Cardiogenic Shock/Severe Congestive Heart Failure (CHF) (see Cardiogenic Shock)
Arrhythmogenic
Cardiomyopathic
Mechanical
Obstructive Shock
Mechanical
Pulmonary Vascular
Management of Cardiogenic Shock
Clinical Efficacy
Systematic Review of Impact of Use of Swan-Ganz Catheter in the Management of Cardiogenic Shock (J Crit Care, 2022) [MEDLINE]; n = 1,166,762 (from 6 observational studies)
The Most Frequent Etiology of Cardiogenic Shock was Post-Myocardial Infarction (75% [95% CI 55-89%] in Swan-Ganz Catheter Group and 81%[95% CI 47-95%] in Non-Swan-Ganz Catheter Group)
Overall, Swan-Ganz Catheter was uUed in 33% (95% CI 24-44%) of Cases
Pooling Data Adjusted for Confounders, a Significant Association Between the Swan-Ganz Catheter Group and a Reduction in Short-Term Mortality Emerged When Compared to the Nn-Swan-Ganz Catheter Group (36% [95% CI 27-45%] vs 47% [95% CI 35-59%]; Adjusted Odds Ratio 0.71, 95% CI 0.59-0.87, p < 0.01)
Mechanical Circulatory Support Use was Significantly Higher in Swan-Ganz Catheter vs Non-Swan-Ganz Catheter Group (59% [95% CI 54-65%]) vs 48% [95% CI 43-53%]); Odds Ratio 1.60 [95% CI 1.27-2.02, p < 0.01])
Perioperative Optimization/Operative Management of Hemodynamics for High-Risk Non-Cardiac Surgery (see Hemodynamics)
Surgical Procedures (Especially in Patients with Suboptimal Cardiac Function)
Pneumonectomy
Clinical Efficacy
Systematic Review and Meta-Analysis of Swan-Ganz Catheter in the Outcome of Moderate to High-Risk Surgical Patients (Anesth Analg, 2011) [MEDLINE]
