

Definitions of Skin/Soft Tissue Infections
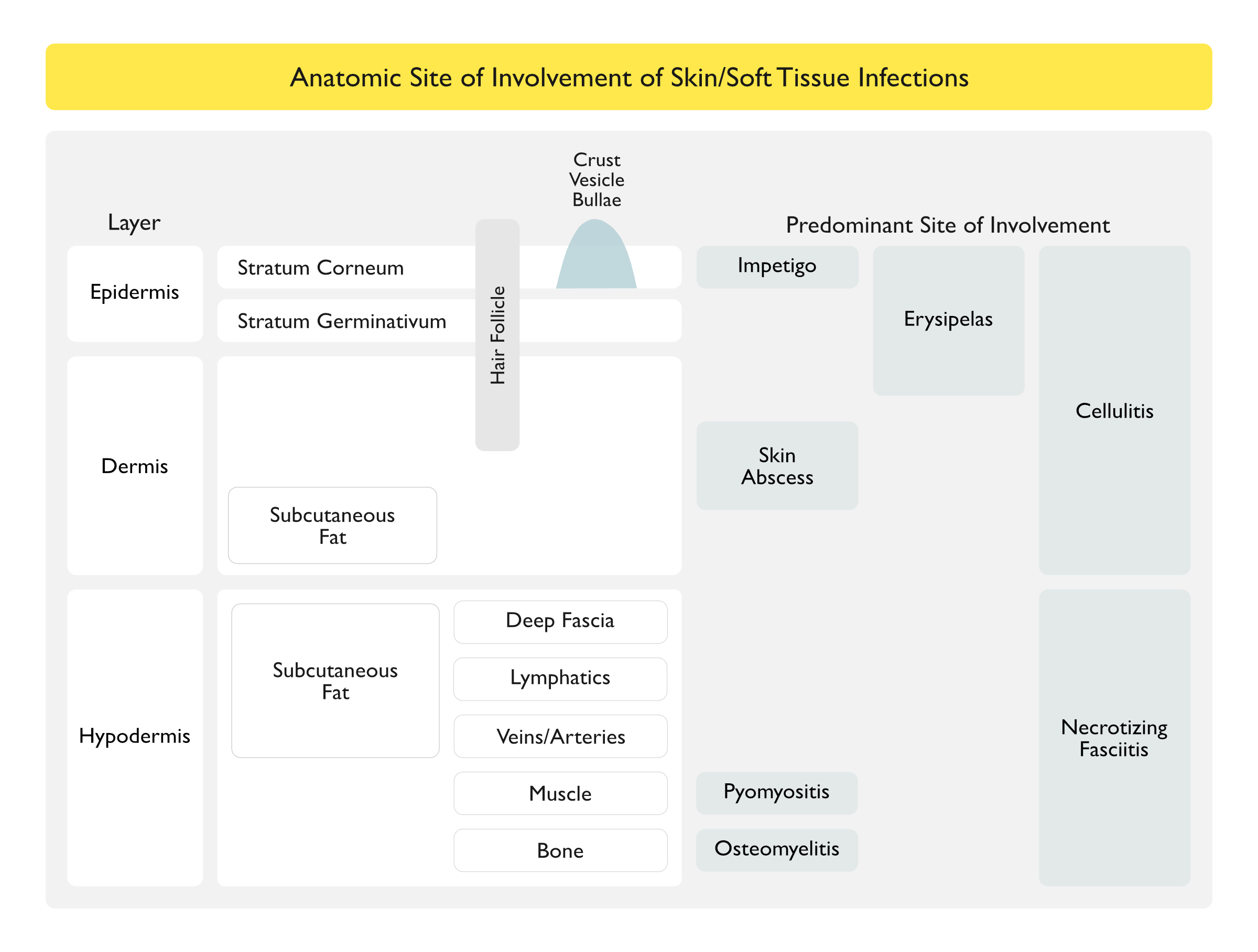
- Impetigo (see Impetigo): infection of superficial layers of the epidermis
- Cellulitis (see Cellulitis): skin infection of deeper dermis and subcutaneous fat (resulting from bacterial breach of the skin) characterized by erythema, warmth, and edema without an underlying suppurative focus
- Erysipelas (see Erysipelas): skin infection of upper dermis and superficial lymphatics (resulting from bacterial breach of the skin) characterized by erythema, warmth, and edema without an underlying suppurative focus
- Furuncle (Boil) (see Skin Abscess): infection of hair follicle where purulent material extends through the dermis into the subcutaneous tissue, forming a small abscess
- Carbuncle (see Skin Abscess): coalescence of several inflamed follicles into a single inflammatory mass with purulent drainage from multiple follicles
- Skin Abscess (see Skin Abscess): collection of pus within dermis and deeper skin tissues
- Necrotizing Soft Tissue Infection (see Necrotizing Soft Tissue Infection): deep tissue infection involving the hypodermis (and contained structures)
- All of These are Characterized by Fulminant Tissue Destruction, Systemic Toxicity (Tachycardia >120 Beats/min, Hypotension, Elevated Creatine Kinase, CRP >15 mg/dL, LRINEC Score >6, etc), and High Mortality Rates

History
- 1861-1865 During the United States Civil War: first description of necrotizing fasciitis by the Confederate Army surgeon, Joseph Jones
- 1883: Fournier described necrotizing fasciitis in the perineal and genital region
- 1952: Wilson first used the term “necrotizing fasciitis”
- Modern Era: lay press commonly refers to the organisms which cause necrotizing soft tissue infection as “flesh-eating bacteria”
Epidemiology
Incidence
- Incidence of Necrotizing Fasciitis is Approximately 0.3-15 Cases per 100,000 Population (NEJM, 2017) [MEDLINE]
Diagnosis
Laboratory Risk Indicator for Necrotizing Soft Tissue Infection (LRINEC)
- C-Reactive Protein (CRP) (mg/L)
- CRP < 150: 0 points
- CRP ≥ 150: 4 points
- White Blood Cell (WBC) Count
- WBC < 15: 0 points
- WBC 15-25: 1 point
- WBC >25: points
- Hemoglobin (Hb) (g/dL)
- Hb >13.6: 0 points
- Hb 11-13.5 : 1 points
- Hb < 10.9: 2 points
- Sodium (Na) (mmol/L)
- Na ≥ 135: 0 points
- Na < 135: 2 points
- Creatinine (Cr) (mg/dL)
- Cr ≤ 1.6: 0 points
- Cr >1.6: 2 points
- Serum Glucose (Glc) (mg/dL)
- Glc ≤ 180: 0 points
- Glc >180: 1 point
- LRINEC Score Represents the Probability of Necrotizing Fasciitis Being Present
- Low Risk (<5 Points): <50% probability of necrotizing fasciitis
- Intermediate Risk (6-7 Points): 50-75% probability of necrotizing fasciitis
- High Risk (>8 points): >75% probability of necrotizing fasciitis
Complete Blood Count (CBC) (see Complete Blood Count)
- Leukocytosis (see Leukocytosis)
X-Rays/Computed Tomography (CT)/Magnetic Resonance Imaging (MRI)
General Comments
- Plain Film Radiographic Studies, CT Scanning, and/or MRI Scanning May Be Useful to Image Soft Tissues (and to Detect Soft Tissue Gas)
- CT Scan is More Sensitive than Plain Film Radiographic Studies for the Detection of Soft Tissue Gas
- Crucially, Obtaining Radiographic Studies Should Not Delay the Definitive Surgical Diagnosis and/or Therapeutic Intervention in Patients with Frank Crepitus on Physical Exam and/or Rapid Clinical Deterioration
Ultrasound with Aspiration of Perifascial Fluid Collections
- May Be Useful
- “Dishwater” Appearance of Fluid
Finger Test
- Procedure: local anesthesia, followed by a 2 cm incision down to the deep fascia with digital exploration
- Lack of Bleeding from the Incision Suggests Necrotizing Fasciitis
- “Dishwater” Fluid Expressed Suggests Necrotizing Fasciitis
- If the Tissues at Level of the Deep Fascia Dissect with Minimal Resistance, the Finger Test is Positive, Suggesting Necrotizing Fasciitis
Tissue Biopsy with Rapid Frozen Section Analysis
- May Demonstrate Obliterative Vasculitis of Subcutaneous Vessels, Acute Inflammation, and Subcutaneous Tissue Necrosis
Clinical
General Comments
- Necrotizing Soft Tissue Infection Includes Any/All of the Following (NEJM, 2017) [MEDLINE]
- Necrotizing Cellulitis
- Involving the Epidermis/Dermis/Subcutaneous Tissue
- Necrotizing Fasciitis
- Distinguishing Necrotizing Fasciitis from Necrotizing Myositis May Be Difficult, Since Skeletal Muscle and Fascia Can Be Involved in Both Syndromes (NEJM, 1989) [MEDLINE] (Scand J Infect Dis, 1992) [MEDLINE] (Emerg Infect Dis, 1995) [MEDLINE]
- Infection Typically Spreads Along the Muscle Fascia Due to its Relatively Poor Blood Supply (In Contrast to Muscle Tissue, Which is Frequently Spared Due to its Better Blood Supply) (Arch Surg, 1986) [MEDLINE]
- Necrotizing Myositis
- Necrotizing Cellulitis
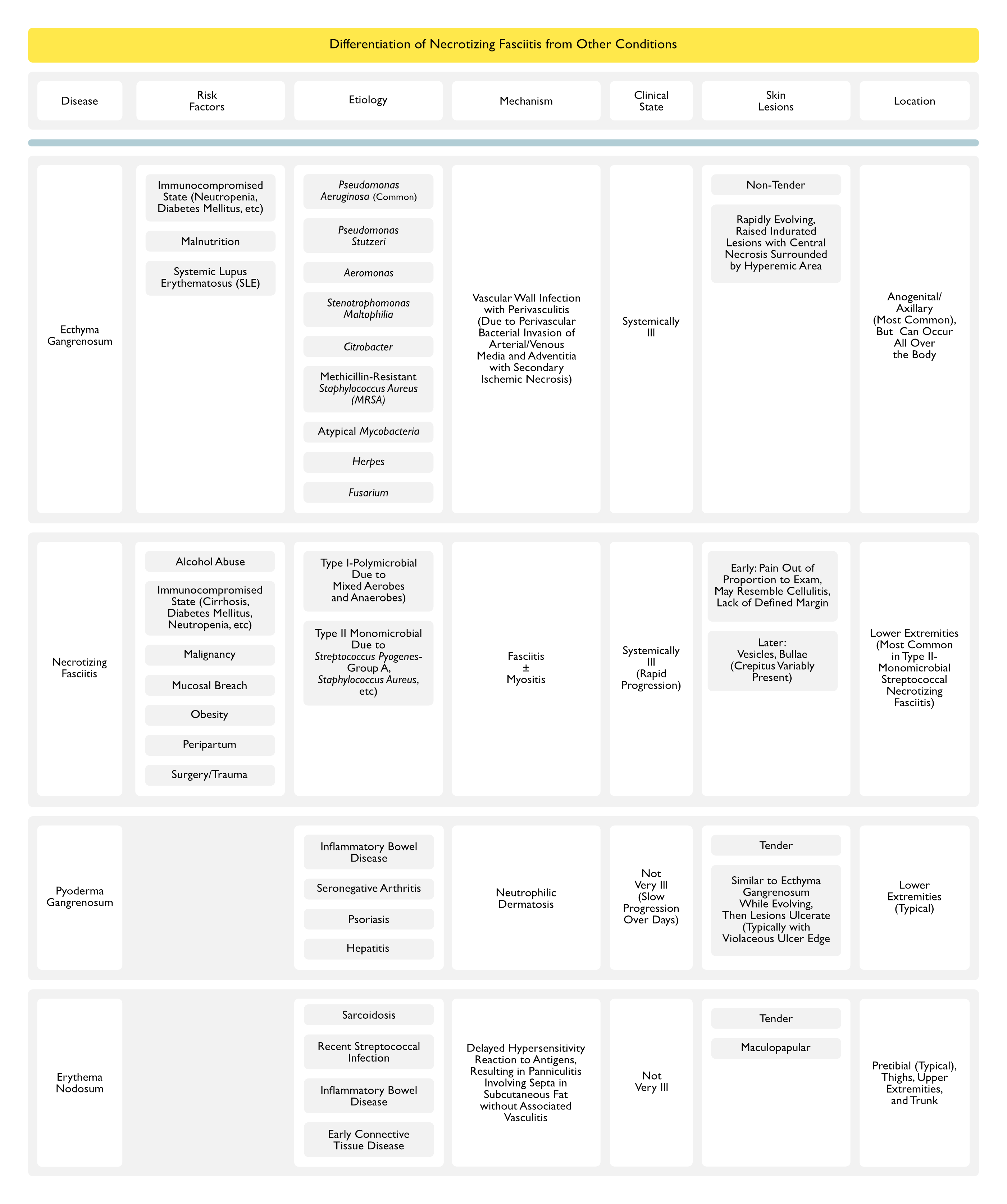
Differentiation of Necrotizing Fasciitis from Other Conditions
Radiologic Presence of Soft Tissue Gas May Allow Clinical Differentiation of Necrotizing Soft Tissue Infections (NEJM, 2017) [MEDLINE]
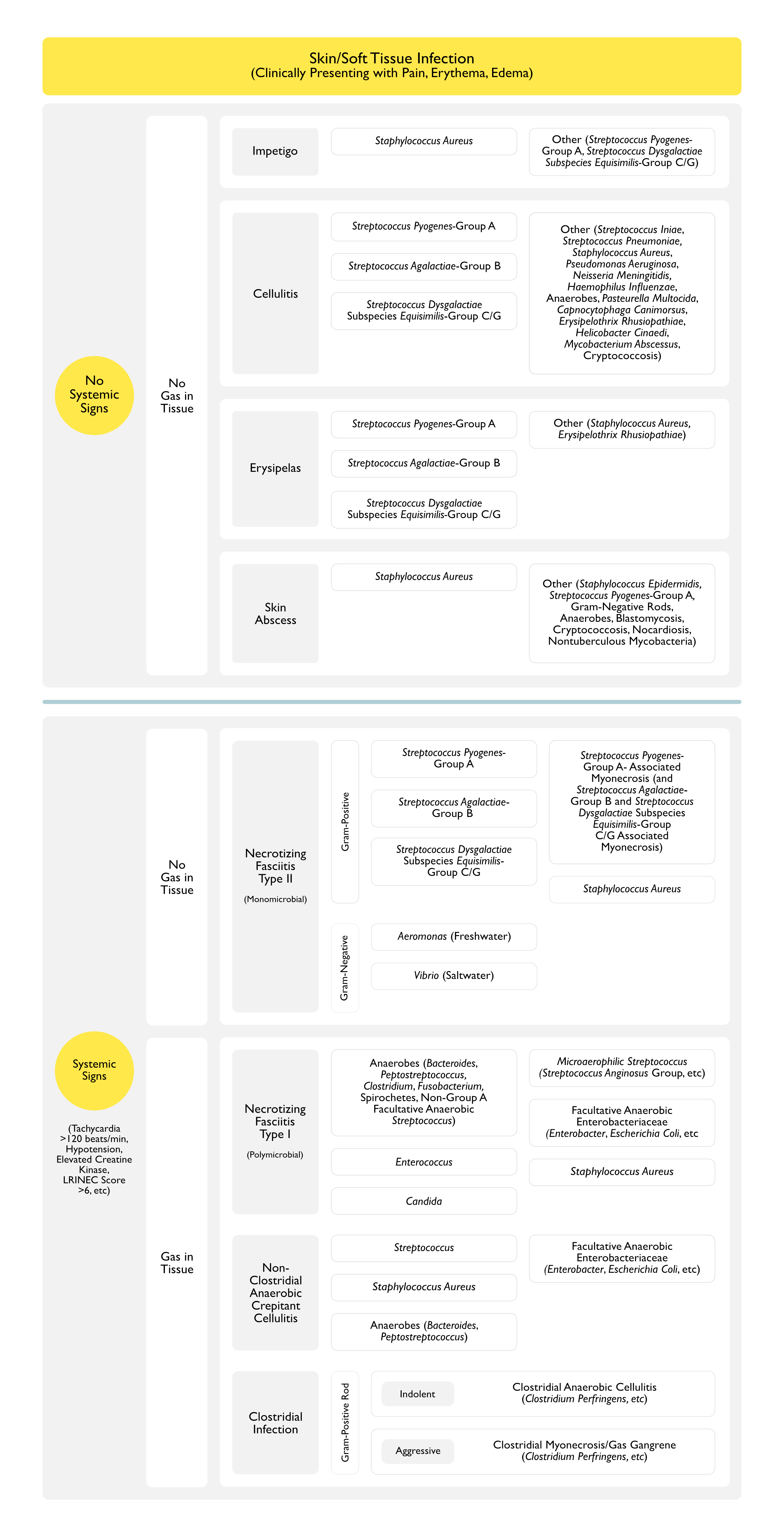
Absence of Soft Tissue Gas on Radiographic Studies
- Necrotizing Fasciitis-Type II (Monomicrobial)
- Gram-Positive Cocci (GPC)
- Necrotizing Fasciitis-Type II (Monomicrobial)
- Streptococcus Pyogenes (Group A) see Streptococcus Pyogenes): β-hemolytic
- Streptococcus Agalactiae (Group B) (see Streptococcus Agalactiae): β-hemolytic
- Streptococcus Dysgalactiae Subspecies Equisimilis (Group C/G) (see Group C+ Group G Streptococcus): β-hemolytic
