Differences Between Cardiopulmonary Bypass and Extracorporeal Membrane Oxygenation (ECMO) (see Cardiopulmonary Bypass, [[Cardiopulmonary Bypass]])
Cardiopulmonary Bypass is Equipped with Reservoir Into Which Blood from the Heart is Drained: allows a bloodless surgical field for valve and aortic operations
In Contrast, the ECMO Circuit Does Not Contain a Reservoir, So Blood Flow Needs to Be Continuous
Cardiopulmonary Bypass Can Be Utilized in Conjunction with Air Vent Tubing, Cardioplegia Line for Myocardial Preservation, or Cell Salvage Tubing
Requirement for Systemic Heparin Anticoagulation is Less Intense for ECMO Because Blood Flow is Continuous and There is No Blood-Air Interface in the Reservoir
Higher Flow Rates of >4 L/min are Used During ECMO (in Contrast to the Lower Flow Rates of 2 L/min Used During CPB)
However, Continuous Anticoagulation is Necessary to Prevent Thrombus Formation on the Synthetic Thrombogenic Surfaces of Both CPB and ECMO
ECMO Circuits are Designed for Longer-Term Use (May Be Used for Weeks, Depending on the Life of the Membrane Oxygenator), While CPB Use is Designed for Use for a Period of Hours
Indications
General Comments
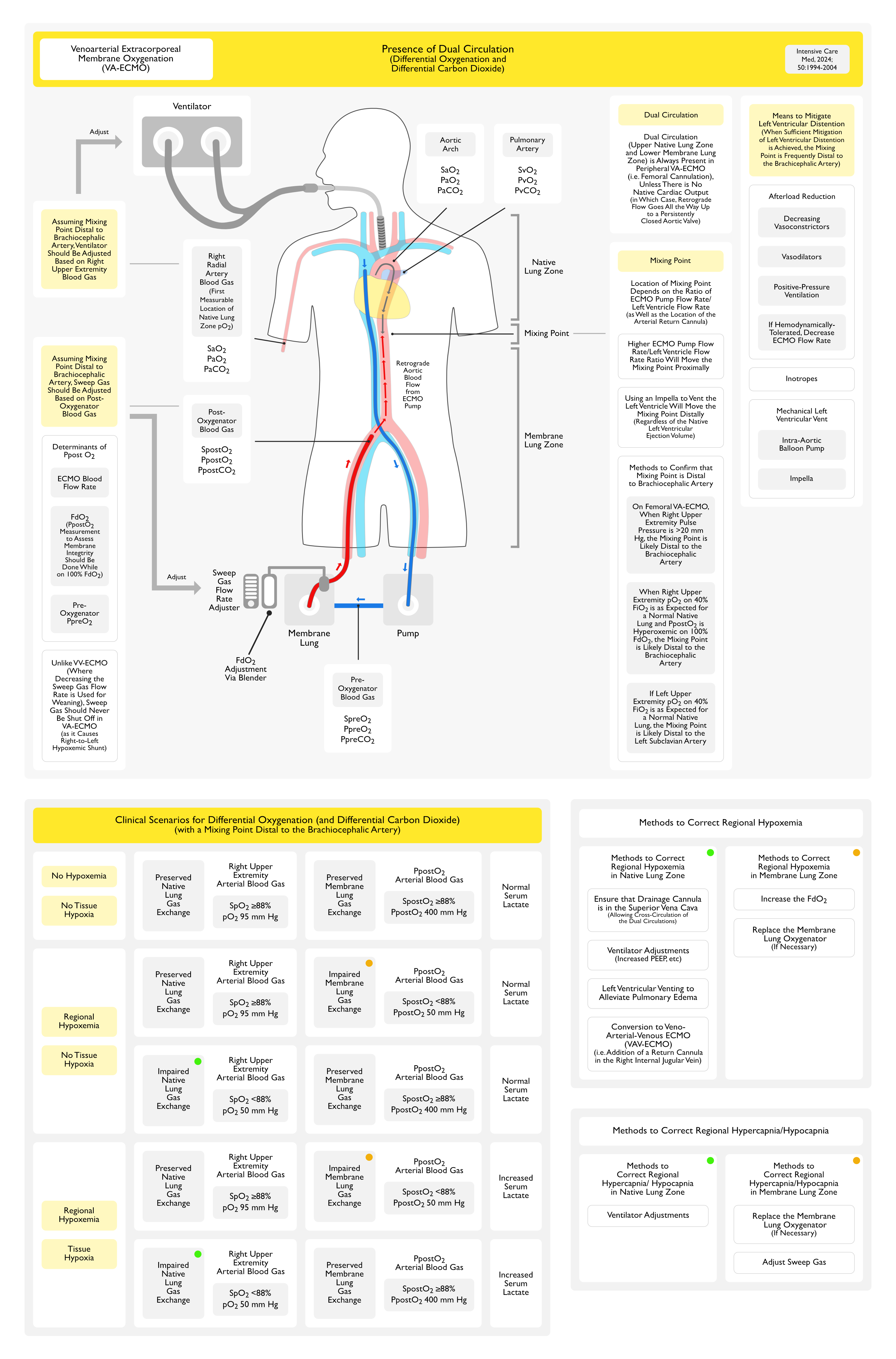
Venoarterial Extracorporeal Membrane Oxygenation (VA-ECMO) Provides Both Respiratory and Hemodynamic Support (see Cardiac Assist Devices, [[Cardiac Assist Devices]]): VA-ECMO does not depend on the patient’s intrinsic cardiac output
Provides full cardiopulmonary support (hemodynamic support + oxygenation of venous blood) analogous to that provided by cardiopulmonary bypass during cardiac surgery
Mainly Used in the Cardiac Catheterization Laboratory: mainly due to the requisite delay between the acute event and achievement of full cardiopulmonary support
Pump Characteristics: pumps can usually generate up to 8-10 L/min of flow (with flow rates being generally limited by venous preload and cannula size)
Requirement for Continuous Technical Support (On-Site Perfusionist)
Duration of Use: may be used for up to 30 days
Systems
Bard Cardiopulmonary Support (CPS): requires placement of large bore catheters with tips positioned in the aorta and right atrium
Blood from the venous catheter is pumped through a heat exchanger/oxygenator and returned to the systemic arterial circulation via the arterial cannula
MagLev Centrifugal Pump in Combination with Long-Term Oxygenators (CentraMag plus Maquet Quadrox)
Maquet CardioHelp
Maquet Rotaflow
Duration of Use: XXXXX
Vascular Access
Venous Catheter in Inferior Vena Cava or Right Atrium (Long Catheter): venous blood is removed from the patient
Arterial Catheter in Femoral Artery (Short Catheter): oxygenated blood is delivered retrograde up the descending aorta and into the ascending aorta to assure delivery to the coronary arteries and great vessels