Preemptive Strategy of Swan-Ganz Catheter Hemodynamic Monitoring and Coupled Therapy Decreased Surgical Mortality and Morbidity
Research Purposes
xxx
Ventricular Pacing
When Using a Swan-Ganz Catheter with Pacing Capabilities
General Principles of the Swan-Ganz Catheter
Swan-Ganz Catheter is Used to Measure Hemodynamic Parameters (see Hemodynamics)
Cardiac Output (CO)
Pulmonary Artery-Systolic Pressure (PA-Systolic Pressure) and Pulmonary Artery-Diastolic Pressure (PA-Diastolic Pressure): these are used to derive the pulmonary artery-mean pressure (PA-Mean Pressure)
Central Venous Pressure (CVP)
Pulmonary Capillary Wedge Pressure (PCWP)
Swan-Ganz Catheter-Derived Data and Mean Arterial Pressure are Subsequently Utilized to Calculate Hemodynamic Parameters (see Hemodynamics)
Systemic Vascular Resistance (SVR)
Pulmonary Vascular Resistance (PVR)
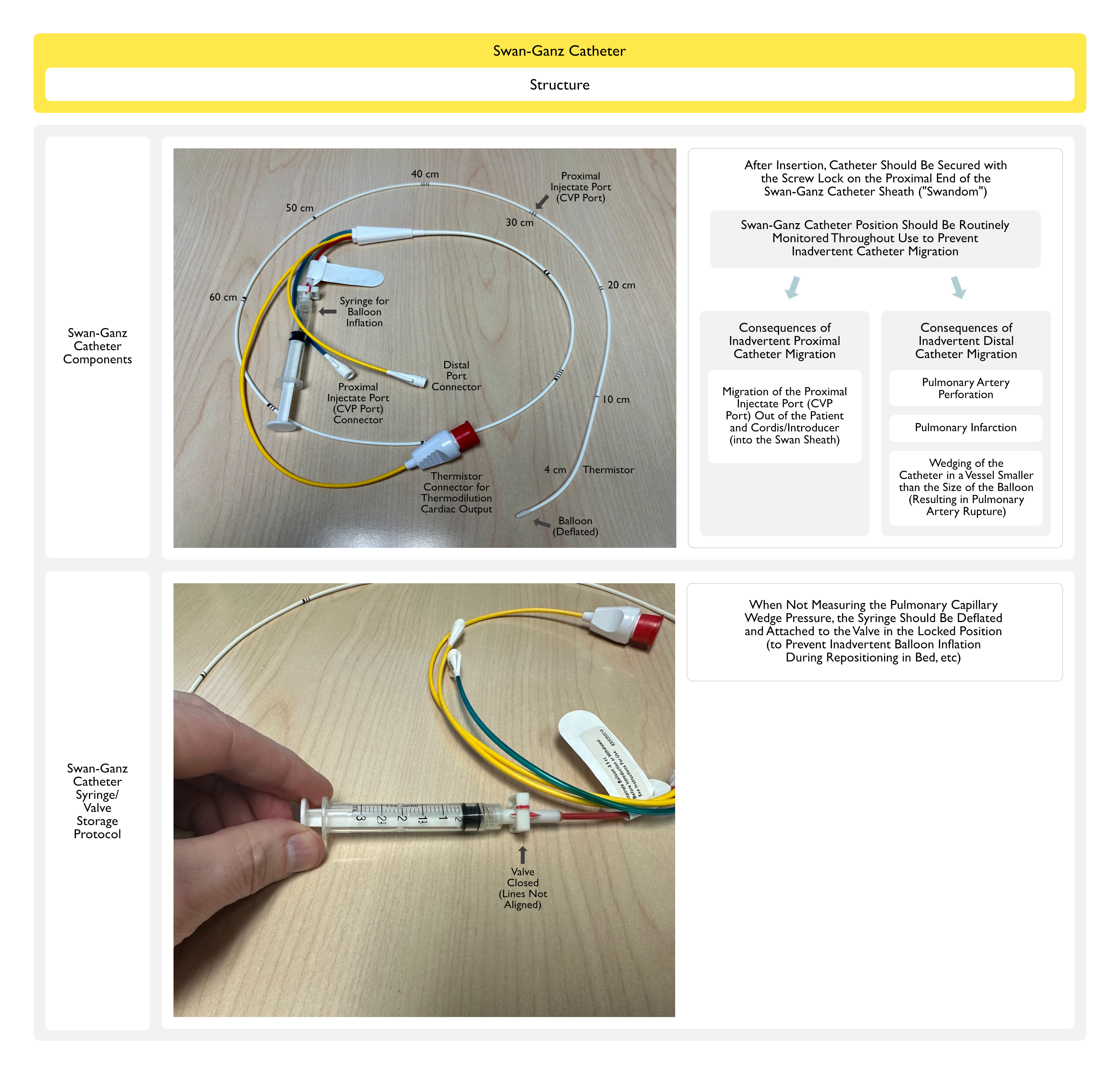
Swan-Ganz Catheter Structure
Catheter and Lumens: PA catheter is an approximate 110 cm radiopaque polyvinylchloride catheter with 2-3 internal lumens
The distal lumen terminates at the tip of the catheter (Distal Port)
The proximal lumen terminates at about 30 cm from the tip (Proximal Port)
An optional third lumen terminates at about 20-30 cm from the tip
Thermistor: PA catheter has a thermistor device approximately 3-5 cm from the tip
Thermistor measures temperature and allows calculation of cardiac output (by thermodilution technique) and sometimes RV ejection fraction
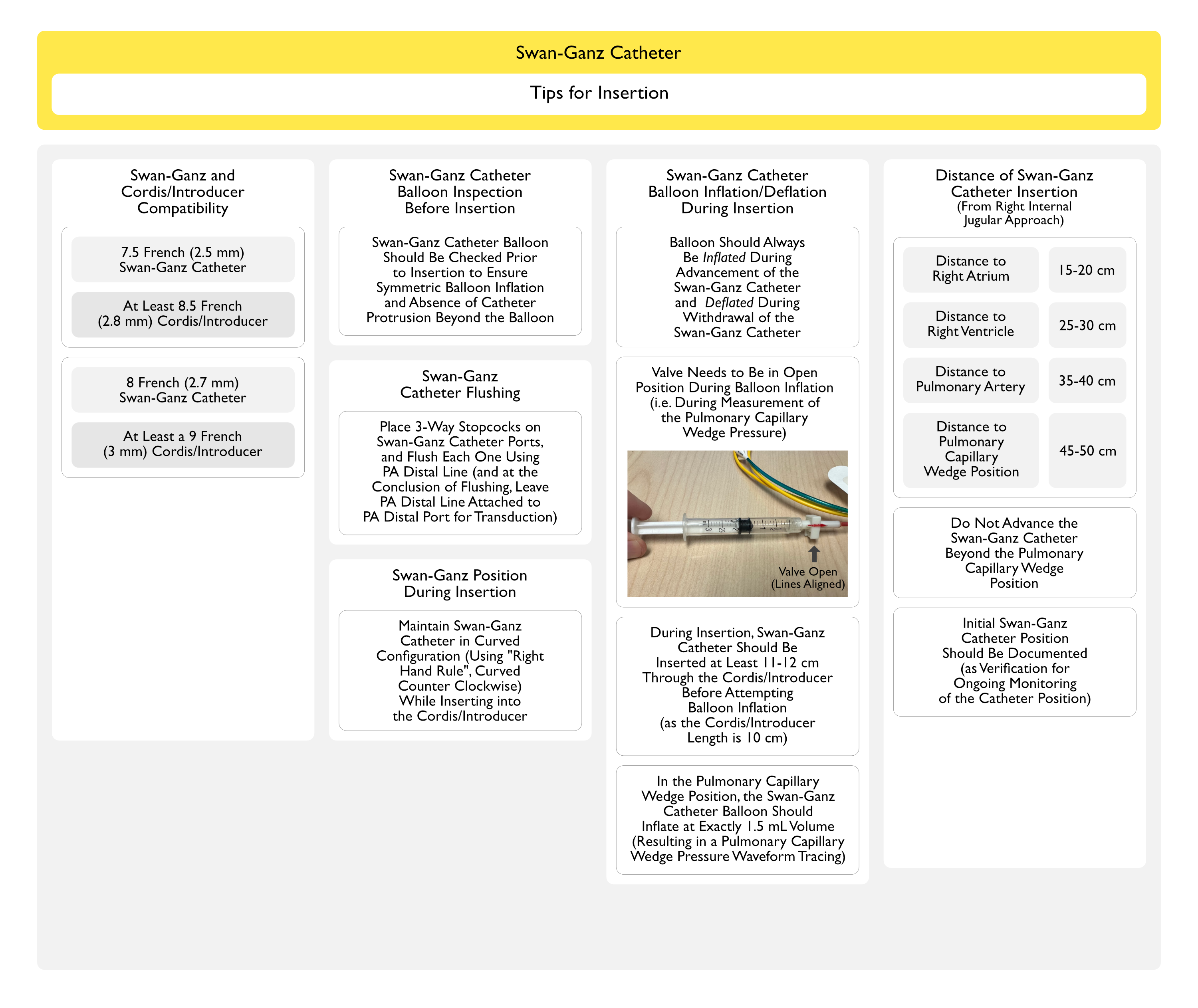
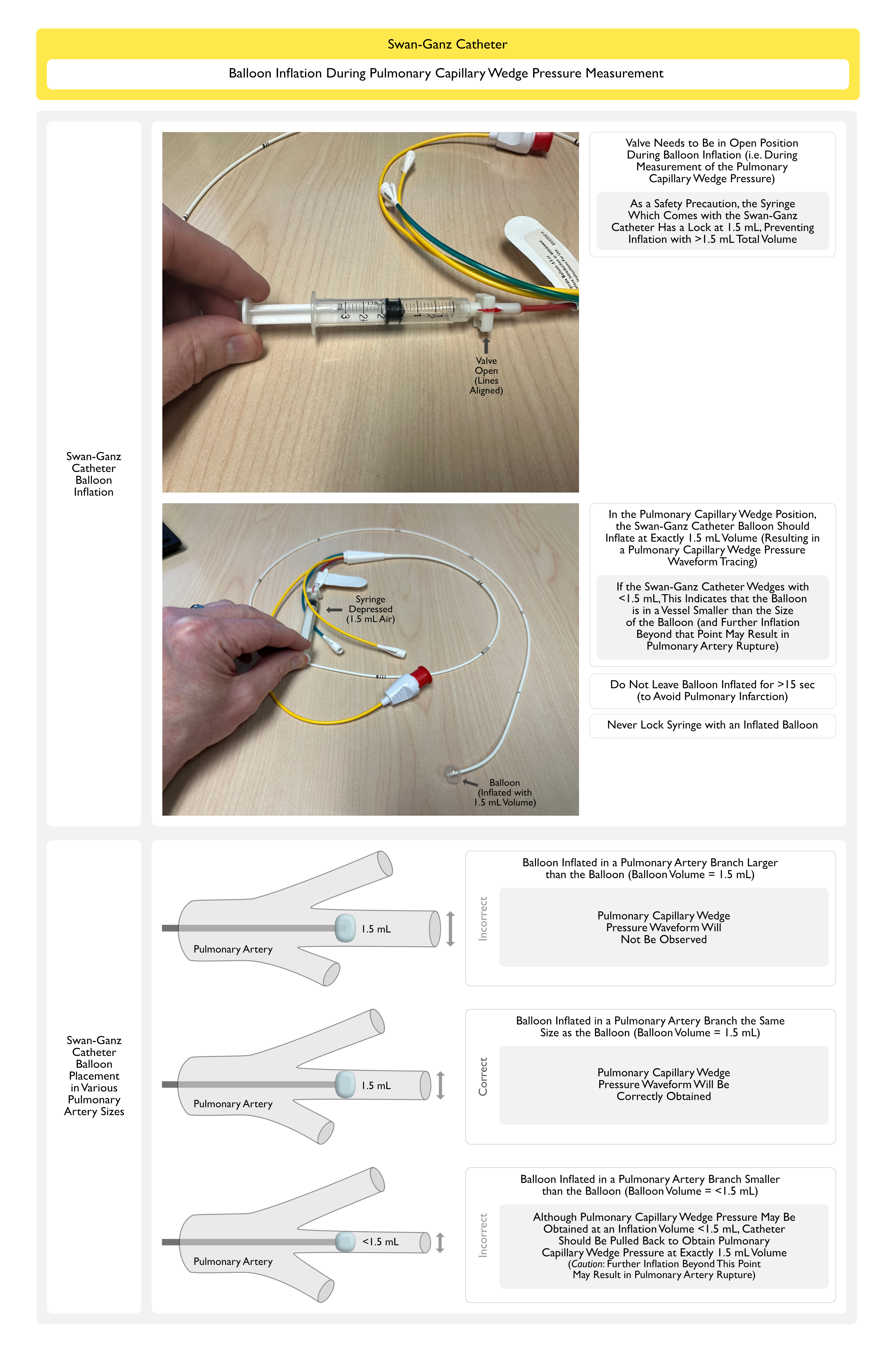