- Staphylococcus Aureus (Methicillin-Sensitive, MSSA or Methicillin-Resistant, MRSA) (Staphylococcus Aureus)
- Necrotizing Myositis
- Streptococcus Pyogenes (Group A) (see Streptococcus Pyogenes): β-hemolytic
- Streptococcus Agalactiae (Group B) (see Streptococcus Agalactiae): β-hemolytic
- Streptococcus Dysgalactiae Subspecies Equisimilis (Group C/G) (see Group C + Group G Streptococcus): β-hemolytic
- Necrotizing Fasciitis-Type II (Monomicrobial)
- Gram-Negative Rods (GNR)
- Gram-Positive Cocci (GPC)
Presence of Soft Tissue Gas on Radiographic Studies
- Necrotizing Fasciitis-Type I (Polymicrobial)
- Anaerobes
- Bacteroides Fragilis (see Bacteroides Fragilis)
- Clostridium (see Clostridium)
- Fusobacterium (see Fusobacterium)
- Peptostreptococcus (see Peptostreptococcus
- Prevotella (see Prevotella)
- Porphyromonas (see Porphyromonas)
- Spirochetes: such as Treponema Denticola (see Treponema Denticola)
- Microaerophilic Streptococcus
- Streptococcus Anginosus Group (see Streptococcus Anginosus Group)
- Facultative Anaerobes (Can Grow Both in the Presence or Absence of Oxygen)
- Enterobacteriaceae (see Enterobacteriaceae)
- Enterobacter (see Enterobacter)
- Escherichia Coli (see Escherichia Coli)
- Klebsiella (see Klebsiella)
- Proteus (see Proteus)
- Enterococcus (see Enterococcus)
- Non-Group A Facultative Anaerobic Streptococcus (see Streptococcus)
- Enterobacteriaceae (see Enterobacteriaceae)
- Staphylococcus Aureus (see Staphylococcus Aureus)
- Candida (see Candida)
- Anaerobes
- Nonclostridial Anaerobic Crepitant Cellulitis
- Anaerobes
- Bacteroides (see Bacteroides)
- Peptostreptococcus (see Peptostreptococcus)
- Streptococcus (see Streptococcus)
- Staphylococcus Aureus (see Staphylococcus Aureus)
- Facultative Anaerobic Enterobacteriaceae
- Enterobacter (see Enterobacter)
- Escherichia Coli (see Escherichia Coli)
- Klebsiella (see Klebsiella)
- Proteus (see Proteus)
- Anaerobes
- Clostridial Infection
- Gram-Positive Rods (GPR)
- Clostridial (Anaerobic) Cellulitis: indolent clinical presentation
- Clostridium Perfingens (see Clostridium Perfingens): more common
- Clostridium Septicum (see Clostridium Septicum): less common
- Clostridial Myonecrosis (Gas Gangrene): acute clinical presentation
- Clostridium Perfingens (see Clostridium Perfingens): accounts for 80% of cases
- Clostridium Septicum (see Clostridium Septicum)
- Clostridium Novyii (see Clostridium Novyii)
- Clostridium Histolyticum (see Clostridium Histolyticum)
- Clostridium Bifermentans (see Clostridium Bifermentans)
- Clostridium Tertium (see Clostridium Tertium)
- Clostridium Fallax (see Clostridium Fallax)
- Clostridium Sordellii (see Clostridium Sordellii)
- Clostridial (Anaerobic) Cellulitis: indolent clinical presentation
- Gram-Positive Rods (GPR)
Clinical Pattern-No Gas In Tissue
Type II Necrotizing Fasciitis (Monomicrobial)
Streptococcal Gangrene
- Epidemiology
- Age: can occur in any age group
- Most Cases are Community-Acquired
- Most Cases Occur in Patients without Underlying Co-Morbid Conditions (in Contrast to Type I Necrotizing Fasciitis Cases) (J Bone Joint Surg Am, 2003) [MEDLINE]
- Of the 3.5 Cases Per 100,00 Population of Invasive Streptococcus Pyogenes Cases in the US (8,950-11,500 Cases of Invasive Streptococcus Pyogenes Infections Annually in the US), Necrotizing Fasciitis Accounts for Approximately 6% of These Cases (Clin Infect Dis, 2007) [MEDLINE]
- Incidence: appears to be increasing since 1985
- Risk Factors (NEJM, 2017) [MEDLINE]
- Alcohol Abuse (see Ethanol)
- Blunt Trauma (Strain. Sprain, Contusion)
- Exposure to a Known Case
- Immunosuppression
- Diabetes Mellitus (DM) (see Diabetes Mellitus)
- Cirrhosis (see Cirrhosis)
- Human Immunodeficiency Virus (HIV) (see Human Immunodeficiency Virus)
- Neutropenia (see Neutropenia)
- Malignancy
- Major Penetrating Trauma
- Mucosal Breach
- Hemorrhoids (see Hemorrhoids)
- Rectal Fissure (see Rectal Fissure)
- Nonsteroidal Anti-Inflammatory Drugs (NSAID’s) (see Nonsteroidal Anti-Inflammatory Drug)
- Controversial Predisposing Factor for Necrotizing Soft Tissue Infection (NEJM, 2017) [MEDLINE]
- Regardless of Their Association with Causation, NSAID’s May Mask the Clinical Symptoms/Signs in Necrotizing Soft Tissue Infection, Which May Delay Diagnosis
- Obesity (see Obesity)
- Peripheral Arterial Disease (PAD) (see Peripheral Arterial Disease)
- Recent Surgery (Including Colonic Procedure, Urologic Procedure, and Gynecologic Procedure, Neonatal Circumcision)
- Reproductive
- Childbirth
- Endometritis (see Endometritis)
- Episiotomy (see Episiotomy)
- Pregnancy (see Pregnancy)
- Pregnancy Loss/Miscarriage (see Pregnancy Loss)
- Skin Breach
- Burns (see Burns)
- Insect Bite
- Intravenous Drug Abuse (IVDA) (see Intravenous Drug Abuse)
- Skin Laceration
- Varicella-Zoster Virus (Chickenpox) (see Varicella-Zoster Virus)
- Sodium-Glucose Cotransporter-2 (SGLT-2) Inhibitors Use in Diabetes Mellitus (see Sodium-Glucose Cotransporter-2 Inhibitors)
- Increased Risk of Fournier’s Gangrene
- Microbiology
- Streptococcus Pyogenes (Group A) (see Streptococcus Pyogenes)
- β-Hemolytic
- M-Protein is an Important Determinant of Virulence (with M Type 1 and 3 Being Associated with Streptococcal Toxic Shock Syndrome in 50% of Cases) (Clin Infect Dis, 2007) [MEDLINE]
- Strains with These M-Proteins Can Produce Pyrogenic Exotoxins, Which Induce Cytokine Production (Contributing to Shock, Tissue Destruction, and Organ Failure)
