Tracheostomy is Generally Performed in Patients Who Require >3 wks of Mechanical Ventilator Support
The 3 Week Cutoff Has Been Derived from Historical Data Related to the Adverse Effects of Prolonged Endotracheal Tube Cuff Pressure on the Tracheal Wall Associated with High-Pressure Cuffs
However, Current Generation Endotracheal Tubes Have Low-Pressure Cuffs and This Data Likely No Longer Applies
Studies of Duration of Mechanical Ventilation Before Tracheostomy
In a Spanish International Study of Medical-Surgical ICU Patients, Tracheostomy was Performed After a Median of 11 Days (Am J Respir Crit Care Med, 2000) [MEDLINE]: n = 1,638
In the Project Impact Database Study of Impact of Timing of Tracheostomy and Duration of Mechanical Ventilation, Tracheostomy was Performed After a Median of 9 Days (Crit Care Med, 2005) [MEDLINE]
The Decision to Proceed with Tracheostomy Placement Should Be Individualized for Each Patient
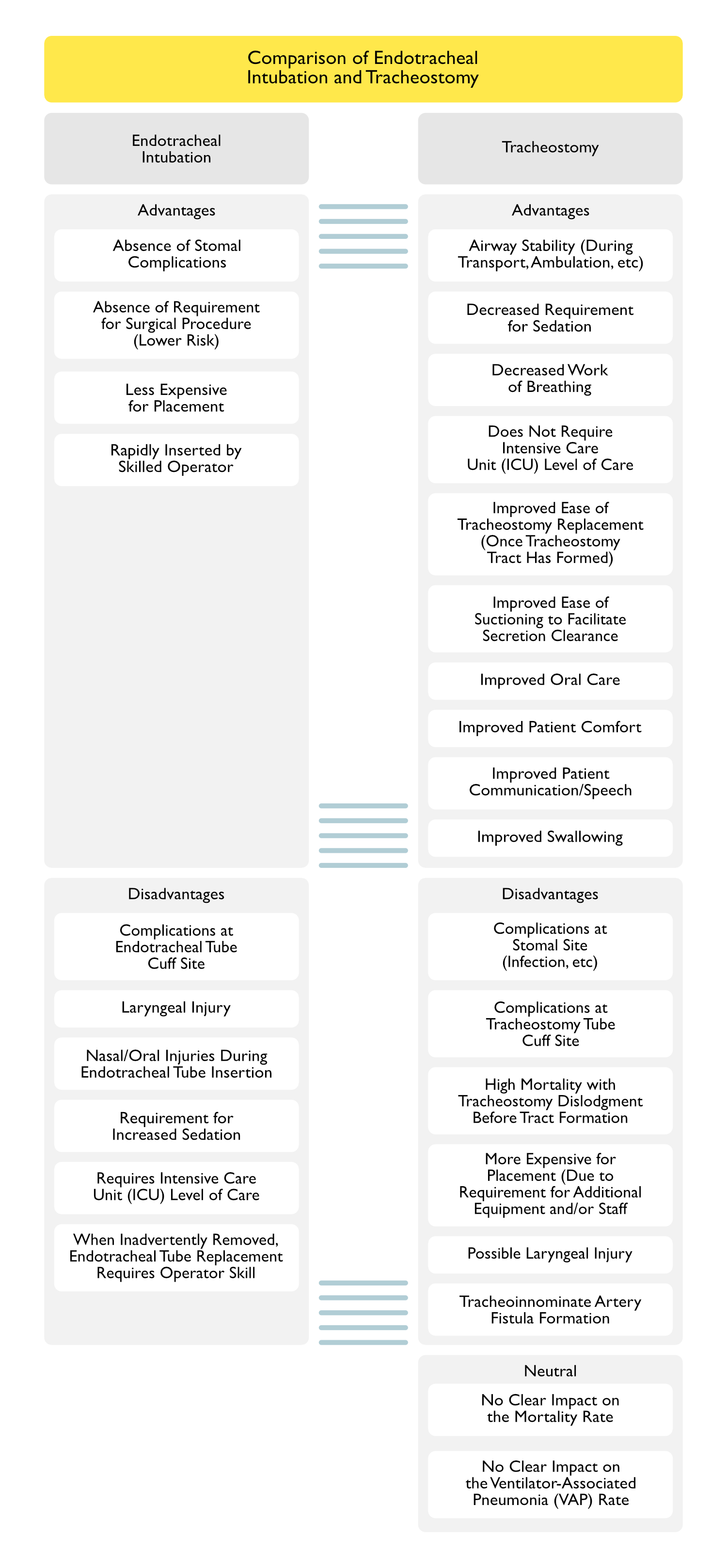
Comparison of Endotracheal Intubation and Tracheostomy
Clinical Efficacy-Improved Respiratory Mechanics Associated with Tracheostomy (as Compared to Endotracheal Intubation)
Study of the Effects of Tracheostomy on Respiratory Mechanics (Am J Respir Crit Care Med, 1999) [MEDLINE]
Tracheostomy Decreased the Work of Breathing, Pressure-Time Index of the Respiratory Muscles, and PEEP/Auto-PEEP (as Compared to Endotracheal Tube)
Study of the Effects of Tracheostomy on Respiratory Mechanics (Arch Surg, 1999) [MEDLINE]
Tracheostomy Decreased the Work of Breathing, Due to the Short, Rigid Nature of the Tube (as Compared to the Longer, Thermolabile Endotracheal Tube): effect is more pronounced at higher respiratory rates
Study of the Effects of Tracheostomy on Respiratory Mechanics (Anaesth Intensive Care, 1999) [MEDLINE]
Tracheostomy Decreased Peak Inspiratory Pressure, But Changed Respiratory Mechanics Very Little
Patients Who Had Better Underlying Mechanics (Higher Cstatic, Lower PEEP) Had Better Chances of Weaning from Mechanical Ventilation After Tracheostomy
Study of the Effects of Tracheostomy Dead Space (J Trauma, 2001) [MEDLINE]
Post-Tracheostomy Change in Physiologic Dead Space Did Not Predict Outcome of Weaning from Mechanical Ventilation
Tracheostomy Improved Pulmonary Toilet, Initiation of the Removal of Mechanical Ventilation, and Control of the Upper Airway
Study of the Effects of Tracheostomy on Respiratory Mechanics (Eur Respir J, 2002) [MEDLINE]
Tracheostomy Decreased Inspiratory Resistive Work, Intrinsic PEEPi, Inspiratory Pressure-Time Product (and its Resistive and Elastic Components)
Observational Study of the Effects of Tracheostomy on Respiratory Mechanics in Difficult to Wean Mechanically Ventilated Patients (PLoS One, 2015) [MEDLINE]
Tracheostomy Improved Weaning Parameters (Rapid Shallow Breathing Index, etc) in Difficult to Wean Mechanically Ventilated Patients Who Weaned from the Ventilator
However, Tracheostomy Only Improved Airway Resistance in Mechanically Ventilated Patients Who Failed to Wean from the Ventilator
Clinical Efficacy-Patient Comfort (as Compared to Endotracheal Intubation)
Observational Study of the Effect of Tracheostomy on Sedation Requirements (Crit Care Med, 2005) [MEDLINE]
Tracheostomy Decreased the Intravenous Sedation and Analgesic Requirement, Spent Less Time Heavily Sedated, and Achieved Autonomy Earlier in the Hospital Course
Clinical Efficacy-Need for Sedation (as Compared to Endotracheal Intubation)
Observational Study of the Effect of Tracheostomy on Sedation Requirements (Crit Care Med, 2005) [MEDLINE]
Tracheostomy Decreased the Intravenous Sedation and Analgesic Requirement, Spent Less Time Heavily Sedated, and Achieved Autonomy Earlier in the Hospital Course
Clinical Efficacy-Mortality Rate (as Compared to Endotracheal Intubation)
Study of Outcome of Tracheostomy in the Intensive Care Unit (Crit Care Med, 1999) ([MEDLINE]
Tracheostomy Patients Had a Lower Hospital Mortality Rate than Non-Tracheostomy Patients (13.7% vs 26.4%)
Tracheostomy Patients Had a Longer Duration of Mechanical Ventilation and Hospital Length of Stay, as Compared to Non-Tracheostomy Patients
Retrospective Study of the Outcome After Respiratory Failure and Tracheostomy Placement (Chest, 2004) [MEDLINE]
Overall Survival and Functional Status are Poor for Patients with Respiratory Failure and Tracheostomy
Survival is Highest in Patients Who are Weaned from Mechanical Ventilation and Have Tracheostomy Removed
Spanish Cohort Study of the Effect of Tracheostomy (Crit Care Med, 2005) [MEDLINE]
Tracheostomy Improved ICU Mortality Rate, But Increased the Length of Stay in the ICU
Tracheostomy Did Not Impact the Hospital Mortality Rate
Project Impact Database Study of Impact of Timing of Tracheostomy and Duration of Mechanical Ventilation (Crit Care Med, 2005) [MEDLINE]
Tracheostomy Patients Had a Lower Mortality Rate than Non-Tracheostomy Patients (78.1% vs 71.1%)
Tracheostomy Timing is Significantly Associated with Duration of Mechanical Ventilation, ICU Length of Stay, and Hospital Length of Stay
Study of Effect of Early Tracheostomy (Within 12 Days) on Outcome (Crit Care Med, 2007) [MEDLINE]
Tracheostomy Decreased the ICU and In-Hospital Mortality Rates
Multicenter Prospective Cohort Study of the Effect of Tracheostomy on Outcome (Crit Care Med, 2007) [MEDLINE]
Tracheostomy Did Not Improve ICU Mortality Rate or Ventilator-Associated Pneumonia Rate
No Difference in ICU Mortality When Tracheostomy was Performed Early vs Late
Post-ICU Mortality Rate was Higher in Patients Who Underwent Tracheostomy (Particularly in Those in Whom Tracheostomy was Left in Place)
This May Be Related to Comorbidities in this Patient Population, Rather than an Adverse Effect of Tracheostomy Itself
Randomized SETPOINT2 Trial of Early Tracheostomy in Severe Acute Ischemic/Hemorrhagic Cerebrovascular Accident (CVA) (JAMA, 2022) [MEDLINE]: n = 366
Tracheostomy (Predominantly Percutaneously) was Performed in 95.2% of the Early Tracheostomy Group at a Median of 4 Days After Intubation (Interquartile Range: 3-4 Days) and in 67% of the Control Group at a Median of 11 Days After Intubation (Interquartile Range: 10-12 Days)
The Proportion without Severe Disability (Modified Rankin Scale Score: 0-4) at 6 Months was Not Significantly Different in the Early Tracheostomy vs the Control Group (43.5% vs 47.1%; Difference: −3.6%; 95% CI: −14.3% to 7.2%]; Adjusted Odds Ratio 0.93; 95% CI: 0.60-1.42]; P = 0.73)
Of the Serious Adverse Events (Related to Tracheostomy), Rates were 5.0% in the Early Tracheostomy Group vs 3.4% in the Control Group
Conclusion
In Patients with Severe Ischemic/Hemorrhagic Stroke Requiring Invasive Mechanical Ventilation, a Early Tracheostomy Did Not Significantly Improve the Survival Rate without Severe Disability at 6 Months, as Compared to Standard Approach to Tracheostomy
However, the Wide Confidence Intervals Around the Effect Estimate May Include a Clinically Important Difference (Therefore, a Clinically Relevant Benefit or Harm from Early Tracheostomy Cannot Be Excluded)
Clinical Efficacy-Timing of Tracheostomy Placement in Respiratory Failure
Study of Outcome of Tracheostomy in the Intensive Care Unit (Crit Care Med, 1999) ([MEDLINE]
Tracheostomy Patients Had a Lower Hospital Mortality Rate than Non-Tracheostomy Patients (13.7% vs 26.4%)
Tracheostomy Patients Had a Longer Duration of Mechanical Ventilation and Hospital Length of Stay, as Compared to Non-Tracheostomy Patients
Randomized Trial of Early Tracheostomy in Medical ICU Patients (Crit Care Med, 2004) [MEDLINE]
Early Tracheostomy (Within 48 hrs), as Compared to Late Tracheostomy (at 14-16 Days), was Associated with Decreased Mortality, Decreased VAP Rate, Decreased Rate of Accidental Extubation, Decreased ICU Length of Stay, Decreased Duration of Mechanical Ventilation, and Decreased Upper Airway Mucosal Trauma
Prospective ICU Database Study of Early vs Late Tracheostomy In Trauma Patients (Crit Care, 2004) [MEDLINE]
Early Tracheostomy (within 7 Days of Start of Mechanical Ventilation) was Associated with Shorter Duration of Mechanical Ventilation and Shorter ICU Length of Stay, But Did Not Impact the ICU or Hospital Mortality Rate
Retrospective Review of Early vs Late Tracheostomy in a Surgical ICU Population (Am J Surg, 2005) [MEDLINE]: n = 185
Early Tracheostomy (Within 7 Days of ICU Admission) was Associated with Decreased Incidence of VAP, Decreased Ventilator Time, and Decreased ICU Length of Stay in a Surgical ICU Population
Systematic Review Studying the Impact of the Timing of Tracheostomy in Adults Supported on Mechanical Ventilation (BMJ, 2005) [MEDLINE]: n= 406 (from 5 studies)
Performance of Early Tracheostomy Did Not Impact the Mortality Rate or Risk of Pneumonia
Performance of Early Tracheostomy Decreased the Duration of Mechanical Ventilation (8.5 Days Less; 95% Confidence Interval: -15.3 to -1.7 Days) and Duration of ICU Stay (15.3 Days Less; 95% Confidence Interval: -24.6 to -6.1 Days)