Balloon: 1.5 inflatable balloon is located near the tip of the catheter
Balloon guides passage and occludes the pulmonary capillary when catheter is “wedged”
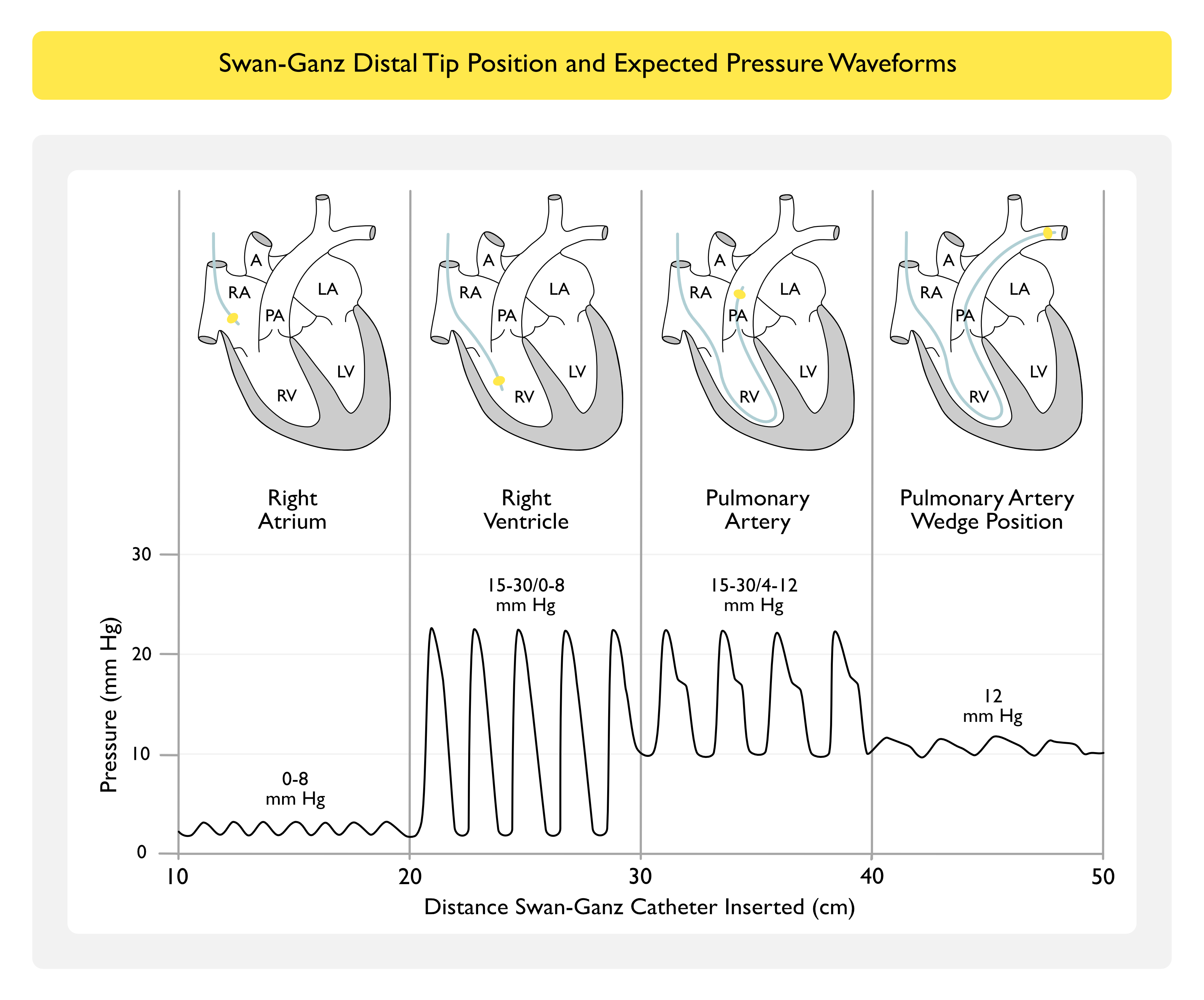
Circulatory Anatomy and Pressure Waveforms from the Swan-Ganz Catheter
Normal Pressure Values
Right Atrial Pressure (RA)/Central Venous Pressure (CVP): 0-8 mm Hg
Right Ventricular Pressure (RV): 15-30 mm Hg/ 0-8 mm Hg
Pulmonary Artery Systolic Pressure (PA-Systolic): 15-30 mm Hg
Pulmonary Artery Diastolic Pressure (PA-Diastolic): 4-12 mm Hg
Pulmonary Artery Mean Pressure (PA-Mean): 9-16 mm Hg
Pulmonary Capillary Wedge Pressure (PCWP): 12 mm Hg
By Convention, the Pulmonary Capillary Wedge Pressure (PCWP) is Measured at End-Expiration
For a Patient Not on the Ventilator, End-Expiration Corresponds to the Highest Point in the Respiratory Cycle (Since Intrathoracic Pressure Decreases During Inspiration While Spontaneously Ventilating)
For a Patient on a Positive-Pressure Ventilator (“Vent = Valley”), End-Expiration Corresponds to the Lowest Point in the Respiratory Cycle (Since Intrathoracic Pressure Increases During Inspiration on While on Positive-Pressure Ventilation)
Note: the Pulmonary Capillary Wedge Pressure (PCWP) is Always Less than the PA-Mean Pressure and is Usually Less than the PA-Diastolic Pressure (Unless Large “v” Waves are Present, Due to Mitral Regurgitation, etc)
Pressure Transduction with the Swan-Ganz Catheter
Lumens of PA Catheter: connected to pressure transducers, which provide continuous pressure tracings of RA pressure and PA pressure
