Oral Aspirin (Initial Dose: 325 mg) is Recommended within 24-48 hrs After Stroke Onset (Class I, Level of Evidence A)
Administration of Aspirin (or Other Antiplatelet Agents) as an Adjunctive Therapy within 24 hrs of Intravenous rtPA is Not Recommended (Class III, Level of Evidence C)
Aspirin is Not Recommended as a Substitute for Other Acute Interventions in Stroke, Including Intravenous rtPA (Class III, Level of Evidence B)
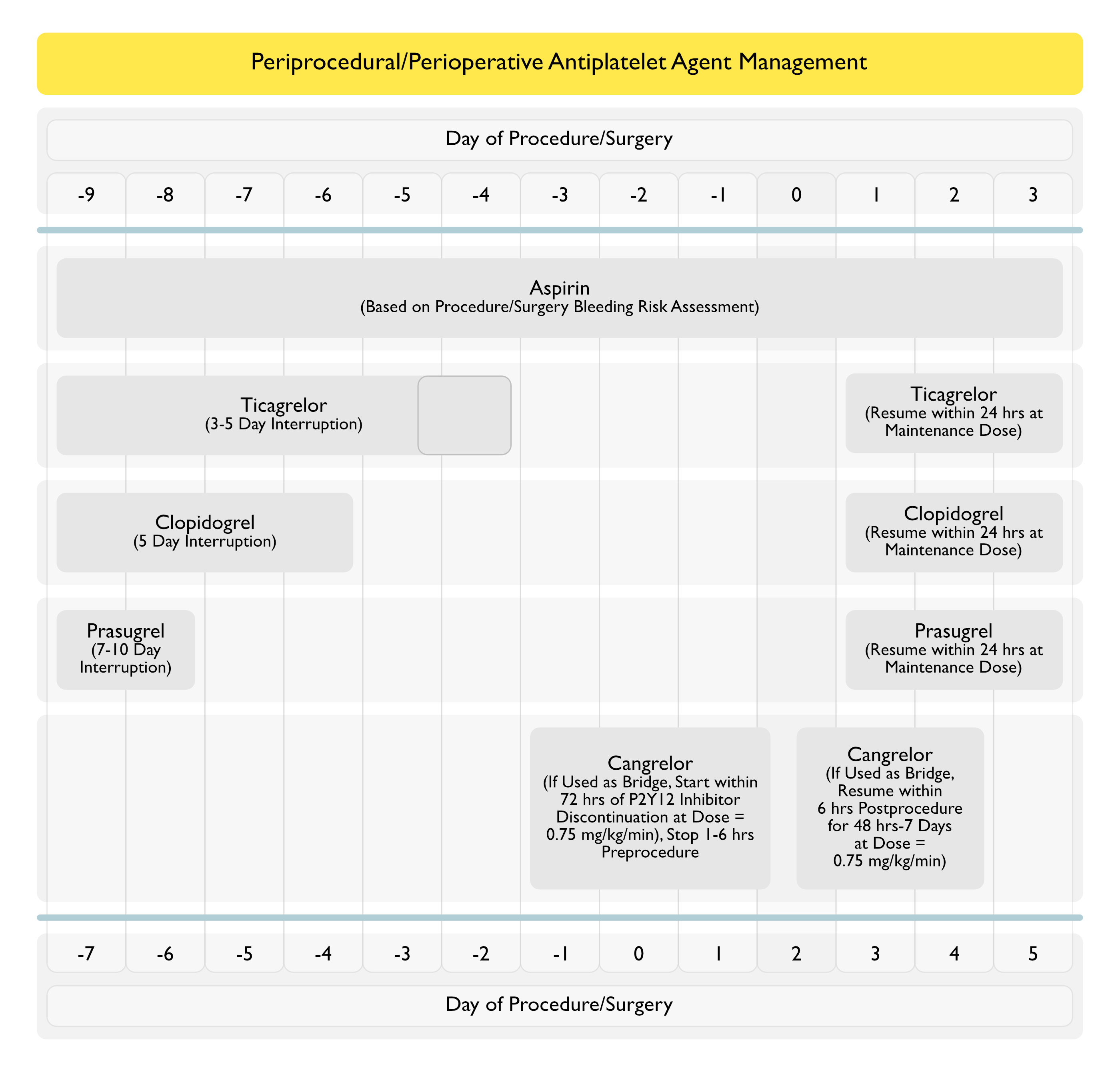
Recommendations for Periprocedural/Perioperative Management of Aspirin (American College of Chest Physicians Clinical Practice Guideline for the Perioperative Management of Antithrombotic Therapy) (Chest, 2022) [MEDLINE]
Minor Procedures (Dental, Dermatologic, Ophthalmologic)
In Patients Receiving an Antiplatelet Drug (Aspirin or P2Y12 Inhibitor) Who are Undergoing a Minor Dental Procedure, Continue the Antiplatelet Drug (Aspirin or P2Y12 Inhibitor) (Conditional Recommendation, Very Low Certainty of Evidence)
Patients Who are Receiving Dual Antiplatelet Therapy with Aspirin and a P2Y12 Inhibitor Can Continue Aspirin and Interrupt the P2Y12 Inhibitor
In Patients Receiving an Antiplatelet Drug (Aspirin or P2Y12 Inhibitor) Who are Undergoing a Minor Dermatologic Procedure, Continue the Antiplatelet Drug (Aspirin or P2Y12 Inhibitor) (Conditional Recommendation, Very Low Certainty of Evidence)
Patients Who are Receiving Dual Antiplatelet Therapy with Aspirin and a P2Y12 Inhibitor Can Continue Aspirin and Interrupt the P2Y12 Inhibitor
In Patients Receiving an Antiplatelet Drug (Aspirin or P2Y12 Inhibitor) Who are Undergoing a Minor Ophthalmologic Procedure, Continue the Antiplatelet Drug (Aspirin or P2Y12 Inhibitor) Throughout the Ophthalmologic Procedure (Conditional Recommendation, Low Certainty of Evidence)
Patients Who are Receiving Dual Antiplatelet Therapy with Aspirin and a P2Y12 Inhibitor Can Continue Aspirin and Interrupt the P2Y12 Inhibitor
Elective Non-Cardiac Surgery
In Patients Receiving Aspirin Who are Undergoing Elective Non-Cardiac Surgery, Aspirin Continuation is Recommended (Conditional Recommendation, Moderate Certainty of Evidence)
Recommendation May Be Modified on a Case-by-Case Basis (Such as for Non-Cardiac Surgery Associated with a High Bleeding Risk: Intracranial or Spinal Surgery)
If Aspirin Interruption is Adopted, Interruption for ≤7 Days is Recommended
Elective Surgery
In Patients Receiving Antiplatelet Drug Therapy Who are Undergoing an Elective Procedure/Surgery, Routine Use of Platelet Function Testing Prior to Procedure/Surgery is Not Recommended (Conditional Recommendation, Very Low Certainty of Evidence)