- Streptococcus Pyogenes is the Most Common Streptococcus Species Associated with Necrotizing Soft Tissue Infection
- Concomitant Streptococcus Pyogenes and Staphylococcus Infection May Occur in Some Cases (see Staphylococcus Aureus)
- Streptococcus Agalactiae (Group B) (see Streptococcus Agalactiae)
- β-Hemolytic
- Some Reported Cases
- Streptococcus Pyogenes (Group A) (see Streptococcus Pyogenes)
- Physiology
- Cases with Defined Portal of Entry: 50% of cases
- Infection Usually Enters Through Penetrating Trauma or Cutaneous Site of Infection
- Early Findings
- Signs of Superficial Skin Infection
- Later Findings
- Purple (Violaceous) Bullae
- Skin Sloughing
- Once Infection Reaches the Deep Fascia, it Rapidly Spreads Along Fascial Planes, Through Venous Channels and Lymphatics
- Cases with No Defined Portal of Entry: 50% of cases (NEJM, 2017) [MEDLINE]
- Asymptomatic/Symptomatic Pharyngitis Likely Results in Subsequent Hematogenous Dissemination to a Site of Non-Penetrating Minor Trauma (Such as a Bruise or Muscle Strain)
- Early Findings
- Severe Pain
- Fever (without Signs of Superficial Skin Infection) (see Fever)
- Later Findings
- Purple (Violaceous) Bullae
- Skin Sloughing
- Cases with Defined Portal of Entry: 50% of cases
- Clinical Sites of Infection
- Lower Extremities
- Approximately 66% of Cases Occur in the Lower Extremities (Especially in Patients with Underlying Diabetes Mellitus and Peripheral Arterial Disease)
- Necrotizing Fasciitis of the Head and Neck
- While Most Head and Neck Necrotizing Soft Tissue Infections are Type I-Polymicrobial (See Below), Some Cases May Be Type II-Monomicrobial (Associated with Streptococcus Pyogenes)
- Predisposed by Breach in the Oropharyngeal Mucous Membrane Due to Surgery, Instrumentation, or Odontogenic Infection (see Deep Neck Infection) (Head Neck, 2018) [MEDLINE]
- Most Cases (78%) are of Dental Origin (Clin Infect Dis, 1995) [MEDLINE]
- Fasciitis May Spread to Face, Lower Neck, or Mediastinum (Clin Infect Dis, 1995) [MEDLINE]
- Mediastinal Spread is Predisposed by Prior Corticosteroid Use, Infection by Gas-Producing Organism, or Pharyngeal Focus of Infection (Ann Thorac Surg, 2012) [MEDLINE]
- Lower Extremities
- Clinical Manifestations
- Early Findings
- Early Anesthesia in the Affected Area May Occur (Due to in the thrombosis of Small Blood Vessels and Destruction of the Superficial Nerves in the Subcutaneous Tissues)
- Initially, the Overlying Tissue May Appear Unaffected (For This Reason, Necrotizing Fasciitis is Difficult to Diagnose without Direct Visualization of the Fascia)
- Erythema (Without Sharp Margins): present in 72% of cases (NEJM, 2017) [MEDLINE]
- Severe Pain Over Skin and Underlying Muscle Out of Proportion to the Exam: present in 72% of cases (NEJM, 2017) [MEDLINE]
- This is a Sensitive, Early Finding Which May Precede Development of Fever and Other Constitutional Symptoms (Chest, 2005) [MEDLINE]
- Crepitus (see Skin Crepitus): present in 50% of cases (NEJM, 2017) [MEDLINE]
- Fever (see Fever): may be absent early, but is present in 60% of cases (NEJM, 2017) [MEDLINE]
- Brawny Edema Which May Extend Beyond the Area of Erythema: present in 75% of cases (NEJM, 2017) [MEDLINE]
- Subcutaneous Tissues May Feel Wooden/Hardened with Loss of Palpable Separation of Fascial Planes and Muscle Groups (Clin Infect Dis, 2014) [MEDLINE]
- Vesicular Skin Lesions (see Vesicular-Bullous-Pustular Skin Lesions): may occur
- Lymphangitis/Lymphadenopathy (see Lymphadenopathy): infrequent
- Later Findings
- Dark Red Induration of Skin
- Skin Bullae (Often Filled with Blue/Purple Fluid)/Necrosis/Ecchymosis: present in 38% of cases (NEJM, 2017) [MEDLINE]
- Late Findings
- Friable Bluish/Maroon/Necrotic Black Skin (Due to Extensive Thrombosis of Blood Vessels in Dermal Papillae)
- Brownish/Gray Skin (Due to Extension into the Deep Fascia)
- Extremity Compartment Syndrome (see Extremity Compartment Syndrome): due to myonecrosis
- Systemic Symptoms
- Early Findings
Staphylococcal Necrotizing Fasciitis
- Epidemiology
- Community-Acquired Methicillin-Resistance Staphylococcus Aureus (CA-MRSA) Has Been Associated with Necrotizing Fasciitis (NEJM, 2005) [MEDLINE]
- Risk Factors
- Diabetes Mellitus (DM) (see Diabetes Mellitus)
- Insect Bite
- Intravenous Drug Abuse (IVDA) with Subcutaneous Injection of Black Tar Heroin (see Intravenous Drug Abuse)
- Peripheral Arterial Disease (PAD) (see Peripheral Arterial Disease)
- Skin Laceration
- Surgery/Trauma
- Microbiology
- Staphylococcus Aureus (see Staphylococcus Aureus)
- Associated with Strains of Methicillin-Resistant Staphylococcus Aureus (MRSA) Which Produce the Panton-Valentine Leukocidin (PVL) Toxin
- Concomitant Streptococcus Pyogenes and Staphylococcus Infection May Occur in Some Cases (As Noted Above)
- Staphylococcus Aureus (see Staphylococcus Aureus)
- Physiology
- Once Infection Reaches the Deep Fascia, There is Rapid Spread Along Fascial Planes, Through Venous Channels and Lymphatics
- Clinical
- Early Findings
- Severe Pain Over Skin and Underlying Muscle: sensitive, early finding that may precede development of fever and other constitutional symptoms [MEDLINE]
- Fever (see Fever): may be absent early
- Brawny Edema: may extend beyond the area of erythema
- Subcutaneous tissues may feel wooden/hardened with loss of feeling of fascial planes and muscle groups
- Vesicular Skin Lesions: may occur
- Crepitus (see Skin Crepitus): may occur
- Later Findings
- Dark Red Induration of Skin