Project Impact Database Study of Impact of Timing of Tracheostomy and Duration of Mechanical Ventilation (Crit Care Med, 2005) [MEDLINE]
Tracheostomy Patients Had a Lower Mortality Rate than Non-Tracheostomy Patients (78.1% vs 71.1%)
Tracheostomy Timing is Significantly Associated with Duration of Mechanical Ventilation, ICU Length of Stay, and Hospital Length of Stay
Study of Effect of Early Tracheostomy (Within 12 Days) on Outcome (Crit Care Med, 2007) [MEDLINE]
Tracheostomy Decreased the ICU and In-Hospital Mortality Rates
Retrospective Review of Early vs Late Tracheostomy in Patients with Severe Traumatic Brain Injury (Surg Infect-Larchmt, 2007) [MEDLINE]: n = 55
Early Tracheostomy (5.5 +/-1.8 Days), as Compared to Late Tracheostomy (11.0 +/- 4.3 Days) Decreased ICU Length of Stay, But Did Not Decrease Ventilator Days, Incidence of Pneumonia Prior to Tracheostomy, Hospital Cost, Hospital Length of Stay, or Mortality Rate
Multicenter Prospective Cohort Study of the Effect of Tracheostomy on Outcome (Crit Care Med, 2007) [MEDLINE]
Tracheostomy Did Not Improve ICU Mortality Rate or Ventilator-Associated Pneumonia Rate
No Difference in ICU Mortality When Tracheostomy was Performed Early vs Late
Post-ICU Mortality Rate was Higher in Patients Who Underwent Tracheostomy (Particularly in Those in Whom Tracheostomy was Left in Place): this may be related to comorbidities in this patient population, rather than an adverse effect of the tracheostomy itself
Systematic Review and Meta-Analysis of Effect of Early Tracheostomy on VAP Rates (Chest, 2011) [MEDLINE]
Early Tracheostomy Did Not Impact VAP Rates, Duration of Mechanical Ventilation, or Mortality Rate
Study of Early Tracheostomy in Cardiothoracic Surgery Population (Ann Intern Med 2011) [MEDLINE]
Early Tracheostomy Did Not Decrease Length of Hospital Stay, Mortality Rate, Infectious Complication Rate, Long-Term Health-Related Quality of Life in Patients Who Required Long-Term Mechanical Ventilation After Cardiothoracic Surgery
Early Tracheostomy was Well-Tolerated and Associated with Decreased Sedation Use, Better Comfort, and Earlier Resumption of Autonomy
Italian Multicenter, Randomized, Controlled Trial of Early vs Late Tracheostomy (JAMA, 2010) [MEDLINE]
Early Tracheostomy Did Not Decrease the Risk of VAP or Mortality Rate
Critique of Trial: 31% of early group and 43% of late group did not ultimately undergo tracheostomy placement
Cochrane Database Systematic Review of Early vs Late Tracheostomy (Cochrane Database Syst Rev, 2012) [MEDLINE]
Evidence is Low Quality, But No Data Indicate Benefit to Early vs Late Tracheostomy
United Kingdom TracMan Multicenter, Randomized Trial of Early vs Late Tracheostomy (JAMA, 2013) [MEDLINE]
Early Tracheostomy (Within 4 Days of Intubation) Did Not Improve 30-Day All-Cause Mortality, 2-Year Mortality, or Length of ICU Stay
Over 50% of the Patients Randomized to the Late Tracheostomy Arm Did Not Ultimately Receive the Intervention
Suggests that Postponing Tracheostomy Allows a Subset of Patients to Avoid Tracheostomy Completely
The Ability of Clinicians to Predict Which Patients Would Require Extended Mechanical Ventilation Support was Limited
Meta-Analysis of Timing of Tracheostomy (Crit Care, 2015) [MEDLINE]
Early Tracheostomy is Associated with Higher Tracheostomy Rates, Increased Ventilator-Free Days, Decreased ICU Length of Stay, Decreased Need for Sedation, and Decreased Mortality Rate
Meta-Analysis of Early vs Late Tracheostomy (Br J Anaesth, 2015) [MEDLINE]
Early Tracheostomy (Within 10 Days) was Not Associated with Decreased Mortality Rate, ICU Length of Stay, Duration of Mechanical Ventilation, or Incidence of VAP
Early Tracheostomy was Associated with Increased Number of Procedures and Shorter Duration of Sedation
Retrospective Cohort Study of Clinical Variations in Tracheostomy Use (Crit Care Med, 2016) [MEDLINE]
Early Tracheostomy is Potentially Overused in Mechanically Ventilated Trauma Patients (21.9-81.9%), as Compared to Pneumonia/Sepsis Patients (14.9-38.3%)
Nearly 50% of All Tracheostomies in the Trauma Population were Performed within the First 7 Days of Mechanical Ventilation, with Large Unexplained Variation from Hospital to Hospital and No Impact on the Mortality Rate
Multicenter Retrospective Cohort Study of Timing of Tracheostomy in Critically Ill, Mechanically Ventilated Patients (J Intensive Care, 2022) [MEDLINE]: n = 1,538 (from 46 ICU’s)
Quartiles for Timing of Tracheostomy Placement
Quartile 1: ≤ 6 days
Quartile 2: 7-10 days
Quartile 3: 11-14 days
Quartile 4: > 14 days
Hospital Mortality was Significantly Higher in Quartile 2 (Adjusted Odds Ratio 1.52, 95% CI: 1.08-2.13), Quartile 3 (Adjusted Odds Ratio 1.82, 95% CI: 1.28-2.59), and Quartile 4 (Adjusted Odds Ratio 2.26, 95% CI: 1.61-3.16) (p for Trend < 0.001), as Compared to Quartile 1
A Similar Trend was Observed in the Subgroup Analyses of Patients with Impaired Consciousness (Glasgow Coma Scale Score < 8) and Respiratory Failure (pO2:FiO2 Ratio ≤ 300) at ICU Admission (p for Trend = 0.081 and 0.001, Respectively)
Authors Concluded that the Timing of Tracheostomy was Significantly and Independently Associated with Hospital Mortality Rate in a Stepwise Manner
Procedural Aspects of Percutaneous Dilational Tracheostomy
Percutaneous Dilational Tracheostomy is Placed Between the First and Second Tracheal Rings
Routine Postprocedural Chest X-Ray Following Percutaneous Dilational Tracheostomy is Unnecessary in the Absence of Clinical Deterioration or the Anticipation of Postprocedural Complications (Chest, 2003) [MEDLINE]
Relative Contraindications to Percutaneous Dilational Tracheostomy
Age <15 y/o
Due to Presence of an Immature Trachea
Anatomic Distortion of the Neck (Due to Hematoma/Tumor/Scarring/Surgery/Thyromegaly)
High Levels of Ventilator Support Required
High Level of Positive End-Expiratory Pressure (PEEP)
In Some Cases, PEEP-Dependent Patients May Not Be Able to Tolerate the Loss of PEEP During the Procedure
However, Bronchoscopically-Guided Percutaneous Dilational Tracheostomy is Probably Safe Even in Patients Requiring PEEP ≥10 cm H2O (Intensive Care Med, 2003) [MEDLINE]
Inability to Tolerate Periods of Respiratory Acidosis During Percutaneous Dilational Tracheostomy
Induction of Respiratory Acidosis May Be a Contraindication to Percutaneous Dilational Tracheostomy in Patients with Increased Intracranial Pressure (Associated with Traumatic Brain Injury, etc) (see Increased Intracranial Pressure)
Intraprocedural Respiratory Acidosis Appears to Be More Significant During Percutaneous Dilational Tracheostomy than During Surgical Tracheostomy (Intensive Care Med, 1997) [MEDLINE]
Inability to Extend Neck (Due to Cervical Fusion, Rheumatoid Arthritis, Cervical Spine Instability, etc)
Neck Infection
Obesity/Short Neck with Inability to Palpate Trachea
Morbid Obesity is Associated with Increased Risk of Life-Threatening Complications with Surgical Tracheostomy (Crit Care, 2007) [MEDLINE]
Complication Rates are Particularly Higher in Obese Patients with BMI ≥35
Complication Rates are Particularly Higher in Obese Patients the Intraoperative and Early Postoperative Periods
Procedure Duration Has Also Been Noted to Be Longer in Obese Patients
In Systematic Reviews/Meta-Analyses (n = 1,355, 18 Studies), Obesity Has Been Demonstrated to Increases the Complication Rate of Percutaneous Dilational Tracheostomy in Critically Ill Patients (JAMA Otolaryngol Head Neck Surg, 2023) [MEDLINE]
Complication Rate was 16.6% Among Patients with Obesity Overall (n = 791, 17 Studies)
Most of Which were Not Life-Threatening
Only 0.6% of Cases (8 of 1314 Patients, 17 Studies) were Aborted or Converted to an Open Surgical Tracheostomy
A Meta-Analysis of 12 Studies (n = 4,212; 1,078 with Obesity and 3,134 without Obesity) Demonstrated that Patients with Obesity Had a Higher Rate of Complications Associated with Percutaneous Dilational Tracheostomy, as Compared with Their Counterparts without Obesity (Risk Ratio 1.78; 95% CI: 1.38-2.28)
A Single Study Compared Percutaneous Dilational Tracheostomy with Open Surgical Tracheostomy Directly for Critically Ill Adults with Obesity (Thus, the Intended Meta-Analysis Could Not Be Performed in This Subgroup)
Prior Complex Tracheal Surgery (Tracheoplasty, Tracheal Resection, or Tracheal Reconstruction)
Previous Tracheostomy is Not a Contraindication
Requirement for Emergency Airway Placement
While Cricothyrotomy is Considered the Preferred Approach During Emergencies, Percutaneous Tracheostomy May Be an Alternative When Performed by an Experienced Operator
Tracheomalacia (Severe with Associated Cartilage Destruction) (see Tracheobronchomalacia
Cartilage Abnormalities Predispose to Airway Collapse, Resulting in Poor Airway Control
