Periprocedural/Perioperative Management of Coumadin
Clinical Efficacy
BRIDGE Trial Studying Perioperative Low Molecular Weight Heparin Bridge Therapy in Atrial Fibrillation Patients on Coumadin with Planned Interruption for Surgery/Procedures (NEJM, 2015) [MEDLINE]
In Atrial Fibrillation with Coumadin Interruption for Elective Surgery/Invasive Procedure, Forgoing Low Molecular Weight Heparin Bridge Therapy Decreased the Rate of Bleeding and was Non-Inferior to Using Low Molecular Weight Heparin Bridge Therapy for the Prevention of Arterial Thromboembolism
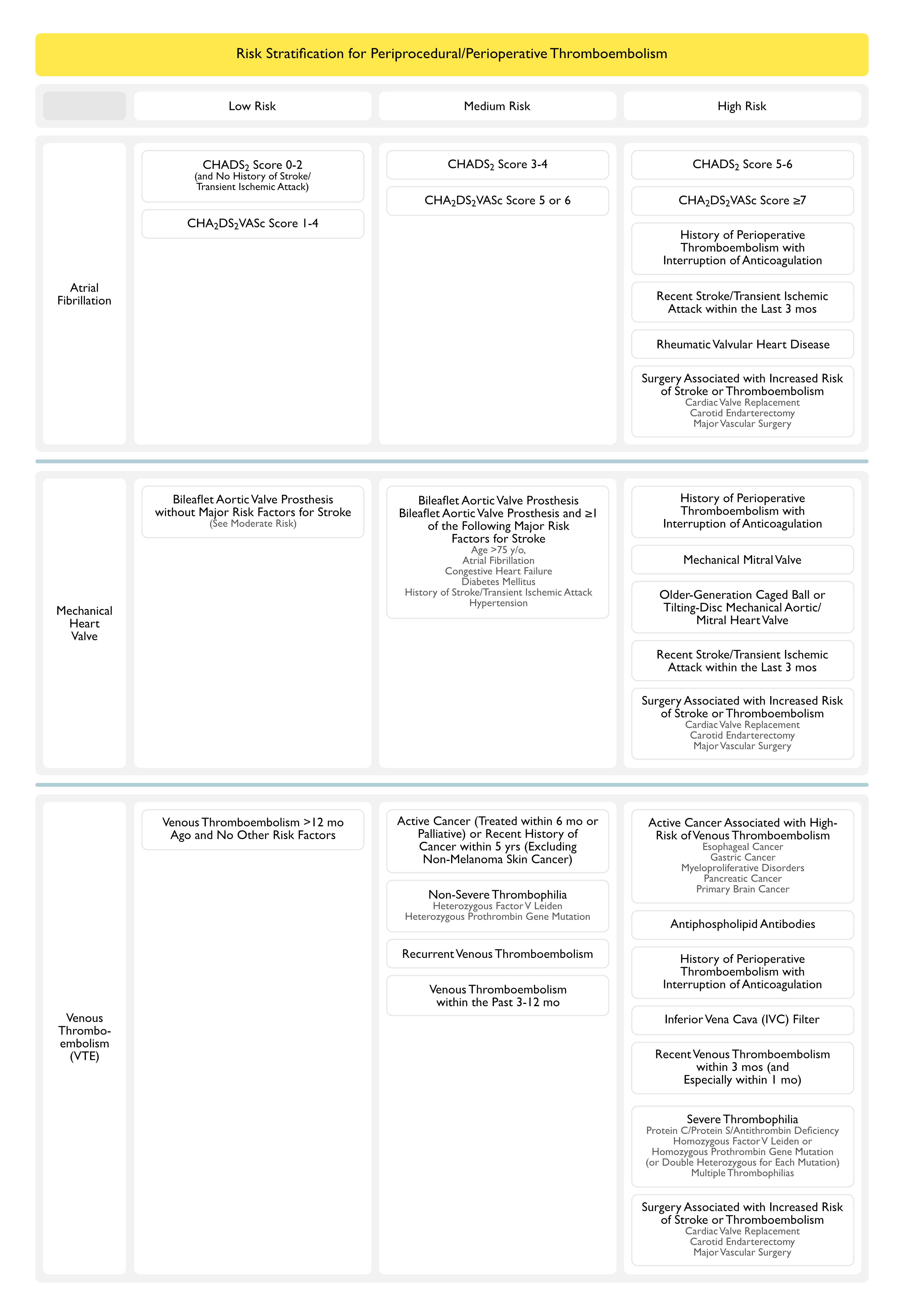
Risk Stratification for Periprocedural/Perioperative Thromboembolism
Venous Thromboembolism >12 mo Ago and No Other Risk Factors
Moderate Risk for Perioperative Thromboembolism
Active Cancer (Treated within 6 mo or Palliative) or Recent History of Cancer within 5 yrs (Excluding Non-Melanoma Skin Cancer)
Non-Severe Thrombophilia (Heterozygous Factor V Leiden or Heterozygous Prothrombin Gene Mutation)
Recurrent Venous Thromboembolism
Venous Thromboembolism within the Past 3-12 mo
High Risk for Perioperative Thromboembolism
Active Cancer Associated with High-Risk of Venous Thromboembolism (Esophageal Cancer, Gastric Cancer, Myeloproliferative Disorders, Pancreatic Cancer, or Primary Brain Cancer)
Antiphospholipid Antibodies
History of Perioperative Thromboembolism with Interruption of Anticoagulation
Inferior Vena Cava (IVC) Filter
Recent Venous Thromboembolism within 3 mos (and Especially within 1 mo)
Severe Thrombophilia (Protein C/Protein S/Antithrombin Deficiency, Homozygous Factor V Leiden or Homozygous Prothrombin Gene Mutation or Double Heterozygous for Each Mutation, Multiple Thrombophilias)
Surgery Associated with Increased Risk of Stroke or Thromboembolism (Cardiac Valve Replacement, Carotid Endarterectomy, Major Vascular Surgery)
Recommendations for Periprocedural/Perioperative Management of Coumadin (American College of Chest Physicians Clinical Practice Guideline for the Perioperative Management of Antithrombotic Therapy) (Chest, 2022) [MEDLINE]
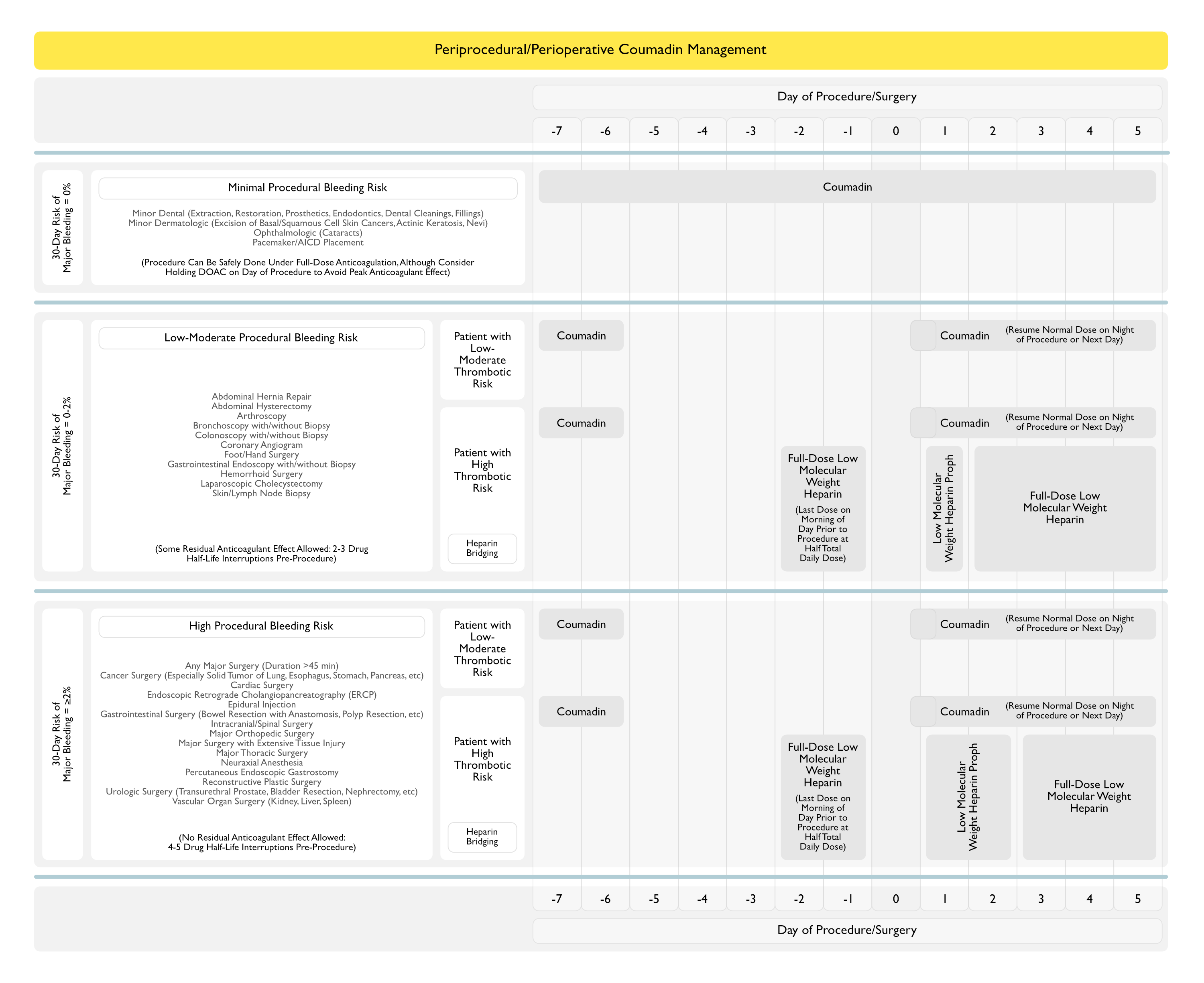
Patients Receiving Coumadin Who Require Minor Procedure (Dental, Dermatologic, Ophthalmologic, Pacemaker/ICD, Colonoscopy With/Without Polypectomy)
In Patients Receiving Coumadin Who Require a Dental Procedure, Continuation of Coumadin is Recommended (as Opposed to Interruption) (Conditional Recommendation, Low Certainty of Evidence)
Risk of Dental Procedure-Related Bleeding May Vary, Being Lower with Single Tooth Extractions and Higher with Multiple Tooth Extractions or in Patients with Poor Gingival Health
