemoglobin x Arterial SaO2 + (Arterial pO2 x 0.031)
Pre-Oxygenator Oxygen Content = 13.4 x Hemoglobin x Pre-Oxygenator SaO2 + (Pre-Oxygenator pO2 x 0.031)
Post-Oxygenator Oxygen Content = 13.4 x Hemoglobin x Post-Oxygenator SaO2 + (Post-Oxygenator pO2 x 0.031)
Terms
Constant 13.4 mL O2/g Hb: accounts for the fact that 1.34 ml of O2 is carried per g of Hb (13.4 is used in the equation to correct the units from dL to L)
The Normal Oxygen Carrying Capacity is 1.39 ml O2 per g of Hb
However, Due to the Presence of Abnormal Hemoglobins (Such as Carboxyhemoglobin and Methemoglobin), this Value is Decreased to 1.34 ml O2 per g of Hb
Hemoglobin: in g/dL
SaO2: as decimal
pO2: in mm Hg
Constant 0.0031 mL O2/L/mm Hg: solubility coefficient of oxygen at body temperature
Step 2: Calculation of Flows
General Comments
When Two Blood Flows Containing Different Oxygen Contents Mix, the Resultant Oxygen Content is the Average of the Amount of Oxygen Content in Each of the Two Flows (Not the Average of the Partial Pressures of Oxygen, i.e. the pO2’s) (Extracorporeal Life Support: The ELSO Red Book (5th Edition, 2017) [LINK]
Total Oxygen Content = [(Post-Oxygenator Oxygen Content x VV-ECMO Flow)/Total Flow] + [(Pre-Oxygenator Oxygen Content x Native Venous Flow)/Total Flow]
Assumes No Native Lung Function
Solving for Total Flow (i.e. Total Cardiac Output)
Step 3: Calculation of Oxygen Delivery (DO2)/Oxygen Consumption (VO2) Ratio (see Hypoxemia)
Oxygen Delivery = [Arterial Oxygen Content] x CO = [Hb x 13.4 x SaO2 + (pO2 x 0.0031)] x CO
Hemoglobin (Hb): in g/dL
Constant 13.4: accounts for the fact that 1.34 ml of O2 is carried per g of Hb (13.4 is used in the equation to correct the units from dL to L)
Arterial Oxygen Saturation (SaO2): as a decimal
Thermodilution-Measured Cardiac Output (CO) (from Swan-Ganz Catheter, etc) or Flow: in L/min
Normal Arterial Oxygen Content: approximately 200 mL O2/L (or 20 mL O2/dL)
Note: the Equation Used Here Yields the Arterial Oxygen Content in mL O2/L, Which Allows the Arterial Oxygen Content Value to Be Plugged into the Oxygen Delivery Equation without Unit Conversion
Normal Oxygen Delivery (Using Cardiac Output = CO): approximately 1000 mL O2/min
Calculation of Approximate Oxygen Consumption
Oxygen Consumption = Weight (in kg) x 3 mL O2/kg/min
Calculation of the Oxygen Delivery (DO2)/Oxygen Consumption (VO2) Ratio
Recommendations (Extracorporeal Life Support: The ELSO Red Book (5th Edition, 2017) [LINK]
Maintain Oxygen Delivery/Oxygen Consumption Ratio >3
In Sepsis Where Cardiac Output is Typically Elevated, This 3:1 Ratio Can Only Be Maintained if Flow is Augmented
Factors Contributing to Hypoxemia During VV-ECMO (Excluding Equipment Failure)
Mixture Between ECMO Oxygenated Blood Flow and Patient’s Native Venous Blood Flow: as described above
Recirculation
