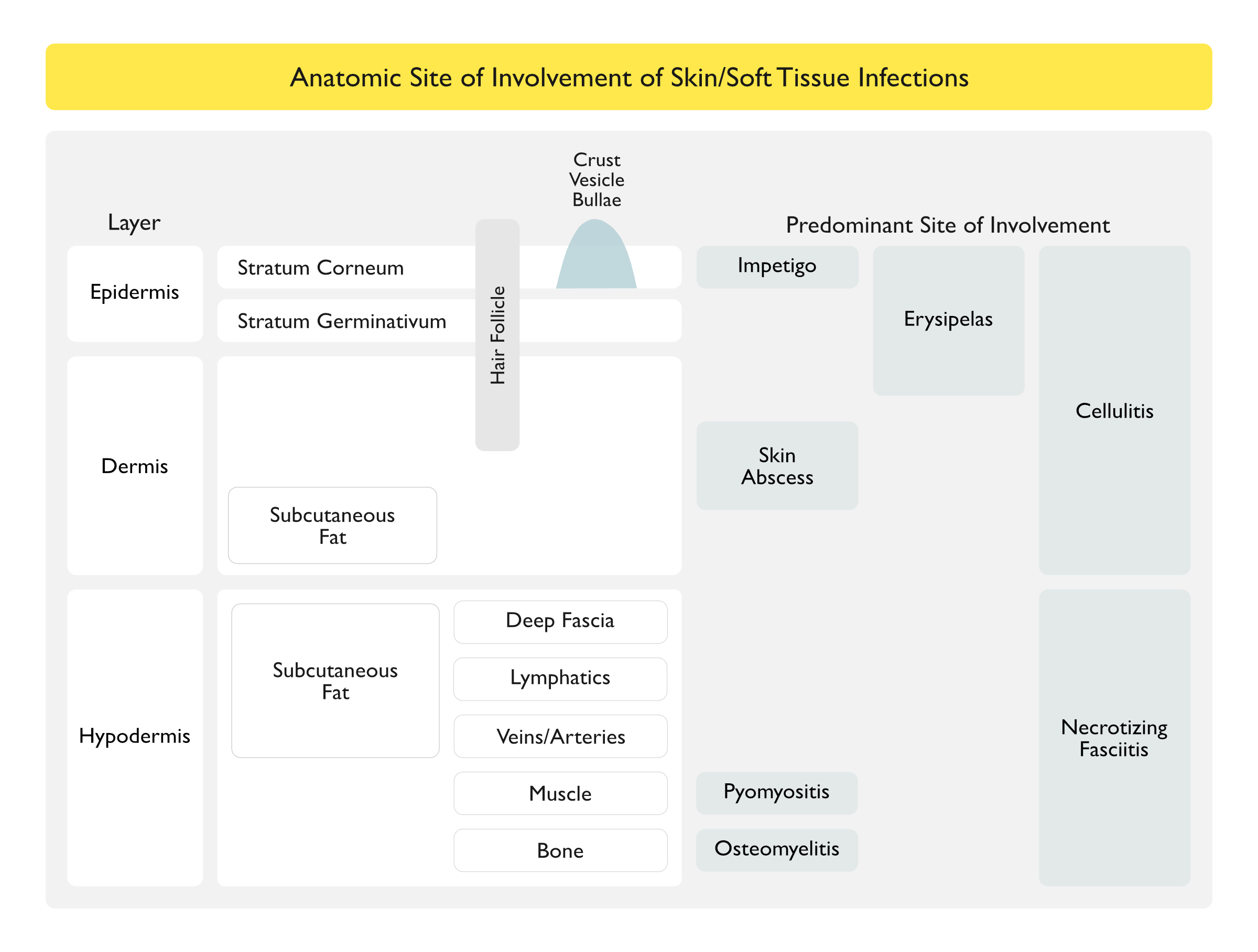
Impetigo (see Impetigo): infection of superficial layers of the epidermis
Cellulitis (see Cellulitis): skin infection of deeper dermis and subcutaneous fat (resulting from bacterial breach of the skin) characterized by erythema, warmth, and edema without an underlying suppurative focus
Erysipelas (see Erysipelas): skin infection of upper dermis and superficial lymphatics (resulting from bacterial breach of the skin) characterized by erythema, warmth, and edema without an underlying suppurative focus
Furuncle (Boil) (see Skin Abscess): infection of hair follicle where purulent material extends through the dermis into the subcutaneous tissue, forming a small abscess
Carbuncle (see Skin Abscess): coalescence of several inflamed follicles into a single inflammatory mass with purulent drainage from multiple follicles
Skin Abscess (see Skin Abscess): collection of pus within dermis and deeper skin tissues
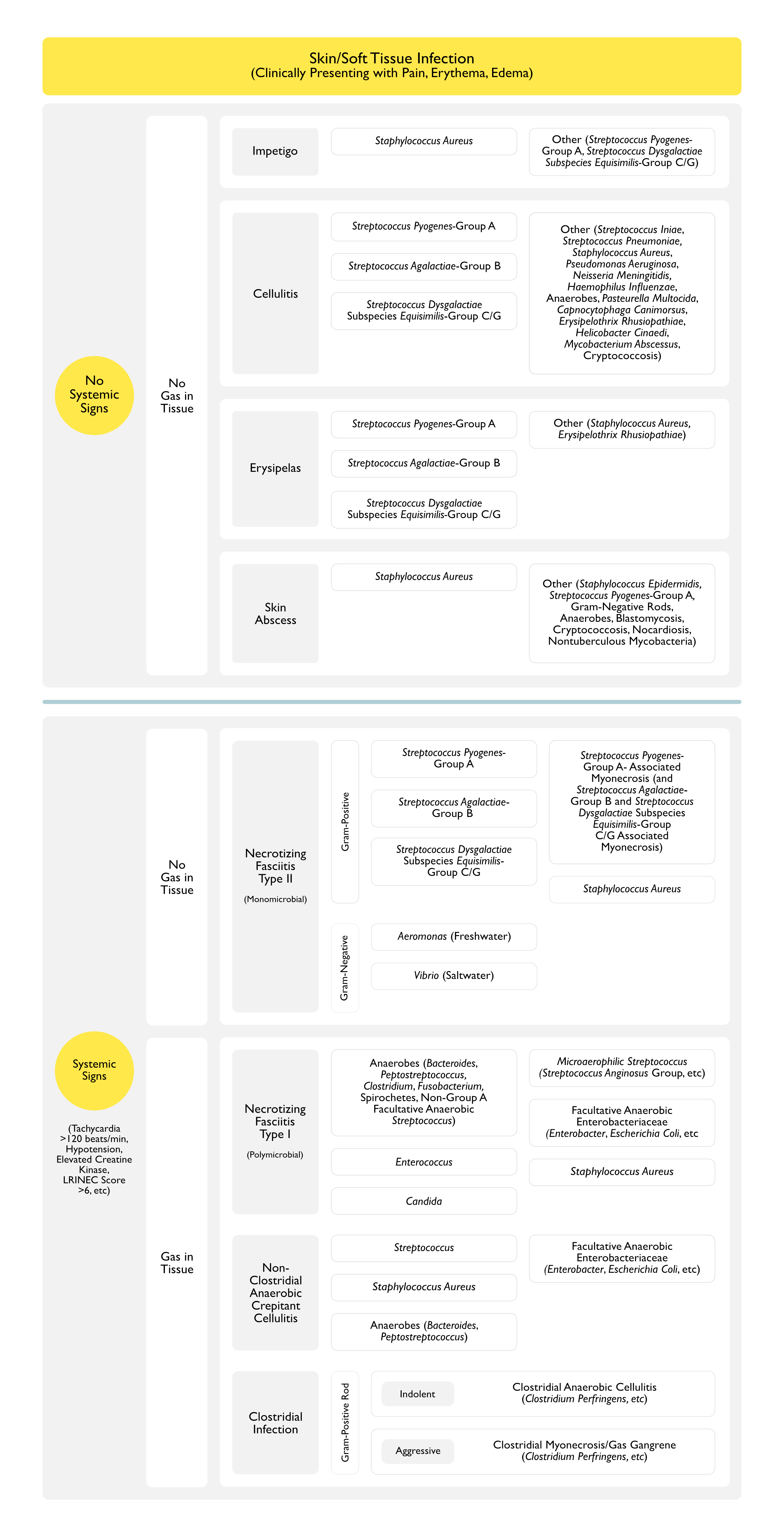
Necrotizing Soft Tissue Infection (see Necrotizing Soft Tissue Infection): deep tissue infection involving the hypodermis (and contained structures)
All of These are Characterized by Fulminant Tissue Destruction, Systemic Toxicity (Tachycardia >120 Beats/min, Hypotension, Elevated Creatine Kinase, CRP >15 mg/dL, LRINEC Score >6, etc), and High Mortality Rates
May Be the Only Risk Factor Present in a Normal Patient Who Develops Skin Abscess