Accordingly, Coumadin Interruption May be Preferred in Situations Where Oral Bleeding is Expected to Be Considerable
In Patients Receiving Coumadin Who Require a Dental Procedure, Use of a Pro-Hemostatic Agent with Continuation of Coumadin (as Opposed to Discontinuation of Coumadin with/without Heparin Bridging) is Recommended (Conditional Recommendation, Low Certainty of Evidence)
Pro-Hemostatic Options
Pre-Procedure and Post-Procedure Administration of Oral Tranexamic Acid Mouthwash (BID-TID)
Intervention-Specific Measures (Extra Sutures, Gauze Soaked in Tranexamic Acid)
In Patients Receiving Coumadin Who Require a Minor Dermatologic Procedure, Continuation of Coumadin (as Opposed to Discontinuation of Coumadin) is Recommended (Conditional Recommendation, Very Low Certainty of Evidence)
Risk for Dermatologic Procedure-Related Bleeding May Vary, Being Lower with Resections of Small (1-2 cm) Skin Cancers and Biopsies, and Higher with Resections of Larger (>3 cm) Skin Cancers, Particularly if Skin Grafting is Required
Accordingly, Coumadin Interruption May be Preferred in Situations Where Site-Related Bleeding is Expected to Be Considerable or if Lengthy Wound Healing is Expected (i.e. Skin Graft)
In Patients Receiving Coumadin Who Require a Minor Ophthalmologic Procedure, Continuation of Coumadin (as Opposed to Discontinuation of Coumadin) is Recommended (Conditional Recommendation, Very Low Certainty of Evidence)
Coumadin Interruption May be Preferred in Patients Considered at Higher Risk for Bleeding (Those Having More Complex Retinal Surgery or Patients Having Surgery with Retrobulbar Anesthesia)
Cataract Surgery is Performed with Topical Anesthesia (and Less Commonly, with Retrobulbar Anesthesia)
In Patients Receiving Coumadin Who Require a Pacemaker or ICD Implantation, Continuation of Coumadin (as Opposed to Discontinuation of Coumadin with Heparin Bridging) is Recommended (Strong Recommendation, Moderate Certainty of Evidence)
Continuation of Coumadin Around Cardiac Device Procedures is Based on the Premise that the Patient’s INR at the Time of the Procedure is <3.0
In Patients Receiving Coumadin Who Require Coumadin Interruption for a Colonoscopy with Anticipated Polypectomy, Heparin Bridging is Not Recommended During Period of Coumadin Interruption (Conditional Recommendation, Very Low Certainty of Evidence)
Patients Receiving Coumadin Who Require an Elective Surgery/Procedure
