Commercially Available Low Molecular Weight Heparins are Derived from Unfractionated Heparin by Chemical or Enzymatic Depolymerization
Low Molecular Weight Heparins are Chemically and Pharmacokinetically Distinct from Each Other
Advantages of Low Molecular Weight Heparins Over Unfractionated Heparin
Low Molecular Weight Heparins Have Greater Bioavailability than Unfractionated Heparin
Low Molecular Weight Heparins Have Been Extensively Used Via the Subcutaneous Route: allows for outpatient administration
Low Molecular Weight Heparins Have a Greater Duration of Action than Unfractionated Heparin: allows for once-twice daily dosing
Low Molecular Weight Heparins Have a Better Correlation Between Dose and Anticoagulant Response: allows for fixed dosing without monitoring
Low Molecular Weight Heparins Have a Generally Lower Risk of Heparin-Induced Thrombocytopenia than Unfractionated Heparin (see Heparin-Induced Thrombocytopenia)
Low Molecular Weight Heparins Have a Lower Incidence of Osteoporosis (see Osteoporosis)
Disadvantages of Low Molecular Weight Heparins, as Compared to Unfractionated Heparin
Low Molecular Weight Heparins Have a Slightly Delayed Onset of Action (20-30 min), as Compared to the Instantaneous Onset of Action of Unfractionated Heparin
Low Molecular Weight Heparins Have a Longer Duration of Action, Making Discontinuation of Therapy More Difficult
Low Molecular Weight Heparins are Less Easily Activated with Protamine Sulfate (see Protamine)
Low Molecular Weight Heparins Have a Prolonged Half-Life in Patients with Renal Failure (Especially with Enoxaparin)
If Monitoring is Required for Low Molecular Weight Heparin Use, Anti-Factor Xa Activity Testing with a Rapid Turnaround Time May Not Be Available at All Institutions
Enoxaparin (and All Heparins) Act by Binding to Antithrombin (Previously Called Antithrombin III, Also Known as Heparin Cofactor I)
Binding to Antithrombin is Mediated by a Pentasaccharide Sequence Which is Randomly Distributed Along the Heparin Chains
Binding of Heparins to Antithrombin Induces a Conformational Change in Antithrombin, Resulting in Conversion to a More Rapid Inactivator of Coagulation Factors (Thrombin/Factor IIa and Factor Xa): the enhancement of antithrombin activity is approximately 1000-4000 fold
While Both Unfractionated Heparin and Low Molecular Weight Heparins Efficiently Inactivate Factor Xa, Unfractionated Heparin is a More Efficient Inactivator of Thrombin/Factor IIa
Fondaparinux is a Pure Anti-Factor Xa Inhibitor
Metabolism
Hepatic: low molecular weight heparins are metabolized in the liver and excreted by the kidneys
CrCl <30 mL/min: may lead to significantly increased plasma levels of low molecular weight heparins
Enoxaparin does not cross the placenta, making it the anticoagulant of choice in pregnancy
Use in Breastfeeding
Low molecular weight heparins do not accumulate in breast milk
Therapeutic/Full-Dose Anticoagulation
SQ: 1 mg/kg q12hrs
Dose Adjustment for Organ Dysfunction
Hepatic: xxx
Renal: xxx
Enoxaparin Dosing in the Setting of Obesity (see Obesity)
Therapeutic Enoxaparin Dosing in the Setting of Morbid Obesity
Proposed Enoxaparin Dosing Regimen in Morbid Obesity (NEJM, 2014) [MEDLINE]