Recirculation is Defined as the Fraction of Oxygenated Blood Which is Infused into the Right Atrium and Subsequently Aspirated Back into the Venous Limb of the ECMO Circuit
Factors Contributing to Recirculation
Cannula Type/Size
Cannula Position: catheter position can be most problematic with the use of a single (Avalon) catheter, where the inflow and outflow ports are in closer proximity than they are with a double catheter setup
This is the Main Mechanism of Hypoxemia in ARDS (Occurs Due to Alveolar Filling with Protein-Rich Fluid/Red Blood Cell/Neutrophils and Interstitial Changes)
Degree of Intrapulmonary Shunt is Related to Vascular Pressures, Vasoactive Medications/Substances, and Degree of Lung Inflation
Cardiac Output is Positively Correlated with the Degree of Intrapulmonary Shunt
Flow Exceeding Oxygenator Performance
Rarely Occurs with the Current Generation of Technology
Strategies to Improve Systemic Oxygenation During VV-ECMO
Increase Blood Oxygen Content
Increase ECMO Blood Flow Rate
In Some Cases, Increasing the Blood Flow Rate Will Not Improve Oxygenation, Due to Increased Recirculation
Higher Flow Rates Increase the Risk of Hemolysis (see Hemolytic Anemia): may occur when using high RPM with venous occlusion in the catheter (due to coughing, hypovolemia, catheter kinking, etc), resulting in a vacuum created in the pump head
Increase Hematocrit (Oxygen-Carrying Capacity)
The ECMO Oxygenator Functions Optimally at a Normal Hematocrit
ECMO Utilization is Blood Resource Intensive: due to the need for frequent PRBC transfusion related to both hemolysis/bleeding issues and the need to maintain a high hematocrit to increase oxygen delivery
Extracorporeal Life Support Organization (ELSO) Guidelines Recommend Maintaining a Hemoglobin of 12-14 g/dL with a Normal Hematocrit (v1.3 (2013) [LINK]: due to the fact that oxygen delivery is determined by blood flow through the artificial lung, and if anemia is present, a higher blood flow will be necessary to obtain the same level of oxygen delivery
While There are No Trials Examining Restrictive Transfusion Protocols in VV-ECMO, Data Suggest that Red Blood Transfusion is a Clinical Predictor of Mortality (Crit Care Med, 2005) [MEDLINE] and (Chest, 2007) [MEDLINE]
Esmolol Has Been Used to Decrease the Cardiac Output (in Patients with Cardiac Output >7 L/min), Improving the Ratio Between the Cardiac Output and the ECMO Blood Flow (Preventing the Need for Increases in the ECMO Blood Flow Rate): this treatment did not decrease the oxygen delivery (DO2)
Decreasing CO Also Decreases Intrapulmonary Shunt
Proning: while trials of combined proning and VV-ECMO have been performed, the efficacy of this strategy is unclear
Switch to Venoarterial ECMO (VA-ECMO) or Hybrid Configuration
Utilization of VA-ECMO Allows Complete Bypass of the Native Lung: allowing a strategy to manage refractory hypoxemia occurring during VV-ECMO
