Place Transducer in Interspace Between the Ribs: assess systematically in 4 anterior chest wall quadrants
Normal Lung Anatomy by Ultrasound
2D Ultrasound
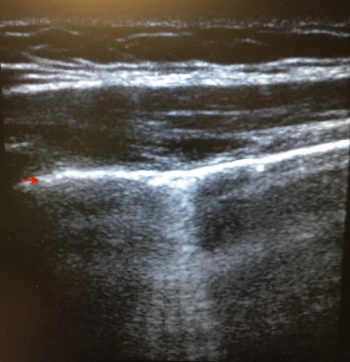
Pleural Line
Definition: bright, shimmering line observed approximately 0.5 cm deep to the rib cortex
Lung Sliding
Definition: sliding appearance at interface between visceral and parietal pleura, indicating that the lung is inflated and moving (during tidal ventilation)
Technique
In a Mechanically Ventilated Patient, Increase the Tidal Volume to Accentuate Visualization of Lung Sliding
Decrease the Gain and Depth to Accentuate Visualization of Lung Sliding
Lung Sliding May Be Less Apparent at the Apices: however, even the slightest movement is significant (“All or Nothing” Rule)
Etiology-Lung Sliding Present
Normal
Etiology-Lung Sliding Absent
Pneumothorax (see Pneumothorax): absence of lung sliding alone has 100% sensitivity/78% specificity for pneumothorax [MEDLINE]
Diaphragmatic Paralysis
Endobronchial Obstruction
Post-Pleurodesis/Pleural Adhesions
Lung Pulse
Definition: phasic sliding of interface between visceral and parietal pleura due to cardiac motion
A-Lines
Definition: equally-spaced parallel horizontal lines within the lung (seen at a multiple of distance from the pleural line to the skin, parellel to the pleural line)
A-Lines Represent a Reverberation Artifact: they are observed in normal lung, diseased lung, and pneumothorax
Presence of A-Lines Over the Entire Chest (Unilateral or Bilateral) Rules Out Cardiogenic Pulmonary Edema: presence of such an A-line pattern indicates that the PCWP <18 mm Hg [MEDLINE]
B-Lines
Definition: perpendicular, vertical lines extending from the pleural line to bottom of the ultrasound screen
A-Lines Transform into B-Lines (at the Anterior Chest Wall) with PCWP >18 (Chest, 2009) [MEDLINE]
B-Lines are Generated by the Visceral and Not the Parietal Pleura: therefore, the presence of B-lines indicates that the lung is inflated, as they are not visible in the presence of pneumothorax (Intensive Care Med, 1999) [MEDLINE]
Move with Lung Sliding: presence of B-lines indicates that the lung is inflated
Extend to the Bottom Edge of the Ultrasound Screen without Fading (“Lung Rockets”, “Comet Tails”)
Well-Defined (Laser Beam-Like)
Number of B-Lines
More Than 3 B-Lines Per Field is Abnormal: normal patients can have a few B-lines over the lower lateral chest and occasionally single B-lines in other locations
Spacing of B-Lines
B-Lines 7 mm Apart (B7 Lines) Represent Thickened Interlobular Septae (Equivalent to Kerley B Lines) [MEDLINE]