- Bullae Filled with Blue/Purple Fluid
- Late Findings
- Friable Bluish/Maroon/Black Skin (due to extensive thrombosis of blood vessels in dermal papillae)
- Brownish/Gray Skin (due to extension into the deep fascia)
- Septic Shock/Multiorgan Failure (see Sepsis)
- Early Findings
Necrotizing Myositis
- Epidemiology
- Microbiology
- Streptococcus Pyogenes (Group A) (see Streptococcus Pyogenes)
- Other β-Hemolytic Streptococcus (see Streptococcus Agalactiae)
Aeromonas Hydrophila-Associated Necrotizing Fasciitis (see Aeromonas Hydrophila)
- Epidemiology
- Associated with Traumatic Injuries in Freshwater
- Clinical
- XXXXXXX
Vibrio Vulnificus-Associated Necrotizing Fasciitis (see Vibrio Vulnificus)
- Epidemiology
- Associated with Traumatic Injuries in Seawater
- In Patients with Cirrhosis, it is Associated with Ingestion of Contaminated Oysters
- Portal of Entry
- Breach of Skin/Mucosa
- Clinical
- XXXXXXXX
Bacteroides-Associated Necrotizing Fasciitis (see Bacteroides)
- Epidemiology
- Monomicrobial Necrotizing Fasciitis Cases Have Been Reported
- However, Despite These Cases Being Monomicrobial, They are Not Typically Classified as Type II Necrotizing Fasciitis
- Risk Groups
- Diabetes Mellitus (see Diabetes Mellitus)
- Immunocompromised State
- Obesity (see Obesity)
- Postoperative State
- Pre-Existing, Chronic Organ Dysfunction
- Monomicrobial Necrotizing Fasciitis Cases Have Been Reported
Escherichia Coli-Associated Necrotizing Fasciitis (see Escherichia Coli)
- Epidemiology
- Monomicrobial Necrotizing Fasciitis Cases Have Been Reported
- However, Despite These Cases Being Monomicrobial, They are Not Typically Classified as Type II Necrotizing Fasciitis
- Risk Groups
- Diabetes Mellitus (see Diabetes Mellitus)
- Immunocompromised State
- Obesity (see Obesity)
- Postoperative State
- Pre-Existing, Chronic Organ Dysfunction
- Monomicrobial Necrotizing Fasciitis Cases Have Been Reported
Clinical Pattern-Gas In Tissue
Type I Necrotizing Fasciitis (Polymicrobial, Involving Both Aerobes and Anaerobes)
Epidemiology
- Alternative Names
- Progressive Bacterial Synergistic Gangrene
- Synergistic Necrotizing Cellulitis
- Type I is the Most Common Type of Necrotizing Fasciitis
- Risk Factors
- Diabetes Mellitus (DM) (see Diabetes Mellitus): most commonly involving the lower extremity
- Immunocompromised State
- Obesity (see Obesity)
- Peripheral Arterial Disease (PAD) (see Peripheral Arterial Disease): most commonly involving the lower extremity
- Surgery/Trauma
Microbiology
- General Comments
- Mixed Aerobic and Anaerobic Infection: multiple organisms can be isolated from almost all of these cases (there is an average of 5 pathogens in each wound)
- At Least One Anaerobe is Isolated in Conjunction with Enterobacteriaceae and One or More Non-Group A Facultative Anaerobic Streptococcus Species (J Clin Microbiol, 1995) [MEDLINE] (J Bone Joint Surg Am, 2003) [MEDLINE] (Clin Infect Dis, 2007) [MEDLINE]
- Obligate Aerobes (Such as Pseudomonas Aeruginosa) are Rarely Present in Such Infections
- Mixed Aerobic and Anaerobic Infection: multiple organisms can be isolated from almost all of these cases (there is an average of 5 pathogens in each wound)
- Anaerobes
- Bacteroides Fragilis (see Bacteroides Fragilis)
- Clostridium (see Clostridium)
- Fusobacterium (see Fusobacterium)
- Peptostreptococcus (see Peptostreptococcus
- Prevotella (see Prevotella)
- Porphyromonas (see Porphyromonas)
- Spirochetes
- Treponema Denticola (see Treponema Denticola)
- Microaerophilic Streptococcus (Streptococcus Anginosus Group, etc) (see Streptococcus)
- Facultative Anaerobes (Can Grow Both in the Presence or Absence of Oxygen)
- Enterobacteriaceae (see Enterobacteriaceae)
- Enterobacter (see Enterobacter)
- Escherichia Coli (see Escherichia Coli)
- Klebsiella (see Klebsiella)
- Proteus (see Proteus)
- Enterococcus (see Enterococcus)
- Non-Group A Facultative Anaerobic Streptococcus (see Streptococcus)
- Enterobacteriaceae (see Enterobacteriaceae)
- Staphylococcus Aureus (see Staphylococcus Aureus)
- Candida (see Candida)
- Presence of Fungi in Polymicrobial Necrotizing Soft Tissue Infection Increases the Probability of Requiring ≥2 Surgical Interventions and is Associated with a 3-Fold Increase in Mortality Rate (Surg Infect-Larchmt, 2017) [MEDLINE]
Clinical Sites of Infection
- Lower Extremity Necrotizing Fasciitis
- Epidemiology
- Most Common Site in Cases Associated with Diabetes Mellitus and Peripheral Arterial Disease
- Epidemiology
- Necrotizing Fasciitis of the Head and Neck
- Portal of Entry
- Breach in the Oropharyngeal Mucous Membrane Due to Surgery, Instrumentation, or Odontogenic Infection (see Deep Neck Infection) (Head Neck, 2018) [MEDLINE]
- Most Cases (78%) are of Dental Origin (Clin Infect Dis, 1995) [MEDLINE]
- Breach in the Oropharyngeal Mucous Membrane Due to Surgery, Instrumentation, or Odontogenic Infection (see Deep Neck Infection) (Head Neck, 2018) [MEDLINE]
- Microbiology
- Most Cases are Due to Mixed Aerobic and Anaerobic Infection (Clin Infect Dis, 1995) [MEDLINE]
- Oral Anaerobes
- Anaerobic Streptococcus (see Streptococcus)
- Fusobacterium (see Fusobacterium)
- Bacteroides (see Bacteroides)
- Spirochetes
- Treponema Denticola (see Treponema Denticola)
- Clinical
- Portal of Entry
- Ludwig’s Angina (see Ludwig’s Angina)
- Physiology
- Submandibular Space Infection
- Physiology
- Fournier’s Gangrene (Perineal Necrotizing Soft Tissue Infection)
- Sex
- Most Common in Older Males