Risk of Acute Bleeding with Percutaneous Dilational Tracheostomy was Independent of Coagulation Variables Tested (Anaesthesia, 2007) [MEDLINE]
Risk of Chronic Bleeding with Percutaneous Dilational Tracheostomy was Most Associated with PTT >50 sec, Platelet Count <50k, and in the Presence of ≥2 Abnormal Coagulation Variables, But Not with the Use of Heparin Prophylaxis (Anaesthesia, 2007) [MEDLINE]
Vascular Structures (Such as High-Riding Innominate or Thyroid Internal Mammary Artery) on Palpation or Ultrasound
Predisposes to Hemorrhagic Complications
Advantages of Percutaneous Dilational Tracheostomy (as Compared to Surgical Tracheostomy)
Can Be Performed at the Bedside
Comparable Rates of Tracheal Stenosis
In Trauma Population, Percutaneous Dilational Tracheostomy Had a Similar Rate of Tracheal Stenosis, as Compared to Surgical Tracheostomy (Am J Surg, 2014) [MEDLINE]
Systematic Review/Meta-Analysis Reported that Percutaneous Dilational Tracheostomy Had Comparable Rates of Tracheal Stenosis, as Compared to Surgical Tracheostomy (Crit Care Med, 2016) [MEDLINE]
Decreased Cost
Cost of ICU Stay with Percutaneous Dilational Tracheostomy was Lower than with Surgical Tracheostomy ($123k vs $156k) in Neurologic Critical Care Populations (Neurocrit Care, 2009) [MEDLINE]
Decreased Duration of Mechanical Ventilation
Percutaneous Dilational Tracheostomy Had Shorter Duration of Mechanical Ventilation, as Compared to Surgical Tracheostomy (19 Days vs 24 Days) in Neurologic Critical Care Populations (Neurocrit Care, 2009) [MEDLINE]
Decreased Risk of Stomal Site Infection
Systematic Review/Meta-Analysis Demonstrated a Decreased Rate of Stomal Infection with Percutaneous Dilational Tracheostomy, as Compared to Surgical Tracheostomy Performed in the Operating Room (Crit Care, 2006) [MEDLINE]
Systematic Review/Meta-Analysis Reported that Percutaneous Dilational Tracheostomy Had a Lower Rate of Stomal Infection, as Compared to Surgical Tracheostomy (Crit Care Med, 2016) [MEDLINE]
Cochrane Database Systematic Review Demonstrated a Decreased Risk of Stomal Infection With Percutaneous Dilational Tracheostomy, as Compared to Surgical Tracheostomy (Moderate Quality Evidence) (Cochrane Database Syst Rev, 2016) [MEDLINE]
Decreased Risk of Stomal Site Scarring
Systematic Review/Meta-Analysis Reported that Percutaneous Dilational Tracheostomy Had Comparable Rate of Stomal Scarring, as Compared to Surgical Tracheostomy (Crit Care Med, 2016) [MEDLINE]
Cochrane Database Systematic Review Demonstrated a Decreased Risk of Stomal Scarring With Percutaneous Dilational Tracheostomy, as Compared to Surgical Tracheostomy (Low Quality Evidence) (Cochrane Database Syst Rev, 2016) [MEDLINE]
Generally Performed Sooner (Since Operating Room Time is Not Required to Be Scheduled)
Percutaneous Dilational Tracheostomy was Performed Sooner (Ventilator Day 8), as Compared to Surgical Tracheostomy (Ventilator Day 12) in Neurologic Critical Care Populations (Neurocrit Care, 2009) [MEDLINE]
High Level of Safety
Percutaneous Dilational Tracheostomy was Associated with Increased Risk of Perioperative Complications and Increased Perioperative Mortality Rate, as Compared to Surgical Tracheostomy (Crit Care Med, 1999) [MEDLINE]
Overall Complication Rates of Percutaneous Dilational Tracheostomy were Similar to Surgical Tracheostomy (Odds Ratio 0.732; 95% CI 0.05-9.37) with Similar Mortality Rates (Chest, 2000) [MEDLINE]
Systematic Review/Meta-Analysis Demonstrated a Decreased Clinically Relevant Bleeding and Mortality with Percutaneous Dilational Tracheostomy, as Compared to Surgical Tracheostomy Performed in the Operating Room (Crit Care, 2006) [MEDLINE]
Spanish Study Reported Overall Complication Rate of 4% (intraprocedural: 2.1%, early postprocedural: 0.75%, and late postprocedural: 1.1%)(Anaesthesia, 2008) [MEDLINE]
Approximately 85% of Procedures were Performed by Residents Supervised by Critical Care Staff
Highest Complication Rates Occurred in Cases Performed by Residents During Their First 5 Attempts (9.2%), as Compared to Their Later Attempts (2.6%)
No Deaths Attributable to Tracheostomy Were Reported
Complication Rates of Percutaneous Dilational Tracheostomy were Similar to Surgical Tracheostomy (8% vs 9%) in Neurologic Critical Care Populations (Neurocrit Care, 2009) [MEDLINE]
In Trauma Population, Percutaneous Dilational Tracheostomy Had a Lower Mortality Rate, as Compared to Surgical Tracheostomy (Am J Surg, 2014) [MEDLINE]
When Performing Percutaneous Dilational Tracheostomy, the Use of a Multidisciplinary Bedside Checklist was Associated with Decreased Procedural Complications (J Trauma Acute Care Surg, 2015) [MEDLINE]
Systematic Review/Meta-Analysis Reported that Percutaneous Dilational Tracheostomy Had Comparable Rate of Major Bleeding, as Compared to Surgical Tracheostomy (Crit Care Med, 2016) [MEDLINE]
Cochrane Database Systematic Review Demonstrated Similar Major Bleeding and Mortality Rates With Percutaneous Dilational Tracheostomy, as Compared to Surgical Tracheostomy (Low Quality Evidence) (Cochrane Database Syst Rev, 2016) [MEDLINE]
Shorter Operative Time
Percutaneous Dilational Tracheostomy Took 9.84 min Less to Perform than Surgical Tracheostomy (Chest, 2000) [MEDLINE]
Disadvantages of Percutaneous Dilational Tracheostomy (as Compared to Surgical Tracheostomy)
Risk of Anterior Tracheal Injury (Chest, 1999) [MEDLINE]
Risk of Posterior Tracheal Wall Perforation
Approximately 12.5% Rate of Posterior Tracheal Wall Injury Has Been Reported in Some Cadaver/Animal Studies (Associated with Poor Stabilization of Guidewire and Guiding Catheter (Chest, 1999) [MEDLINE]
Tracheal Ring Fracture
With Percutaneous Dilational Tracheostomy, Conical Dilation Technique Appears to Result in a Greater Risk of Tracheal Ring Fractures than the Stepwise Dilation Technique (Intensive Care Med, 2002) [MEDLINE]
TRACHUS Trial Demonstrated that Ultrasound-Guided Percutaneous Dilational Tracheostomy was Non-Inferior to Bronchoscopy-Guided Percutaneous Dilational Tracheostomy (Intensive Care Med, 2016) [MEDLINE]
Morbid Obesity is Associated with Increased Risk of Life-Threatening Complications with Surgical Tracheostomy (Crit Care, 2007) [MEDLINE]
Tracheostomy Complication Rates are Higher in Obese Patients (Laryngoscope, 2015) [MEDLINE]: n= 151
Complication Rates are Particularly Higher in Obese Patients with BMI ≥35
Complication Rates are Particularly Higher in Obese Patients the Intraoperative and Early Postoperative Periods
Procedure Duration Has Also Been Noted to Be Longer in Obese Patients
Relative Contraindications
High Levels of Ventilator Support Required
High Level of Positive End-Expiratory Pressure (PEEP): in some cases, PEEP-dependent patients may not be able to tolerate the loss of PEEP during the procedure
Inability to Tolerate Periods of Respiratory Acidosis During Procedure
Intraprocedural Respiratory Acidosis Appears to Be More Significant During Percutaneous Dilational Tracheostomy than During Surgical Tracheostomy (Intensive Care Med, 1997) [MEDLINE]
Bleeding and Stomal Infection Rates for Bedside Tracheostomy are Comparable to Operating Room Tracheostomy (Otolaryngol Head Neck Surg, 1993) [MEDLINE]
Special Aspects
Bjork Flap: used to create an inferior flap with connected sutures XXXX
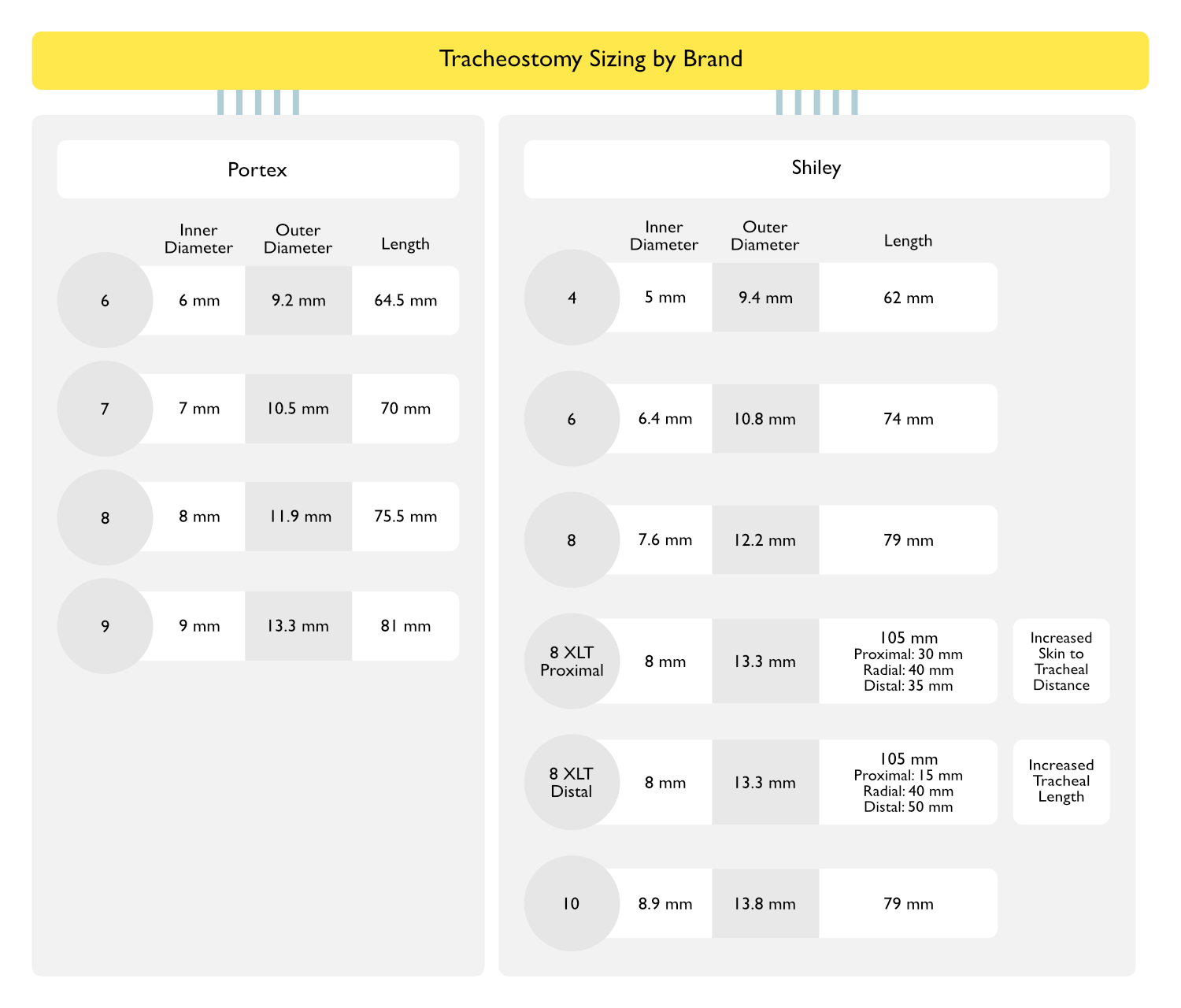
Size 6: 6 mm inner diameter, 9.2 mm outer diameter, maximum usable length 110 mm
Size 7: 7 mm inner diameter, 10.6 mm outer diameter, maximum usable length 120 mm
Size 8: 8 mm inner diameter, 11.7 mm outer diameter, maximum usable length 130 mm
Size 9: 9 mm inner diameter, 12.9 mm outer diameter, maximum usable length 140 mm
Cuff: cuffed
Portex Cuffed Blue Line Ultra Suctionaid Tracheostomy Tube: with subglottic suction port
Sizes: 6, 7, 8, and 9
Cuff: cuffed
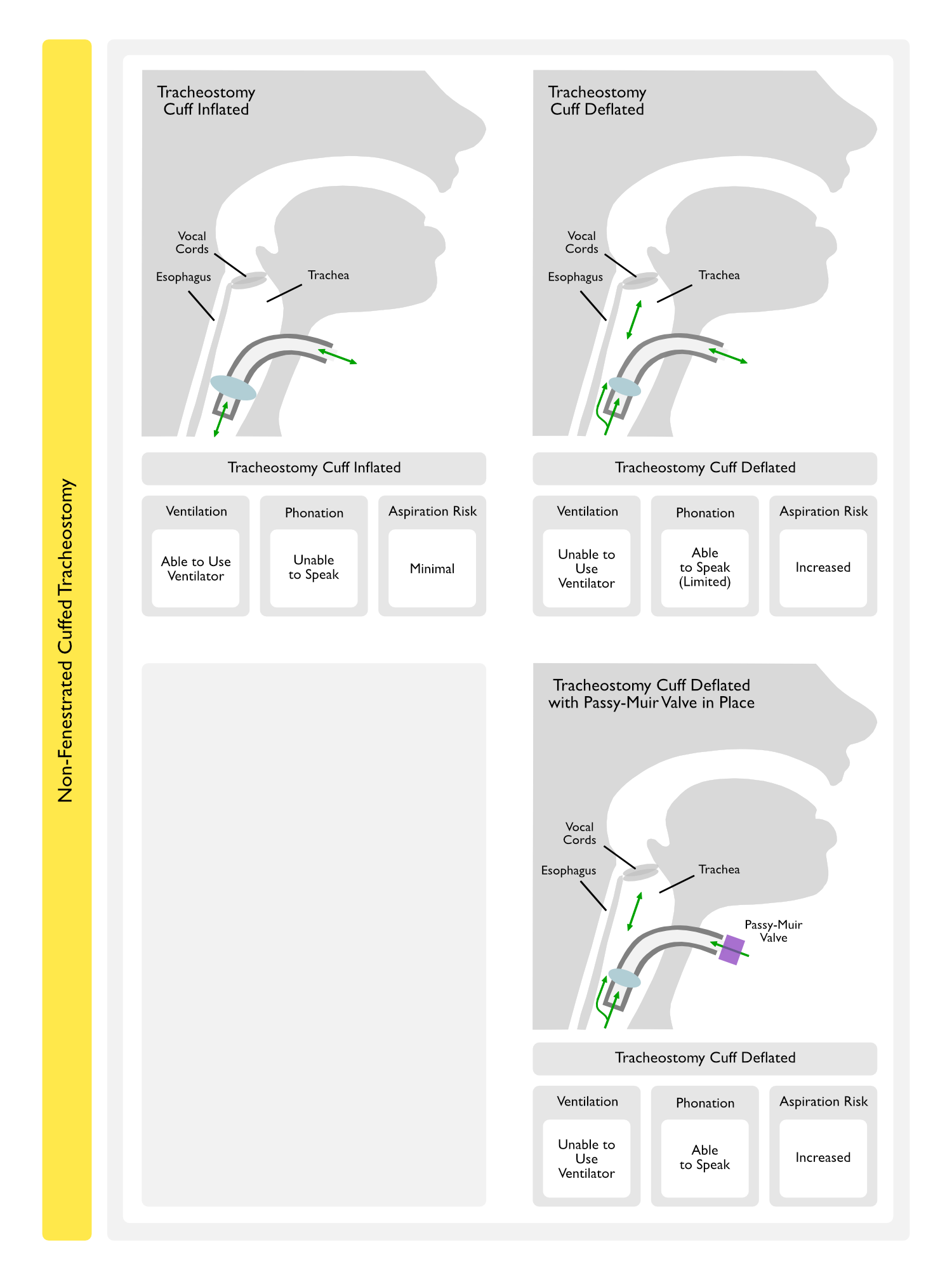
Passy-Muir Valve
Use of the Passy-Muir Valve
Passy-Muir Valve is a One-Way Low-Resistance Valve Which Requires Deflation of the Tracheostomy Tube Cuff and Permits Inspiration, But Not Exhalation, Via the Tracheostomy Tube: exhalation is directed through the glottis/vocal cords, allowing phonation
Use of Passy-Muir Valve with Patient with Tracheostomy, But Not on Mechanical Ventilation
Since Mechanical Ventilation is Not Required and Tidal Volume Leak is Not an Issue, this is Tolerated in Almost All Patients (Assuming that the Non-Fenestrated Tracheostomy Size is Small Enough, Relative the Size of the Patient’s Trachea, to Allow Adequate Airflow in the Patient)
Use of Passy-Muir Valve with Patient with Tracheostomy and on Mechanical Ventilation
Since Mechanical Ventilation is Required and Tidal Volume Leak May Be an Issue, Patient Selection is Critical to Determine if the Patient Will Tolerate Trials
Due to Tracheostomy Tube Cuff Deflation in Patients Requiring Ventilator Support, Passy-Muir Valve Use Requires an Approximate 50% Increase in Ventilator Tidal Volume (on Volume-Cycled Ventilation) to Maintain Adequate Ventilation (Crit Care Med, 1993) [MEDLINE]