If the Left Ventricular Cardiac Output is Negligible: the required extracorporeal flow will be low
As the Left Ventricular Cardiac Output Recovers and Cardiac Output Increases: the required extracorporeal flow will need to increase
In this case, anterograde aortic flow will compete with retrograde flow from the femoral arterial cannula, and a mixing zone of anterograde deoxygenated (in patients with respiratory failure) and retrograde oxygenated blood flow will occur: the flow required to assure that this mixing zone remains in the ascending aorta will increase as the native CO increases
Monitoring pulse oximetry from the right upper extremity or arterial blood gases from the right radial artery will elucidate whether VA-ECMO is providing adequate cerebral (although not necessarily cardiac) oxygenation
Ischemic Cerebrovascular Accident (CVA) (see Ischemic Cerebrovascular Accident, [[Ischemic Cerebrovascular Accident]]): stroke rates have been reported to be as high as 8% (Crit Care Med, 2008) [MEDLINE]
Local Arterial or Venous Complications: improving technique has decreased the vascular complication rate to approximately 1.4% of cases
Lower Limb Ischemia (see Acute Limb Ischemia, [[Acute Limb Ischemia]]): this risk can decreased by using a small anterograde perfusion cannula in the supercial femoral artery, to perfuse the leg distal to the femoral arterial cannula
Other Mechanical Complications
Oxygenator Failure
Thrombosis: second most common complication (occurs in 17% of cases)
Platelet Consumption in ECMO Circuit: due to fibrin stranding in oxygenator
References
Extracorporeal membrane oxygenation in severe acute respiratory failure. A randomized prospective study. JAMA. 1979 Nov 16;242(20):2193-6 [MEDLINE]
Low-frequency positive-pressure ventilation with extracorporeal CO2 removal in severe acute respiratory failure. JAMA. 1986;256(7):881-886 [MEDLINE]
Randomized clinical trial of pressure-controlled inverse ratio ventilation and extracorporeal CO2 removal for adult respiratory distress syndrome. Am J Respir Crit Care Med. 1994 Feb;149(2 Pt 1):295-305 [MEDLINE]
Venoarterial extracorporeal membrane oxygenation for treatment of cardiogenic shock: clinical experiences in 45 adult patients. J Thorac Cardiovasc Surg. 2008;135(2):382–388 [MEDLINE]
Outcomes and long-term quality-of-life of patients supported by extracorporeal membrane oxygenation for refractory cardiogenic shock. Crit Care Med. 2008;36:1404–1411 [MEDLINE]
Review of ECMO (extra corporeal membrane oxygenation) support in critically ill adult patients. Heart Lung Circ 2008;17:S41–S47. doi: 10.1016/j.hlc.2008.08.009. Epub 2008 Oct 29 [MEDLINE]