- Female Cases May Occur in the Setting of Diabetes Mellitus (see Diabetes Mellitus)
- Risk Factors
- Diabetes Mellitus (DM) (see Diabetes Mellitus)
- Penetating Abdominal Injury
- Peripheral Arterial Disease (PVD) (see Peripheral Arterial Disease)
- Sodium-Glucose Cotransporter-2 (SGLT-2) Inhibitors Use in Diabetes Mellitus (see Sodium-Glucose Cotransporter-2 Inhibitors)
- Increased Risk of Fournier’s Gangrene
- Surgery
- Physiology
- Breach in Gastrointestinal/Genitourinary Tract or Labia: by diverticulum, malignancy, hemorrhoid, anal fissure/perianal abscess, Bartholin abscess, episiotomy, vulvovaginal infection, decubitus ulcer, or urethral tear
- Once Infection Reaches the Deep Fascia of Perineum, Rapid Spread Along Fascial Planes, Through Venous Channels and Lymphatics to Involve the Anterior Abdominal Wall/Gluteal Muscles/Scrotum/Penis
- Microbiology (Br J Surg, 2000) [MEDLINE]
- Anaerobes
- Bacteroides (see Bacteroides)
- Clostridium (see Clostridium)
- Fusobacterium (see Fusobacterium)
- Anaerobic/Microaerophilic Streptococcus (see Streptococcus)
- Facultative Anaerobes (Can Grow Both in the Presence or Absence of Oxygen)
- Enterobacteriaceae (ee Enterobacteriaceae)
- Enterobacter (see Enterobacter)
- Escherichia Coli (see Escherichia Coli)
- Klebsiella (see Klebsiella)
- Proteus (see Proteus)
- Enterococcus (see Enterococcus)
- Anaerobes
- Clinical
- Fever (see Fever): early finding
- Abrupt Onset of Severe Pain Over Skin and Underlying Muscle
- This is a Sensitive, Early Finding Which May Precede the Development of Fever (Chest, 2005) [MEDLINE]
- Crepitus (see Skin Crepitus): may occur
- Labial Edema (see Labial Edema)
- Penile Edema (see Penile Edema)
- Scrotal Swelling (see Scrotal Edema)
- Vesicular Skin Lesions (see Vesicular-Bullous-Pustular Skin Lesions): may occur
- Extension into Perineum/Abdominal Wall/Lower Extremities (with Skin Findings, as Noted for Other Presentations)
- Myositis (Occurs Concomitantly in 20-40% of Cases): elevated CK (see Myositis)
- Septic Shock/Multiorgan Failure (see Sepsis)
- Treatment: early aggressive drainage/debridement (may require cystostomy, colostomy, or orchiectomy)
- Sex
- Surgical Wound Infection
- Clinical
- Copious Drainage
- Dusky, Friable Subcutaneous Tissue with Pale, Devitalized Fascia
- Clinical
- Neonatal Necrotizing Fasciitis
- Clinical
- Usually Associated with Omphalitis (Most Commonly), Balanitis (Associated with Circumcision), Mammitis, or Fetal Monitoring
- Most Commonly Involves the Abdomen/Perineum
- Clinical
Non-Clostridial Anaerobic Necrotizing Cellulitis
- Epidemiology
- Risk Factors
- Diabetes Mellitus (DM) (see Diabetes Mellitus)
- Risk Factors
- Microbiology: non-spore forming anaerobic bacteria with/without facultative organisms
- Non-Spore Forming Anaerobes
- Bacteroides (see Bacteroides)
- Peptostreptococcus (see Peptostreptococcus)
- Facultative Anaerobes (Can Grow Both in the Presence or Absence of Oxygen)
- Enterobacteriaceae (ee Enterobacteriaceae)
- Enterobacter (see Enterobacter): facultative anaerobe
- Escherichia Coli (see Escherichia Coli): facultative anaerobe
- Klebsiella (see Klebsiella): facultative anaerobe
- Proteus (see Proteus): facultative anaerobe
- Staphylococcus (see Staphylococcus)
- Streptococcus (see Streptococcus)
- Enterobacteriaceae (ee Enterobacteriaceae)
- Non-Spore Forming Anaerobes
- Clinical
- Gradual Onset with Subsequent Rapid Spread
- Pain/Swelling/Systemic Toxicity are Not Prominent Features
- Milder Clinical Illness Distinguishes this from True Gas Gangrene
- Thin, Dark, Foul-Smelling Wound Drainage (Which May Contain Fat Globules)
- Tissue Gas Formation (see Skin Crepitus)
- Sparing of Fascia and Deep Muscle
Clostridial Infection
Clostridial Anaerobic Necrotizing Cellulitis
- Microbiology
- Clostridium Perfringens (see Clostridium Perfringens)
- Most Common Etiology
- Typically Associated with Trauma
- Clostridium Septicum (see Clostridium Septicum)
- Less Frequent Etiology
- Typically Spontaneous (without Associated Predisposing Condition)
- Clostridium Sordellii (see Clostridium Sordellii)
- Typically Associated with Gynecologic Etiology
- Clostridium Perfringens (see Clostridium Perfringens)
- Physiology
- Portal of Entry
- Spread of Infection from Bowel to Perineum/Abdominal Wall/Lower Extremities
- Surgical Contamination
- Trauma
- Portal of Entry
- Clinical
- Gradual Onset with Subsequent Rapid Spread
- Pain/Swelling/Systemic Toxicity are Not Prominent Features
- Milder Clinical Illness Distinguishes this from True Gas Gangrene
- Thin, Dark, Foul-Smelling Wound Drainage: may contain fat globules
- Tissue Gas Formation (see Skin Crepitus)
- Sparing of Fascia and Deep Muscle
- Treatment
- Surgical Exploration/Debridement is Required to Distinguish Anaerobic Cellulitis from Fasciitis and Myonecrosis
Clostridial Myonecrosis (Gas Gangrene)
- Traumatic Gas Gangrene
- Epidemiology
- Trauma Accounts for 70% of Clostridial Gas Gangrene Cases and 80% of These are Due to Clostridium Perfringens (Mol Microbiol, 1995) [MEDLINE]
- Traumatic Gas Gangrene was Common During the Civil War, World War I, and World War II (Due to Delayed Treatment of Injuries
- In the Modern Era, Delayed Treatment of Injuries (During Earthquakes, etc) Still Results in High Traumatic Gas Gangrene Mortality Rates
- In an Earthquake in China, the Average Time from Injury to Medical Treatment was 3.5 Days and 20% of Those with Open Wounds Developed Clostridium Perfringens Gas Gangrene (with a 50-8% Mortality Rate) (Chin Med J-Engl, 2013) [MEDLINE]