Platelet Function Testing Could Be Used with a Possible Small Benefit and Little Harm in Certain Scenarios Such as Patients Undergoing Coronary Artery Bypass Graft (CABG) Surgery Who Have Recently Started Taking a P2Y12 Inhibitor
Costs Would Be Moderate for Implementation
In Patients Receiving Aspirin Who are Undergoing Elective Surgery and Require Aspirin Interruption, Stop Aspirin ≤7 Days (Instead of 7-10 Days) Before Surgery (Conditional Recommendation, Very Low Certainty of Evidence)
Recommendation May Be Modified on a Case-by-Case Basis, Depending on Individual Patient Circumstances (Such as Surgery-Related Bleeding Risk)
In Patients Who Require Antiplatelet Drug Interruption for an Elective Procedure/Surgery, Resume Antiplatelet Drugs ≤24 hrs (Instead of >24 hrs) After the Procedure/Surgery (Conditional Recommendation, Very Low Certainty of Evidence)
Specific Management inPatients with Coronary Stents
In Patients Receiving ASA and a P2Y12 Inhibitor with Coronary Stents Placed within the Last 6-12 wks Who are Undergoing an Elective Procedure/Surgery, Continue Both Antiplatelet Agents or Stop One Antiplatelet Agent within 7-10 Days of Procedure/Surgery (Conditional Recommendation, Very Low Certainty of Evidence)
Either Approach is Reasonable Depending on the Bleeding Risk Associated with the Procedure/Surgery if Antiplatelet Therapy is Continued and Risk for Acute Coronary Syndrome/Coronary Stent Thrombosis if Antiplatelet Therapy is Interrupted
Following Factors Should Be Considered in the Decision About Whether to Continue Dual Antiplatelet Therapy or Interrupt One Agent
Timing of Stent Placement (Whether Closer to 6 wks or 12 wks)
Type of Stent (Drug-Eluting or Bare-Metal)
Location of the Stent (Whether at a Dominant Coronary Artery or Not)
Number and length of Stents Implanted
In Patients Receiving Aspirin and a P2Y12 Who Had Coronary Stents Placed within the Last 3-12 mos and are Undergoing an Elective Procedure/Surgery, Stop the P2Y12 Inhibitor Prior to Procedure/Surgery (as Opposed to Continuing the P2Y12 Inhibitor (Conditional Recommendation, Very Low Certainty of Evidence)
Recommendation is Based on Indirect Evidence and Expert-Based Consensus that Stopping P2Y12 Inhibitors in Patients with Stents > 3 mos Postimplantation is Likely Safe
Following Factors Should Be Considered in the Decision About Whether to Interrupt the P2Y12 Inhibitor
Timing of Stent Placement (Whether Closer to 3 mos or 12 mos)
Type of Stent (Drug-Eluting or Bare-Metal)
Location of the Stent (Whether at a Dominant Coronary Artery or Not)
Number and length of Stents Implanted
In Patients with Coronary Stents Who Require Interruption of Antiplatelet Drugs for an Elective Procedure/Surgery, Routine Bridging Therapy with a Glycoprotein IIb-IIIa Inhibitor, Cangrelor, or Low Molecular Weight Heparin is Not Recommended (Conditional Recommendation, Low Certainty of Evidence)