Alternatively, if the Patient is Able to Tolerate Pressure Support Ventilation, this Ventilation Approach May Be Utilized (Especially in Patients with Neuromuscular Disease) (Am J Respir Crit Care Med, 2003) [MEDLINE] (Chest, 2003) [MEDLINE]
Requirements for Passy-Muir Valve Use
Ability to Clear Secretions
Ability to Tolerate Tracheostomy Cuff Deflation
Adequate Gas Exchange
Hemodynamic Stability
Normal Mental Status
Advantages of the Passy-Muir Valve
Allows Laryngeal Airflow, Facilitating Recovery of Laryngeal Reflex Activity, Phonation, and Cough
Decreases Aspiration During Eating
Passy-Muir Valve Restores More Normal Subglottic and Glottic Airflow During Exhalation
Decreases Bronchial and Pharyngeal Secretions
Since Air Escaping through the Mouth and Nose Contributes to Evaporation of Secretions
Facilitates Secretion Clearance
Since Airflow is Directed Toward the Larynx
Improves Cough Effectiveness
Due to Restoration of Glottic Function
Reestablishes Ability to Smell
Well-Tolerated
Can Even Be Used in Patients with Neuromuscular Disease
Adverse Effects/Complications of the Passy-Muir Valve
Inappropriate Use of Excessively Large Tracheostomy, Which Impedes Expiratory Airflow Through the Trachea
Tracheostomy Downsizing (If Tolerated) is the Usual Solution in These Cases
Accidental Use of the Passy-Muir Valve with Tracheostomy Cuff Still Inflated, Which Results in Completely Obstructed Expiratory Airflow
Tracheostomy Configurations
Tracheostomy Tube Change
Routine Tracheostomy Tube Change
The Tracheostomy Tube is Typically First Changed 7-14 Days After the Initial Tracheostomy Placement (Once the Tract Has Formed)
The First Tracheostomy Tube Change Should Be Performed in a Controlled Environment with Emergency Resources Available, in Case the Tracheostomy Cannot Be Safely Replaced and Endotracheal Intubation is Required (Respir Care, 2010) [MEDLINE]
Otolaryngologic Consensus Guidelines Suggest Changing the Tracheostomy Tube at 3-7 Days if Placed Operatively or at 10-14 Days if Placed Via a Percutaneous Dilational Method (Otolaryngol Head Neck Surg, 2013) [MEDLINE]
Subsequently, the Tracheostomy Tube Should Be Changed Every 60-90 Days
Recommended Tracheostomy Tube Changes to Address Specific Clinical Issues (Respir Care, 2010) [MEDLINE]
Patient Discomfort
Tracheostomy Tube Downsizing
Tracheostomy Malpositioning
Tracheostomy Tube Downsizing
Change to Longer Tracheostomy Tube
Patient-Ventilator Dyssynchrony
Change to Different Tracheostomy Tube
Tracheostomy Tube Cuff Leak: may occur in the setting of tracheomalacia
Change to Different Tracheostomy Tube
Tracheostomy Tube Fracture/Cuff Rupture
Change to New Tracheostomy Tube (of Same Size/Brand)
Need for Mechanical Ventilation
If Fenestrated or Uncuffed Tracheostomy is Being Used, Change to Cuffed, Non-Fenestrated Tracheostomy to Allow Mechanical Ventilation
Bronchoscopy Generally Requires Tracheostomy Tube with Inner Diameter of ≥7.0-7.5 mm
Change to Larger Tracheostomy Tube (if Possible)
Tracheostomy Tube Weaning and Decannulation
Airway Evaluation by Bronchoscopy (see Bronchoscopy)
May Be Required in Some Cases to Evaluate for Tracheal Granulation Tissue or Other Airway Abnormalities Prior to Tracheostomy Decannulation (Chest, 1993) [MEDLINE]: while they may be present, these abnormalities are often not clinically significant
An Unsuccessful Initial Capping Trial May Predict a Subset of Patients Who Require Bronchoscopic Evaluation Prior to Consideration of Decannulation (Crit Care Med, 1997) [MEDLINE]
Methods of Tracheostomy Weaning
Progressive Tracheostomy Downsizing
Using a Decisional Flow Chart (with Progression to 6 mm Tracheostomy or Portex Minitrach for at Least 1 wk Prior to Decannulation), Success Rate (without Major Clinical Complications) was 80% (Intensive Care Med, 2003) [MEDLINE]
Progressive Trials of Fenestrated Tracheostomy Capping with Cuff Deflated (Until Tolerated for 12-48 hrs)
Consensus Guidelines Suggest Progressive Capping Trials Prior to Decannulation (with Downsizing When a Large Tracheostomy is Being Used) (Otolaryngol Head Neck Surg, 2013) [MEDLINE]
Observe Patient for Stridor and Absence of Effective Cough to Determine Success of the Capping Trial
Passy-Muir Valve Trials: may be used instead of capping
Passy-Muir Valves Do Not Impact Time to Decannulation, as Compared to Capping Trials
Single-Stage Tracheostomy Decannulation Protocol with Bronchoscopy (Laryngoscope, 2016) [MEDLINE]
Indications for Single-Stage Tracheostomy Decannulation
Absence of Active Infection
Absence of Dyspnea
Absence of Requirement for Ventilatory Support
Normal or Adequate Spirometry
Normal Bronchoscopy
Presence of Leak Around Tracheostomy Tube Cuff
Stable Arterial Blood Gas (ABG)
Stable Hemodynamic Status
Use of Tracheostomy Button (Tracheostomy Retainer): device which maintains the tracheostomy tract and which may be particularly useful in patients with borderline respiratory status during a prolonged period of clinical observation
Button May Be Particularly Useful in Patients Who Have Undergone Percutaneous Dilational Tracheostomy, as the Tracheal Stoma Tends to Close Rapidly in These Patients (Respiration, 2012) [MEDLINE]
Indications for Tracheostomy Decannulation (Respir Care, 2010) [MEDLINE]
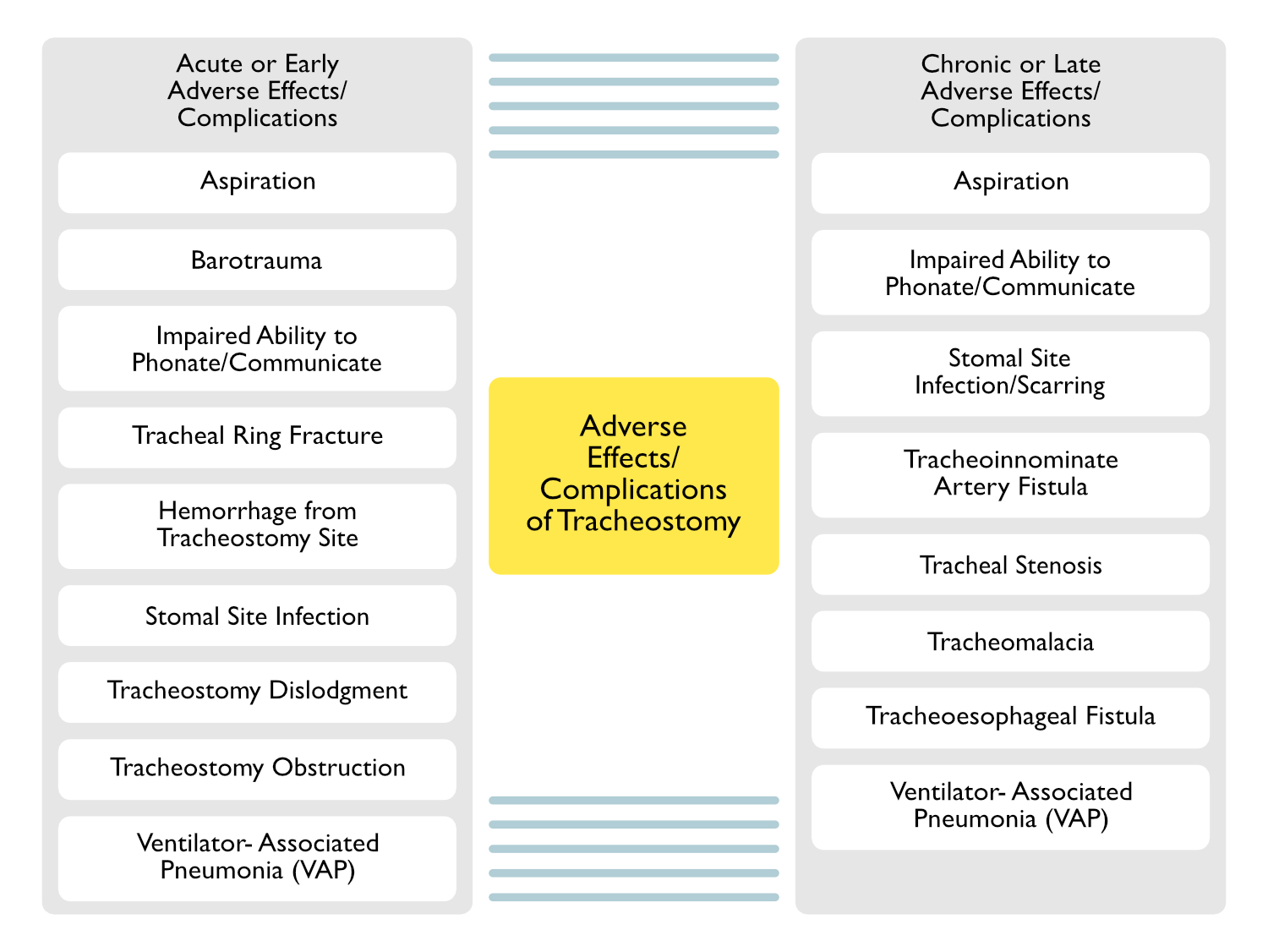
Aspiration of Oropharyngeal Secretions Commonly Occurs with Both Endotracheal Tubes and Tracheostomy Tubes (see Endotracheal Intubation)
Presence of Gag Reflex Does Not Confer Protection Against Aspiration with Endotracheal Intubation or Tracheostomy (Crit Care Med, 1990) [MEDLINE]
Aspiration is Not Increased with Occlusion of the Tracheostomy with a Cap/Finger for Phonation (Ear Nose Throat J, 2006) [MEDLINE]
Physiologic Mechanisms
Delayed Triggering of the Swallowing Response (Crit Care Med, 1990) [MEDLINE] (Br J Anaesth, 2012) [MEDLINE]
Swallowing Dysfunction (Particularly Disorder of the Pharyngeal Phase) and Aspiration are Common with Tracheostomy (Chest, 1994) [MEDLINE]: increasing age increases the risk of aspiration and aspiration is frequently silent
Increasing Tracheostomy Cuff Pressure Worsens Swallowing Dysfunction (as Measured by Submental Electromyogram and Amplitude of Laryngeal Acceleration) (Br J Anaesth, 2012) [MEDLINE]
Tracheostomy Removal Does Not Appear to Immediately Improve Swallowing Dysfunction (Dysphagia, 2012) [MEDLINE]
Pooling of Oropharyngeal Secretions Above the Tracheostomy Tube Cuff (Crit Care Med, 1990) [MEDLINE]
Risk of Aspiration is Correlated with the Amount of Oropharyngeal Secretions
Diagnosis
Methods to Detect Aspiration
Direct Visualization: considered the gold standard method to detect aspiration in tracheostomized patients
Glucose Oxidase Testing of Tracheal Secretions: glucose oxidase testing is easier to perform and has higher sensitivity for aspiration than methylene blue dye testing (Chest, 1993) [MEDLINE]
Dye Added to Tube Feedings (Evans Blue, Methylene Blue): detection of dye in tracheal aspirate indicates aspiration (Ear Nose Throat J, 2006) [MEDLINE] (J Cardiothorac Vasc Anesth, 2017) [MEDLINE]
Clinical
Fiberoptic Study of Swallowing Function in Patients with Tracheostomy (Chest, 2002) [MEDLINE]
Approximately 33% of Patients Manifested Aspiration
When Aspiration Occurred, 82% of These Cases were Silent Aspiration
Swallowing Success Occurred Most Frequently in Patients <70 y/o with Improving Respiratory and Medical Status
The Optimal Timing for Successful Swallowing Outcome was Approximately 3 wks Post-Tracheostomy in Patients >70 yo/ and 1 wk in Patients <70 y/o
Barotrauma
Physiology
Inadvertent Extraluminal Positioning of the Tracheostomy Fenestration During Tracheostomy Placement: for this reason, fenestrated tracheostomies are typically not selected for initial percutaneous tracheostomy placement
Laceration of the Posterior Tracheal Wall
Clinical
Pneumothorax (see Pneumothorax): occurs in 0.6% of cases (Chest, 2004) [MEDLINE]
Decreased Phonation/Impaired Ability to Communicate
Epidemiology
Lack of Verbal Communication Can Be Very Frustrating for Patients Requiring Prolonged Mechanical Ventilatory Support with Either Endotracheal Intubation of Tracheostomy (Chest, 1990) [MEDLINE]
Clinical
Decreased Phonation May Be Prolonged (or Indefinite in Some Cases)
Prevention
Early Passy-Muir Valve Trials with Speech Pathology: although Passy-Muir speech valves have historically been used in tracheostomized patients (with a deflated cuff) after they have weaned from the ventilator (for at least some part of the day), data suggest that speech valve trials can be started even in mechanically ventilated tracheostomized patients and may shorten the time to phonation (Crit Care Med, 2016) [MEDLINE]
Treatment
Passy-Muir Valve: one-way valve device which requires tracheostomy cuff deflation