- Risk Factors
- Black Tar Heroin Injection (Skin Popping): associated with Clostridium Novyii and Clostridium Sordellii (MMWR Morb Mortal Wkly Rep, 2000) [MEDLINE] (Clin Infect Dis, 2006) [MEDLINE]
- Bowel/Biliary Tract Surgery
- Intramuscular Injection
- Reproductive
- Abortion
- Pregnancy Loss/Miscarriage/Intrauterine Fetal Demise (see Pregnancy Loss)
- Retained Placenta
- Prolonged Rupture of Membranes
- Trauma
- Compound Fracture
- Crush Injury
- Gunshot Wound
- Knife Wound
- Microbiology: while traumatic gas gangrene may have other microbes isolated from the site of trauma, Clostridium are considered the major organisms causing tissue destruction
- Clostridium Perfringens (see Clostridium Perfringens): accounts for 80% of cases
- Clostridium Septicum (see Clostridium Septicum)
- Clostridium Novyii (see Clostridium Novyii)
- Clostridium Histolyticum (see Clostridium Histolyticum)
- Clostridium Bifermentans (see Clostridium Bifermentans)
- Clostridium Tertium (see Clostridium Tertium)
- Clostridium Fallax (see Clostridium Fallax)
- Clostridium Sordellii (see Clostridium Sordellii)
- Physiology
- Trauma Introduces Clostridium Organisms (Vegetative or Spore Forms) Directly into Deep Tissue
- Traumatic Vascular Injury with Compromised Blood Supply Creates an Anaerobic Environment (with Low Oxidation-Reduction Potential and an Acidic pH) Which Facilitates the Growth of Clostridium (Mol Microbiol, 1995) [MEDLINE]
- Clostridium Perfringens Secretes Many Extracellular Toxins (Alpha Toxin is a Hemolytic Toxin with Both Phospholipase C and Sphingomyelinase Activities, Theta Toxin, aka Perfringolysin O, is a Pore-Forming Toxin)
- Tissue Necrosis Can Occur within Hours of the Initial Injury and Progresses Rapidly (Inches Per Hour) in the Absence of Adequate Treatment
- Severe Muscle Necrosis and Absent Neutrophils from the Site (In Contrast to Staphylococcus Aureus Infection, Where There is an Absence of Adjacent Tissue/Vascular Destruction and Neutrophils are Abundant)
- Due to Large Heterotypic Aggregates of Activated Platelets (Caused by Alpha Toxin Activation of the Platelet Glycoprotein IIb/IIIa Fibrinogen Receptor), Neutrophils Accumulate Along the Capillary/Small Arteriole/Postcapillary Venule Endothelium, But are Unable to Cross the Vascular Endothelium into the Infected Tissue (Br Med J, 1917) [MEDLINE]
- Alpha and Theta Toxins are Also Cytotoxic to Neutrophils
- Alpha Toxin Directly Inhibits Myocardial Contractility, Resulting in a Decrease in Cardiac Output ( J Infect Dis, 1988) [MEDLINE] (J Infect Dis, 1995) [MEDLINE]
- Theta Toxin Decreases Systemic Vascular Resistance (SVR) (Via the Actions of Vasodilatory Prostacyclin, Platelet Activating Factor, and Other Lipid Autocoids), Resulting in “Warm Shock” ( J Infect Dis, 1988) [MEDLINE] (J Biol Chem, 1989) [MEDLINE] (J Infect Dis, 1995) [MEDLINE]
- The Combined Effects of Alpha Toxin Depressing Cardiac Output and Theta Toxin Causing Vasodilation Results in Severe Hemodynamic Compromise
- Alpha and Theta Toxins Directly Cause Hemolysis (Ann Hematol, 1993) [MEDLINE] (J Infect Dis, 1995) [MEDLINE]
- Diagnosis
- Complete Blood Count (CBC) (see Complete Blood Count)
- Hemolytic Anemia (see Hemolytic Anemia): typically brisk
- Blood Culture (see Blood Culture)
- X-Ray/CT Scan/MRI: useful to detect gas in soft tissues
- Needle Aspiration/Punch Biopsy: diagnostic in 20% of cases (however, biopsy does not address the need for surgical debridement)
- Complete Blood Count (CBC) (see Complete Blood Count)
- Clinical
- Sudden Onset of Severe Pain at the Site of Surgery or Trauma (Due to Toxin-Mediated Ischemia) (NEJM, 1973) [MEDLINE]
- Mean Incubation Period (Which Depends on the Size of the Bacterial Inoculum and the Degree of Vascular Compromise): <24 hrs (Range: 6 hrs-Several Days)
- Skin Initially May Appear Pale
- Then Rapidly Develops a Bronze Color, Followed by Purple-Red Discoloration
- Skin Then Becomes Tense and Exquisitely Tender
- Skin Crepitus (see Skin Crepitus): most sensitive and specific examination finding (Arch Surg, 1986) [MEDLINE]
- Skin Bullae May Be Clear, Red, Blue, or Purple (see Vesicular-Bullous-Pustular Skin Lesions)
- Rhabdomyolysis (see Rhabdomyolysis)
- Systemic Toxicity (Tachycardia, Fever, Hypotension/Sepsis, Multiorgan Failure) Develops Rapidly (see Sepsis)
- Shock is Present in 50% of Case at the Time of Presentation to the Hospital (J Trauma, 1983) [MEDLINE]
- Hemolytic Anemia (see Hemolytic Anemia): typically brisk
- Acute Kidney Injury (AKI) (see Acute Kidney Injury)
- Due to Hemoglobinuria (from Hemolysis)/Myoglobinuria (from Rhabdomyolysis) and Probable Bacterial Toxin Effects on Renal Tubular Cells
- Hepatic Necrosis (see Acute Liver Failure)
- Sudden Onset of Severe Pain at the Site of Surgery or Trauma (Due to Toxin-Mediated Ischemia) (NEJM, 1973) [MEDLINE]
- Treatment
- Antibiotics
- Preferred Empiric Regimen is Piperacillin-Tazobactam (4.5 g IV q8hrs) (or Carbapenem) + Clindamycin (900 mg IV q8hrs)
- Preferred Definitive Regimen is Penicillin (3-4 million U IV q4hrs) + Clindamycin (900 mg IV q8hrs) or Tetracycline (500 mg IV q6hrs)
- Surgical Exploration: edematous and reddish/blue/black muscle, which does not bleed or contract when stimulated
- Tissue Gram Stain and Culture: large gram-variable rods at site of injury (can appear as either Gram-positive and Gram-negative rods when stained directly from infected tissues, but stain as Gram-positive rods when obtained from culture media)