Clinical Correlate: Z-Lines have no pathologic significance
Found in Both Normal Patients and in Pneumothorax
O Line Pattern
Definition: absence of both A-lines and B-lines
Curtain Sign
Definition: sudden loss of deeper anatomic structures when the lung interposes itself (due to respiratory motion) between the probe and the deeper tissue
This is a Normal Finding Generally Observed When Imaging the Upper Abdomen Above the Lower Limit of the Pleura
M-Mode Ultrasound
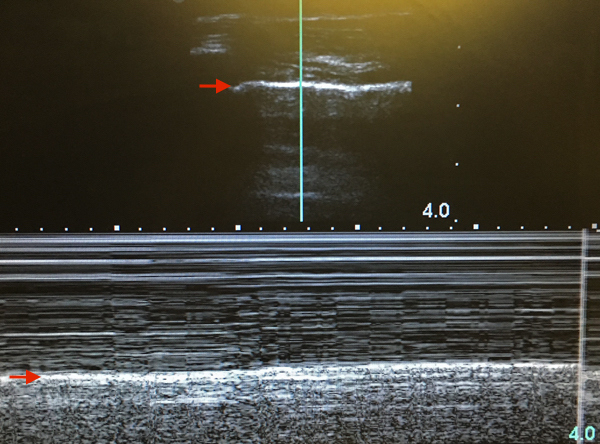
“Seashore Sign”: the presence of seashore sign rules out the presence of a pneumothorax
Wavelike Pattern Above the Pleural Line: pleural line is indicated by the red arrow
Sandlike Pattern Below the Pleural Line (Produced by Movement of the Lung Below the Pleural Line): pleural line is indicated by the red arrow
Evaluation for Alveolar/Interstitial Lung Abnormalities
2D Ultrasound Features
A-Lines
Presence of A-Lines Over the Entire Chest (Unilateral or Bilateral) Rules Out Cardiogenic Pulmonary Edema: presence of such an A-line pattern indicates that the PCWP <18 mm Hg and probably <12 mm Hg (Chest, 2009) [MEDLINE]
Diffuse B-Line Pattern with Smooth Pleural Line: indicates the presence of cardiogenic pulmonary edema
Diffuse B-Line Pattern with Rough Pleural Line: indicates the presence of ARDS, ILD, or pneumonia
B-line distribution is heterogeneous with small subpleural areas of lung consolidation
Consolidated Lung: appears similar in density to liver and spleen
Air Bronchograms: may be seen as punctate echogenic foci within the consolidated lung
If they move in synchrony with the respiratory cycle, the bronchus supplying the area is patent
E-Lines (E = Emphysema)
E-Lines Arise from Superficial Collections of Parietal/Subcutaneous Emphysema
Features of E-Lines
Arise From Above the Pleural Line
Pleural Line is Not Visible
Spreads to the Bottom Edge of the Ultrasound Screen without Fading
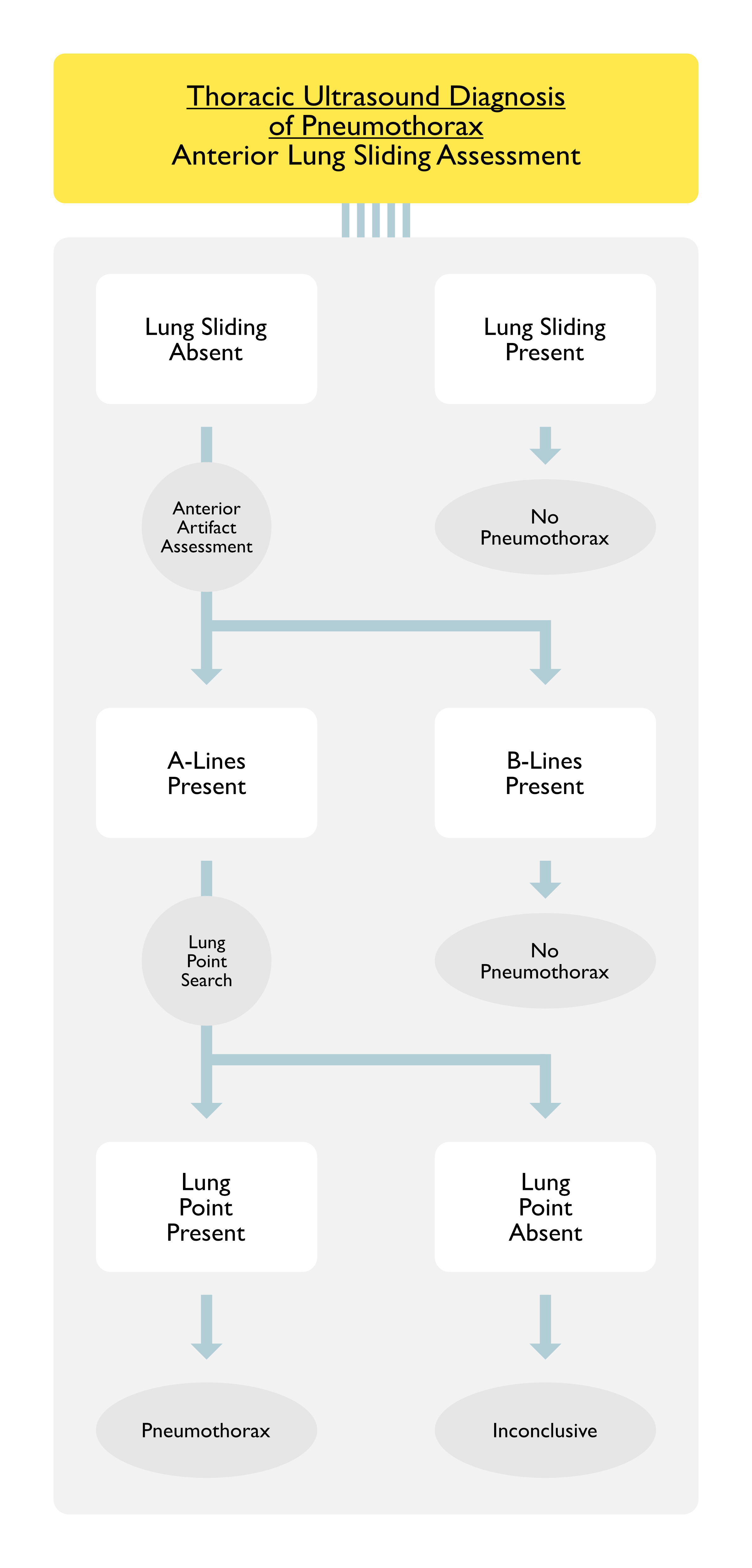
Evaluation for Pneumothorax
General Evaluation
Location of Assessment: several areas of chest should be assessed when pneumothorax is suspected, especially areas where air would likely accumulate (anterior-superior and lateral chest wall)
General Clinical Data
Prospective Study of the Sensitivity/Specificity of Thoracic Ultrasound for Traumatic Pneumothorax in the ED (Chest, 2008) [MEDLINE]
Gold Standard for Diagnosis of Traumatic Pneumothorax in the Study was Spiral CT
Thoracic Ultrasound Had a Sensitivity of 92%/Specificity of 99.4% for the Diagnosis of Traumatic Pneumothorax in the ED