Arterial Catheterization Needs to Be as Close to the Heart as Possible to Avoid the “Harlequin Syndrome” (Blue Head and Red Legs): this occurs due to competition between the anterograde blood flow related to native cardiac output and ECMO flow delivered via a femoral cannula, resulting in compromised perfusion of the upper body
Technique
Equipment
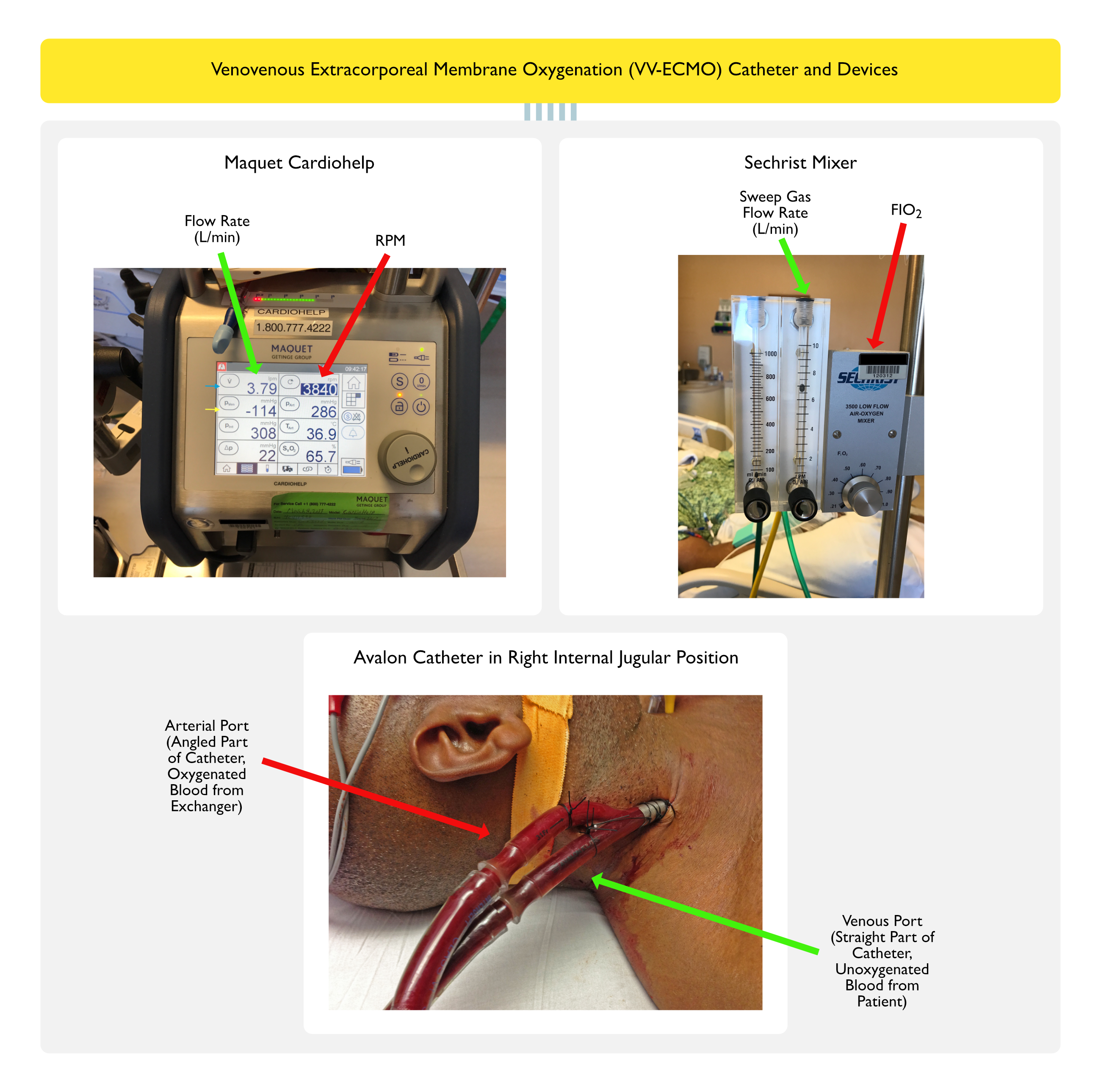
Maquet Cardiohelp
Centrifugal Pump (Constrained Vortex Pump)
Centrifugal Pump Moves Blood by Creating a Pressure Differential Across the Pump Head Which Contains a Magnetically Driven Impeller Spinning at Approximately 3000 RPM
Centrifugal Pumps Require Lower Levels of Anticoagulation than Roller Pumps
Centrifugal Pumps Result in Lesser Degree of Hemolysis than Roller Pumps
Centrifugal Pumps Exhibit an Increased Risk of Non-Surgical (Gastrointestinal, Pulmonary, and Neurological) Bleeding, as Compared to Roller Pumps, Despite Lower Levels of Heparin Anticoagulation (ASAIO J, 2015) [MEDLINE]
Duration of Use: Maquet Cardiohelp may be used for up to 30 days (per manufacturer recommendation)
Vascular Access
Requirement for Technical Support
Requires Continuous Monitoring by Technical Support Personnel (i.e. Perfusionist)
Avalon Catheter Placement into the Right Internal Jugular (IJ) Vein (Avalon Laboratory, Los Angeles, CA, USA)
Required Supplies
Arrow Dilator Kit
Avalon Catheter
Insertion and Set-Up
Procure Right Internal Jugular (IJ) Access
Insert Long Stiff Wire
Serial Grey Dilators
Insert Black Wire Sheath Over Wire
Serial Dilation of Tract with Blue Dilators Over Wire/Sheath (Both Remain in Place During Dilation)
Insert Avalon Catheter Over Wire: orient arterial port toward patient chin (this angles the arterial port toward the tricuspid valve)
Remove White Stylet from Avalon Catheter
Use Trans-Esophageal Echocardiogram (TEE) to Assure that Arterial Port is Angled Toward the Tricuspid Valve
After Avalon Catheter Placement, Immediately Give Heparin 10,000 units IV: to prevent Avalon catheter from clotting
Fill Avalon Catheter Lines with Saline: squirt into ends of catheter just to fill
Connect Straight Venous Port (Green Arrow in Photograph) to ECMO Machine: unoxygenated blood should be seen in this line
Connect the Angled Arterial Port (Red Arrow in Photograph) to ECMO Machine: oxygenated blood should be seen in this line
However, Anticoagulation May Be Held for Short Periods During EMCO (Using Heparin-Bonded Circuits)
Extracorporeal Life Support Organization (ELSO) Guidelines for Adult Respiratory Failure v1.3 (2013) [LINK]
Titrate Heparin Drip to Maintain ACT 180-200
Management (Extracorporeal Life Support Organization (ELSO) Guidelines for Adult Respiratory Failure v1.3, 2013) [LINK]
Adjustments To Increase the Arterial pO2
Increase ECMO Circuit Blood Flow Rate (Green Arrow in First Panel Photograph)