- Tissue Pathology: widespread tissue destruction, muscle necrosis (necrosis of skin, fat, subcutaneous tissue, and fascia may also be present), presence of organisms, and absence of neutrophils in the tissue
- Booster Tetanus Vaccine (if Not Received within the Last 5 Years)
- Hyperbaric Oxygen (HBO) (see Hyperbaric Oxygen): controversial
- Antibiotics
- Prognosis
- Prognosis for Gas Gangrene of an Extremity is Better than for Gas Gangrene of the Trunk or Visceral Organs (Due to Ease of Debridement)
- Survival Rate with Proper Antibiotics + Debridement + Hyperbaric Oxygen Has Been Reported to Be 81% (J Trauma, 1983) [MEDLINE]
- Presence of Bacteremia and Hemolysis Predicts the Highest Likelihood of Progression to Shock and Death
- Recurrent Gas Gangrene Due to Clostridium Perfringens Has Been Observed in Patients with Minor Trauma at a Site of Prior Gas Gangrene (Likely Related to Spores Residing for a Prolonged Period in Tissue Which was Not Adequately Debrided) (West J Med, 1988) [MEDLINE]
- Epidemiology
- Spontaneous Gas Gangrene
- Risk Factors
- Advanced Human Immunodeficiency Virus (HIV)/Acquired Immune Deficiency Syndrome (AIDS) (see Human Immunodeficiency Virus)
- Chemotherapy
- Colonic Malignancy (see Colon Cancer)
- Diverticulitis (see Diverticulitis)
- Gastrointestinal Surgery
- Inflammatory Bowel Disease (see Crohns Disease and Ulcerative Colitis)
- Leukemia (see Acute Myeloid Leukemia and Acute Lymphocytic Leukemia)
- Lymphoproliferative Disorders
- Necrotizing Enterocolitis/Cecitis/Distal Ileitis
- Neutropenia (see Neutropenia)
- Radiation Therapy (see Radiation Therapy)
- Microbiology
- Clostridium Septicum (see Clostridium Septicum): most cases
- Clostridium Tertium (see Clostridium Tertium)
- Physiology
- Congenital/Cyclic Neutropenia (see Neutropenia)
- Use of Contaminated Musculoskeletal Allografts (Tendons, Menisci, Femoral Condyles) Harvested from Cadaveric Tissues
- Hematogenous Seeding of Muscle with Bacteria from a Gastrointestinal Port of Entry (Typically Colon Adenocarcinoma) (see Colon Cancer)
- Usually Clostridium Septicum (see Clostridium Septicum)
- Clostridium Tertium (see Clostridium Tertium): typically resistant to penicillin, cephalosporins, and clindamycin, allowing survival in the gastrointestinal tract (especially in patients who have received broad-spectrum antibiotics)
- Prior Abdominal Radiation Therapy (see Radiation Therapy)
- Diagnosis
- Blood Culture (see Blood Culture): useful, since Clostridium Septicum bacteremia usually precedes skin manifestations by several hours
- Gram Stain of Bullae Fluid May Be Useful to Identify Gram-Positive Rods (Characteristic of Clostridium)
- Surgical Exploration
- Clinical (Rev Infect Dis, 1990) [MEDLINE]
- Distinguishing Spontaneous Clostridial Gas Gangrene from Streptococcal Myonecrosis May Be Difficult, But the Presence of Tissues Crepitus Favors the Diagnosis of Clostridial Infection
- Abrupt Onset of Severe Muscle Pain (see Myalgias)
- Pathologic Features Include Muscle Cell Lysis and Absent Inflammatory Cells (Rev Infect Dis, 1990) [MEDLINE]
- Muscle Heaviness
- Numbness
- Malaise (see Malaise): may occur early in some cases
- Confusion (see Obtundation-Coma): may occur early in some cases
- Edema and Bullae Filled with Clear, Cloudy, Hemorrhagic, or Purplish Fluid (see Vesicular-Bullous-Pustular Skin Lesions)
- Treatment
- Empiric Antibiotics (to Cover for Streptococcus Pyogenes, Clostridium, and Mixed Aerobes/Anaerobes): preferred regimen is piperacillin-tazobactam (4.5 g IV q8hrs) + clindamycin (900 mg IV q8hrs)
- Definitive Antibiotics for Clostridium Septicum: penicillin (3-4 million U IV q4hrs) + clindamycin (900 mg IV q8hrs) or tetracycline (500 mg IV q6hrs)
- Definitive Antibiotics For Clostridium Tertium: vancomycin or metronidazole are preferred agents
- Early Surgical Debridement
- Empiric Antibiotics (to Cover for Streptococcus Pyogenes, Clostridium, and Mixed Aerobes/Anaerobes): preferred regimen is piperacillin-tazobactam (4.5 g IV q8hrs) + clindamycin (900 mg IV q8hrs)
- Prognosis: mortality of spontaneous gangrene is 67-100% ( Ann Chir Gynaecol, 1986) [MEDLINE] (Cancer, 1991) [MEDLINE]
- Risk Factors
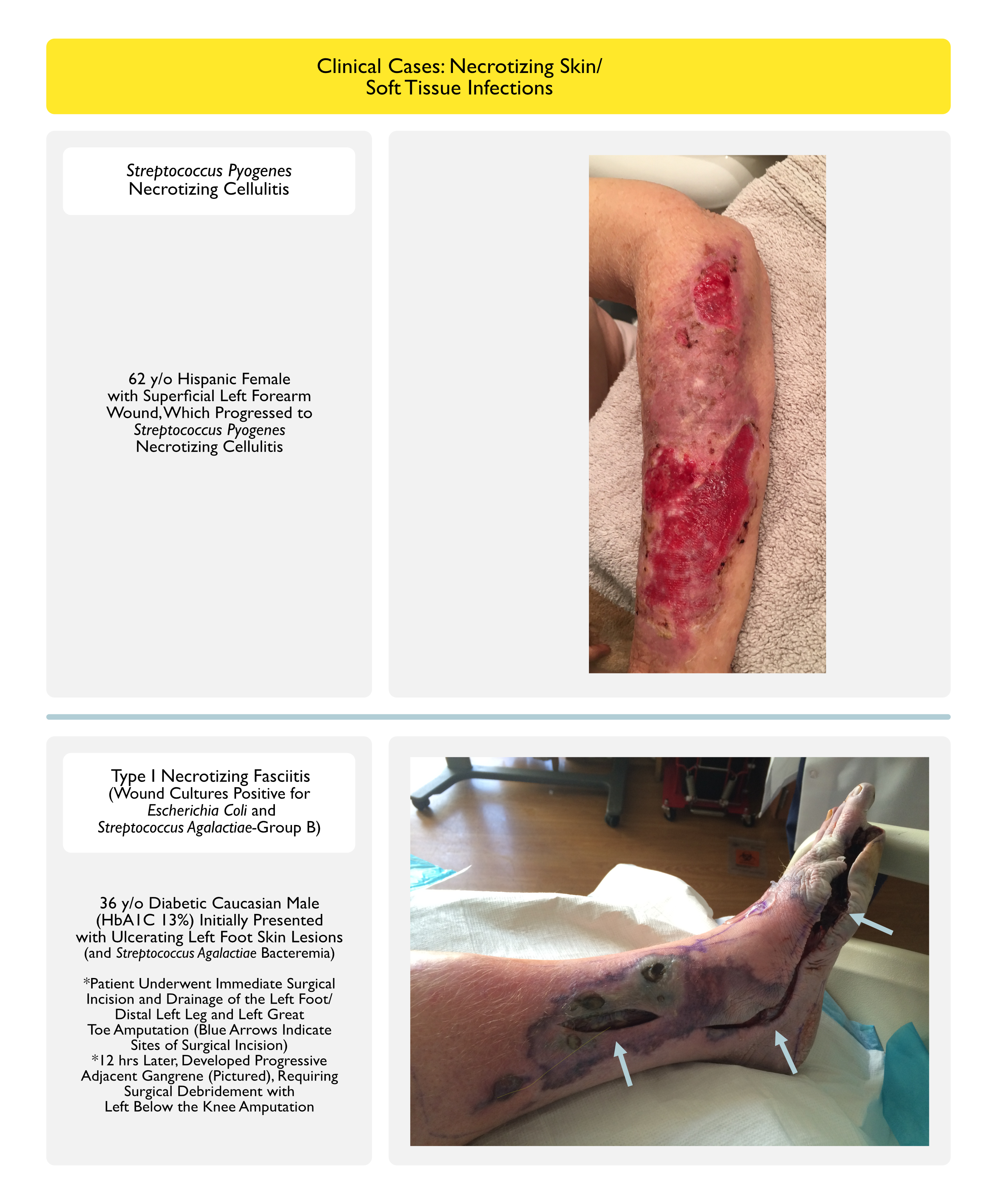
Clinical Cases
Treatment
Antibiotics
- Clindamycin (see Clindamycin)
- Unlike penicillin, the efficacy of clindamycin is not affected by the inoculum size or stage of bacterial growth
- Clindamycin suppresses bacterial toxin synthesis
- Subinhibitory concentrations of clindamycin facilitate Strep Pyogenes phagocytosis
- Clindamycin decreases the synthesis of penicillin-binding protein, which, in addition to being a target for penicillin, is also an enzyme involved in cell wall synthesis and degradation
- Clindamycin has a longer postantibiotic effect than β-lactams (such as penicillin)
- Clindamycin suppresses LPS-induced mononuclear synthesis of tumor necrosis factor-α
- Vancomycin (see Vancomycin): or comparable agent, to cover for possible MRSA
- Gram-Negative Coverage: also useful
Intravenous Immunoglobulin (IVIG) (see Intravenous Immunoglobulin)
- Reported in the Treatment of Streptococcal Toxic Shock Syndrome (see Streptococcal Toxic Shock Syndrome): may have a role in Streptococcus-associated necrotizing faasciitis cases (although this is not an FDA-approved indication)
Prompt Surgical Debridement Down to Fascia with Wide Excision
- Early surgical intervention has been demonstrated to improve mortality and decrease tissue loss (amputation, etc).