Extracorporeal Life Support Organization (ELSO). Patient Specific Supplements to the ELSO General Guidelines, 2009. http://square.umin.ac.jp/jrcm/pdf/ecmo/ecmotext12.pdf
Efficacy and economic assessment of conventional ventilatory support versus extracorporeal membrane oxygenation for severe adult respiratory failure (CESAR): a multicentre randomised controlled trial. Lancet. 2009 Oct 17;374(9698):1351-63 [MEDLINE]
Extracorporeal Membrane Oxygenation for 2009 Influenza A (H1N1) Acute Respiratory Distress Syndrome. JAMA. 2009 Nov 4;302(17):1888-95 [MEDLINE]
Extracorporeal Life Support Organization. Patient specific guidelines: a supplement to the ELSO general guidelines. April 2009:15-19 (http://www.elso.med.umich .edu/WordForms/ELSO%20P+%20Specif ic %20Guidelines.pdf)
Early and intermediate results of rescue extracorporeal membrane oxygenation in adult cardiogenic shock. Ann Thorac Surg. 2009;88(6):1897–1903 [MEDLINE]
Extracorporeal membrane oxygenation in nonintubated patients as bridge to lung transplantation. Am J Transplant 2010;10:2173–2178 [MEDLINE]
A review of the fundamental principles and evidence base in the use of extracorporeal membrane oxygenation (ECMO) in critically ill adult patients. J Intensive Care Med. 2011;26:13– 26. doi: 10.1177/0885066610384061 [MEDLINE]
Extracorporeal membrane oxygenation for ARDS in adults. N Engl J Med. 2011;365:1905–1914 [MEDLINE]
Extracorporeal membrane oxygenation for respiratory failure in adults. Curr Opin Crit Care Med. 2012;18:99–104 [MEDLINE]
Venovenous extracorporeal membrane oxygenation in adults: Practical aspects of circuits, cannulae, and procedures. J Cardiothorac Vasc Anesth 2012;26:893–909 [MEDLINE]
Venoarterial extracorporeal membrane oxygenation support for refractory cardiovascular dysfunction during severe bacterial septic shock. Crit Care Med. 2013 Jul;41(7):1616-26. doi: 10.1097/CCM.0b013e31828a2370 [MEDLINE]
Extracorporeal life support devices and strategies for management of acute cardiorespiratory failure in adult patients: a comprehensive review. Crit Care. 2014;18(3):219–229 [MEDLINE]
Mechanical ventilation during extracorporeal membrane oxygenation. Crit Care. 2014 Jan 21;18(1):203. doi: 10.1186/cc13702 [MEDLINE]
Roller and Centrifugal Pumps: A Retrospective Comparison of Bleeding Complications in Extracorporeal Membrane Oxygenation. ASAIO J. 2015 Sep-Oct;61(5):496-501. doi: 10.1097/MAT.0000000000000243 [MEDLINE]
Extracorporeal membrane oxygenation for critically ill adults. Cochrane Database Syst Rev. 2015 Jan 22;1:CD010381. doi: 10.1002/14651858.CD010381.pub2 [MEDLINE]
Extracorporeal membrane oxygenation in adults with cardiogenic shock. Circulation. 2015;131(7): 676–680 [MEDLINE]
Contemporary extracorporeal membrane oxygenation therapy in adults: Fundamental principles and systematic review of the evidence [MEDLINE]