Cangrelor Bridging Approach May Be Considered in Selected High-Risk Patients (Those with Coronary Stent Placed within 3 mos in a Critical Location
In Patients with Coronary Stents Who Require Continued Dual Antiplatelet Therapy, Delaying an Elective Procedure/Surgery is Recommended (Conditional Recommendation, Very Low Certainty of Evidence)
Duration of Procedure/Surgery Delay Should Be Made a Case-by-Case Basis and Consider the Following
Urgency of the Procedure/Surgery
Time Elapsed Since Coronary Stenting
Risk Profile of the Coronary Stenting (Critical Location, Multiple Stents, etc)
In Patients Who are Receiving Aspirin and Undergoing Coronary Artery Bypass Graft (CABG) Surgery, Continue Aspirin (Conditional Recommendation, Low Certainty of Evidence)
In Patients Receiving ASA or a P2Y12 Inhibitor Who are Undergoing Coronary Artery Bypass Graft (CABG) Surgery, Resume the Aspirin or the P2Y12 Inhibitor in ≤24 hrs (as Opposed to ≥24 hours) After Surgery (Conditional Recommendation, Low Certainty of Evidence)
Resumption of Antiplatelet Therapy May Be Delayed in Patients Who Develop Post-Coronary Artery Bypass Graft Thrombocytopenia (Platelet Count < 50k), Which Typically Occurs with On-Pump Surgery
Death following ingestion of five grains of acetylsalicylic acid. JAMA 1933; 101: 446
Transient pulmonary eosinophilia and asthma. A review of 20 cases occurring in 5,702 asthma sufferers. Am Rev Respir Dis. 1966 May;93(5):797-803 [MEDLINE]
Intolerance to aspirin: clinical studies and consideration of its pathogenesis. Ann Intern Med 1968; 68: 975-983
Salicylate-induced pulmonary edema: clinical features and prognosis. Ann Intern Med 1981; 95: 405-409
Adverse pulmonary responses to aspirin and acetaminophen in chronic chilhood asthma. Pediatrics 1983; 71: 313-318
Guidelines for the early management of patients with acute ischemic stroke: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2013 Mar;44(3):870-947. doi: 10.1161/STR.0b013e318284056a. Epub 2013 Jan 31 [MEDLINE]
Administration
XXXXXX
Periprocedural/Perioperative Management of Aspirin
Executive summary: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012 Feb;141(2 Suppl):7S-47S. doi: 10.1378/chest.1412S3 [MEDLINE]
Perioperative Management of Antithrombotic Therapy: An American College of Chest Physicians Clinical Practice Guideline. Chest. 2022 Aug 11;S0012-3692(22)01359-9. doi: 10.1016/j.chest.2022.07.025 [MEDLINE]
Adverse Effects
Mechanism of aspirin-induced asthma. Allergy 1997; 52: 613-619
Recurrent ARDS in an 39-year-old woman with migraine headaches. Chest 1998; 114: 919-22