Chest X-Ray Had a Sensitivity of 52%/Specificity of 100% for the Diagnosis of Traumatic Pneumothorax in the ED
2D Ultrasound Features Which Indicate Pneumothorax
Absence of Lung Sliding and Lung Pulse
Presence of Lung Sliding and Lung Pulse: rules out the presence of pneumothorax
Presence of Lung Sliding and B-Lines Has a 100% Negative Predictive Value for Ruling Out Pneumothorax (in the Area of the Probe) [MEDLINE] [MEDLINE]
Presence of Lung Point: intermittent visualization of lung sliding from mobile partially collapsed lung -> sliding part of lung comes on/off of the screen
Sensitivity: the sensitivity of lung point for pneumothorax is inversely proportional to the size of the pneumothorax: since a large pneumothorax would prevent lung parenchyma from opposing the chest wall
Specificity: lung point has a 100% specificity for pneumothorax -> lung point is diagnostic of pneumothorax [MEDLINE]
Presence of A-Lines: since A-lines are observed in normal lung, diseased lung, and pneumothorax
Absence of B-Lines
B-Lines are Generated by the Visceral and Not the Parietal Pleura: therefore, the presence of B-lines indicates that the lung is inflated, as they are not visible in the presence of pneumothorax (Intensive Care Med, 1999) [MEDLINE]
Presence of Lung Sliding and B-Lines Has a 100% Negative Predictive Value for Ruling Out Pneumothorax (in the Area of the Probe) [MEDLINE] [MEDLINE]
M-Mode Ultrasound Features Which Indicate Pneumothorax
Presence of “Stratosphere Sign” (Also Called the “Bar Code” Sign): strictly horizontal lines replace the normal granular (sandy) pattern of the lung, indicating the presence of gas below the pleural line
Specificity: the stratosphere sign is not specific to pneumothorax
Presence of “Seashore Sign”: rules out pneumothorax
Presence of Lung Point: abrupt transition from seashore sign to stratosphere sign
Thoracic Ultrasound is More Sensitive than Chest X-Ray for the Diagnosis of Rib Fractures
References
Radiology in heart disease. Br Med J 1933; 2:594 [MEDLINE]
A bedside ultrasound sign ruling out pneumothorax in the critically ill. Lung sliding. Chest 1995;108(5):1345-1348 [MEDLINE]
The comet-tail artifact: An ultrasound sign of alveolar-interstitial syndrome. Am J Respir Crit Care Med 1997; 156:1640-1646 [MEDLINE]
The comet-tail artifact, an ultrasound sign ruling out pneumothorax. Intensive Care Med 1999; 25:383–388 [MEDLINE]
The “lung point”: an ultrasound sign specific to pneumothorax. Intensive Care Med 2000; 26:1434-1440 [MEDLINE]
Ultrasonic examination: an alternative to chest radiography after central venous catheter insertion? Am J Respir Crit Care Med. 2001;164(3):403-405 [MEDLINE]