Skin Barrier Breach
Microbiology
General Comments
Approximately 7% of Skin Abscess Cases are Polymicrobial (Ann Intern Med, 1977) [MEDLINE] (Br J Surg, 1981) [MEDLINE] (Arch Surg, 1990) [MEDLINE] (Clin Infect Dis, 1995) [MEDLINE]
Isolation of Multiple Organisms (Including Staphylococcus Aureus in Combination with Streptococcus Pyogenes and Gram-Negative Bacilli with Anaerobes) is More Common in Patients with Skin Abscess Involving the Following Specific Anatomic Sites
Warm Compress: when used alone, may promote drainage of the skin abscess
Skin Abscess or Medium-Large Furuncle/Carbuncle
Incision and Drainage (I+D)
Indications for Concomitant Antibiotic Therapy (Based on Infectious Disease Society America/IDSA guidelines)
Abscess Present in Difficult to Drain Area: face, hand, genitals
Associated Septic Phlebitis
Comorbid Disease
Extreme of Age
Immunosuppression
Lack of Clinical Response to Incision and Drainage (I+D) Alone
Rapid Progression with Associated Cellulitis
Severe or Extensive Disease with Multiple Sites of Infection
Systemic Toxicity
Clinical Efficacy
Trial of Sulfamethoxazole-Trimethoprim for Skin Abscess (NEJM, 2016)MEDLINE]: in skin abscesses at least 2 cm in size which were drained, sulfamethazole-trimethoprim increased cure rate at 7 and 14 days
Wound Cultures were Positive for MRSA in 45% of Cases