Use of Voice Tracheostomy Tube in Patients with Low PEEP Requirement (Chest, 2004) [MEDLINE]: utilizes slits to expand with positive-pressure inspiration and deflate during expiration, allowing phonation
Use of Communicating Tracheostomy Device (Portex Talk Tube, Communitrach I): these devices use a small diameter tube which expels gas above the tracheostomy tube cuff when the proximal end has been manually occluded (however, these devices require the use of manual occlusion and the patient frequently will be able to speak only in short sentences)
Hemorrhage from Tracheostomy Site
Physiology
Hemorrhage from the Tracheostomy Site May Result in Significant Blood Clots in the Airways with Consequent Difficulty Ventilating the Patient
Increased Peak Inspiratory Pressure (PIP) on the Ventilator
Treatment
Control of Hemorrhage
Removal of Airway Clots: cryoprobe removal of clots may be required in cases where clots are difficult to evacuate
Tracheostomy Removal and Endotracheal Reintubation: may be required in cases with significant hemorrhage, as reintubation allows clot to form above the endotracheal tube cuff (tamponading the bleeding site) and prevents further soiling of the airways with blood
Stomal Site Infection
Epidemiology
Percutaneous Dilational Tracheostomy Has Been Demonstrated to Have a Lower Rate of Stomal Site Infection than Surgical Tracheostomy
Systematic Review/Meta-Analysis Demonstrated a Decreased Rate of Stomal Infection with Percutaneous Dilational Tracheostomy, as Compared to Surgical Tracheostomy Performed in the Operating Room (Crit Care, 2006) [MEDLINE]
Systematic Review/Meta-Analysis Reported that Percutaneous Dilational Tracheostomy Had a Lower Rate of Stomal Infection, as Compared to Surgical Tracheostomy (Crit Care Med, 2016) [MEDLINE]
Cochrane Database Systematic Review Demonstrated a Decreased Risk of Stomal Infection With Percutaneous Dilational Tracheostomy, as Compared to Surgical Tracheostomy (Moderate Quality Evidence) (Cochrane Database Syst Rev, 2016) [MEDLINE]
Tracheal Ring Fracture
Epidemiology
With Percutaneous Dilational Tracheostomy, Conical Dilation Technique Appears to Result in a Greater Risk of Tracheal Ring Fractures than the Stepwise Dilation Technique (Intensive Care Med, 2002) [MEDLINE]
Uncommon when Vigilant Postoperative Management is Utilized in the Intensive Care Unit
Clinical
Inability to Ventilate
Attempting to Ventilate Via a Dislodged Tracheostomy (with a Bag-Valve-Mask or Ventilator) Can Result in Pneumomediastinum (and Resultant Pneumothorax)
Inability to Ventilate May Require Emergent Removal of the Tracheostomy and Endotracheal Reintubation
Prevention
Strict Precautions Should Be Employed Regarding Patient Movement/Repositioning in the Days Following Tracheostomy Placement to Prevent Dislodgment
Tracheal Ring Sutures: unclear if the use of tracheal ring sutures at the time of tracheostomy placement decreases the risk of tracheostomy dislodgement (or improves the ability to replace a dislodged tracheostomy, if it occurs)
Tracheostomy Obstruction
Epidemiology
Partial Tracheostomy Obstruction by the Posterior Tracheal Membrane Can Occur with Percutaneous Tracheostomy: has been reported with use of the Portex Per-Fit tracheostomy tube (Chest, 2002) [MEDLINE]
Periodic Swelling of the Posterior Tracheal Wall with Intermittent Tracheostomy Obstruction Has Been Reported (Chest, 2003) [MEDLINE]
Tracheostomy Malpositioning (with >50% Obstruction of the Tracheostomy Lumen by Tissue) Has Been Reported in Up to 10% of Cases (Chest, 2008) [MEDLINE]: reported in 40/430 patients in this retrospective study performed in a acute care facility specializing in ventilator weaning
While Thoracic/General Surgeons were Equally Likely to Have Malpositioned Tracheostomies, Other Subspecialty Surgeons were More Likely to Have Malpositioned Tracheostomies (Odds Ratio: 6.42)
Malpositioned Tracheostomy was Associated with Prolonged Mechanical Ventilation
Malpositioned Tracheostomy was Not Associated with Increased Hospital Length of Stay or Mortality Rate
Physiology
Tracheostomy Obstruction by the Posterior Tracheal Membrane
Data are Inconclusive as to the Impact of Tracheostomy on the Risk of VAP
Tracheostomy (6-Fold Increased Risk), Multiple Central Venous Catheter Insertions, Use of Antacids, and Reintubation were Associated with an Increased Risk of VAP (Chest, 2001) [MEDLINE]
In Medical ICU Population, Early Tracheostomy (Within 48 hrs) was Associated with Decreased Mortality, Decreased VAP Rate, Decreased Rate of Accidental Extubation, Decreased ICU Length of Stay, Decreased Duration of Mechanical Ventilation, and Decreased Upper Airway Mucosal Trauma (Crit Care Med, 2004) [MEDLINE]
In a Surgical ICU Population, Tracheostomy Performed within 7 Days of ICU Admission was Associated with Decreased Incidence of VAP, Decreased Ventilator Time, and Decreased ICU Length of Stay (Am J Surg, 2005) [MEDLINE]: n = 185
Systematic Review of Mechanically Ventilated Patients Indicated that Early Tracheostomy Did Not Impact the Mortality Rate or Risk of Pneumonia, But Decreased the Duration of Mechanical Ventilation and Duration of ICU Stay (BMJ, 2005) [MEDLINE]
In Non-Trauma, Non-Immunocompromised Patients, Tracheostomy was Associated with a Lower Risk of VAP (Eur Respir J, 2007) [MEDLINE]
In Patients with Severe Traumatic Brain Injury, Early Tracheostomy (5.5 +/-1.8 Days), as Compared to Late Tracheostomy (11.0 +/- 4.3 Days) Decreased ICU Length of Stay, But Did Not Decrease Ventilator Days, Incidence of Pneumonia Prior to Tracheostomy, Hospital Cost, Hospital Length of Stay, or Mortality Rate (Surg Infect-Larchmt, 2007) [MEDLINE]
In Multicenter Prospective Cohort Study, Tracheostomy Did Not Improve the ICU Mortality Rate or Ventilator-Associated Pneumonia Rate (Crit Care Med, 2007) [MEDLINE]
In Multicenter, Randomized Italian Trial, Early Tracheostomy (Mean: 7 Days) Did Not Decrease the Risk of VAP or Mortality Rate (JAMA, 2010) [MEDLINE]
Early Tracheostomy (Within 10 Days) was Not Associated with Decreased Mortality Rate, ICU Length of Stay, Duration of Mechanical Ventilation, or Incidence of VAP, But was Associated with and Increased Number of Procedures and Shorter Duration of Sedation (Br J Anaesth, 2015) [MEDLINE]
Risk Factors Associated with Early Post-Tracheostomy VAP (Occurring ≤5 Days of Tracheostomy Placement) (Chest, 2000) [MEDLINE]: in this retrospective study, incidence of VAP was 26%, VAP occurred at mean of 9 days post-tracheostomy placement, and overall mortality rate was 33% (VAP increased mortality rate to 54%)
Endotracheal Aspirate with Significant Bacterial Colonization (>100k cfu/mL): the responsible VAP pathogen was present in the endotracheal aspirate on the day of tracheostomy
Fever (≥38.3 C) on Day of Tracheostomy Placement
Requirement for Sedation >24 hrs Post-Tracheostomy
Risk Factors Associated with Late Post-Tracheostomy VAP (Occurring >5 Days of Tracheostomy Placement) (Chest, 2000) [MEDLINE]: in this retrospective study, incidence of VAP was 26%, VAP occurred at mean of 9 days post-tracheostomy placement, and overall mortality rate was 33% (VAP increased mortality rate to 54%)
Duration of Sedation Prior to Tracheostomy
Fever (≥38.3 C) on Day of Tracheostomy Placement
Risk Factors Not Associated with Post-Tracheostomy VAP (Early or Late) (Chest, 2000) [MEDLINE]: in this retrospective study, incidence of VAP was 26%, VAP occurred at mean of 9 days post-tracheostomy placement, and overall mortality rate was 33% (VAP increased mortality rate to 54%)
Arterial pO2/FIO2 Ratio
Duration of Antimicrobial Administration
Duration of Mechanical Ventilation Prior to Tracheostomy
Intensive Care Unit Admitting Diagnosis
Indication for Tracheostomy
Prior Nosocomial Pneumonia
Use of Steroids on the Day of Tracheostomy
Physiologic Mechanisms Which May Contribute to Lower Airway Infection
Aspiration of Oropharyngeal Secretions
Bypass of Upper Airway Filtration Mechanism
Contaminated Equipment/Solutions Used for Respiratory Care
Impaired Tracheal Mucociliary Clearance
Ineffective Cough Clearance of Secretions
Tracheal Wall Mucosal Damage Due to Tracheostomy or Suction Trauma
Chronic or Late Adverse Effects/Complications (Weeks-Months)
Pulmonary Adverse Effects/Complications
Aspiration
Epidemiology
Aspiration of Oropharyngeal Secretions Commonly Occurs with Both Endotracheal Tubes and Tracheostomy Tubes (see Endotracheal Intubation)
Presence of Gag Reflex Does Not Confer Protection Against Aspiration with Endotracheal Intubation or Tracheostomy (Crit Care Med, 1990) [MEDLINE]
Aspiration is Not Increased with Occlusion of the Tracheostomy with a Cap/Finger for Phonation (Ear Nose Throat J, 2006) [MEDLINE]
Physiologic Mechanisms
Delayed Triggering of the Swallowing Response (Crit Care Med, 1990) [MEDLINE] (Br J Anaesth, 2012) [MEDLINE]
Swallowing Dysfunction (Particularly Disorder of the Pharyngeal Phase) and Aspiration are Common with Tracheostomy (Chest, 1994) [MEDLINE]: increasing age increases the risk of aspiration and aspiration is frequently silent