In Patients Requiring Coumadin Interruption for an Elective Surgery/Procedure, Stop Coumadin for ≥5 Days (as Opposed to an Interruption of <5 Days) Before Elective Surgery/Procedure (Conditional Recommendation, Low Certainty of Evidence)
In Selected Patients Per the Following Clinical Situations, a Longer Period of Coumadin Interruption May be Required
Elderly Patient with Comorbidities
Patient with a Higher Target INR Range
Patient with Very Low-Dose Coumadin Requirement
In Patients Requiring Coumadin Interruption for an Elective Surgery/Procedure Who Have an Elevated INR (≥1.5) 1-2 Days Before the Elective Surgery/Procedure, Use of Preoperative Vitamin K is Not Recommended (Conditional Recommendation, Very Low Certainty of Evidence)
Uncertainty About Routine Preoperative Vitamin K Administration Relates to the Dose of Vitamin K, Limited Availability of Oral Vitamin K Formulations, and Potential for Resistance to Postoperative Re-Anticoagulation
In Patients Receiving Coumadin for a Mechanical Heart Valve Who Require Coumadin Interruption for an Elective Surgery/Procedure, Heparin Bridging is Not Recommended (Conditional Recommendation, Very Low Certainty of Evidence)
In Selected Patients Who are at High-Risk for Perioperative Thromboembolism Per the Following Clinical Situations, Preoperative and Postoperative Heparin Bridging is Recommended
History of Perioperative Thromboembolism
Mechanical Mitral Valve
Older-Generation Caged Ball or Tilting-Disc Mechanical Aortic/Mitral Heart Valve
Recent Stroke/Transient Ischemic Attack within the Last 3 mos
Surgery Associated with Increased Risk of Stroke or Thromboembolism (Cardiac Valve Replacement, Carotid Endarterectomy, Major Vascular Surgery)
In Patients Receiving Coumadin for Atrial Fibrillation Who Require Coumadin Interruption for an Elective Surgery/Procedure, Heparin Bridging is Not Recommended (Strong Recommendation, Moderate Certainty of Evidence
In Selected Patients Who are at High-Risk for Perioperative Thromboembolism Per the Following Clinical Situations, Preoperative and Postoperative Heparin Bridging is Recommended
History of Perioperative Thromboembolism
CHADS2 Score (Congestive Heart Failure, Hypertension, Age ≥75 years, Diabetes Mellitus, Prior Stroke/Transient Ischemic Attack) of 5 or 6
Recent Stroke/Transient Ischemic Attack within the Last 3 mos
Rheumatic Valvular Heart Disease
Surgery Associated with Increased Risk of Stroke or Thromboembolism (Cardiac Valve Replacement, Carotid Endarterectomy, Major Vascular Surgery)
In Patients Receiving Coumadin for Venous Thromboembolism as the Sole Clinical Indication Who Require Coumadin Interruption for an Elective Surgery/Procedure, Heparin Bridging is Not Recommended (Conditional Recommendation, Very Low Certainty of Evidence)