Dose for Body Mass Index (BMI) >40 or Weight >200 kg (441 lbs) = 0.75 mg/kg (Actual Body Weight)
Monitoring of Anti-Factor Xa Activity Level When Using Therapeutic Enoxaparin in the Setting of Morbid Obesity (see Anti-Factor Xa Activity)
Anti-Factor Xa Activity Level Monitoring Should Be Considered in the Setting of Morbid Obesity (Especially for Body Weight >150 kg), Due to Variable Absorption
Measure Anti-Factor Xa Activity Level 4 hrs After the Enoxaparin Dose
Factor Xa Activity Level is Inversely Proportional to the Amount of Heparin or Other Factor Xa Inhibitor Present in the Plasma
Therapeutic Range Factor Xa Assay (When Measured 4-6 hrs After Injection): 0.5-1.0 anti-Xa units/mL
When Using the Enoxaparin Factor Xa Assay, a High Value (i.e. Greater than the Therapeutic Range: 0.5-1.0 Units/mL) Indicates that the Enoxaparin Dose Should Be Decreased
Deep Venous Thrombosis (DVT) Prophylaxis Enoxaparin Dosing in the Setting of Obesity
Literature Review of Enoxaparin Dosing for Patients at Extremes of Weight (Ann Pharmacother, 2018) [MEDLINE]
Low Body Weight Patients May Benefit from Enoxaparin 30 mg SQ qday for Venous Thromboembolism Prophylaxis, and Standard Weight-Based Dosing for Venous Thromboembolism Treatment
In Patients with BMI ≥40 kg/m2, Enoxaparin 40 mg SQ BID is Recommended for Venous Thromboembolism Prophylaxis
In Patients with BMI ≥50 kg/m2, Consideration Should Be Given for Higher Doses for Venous Thromboembolism Prophylaxis
Enoxaparin does not cross the placenta, making it the anticoagulant of choice in pregnancy
Enoxaparin Use During Breast Feeding
Low Molecular Weight Heparins Do Not Accumulate in Breast Milk
Effect of Enoxaparin on Anticoagulation Tests
Prothrombin Time (PT)/International Normalized Ratio (INR) (see Prothrombin Time): no effect
Enoxaparin is an indirect thrombin inhibitor and should theoretically prolong the INR: however, most INR assay reagents contain heparin-binders which block the effect of heparin (or similar agents) at concentrations <1 unit/mL -> therefore, at heparin concentration of >1 unit/mL, the INR may be prolonged
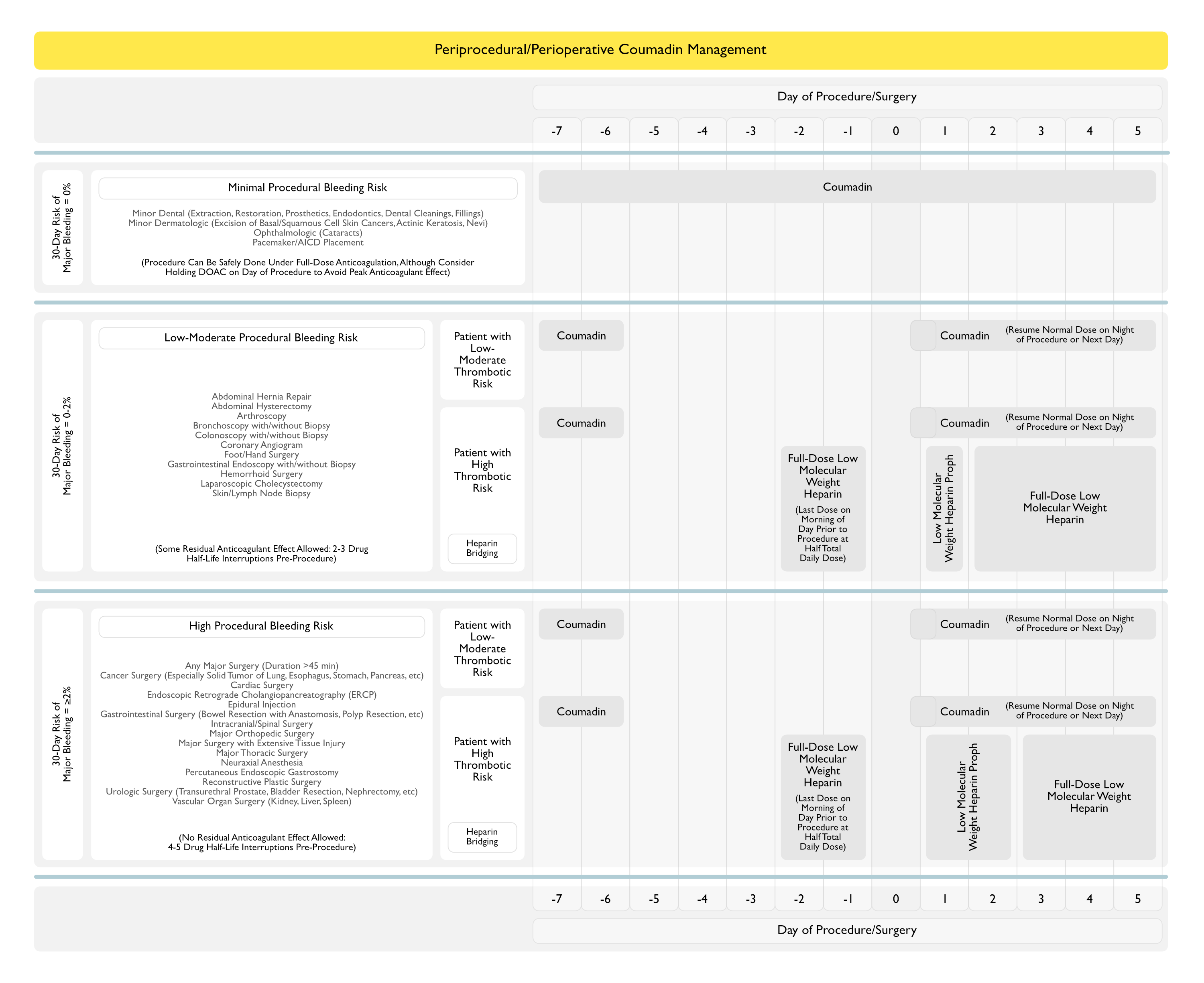
Periprocedural/Perioperative Management of Enoxaparin Anticoagulation
Recommendations for Periprocedural/Perioperative Management of Coumadin (American College of Chest Physicians Clinical Practice Guideline for the Perioperative Management of Antithrombotic Therapy) (Chest, 2022) [MEDLINE]
In Patients Receiving Low Molecular Weight Heparin (as Part of Bridging Regimen or Not) for an Elective Procedure/Surgery, Administer the Last Preprocedure/Preoperative Low Molecular Weight Heparin Dose Approximately 24 hrs Before the Elective Procedure/Surgery (as Opposed to Administering the Last Dose 10-12 hrs Before the Elective Procedure/Surgery (Conditional Recommendation, Very Low Certainty of Evidence)
In Patients Receiving Low Molecular Weight Heparin (as Part of Bridging Regimen or Not) for an Elective Procedure/Surgery, Administer the First Postprocedure/Postoperative Low Molecular Weight Heparin Dose at Least 24 hrs After the Procedure/Surgery (as Opposed to Administering it <24 hrs After the Procedure/Surgery (Conditional Recommendation, Very Low Certainty of Evidence)
Low-Moderate Bleeding Risk Procedure/Surgery