This Represent the Blood Flow Rate through the Exchanger
Start with 50-80 ml/Dry Weight/min (Approximately 3.5-5.6 L/min for a 70 kg Patient): this will achieve a DO2 of approximately 3 mL/kg/min (assuming a cardiac output of 5 L/min and hemoglobin concentration of 15 g/dL)
Start with the Maximum End of This Range Initially, Then Decrease to Lowest Blood Flow Rate to Maintain SaO2 >80-85% (at Resting Vent Settings)
Arterial pO2 Will Be 45-55 mm Hg in this Scenario: the lower limit of pO2 below which brain injury may occur during VV-ECMO is unknown (ASAIO J, 2015) [MEDLINE]
Note that the Compensatory Increase in Cardiac Output Which Occurs and Transfusion to Achieve a Hematocrit >40% Will Ensure Adequate Oxygen Delivery (DO2)
Goal DO2:VO2 Ratio >3 (Corresponds to an SvO2 Which is 25-30% Less than the SaO2)
Total DO2 = Patient Lung DO2 + Circuit DO2
Circuit DO2 = Flow x Outlet-Inlet O2 Content
VO2 = 3 ml/kg/min
The Ability to Achieve a Specific Blood Flow Rate Will Depend on the Vascular Access Characteristics, Drainage Tubing Resistance, and Pump Properties
Typical Pven (Venous Limb Pressure, Yellow Airway in Photograph) is Approximately -70 mm Hg (Example: -140 mm Hg Indicates an Excessively High Negative Pressure in Venous Limb of the Avalon Catheter, Which Might Prevent an Increase in the Blood Flow)
Increase Sweep Gas FIO2 (Red Arrow in Second Panel Photograph)
Adjustments To Change the Arterial pCO2
Maintain Arterial pCO2 at 40 mm Hg by Altering the Sweep Gas Flow Rate (Green Arrow in Second Panel Photograph): oxygen flow rate through exchanger (range: 1-10 L/min)
Increase in Sweep Gas Flow Rate Will Decrease the Arterial pCO2: functions similarly to the minute ventilation (VE) on the ventilator
Decrease in Sweep Gas Flow Rate Will Increase the Arterial pCO2: functions similarly to the minute ventilation (VE) on the ventilator
Sweep Gas Flow Rate is Usually 1:1 with the ECMO Blood Flow Rate
However, Sweep Gas Flow Rate Can Be Decreased to as Low as 1 L/min to Increase the Arterial pCO2
However, Sweep Gas Flow Rate Can Be Increased to as High as 10-15 L/min to Decrease the Arterial pCO2
Maintenance of a Near-Normal Hematocrit
Maintain Hemoglobin 12-14 g/dL (with a Normal Hematocrit)
Extracorporeal Life Support Organization (ELSO) Guidelines Recommend Maintaining a Hemoglobin of 12-14 g/dL with a Normal Hematocrit (v1.3 (2013) [LINK]
Due to the Fact that Oxygen Delivery (DO2) is Determined by Blood Flow Through the Artificial Lung, and if Anemia is Present, a Higher Blood Flow Rate Will Be Necessary to Obtain the Same Level of Oxygen Delivery (DO2)
Ventilator Management During Venovenous Extracorporeal Membrane Oxygenation (VV-ECMO)
Optimal Ventilator Management During ECMO is Unknown
Rationale is to Use Adequate Tidal Volume to Prevent Lung Atelectasis and Use Low Respiratory Rate to Prevent Ventilator-Induced Lung Injury