Suggesting Against Bridging with a Therapeutic-Dose Heparin Regimen Does Not Preclude the Empiric Use of a Low-Dose Heparin Regimen (Typically Started within 24 hrs After Surgery and Continued for Up to 5 Days While Coumadin Therapy is Resumed, to Decrease the Risk for Postoperative Venous Thromboembolism
In Selected Patients at High-Risk for Venous Thromboembolism Per the Following Clinical Situations, Preoperative and Postoperative Heparin Bridging is Recommended
Active Cancer Associated with High Venous Thromboembolism Risk (Pancreatic Cancer, Myeloproliferative Disorders, Primary Brain Cancer, Gastric Cancer, and Esophageal Cancer)
Antiphospholipid Antibodies
History of Perioperative Thromboembolism
Inferior Vena Cava (IVC) Filter
Recent Venous Thromboembolism within 3 mos (and Especially within 1 mo)
Severe Thrombophilia (Deficiency of Protein C, Protein S or Antithrombin; Homozygous Factor V Leiden or Prothrombin Gene Mutation or Double Heterozygous for Each Mutation, Multiple Thrombophilias)
Surgery Associated with Increased Risk of Stroke or Thromboembolism (Cardiac Valve Replacement, Carotid Endarterectomy, Major Vascular Surgery)
In Patients Requiring Coumadin Interruption for an Elective Surgery/Procedure, Resume Coumadin within 24 hrs (as Opposed to Delay >24 hrs) After Elective Surgery/Procedure (Conditional Recommendation, Low Certainty of Evidence)
For Most Patients, Resuming Coumadin within 24 hrs Implies Resumption on the Evening of the Elective Surgery/Procedure
Implicit in the Early (within 24 hrs) Resumption of Coumadin is that it Typically Takes 2-3 Days for a Partial Anticoagulant Effect and 5-6 Says for a Full Anticoagulant Effect to Occur
Coumadin Resumption May Be Delayed in Certain Postoperative Circumstances (Such as Inadequate Surgery/Procedure-Site Hemostasis, an Anticipated Need for Additional Intervention, or Patient Inability to Take Oral Medications)
In Patients Requiring Coumadin Interruption for an Elective Surgery/Procedure, Resume the First Postoperative Coumadin Dose at the Patient’s Usual Dose (as Opposed to Resuming Coumadin with Double the Usual Dose) (Conditional Recommendation, Very Low Certainty of Evidence)
Although Postoperative Doubling of the Coumadin Dose for 1-2 Days May Lead to a More Rapid Attainment of an INR ≥2.0 in Some Patients, There are Concerns in Applying this Approach in Practice (For Example, in Patients with Variable Coumadin Dose Regimens and Those Expected to Be Hospitalized for >1 Day)