Balloon Inflation (“wedging the catheter”): causes migration of catheter tip into a pulmonary capillary -> PA pressure waveform changes to the Pulmonary Capillary Wedge Pressure (PCWP) waveform
Measurement of Cardiac Output (CO) with the Swan-Ganz Catheter
Thermodilution Method
Technique: utilizes thermistor on end of Swan-Ganz catheter to measure clearance of cold, injected saline (clearance is proportional to the blood flow rate) -> thermodilution method (based on principles developed by Fick in the late Nineteenth Century) utilizes the temperature change after injection as a function of CO
When the CO is high, the injectate is rapidly dispersed and the area under the curve is small -> therefore, area under the thermodilution curve is inversely related to the CO value
Variability: variability in CO calculations by thermodilution is approximately 10% (thus, changes in CO should generally be on the order of 15% to be regarded as valid)
Falsely Decreased CO
Tricuspid Regurgitation (TR) (see Tricuspid Regurgitation): local “recirculation” of injectate -> mimics slow injectate clearance
Low Cardiac Output State: injectate can disperse into the surrounding tissue, mimics rapid injectate clearance
Erroneously Low Injectate Volume
Early Recirculation on Thermodilution Curve: suggests presence of L->R intracardiac shunt
“Continuous” Cardiac Output Measurement: PA catheters with capability to measure CO “continuously” (actually averages the CO over a few minute window) are commercially available
Inadvertent Distal Migration of Swan-Ganz Catheter