- Delayed surgical intervention is associated with increased risk of death [MEDLINE]
- Average latency from admission to surgery in survivors: 25 hrs
- Average latency from admission to surgery in non-survivors: 90 hrs
- Delayed surgical intervention is associated with increased risk of death [MEDLINE]
Hyperbaric Oxygen (HBO) (see Hyperbaric Oxygen)
- Unclear Benefit in Necrotizing Fasciitis
Treatment of Septic Shock (see Sepsis)
- Standard Measures
Prognosis
- Death: may occur if necrotizing fasciitis is not promptly recognized and treated
References
General
- The Method of Spread of Gas Gangrene into Living Muscle. Br Med J. 1917;1(2944):726.4 [MEDLINE]
- The histotoxic clostridial infections of man. Bacteriol Rev. 1962;26:177 [MEDLINE]
- Peracute spontaneous streptococcal myositis. A report on 2 fatal cases with review of literature. Acta Chir Scand. 1971;137(2):155 [MEDLINE]
- Gas gangrene. N Engl J Med. 1973;289(21):1129 [MEDLINE]
- Spontaneous streptococcal myositis associated with disseminated intravascular coagulopathy. J Am Osteopath Assoc. 1977;76(9):675 [MEDLINE]
- Gas gangrene. J Trauma. 1983;23(11):991 [MEDLINE]
- Streptococcal myositis. Arch Intern Med. 1985;145(6):1020 [MEDLINE]
- Spontaneous clostridial myonecrosis. A collective review and report of a case. Ann Chir Gynaecol. 1986;75(5):274 [MEDLINE]
- Necrotizing fasciitis. Arch Surg. 1986;121(2):233 [MEDLINE]
- Spontaneous gangrenous myositis induced by Streptococcus pyogenes: case report and review of the literature. Rev Infect Dis. 1987;9(2):382 [MEDLINE]
- Spontaneous gas gangrene at a site of remote injury–localization due to circulating antitoxin. West J Med. 1988;148(2):204 [MEDLINE]
- Lethal effects and cardiovascular effects of purified alpha- and theta-toxins from Clostridium perfringens. J Infect Dis. 1988;157(2):272 [MEDLINE]
- Severe group A streptococcal infections associated with a toxic shock-like syndrome and scarlet fever toxin A. N Engl J Med. 1989;321(1):1 [MEDLINE]
- The regulation of platelet-activating factor production in endothelial cells. The role of calcium and protein kinase C. J Biol Chem. 1989;264(11):6325 [MEDLINE]
- Streptococcal myositis. Scand J Infect Dis. 1992;24(5):661 [MEDLINE]
- Spontaneous, nontraumatic gangrene due to Clostridium septicum. Rev Infect Dis. 1990;12(2):286 [MEDLINE]
- Clostridial bacteremia in cancer patients. A 12-year experience. Cancer. 1991;67(7):1928 [MEDLINE]
- Defining the group A streptococcal toxic shock syndrome. Rationale and consensus definition. The Working Group on Severe Streptococcal Infections. JAMA. 1993;269(3):390 [MEDLINE]
- Investigation of the pathogenesis of massive hemolysis in a case of Clostridium perfringens septicemia. Ann Hematol. 1993;67(3):145 [MEDLINE]
- Necrotising fasciitis due to group A streptococci in western Norway: incidence and clinical features. Lancet. 1994;344(8930):1111 [MEDLINE]
- Cervical necrotizing fasciitis: clinical manifestations and management. Clin Infect Dis. 1995;21(1):51 [MEDLINE]
- Virulence studies on chromosomal alpha-toxin and theta-toxin mutants constructed by allelic exchange provide genetic evidence for the essential role of alpha-toxin in Clostridium perfringens-mediated gas gangrene. Mol Microbiol. 1995;15(2):191 [MEDLINE]
- Clinical and microbiological features of necrotizing fasciitis. J Clin Microbiol. 1995;33(9):2382 [MEDLINE]
- Streptococcal toxic-shock syndrome: spectrum of disease, pathogenesis, and new concepts in treatment. Emerg Infect Dis. 1995;1(3):69 [MEDLINE]
- Effects of Clostridium perfringens recombinant and crude phospholipase C and theta-toxin on rabbit hemodynamic parameters. J Infect Dis. 1995;172(5):1317 [MEDLINE]
- Determinants of mortality for necrotizing soft-tissue infections. Ann Surg. May 1995;221(5):558-63 [MEDLINE]
- Necrotizing fasciitis. Chest. Jul 1996;110:219-29 [MEDLINE]
- Streptococcal infections of skin and soft tissues. N Engl J Med. 1996;334(4):240 [MEDLINE]
- The changing spectrum. Dermatol Clin. Apr 1997;15(2):213-20 [MEDLINE]
- Population-based surveillance for group A streptococcal necrotizing fasciitis: Clinical features, prognostic indicators, and microbiologic analysis of seventy-seven cases. Ontario Group A Streptococcal Study. Am J Med. 1997;103(1):18 [MEDLINE]
- Group B streptococcal necrotizing fasciitis and streptococcal toxic shock-like syndrome in adults. Arch Intern Med. 1998 Aug 10-24;158(15):1704-8 [MEDLINE]
- Fournier’s gangrene: a review of 1726 cases. Br J Surg. 2000;87(6):718[MEDLINE]
- Update: Clostridium novyi and unexplained illness among injecting-drug users–Scotland, Ireland, and England, April-June 2000. MMWR Morb Mortal Wkly Rep. 2000;49(24):543 [MEDLINE]
- Necrotizing fasciitis: clinical presentation, microbiology, and determinants of mortality. J Bone Joint Surg Am. 2003;85-A(8):1454 [MEDLINE]
- Necrotizing fasciitis caused by community-associated methicillin-resistant Staphylococcus aureus in Los Angeles. N Engl J Med. 2005;352(14):1445 [MEDLINE]
- A 46-year-old man with excruciating shoulder pain. Chest. Mar 2005;127(3):1039-44 [MEDLINE]
- Clostridium sordellii infection: epidemiology, clinical findings, and current perspectives on diagnosis and treatment. Clin Infect Dis. 2006 Dec 1;43(11):1436-46. doi: 10.1086/508866 [MEDLINE]
- Necrotizing soft-tissue infection: diagnosis and management. Clin Infect Dis. 2007;44(5):705 [MEDLINE]
- Molecular and clinical characteristics of invasive group A streptococcal infection in Sweden. Clin Infect Dis. 2007;45(4):450 [MEDLINE]
- The epidemiology of invasive group A streptococcal infection and potential vaccine implications: United States, 2000-2004. Clin Infect Dis. 2007;45(7):853 [MEDLINE]
- Group B streptococcal necrotizing fasciitis from a decubitus ulcer. Int J Emerg Med. 2010 Dec; 3(4): 519–520 [MEDLINE]
- Factors associated with the mediastinal spread of cervical necrotizing fasciitis. Ann Thorac Surg. 2012 Jan;93(1):234-8 [MEDLINE]
- Comprehensive treatment for gas gangrene of the limbs in earthquakes. Chin Med J-Engl. 2013;126(20):3833 [MEDLINE]
- Practice Guidelines for the Diagnosis and Management of Skin and Soft Tissue Infections: 2014 Update by the Infectious Diseases Society of America. Clin Infect Dis. 2014 Jul 15;59(2):e10-52. doi: 10.1093/cid/ciu444 [MEDLINE]
- Necrotising soft tissue infection in a UK metropolitan population. Ann R Coll Surg Engl. 2015 Jan;97(1):46-51. doi: 10.1308/003588414X14055925058553 [MEDLINE]
- Fungal Infections Increase the Mortality Rate Three-Fold in Necrotizing Soft-Tissue Infections. Surg Infect (Larchmt). 2017;18(7):793 [MEDLINE]
- Evaluation and Management of Necrotizing Soft Tissue Infections. Infect Dis Clin North Am. 2017;31(3):497 [MEDLINE]
- Necrotizing Soft-Tissue Infections. N Engl J Med. 2017;377(23):2253 [MEDLINE]
- Cervical necrotizing fasciitis: Systematic review and analysis of 1235 reported cases from the literature. Head Neck. 2018;40(9):2094 [MEDLINE]
Diagnosis
- Isolation of Clostridium in human infections: evaluation of 114 cases. J Infect Dis. 1975;131 Suppl:S81 [MEDLINE]
- Anaerobic bacterial bacteremia: 12-year experience in two military hospitals. J Infect Dis. 1989;160(6):1071 [MEDLINE]
- Practice Guidelines for the Diagnosis and Management of Skin and Soft Tissue Infections: 2014 Update by the Infectious Diseases Society of America. Clin Infect Dis. 2014 Jul 15;59(2):e10-52. doi: 10.1093/cid/ciu444 [MEDLINE]
Treatment
- Practice Guidelines for the Diagnosis and Management of Skin and Soft Tissue Infections: 2014 Update by the Infectious Diseases Society of America. Clin Infect Dis. 2014 Jul 15;59(2):e10-52. doi: 10.1093/cid/ciu444 [MEDLINE]