Recommendations (Neurocritical Care Society and Society of Critical Care Medicine Guidelines for Reversal of Antithrombotics in the Setting of Intracranial Hemorrhage, 2016) [MEDLINE]
Factor VIIa is Not Recommended in this Setting (Strong Recommendation, Low Quality Evidence)
Contains all of the coagulation factors which are present in whole blood
The Amount of FFP Required to Correct the INR Individually Varies Due to the Non-Linear Exponential Relationship Between Coagulation Factor Levels and Coagulation Test Results
Advantages
Low Cost: $200-400 per dose
Widely Available
Disadvantages
Fluid Loadx
Long Latency to Correction of the INR: may take >30 hrs
Recommendation
May Be Considered if Prothrombin Complex Concentrate-4 Factor is Not Available or if Patient Cannot Tolerate Prothrombin Complex Concentrates
Trial Comparing Prothrombin Complex Concentrate-4 Factor to Fresh Frozen Plasma in the Correction of INR in Coumadin-Associated Hemorrhage (Circulation, 2013) [MEDLINE]
Prothrombin Complex Concentrate-4 Factor was Superior to Fresh Frozen Plasma in Terms of Achieving Rapid INR Correction
Randomized, Non-Inferiority Trial Comparing Prothrombin Complex Concentrate-4 Factor vs Fresh Frozen Plasma in Reversing Coumadin (Lancet, 2015) [MEDLINE]
Prothrombin Complex Concentrate-4 Factor Achieved Effective Hemostasis in 90% of Subjects, as Compared to 75% in the Fresh Frozen Plasma Group
Safety Profile (Thromboembolic Events, Fluid Overload, and Late Bleeding Events) were Similar Between the Two Groups
Review of Prothrombin Complex Concentrate to Reverse Coumadin Anticoagulation in the Setting of Bleeding or the Need for an Invasive Procedure (Ann Intern Med, 2016) [MEDLINE]: review of 5 randomized controlled trials and 8 observational studies
Prothrombin Complex Concentrate Decreased the Mortality Rate in Reversing Coumadin Anticoagulation, as Compared to Fresh Frozen Plasma
Recommendations (Chest Antithrombotic Therapy and Prevention of Thrombosis 2012 Guidelines) [MEDLINE]
For Coumadin Anticoagulation with Associated Major Hemorrhage, Prothrombin Complex Concentrate-4 Factor is Recommended Over Fresh Frozen Plasma* (Grade 2C Recommendation)
Intravenous Vitamin K (5-10 mg IV) is Also Recommended: see below
Recommendations (Neurocritical Care Society and Society of Critical Care Medicine Guidelines for Reversal of Antithrombotics in the Setting of Intracranial Hemorrhage, 2016) [MEDLINE]
Prothrombin Complex Concentrate-3 Factor or Prothrombin Complex Concentrate-4 Factor are Recommended Over Fresh Frozen Plasma or Factor VIIa (Conditional Recommendation, Low Quality Evidence)