Increasing Tracheostomy Cuff Pressure Worsens Swallowing Dysfunction (as Measured by Submental Electromyogram and Amplitude of Laryngeal Acceleration) (Br J Anaesth, 2012) [MEDLINE]
Tracheostomy Removal Does Not Appear to Immediately Improve Swallowing Dysfunction (Dysphagia, 2012) [MEDLINE]
Pharyngeal Pooling of Secretions Above the Airway Cuff (Crit Care Med, 1990) [MEDLINE]
Risk of Aspiration is Correlated with the Amount of Oropharyngeal Secretions
Diagnosis
Methods to Detect Aspiration
Direct Visualization: considered the gold standard method to detect aspiration in tracheostomized patients
Glucose Oxidase Testing of Tracheal Secretions: glucose oxidase testing is easier to perform and has higher sensitivity for aspiration than methylene blue dye testing (Chest, 1993) [MEDLINE]
Dye Added to Tube Feedings (Evans Blue, Methylene Blue): detection of dye in tracheal aspirate indicates aspiration (Ear Nose Throat J, 2006) [MEDLINE] (J Cardiothorac Vasc Anesth, 2017) [MEDLINE]
Clinical
Fiberoptic Study of Swallowing Function in Patients with Tracheostomy (Chest, 2002) [MEDLINE]
Approximately 33% of Patients Manifested Aspiration
When Aspiration Occurred, 82% of These Cases were Silent Aspiration
Swallowing Success Occurred Most Frequently in Patients <70 y/o with Improving Respiratory and Medical Status
The Optimal Timing for Successful Swallowing Outcome was Approximately 3 wks Post-Tracheostomy in Patients >70 yo/ and 1 wk in Patients <70 y/o, Suggesting that the Probability of Aspiration Likely Decreases Over Time
Decreased Phonation/Impaired Ability to Communicate
Epidemiology
Lack of Verbal Communication Can Be Very Frustrating for Patients Requiring Prolonged Mechanical Ventilatory Support with Either Endotracheal Intubation of Tracheostomy (Chest, 1990) [MEDLINE]
Clinical
Decreased Phonation May Be Prolonged (or Indefinite in Some Cases)
Prevention
Early Passy-Muir Valve Trials with Speech Pathology: although Passy-Muir speech valves have historically been used in tracheostomized patients (with a deflated cuff) after they have weaned from the ventilator (for at least some part of the day), data suggest that speech valve trials can be started even in mechanically ventilated tracheostomized patients and may shorten the time to phonation (Crit Care Med, 2016) [MEDLINE]
Treatment
Passy-Muir Valve: one-way valve device which requires tracheostomy cuff deflation
Use of Voice Tracheostomy Tube in Patients with Low PEEP Requirement (Chest, 2004) [MEDLINE]: utilizes slits to expand with positive-pressure inspiration and deflate during expiration, allowing phonation
Use of Communicating Tracheostomy Device (Portex Talk Tube, Communitrach I): these devices use a small diameter tube which expels gas above the tracheostomy tube cuff when the proximal end has been manually occluded (however, these devices require the use of manual occlusion and the patient frequently will be able to speak only in short sentences)
Stomal Site Infection
Epidemiology
Percutaneous Dilational Tracheostomy Has Been Demonstrated to Have a Lower Rate of Stomal Site Infection than Surgical Tracheostomy
Systematic Review/Meta-Analysis Demonstrated a Decreased Rate of Stomal Infection with Percutaneous Dilational Tracheostomy, as Compared to Surgical Tracheostomy Performed in the Operating Room (Crit Care, 2006) [MEDLINE]
Systematic Review/Meta-Analysis Reported that Percutaneous Dilational Tracheostomy Had a Lower Rate of Stomal Infection, as Compared to Surgical Tracheostomy (Crit Care Med, 2016) [MEDLINE]
Cochrane Database Systematic Review Demonstrated a Decreased Risk of Stomal Infecti
Stomal Site Scarring
Epidemiology
Percutaneous Dilational Tracheostomy Has Been Demonstrated to Have a Lower Rate of Stomal Scarring than Surgical Tracheostomy
Systematic Review/Meta-Analysis Reported that Percutaneous Dilational Tracheostomy Had Comparable Rate of Stomal Scarring, as Compared to Surgical Tracheostomy (Crit Care Med, 2016) [MEDLINE]
Cochrane Database Systematic Review Demonstrated a Decreased Risk of Stomal Scarring With Percutaneous Dilational Tracheostomy, as Compared to Surgical Tracheostomy (Low Quality Evidence) (Cochrane Database Syst Rev, 2016) [MEDLINE]
Tracheal Ring Fracture
Epidemiology
With Percutaneous Dilational Tracheostomy, Conical Dilation Technique Appears to Result in a Greater Risk of Tracheal Ring Fractures than the Stepwise Dilation Technique (Intensive Care Med, 2002) [MEDLINE]
Tracheal Stenosis Below the Glottis But Above the Tracheal Stoma Has Been Reported Following Percutaneous Tracheostomy (Crit Care Med, 2003) [MEDLINE]
Studies Report that Tracheal Stenosis Occurred a Mean of 54.5 Days After Tracheostomy Placement with 85% of Cases Demonstrating Stenosis Located Around the Tracheal Stoma (BMC Pulm Med, 2008) [MEDLINE]
In Contrast, Patients with Tracheal Stenosis Due to Endotracheal Intubation Predominantly Manifest Web-Like Stenosis at the Cuff Site
Incidence of Post-Tracheostomy Tracheal Stenosis is Approximately 2.6% (Otolaryngol Head Neck Surg, 2018) [MEDLINE]
Risk Factors for Post-Tracheostomy Tracheal Stenosis (Otolaryngol Head Neck Surg, 2018) [MEDLINE]
This Complication Occurred More Commonly in the Past, Associated with a Low-Positioned Tracheostomy Tube (Ann Surg, 1976) [MEDLINE]
Current Incidence: <1% of cases (Chest, 2005) [MEDLINE]
Physiology
Usually a Tracheoinnominate Artery Fistula
Erosion of the Tracheostomy Tube Tip or Cuff into the Anterior Wall of the Trachea, Resulting in a Fistula into the Innominate Artery as it Passes Anterior to the Trachea
Diagnostic
Bronchoscopy (see Bronchoscopy): may be useful in cases which are not massive
CT Angiogram (see xxxxx): may be useful in cases which are not massive
Clinical
Hemoptysis (see Hemoptysis): may be preceded by a “sentinel bleed” and may be massive
Treatment
Temporizing Measures: overinflate the tracheostomy tube/endotracheal tube cuff (to compress the innominate artery), remove tracheostomy and place an oral endotracheal tube (with cuff distal to the site of the fistula), or insert a finger into the tracheostomy stoma and advance distally in the trachea with compression anteriorly toward the sternum (“little Dutch boy maneuver”)
Damage to Tracheal Cartilage at Stoma/Cuff/Distal Tube Sites Due to Pressure Necrosis, Impaired Blood Flow, Recurrent Infection, Mucosal Friction, or Mucosal Inflammation
Clinical
Usually Segmental Tracheomalacia (with Maximum Length of 3 cm)
Data are Inconclusive as to the Impact of Tracheostomy on the Risk of VAP
Tracheostomy (6-Fold Increased Risk), Multiple Central Venous Catheter Insertions, Use of Antacids, and Reintubation were Associated with an Increased Risk of VAP (Chest, 2001) [MEDLINE]
In Medical ICU Population, Early Tracheostomy (Within 48 hrs) was Associated with Decreased Mortality, Decreased VAP Rate, Decreased Rate of Accidental Extubation, Decreased ICU Length of Stay, Decreased Duration of Mechanical Ventilation, and Decreased Upper Airway Mucosal Trauma (Crit Care Med, 2004) [MEDLINE]
In a Surgical ICU Population, Tracheostomy Performed within 7 Days of ICU Admission was Associated with Decreased Incidence of VAP, Decreased Ventilator Time, and Decreased ICU Length of Stay (Am J Surg, 2005) [MEDLINE]: n = 185
Systematic Review of Mechanically Ventilated Patients Indicated that Early Tracheostomy Did Not Impact the Mortality Rate or Risk of Pneumonia, But Decreased the Duration of Mechanical Ventilation and Duration of ICU Stay (BMJ, 2005) [MEDLINE]
In Non-Trauma, Non-Immunocompromised Patients, Tracheostomy was Associated with a Lower Risk of VAP (Eur Respir J, 2007) [MEDLINE]
In Patients with Severe Traumatic Brain Injury, Early Tracheostomy (5.5 +/-1.8 Days), as Compared to Late Tracheostomy (11.0 +/- 4.3 Days) Decreased ICU Length of Stay, But Did Not Decrease Ventilator Days, Incidence of Pneumonia Prior to Tracheostomy, Hospital Cost, Hospital Length of Stay, or Mortality Rate (Surg Infect-Larchmt, 2007) [MEDLINE]
In Multicenter Prospective Cohort Study, Tracheostomy Did Not Improve the ICU Mortality Rate or Ventilator-Associated Pneumonia Rate (Crit Care Med, 2007) [MEDLINE]
In Multicenter, Randomized Italian Trial, Early Tracheostomy (Mean: 7 Days) Did Not Decrease the Risk of VAP or Mortality Rate (JAMA, 2010) [MEDLINE]
Early Tracheostomy (Within 10 Days) was Not Associated with Decreased Mortality Rate, ICU Length of Stay, Duration of Mechanical Ventilation, or Incidence of VAP, But was Associated with and Increased Number of Procedures and Shorter Duration of Sedation (Br J Anaesth, 2015) [MEDLINE]
Risk Factors Associated with Early Post-Tracheostomy VAP (Occurring ≤5 Days of Tracheostomy Placement) (Chest, 2000) [MEDLINE]: in this retrospective study, incidence of VAP was 26%, VAP occurred at mean of 9 days post-tracheostomy placement, and overall mortality rate was 33% (VAP increased mortality rate to 54%)