Ultrasound diagnosis of occult pneumothorax. Crit Care Med 2005; 33(6):1231-1238 [MEDLINE]
Ultrasound comet-tail images: a marker of pulmonary edema: a comparative study with wedge pressure and extravascular lung water. Chest 2005;127(5):1690-1695 [MEDLINE]
Pleural ultrasonography. Clin Chest Med 2006; 27:215-227 [MEDLINE]
Clinical review: bedside lung ultrasound in critical care practice. Crit Care 2007; 11:205 [MEDLINE]
Relevance of lung ultrasound in the diagnosis of acute respiratory failure: the BLUE protocol. Chest 2008;134(1):117-125 [MEDLINE]
Occult traumatic pneumothorax: diagnostic accuracy of lung ultrasonography in the emergency department. Chest. 2008 Jan;133(1):204-11. Epub 2007 Oct 9 [MEDLINE]
A-lines and B-lines: lung ultrasound as a bedside tool for predicting pulmonary artery occlusion pressure in the critically ill. Chest. 2009;136(4):1014-1020 [MEDLINE]
Pleural procedures and thoracic ultrasound: British Thoracic Society Pleural Disease Guideline. Thorax 2010; 65(Suppl 2):ii61-ii76 [MEDLINE]
Lung ultrasound: a new tool for the emergency physician. Intern Emerg Med. 2010 Aug;5(4):335-40. doi: 10.1007/s11739-010-0381-x. Epub 2010 May 5 [MEDLINE]
Thoracic Ultrasonography for the Pulmonary Specialist. Chest 2011; 140(5):1332–1341 [MEDLINE]
Sonographic diagnosis of pneumothorax. Intensive Care Med 2011; 37:224-232 [MEDLINE]
Clinical applications of bedside ultrasonography in internal and emergency medicine. Intern Emerg Med 2011 Jun;6(3):195-201. doi: 10.1007/s11739-010-0424-3. Epub 2010 Aug 3 [MEDLINE]
Can chest ultrasonography substitute standard chest radiography for evaluation of acute dyspnea in the emergency department? Chest 2011; 139(5):1140-1147 [MEDLINE]
Lung ultrasound in the ICU: From diagnostic instrument to respiratory monitoring tool. Minerva Anestesiol 2012; 78:1282-1296 [MEDLINE]
Thoracic ultrasound. Emerg Med Clin North Am. 2012 May;30(2):451-73, ix. doi: 10.1016/j.emc.2011.12.003 [MEDLINE]
Pneumothorax in the critically ill patient. Chest 2012; 141:1098-1105 [MEDLINE]
Lung ultrasound in the critically ill. Ann Intensive Care. 2014;4:1 [MEDLINE]
Bedside ultrasonography for the intensivist. Crit Care Clin. 2015 Jan;31(1):43-66. doi: 10.1016/j.ccc.2014.08.003. Epub 2014 Oct 3 [MEDLINE]
BLUE-protocol and FALLS-protocol: two applications of lung ultrasound in the critically ill. Chest. 2015;147(6):1659-1670 [MEDLINE] 26033127
From FAST to E-FAST: an overview of the evolution of ultrasound-based traumatic injury assessment. Eur J Trauma Emerg Surg. 2016 Apr;42(2):119-26. doi: 10.1007/s00068-015-0512-1. Epub 2015 Mar 14 [MEDLINE]