Abscess Size of At Least 2 cm is Considered a Useful Threshold Regarding Deciding on Antibiotic Use as Adjunctive Therapy for Skin Abscess
References
Cutaneous abscesses. Anaerobic and aerobic bacteriology and outpatient management. Ann Intern Med. 1977;87(2):145 [MEDLINE] Aerobic and anaerobic bacteriology of subcutaneous abscesses. Br J Surg. 1981;68(7):498 [MEDLINE]
Aerobic and anaerobic bacteriology of wounds and cutaneous abscesses. Arch Surg. 1990;125(11):1445 [MEDLINE]
Bacteriology of skin and soft-tissue infections: comparison of infections in intravenous drug users and individuals with no history of intravenous drug use. Clin Infect Dis. 1995;20 Suppl 2:S279 [MEDLINE]
Practice Guidelines for the Diagnosis and Management of Skin and Soft Tissue Infections: 2014 Update by the Infectious Diseases Society of America. Clin Infect Dis. 2014 Jul 15;59(2):e10-52. doi: 10.1093/cid/ciu444 [MEDLINE]
Management of Skin Abscesses in the Era of Methicillin-Resistant Staphylococcus aureus. N Engl J Med 2014; 370:1039-1047March 13, 2014DOI: 10.1056/NEJMra1212788 [MEDLINE]
The Massachusetts abscess rule: a clinical decision rule using ultrasound to identify methicillin-resistant Staphylococcus aureus in skin abscesses. Acad Emerg Med. 2014 May;21(5):558-67. doi: 10.1111/acem.12379 [MEDLINE]
Trimethoprim-Sulfamethoxazole versus Placebo for Uncomplicated Skin Abscess. N Engl J Med. 2016;374(9):823 [MEDLINE]