Suggested Settings (Same as Used in the CESAR Trial)
Turn Down Ventilator Settings Gradually, While Monitoring Serial Arterial Blood Gases (ABG’s)
Pressure Control Ventilation (PCV) with RR 10, PIP 20-25 cm H2O (with Tidal Volume <4 mL/kg PBW), PEEP +10-15, and FiO2 30%
Addition of Prone Positioning to Venovenous Extracorporeal Membrane Oxygenation (VV-ECMO) Therapy
Clinical Efficacy
Systematic Review of Prone Positioning as Add-On Therapy to VV-ECMO (Respir Care. 2016) [MEDLINE]
Addition of Prone Positioning to VV-ECMO Had Unclear Benefit
Risk of Hemodynamic Instability and Catheter Dislodgment Were Low
Use of Combination Continuous Venovenous Hemodialysis (CVVHD) with Venovenous Extracorporeal Membrane Oxygenation (VV-ECMO)
Clinical Efficacy
The Pulmonary and Renal Support in Acute Respiratory Distress Syndrome Study (Crit Care Med. 2015) [MEDLINE]
Combination CVVHD and ECMO is Safe and Effective
Oxygenator Blood Flow Rate was 410 +/= 30 mL/min (Around 10% of Cardiac Output): at these low flow rates, oxygenation would be expected to be minimal (due to the low blood flow rate) and CO2 removal would be around 20-30% of total CO2 production (since sweep gas flow rate could remain at an adequate level)
Monitoring of Arterial Oxygen Saturation and pO2 During Venovenous Extracorporeal Membrane Oxygenation (VV-ECMO)
During VV-EMCO, the Arterial Oxygen Saturation Typically Ranges from 60-90%, Depending on the Relative Amount of ECMO Blood Flow, Native Venous Blood Flow, Lung Function, and Cardiac Output
This Desaturated Arterial Blood Results in Normal Systemic Levels of Oxygen Delivery as Long as the Cardiac Output and Hemoglobin Concentration (i.e. Arterial Oxygen Content) are Adequate
This Observation May Be Confusing to ICU Staff, Since the Usual Goal of Management is to Keep the Arterial Oxygen Saturation >90%
Higher Flow Rates Increase the Risk of Hemolysis (see Hemolytic Anemia): may occur when using high RPM with venous occlusion in the catheter (due to coughing, hypovolemia, catheter kinking, etc), resulting in a vacuum created in the pump head
Hemorrhage
Cannulation-Site Hemorrhage
Cannulation-Site Hemorrhage Accounts for 17.1% of Adverse Events
Platelet Consumption in ECMO Circuit: due to fibrin stranding in oxygenator
Thrombosis
Thrombosis in Oxygenator
Epidemiology
Thrombosis in the Oxygenator Accounts for 12.2% of Adverse Events
Thrombosis in Other Circuit
Epidemiology
Thrombosis in Other Circuit Accounts for 17.8% of Adverse Events
Prognosis
Taiwanese Study of ECMO Outcomes from 2002-2012 Associated with Coronary Artery Bypass Graft Surgery, Myocardial Infarction/Cardiogenic Shock, Trauma, and Infection/Septic Shock (Circulation, 2016) [MEDLINE]
Mean±SD age of the 4227-patient cohort was 57±17 years, and 72% were male
The overall mortalities were 59.8% and 76.5% at 1 month and 1 year