Prothrombin Complex Concentrate-4 Factor is Recommended Over Prothrombin Complex Concentrate-3 Factor (Conditional Recommendation, Low Quality Evidence)
Intravenous Vitamin K (5-10 mg IV) is Also Recommended: see below
Executive summary: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012 Feb;141(2 Suppl):7S-47S. doi: 10.1378/chest.1412S3 [MEDLINE]
Antithrombotic Therapy for VTE Disease: CHEST Guideline and Expert Panel Report. Chest. 2016 Feb;149(2):315-52. doi: 10.1016/j.chest.2015.11.026. Epub 2016 Jan 7 [MEDLINE]
Perioperative Management of Antithrombotic Therapy: An American College of Chest Physicians Clinical Practice Guideline. Chest. 2022 Aug 11;S0012-3692(22)01359-9. doi: 10.1016/j.chest.2022.07.025 [MEDLINE]
Administration
A pharmacogenetic versus a clinical algorithm for warfarin dosing. N Engl J Med 2013;369(24):2283-2293 [MEDLINE]
A randomized trial of genotype-guided dosing of warfarin. N Engl J Med 2013;369(24):2294-2303 [MEDLINE]
Efficacy and safety of a 4-factor prothrombin complex concentrate in patients on vitamin K antagonists presenting with major bleeding: a randomized, plasma- controlled, phase IIIb study. Circulation. 2013;128:1234–43 [MEDLINE]
Outcomes of urgent warfarin reversal with frozen plasma versus prothrombin complex concentrate in the emergency department. Circulation. 2013 Jul 23;128(4):360-4. doi: 10.1161/CIRCULATIONAHA.113.001875. Epub 2013 Jun 14 [MEDLINE]
Genotype-guided drug prescribing: a systematic review and meta-analysis of randomized control trials. Br J Clin Pharmacol. 2015 Oct;80(4):868-77. doi: 10.1111/bcp.12475. Epub 2015 Jul 22 [Epub ahead of print] [MEDLINE]
Four-factor prothrombin complex concentrate versus plasma for rapid vitamin K antagonist reversal in patients needing urgent surgical or invasive interventions: a phase 3b, open-label, non-inferiority, randomised trial. Lancet 2015 May 23;385(9982):2077-87. doi: 10.1016/S0140-6736(14)61685-8. Epub 2015 Feb 27 [MEDLINE]
Perioperative Bridging Anticoagulation in Patients with Atrial Fibrillation. N Engl J Med. 2015;373(9):823 [MEDLINE]
Guideline for Reversal of Antithrombotics in Intracranial Hemorrhage: A Statement for Healthcare Professionals from the Neurocritical Care Society and Society of Critical Care Medicine. Neurocrit Care. 2016 Feb;24(1):6-46. doi: 10.1007/s12028-015-0222-x [MEDLINE]
Review: For warfarin reversal, prothrombin complex concentrates reduce mortality compared with fresh frozen plasma. Ann Intern Med. 2016 Dec 20;165(12):JC65. doi: 10.7326/ACPJC-2016-165-12-065 [MEDLINE]