Endotracheal Aspirate with Significant Bacterial Colonization (>100k cfu/mL): the responsible VAP pathogen was present in the endotracheal aspirate on the day of tracheostomy
Fever (≥38.3 C) on Day of Tracheostomy Placement
Requirement for Sedation >24 hrs Post-Tracheostomy
Risk Factors Associated with Late Post-Tracheostomy VAP (Occurring >5 Days of Tracheostomy Placement) (Chest, 2000) [MEDLINE]: in this retrospective study, incidence of VAP was 26%, VAP occurred at mean of 9 days post-tracheostomy placement, and overall mortality rate was 33% (VAP increased mortality rate to 54%)
Duration of Sedation Prior to Tracheostomy
Fever (≥38.3 C) on Day of Tracheostomy Placement
Risk Factors Not Associated with Post-Tracheostomy VAP (Early or Late) (Chest, 2000) [MEDLINE]: in this retrospective study, incidence of VAP was 26%, VAP occurred at mean of 9 days post-tracheostomy placement, and overall mortality rate was 33% (VAP increased mortality rate to 54%)
Arterial pO2/FIO2 Ratio
Duration of Antimicrobial Administration
Duration of Mechanical Ventilation Prior to Tracheostomy
Intensive Care Unit Admitting Diagnosis
Indication for Tracheostomy
Prior Nosocomial Pneumonia
Use of Steroids on the Day of Tracheostomy
Physiologic Mechanisms Which May Contribute to Lower Airway Infection
Aspiration of Oropharyngeal Secretions
Bypass of Upper Airway Filtration Mechanism
Contaminated Equipment/Solutions Used for Respiratory Care
Impaired Tracheal Mucociliary Clearance
Ineffective Cough Clearance of Secretions
Tracheal Wall Mucosal Damage Due to Tracheostomy or Suction Trauma
References
General
Verbal communication of ventilator-dependent patients. Crit Care Med 1993; 21:512-517
Scintigraphic quantification of aspiration reduction with the Passy-Muir valve. Laryngoscope 1996; 106:231-234
Indications
Changes in the work of breathing induced by tracheotomy in ventilator-dependent patients. Am J Respir Crit Care Med. 1999;159(2):383 [MEDLINE]
Changes in respiratory mechanics after tracheostomy. Arch Surg. 1999;134(1):59 [MEDLINE]
Pulmonary mechanics in patients with prolonged mechanical ventilation requiring tracheostomy. Anaesth Intensive Care. 1999;27(6):581 [MEDLINE]
Clinical predictors and outcomes for patients requiring tracheostomy in the intensive care unit. Crit Care Med. 1999;27(9):1714 [MEDLINE]
How is mechanical ventilation employed in the intensive care unit? An international utilization review. Am J Respir Crit Care Med. 2000;161(5):1450 [MEDLINE]
The role of dead space ventilation in predicting outcome of successful weaning from mechanical ventilation. J Trauma. 2001;51(5):843 [MEDLINE]
Effects of tracheotomy on respiratory mechanics in spontaneously breathing patients. Eur Respir J. 2002;20(1):112 [MEDLINE]
Hospital and long-term outcome after tracheostomy for respiratory failure. Chest. 2004;125(1):220 [MEDLINE]
Impact of tracheotomy on sedative administration, sedation level, and comfort of mechanically ventilated intensive care unit patients. Crit Care Med. 2005;33(11):2527 [MEDLINE]
Outcome of mechanically ventilated patients who require a tracheostomy. Crit Care Med. 2005;33(2):290 [MEDLINE]
Systematic review and meta-analysis of studies of the timing of tracheostomy in adult patients undergoing artificial ventilation. BMJ. 2005;330:1243 [MEDLINE]
Relationship between tracheostomy timing and duration of mechanical ventilation in critically ill patients. Crit Care Med. 2005;33(11):2513 [MEDLINE]
Impact of tracheotomy on sedative administration, sedation level, and comfort of mechanically ventilated intensive care unit patients. Crit Care Med. 2005;33(11):2527 [MEDLINE]
Is tracheostomy associated with better outcomes for patients requiring long-term mechanical ventilation? Crit Care Med. 2007;35(3):802 [MEDLINE]
Tracheostomy does not improve the outcome of patients requiring prolonged mechanical ventilation: a propensity analysis. Crit Care Med. 2007;35(1):132 [MEDLINE]
Early vs late tracheotomy for prevention of pneumonia in mechanically ventilated adult ICU patients: a randomized controlled trial. JAMA. 2010;303(15):1483 [MEDLINE]
The timing of tracheotomy in critically ill patients undergoing mechanical ventilation: a systematic review and meta-analysis of randomized controlled trials. Chest 2011;140(6):1456–1465 [MEDLINE]
Early percutaneous tracheotomy versus prolonged intubation of mechanically ventilated patients after cardiac surgery: a randomized trial. Ann Intern Med 2011;154:373–383 [MEDLINE]
Early versus late tracheostomy for critically ill patients. Cochrane Database Syst Rev. 2012 [MEDLINE]
Effect of early vs late tracheostomy placement on survival in patients receiving mechanical ventilation: the TracMan randomized trial. JAMA. 2013;309(20):2121 [MEDLINE]
Effect of Tracheostomy on Weaning Parameters in Difficult-to-Wean Mechanically Ventilated Patients: A Prospective Observational Study. PLoS One. 2015;10(9):e0138294 [MEDLINE]
Effect of early tracheostomy on resource utilization and clinical outcomes in critically ill patients: meta-analysis of randomized controlled trials. Br J Anaesth. 2015;114(3):396 [MEDLINE]
Timing of tracheotomy in ICU patients: a systematic review of randomized controlled trials. Crit Care. 2015;19:424 [MEDLINE]
Hospital Variation in Early Tracheostomy in the United States: A Population-Based Study. Crit Care Med. 2016 Aug;44(8):1506-14 [MEDLINE]
Association between early tracheostomy and patient outcomes in critically ill patients on mechanical ventilation: a multicenter cohort study. J Intensive Care. 2022 Apr 11;10(1):19. doi: 10.1186/s40560-022-00610-x [MEDLINE]
Effect of Early vs Standard Approach to Tracheostomy on Functional Outcome at 6 Months Among Patients With Severe Stroke Receiving Mechanical Ventilation: The SETPOINT2 Randomized Clinical Trial. JAMA. 2022 May 4. doi: 10.1001/jama.2022.4798 [MEDLINE]
Technique
Comparative clinical trial of standard operative tracheostomy with percutaneous tracheostomy. Crit Care Med. 1991;19(8):1018 [MEDLINE]
The safety and efficacy of bedside tracheotomy. Otolaryngol Head Neck Surg. 1993;109(4):707 [MEDLINE]
Comparison between conventional cap and one-way valve in the decannulation of patients with long-term tracheostomies. Respir Care. 1993; 38:1161
The technique of weaning from tracheostomy. Criteria for weaning; practical measures to prevent failure. J Crit Illn. 1995;10(10):729 [MEDLINE]
Some important details in the technique of percutaneous dilatational tracheostomy via the modified Seldinger technique. Chest. 1996;110(3):762 [MEDLINE]
Hypercarbia during tracheostomy: a comparison of percutaneous endoscopic, percutaneous Doppler, and standard surgical tracheostomy. Intensive Care Med. 1997;23(8):859 [MEDLINE]
Tracheostomy tube occlusion protocol predicts significant tracheal obstruction to air flow in patients requiring prolonged mechanical ventilation. Crit Care Med. 1997;25(3):413 [MEDLINE]
Percutaneous dilatational tracheostomy versus conventional surgical tracheostomy. A clinical randomised study. Acta Anaesthesiol Scand. 1998;42(5):545 [MEDLINE]
Posterior tracheal wall perforation during percutaneous dilational tracheostomy: an investigation into its mechanism and prevention. Chest. 1999;115(5):1383 [MEDLINE]
Percutaneous or surgical tracheostomy: a meta-analysis. Crit Care Med. 1999;27(8):1617 [MEDLINE]
A meta-analysis of prospective trials comparing percutaneous and surgical tracheostomy in critically ill patients. Chest. 2000;118(5):1412 [MEDLINE]
Complications of bronchoscopically guided percutaneous dilational tracheostomy: beyond the learning curve. Intensive Care Med. 2002;28(1):59 [MEDLINE]
Safety of percutaneous dilational tracheostomy in patients ventilated with high positive end-expiratory pressure (PEEP). Intensive Care Med. 2003;29(6):944 [MEDLINE]
The utility of chest radiographs following percutaneous dilatational tracheostomy. Chest. 2003;123(5):1603 [MEDLINE]
Weaning from tracheotomy in long-term mechanically ventilated patients: feasibility of a decisional flowchart and clinical outcome. Intensive Care Med. 2003;29(5):845 [MEDLINE]
Percutaneous versus surgical tracheostomy: A randomized controlled study with long-term follow-up. Crit Care Med. 2006;34(8):2145 [MEDLINE]
Percutaneous dilatational tracheostomy versus surgical tracheostomy in critically ill patients: a systematic review and meta-analysis. Crit Care. 2006;10(2):R55 [MEDLINE]
A comparative study of the complications of surgical tracheostomy in morbidly obese critically ill patients. Crit Care. 2007;11(1):R3 [MEDLINE]
Risk factors associated with bleeding during and after percutaneous dilational tracheostomy. Anaesthesia. 2007;62(4):342 [MEDLINE]
Safety and complications of percutaneous tracheostomy in a cohort of 800 mixed ICU patients. Anaesthesia. 2008;63(11):1198 [MEDLINE]