Survival statistics deteriorated sharply when ECMO was required for >3 days
Acute (30-day) survival was more favorable in the infection/septic shock (n=1076; hazard ratio, 0.61; 95% confidence interval, 0.55–0.67), coronary artery bypass graft surgery (n=1077; hazard ratio, 0.68; 95% confidence interval, 0.61–0.75), and Trauma (n=369, hazard ratio, 0.82; 95% confidence interval, 0.70–0.95) groups
The extended survival rapidly approached an asymptote near 20% for the infection/septic shock, myocardial infarction/cardiogenic shock (n=1705), and coronary artery bypass graft surgery groups
The pattern of survival for the Trauma group was somewhat better, exceeding 30% at year-end
References
General
Extracorporeal membrane oxygenation in severe acute respiratory failure. A randomized prospective study. JAMA. 1979 Nov 16;242(20):2193-6 [MEDLINE]
Low-frequency positive-pressure ventilation with extracorporeal CO2 removal in severe acute respiratory failure. JAMA. 1986;256(7):881-886 [MEDLINE]
Randomized clinical trial of pressure-controlled inverse ratio ventilation and extracorporeal CO2 removal for adult respiratory distress syndrome. Am J Respir Crit Care Med. 1994 Feb;149(2 Pt 1):295-305 [MEDLINE]
Clinical predictors of and mortality in acute respiratory distress syndrome: potential role of red cell transfusion. Crit Care Med 33: 1191–1198, 2005 [MEDLINE]
Association of RBC transfusion with mortality in patients with acute lung injury. Chest 132: 1116–1123, 2007 [MEDLINE]
Venoarterial extracorporeal membrane oxygenation for treatment of cardiogenic shock: clinical experiences in 45 adult patients. J Thorac Cardiovasc Surg. 2008;135(2):382–388 [MEDLINE]
Outcomes and long-term quality-of-life of patients supported by extracorporeal membrane oxygenation for refractory cardiogenic shock. Crit Care Med. 2008;36:1404–1411 [MEDLINE]
Review of ECMO (extra corporeal membrane oxygenation) support in critically ill adult patients. Heart Lung Circ 2008;17:S41–S47. doi: 10.1016/j.hlc.2008.08.009. Epub 2008 Oct 29 [MEDLINE]
Extracorporeal Life Support Organization (ELSO). Patient Specific Supplements to the ELSO General Guidelines, 2009. https://square.umin.ac.jp/jrcm/pdf/ecmo/ecmotext12.pdf
Efficacy and economic assessment of conventional ventilatory support versus extracorporeal membrane oxygenation for severe adult respiratory failure (CESAR): a multicentre randomised controlled trial. Lancet. 2009 Oct 17;374(9698):1351-63 [MEDLINE]
Extracorporeal Membrane Oxygenation for 2009 Influenza A (H1N1) Acute Respiratory Distress Syndrome. JAMA. 2009 Nov 4;302(17):1888-95 [MEDLINE]
Extracorporeal Life Support Organization. Patient specific guidelines: a supplement to the ELSO general guidelines. April 2009:15-19 (https://www.elso.med.umich .edu/WordForms/ELSO%20P+%20Specif ic %20Guidelines.pdf)