Wait at Least 24 hrs Before Resuming Low Molecular Weight Heparin
High Bleeding Risk Procedure/Surgery
Wait at least 48-72 hrs Before Resuming Low Molecular Weight Heparin
For Patients in Whom the Management Plan is to Delay Resumption of Low Molecular Weight Heparin for 48-72 hrs and Who are at High Risk for Postprocedural/Postoperative Venous Thromboembolism, Low-Dose Low Molecular Weight Heparin Can Be Administered for the Initial 2-3 Days Before the Transition to Full-Dose Low Molecular Weight Heparin Anticoagulation
In Patients Receiving Low Molecular Weight Heparin (as Part of Bridging Regimen or Not) for an Elective Procedure/Surgery, Administer Half the Total Daily Dose of Low Molecular Weight Heparin the Day Prior to the Elective Procedure/Surgery (as Opposed to Administering the Full Dose of Low Molecular Weight Heparin the Day Prior (Conditional Recommendation, Very Low Certainty of Evidence)
This Guidance May Apply More to Patients having a High Bleeding Risk Procedure/Surgery (Including Patients Having Neuraxial, Spinal or Epidural, Anesthesia, Rather than in Patients Having a Low-Moderate Bleeding Risk Procedure/Surgery
Administering Half the Total Daily Dose of Low Molecular Weight Heparin Can Be Done by Giving, on the Morning of the Day Before the Procedure/Surgery, Only the Morning Dose of a BID Low Molecular Weight Heparin Regimen or Approximately 50% of the Dose of a Once Daily Low Molecular Weight Heparin Regimen
In Patients Receiving Low Molecular Weight Heparin (as Part of Bridging Regimen or Not) for an Elective Procedure/Surgery, Measurement of Anti-Factor Xa Levels is Not Routinely Recommended to Guide Perioperative Low Molecular Weight Heparin Management (Conditional Recommendation, Very Low Certainty of Evidence)
There May Be Select Patients Undergoing High Bleeding Risk Procedures/Surgeries (Intracranial, Spinal, etc) or Patients Who Require an Urgent (Non-Elective) Procedure/Surgery Where Anti-Factor Xa Measurement May Be Considered
Parenteral anticoagulants: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (8th Edition). Chest. 2008;133(6 Suppl):141S [MEDLINE]
Executive summary: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012 Feb;141(2 Suppl):7S-47S. doi: 10.1378/chest.1412S3 [MEDLINE]
Perioperative Management of Antithrombotic Therapy: An American College of Chest Physicians Clinical Practice Guideline. Chest. 2022 Aug 11;S0012-3692(22)01359-9. doi: 10.1016/j.chest.2022.07.025 [MEDLINE]
Indications
Fibrinolysis for patients with intermediate risk pulmonary embolism. N Engl J Med 2014;370:1402–1411 [MEDLINE]
Administration
Dosing in heavy-weight/obese patients with the LMWH, tinzaparin: a pharmacodynamic study. Thromb Haemost. 2002;87(5):817 [MEDLINE]
The safety of dosing dalteparin based on actual body weight for the treatment of acute venous thromboembolism in obese patients. J Thromb Haemost. 2005;3(1):100 [MEDLINE]
Low-molecular-weight heparins in renal impairment and obesity: available evidence and clinical practice recommendations across medical and surgical settings. Ann Pharmacother. 2009;43(6):1064 [MEDLINE]
Enoxaparin Dosing at Extremes of Weight: Literature Review and Dosing Recommendations. Ann Pharmacother. 2018 Sep;52(9):898-909. doi: 10.1177/1060028018768449 [MEDLINE]