Safety and feasibility of percutaneous tracheostomy performed by neurointensivists. Neurocrit Care. 2009;10(3):264 [MEDLINE]
When to change a tracheostomy tube. Respir Care. 2010 Aug;55(8):1069-75 [MEDLINE]
Predictors of successful decannulation using a tracheostomy retainer in patients with prolonged weaning and persisting respiratory failure. Respiration. 2012;84(6):469-76 [MEDLINE]
Advantages of US in percutaneous dilatational tracheostomy: randomized controlled trial and review of the literature. Radiology. 2014 Dec;273(3):927-36 [MEDLINE]
Incidence of overall complications and symptomatic tracheal stenosis is equivalent following open and percutaneous tracheostomy in the trauma patient. Am J Surg. 2014;208(5):770 [MEDLINE]
The impact of obesity on adult tracheostomy complication rate. Laryngoscope. 2015 Jan;125(1):105-10 [MEDLINE]
The impact of a multidisciplinary safety checklist on adverse procedural events during bedside bronchoscopy-guided percutaneous tracheostomy. J Trauma Acute Care Surg. 2015 Jul;79(1):111-6 [MEDLINE]
Long-Term Outcome Following Tracheostomy in Critical Care: A Systematic Review. Crit Care Med. 2016 Mar;44(3):617-28 [MEDLINE]
Ultrasound-guided percutaneous dilational tracheostomy versus bronchoscopy-guided percutaneous dilational tracheostomy in critically ill patients (TRACHUS): a randomized noninferiority controlled trial. Intensive Care Med. 2016 Mar;42(3):342-51 [MEDLINE]
Use of Bronchoscopy in Percutaneous Dilational Tracheostomy. JAMA Otolaryngol Head Neck Surg. 2016 Feb;142(2):143-9[MEDLINE]
Percutaneous techniques versus surgical techniques for tracheostomy. Cochrane Database Syst Rev. 2016;7:CD008045 [MEDLINE]
Feasibility of a single-stage tracheostomy decannulation protocol with endoscopy in adult patients. Laryngoscope. 2016;126(9):2057 [MEDLINE]
Decannulation
A North American survey of respiratory therapist and physician tracheostomy decannulation practices. Respir Care 2009;54(12):1658-166 [MEDLINE]
Ulcerative tracheo-oesophageal fistula during treatment by tracheostomy and intermittent positive pressure ventilation. Thorax. 1972;27(3):338 [MEDLINE]
Tracheo-innominate artery erosion: Successful surgical management of a devastating complication. Ann Surg. 1976;184(2):194 [MEDLINE]
Tracheostomy and its complications. A retrospective study of 794 tracheostomized patients. Ann Chir Gynaecol. 1981;70(3):96 [MEDLINE]
Tracheoesophageal fistula formation in intubated patients. Risk factors and treatment with high-frequency jet ventilation. Chest. 1990;98(1):161 [MEDLINE]
Importance of verbal communication for the ventilator-dependent patient. Chest. 1990;98(4):792 [MEDLINE]
Swallowing disorders in patients with prolonged orotracheal intubation or tracheostomy tubes. Crit Care Med. 1990;18(12):1328 [MEDLINE]
Late complications of tracheotomy. Clin Chest Med. 1991 Sep;12(3):597-609 [MEDLINE]
Comparison of blue dye visualization and glucose oxidase test strip methods for detecting pulmonary aspiration of enteral feedings in intubated adults. Chest. 1993;103(1):117 [MEDLINE]
Verbal communication of ventilator-dependent patients. Crit Care Med. 1993;21(4):512 [MEDLINE]
Increased frequency of obstructive airway abnormalities with long-term tracheostomy. Chest. 1993;104(1):136 [MEDLINE]
Pulmonary aspiration in mechanically ventilated patients with tracheostomies. Chest. 1994;105(2):563 [MEDLINE]
Management of acquired tracheoesophageal fistula. Chest Surg Clin N Am. 1996 Nov;6(4):819-36 [MEDLINE]
Predisposing factors for nosocomial pneumonia in patients receiving mechanical ventilation and requiring tracheotomy. Chest. 2000;118(3):767 [MEDLINE]
The occurrence of ventilator-associated pneumonia in a community hospital: risk factors and clinical outcomes. Chest. 2001;120(2):555 [MEDLINE]
Complications of bronchoscopically guided percutaneous dilational tracheostomy: beyond the learning curve. Intensive Care Med. 2002;28(1):59 [MEDLINE]
Incidence and type of aspiration in acute care patients requiring mechanical ventilation via a new tracheotomy. Chest. 2002;122(5):1721 [MEDLINE]
Percutaneous dilatational tracheostomy in the ICU: optimal organization, low complication rates, and description of a new complication. Chest. 2003;123(5):1595 [MEDLINE]
Tracheoesophageal fistula. Chest Surg Clin N Am. 2003 May;13(2):271-89 [MEDLINE]
Comparative effects of two ventilatory modes on speech in tracheostomized patients with neuromuscular disease. Am J Respir Crit Care Med. 2003;167(2):114 [MEDLINE]
Clinical ventilator adjustments that improve speech. Chest. 2003;124(4):1512 [MEDLINE]
Tracheal stenosis and obliteration above the tracheostoma after percutaneous dilational tracheostomy. Crit Care Med. 2003;31(5):1574 [MEDLINE]
Tracheostomy tube enabling speech during mechanical ventilation. Chest. 2004;125(3):1046 [MEDLINE]
A prospective, randomized, study comparing early percutaneous dilational tracheotomy to prolonged translaryngeal intubation (delayed tracheotomy) in critically ill medical patients. Crit Care Med. 2004;32(8):1689 [MEDLINE]
Emphysema and pneumothorax after percutaneous tracheostomy: case reports and an anatomic study. Chest. 2004;125(5):1805 [MEDLINE]
Early tracheostomy in intensive care trauma patients improves resource utilization: a cohort study and literature review. Crit Care. 2004;8(5):R347 [MEDLINE]
The incidence of tracheoarterial fistula in patients with chronic tracheostomy tubes: a retrospective study of 544 patients in a long-term care facility. Chest. 2005;128(6):3906 [MEDLINE]
Early tracheostomy versus late tracheostomy in the surgical intensive care unit. Am J Surg. 2005;189(3):293 [MEDLINE]
Secretions, occlusion status, and swallowing in patients with a tracheotomy tube: a descriptive study. Ear Nose Throat J. 2006;85(12):831 [MEDLINE]
A comparative study of the complications of surgical tracheostomy in morbidly obese critically ill patients. Crit Care. 2007;11(1):R3 [MEDLINE]
Review of tracheo-esophageal fistula associated with endotracheal intubation. J Surg Educ. 2007 Jul-Aug;64(4):237-40 [MEDLINE]
Relationship between tracheotomy and ventilator-associated pneumonia: a case control study. Eur Respir J. 2007;30(2):314 [MEDLINE]
Early versus late tracheostomy in patients with severe traumatic head injury. Surg Infect (Larchmt). 2007;8(3):343 [MEDLINE]
Effect of positive expiratory pressure and type of tracheal cuff on the incidence of aspiration in mechanically ventilated patients in an intensive care unit. Crit Care Med. 2008;36(2):409 [MEDLINE]
Tracheostomy tube malposition in patients admitted to a respiratory acute care unit following prolonged ventilation. Chest. 2008;134(2):288 [MEDLINE]
Post tracheostomy and post intubation tracheal stenosis: report of 31 cases and review of the literature. BMC Pulm Med. 2008 [MEDLINE]
Preliminary report of laryngeal phonation during mechanical ventilation via a new cuffed tracheostomy tube. Respir Care. 2010 Dec;55(12):1661-70 [MEDLINE]
A clinical audit of the management of patients with a tracheostomy in an Australian tertiary hospital intensive care unit: Focus on speech-language pathology. Int J Speech Lang Pathol. 2011 Dec;13(6):518-2 [MEDLINE]
Influence of the cuff pressure on the swallowing reflex in tracheostomized intensive care unit patients. Br J Anaesth. 2012 Oct;109(4):578-83 [MEDLINE]
Does removal of tracheostomy affect dysphagia? A kinematic analysis. Dysphagia. 2012 Dec;27(4):498-503 [MEDLINE]
Surgical treatment of nonmalignant tracheoesophageal fistula: a thirty-five year experience. Ann Thorac Surg. 2013 Apr;95(4):1141-6 [MEDLINE]
Optimizing Communication in Mechanically Ventilated Patients. J Med Speech Lang Pathol. 2014;21(4):309-31 [MEDLINE]
Causes and consequences of adult laryngotracheal stenosis. Laryngoscope. 2015 May;125(5):1137-43 [MEDLINE]
The impact of obesity on adult tracheostomy complication rate. Laryngoscope. 2015 Jan;125(1):105-10 [MEDLINE]
Endoscopic closure of acquired oesophagorespiratory fistulas with cardiac septal defect occluders or vascular plugs. Respir Med. 2015 Aug;109(8):1069-78 [MEDLINE]
Split latissimus dorsi muscle flap repair of acquired, nonmalignant, intrathoracic tracheoesophageal and bronchoesophageal fistulas. Heart Lung Circ. 2015 Jun;24(6):e75-8 [MEDLINE]
Return of Voice for Ventilated Tracheostomy Patients in ICU: A Randomized Controlled Trial of Early-Targeted Intervention. Crit Care Med. 2016 Jun;44(6):1075-81 [MEDLINE]
Surgical Management of Benign Acquired Tracheoesophageal Fistulas: A Ten-Year Experience. Ann Thorac Surg. 2016;102(4):1081 [MEDLINE]
Treatment of large persistent tracheoesophageal peristomal fistulas using silicon rings. Braz J Otorhinolaryngol. 2016 Jul [MEDLINE]
A New Modified Evans Blue Dye Test as Screening Test for Aspiration in Tracheostomized Patients. J Cardiothorac Vasc Anesth. 2017;31(2):441 [MEDLINE]
Risk Factors for Posttracheostomy Tracheal Stenosis. Otolaryngol Head Neck Surg. 2018 Aug 21:194599818794456 [MEDLINE]