Early and intermediate results of rescue extracorporeal membrane oxygenation in adult cardiogenic shock. Ann Thorac Surg. 2009;88(6):1897–1903 [MEDLINE]
Extracorporeal membrane oxygenation in nonintubated patients as bridge to lung transplantation. Am J Transplant 2010;10:2173–2178 [MEDLINE]
A review of the fundamental principles and evidence base in the use of extracorporeal membrane oxygenation (ECMO) in critically ill adult patients. J Intensive Care Med. 2011;26:13– 26. doi: 10.1177/0885066610384061 [MEDLINE]
Extracorporeal membrane oxygenation for ARDS in adults. N Engl J Med. 2011;365:1905–1914 [MEDLINE]
Extracorporeal membrane oxygenation for respiratory failure in adults. Curr Opin Crit Care Med. 2012;18:99–104 [MEDLINE]
Venovenous extracorporeal membrane oxygenation in adults: Practical aspects of circuits, cannulae, and procedures. J Cardiothorac Vasc Anesth 2012;26:893–909 [MEDLINE]
Venoarterial extracorporeal membrane oxygenation support for refractory cardiovascular dysfunction during severe bacterial septic shock. Crit Care Med. 2013 Jul;41(7):1616-26. doi: 10.1097/CCM.0b013e31828a2370 [MEDLINE]
Extracorporeal membrane oxygenation for severe respiratory failure in adult patients: a systematic review and meta-analysis of current evidence. J Crit Care. 2013 Dec;28(6):998-1005. doi: 10.1016/j.jcrc.2013.07.047. Epub 2013 Aug 16 [MEDLINE]
Extracorporeal Life Support Organization (ELSO) Guidelines for Adult Respiratory Failure v1.3 (2013) [LINK]
Blood oxygenation and decarboxylation determinants during veno-venous ECMO for respiratory failure in adults. Int Care Med. 2013;39(5):838-846 [MEDLINE]
Use of extracorporeal membrane oxygenation in adults. Heart Lung Circ. 2014;23(1):10-23 [MEDLINE]
Extracorporeal life support devices and strategies for management of acute cardiorespiratory failure in adult patients: a comprehensive review. Crit Care. 2014;18(3):219–229 [MEDLINE]
Mechanical ventilation during extracorporeal membrane oxygenation. Crit Care. 2014 Jan 21;18(1):203. doi: 10.1186/cc13702 [MEDLINE]
Extracorporeal membrane oxygenation for critically ill adults. Cochrane Database Syst Rev. 2015 Jan 22;1:CD010381. doi: 10.1002/14651858.CD010381.pub2 [MEDLINE]
Safety and efficacy of combined extracorporeal CO2 removal and renal replacement therapy in patients with acute respiratory distress syndrome and acute kidney injury: The Pulmonary and Renal Support in Acute Respiratory Distress Syndrome Study. Crit Care Med. 2015;43(12):2570-2581 [MEDLINE]
Roller and Centrifugal Pumps: A Retrospective Comparison of Bleeding Complications in Extracorporeal Membrane Oxygenation. ASAIO J. 2015 Sep-Oct;61(5):496-501. doi: 10.1097/MAT.0000000000000243 [MEDLINE]
A novel, highly efficient extracorporeal CO2 removal technique. Am J Respir Crit Care Med. 2015;192(6):719-726 [MEDLINE]
Extracorporeal membrane oxygenation in adults with cardiogenic shock. Circulation. 2015;131(7): 676–680 [MEDLINE]