Prevention
Deflate the Balloon After Wedging
Evacuate Air from the Syringe and Close Valve After Measuring the Pulmonary Capillary Wedge Pressure (to Prevent Inadvertent Balloon Inflation)
References
Indications
Cardiac Surgery
Use of pulmonary artery catheter in coronary artery bypass graft. Costs and long-term outcomes. PLoS One. 2015 Feb 17;10(2):e0117610. doi: 10.1371/journal.pone.0117610 [MEDLINE]
Prognostic implications of pulmonary artery catheter monitoring in patients with cardiogenic shock: A systematic review and meta-analysis of observational studies. J Crit Care. 2022 Mar 25;69:154024. doi: 10.1016/j.jcrc.2022.154024 [MEDLINE]
General
Inaccuracy of cardiac output by thermodilution during acute tricuspid regurgitation. Ann Thorac Surg 1992; 53:706-708 [MEDLINE]
The thermodilution method for the clinical assessment of cardiac output. Intensive Care Med 1995; 21:691-697 [MEDLINE]
The effectiveness of right heart catheterization in the initial care of critically ill patients. SUPPORT Investigators. JAMA 1996; 276:889–897 [MEDLINE]
Magder S. Cardiac output. In: Tobin MS, ed. Principles and practice of intensive care monitoring. New York: McGraw-Hill, 1998; 797-810
A randomised, controlled trial of the pulmonary artery catheter in critically ill patients. Intensive Care Med 2002; 28:256–264 [MEDLINE]
Predicting fluid responsiveness in ICU patients: A critical analysis of the evidence. Chest 2002; 121:2000–2008 [MEDLINE]