Contemporary extracorporeal membrane oxygenation therapy in adults: Fundamental principles and systematic review of the evidence. J Thorac Cardiovasc Surg. 2016 Jul;152(1):20-32. doi: 10.1016/j.jtcvs.2016.02.067. Epub 2016 Mar 12 [MEDLINE]
Management of refractory hypoxemia during venovenous extracorporeal membrane oxygenation for ARDS. ASAIO J. 2015 May-Jun;61(3):227-36. doi: 10.1097/MAT.0000000000000207 [MEDLINE]
Complications of Prone Positioning During Extracorporeal Membrane Oxygenation for Respiratory Failure: A Systematic Review. Respir Care. 2016 Feb;61(2):249-54. doi: 10.4187/respcare.03882. Epub 2015 Oct 13 [MEDLINE]
Long-term survival and quality of life after extracorporeal life support: a 10-year report. Eur J Cardiothorac Surg. 2017 May 18. doi: 10.1093/ejcts/ezx100 [MEDLINE]
Long-Term Survival in Adults Treated With Extracorporeal Membrane Oxygenation for Respiratory Failure and Sepsis. Crit Care Med, 2017 Feb;45(2):164-170. doi: 10.1097/CCM.0000000000002078 [MEDLINE]
Systematic review and meta-analysis of complications and mortality of venovenous extracorporeal membrane oxygenation for refractory acute respiratory distress syndrome. Ann Intensive Care. 2017 Dec;7(1):51. doi: 10.1186/s13613-017-0275-4. Epub 2017 May 12 [MEDLINE]
Extracorporeal membrane oxygenation (ECMO) as a treatment strategy for severe acute respiratory distress syndrome (ARDS) in the low tidal volume era: A systematic review. J Crit Care. 2017 Apr 27;41:64-71. doi: 10.1016/j.jcrc.2017.04.041 [MEDLINE]
Fifty Years of Research in ARDS. Is Extracorporeal Circulation the Future of Acute Respiratory Distress Syndrome Management? Am J Respir Crit Care Med. 2017 May 1;195(9):1161-1170. doi: 10.1164/rccm.201701-0217CP [MEDLINE]
Extracorporeal Life Support: The ELSO Red Book (5th Edition, 2017) [LINK]
Indications
EOLIA Trial. Extracorporeal Membrane Oxygenation for Severe Acute Respiratory Distress Syndrome. N Engl J Med. 2018 May 24;378(21):1965-1975. doi: 10.1056/NEJMoa1800385 [MEDLINE]
ECMO for Severe Acute Respiratory Distress Syndrome. N Engl J Med. 2018 Sep 13;379(11):1090. doi: 10.1056/NEJMc1808731 [MEDLINE]
ECMO for Severe Acute Respiratory Distress Syndrome. N Engl J Med. 2018 Sep 13;379(11):1090-1. doi: 10.1056/NEJMc1808731 [MEDLINE]
ECMO for Severe Acute Respiratory Distress Syndrome. N Engl J Med. 2018 Sep 13;379(11):1091. doi: 10.1056/NEJMc1808731 [MEDLINE]
Learning from a Trial Stopped by a Data and Safety Monitoring Board. N Engl J Med. 2018 May 24;378(21):2031-2032. doi: 10.1056/NEJMe1805123 [MEDLINE]
ECMO for Severe ARDS. N Engl J Med. 2018 May 24;378(21):2032-2034. doi: 10.1056/NEJMe1802676 [MEDLINE]
Prognosis
Survival Analysis After Extracorporeal Membrane Oxygenation in Critically Ill Adults: A Nationwide Cohort Study. Circulation. 2016 Jun 14;133(24):2423-33. doi: 10.1161/CIRCULATIONAHA.115.019143 [MEDLINE]