French Pulmonary Artery Catheter Study Group: Early use of the pulmonary artery catheter and outcomes in patients with shock and acute respiratory distress syndrome: A randomized controlled trial. JAMA 2003; 290:2713–2720 [MEDLINE]
Impact of the pulmonary artery catheter in critically ill patients: Meta-analysis of randomized clinical trials. JAMA 2005; 294:1664–1670 [MEDLINE]
PAC-Man study collaboration: Assessment of the clinical effectiveness of pulmonary artery catheters in management of patients in intensive care (PAC-Man): A randomised controlled trial. Lancet 2005; 366:472–477 [MEDLINE]
Pulmonary-artery versus central venous catheter to guide treatment of acute lung injury. N Engl J Med 2006; 354:2213–2224 [MEDLINE]
Does central venous pressure predict fluid responsiveness? A systematic review of the literature and the tale of seven mares. Chest 2008; 134:172–178 [MEDLINE]
Fluid therapy in resuscitated sepsis: Less is more. Chest 2008; 133:252–263 [MEDLINE]
Functional hemodynamic monitoring and dynamic indices of fluid responsiveness. Minerva Anestesiol 2008; 74:123–135 [MEDLINE]
A systematic review and meta-analysis on the use of preemptive hemodynamic intervention to improve postoperative outcomes in moderate and high-risk surgical patients. Anesth Analg 2011; 112:1392–1402 [MEDLINE]
Surviving sepsis campaign: international guidelines for management of severe sepsis and septic shock: 2012. Crit Care Med. 2013 Feb;41(2):580-637. doi: 10.1097/CCM.0b013e31827e83af [MEDLINE]
Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016. Intensive Care Med. 2017 Jan 18. doi: 10.1007/s00134-017-4683-6 [MEDLINE]